- PopQuiz: Managing Patients With Advanced HCC

Содержание
- 2. About These Slides Please feel free to use, update, and share some or all of these
- 3. Quiz Question 1: The incidence of HCC in the United States has tripled over the past
- 4. Quiz Question 1: The incidence of HCC in the United States has tripled over the past
- 5. Age-Adjusted Incidence of HCC by Race 1975-2007 Incidence consistently higher among Asian population Mittal S, et
- 6. 2016 Estimated US Cancer Deaths Liver cancer in 2016 estimated as: The #5 cancer killer in
- 7. Association of Glucose and Lipid Metabolism With HCC Pathogenesis Glucose Metabolism Lipid Metabolism Glycolysis ↓ Glucose
- 8. Case: Diagnosis of HCC 62-yr-old man referred to your clinic with history of self-administered tattoos Saw
- 9. Quiz Question 2: What further testing should be done in order to make the diagnosis of
- 10. Quiz Question 2: What further testing should be done in order to make the diagnosis of
- 11. Diagnosis of HCC by MRI Imaging Baird AJ, et al. J Med Imaging Radiat Oncol. 2013;57:314-320.
- 12. Case: Management of Large Solitary HCC A 32-yr-old woman recently emigrated from Shanghai infected with HBV
- 13. Quiz Question 3: Which of the following is the optimal next step in the management of
- 14. Quiz Question 3: Which of the following is the optimal next step in the management of
- 15. Curative Treatments Transplant Cures both cirrhosis and HCC MELD exception Milan criteria Downsizing Demand > supply
- 16. Survival After Resection for HCC Of 1265 pts with HCC evaluated, only 35 were ideal candidates
- 17. Case: Multifocal HCC With Esophageal Varices A 59-yr-old man with a history of alcohol abuse, who
- 18. Quiz Question 4: Once he has been treated, stabilized, and discharged, further management of this pt
- 19. Quiz Question 4: Once he has been treated, stabilized, and discharged, further management of this pt
- 20. Liver transplantation RFA/PEI Curative treatments (30%); 5-yr survival: 40% to 70% TACE Single Increased Associated diseases
- 21. Case: Large Solitary HCC With Preserved Liver Function A 71-yr-old asymptomatic man with a history of
- 22. Quiz Question 5: Which of the following treatment options would be most suitable for this pt?
- 23. Quiz Question 5: Which of the following treatment options would be most suitable for this pt?
- 24. Current HCC Treatment Algorithm Potentially resectable Assess severity of liver disease Liver transplant candidate? Optimize medical
- 25. Case: Newly Diagnosed Metastatic HCC A 68-yr-old man with PMH significant only for diabetes presents with
- 26. Quiz Question 6: Which of the following is the best choice for this pt? Sorafenib Gemcitabine
- 27. Quiz Question 6: Which of the following is the best choice for this pt? Sorafenib Gemcitabine
- 28. Targeted Therapy: Sorafenib Wilhelm SM, et al. Cancer Res. 2004;64:7099-7109. Wilhelm SM, et al. Mol Cancer
- 29. Phase III SHARP Study: Sorafenib vs Placebo in Advanced HCC Primary endpoints: OS, time to symptomatic
- 30. SHARP: Overall Survival Sorafenib improved OS vs placebo in unresectable HCC Llovet JM, et al. N
- 31. SHARP: Treatment-Emergent AEs Kane RC, et al. Oncologist. 2009:14;95-100.
- 32. Case: Multifocal HCC With Portal Vein Thrombosis A 53-yr-old asymptomatic man without significant past medical history
- 33. Quiz Question 7: Which of the following is the optimal treatment choice for this pt? Referral
- 34. Quiz Question 7: Which of the following is the optimal treatment choice for this pt? Referral
- 35. Radioembolization in HCC Pts With vs Without Portal Vein Thrombosis Radioembolization achieved survival benefit independent of
- 36. Quiz Question 8: In which situation has adjuvant therapy for HCC been shown to be effective?
- 37. Quiz Question 8: In which situation has adjuvant therapy for HCC been shown to be effective?
- 38. Phase II START Trial: TACE + Sorafenib in Asian Pts With HCC TACE + sorafenib effective
- 39. Quiz Question 9: Which of the following has demonstrated superior OS in phase III trials when
- 40. Quiz Question 9: Which of the following has demonstrated superior OS in phase III trials when
- 41. Phase III First-line Targeted Drug Trials for HCC References listed in slide notes.
- 42. Case: Management Following Progression on Sorafenib The pt described above (a 68-yr-old diabetic man with HCC
- 43. Quiz Question 10: Which of the following agents was shown in a phase III trial to
- 44. Quiz Question 10: Which of the following agents was shown in a phase III trial to
- 45. Phase III Second-line Targeted Drug Trials for HCC References listed in slide notes.
- 46. Phase III RESORCE: Regorafenib in HCC After Progression on Sorafenib Randomized, double-blind phase III trial Primary
- 47. RESORCE: Efficacy of Regorafenib vs Placebo 38% reduction in risk of death (HR: 0.62; 95% CI:
- 48. RESORCE: Safety Bruix J, et al. ESMO GI 2016. Abstract LBA-03
- 50. Скачать презентацию
About These Slides
Please feel free to use, update, and share some
About These Slides
Please feel free to use, update, and share some
Quiz Question 1: The incidence of HCC in the United States
Quiz Question 1: The incidence of HCC in the United States
Quiz Question 1: The incidence of HCC in the United States
Quiz Question 1: The incidence of HCC in the United States
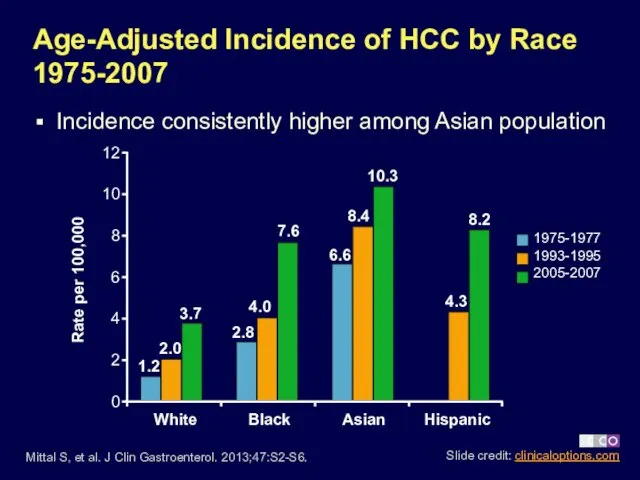
Age-Adjusted Incidence of HCC by Race 1975-2007
Incidence consistently higher among Asian
Age-Adjusted Incidence of HCC by Race 1975-2007
Incidence consistently higher among Asian
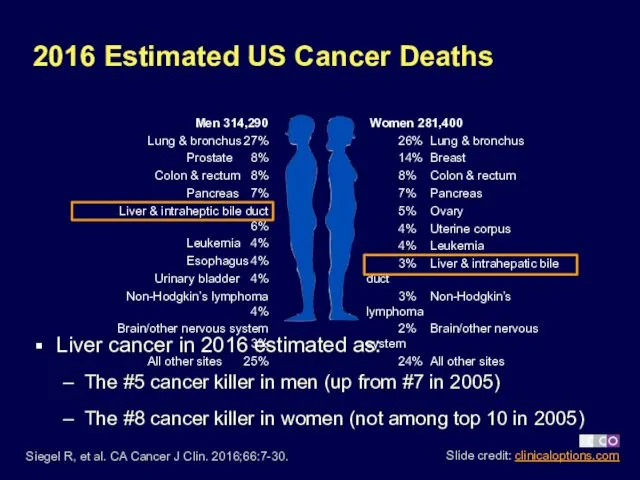
2016 Estimated US Cancer Deaths
Liver cancer in 2016 estimated as:
The #5
2016 Estimated US Cancer Deaths
Liver cancer in 2016 estimated as:
The #5
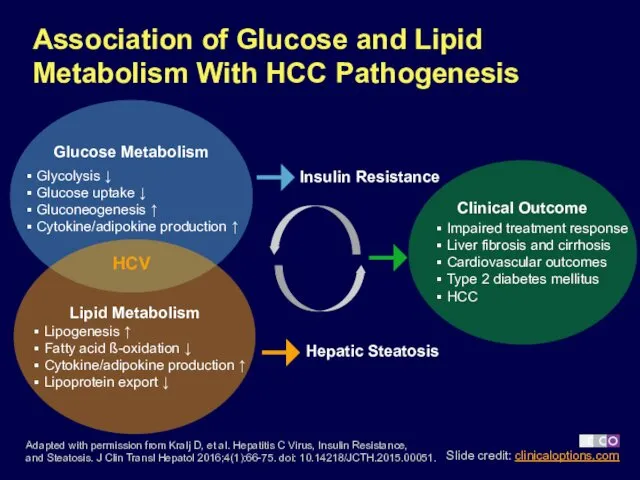
Association of Glucose and Lipid Metabolism With HCC Pathogenesis
Glucose Metabolism
Lipid Metabolism
Glycolysis
Association of Glucose and Lipid Metabolism With HCC Pathogenesis
Glucose Metabolism
Lipid Metabolism
Glycolysis
Case: Diagnosis of HCC
62-yr-old man referred to your clinic with history
Case: Diagnosis of HCC
62-yr-old man referred to your clinic with history
Quiz Question 2: What further testing should be done in order
Quiz Question 2: What further testing should be done in order
Quiz Question 2: What further testing should be done in order
Quiz Question 2: What further testing should be done in order
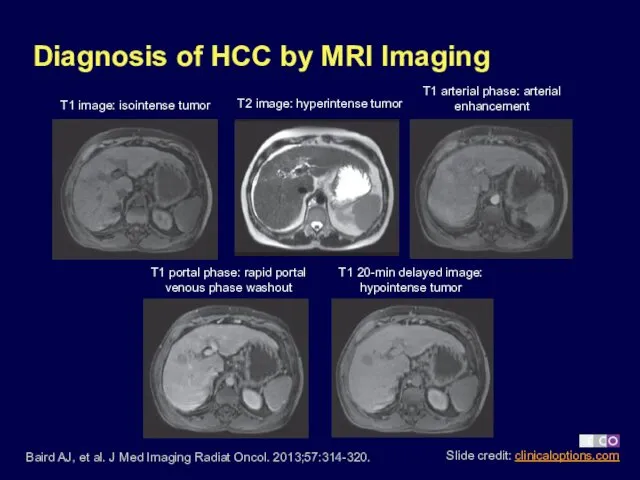
Diagnosis of HCC by MRI Imaging
Baird AJ, et al. J Med
Diagnosis of HCC by MRI Imaging
Baird AJ, et al. J Med
Case: Management of Large Solitary HCC
A 32-yr-old woman recently emigrated from
Case: Management of Large Solitary HCC
A 32-yr-old woman recently emigrated from
Quiz Question 3: Which of the following is the optimal next
Quiz Question 3: Which of the following is the optimal next
Quiz Question 3: Which of the following is the optimal next
Quiz Question 3: Which of the following is the optimal next
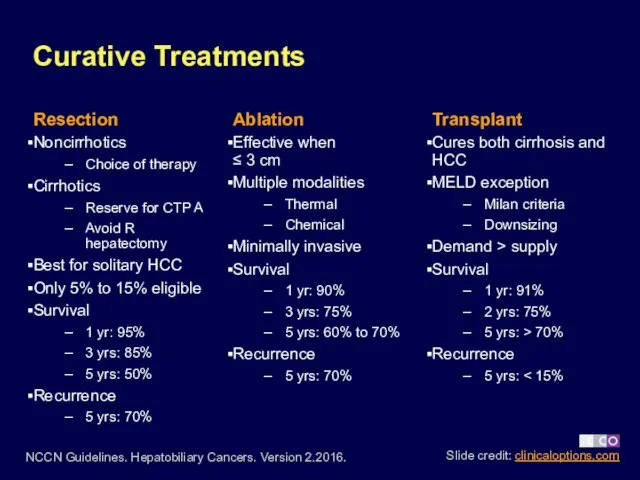
Curative Treatments
Transplant
Cures both cirrhosis and HCC
MELD exception
Milan criteria
Downsizing
Demand > supply
Survival
Curative Treatments
Transplant
Cures both cirrhosis and HCC
MELD exception
Milan criteria
Downsizing
Demand > supply
Survival
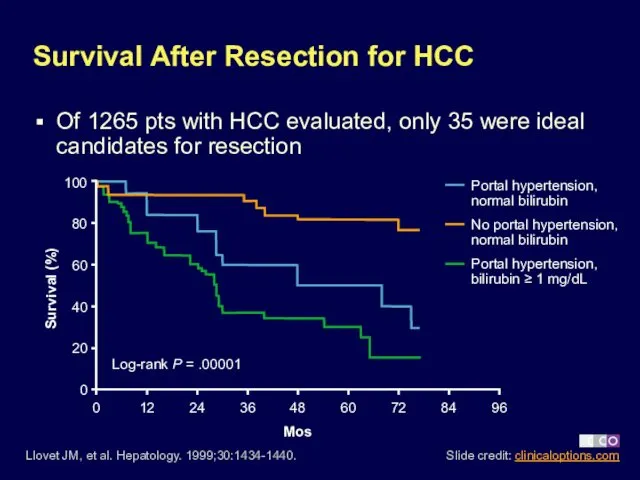
Survival After Resection for HCC
Of 1265 pts with HCC evaluated, only
Survival After Resection for HCC
Of 1265 pts with HCC evaluated, only
Case: Multifocal HCC With Esophageal Varices
A 59-yr-old man with a history
Case: Multifocal HCC With Esophageal Varices
A 59-yr-old man with a history
Quiz Question 4: Once he has been treated, stabilized, and discharged,
Quiz Question 4: Once he has been treated, stabilized, and discharged,
Quiz Question 4: Once he has been treated, stabilized, and discharged,
Quiz Question 4: Once he has been treated, stabilized, and discharged,
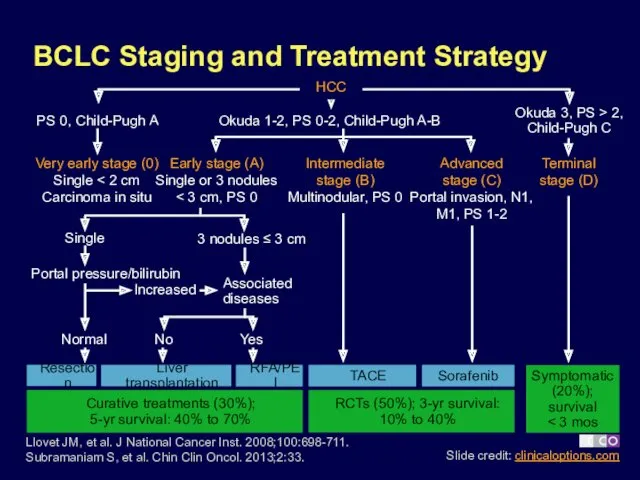
Liver transplantation
RFA/PEI
Curative treatments (30%);
5-yr survival: 40% to 70%
TACE
Single
Increased
Associated
diseases
Normal
No
Yes
Sorafenib
Portal pressure/bilirubin
3 nodules
Liver transplantation
RFA/PEI
Curative treatments (30%);
5-yr survival: 40% to 70%
TACE
Single
Increased
Associated
diseases
Normal
No
Yes
Sorafenib
Portal pressure/bilirubin
3 nodules
Case: Large Solitary HCC With Preserved Liver Function
A 71-yr-old asymptomatic man
Case: Large Solitary HCC With Preserved Liver Function
A 71-yr-old asymptomatic man
Quiz Question 5: Which of the following treatment options would be
Quiz Question 5: Which of the following treatment options would be
Quiz Question 5: Which of the following treatment options would be
Quiz Question 5: Which of the following treatment options would be
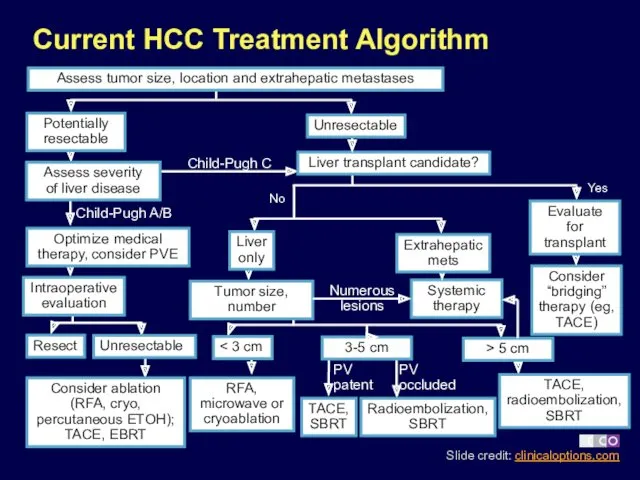
Current HCC Treatment Algorithm
Potentially
resectable
Assess severity
of liver disease
Liver transplant candidate?
Optimize medical
therapy, consider
Current HCC Treatment Algorithm
Potentially
resectable
Assess severity
of liver disease
Liver transplant candidate?
Optimize medical therapy, consider
Case: Newly Diagnosed Metastatic HCC
A 68-yr-old man with PMH significant only
Case: Newly Diagnosed Metastatic HCC
A 68-yr-old man with PMH significant only
Quiz Question 6: Which of the following is the best choice
Quiz Question 6: Which of the following is the best choice
Quiz Question 6: Which of the following is the best choice
Quiz Question 6: Which of the following is the best choice
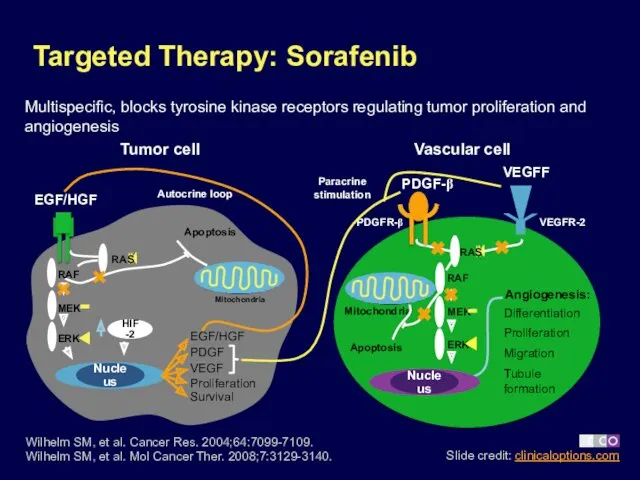
Targeted Therapy: Sorafenib
Wilhelm SM, et al. Cancer Res. 2004;64:7099-7109.
Wilhelm
Targeted Therapy: Sorafenib
Wilhelm SM, et al. Cancer Res. 2004;64:7099-7109. Wilhelm
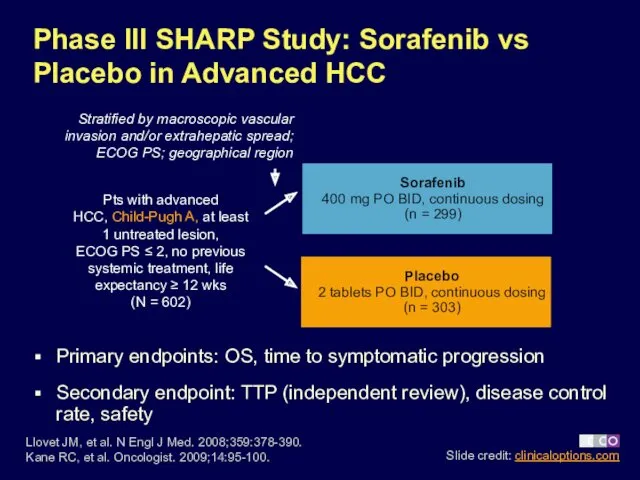
Phase III SHARP Study: Sorafenib vs Placebo in Advanced HCC
Primary endpoints:
Phase III SHARP Study: Sorafenib vs Placebo in Advanced HCC
Primary endpoints:
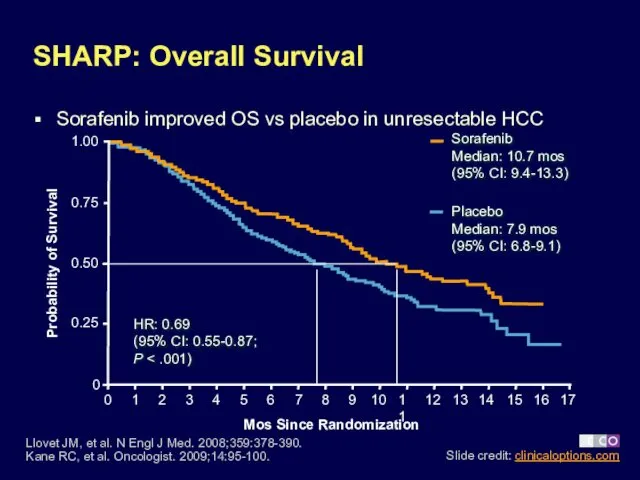
SHARP: Overall Survival
Sorafenib improved OS vs placebo in unresectable HCC
Llovet JM,
SHARP: Overall Survival
Sorafenib improved OS vs placebo in unresectable HCC
Llovet JM,
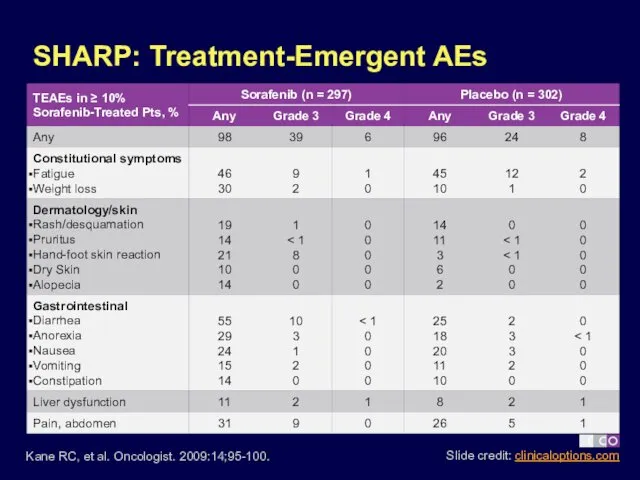
SHARP: Treatment-Emergent AEs
Kane RC, et al. Oncologist. 2009:14;95-100.
SHARP: Treatment-Emergent AEs
Kane RC, et al. Oncologist. 2009:14;95-100.
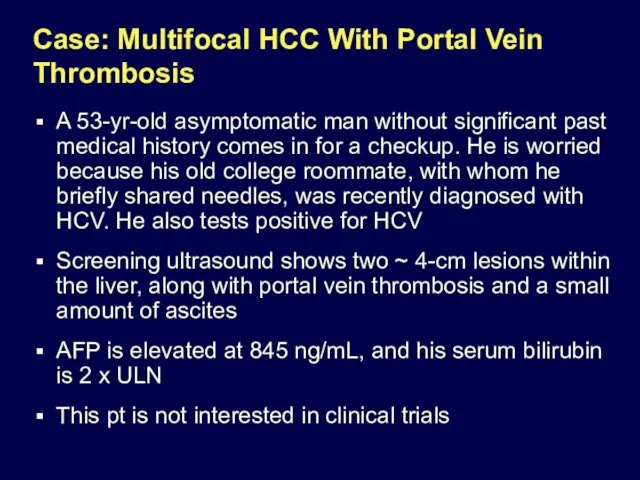
Case: Multifocal HCC With Portal Vein Thrombosis
A 53-yr-old asymptomatic man without
Case: Multifocal HCC With Portal Vein Thrombosis
A 53-yr-old asymptomatic man without
Quiz Question 7: Which of the following is the optimal treatment
Quiz Question 7: Which of the following is the optimal treatment
Quiz Question 7: Which of the following is the optimal treatment
Quiz Question 7: Which of the following is the optimal treatment
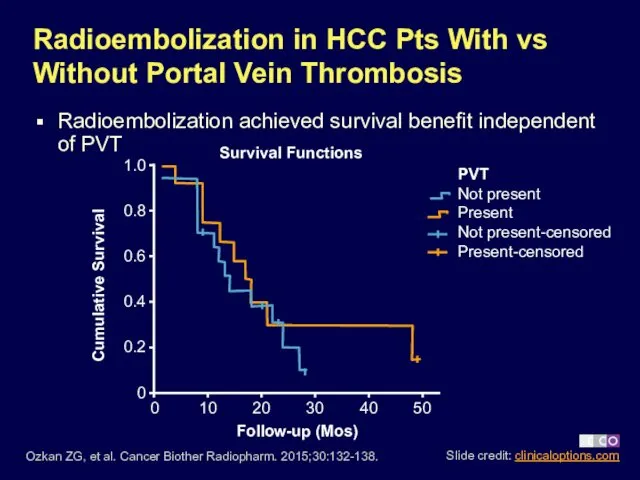
Radioembolization in HCC Pts With vs Without Portal Vein Thrombosis
Radioembolization achieved
Radioembolization in HCC Pts With vs Without Portal Vein Thrombosis
Radioembolization achieved
Quiz Question 8: In which situation has adjuvant therapy for HCC
Quiz Question 8: In which situation has adjuvant therapy for HCC
Quiz Question 8: In which situation has adjuvant therapy for HCC
Quiz Question 8: In which situation has adjuvant therapy for HCC
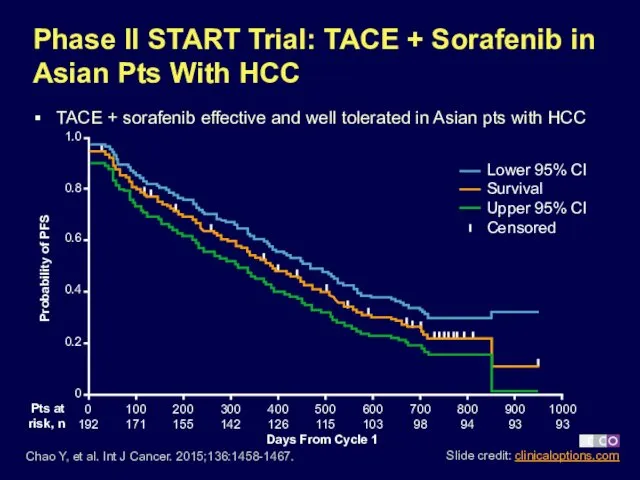
Phase II START Trial: TACE + Sorafenib in Asian Pts With
Phase II START Trial: TACE + Sorafenib in Asian Pts With
Quiz Question 9: Which of the following has demonstrated superior OS
Quiz Question 9: Which of the following has demonstrated superior OS
Quiz Question 9: Which of the following has demonstrated superior OS
Quiz Question 9: Which of the following has demonstrated superior OS
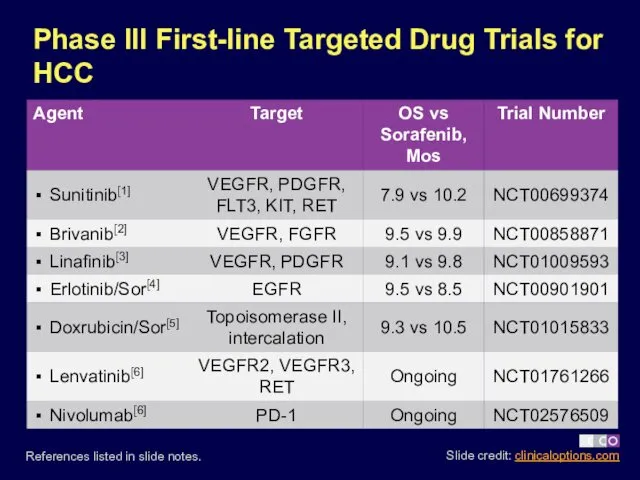
Phase III First-line Targeted Drug Trials for HCC
References listed in
Phase III First-line Targeted Drug Trials for HCC
References listed in
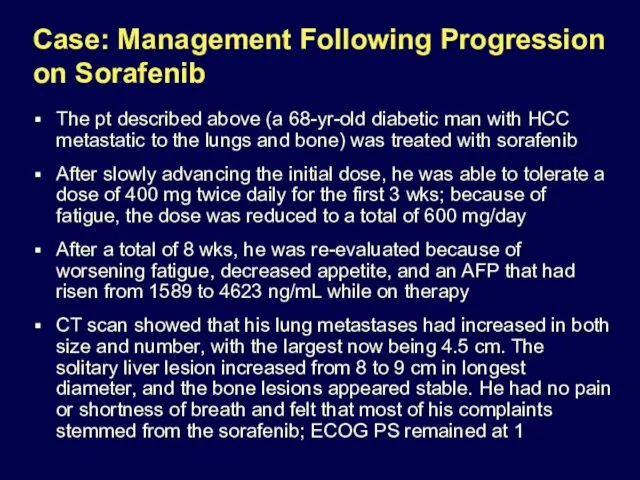
Case: Management Following Progression on Sorafenib
The pt described above (a 68-yr-old
Case: Management Following Progression on Sorafenib
The pt described above (a 68-yr-old
Quiz Question 10: Which of the following agents was shown in
Quiz Question 10: Which of the following agents was shown in
Quiz Question 10: Which of the following agents was shown in
Quiz Question 10: Which of the following agents was shown in
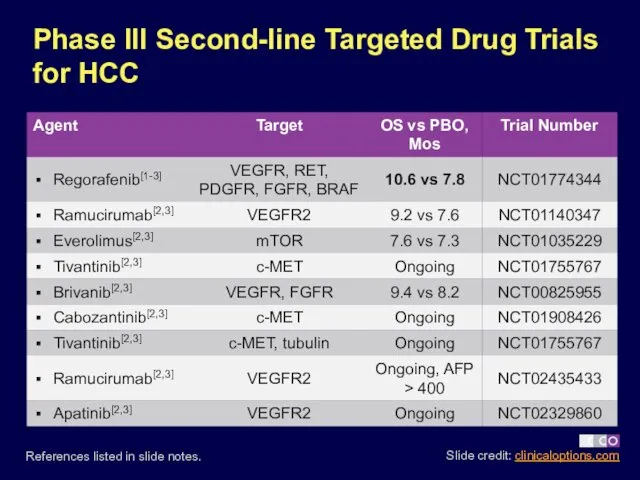
Phase III Second-line Targeted Drug Trials for HCC
References listed in
Phase III Second-line Targeted Drug Trials for HCC
References listed in
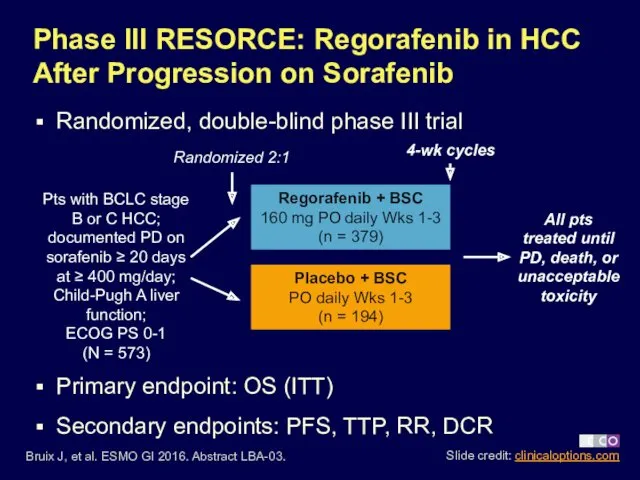
Phase III RESORCE: Regorafenib in HCC After Progression on Sorafenib
Randomized,
Phase III RESORCE: Regorafenib in HCC After Progression on Sorafenib
Randomized,
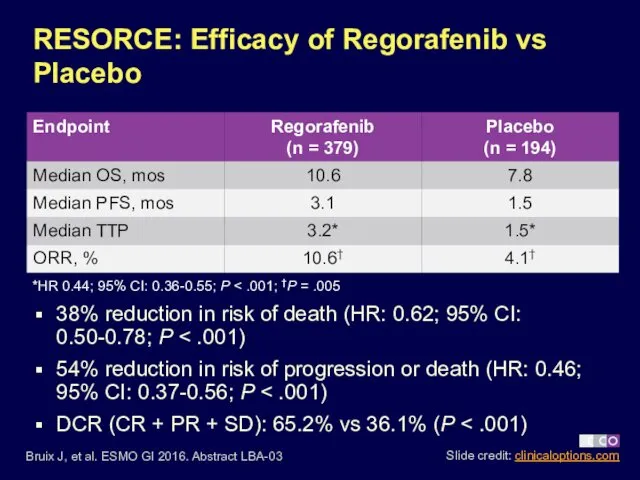
RESORCE: Efficacy of Regorafenib vs Placebo
38% reduction in risk of death
RESORCE: Efficacy of Regorafenib vs Placebo
38% reduction in risk of death
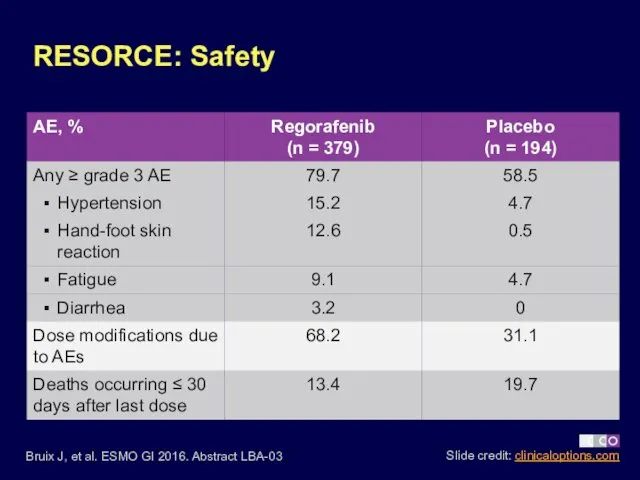
RESORCE: Safety
Bruix J, et al. ESMO GI 2016. Abstract LBA-03
RESORCE: Safety
Bruix J, et al. ESMO GI 2016. Abstract LBA-03
 Социальное медицинское страхование в Республике Казахстан
Социальное медицинское страхование в Республике Казахстан Балалар мен жасөспірімдердің дене тәрбиесі мен шынығуының физикалық-гигиеналық негіздері
Балалар мен жасөспірімдердің дене тәрбиесі мен шынығуының физикалық-гигиеналық негіздері Метаболикалық синдромның биохимиясы
Метаболикалық синдромның биохимиясы ppt
ppt District sales manager, Novo Nordisk
District sales manager, Novo Nordisk 3D принтер в медицине
3D принтер в медицине Методы определения подлинности лекарственного растительного сырья. Занятие №2
Методы определения подлинности лекарственного растительного сырья. Занятие №2 Ампутация в хирургической практике
Ампутация в хирургической практике Лямблиоз. Клиника
Лямблиоз. Клиника Ғалымдар қоршаған ортадан келетін токсиндер ағзаның қартаюының жеделдетілуінің негізгі себептерінің бірі екенін анықтады
Ғалымдар қоршаған ортадан келетін токсиндер ағзаның қартаюының жеделдетілуінің негізгі себептерінің бірі екенін анықтады Инструментальные методы исследования сердца
Инструментальные методы исследования сердца Патронаж здорового новорожденного на дому с оформлением учебной амбулаторной карты
Патронаж здорового новорожденного на дому с оформлением учебной амбулаторной карты Аритмии сердца: ЭКГ-диагностика
Аритмии сердца: ЭКГ-диагностика Эстрогендерді қабылдау мен әйелдерде эдометрийдің қатерлі ісігінің дамуы арасындағы байланыс
Эстрогендерді қабылдау мен әйелдерде эдометрийдің қатерлі ісігінің дамуы арасындағы байланыс Точечный массаж
Точечный массаж Microscopic colitis
Microscopic colitis Интенсивная терапия осложненных форм СД, основы КЩС
Интенсивная терапия осложненных форм СД, основы КЩС Қазақстан республикасындағы психиатриялық көмекті ұйымдастыру
Қазақстан республикасындағы психиатриялық көмекті ұйымдастыру Порядок проведения обязательных медицинских осмотров
Порядок проведения обязательных медицинских осмотров Пренатальное развитие ребёнка
Пренатальное развитие ребёнка Шылым шегу
Шылым шегу Догляд за хворими із захворюваннями та ушкодженнями органів черевної порожнини
Догляд за хворими із захворюваннями та ушкодженнями органів черевної порожнини Синдром слабости синусового узла
Синдром слабости синусового узла Цереброваскулярные заболевания. Причины роста сосудистых заболеваний
Цереброваскулярные заболевания. Причины роста сосудистых заболеваний Балалардың физикалық критерийлер анықтау
Балалардың физикалық критерийлер анықтау Клеточные факторы врождённого иммунитета. Фагоцитоз и его стадии
Клеточные факторы врождённого иммунитета. Фагоцитоз и его стадии Тік ішектің және анустың атрезиясы
Тік ішектің және анустың атрезиясы Конусно-лучевая компьютерная томография в терапевтической стоматологии
Конусно-лучевая компьютерная томография в терапевтической стоматологии