- Ovarian cancer

Содержание
- 2. Epidemiology 225000 new incidence annually worldwide. Incidence stable since 1970s 1600 new cases in Australia in
- 3. Stage at diagnosis and 5-yr survival Stage I Confined to the Ovary 20% 85% IA Growth
- 4. Subtypes Epithelial High grade serous 75% Mucinous 10% Endometrioid 10% Clear cell Low grade serous Germ
- 5. Ovarian Cancer Risk Factors 50 years of age or older Familial factors Family history of breast,
- 6. Ovarian Cancer and Early Detection Certain factors may reduce a woman's risk of developing ovarian cancer
- 7. Lifetime Risk of Cancers Associated With Specific Genes *MMR (mismatch repair) = HNPCC. Chen S, et
- 8. Red Flags for Cancer Susceptibility: BRCA1/BRCA2 Multiple family members with ovarian or breast cancer Age of
- 9. Natural History Precise natural history is poorly understood There is no direct evidence for a premalignant
- 10. Ovarian Ca Screening for general population: PLCO trial 68557 participants 55-74yo w/o prior hx of oophorectomy
- 11. Ovarian Ca screening in ‘high risk grp’ UKFOCCS Phase 1: annual Ca125 and TVUS Sensitivity >80%,
- 12. Ovarian Ca screening Major organisations do not recommend ovarian cancer screening: Poor understanding of natural history
- 13. Management of Ovarian Cancer SURGICAL STAGING AND DEBULKING
- 14. Initial Surgical management Surgery is usually performed upfront regardless of stage: Obtain tissue diagnosis Perform surgical
- 15. Steps in Surgical Staging
- 17. Stage I And II OC: role of adjuvant chemotherapy 8% 5 year improvement in OS was
- 18. Adjuvant Rx for early stage Ovarian Ca NCCN guideline suggests adjuvant chemo in stage 1C or
- 19. Postop Management of advanced ovarian cancer
- 20. Standard: ?Carbo AUC6 + Pacli GOG 111 and OV10: Cisp/Paclitaxel v Cisp/Cyclo showed 11% ARR favouring
- 21. Improving outcome beyond Carbo/Paclitaxel First line Carbo/Paclitaxel showed RR 70-80% with more than 50% achieving CR
- 22. Better schedule for Carbo/Pacli JCOG 3016 trial Lancet 2009;374:1331-1338 637 pts stage II to IV (65%
- 23. Better carbo/taxol schedule MITO-7 JCO 2013;31 suppl;abstr LBA5501 822 pts stage IC to IV (66% SIII,
- 24. ADDING THIRD CYTOTOXIC Rationale: addition of non-cross resistant drug to platinum/paclitaxel combi may improve OS Multiple
- 25. Role of targeted agents: pazopanib AGO-OVAR16: Pazopanib (24m) v placebo in pts who do not have
- 26. Role of Bevacizumab GOG 218: carbo/paclitaxel v CP+Bev 15mg/kg v CP+Bev->Bev 12m maintenance only managed to
- 27. Role of intraperitoneal chemotherapy Rationale: direct delivery of drug into peritoneal cavity increase the dose intensity
- 28. Neoadjuvant chemotherapy
- 29. Consider in women with extensive disease and poor ECOG. No consensus on who should receive NACT.
- 30. Neoadjuvant chemo: MRC CHORUS 550 Pts stage III to IV. 72 centres in UK and 2
- 31. Recurrent ovarian cancer
- 32. Current Questions in Recurrent Disease How do you define recurrence? Physical exam Imaging Chemical When do
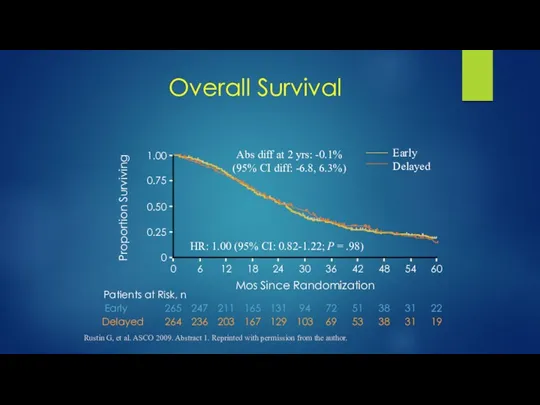
- 33. 264 236 203 167 129 103 69 53 38 31 19 265 247 211 165 131
- 34. Pros & Cons of Treating CA-125 Increase Cons Potential Rx of false positives No improvement in
- 35. Primary Treatment End of Frontline Therapy 0 Mos 6 Mos 12 Mos Refractory Resistant Sensitive Platinum
- 36. Recurrent Ovarian Cancer: Effect of Platinum-Free Interval and Survival Days Percentage Pujade-Lauraine E, et al. ASCO
- 37. 1978 Cisplatin Carboplatin Altretamine Paclitaxel Topotecan Liposomal doxorubicin (PLD) (accelerated) Liposomal doxorubicin (full) Gemcitabine (with carboplatin)
- 38. Positive Trials in Recurrent Ovarian Cancer Paclitaxel vs topotecan[1,2] Topotecan vs pegylated liposomal doxorubicin (PLD)[3,4] Platinum
- 40. Скачать презентацию
Epidemiology
225000 new incidence annually worldwide. Incidence stable since 1970s
1600 new cases
Epidemiology
225000 new incidence annually worldwide. Incidence stable since 1970s
1600 new cases
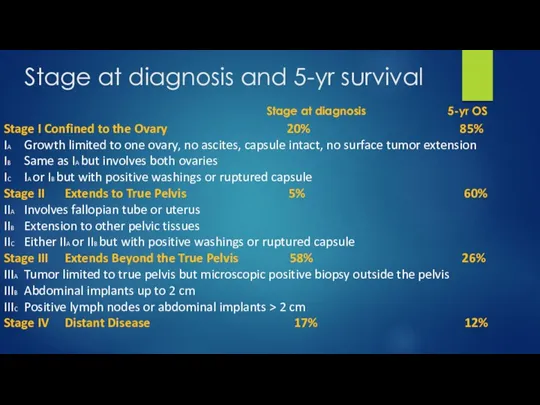
Stage at diagnosis and 5-yr survival
Stage I Confined to the Ovary
Stage at diagnosis and 5-yr survival
Stage I Confined to the Ovary
Subtypes
Epithelial
High grade serous 75%
Mucinous 10%
Endometrioid 10%
Clear cell
Low grade serous
Germ cell/small cell/Krukenberg
Subtypes
Epithelial
High grade serous 75%
Mucinous 10%
Endometrioid 10%
Clear cell
Low grade serous
Germ cell/small cell/Krukenberg
Ovarian Cancer Risk Factors
50 years of age or older
Familial factors
Family history
Ovarian Cancer Risk Factors
50 years of age or older
Familial factors
Family history
Ovarian Cancer and Early Detection
Certain factors may reduce a woman's risk
Ovarian Cancer and Early Detection
Certain factors may reduce a woman's risk
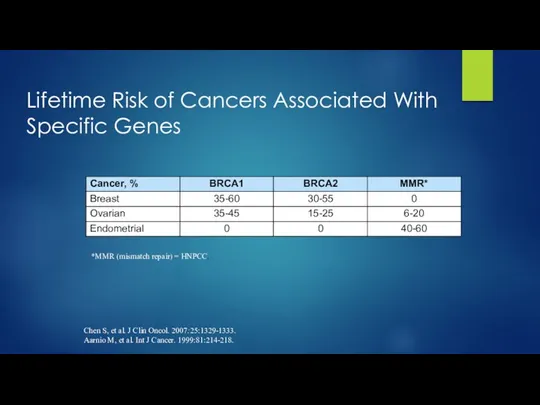
Lifetime Risk of Cancers Associated With Specific Genes
*MMR (mismatch repair) =
Lifetime Risk of Cancers Associated With Specific Genes
*MMR (mismatch repair) =
Red Flags for Cancer Susceptibility: BRCA1/BRCA2
Multiple family members with ovarian or
Red Flags for Cancer Susceptibility: BRCA1/BRCA2
Multiple family members with ovarian or
Natural History
Precise natural history is poorly understood
There is no direct evidence
Natural History
Precise natural history is poorly understood
There is no direct evidence
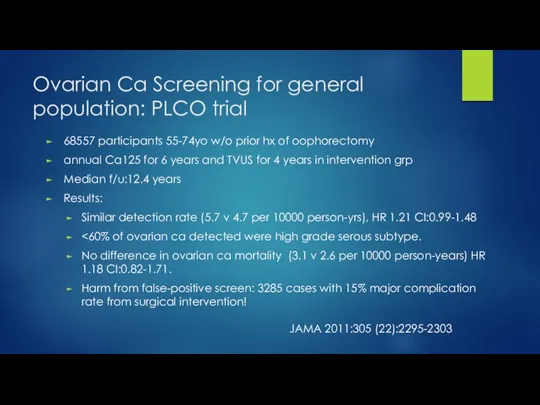
Ovarian Ca Screening for general population: PLCO trial
68557 participants 55-74yo w/o
Ovarian Ca Screening for general population: PLCO trial
68557 participants 55-74yo w/o
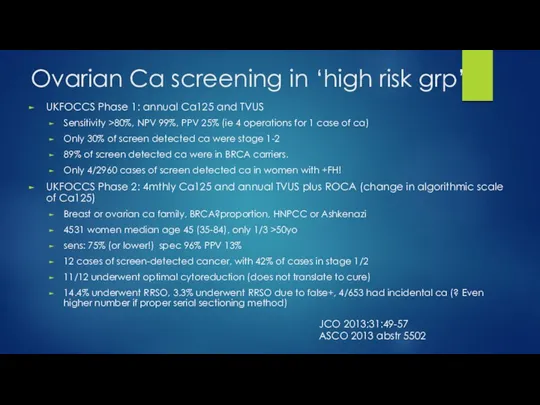
Ovarian Ca screening in ‘high risk grp’
UKFOCCS Phase 1: annual Ca125
Ovarian Ca screening in ‘high risk grp’
UKFOCCS Phase 1: annual Ca125
Ovarian Ca screening
Major organisations do not recommend ovarian cancer screening:
Poor understanding
Ovarian Ca screening
Major organisations do not recommend ovarian cancer screening:
Poor understanding
Management of Ovarian Cancer
SURGICAL STAGING AND DEBULKING
Management of Ovarian Cancer
SURGICAL STAGING AND DEBULKING
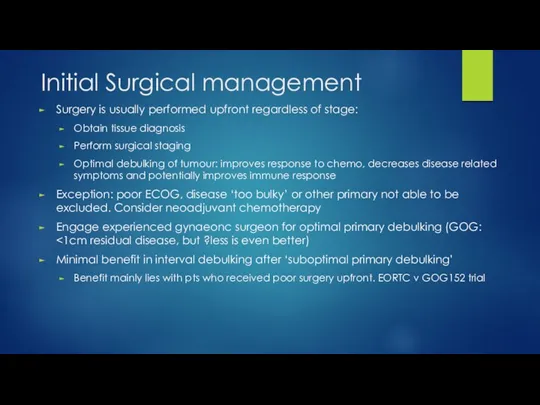
Initial Surgical management
Surgery is usually performed upfront regardless of stage:
Obtain tissue
Initial Surgical management
Surgery is usually performed upfront regardless of stage:
Obtain tissue
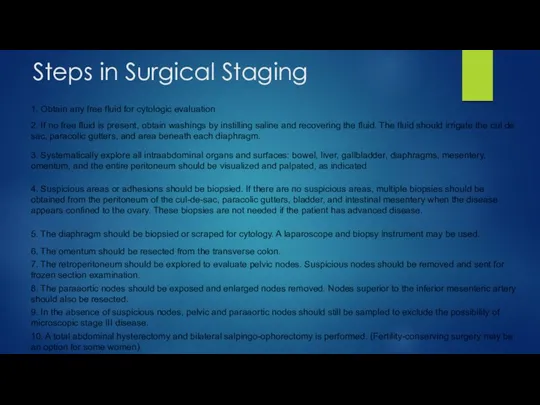
Steps in Surgical Staging
Steps in Surgical Staging
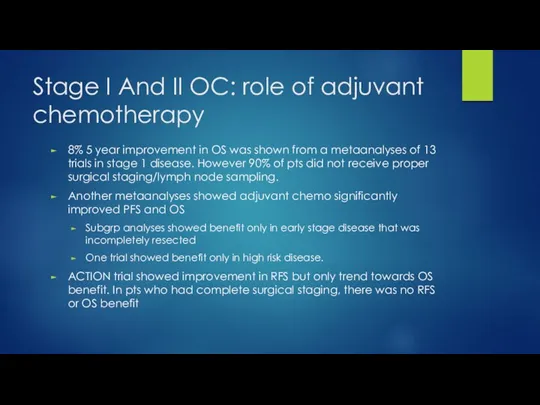
Stage I And II OC: role of adjuvant chemotherapy
8% 5 year
Stage I And II OC: role of adjuvant chemotherapy
8% 5 year
Adjuvant Rx for early stage Ovarian Ca
NCCN guideline suggests adjuvant chemo
Adjuvant Rx for early stage Ovarian Ca
NCCN guideline suggests adjuvant chemo
Postop Management of advanced ovarian cancer
Postop Management of advanced ovarian cancer
Standard: ?Carbo AUC6 + Pacli
GOG 111 and OV10: Cisp/Paclitaxel v Cisp/Cyclo
Standard: ?Carbo AUC6 + Pacli
GOG 111 and OV10: Cisp/Paclitaxel v Cisp/Cyclo
Improving outcome beyond Carbo/Paclitaxel
First line Carbo/Paclitaxel showed RR 70-80% with more
Improving outcome beyond Carbo/Paclitaxel
First line Carbo/Paclitaxel showed RR 70-80% with more
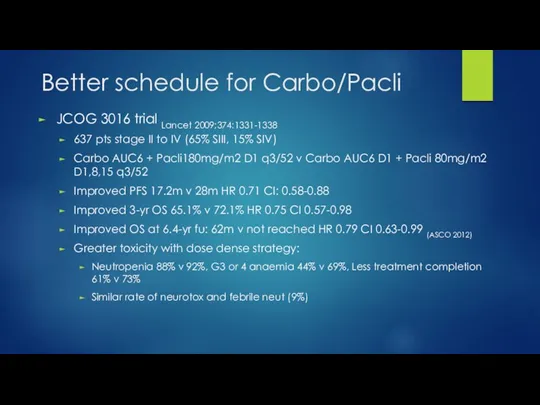
Better schedule for Carbo/Pacli
JCOG 3016 trial Lancet 2009;374:1331-1338
637 pts stage II
Better schedule for Carbo/Pacli
JCOG 3016 trial Lancet 2009;374:1331-1338
637 pts stage II

Better carbo/taxol schedule
MITO-7 JCO 2013;31 suppl;abstr LBA5501
822 pts stage IC to
Better carbo/taxol schedule
MITO-7 JCO 2013;31 suppl;abstr LBA5501
822 pts stage IC to
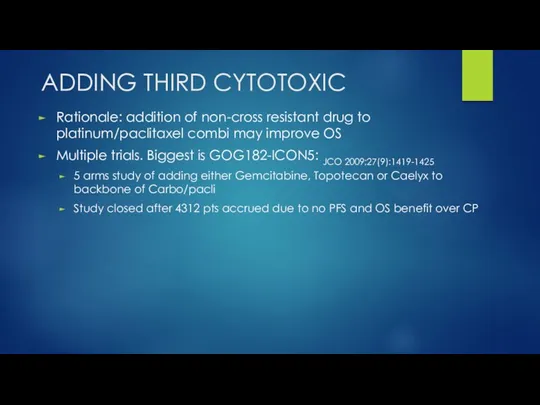
ADDING THIRD CYTOTOXIC
Rationale: addition of non-cross resistant drug to platinum/paclitaxel combi
ADDING THIRD CYTOTOXIC
Rationale: addition of non-cross resistant drug to platinum/paclitaxel combi
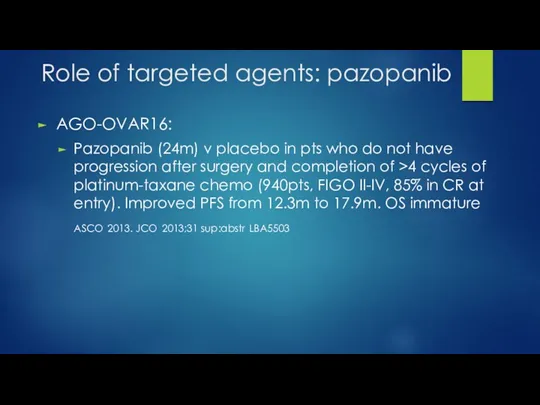
Role of targeted agents: pazopanib
AGO-OVAR16:
Pazopanib (24m) v placebo in pts
Role of targeted agents: pazopanib
AGO-OVAR16:
Pazopanib (24m) v placebo in pts
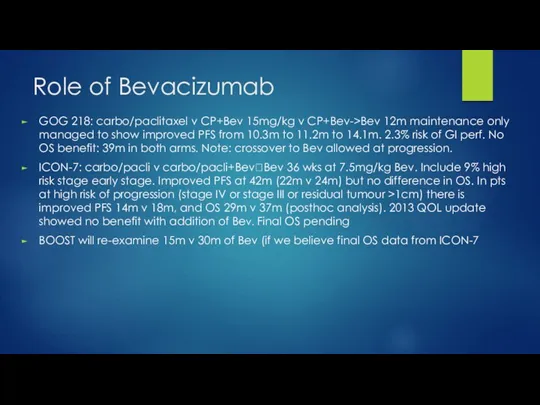
Role of Bevacizumab
GOG 218: carbo/paclitaxel v CP+Bev 15mg/kg v CP+Bev->Bev 12m
Role of Bevacizumab
GOG 218: carbo/paclitaxel v CP+Bev 15mg/kg v CP+Bev->Bev 12m
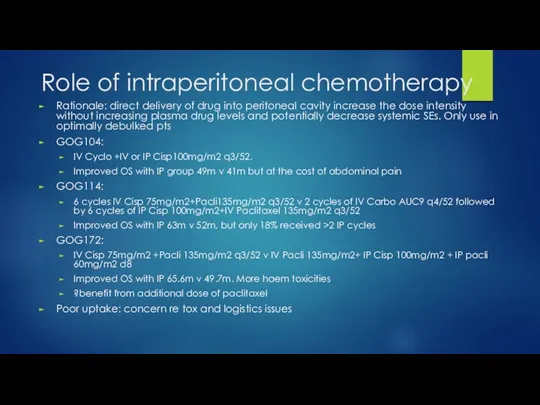
Role of intraperitoneal chemotherapy
Rationale: direct delivery of drug into peritoneal cavity
Role of intraperitoneal chemotherapy
Rationale: direct delivery of drug into peritoneal cavity
Neoadjuvant chemotherapy
Neoadjuvant chemotherapy
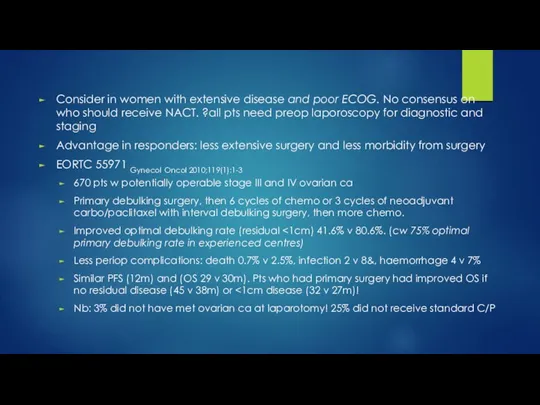
Consider in women with extensive disease and poor ECOG. No consensus
Consider in women with extensive disease and poor ECOG. No consensus
Neoadjuvant chemo: MRC CHORUS
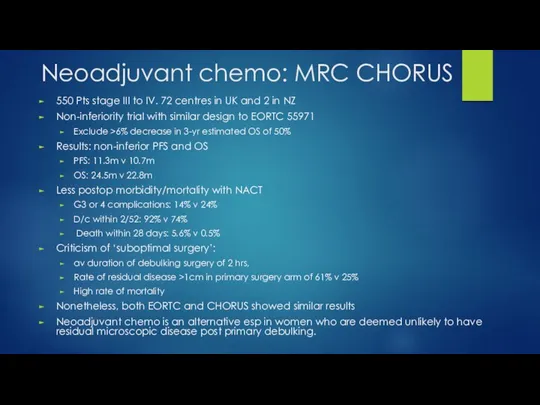
550 Pts stage III to IV. 72 centres
Neoadjuvant chemo: MRC CHORUS
550 Pts stage III to IV. 72 centres
Recurrent ovarian cancer
Recurrent ovarian cancer
Current Questions in Recurrent Disease
How do you define recurrence?
Physical exam
Imaging
Chemical
When do
Current Questions in Recurrent Disease
How do you define recurrence?
Physical exam
Imaging
Chemical
When do
264
236
203
167
129
103
69
53
38
31
19
265
247
211
165
131
94
72
51
38
31
22
Rustin G, et al. ASCO 2009. Abstract 1. Reprinted with permission
264
236
203
167
129
103
69
53
38
31
19
265
247
211
165
131
94
72
51
38
31
22
Rustin G, et al. ASCO 2009. Abstract 1. Reprinted with permission
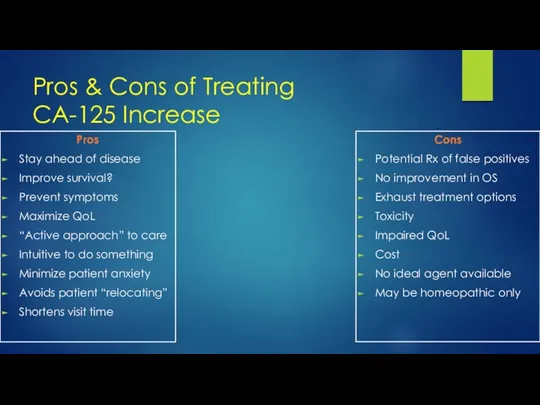
Pros & Cons of Treating
CA-125 Increase
Cons
Potential Rx of false positives
No
Pros & Cons of Treating
CA-125 Increase
Cons
Potential Rx of false positives
No
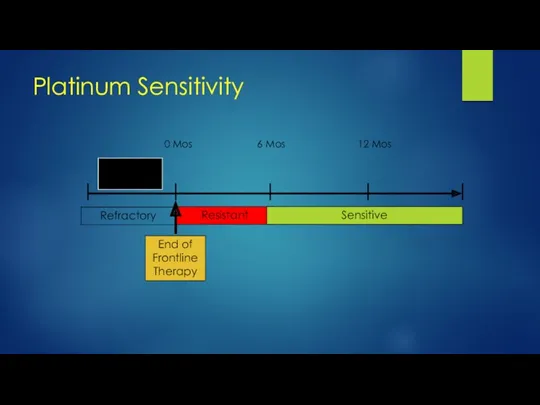
Primary
Treatment
End of
Frontline
Therapy
0 Mos
6 Mos
12 Mos
Refractory
Resistant
Sensitive
Platinum Sensitivity
Primary
Treatment
End of
Frontline
Therapy
0 Mos
6 Mos
12 Mos
Refractory
Resistant
Sensitive
Platinum Sensitivity
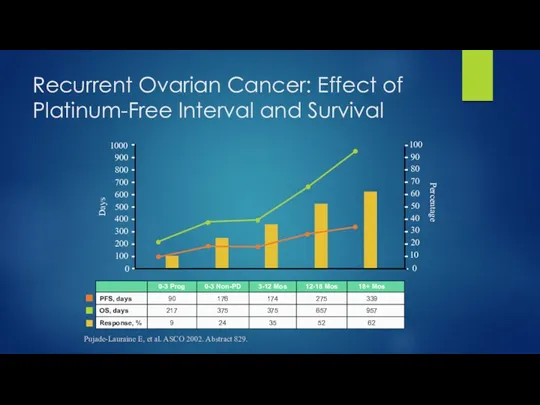
Recurrent Ovarian Cancer: Effect of Platinum-Free Interval and Survival
Days
Percentage
Pujade-Lauraine E, et
Recurrent Ovarian Cancer: Effect of Platinum-Free Interval and Survival
Days
Percentage
Pujade-Lauraine E, et
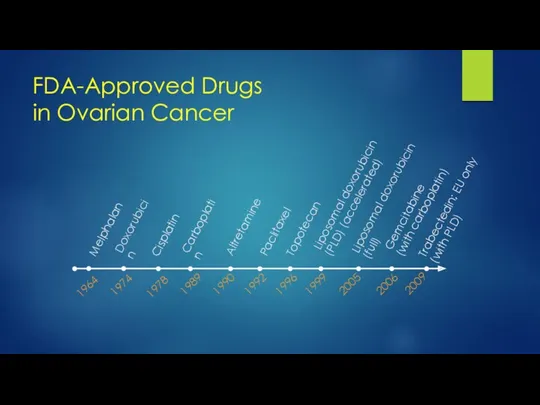
1978
Cisplatin
Carboplatin
Altretamine
Paclitaxel
Topotecan
Liposomal doxorubicin (PLD) (accelerated)
Liposomal doxorubicin (full)
Gemcitabine
(with carboplatin)
2006
1989
1990
1992
1996
1999
2005
2009
Trabectedin; EU only
(with
1978
Cisplatin
Carboplatin
Altretamine
Paclitaxel
Topotecan
Liposomal doxorubicin (PLD) (accelerated)
Liposomal doxorubicin (full)
Gemcitabine
(with carboplatin)
2006
1989
1990
1992
1996
1999
2005
2009
Trabectedin; EU only (with
![Positive Trials in Recurrent Ovarian Cancer Paclitaxel vs topotecan[1,2] Topotecan](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/281807/slide-37.jpg)
Positive Trials in Recurrent
Ovarian Cancer
Paclitaxel vs topotecan[1,2]
Topotecan vs pegylated liposomal doxorubicin
Positive Trials in Recurrent
Ovarian Cancer
Paclitaxel vs topotecan[1,2]
Topotecan vs pegylated liposomal doxorubicin
 Массивная кровопотеря. Современные подходы к интенсивной терапии
Массивная кровопотеря. Современные подходы к интенсивной терапии Фармакогнозия как дисциплина
Фармакогнозия как дисциплина Синдром диабетической стопы
Синдром диабетической стопы Микробиологии, вирусологии и иммунологии
Микробиологии, вирусологии и иммунологии Медико–социальная сущность клонирования
Медико–социальная сущность клонирования Остеохондроз
Остеохондроз Заболевания органов пищеварения у детей
Заболевания органов пищеварения у детей СРС Дәрілік өсімдіктер
СРС Дәрілік өсімдіктер Медицина катастроф. Основные понятия
Медицина катастроф. Основные понятия Противовирусные средства
Противовирусные средства Орбита флегмонасы, орбита веналарының тромбофлебиті, периоститтер этиологиясы, клиникасы, жедел көмек көрсету
Орбита флегмонасы, орбита веналарының тромбофлебиті, периоститтер этиологиясы, клиникасы, жедел көмек көрсету Апное недоношенных детей
Апное недоношенных детей Сотрясение головного мозга
Сотрясение головного мозга Мерез ауруы кезіндегі ауыз қуысының шырышты қабатындағы көріністер
Мерез ауруы кезіндегі ауыз қуысының шырышты қабатындағы көріністер Пожилой пациент: вопросы лекарственного взаимодействия
Пожилой пациент: вопросы лекарственного взаимодействия физиология питания
физиология питания Вывихи и переломы зубов, альвеолярного отростка, методы лечения
Вывихи и переломы зубов, альвеолярного отростка, методы лечения Эректильная дисфункция (ЭД)
Эректильная дисфункция (ЭД) Противокашлевые, отхаркивающие, муколитические средства. Бронхолитические средства
Противокашлевые, отхаркивающие, муколитические средства. Бронхолитические средства Визуальная диагностика при гипоталамо-гипофизарном ожирении
Визуальная диагностика при гипоталамо-гипофизарном ожирении Функціональні зміни в організмі при фізичних навантаженнях
Функціональні зміни в організмі при фізичних навантаженнях Теоретические и методологические основы управления персоналом лечебно-профилактического учреждения
Теоретические и методологические основы управления персоналом лечебно-профилактического учреждения Особенности ухода медицинской сестры в послеоперационном периоде после операции на брюшной полости
Особенности ухода медицинской сестры в послеоперационном периоде после операции на брюшной полости Трофобластическая болезнь
Трофобластическая болезнь Түбір өзектерін толтыруға арналған пломбалық жадығаттар.Жіктелуі, қолдану көрсеткіштері
Түбір өзектерін толтыруға арналған пломбалық жадығаттар.Жіктелуі, қолдану көрсеткіштері Моногибридті будандастыру. Гибридологиялық зерттеу әдісі
Моногибридті будандастыру. Гибридологиялық зерттеу әдісі Анализ номенклатуры препаратов силденафила, применяемых при лечении эректильной дисфункции
Анализ номенклатуры препаратов силденафила, применяемых при лечении эректильной дисфункции Некардиогенный отек легких. Респираторный дистресс-синдром
Некардиогенный отек легких. Респираторный дистресс-синдром