- Pediatric chest X-ray

Содержание
- 2. Pediatric chest X-ray
- 4. Gastric bubble should be on the left Verify Right and Left sides 1-Cardiac shadow is mainly
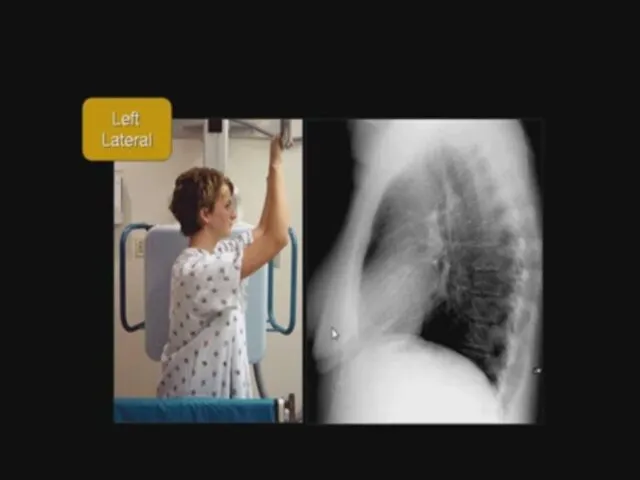
- 5. Plain X-ray chest and heart, PA view Centralization of the patient (Patient is more or less
- 6. Plain
- 7. Supine Supine AP film
- 10. Rotation Check centralization of patient
- 11. Cardiac silhouette Edges of the heart - Cardiac : Site , size, configuration. - Pulmonary vasculature.
- 15. Hilum
- 17. Look for the abnormalities
- 18. Mediastinal shift 1. To the same side of the lesion Massive lung collapse Pulmonary fibrosis 2.
- 19. Abnormalities in lung fields Opaque hemithorax Massive consolidation Massive pleural effusion Massive lung collapse Pleuropulmonary fibrosis
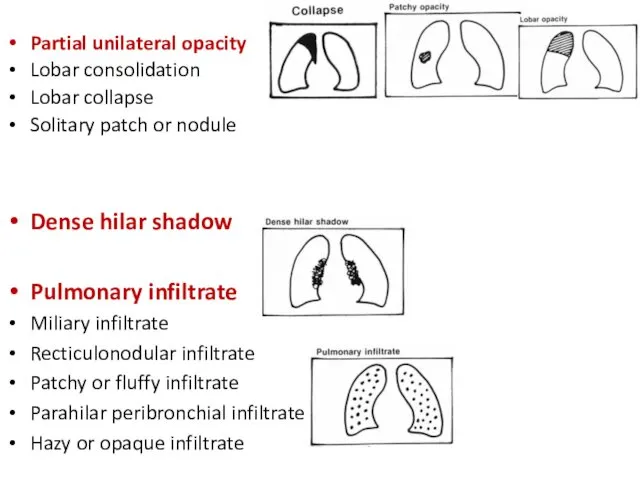
- 20. Partial unilateral opacity Lobar consolidation Lobar collapse Solitary patch or nodule Dense hilar shadow Pulmonary infiltrate
- 21. 1- Opaque hemithorax
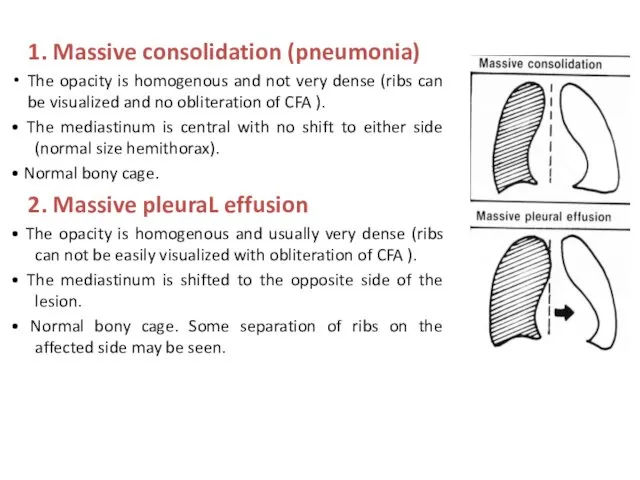
- 22. 1. Massive consolidation (pneumonia) The opacity is homogenous and not very dense (ribs can be visualized
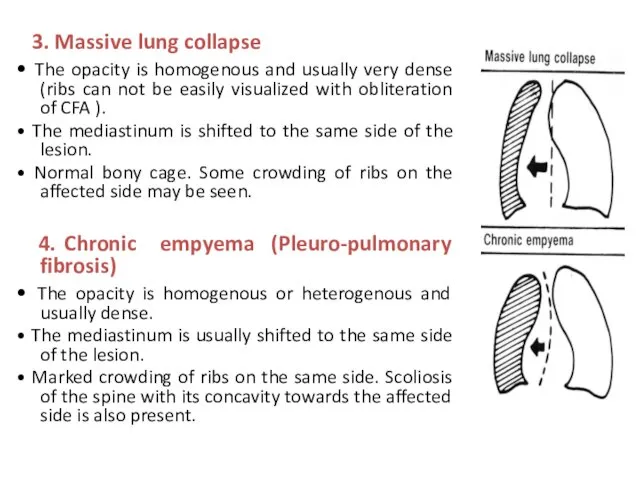
- 23. 3. Massive lung collapse • The opacity is homogenous and usually very dense (ribs can not
- 24. 1. Massive consolidation (pneumonia)
- 25. Massive consolidation (pneumonia) of the Rt. Lung (lobar pneumonia) Homogenous opacity occupying the whole Rt. Hemithorax.
- 26. Massive Rt. sided consolidation and left compansatory emphysema Staphylococcal, streptococcal, hemophilus influenza, klebsiella and pneumococcal.
- 27. 2. Massive pleuraL effusion
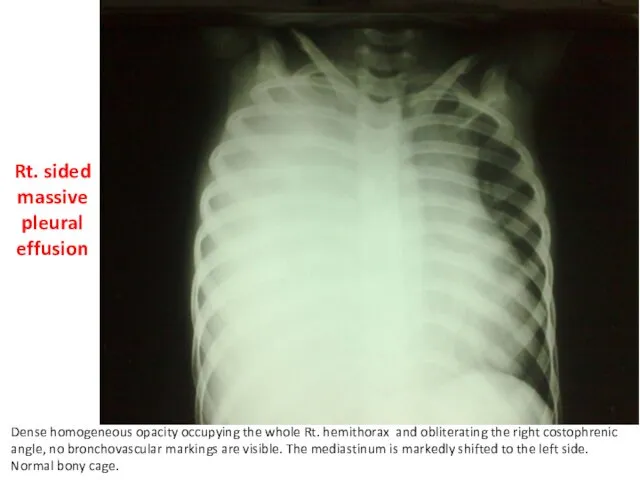
- 28. Rt. sided massive pleural effusion Dense homogeneous opacity occupying the whole Rt. hemithorax and obliterating the
- 30. Causes of pleural effusion Empyema (purulent pleurisy) Bacterial pneumonias (Staphylococcal, Hemophilus influenza). Ruptured lung abscess, mediastinitis,
- 31. 3. Massive lung collapse
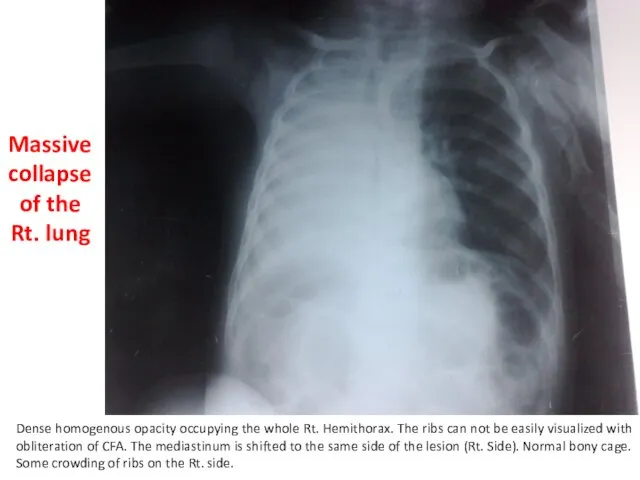
- 32. Dense homogenous opacity occupying the whole Rt. Hemithorax. The ribs can not be easily visualized with
- 33. Massive lung collapse It results from total obstruction of the main Rt. or Lt. bronchus. Causes:
- 34. 4. Chronic empyema (Pleuro-pulmonary fibrosis) .
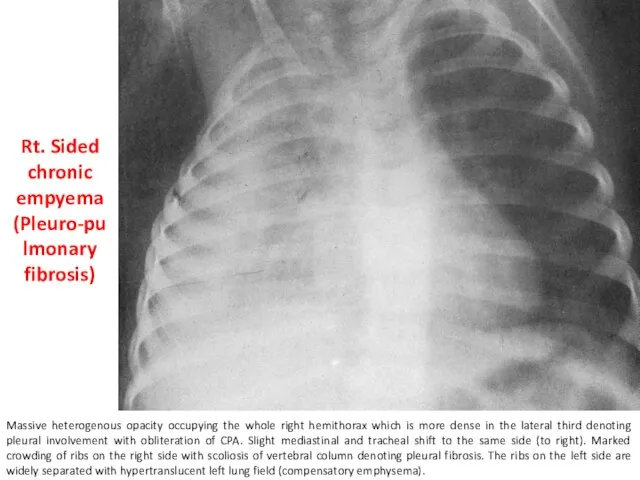
- 35. Rt. Sided chronic empyema (Pleuro-pulmonary fibrosis) Massive heterogenous opacity occupying the whole right hemithorax which is
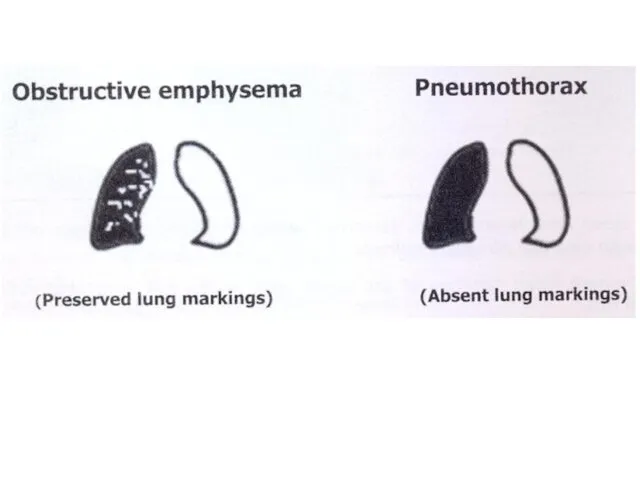
- 36. 2- Hypertranslucent hemithorax A-Obstructive emphysema B-Pneumothorax
- 38. A-Obstructive emphysema
- 39. Obstructive emphysema of the left lung Hypertranslucency of the whole Lt. hemithorax with preserved bronchovascular markings.
- 40. Obstructive Emphysema -It results from partial (incomplete) obstruction of a bronchus which creates a valve type
- 41. B-Pneumothorax
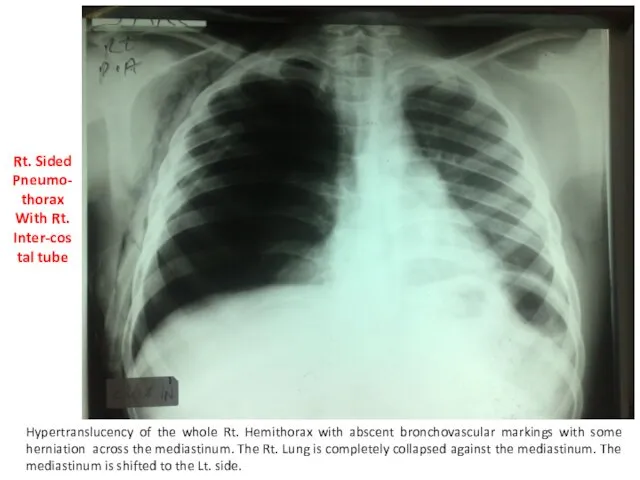
- 42. Rt. Sided Pneumo-thorax With Rt. Inter-costal tube Hypertranslucency of the whole Rt. Hemithorax with abscent bronchovascular
- 45. Causes of pneumothorax (free air in pleural space): 1-Iatrogenic: as a complication of mechanical ventilation or
- 46. 3-Air-fluid level A- Lung abscess B- Hydropneumothorax
- 48. A- Lung abscess
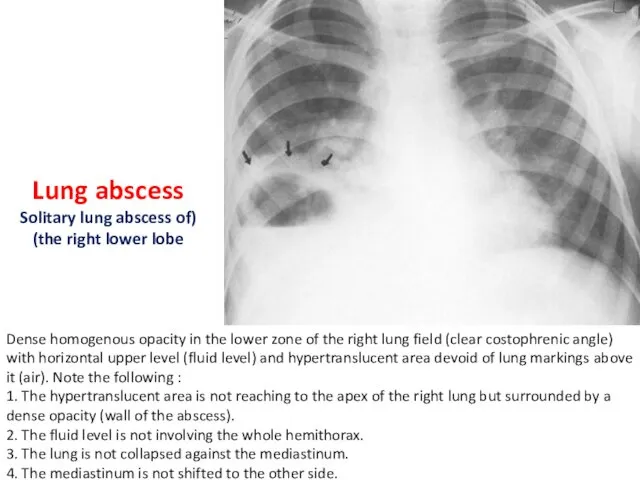
- 49. Dense homogenous opacity in the lower zone of the right lung field (clear costophrenic angle) with
- 51. Lung Abscess It results from suppurative destruction of lung parenchyma and formation of a cavity containing
- 52. B- Hydropneumothorax
- 54. * Plain x-ray of a chest and heart, posteroanterior view. The patient is not centralized. The
- 56. Hydropneumothorax It occurs mostly with cases of pleural effusion due to one of 2 causes: -Iatrogenic
- 57. Failure of expansion of the collapsed lung in spite of the closed intercostal drainage suggests the
- 58. 4-Partial unilateral opacity Lobar consolidation (pneumonia) Lobar collapse (atelectasis) Solitary patch or nodule
- 60. 4-Partial unilateral opacity A--Lobar consolidation (pneumonia)
- 61. Rt. Upper lobe pneumonia Homogenous opacity occupying the upper zone of Rt. Hemithorax. The opacity is
- 62. Silhouette sign
- 64. Right middle and lower lobe consolidation
- 65. Dense homogeneous opacity occupying the Lower zone of Rt. hemithorax and obliterating the right costophrenic angle,
- 66. 4-Partial unilateral opacity B- Lobar collapse (atelectasis)
- 67. Rt. Upper lobe collapse Homogenous opacity in the apical region of the right hemithorax. The opacity
- 70. 4-Partial unilateral opacity C- Solitary patch or nodule
- 71. Solitary nodular shadow in the middle zone of the right lung field. The outline is rounded
- 72. Solitary nodule Common causes Tuberculous granuloma {commonest} Round or spherical pneumonia (mostly pneumococcal) Fungal granuloma Solitary
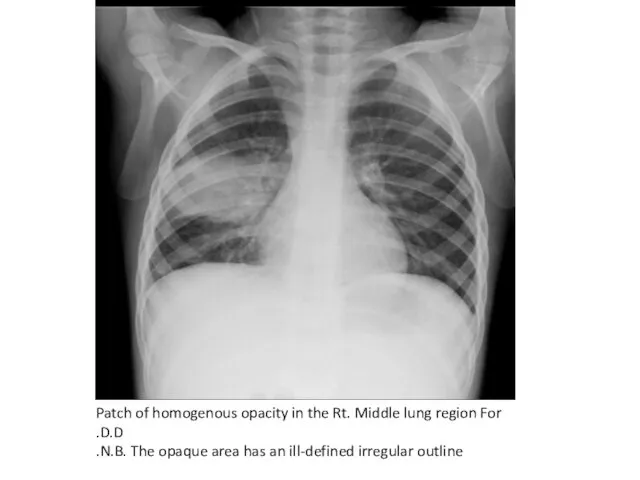
- 73. Patch of homogenous opacity in the Rt. Middle lung region For D.D. N.B. The opaque area
- 74. Solitary patch Patchy pneumonia is the commonest cause of radiological solitary patch. The illness is almost
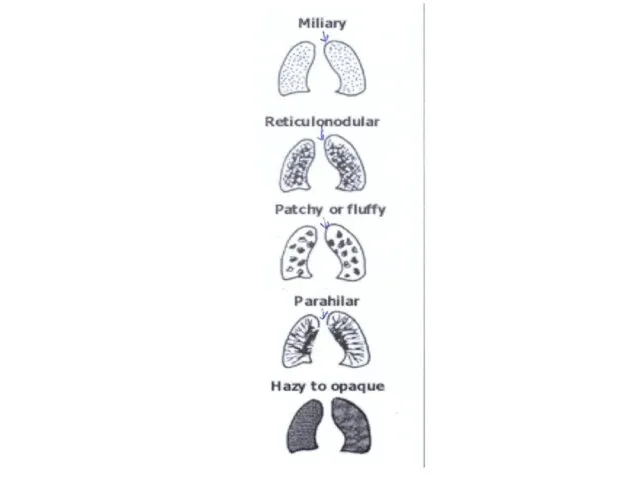
- 75. 5-Pulmonary infiltrate Miliary infiltrate Recticulonodular infiltrate Patchy or fluffy infiltrate Parahilar peribronchial infiltrate (most common) Hazy
- 77. A- Miliary infiltrate
- 78. Miliary infiltrate: Fine dots of uniform size widely distributed throughout the whole lung fields (interstitial)
- 79. Causes of miliary infiltrate 1-Infectious conditions Miliary tuberculosis (commonest) Viral interstitial pneumonias Pulmonary fungal infections. 2-
- 80. B- Recticulonodular infiltrate
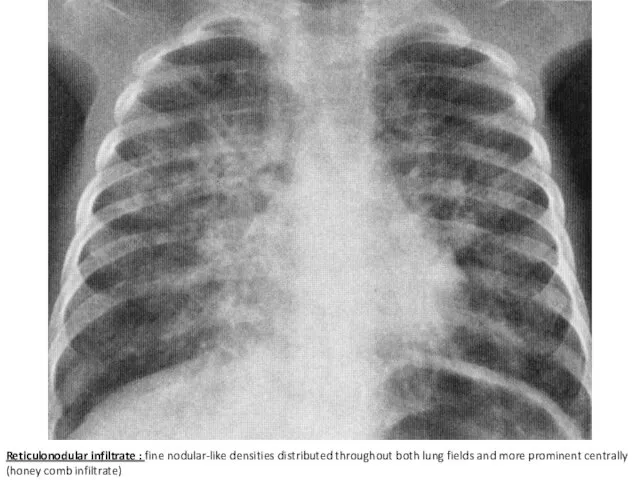
- 81. Reticulonodular infiltrate : fine nodular-like densities distributed throughout both lung fields and more prominent centrally (honey
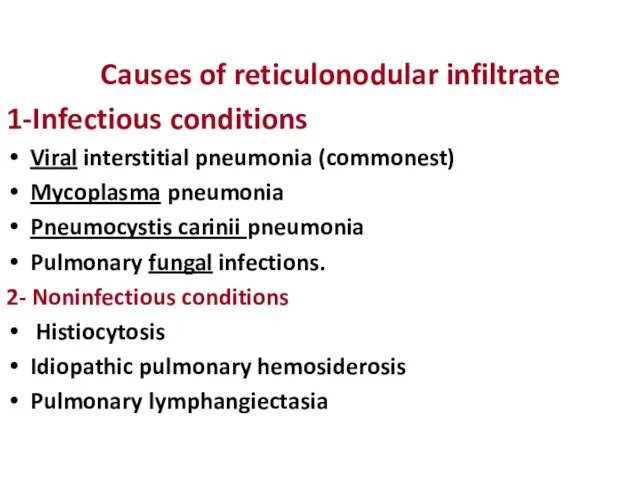
- 82. Causes of reticulonodular infiltrate 1-Infectious conditions Viral interstitial pneumonia (commonest) Mycoplasma pneumonia Pneumocystis carinii pneumonia Pulmonary
- 83. C- Patchy or fluffy infiltrate
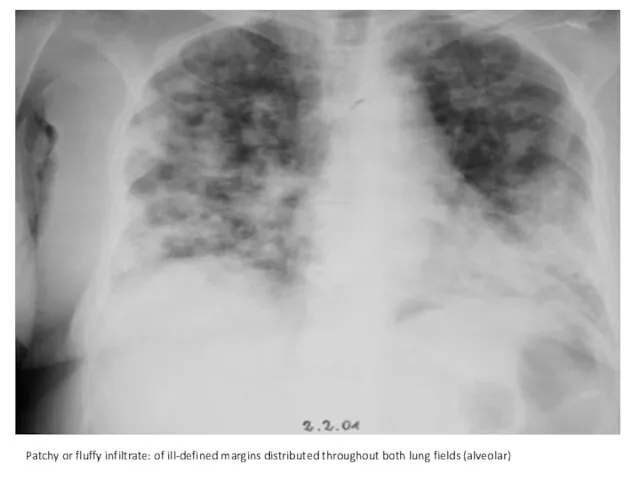
- 84. Patchy or fluffy infiltrate: of ill-defined margins distributed throughout both lung fields (alveolar)
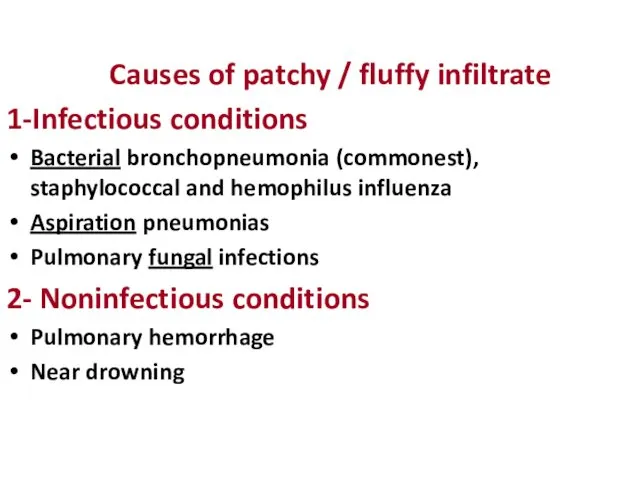
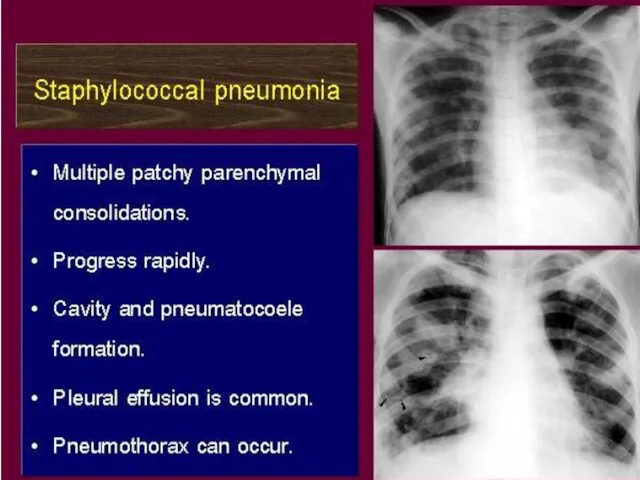
- 85. Causes of patchy / fluffy infiltrate 1-Infectious conditions Bacterial bronchopneumonia (commonest), staphylococcal and hemophilus influenza Aspiration
- 87. D-Parahilar peribronchial infiltrate (most common)
- 88. Parahilar peribronchial infiltrate: streaks radiating towards the periphery of both lung fields and associated with hilar
- 89. Causes of parahilar peribronchial infiltrate 1-Infectious conditions Viral lower respiratory infections as bronchitis (commonest) Bronchial asthma
- 90. E- Hazy to opaque infiltrate (most serious)
- 91. Hazy to opaque infiltrate: diffuse dense homogeneous opacity of both lung fields with the cardiac shadow
- 92. Causes of hazy to opaque infiltrate Pulmonary edema (commonest): -Cardiac causes: myocarditis, CHD with Lt. to
- 93. 6- Dense Hilar Shadow Hilar lymphadenopathy • Bilateral: Viral lower respiratory infections Chronic aspiration Malignancies as
- 94. Bilateral dense hilar shadow. • Lung fields are clear apart from the slightly increased bronchial markings.
- 95. Fine granular opacities widely distributed throughout both lung fields (ground glass appearance) with air bronchogram. Commonest
- 96. Severe RDS (white lungs) Complete opacification of both lung fields (white lungs). The cardiac shadow is
- 97. MAS with pneumothorax
- 98. Multiple cysts of variable sizes ( air –filled bowel) occupying the whole left hemithorax and pushing
- 103. Скачать презентацию
Pediatric chest X-ray
Pediatric chest X-ray


Gastric bubble should be on the left
Verify Right and Left sides
1-Cardiac
Gastric bubble should be on the left
Verify Right and Left sides
1-Cardiac
Plain X-ray chest and heart, PA view
Centralization of the
Plain X-ray chest and heart, PA view
Centralization of the
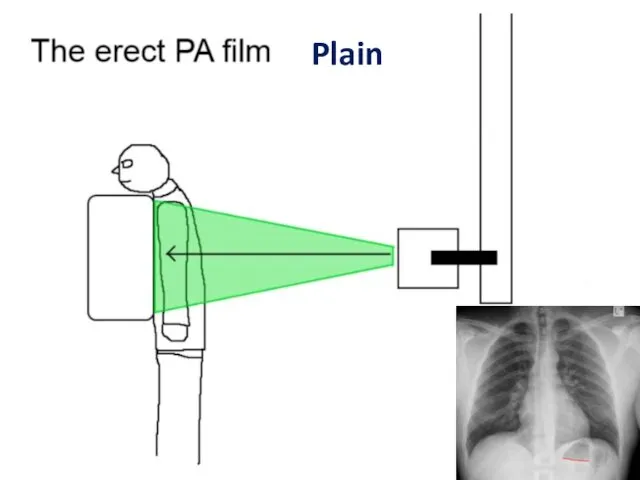
Plain
Plain
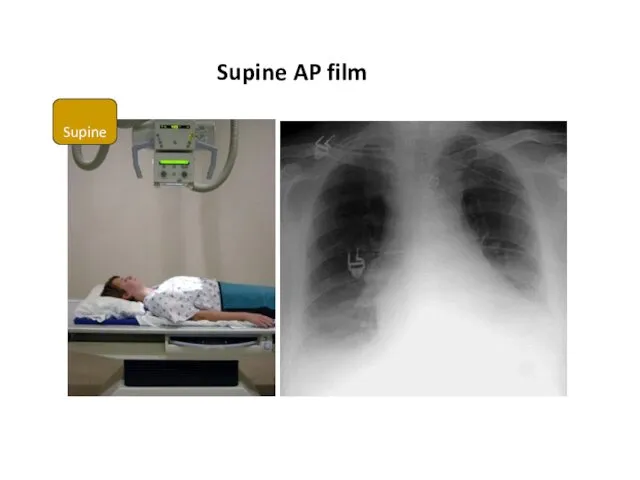
Supine
Supine AP film
Supine
Supine AP film

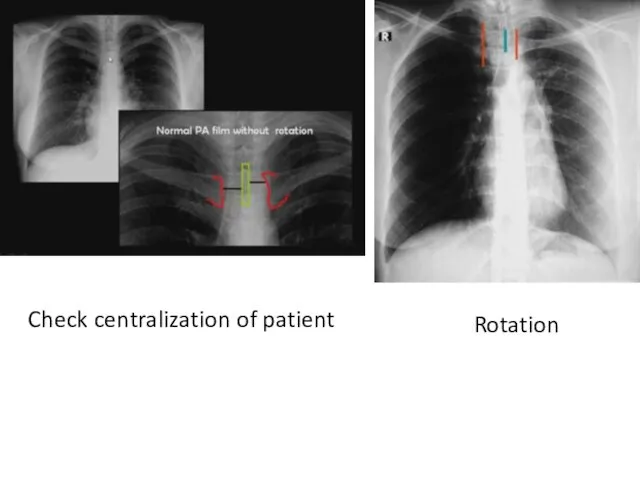
Rotation
Check centralization of patient
Rotation
Check centralization of patient
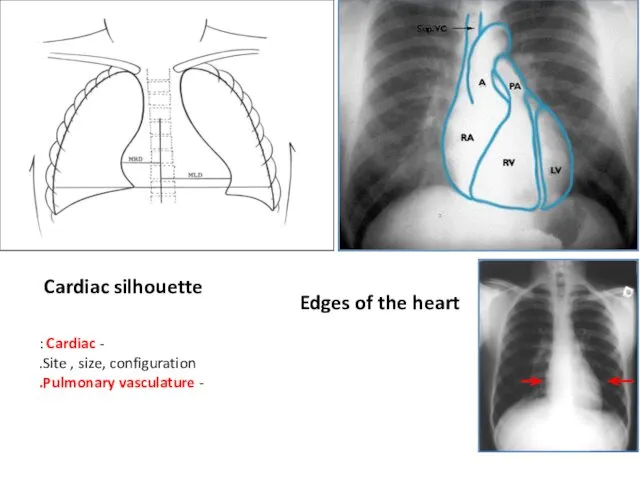
Cardiac silhouette
Edges of the heart
- Cardiac :
Site , size,
Cardiac silhouette
Edges of the heart
- Cardiac :
Site , size,


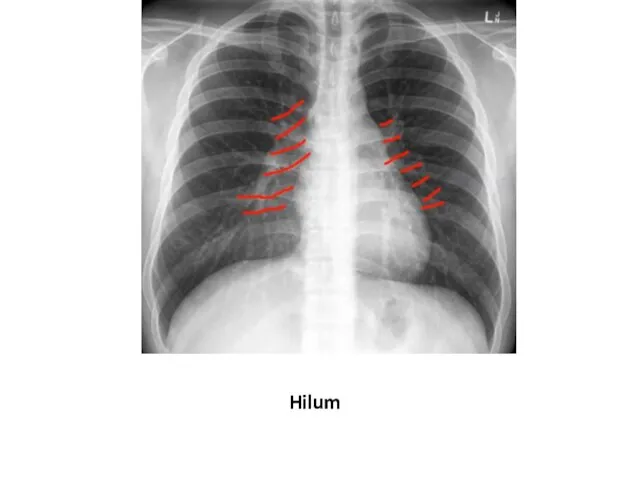
Hilum
Hilum

Look for the abnormalities
Look for the abnormalities
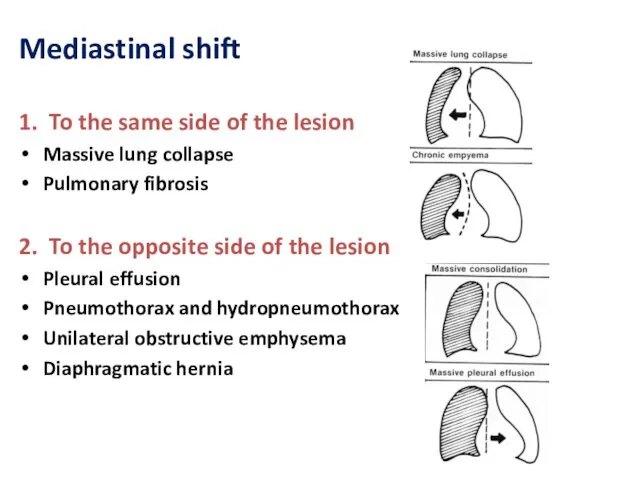
Mediastinal shift
1. To the same side of the lesion
Massive lung collapse
Mediastinal shift
1. To the same side of the lesion
Massive lung collapse
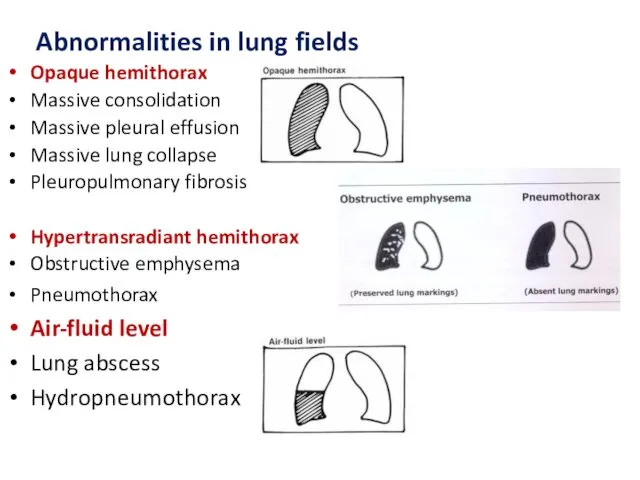
Abnormalities in lung fields
Opaque hemithorax
Massive consolidation
Massive pleural effusion
Massive
Abnormalities in lung fields
Opaque hemithorax
Massive consolidation
Massive pleural effusion
Massive
Partial unilateral opacity
Lobar consolidation
Lobar collapse
Solitary patch or nodule
Dense hilar
Partial unilateral opacity
Lobar consolidation
Lobar collapse
Solitary patch or nodule
Dense hilar
1- Opaque hemithorax
1- Opaque hemithorax
1. Massive consolidation (pneumonia)
The opacity is homogenous and not very
1. Massive consolidation (pneumonia)
The opacity is homogenous and not very
3. Massive lung collapse
• The opacity is homogenous and usually
3. Massive lung collapse
• The opacity is homogenous and usually
1. Massive consolidation (pneumonia)
1. Massive consolidation (pneumonia)
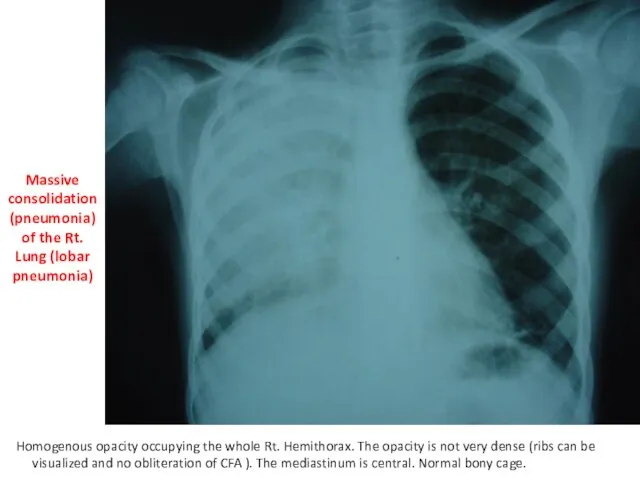
Massive consolidation (pneumonia) of the Rt. Lung (lobar pneumonia)
Homogenous opacity occupying
Massive consolidation (pneumonia) of the Rt. Lung (lobar pneumonia)
Homogenous opacity occupying
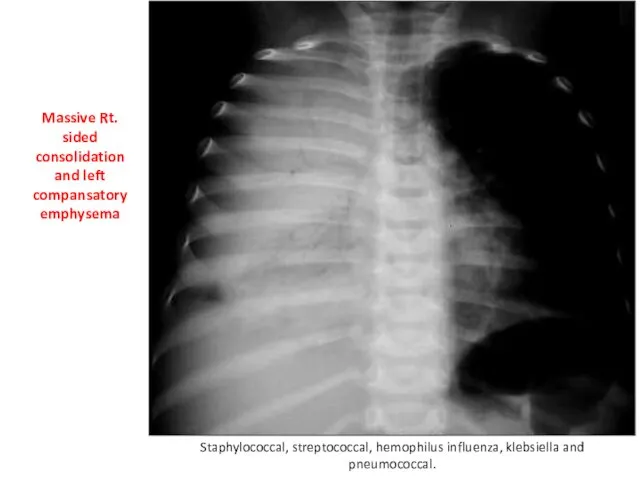
Massive Rt. sided consolidation and left compansatory emphysema
Staphylococcal, streptococcal, hemophilus influenza,
Massive Rt. sided consolidation and left compansatory emphysema
Staphylococcal, streptococcal, hemophilus influenza,
2. Massive pleuraL effusion
2. Massive pleuraL effusion
Rt. sided massive pleural effusion
Dense homogeneous opacity occupying the whole Rt.
Rt. sided massive pleural effusion
Dense homogeneous opacity occupying the whole Rt.

Causes of pleural effusion
Empyema (purulent pleurisy)
Bacterial pneumonias (Staphylococcal, Hemophilus influenza).
Causes of pleural effusion
Empyema (purulent pleurisy)
Bacterial pneumonias (Staphylococcal, Hemophilus influenza).
3. Massive lung collapse
3. Massive lung collapse
Dense homogenous opacity occupying the whole Rt. Hemithorax. The ribs can
Dense homogenous opacity occupying the whole Rt. Hemithorax. The ribs can
Massive lung collapse
It results from total obstruction of the main
Massive lung collapse It results from total obstruction of the main
4. Chronic empyema (Pleuro-pulmonary fibrosis)
.
4. Chronic empyema (Pleuro-pulmonary fibrosis)
.
Rt. Sided chronic empyema (Pleuro-pulmonary fibrosis)
Massive heterogenous opacity occupying the whole
Rt. Sided chronic empyema (Pleuro-pulmonary fibrosis)
Massive heterogenous opacity occupying the whole
2- Hypertranslucent hemithorax
A-Obstructive emphysema
B-Pneumothorax
2- Hypertranslucent hemithorax
A-Obstructive emphysema
B-Pneumothorax
A-Obstructive emphysema
A-Obstructive emphysema
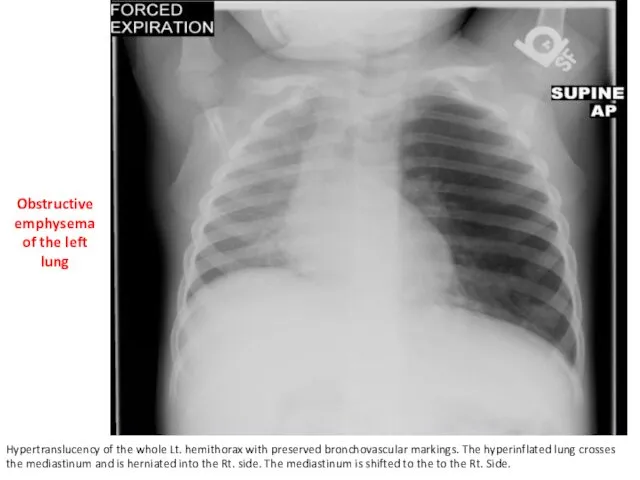
Obstructive emphysema of the left lung
Hypertranslucency of the whole Lt. hemithorax
Obstructive emphysema of the left lung
Hypertranslucency of the whole Lt. hemithorax
Obstructive Emphysema
-It results from partial (incomplete) obstruction of a bronchus which
Obstructive Emphysema -It results from partial (incomplete) obstruction of a bronchus which
B-Pneumothorax
B-Pneumothorax
Rt. Sided Pneumo-thorax With Rt. Inter-costal tube
Hypertranslucency of the whole Rt.
Rt. Sided Pneumo-thorax With Rt. Inter-costal tube
Hypertranslucency of the whole Rt.


Causes of pneumothorax (free air in pleural space):
1-Iatrogenic: as a complication
Causes of pneumothorax (free air in pleural space): 1-Iatrogenic: as a complication
3-Air-fluid level
A- Lung abscess
B- Hydropneumothorax
3-Air-fluid level
A- Lung abscess
B- Hydropneumothorax

A- Lung abscess
A- Lung abscess
Dense homogenous opacity in the lower zone of the right lung
Dense homogenous opacity in the lower zone of the right lung

Lung Abscess
It results from suppurative destruction of lung parenchyma and formation
It results from suppurative destruction of lung parenchyma and formation
B- Hydropneumothorax

* Plain x-ray of a chest and heart, posteroanterior view.
The patient
* Plain x-ray of a chest and heart, posteroanterior view.
The patient


Hydropneumothorax
It occurs mostly with cases of pleural effusion due to one
It occurs mostly with cases of pleural effusion due to one
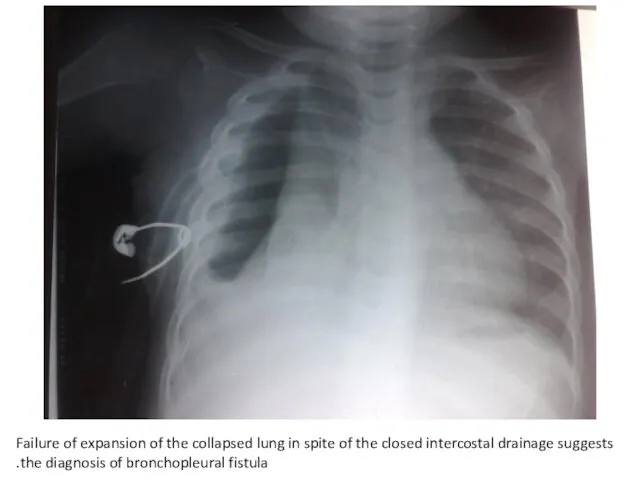
Failure of expansion of the collapsed lung in spite of the
Failure of expansion of the collapsed lung in spite of the
4-Partial unilateral opacity
Lobar consolidation (pneumonia)
Lobar collapse (atelectasis)
Solitary patch
4-Partial unilateral opacity
Lobar consolidation (pneumonia)
Lobar collapse (atelectasis)
Solitary patch

4-Partial unilateral opacity
A--Lobar consolidation (pneumonia)
4-Partial unilateral opacity
A--Lobar consolidation (pneumonia)
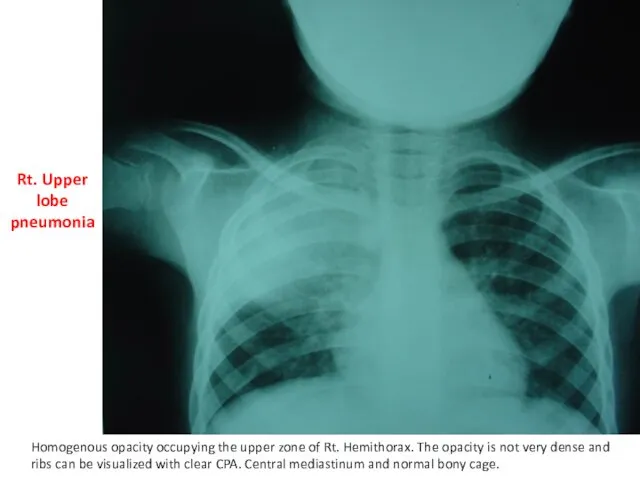
Rt. Upper lobe pneumonia
Homogenous opacity occupying the upper zone of Rt.
Rt. Upper lobe pneumonia
Homogenous opacity occupying the upper zone of Rt.
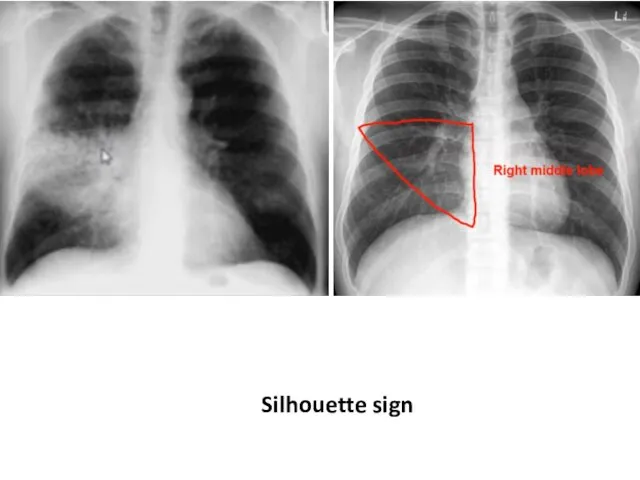
Silhouette sign
Silhouette sign

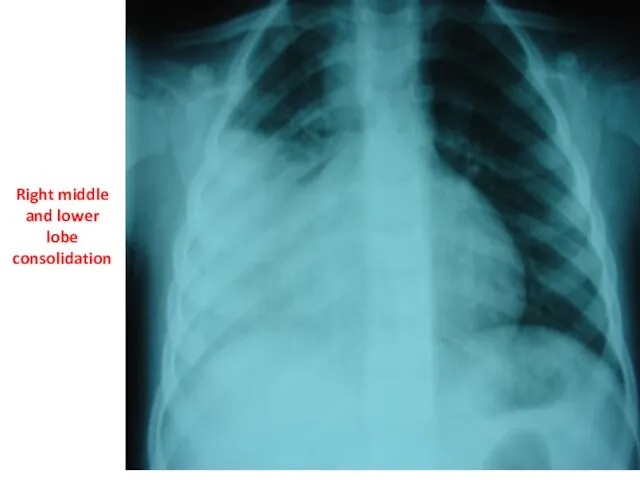
Right middle and lower lobe consolidation
Right middle and lower lobe consolidation

Dense homogeneous opacity occupying the Lower zone of Rt. hemithorax and
Dense homogeneous opacity occupying the Lower zone of Rt. hemithorax and
4-Partial unilateral opacity
B- Lobar collapse (atelectasis)
4-Partial unilateral opacity
B- Lobar collapse (atelectasis)
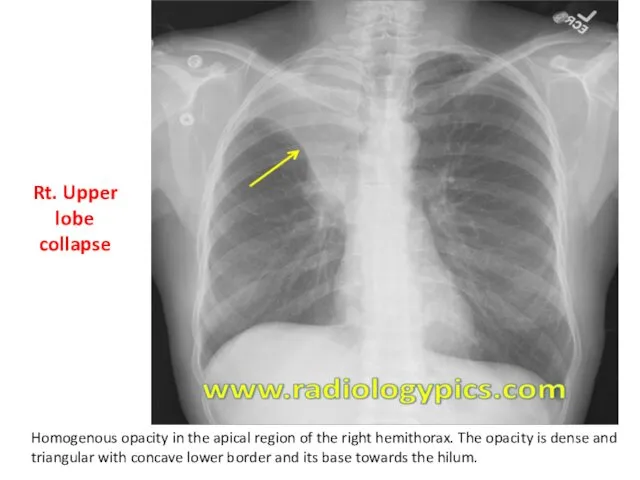
Rt. Upper lobe collapse
Homogenous opacity in the apical region of the
Rt. Upper lobe collapse
Homogenous opacity in the apical region of the


4-Partial unilateral opacity
C- Solitary patch or nodule
4-Partial unilateral opacity
C- Solitary patch or nodule
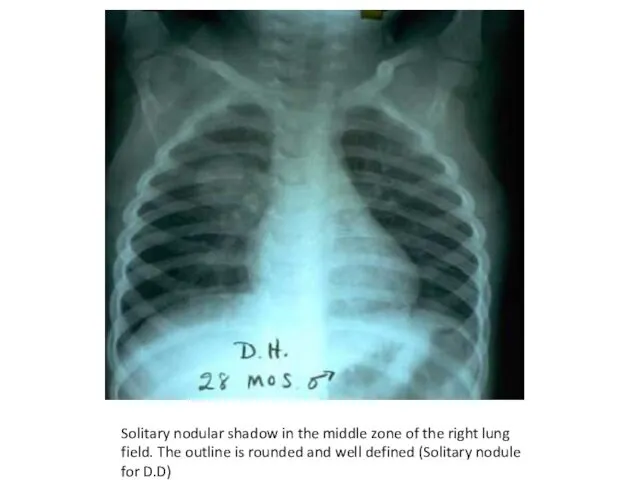
Solitary nodular shadow in the middle zone of the right lung
Solitary nodular shadow in the middle zone of the right lung
Solitary nodule
Common causes
Tuberculous granuloma {commonest}
Round or spherical pneumonia (mostly
Solitary nodule
Common causes
Tuberculous granuloma {commonest}
Round or spherical pneumonia (mostly
Patch of homogenous opacity in the Rt. Middle lung region For
Patch of homogenous opacity in the Rt. Middle lung region For
Solitary patch
Patchy pneumonia is the commonest cause of radiological solitary
Solitary patch
Patchy pneumonia is the commonest cause of radiological solitary
5-Pulmonary infiltrate
Miliary infiltrate
Recticulonodular infiltrate
Patchy or fluffy infiltrate
5-Pulmonary infiltrate
Miliary infiltrate
Recticulonodular infiltrate
Patchy or fluffy infiltrate
A- Miliary infiltrate
A- Miliary infiltrate

Miliary infiltrate: Fine dots of uniform size widely distributed throughout the
Miliary infiltrate: Fine dots of uniform size widely distributed throughout the
Causes of miliary infiltrate
1-Infectious conditions
Miliary tuberculosis (commonest)
Viral interstitial pneumonias
Pulmonary
1-Infectious conditions
Miliary tuberculosis (commonest)
Viral interstitial pneumonias
Pulmonary
B- Recticulonodular infiltrate
B- Recticulonodular infiltrate
Reticulonodular infiltrate : fine nodular-like densities distributed throughout both lung fields
Reticulonodular infiltrate : fine nodular-like densities distributed throughout both lung fields
Causes of reticulonodular infiltrate
1-Infectious conditions
Viral interstitial pneumonia (commonest)
Mycoplasma pneumonia
Pneumocystis carinii
1-Infectious conditions
Viral interstitial pneumonia (commonest)
Mycoplasma pneumonia
Pneumocystis carinii
C- Patchy or fluffy infiltrate
C- Patchy or fluffy infiltrate
Patchy or fluffy infiltrate: of ill-defined margins distributed throughout both lung
Patchy or fluffy infiltrate: of ill-defined margins distributed throughout both lung
Causes of patchy / fluffy infiltrate
1-Infectious conditions
Bacterial bronchopneumonia (commonest), staphylococcal and
1-Infectious conditions
Bacterial bronchopneumonia (commonest), staphylococcal and
D-Parahilar peribronchial infiltrate
(most common)
D-Parahilar peribronchial infiltrate
(most common)
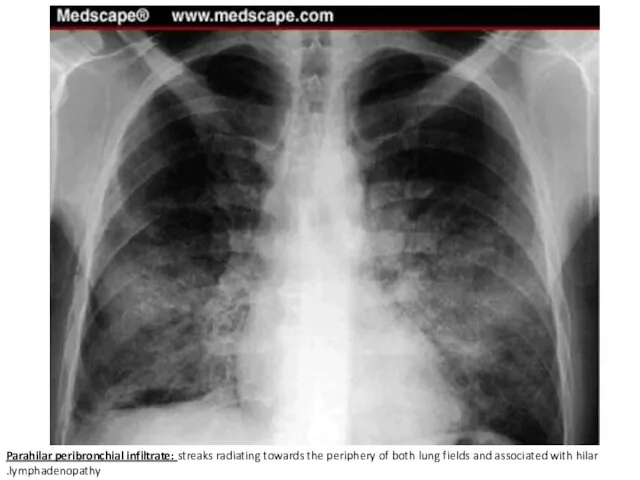
Parahilar peribronchial infiltrate: streaks radiating towards the periphery of both lung
Parahilar peribronchial infiltrate: streaks radiating towards the periphery of both lung
Causes of parahilar peribronchial infiltrate
1-Infectious conditions
Viral lower respiratory infections as bronchitis
1-Infectious conditions
Viral lower respiratory infections as bronchitis
E- Hazy to opaque infiltrate (most serious)
E- Hazy to opaque infiltrate (most serious)
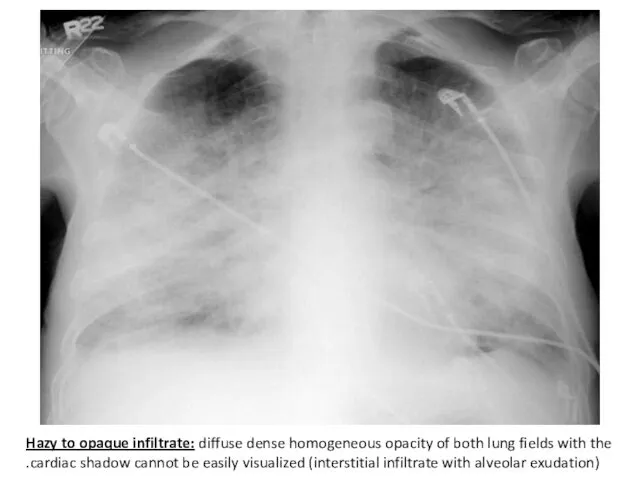
Hazy to opaque infiltrate: diffuse dense homogeneous opacity of both lung
Hazy to opaque infiltrate: diffuse dense homogeneous opacity of both lung
Causes of hazy to opaque infiltrate
Pulmonary edema (commonest):
-Cardiac causes: myocarditis,
Pulmonary edema (commonest):
-Cardiac causes: myocarditis,
6- Dense Hilar Shadow
Hilar lymphadenopathy
• Bilateral:
Viral lower respiratory infections
Chronic aspiration
Malignancies as
6- Dense Hilar Shadow
Hilar lymphadenopathy
• Bilateral:
Viral lower respiratory infections
Chronic aspiration
Malignancies as
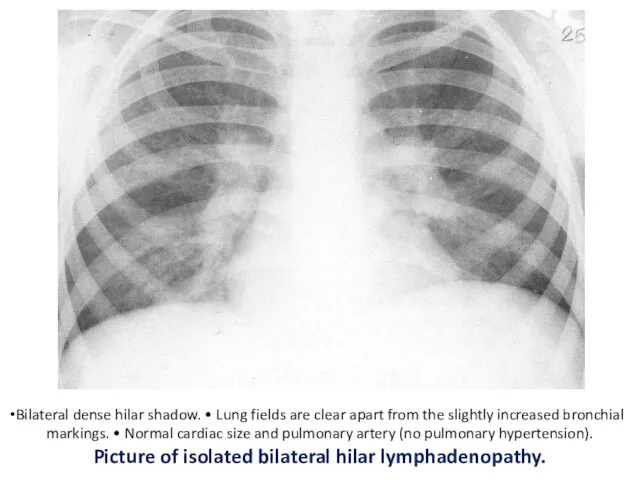
Bilateral dense hilar shadow. • Lung fields are clear apart from
Bilateral dense hilar shadow. • Lung fields are clear apart from
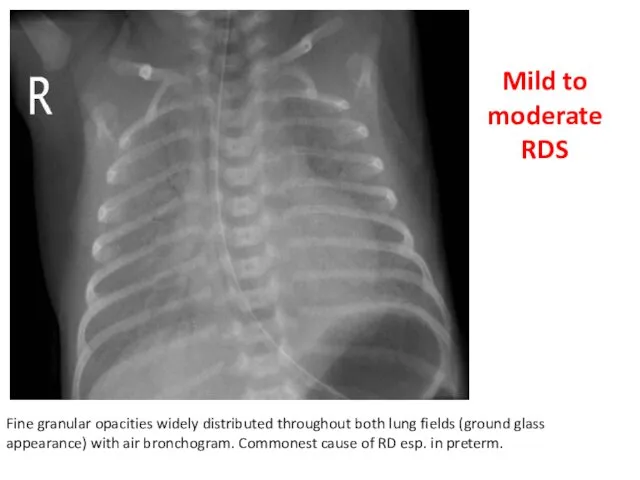
Fine granular opacities widely distributed throughout both lung fields (ground glass
Fine granular opacities widely distributed throughout both lung fields (ground glass
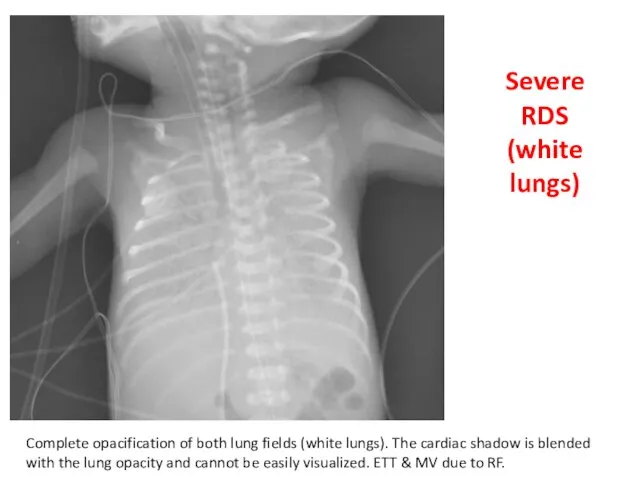
Severe RDS (white lungs)
Complete opacification of both lung fields (white lungs).
Severe RDS (white lungs)
Complete opacification of both lung fields (white lungs).
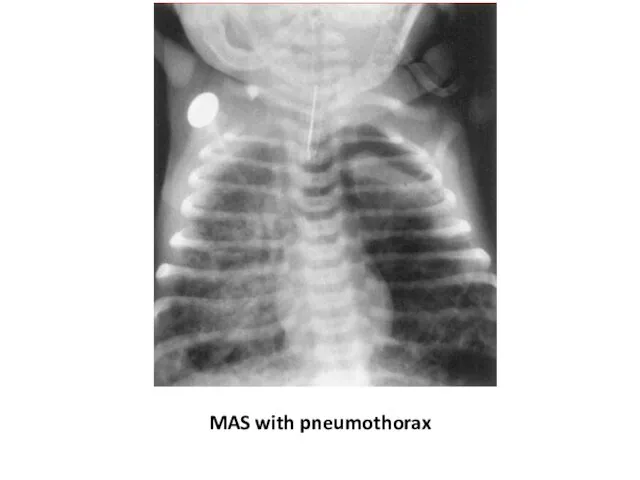
MAS with pneumothorax
MAS with pneumothorax
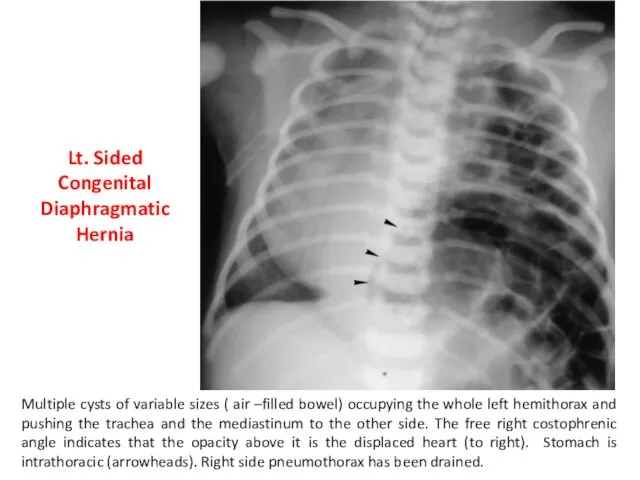
Multiple cysts of variable sizes ( air –filled bowel) occupying the
Multiple cysts of variable sizes ( air –filled bowel) occupying the



 Периоды жизнедеятельности человека. Роль сестринского персонала в сохранении и укреплении здоровья
Периоды жизнедеятельности человека. Роль сестринского персонала в сохранении и укреплении здоровья Влияние ВИЧ на репродуктивную функцию подростка
Влияние ВИЧ на репродуктивную функцию подростка Заболевания передающиеся половым путем
Заболевания передающиеся половым путем Федеральный проект Демография
Федеральный проект Демография Хронический пульпит
Хронический пульпит Синдромы Дауна и Патау
Синдромы Дауна и Патау Деформирующий артроз коленного сустава. Лечение
Деформирующий артроз коленного сустава. Лечение Основы иммунологии. Иммунитет. Иммунная система человека
Основы иммунологии. Иммунитет. Иммунная система человека Дыхательная недостаточность
Дыхательная недостаточность Инфекция или инфекционный процесс
Инфекция или инфекционный процесс Пародонт аурулары. Анықтамасы, жіктелуі, этиологиясы, потогенезі. Пародонт ауруларымен науқастары комплексті тексеру
Пародонт аурулары. Анықтамасы, жіктелуі, этиологиясы, потогенезі. Пародонт ауруларымен науқастары комплексті тексеру Скелет верхней и нижней конечности
Скелет верхней и нижней конечности Организация медико-генетической службы
Организация медико-генетической службы Дом для мамы: я выбираю жизнь
Дом для мамы: я выбираю жизнь Нервно-психическое развитие ребёнка раннего возраста
Нервно-психическое развитие ребёнка раннего возраста Хронический панкреатит и внешнесекреторная недостаточность поджелудочной железы у детей
Хронический панкреатит и внешнесекреторная недостаточность поджелудочной железы у детей Фармацевтическая терминология. Основные понятия фармацевтической терминологии
Фармацевтическая терминология. Основные понятия фармацевтической терминологии Острая почечная и острая печеночная недостаточность
Острая почечная и острая печеночная недостаточность Хроническая обструктивная болезнь легких
Хроническая обструктивная болезнь легких Организация оказания медицинской помощи в амбулаторно - поликлинических учреждениях
Организация оказания медицинской помощи в амбулаторно - поликлинических учреждениях Атипичные нейролептики нового поколения (антипсихотики)
Атипичные нейролептики нового поколения (антипсихотики) Роль медицинской сестры в профилактике и лечении пролежней
Роль медицинской сестры в профилактике и лечении пролежней Прием пациента в стационар. Ведение сестринской документации
Прием пациента в стационар. Ведение сестринской документации Ес және назар аудару бұзылыстарының клиникалық мінездемесі.Сана- сезімнің бұзылыстары
Ес және назар аудару бұзылыстарының клиникалық мінездемесі.Сана- сезімнің бұзылыстары Медико-соціальна експертиза при захворюваннях органів системи кровообігу
Медико-соціальна експертиза при захворюваннях органів системи кровообігу Шина Вебера. Шина Порта
Шина Вебера. Шина Порта Профилактики стоматологических заболеваний у беременных женщин. Содержание стоматологического просвещения для беременных женщин
Профилактики стоматологических заболеваний у беременных женщин. Содержание стоматологического просвещения для беременных женщин Дамудың туа біткен ақауларының түрлері
Дамудың туа біткен ақауларының түрлері