- Esophageal Cancer

Содержание
- 2. Esophageal Cancer Epidemiology and Risk Factors Diagnosis — signs, symptoms, and tests Work-up Treatment Overview Future
- 3. Epidemiology Over 15,000 patients per year in the United States and 7th leading cause of cancer
- 4. Incidence of Esophageal Cancer
- 5. Adenocarcinoma: Barrett’s Esophagus Likely related to chronic GERD, obesity. Pathway of malignant progression. 40 to 125
- 6. Barrett’s Esophagus and Esophageal Cancer ENDOSCOPIC IMAGE OF BARRETT'S ESOPHAGUS WITH PERMISSION TO PLACE IN PUBLIC
- 7. Adenocarcinoma
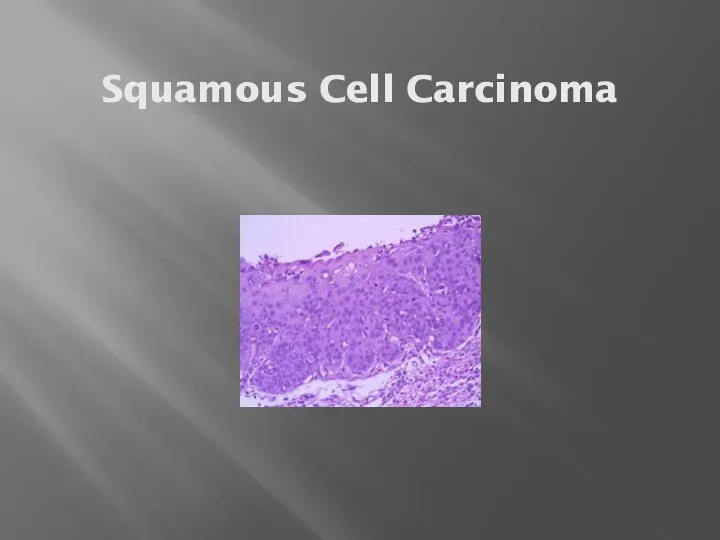
- 9. Squamous Cell Carcinoma Usually upper and middle esophagus. Tends to be a local problem—less metastases. Most
- 10. Squamous Cell Carcinoma
- 11. Anatomy
- 12. Clinical Presentation Signs: weight loss, palpable lymph nodes, usually non-specific. Symptoms: dysphagia, loss of appetite, pain
- 13. Endoscopy ENDOSCOPIC IMAGE OF BARRETT'S ESOPHAGUS WITH PERMISSION TO PLACE IN PUBLIC DOMAIN TAKEN FROM PATIENT
- 14. Tomographic Imaging (CT)
- 15. Positron Emission Tomography
- 16. Staging Two basic groups Locally Advanced (primary tumor and regional lymph nodes): - potentially curable Metastatic
- 17. Locally Advanced Stage “Best” treatment approach is controversial and continually evolving. Concepts to consider: Local control
- 18. Chemotherapy & Radiation Without Surgery 5y survival: radiation therapy only - 0% Combination treatment – 26%
- 19. Pattern of Recurrence Almost always at a distant site. Approaches to this problem. Adjuvant chemotherapy Newer
- 20. Treatment of Metastatic Disease Palliative No standard chemotherapy approach Combination of two drugs based on 5-FU,
- 21. Palliation For swallowing trouble: stent most common For pain: narcotics, radiation For Cachexia: appetite stimulants, feeding
- 23. Скачать презентацию
Esophageal Cancer
Epidemiology and Risk Factors
Diagnosis — signs, symptoms, and tests
Work-up
Treatment Overview
Future
Esophageal Cancer
Epidemiology and Risk Factors
Diagnosis — signs, symptoms, and tests
Work-up
Treatment Overview
Future
Epidemiology
Over 15,000 patients per year in the United States and 7th
Epidemiology
Over 15,000 patients per year in the United States and 7th
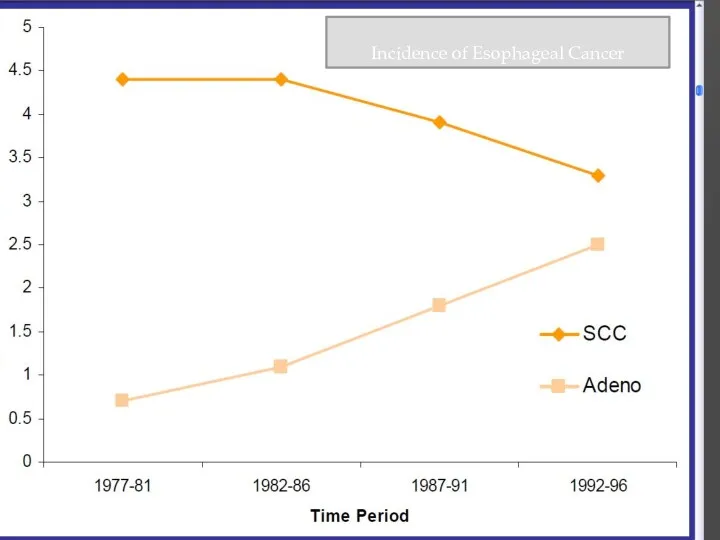
Incidence of Esophageal Cancer
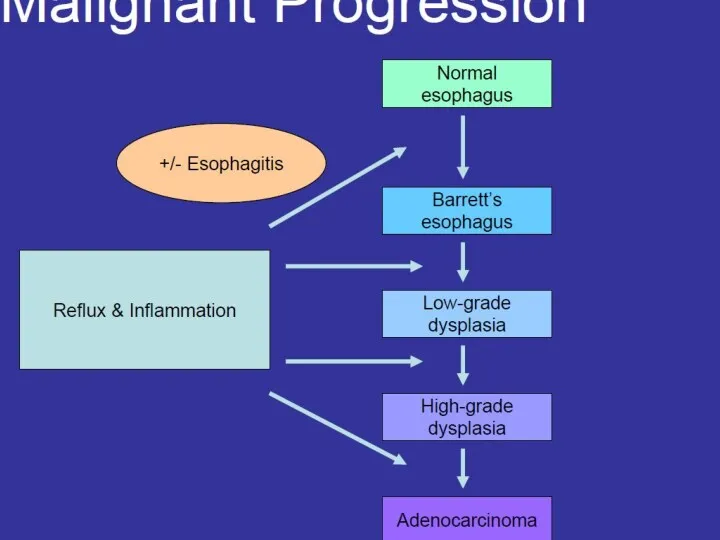
Adenocarcinoma: Barrett’s Esophagus
Likely related to chronic GERD, obesity.
Pathway of malignant progression.
40
Adenocarcinoma: Barrett’s Esophagus
Likely related to chronic GERD, obesity.
Pathway of malignant progression.
40
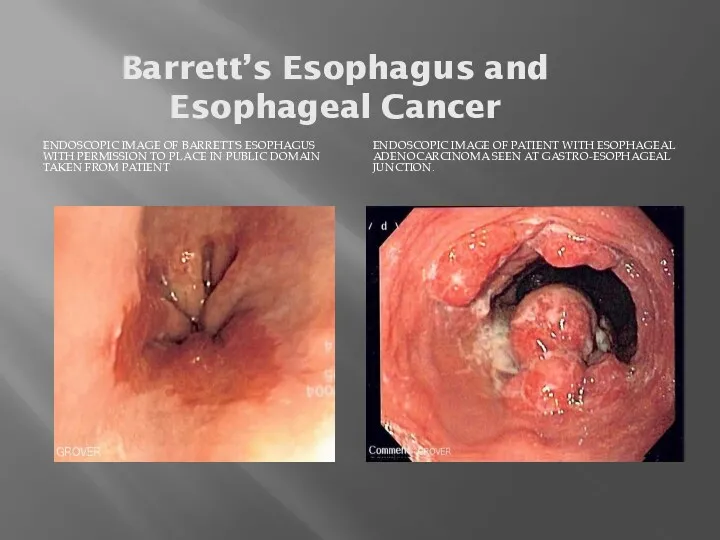
Barrett’s Esophagus and Esophageal Cancer
ENDOSCOPIC IMAGE OF BARRETT'S ESOPHAGUS WITH PERMISSION
Barrett’s Esophagus and Esophageal Cancer
ENDOSCOPIC IMAGE OF BARRETT'S ESOPHAGUS WITH PERMISSION
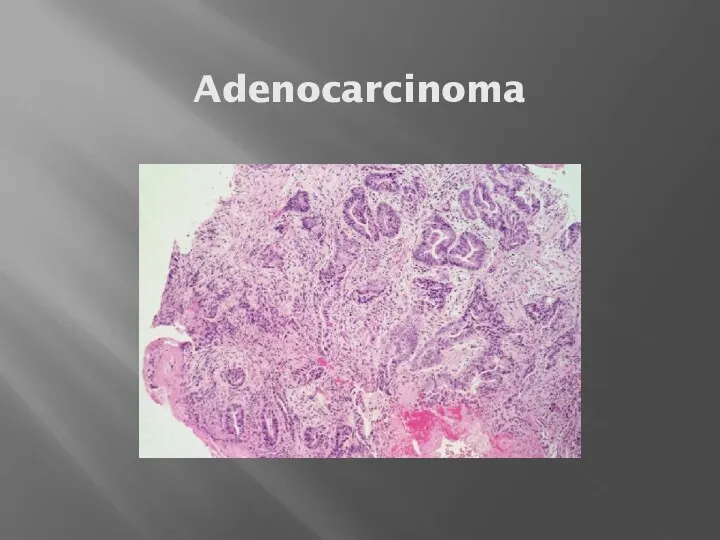
Adenocarcinoma
Adenocarcinoma
Squamous Cell Carcinoma
Usually upper and middle esophagus.
Tends to be a local
Squamous Cell Carcinoma
Usually upper and middle esophagus.
Tends to be a local
Squamous Cell Carcinoma
Squamous Cell Carcinoma
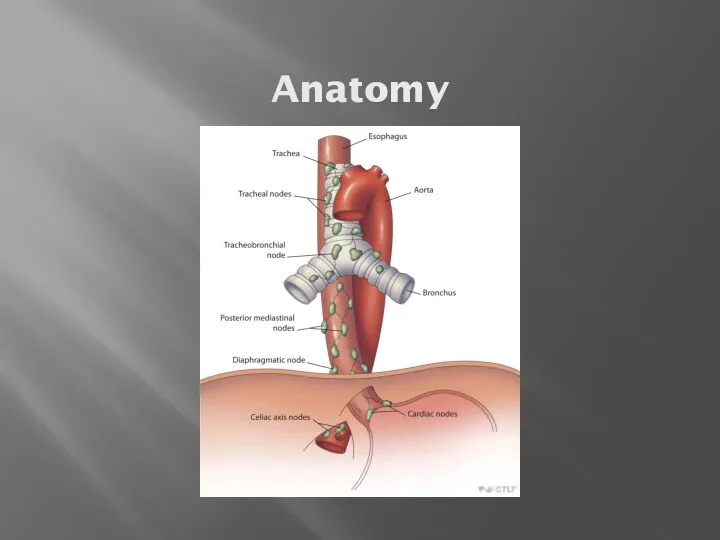
Anatomy
Anatomy
Clinical Presentation
Signs: weight loss, palpable lymph nodes, usually non-specific.
Symptoms: dysphagia, loss
Clinical Presentation
Signs: weight loss, palpable lymph nodes, usually non-specific.
Symptoms: dysphagia, loss
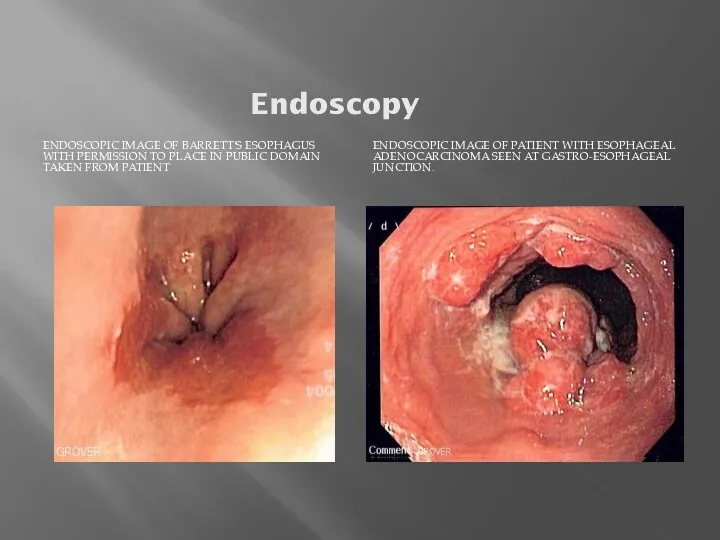
Endoscopy
ENDOSCOPIC IMAGE OF BARRETT'S ESOPHAGUS WITH PERMISSION TO PLACE IN PUBLIC
Endoscopy
ENDOSCOPIC IMAGE OF BARRETT'S ESOPHAGUS WITH PERMISSION TO PLACE IN PUBLIC
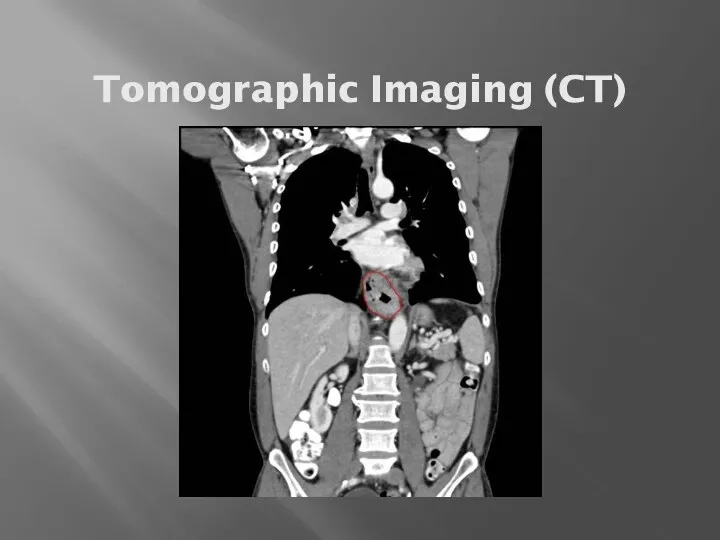
Tomographic Imaging (CT)
Tomographic Imaging (CT)
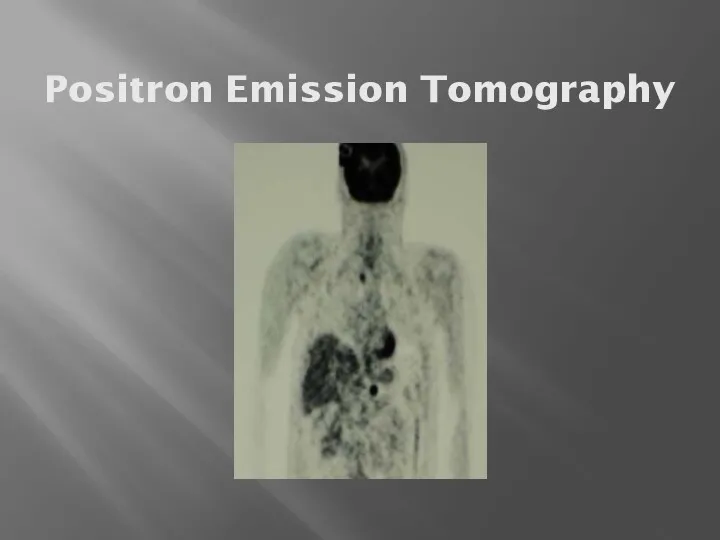
Positron Emission Tomography
Positron Emission Tomography
Staging
Two basic groups
Locally Advanced (primary tumor and regional lymph nodes):
Staging
Two basic groups
Locally Advanced (primary tumor and regional lymph nodes):

Locally Advanced Stage
“Best” treatment approach is controversial and continually evolving.
Concepts to
Locally Advanced Stage
“Best” treatment approach is controversial and continually evolving.
Concepts to
Chemotherapy & Radiation Without Surgery
5y survival:
radiation therapy only - 0%
Combination treatment
Chemotherapy & Radiation Without Surgery
5y survival:
radiation therapy only - 0%
Combination treatment
Pattern of Recurrence
Almost always at a distant site.
Approaches to this problem.
Pattern of Recurrence
Almost always at a distant site.
Approaches to this problem.
Treatment of Metastatic Disease
Palliative
No standard chemotherapy approach
Combination of two drugs based
Treatment of Metastatic Disease
Palliative
No standard chemotherapy approach
Combination of two drugs based
Palliation
For swallowing trouble: stent most common
For pain: narcotics, radiation
For Cachexia: appetite
Palliation
For swallowing trouble: stent most common
For pain: narcotics, radiation
For Cachexia: appetite
 Коллекция от Askona
Коллекция от Askona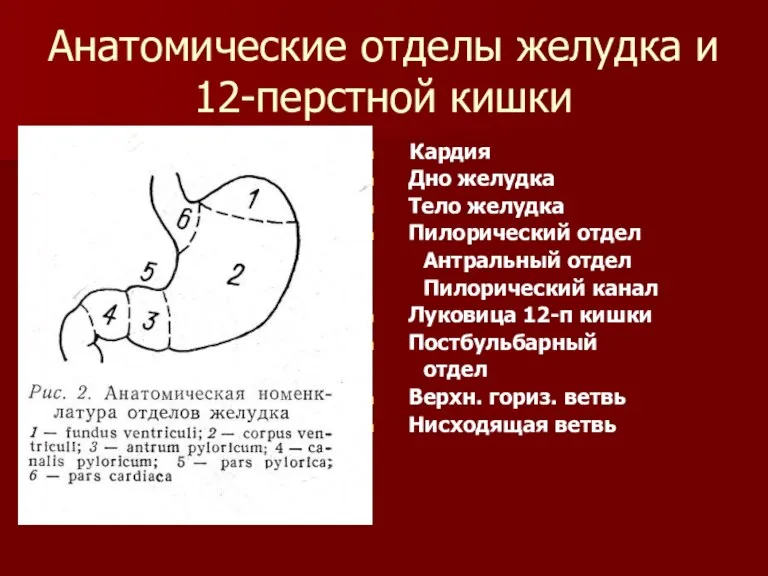 Хирургия язвенной болезни желудка
Хирургия язвенной болезни желудка Физическое развитие детей от рождения до года
Физическое развитие детей от рождения до года Біофармація – теоретична основа виробництва лікарських засобів
Біофармація – теоретична основа виробництва лікарських засобів Острый и хронический парапроктит
Острый и хронический парапроктит Люди з синдромом Дауна
Люди з синдромом Дауна Хроническое нарушение мезентериального кровообращения
Хроническое нарушение мезентериального кровообращения Лекарственные средства, действующие на ЦНС. Лекция 5
Лекарственные средства, действующие на ЦНС. Лекция 5 Лимфедема нижних конечностей
Лимфедема нижних конечностей Қоршаған орта фаркторларының әсерімен байланысты аурулардың алдын алу негізі ретінде гигиеналық нормалау
Қоршаған орта фаркторларының әсерімен байланысты аурулардың алдын алу негізі ретінде гигиеналық нормалау Азбука СПИДа
Азбука СПИДа Пигментный обмен. Желчные пигменты
Пигментный обмен. Желчные пигменты Серологическая диагностика
Серологическая диагностика СП при анемиях
СП при анемиях Проявление старения на молекулярно-генетическом, клеточном, тканевом, органном и организменном уровнях. Понятие о гериатрии
Проявление старения на молекулярно-генетическом, клеточном, тканевом, органном и организменном уровнях. Понятие о гериатрии Частная патологическая анатомия. Болезни ССС
Частная патологическая анатомия. Болезни ССС Медицинское страхование и медицинское обслуживание АО СК Sinoasia B&R (Синоазия БиЭндАр)
Медицинское страхование и медицинское обслуживание АО СК Sinoasia B&R (Синоазия БиЭндАр) Оборотные средства аптечной организации. (Тема 21)
Оборотные средства аптечной организации. (Тема 21) Акушерские кровотечения
Акушерские кровотечения Беременные с преэклампсией. Неотложная помощь при эклампсии и ее осложнения
Беременные с преэклампсией. Неотложная помощь при эклампсии и ее осложнения Патогенетические механизмы действия химических факторов на организм человека
Патогенетические механизмы действия химических факторов на организм человека Улучшение качества материнской и неонатальной помощи. (Модуль 15)
Улучшение качества материнской и неонатальной помощи. (Модуль 15) Условие получения доброкачественного молока
Условие получения доброкачественного молока Основы биомеханики
Основы биомеханики Патогенные Кокки
Патогенные Кокки Принципы лечения злокачественных новообразований
Принципы лечения злокачественных новообразований Государственная регистрация лекарственных средств
Государственная регистрация лекарственных средств Илья Васильевич Буяльский
Илья Васильевич Буяльский