- Primary and secondary tuberculosis. (Lecture 5)

Содержание
- 2. CLINICAL FORMS TB of respiratory organs Primary tuberculous complex. Disseminated lung tuberculosis. Nidus lung tuberculosis. Infiltrative
- 3. CLINICAL FORMS TB of exstrarespiratory organs TB of bronchi, trachea and upper respiratory tract. TB of
- 4. CHARACTERISTIC OF TUBERCULOUS PROCESS Localization and spreading: Localization of defects in lungs according to the numbers
- 5. ETIOLOGIC METHOD OF CONFIRMATION: (MBT +) – it is confirmed by results of bacteriological analysis (cipher
- 6. (Resist 0) MBT resistance to preparations of I line wasn’t analyzed; (Resist -) resistance to preparations
- 7. Types of TB cases New case of TB – A patient who has never been treated
- 8. Previously treated case of TB 1. Relapse patients have previously been treated for TB, were declared
- 9. Case of multidrug-resistant TB (MDR-TB) – TB that is resistant to two first-line drugs: isoniazid and
- 10. Clinical forms of pulmonary tuberculosis There such clinical forms of pulmonary TB, as milliary, disseminated, focal,
- 11. Clinical forms of extra-pulmonary tuberculosis It depends on the affected organ. Miliary tuberculosis, tuberculosis of intrathoracic
- 12. Phases of TB There are such TB process phases: infiltration, decay (corresponding Destruction +), contamination, resorption,
- 13. Diagnosis examples New case of TB (01.02.2016) upper lobe of right lung (infiltrative), contamination phase, Destr
- 14. RADIOLOGICAL SYNDROMS To explain radiological features of tuberculosis clinical form we must understand radiological syndroms. There
- 15. Abnormal pulmonary pattern syndrome Increased and enriching the lung picture (at inflammatory processes, collagenous diseases, tumor,
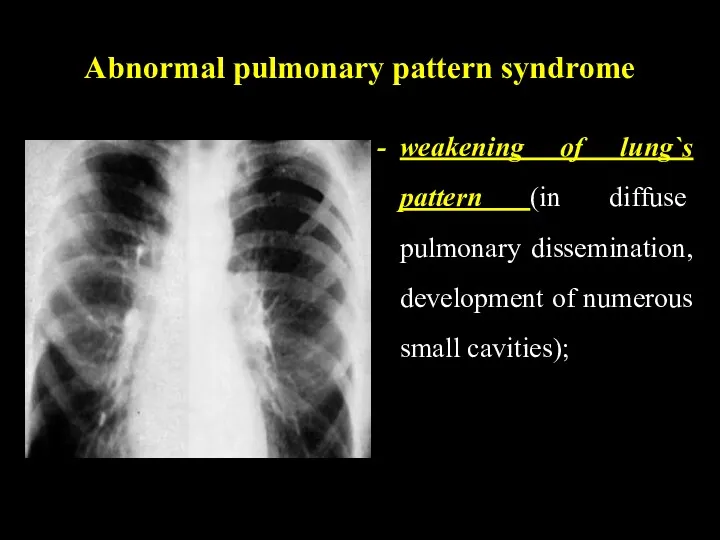
- 16. Abnormal pulmonary pattern syndrome weakening of lung`s pattern (in diffuse pulmonary dissemination, development of numerous small
- 17. Abnormal pulmonary pattern syndrome depletion of the picture (at inflating the lungs, lung arterial nets hypoplasia);
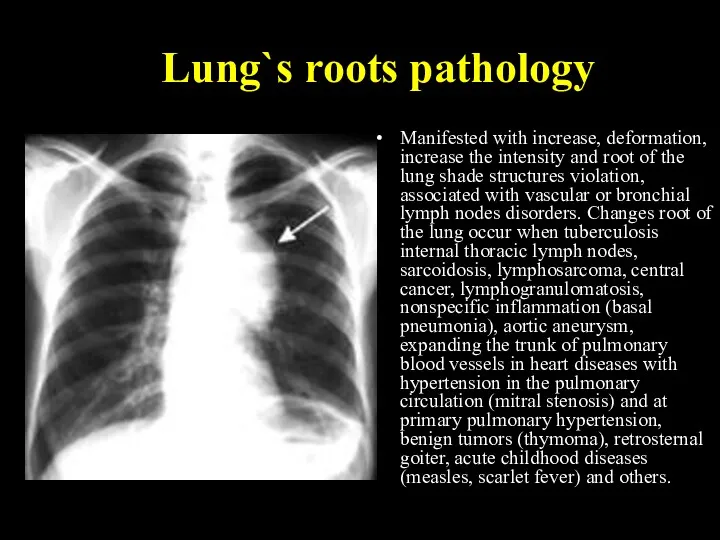
- 18. Lung`s roots pathology Manifested with increase, deformation, increase the intensity and root of the lung shade
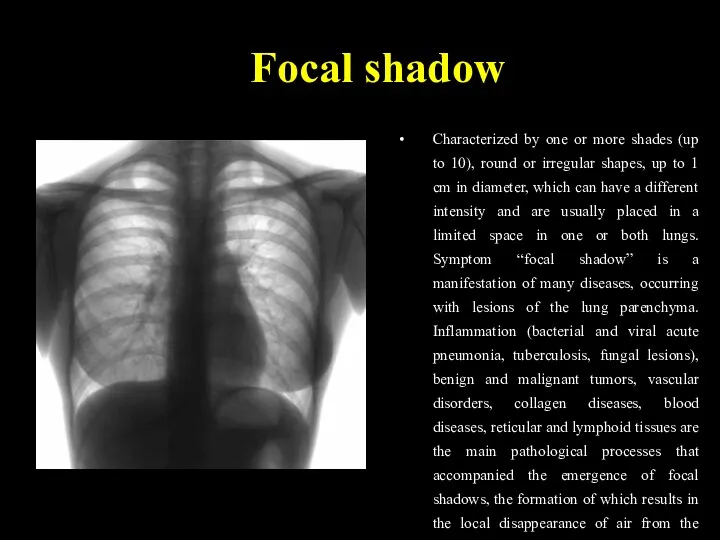
- 19. Focal shadow Characterized by one or more shades (up to 10), round or irregular shapes, up
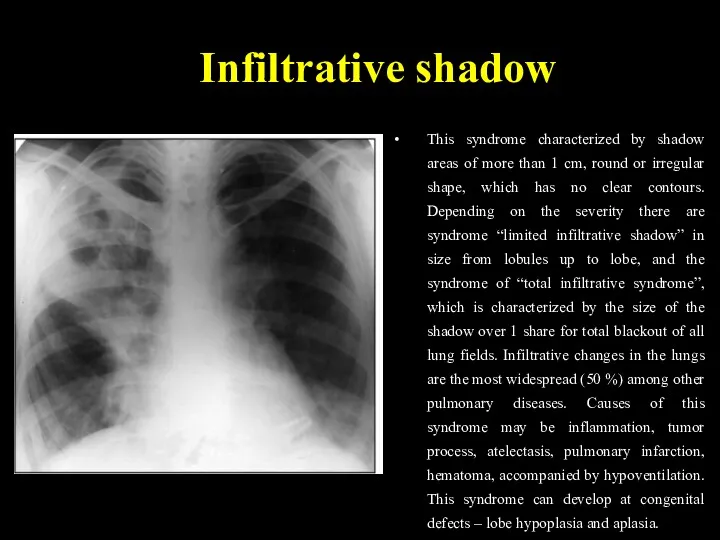
- 20. Infiltrative shadow This syndrome characterized by shadow areas of more than 1 cm, round or irregular
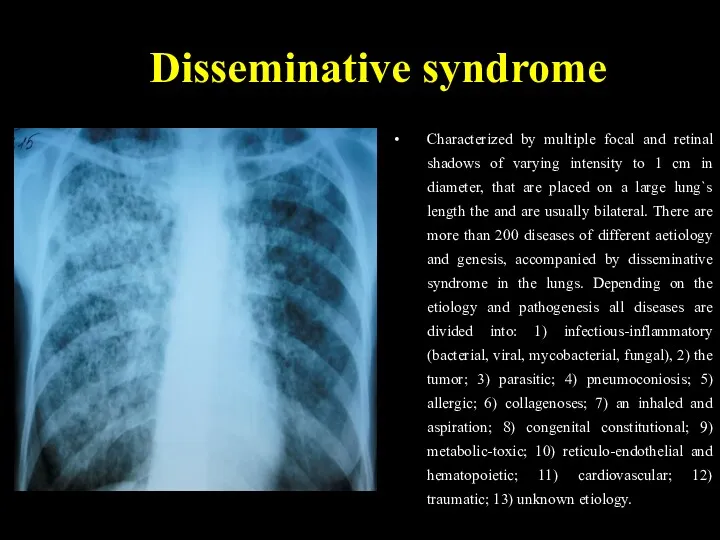
- 21. Disseminative syndrome Characterized by multiple focal and retinal shadows of varying intensity to 1 cm in
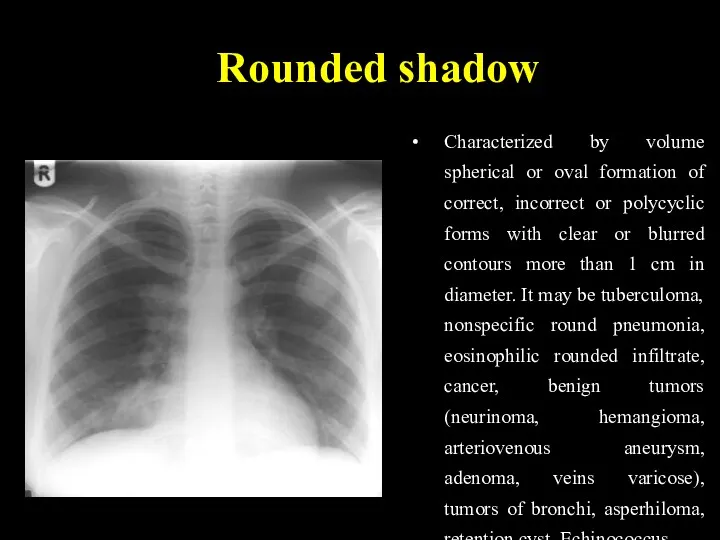
- 22. Rounded shadow Characterized by volume spherical or oval formation of correct, incorrect or polycyclic forms with
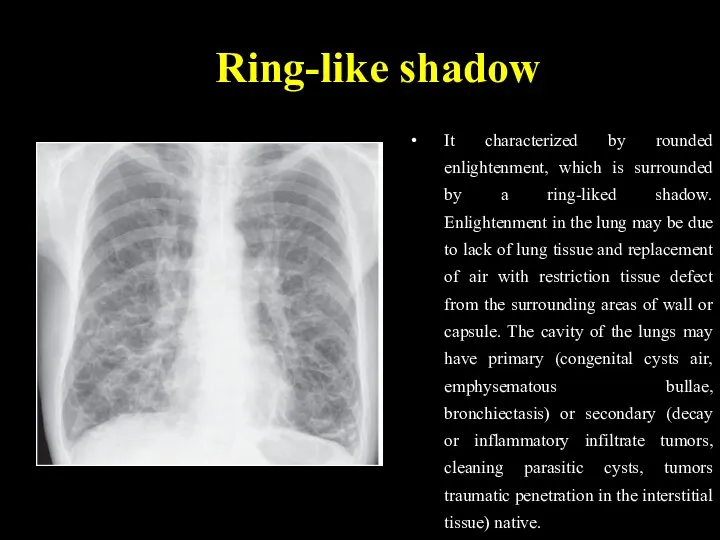
- 23. Ring-like shadow It characterized by rounded enlightenment, which is surrounded by a ring-liked shadow. Enlightenment in
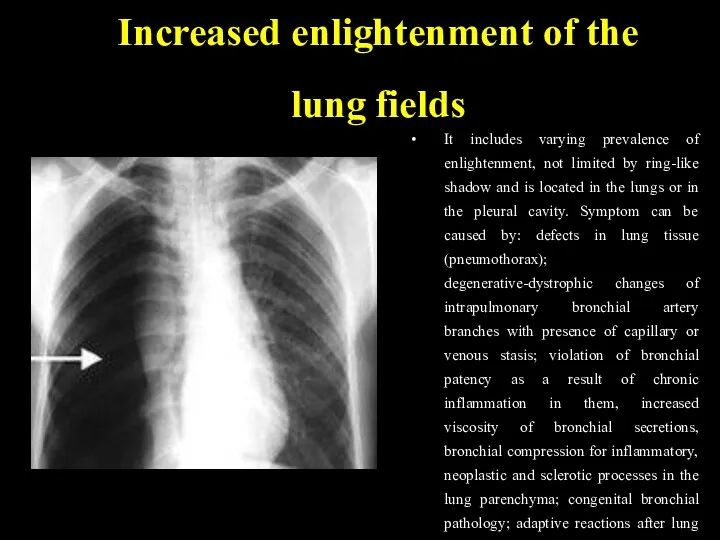
- 24. Increased enlightenment of the lung fields It includes varying prevalence of enlightenment, not limited by ring-like
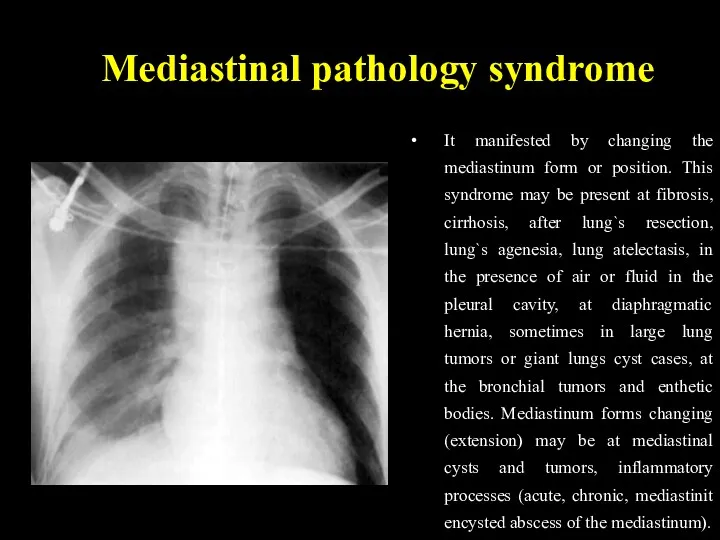
- 25. Mediastinal pathology syndrome It manifested by changing the mediastinum form or position. This syndrome may be
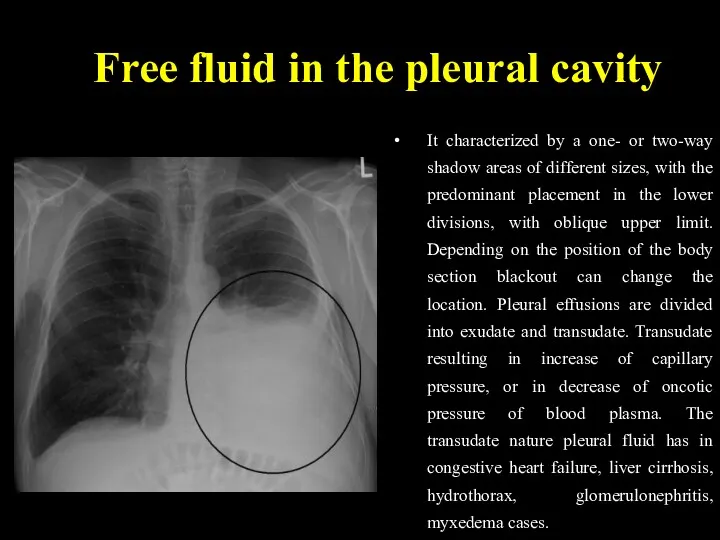
- 26. Free fluid in the pleural cavity It characterized by a one- or two-way shadow areas of
- 27. Free fluid in the pleural cavity The most frequent cause of exudative pleurisy of different etiology
- 28. Depending on pathogenesis the tuberculosis is divided primary and secondary. Primary tuberculosis develops after the first
- 29. PRIMARY TUBERCULOSIS Primary is considered tuberculosis that develops in firstly infected persons. The period from the
- 30. Para-specific reactions (tuberculosis “masks”) In primary tuberculosis there are situations where the disease occurs more on
- 31. “Flu-like” TB mask The most frequently tuberculosis in active phase occurs in such frequent, long, unusual
- 32. “pneumonic” mask The second frequency is “pneumonic” mask. This is repeated recurrent pneumonia, especially in the
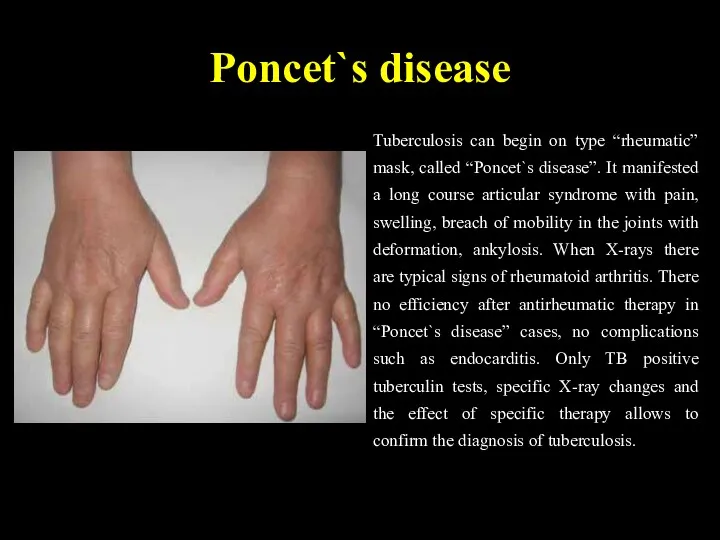
- 33. Poncet`s disease Tuberculosis can begin on type “rheumatic” mask, called “Poncet`s disease”. It manifested a long
- 34. “Neurological” TB mask “Neurological” TB mask manifests as long, persistent neuralgia, which can not be usually
- 35. “Lupus-like” TB mask “Lupus-like” mask manifests typical erythema on the face in the form of "butterfly",
- 36. “Hematological” mask “Hematological” mask of tuberculosis occurs with bone marrow hypoplasia, leukopenia, anemia, thrombocytopenia, sometimes with
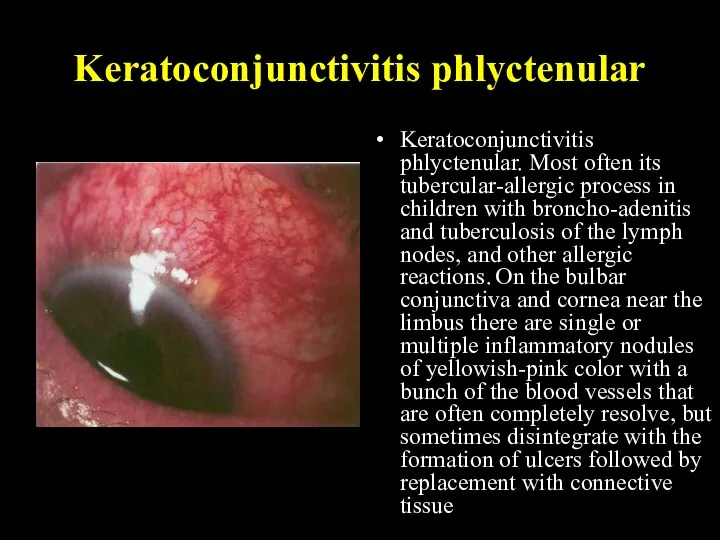
- 37. Keratoconjunctivitis phlyctenular Keratoconjunctivitis phlyctenular. Most often its tubercular-allergic process in children with broncho-adenitis and tuberculosis of
- 38. CHARACTERISTIC SIGNS OF PRIMARY TUBERCULOSIS: the intensity of tuberculin reactions organism hypersensibilization to MBT injury of
- 39. PRIMARY TUBERCULOUS COMPLEX 1. PATHOGENESIS After the penetration of MBT into the lungs, primary lesion (primary
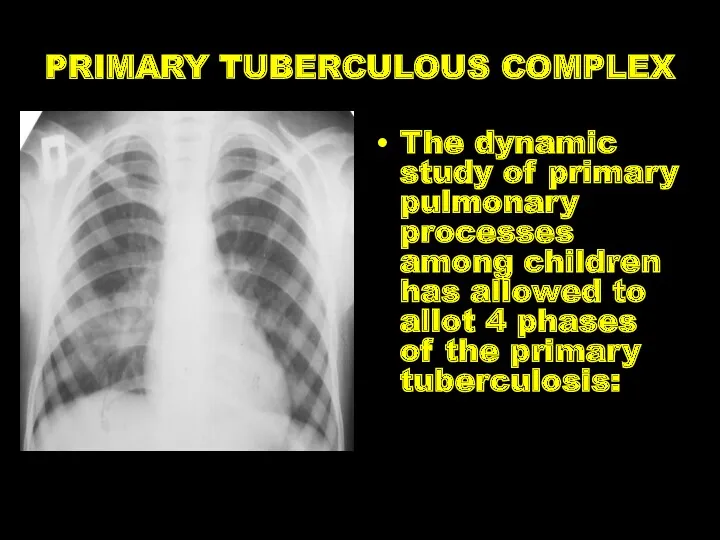
- 40. PRIMARY TUBERCULOUS COMPLEX The dynamic study of primary pulmonary processes among children has allowed to allot
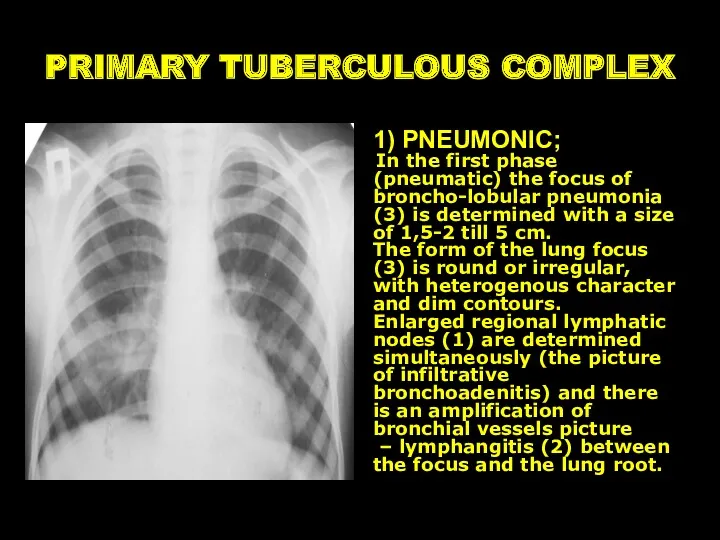
- 41. PRIMARY TUBERCULOUS COMPLEX 1) PNEUMONIC; In the first phase (pneumatic) the focus of broncho-lobular pneumonia (3)
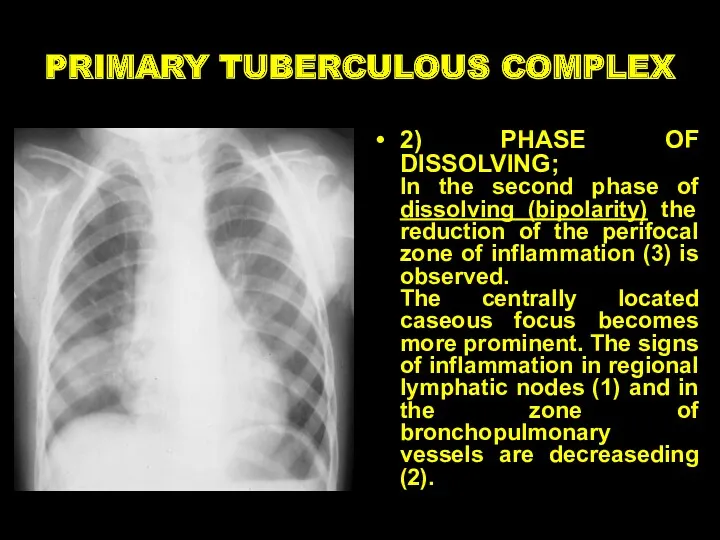
- 42. PRIMARY TUBERCULOUS COMPLEX 2) PHASE OF DISSOLVING; In the second phase of dissolving (bipolarity) the reduction
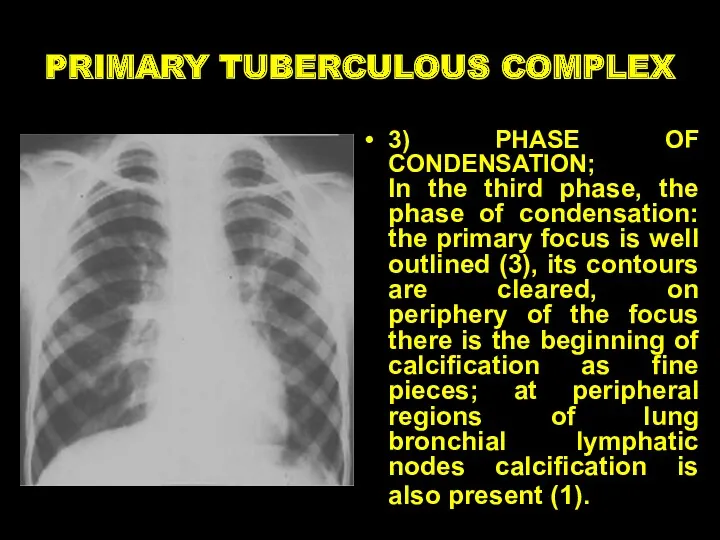
- 43. PRIMARY TUBERCULOUS COMPLEX 3) PHASE OF CONDENSATION; In the third phase, the phase of condensation: the
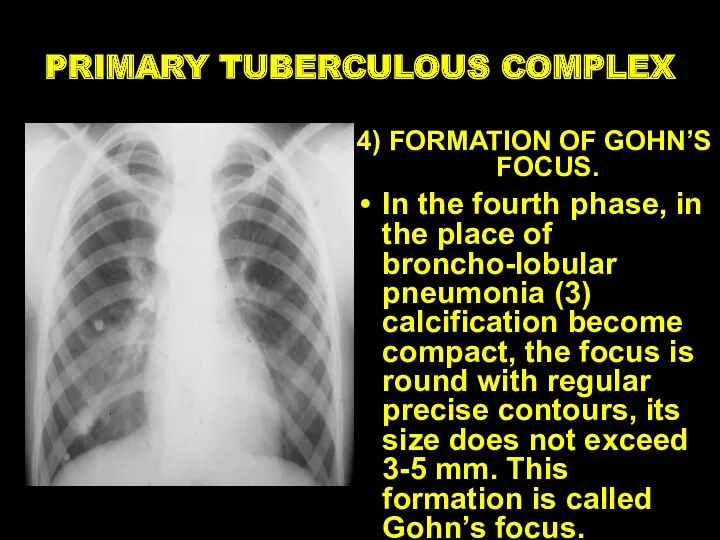
- 44. PRIMARY TUBERCULOUS COMPLEX 4) FORMATION OF GOHN’S FOCUS. In the fourth phase, in the place of
- 45. TUBERCULOSIS OF INTRATHORACIC LYMPHATIC NODES Bronchoadenitis is a disease of the lymph nodes of the lungs
- 46. Clinical pattern of tuberculous bronchoadenitis acute intoxication specific clinical symptoms: subfebrile temperature, deterioration of general condition,
- 47. Clinico-roentgenologically variants of intrathoracic lymphatic nodes TB tumour like (tumoursimilar) form infiltrative form Left side tumorous
- 48. Miliary tuberculosis Generalized TB clinical form with the hematogenic type of dissemination and acute course
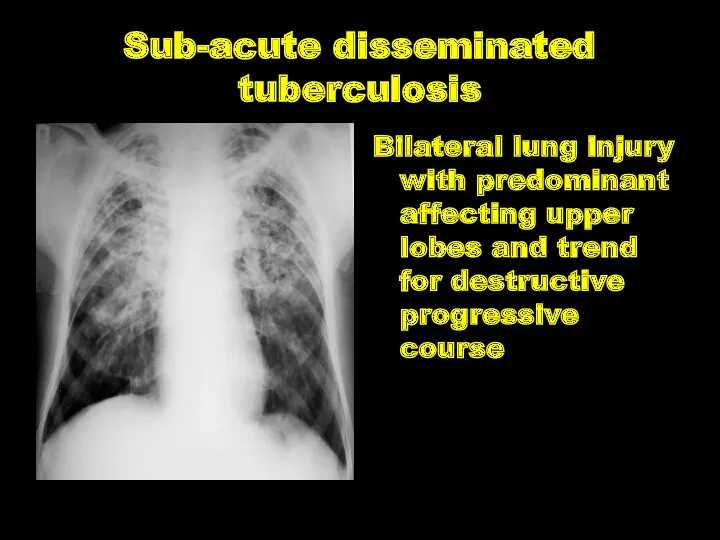
- 49. Sub-acute disseminated tuberculosis Bilateral lung injury with predominant affecting upper lobes and trend for destructive progressive
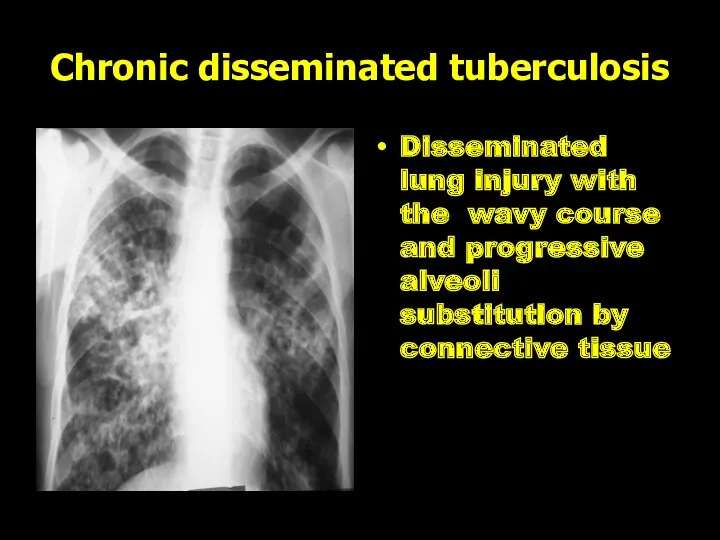
- 50. Chronic disseminated tuberculosis Disseminated lung injury with the wavy course and progressive alveoli substitution by connective
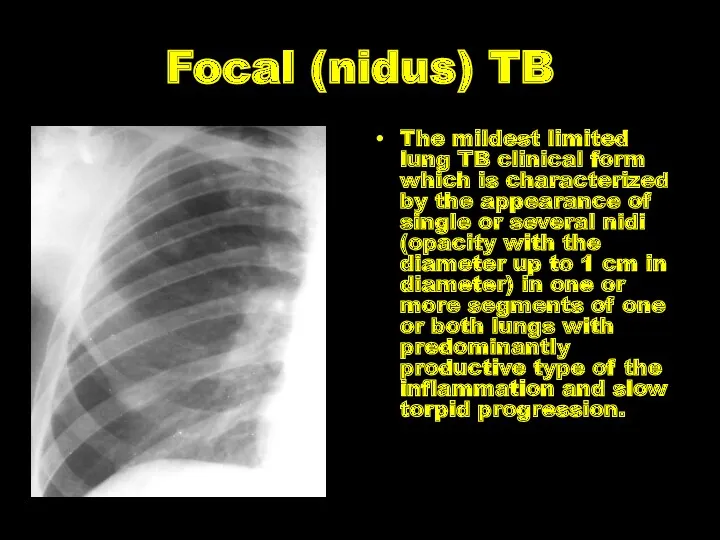
- 51. Focal (nidus) TB The mildest limited lung TB clinical form which is characterized by the appearance
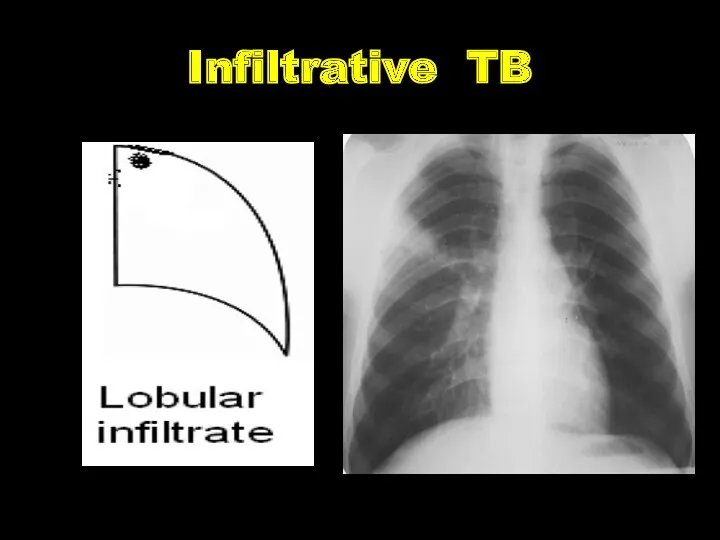
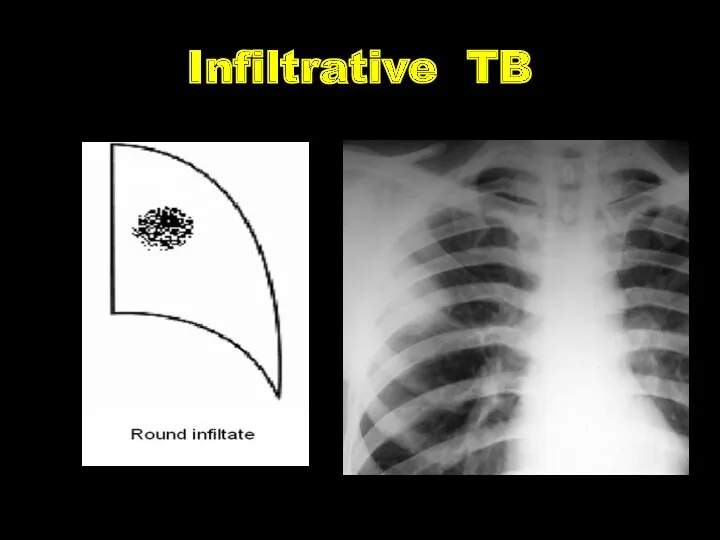
- 52. Infiltrative TB The expansive lung TB clinical form which is characterized by the appearance of different
- 53. Infiltrative TB
- 54. Infiltrative TB
- 55. Infiltrative TB
- 56. Infiltrative TB
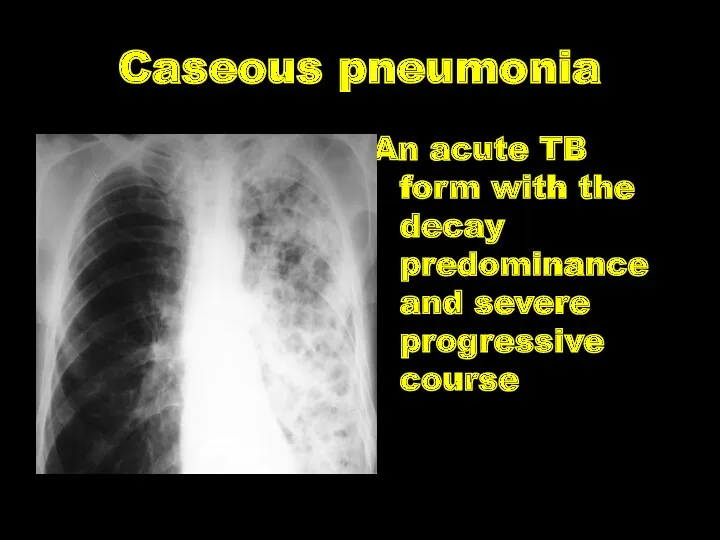
- 57. Caseous pneumonia An acute TB form with the decay predominance and severe progressive course
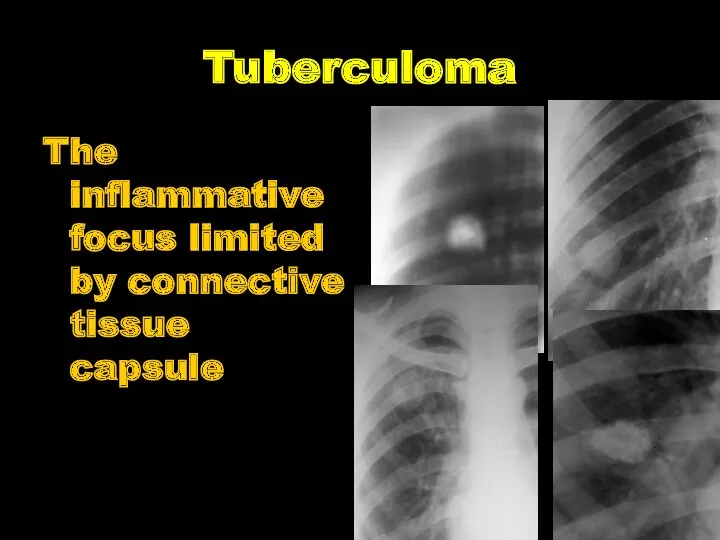
- 58. Tuberculoma The inflammative focus limited by connective tissue capsule
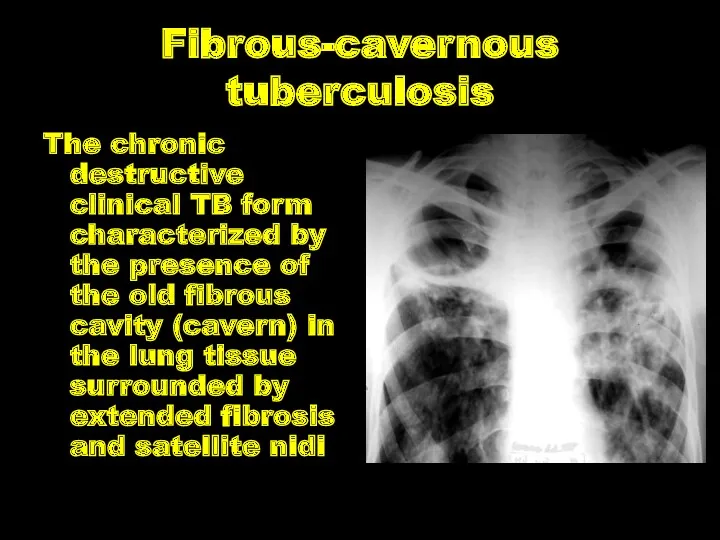
- 59. Fibrous-cavernous tuberculosis The chronic destructive clinical TB form characterized by the presence of the old fibrous
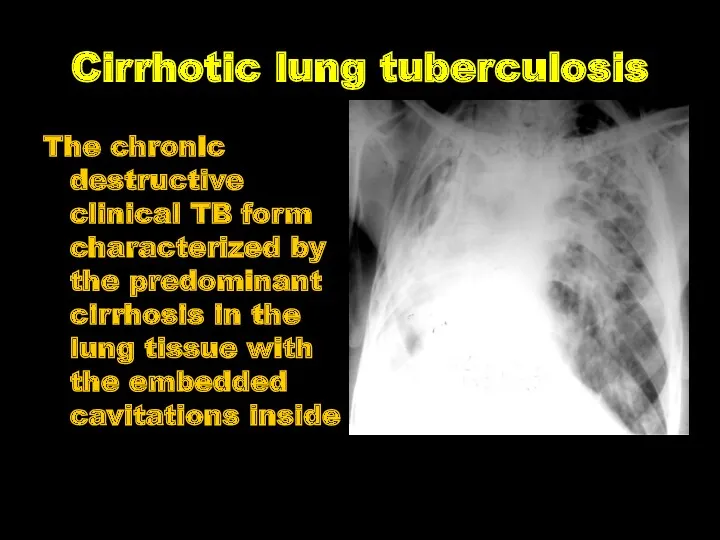
- 60. Cirrhotic lung tuberculosis The chronic destructive clinical TB form characterized by the predominant cirrhosis in the
- 61. Tuberculous meningitis is the inflammation of the membranes of cerebrum and (or) spinal cord, caused by
- 62. Pathogenesis. Tuberculous meningitis may be primary (in 20 %) and secondary (in 80 %), as children
- 63. Pathological anatomy. The specific process is predominantly localized in the soft membrane of cerebral base, in
- 64. Clinic of Tuberculous meningitis I. A prodromic period the duration is from 1 to 4 weeks:
- 65. 5 components (syndromes) are discriminated in the clinical picture of tuberculous meningitis: Intoxicating syndrome Meningeal syndrome:
- 66. Meningeal symptoms rigidity cervical muscles
- 68. Скачать презентацию
CLINICAL FORMS
TB of respiratory organs
Primary tuberculous complex.
Disseminated lung tuberculosis.
CLINICAL FORMS
TB of respiratory organs
Primary tuberculous complex.
Disseminated lung tuberculosis.
CLINICAL FORMS
TB of exstrarespiratory organs
TB of bronchi, trachea and upper respiratory
CLINICAL FORMS
TB of exstrarespiratory organs
TB of bronchi, trachea and upper respiratory
CHARACTERISTIC OF TUBERCULOUS PROCESS
Localization and spreading: Localization of defects in lungs
CHARACTERISTIC OF TUBERCULOUS PROCESS
Localization and spreading: Localization of defects in lungs
ETIOLOGIC METHOD OF CONFIRMATION:
(MBT +) – it is confirmed by results
ETIOLOGIC METHOD OF CONFIRMATION:
(MBT +) – it is confirmed by results

(Resist 0) MBT resistance to preparations of I line wasn’t analyzed;
(Resist
(Resist 0) MBT resistance to preparations of I line wasn’t analyzed;
(Resist
Types of TB cases
New case of TB – A patient who
Types of TB cases
New case of TB – A patient who
Previously treated case of TB
1. Relapse patients have previously been
Previously treated case of TB
1. Relapse patients have previously been
Case of multidrug-resistant TB (MDR-TB) – TB that is resistant to
Case of multidrug-resistant TB (MDR-TB) – TB that is resistant to
Clinical forms of pulmonary tuberculosis
There such clinical forms of pulmonary TB,
Clinical forms of pulmonary tuberculosis
There such clinical forms of pulmonary TB,
Clinical forms of extra-pulmonary tuberculosis
It depends on the affected organ. Miliary
Clinical forms of extra-pulmonary tuberculosis
It depends on the affected organ. Miliary
Phases of TB
There are such TB process phases: infiltration, decay (corresponding
Phases of TB
There are such TB process phases: infiltration, decay (corresponding
Diagnosis examples
New case of TB (01.02.2016) upper lobe of right lung
Diagnosis examples
New case of TB (01.02.2016) upper lobe of right lung
RADIOLOGICAL SYNDROMS
To explain radiological features of tuberculosis clinical form we must
RADIOLOGICAL SYNDROMS
To explain radiological features of tuberculosis clinical form we must
Abnormal pulmonary pattern syndrome
Increased and enriching the lung picture (at inflammatory
Abnormal pulmonary pattern syndrome
Increased and enriching the lung picture (at inflammatory
Abnormal pulmonary pattern syndrome
weakening of lung`s pattern (in diffuse pulmonary dissemination,
Abnormal pulmonary pattern syndrome
weakening of lung`s pattern (in diffuse pulmonary dissemination,

Abnormal pulmonary pattern syndrome
depletion of the picture (at inflating the lungs,
Abnormal pulmonary pattern syndrome
depletion of the picture (at inflating the lungs,
Lung`s roots pathology
Manifested with increase, deformation, increase the intensity and root
Lung`s roots pathology
Manifested with increase, deformation, increase the intensity and root
Focal shadow
Characterized by one or more shades (up to 10), round
Focal shadow
Characterized by one or more shades (up to 10), round
Infiltrative shadow
This syndrome characterized by shadow areas of more than 1
Infiltrative shadow
This syndrome characterized by shadow areas of more than 1
Disseminative syndrome
Characterized by multiple focal and retinal shadows of varying intensity
Disseminative syndrome
Characterized by multiple focal and retinal shadows of varying intensity
Rounded shadow
Characterized by volume spherical or oval formation of correct, incorrect
Rounded shadow
Characterized by volume spherical or oval formation of correct, incorrect
Ring-like shadow
It characterized by rounded enlightenment, which is surrounded by a
Ring-like shadow
It characterized by rounded enlightenment, which is surrounded by a
Increased enlightenment of the lung fields
It includes varying prevalence of enlightenment,
Increased enlightenment of the lung fields
It includes varying prevalence of enlightenment,
Mediastinal pathology syndrome
It manifested by changing the mediastinum form or position.
Mediastinal pathology syndrome
It manifested by changing the mediastinum form or position.
Free fluid in the pleural cavity
It characterized by a one- or
Free fluid in the pleural cavity
It characterized by a one- or
Free fluid in the pleural cavity
The most frequent cause of exudative
Free fluid in the pleural cavity
The most frequent cause of exudative
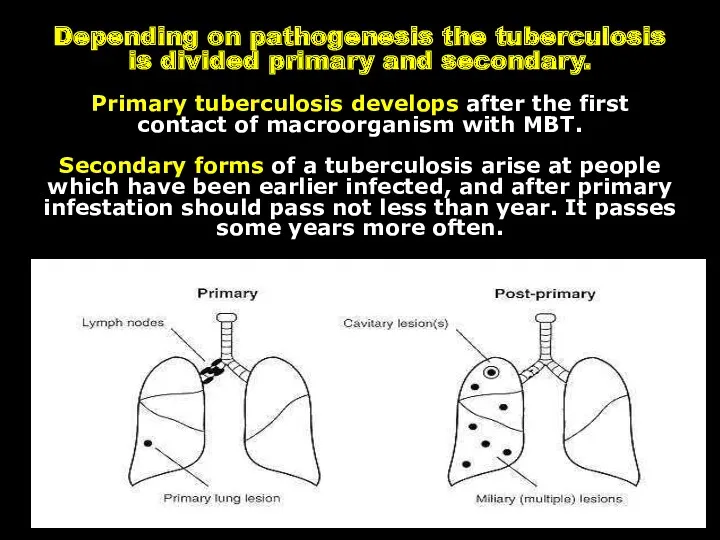
Depending on pathogenesis the tuberculosis is divided primary and secondary.
Primary
Depending on pathogenesis the tuberculosis is divided primary and secondary. Primary
PRIMARY TUBERCULOSIS
Primary is considered tuberculosis that
develops in firstly
PRIMARY TUBERCULOSIS
Primary is considered tuberculosis that
develops in firstly
Para-specific reactions
(tuberculosis “masks”)
In primary tuberculosis there are situations where the
Para-specific reactions
(tuberculosis “masks”)
In primary tuberculosis there are situations where the
“Flu-like” TB mask
The most frequently tuberculosis in active phase occurs in
“Flu-like” TB mask
The most frequently tuberculosis in active phase occurs in
“pneumonic” mask
The second frequency is “pneumonic” mask. This is repeated recurrent
“pneumonic” mask
The second frequency is “pneumonic” mask. This is repeated recurrent
Poncet`s disease
Tuberculosis can begin on type “rheumatic” mask, called “Poncet`s disease”.
Poncet`s disease
Tuberculosis can begin on type “rheumatic” mask, called “Poncet`s disease”.
“Neurological” TB mask
“Neurological” TB mask manifests as long, persistent neuralgia,
“Neurological” TB mask
“Neurological” TB mask manifests as long, persistent neuralgia,

“Lupus-like” TB mask
“Lupus-like” mask manifests typical erythema on the face in
“Lupus-like” TB mask
“Lupus-like” mask manifests typical erythema on the face in
“Hematological” mask
“Hematological” mask of tuberculosis occurs with bone marrow hypoplasia, leukopenia,
“Hematological” mask
“Hematological” mask of tuberculosis occurs with bone marrow hypoplasia, leukopenia,
Keratoconjunctivitis phlyctenular
Keratoconjunctivitis phlyctenular. Most often its tubercular-allergic process in children with
Keratoconjunctivitis phlyctenular
Keratoconjunctivitis phlyctenular. Most often its tubercular-allergic process in children with
CHARACTERISTIC SIGNS OF PRIMARY TUBERCULOSIS:
the intensity of tuberculin reactions
organism
CHARACTERISTIC SIGNS OF PRIMARY TUBERCULOSIS:
the intensity of tuberculin reactions
organism
PRIMARY TUBERCULOUS COMPLEX
1. PATHOGENESIS
After the penetration of MBT into
PRIMARY TUBERCULOUS COMPLEX
1. PATHOGENESIS
After the penetration of MBT into
PRIMARY TUBERCULOUS COMPLEX
The dynamic study of primary pulmonary processes among children
PRIMARY TUBERCULOUS COMPLEX
The dynamic study of primary pulmonary processes among children
PRIMARY TUBERCULOUS COMPLEX
1) PNEUMONIC;
In the first phase (pneumatic) the focus
PRIMARY TUBERCULOUS COMPLEX
1) PNEUMONIC; In the first phase (pneumatic) the focus
PRIMARY TUBERCULOUS COMPLEX
2) PHASE OF DISSOLVING;
In the second phase of dissolving
PRIMARY TUBERCULOUS COMPLEX
2) PHASE OF DISSOLVING; In the second phase of dissolving
PRIMARY TUBERCULOUS COMPLEX
3) PHASE OF CONDENSATION;
In the third phase, the phase
PRIMARY TUBERCULOUS COMPLEX
3) PHASE OF CONDENSATION; In the third phase, the phase
PRIMARY TUBERCULOUS COMPLEX
4) FORMATION OF GOHN’S FOCUS.
In the fourth phase, in
PRIMARY TUBERCULOUS COMPLEX
4) FORMATION OF GOHN’S FOCUS.
In the fourth phase, in
TUBERCULOSIS OF INTRATHORACIC LYMPHATIC NODES
Bronchoadenitis is a disease of the
TUBERCULOSIS OF INTRATHORACIC LYMPHATIC NODES
Bronchoadenitis is a disease of the
Clinical pattern of tuberculous
bronchoadenitis
acute intoxication
specific clinical symptoms: subfebrile temperature,
Clinical pattern of tuberculous
bronchoadenitis
acute intoxication
specific clinical symptoms: subfebrile temperature,

Clinico-roentgenologically variants of intrathoracic lymphatic nodes TB
tumour like (tumoursimilar) form
infiltrative
Clinico-roentgenologically variants of intrathoracic lymphatic nodes TB
tumour like (tumoursimilar) form
infiltrative

Miliary tuberculosis
Generalized TB clinical form with the hematogenic type of dissemination
Miliary tuberculosis
Generalized TB clinical form with the hematogenic type of dissemination
Sub-acute disseminated tuberculosis
Bilateral lung injury with predominant affecting upper lobes and
Sub-acute disseminated tuberculosis
Bilateral lung injury with predominant affecting upper lobes and
Chronic disseminated tuberculosis
Disseminated lung injury with the wavy course and progressive
Chronic disseminated tuberculosis
Disseminated lung injury with the wavy course and progressive
Focal (nidus) TB
The mildest limited lung TB clinical form which is
Focal (nidus) TB
The mildest limited lung TB clinical form which is
Infiltrative TB
The expansive lung TB clinical form which is characterized by
Infiltrative TB
The expansive lung TB clinical form which is characterized by
Infiltrative TB
Infiltrative TB

Infiltrative TB
Infiltrative TB
Infiltrative TB
Infiltrative TB

Infiltrative TB
Infiltrative TB
Caseous pneumonia
An acute TB form with the decay predominance and severe
Caseous pneumonia
An acute TB form with the decay predominance and severe
Tuberculoma
The inflammative focus limited by connective tissue capsule
Tuberculoma
The inflammative focus limited by connective tissue capsule
Fibrous-cavernous tuberculosis
The chronic destructive clinical TB form characterized by the presence
Fibrous-cavernous tuberculosis
The chronic destructive clinical TB form characterized by the presence
Cirrhotic lung tuberculosis
The chronic destructive clinical TB form characterized by the
Cirrhotic lung tuberculosis
The chronic destructive clinical TB form characterized by the
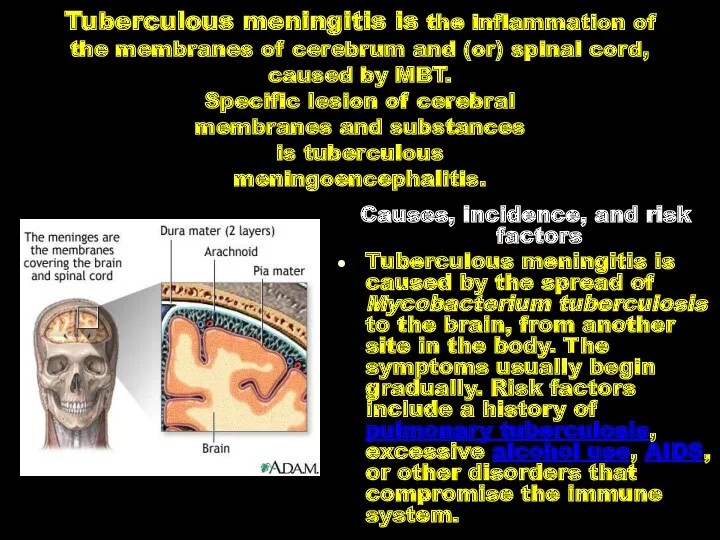
Tuberculous meningitis is the inflammation of the membranes of cerebrum and
Tuberculous meningitis is the inflammation of the membranes of cerebrum and
Pathogenesis. Tuberculous meningitis may be primary (in 20 %) and secondary
Pathogenesis. Tuberculous meningitis may be primary (in 20 %) and secondary
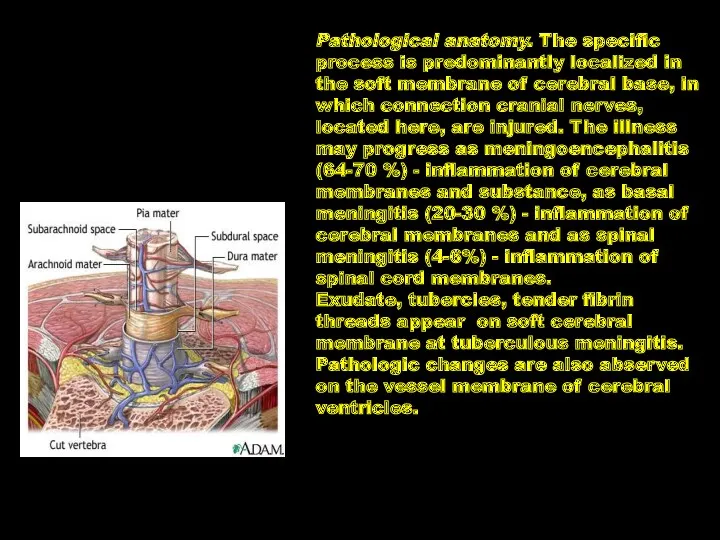
Pathological anatomy. The specific process is predominantly localized in the soft
Pathological anatomy. The specific process is predominantly localized in the soft
Clinic of Tuberculous meningitis
I. A prodromic period
the duration is from
Clinic of Tuberculous meningitis
I. A prodromic period
the duration is from
5 components (syndromes) are discriminated in the clinical picture of tuberculous
5 components (syndromes) are discriminated in the clinical picture of tuberculous
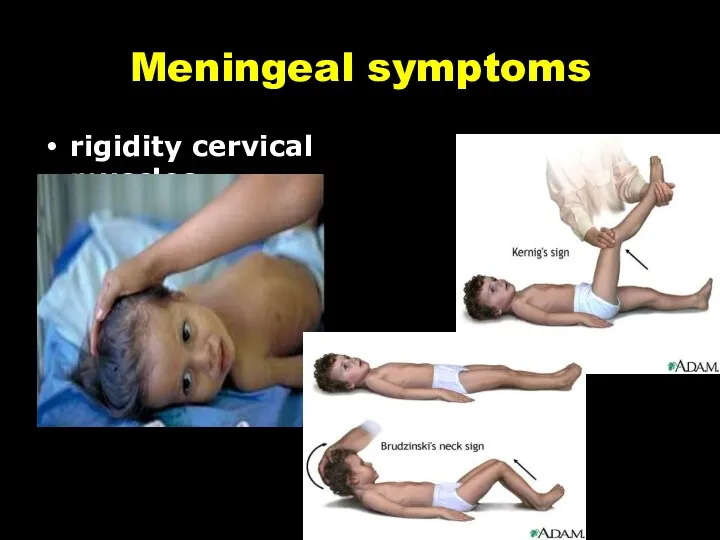
Meningeal symptoms
rigidity cervical muscles
Meningeal symptoms
rigidity cervical muscles
 Врачебно-профессиональное консультирование подростков
Врачебно-профессиональное консультирование подростков Профилактика нарушений зрения у школьников
Профилактика нарушений зрения у школьников Системная склеродермия
Системная склеродермия Қалқанша безі гормондарының. Препараттары және антитиреоидты дәрілер
Қалқанша безі гормондарының. Препараттары және антитиреоидты дәрілер Переломы костей таза
Переломы костей таза Basics of parasitic diseases in surgery
Basics of parasitic diseases in surgery Клинико-психологическое сопровождение в рамках третичной профилактики пожилых с болезнью Пика
Клинико-психологическое сопровождение в рамках третичной профилактики пожилых с болезнью Пика Лабораторная диагностика туберкулёзной инфекции
Лабораторная диагностика туберкулёзной инфекции Приготовление детских лекарственных форм в условиях аптеки
Приготовление детских лекарственных форм в условиях аптеки Механическая травма. Синдром длительного сдавления. Переломы
Механическая травма. Синдром длительного сдавления. Переломы Общение медсестры с детьми
Общение медсестры с детьми Личная гигиена и профилактика пролежней. Питание и кормление пациентов
Личная гигиена и профилактика пролежней. Питание и кормление пациентов Инфаркт миокарда
Инфаркт миокарда ДНК – ның теломерлік бөлімдерінің репликациялануы
ДНК – ның теломерлік бөлімдерінің репликациялануы Слизистые оболочки в норме и патологии
Слизистые оболочки в норме и патологии Менингококковая инфекция у детей
Менингококковая инфекция у детей Ас қорыту жолдарының ісіктері
Ас қорыту жолдарының ісіктері Этика и деонтология для работников регистратур медицинских организаций
Этика и деонтология для работников регистратур медицинских организаций Аномалии развития женской половой системы
Аномалии развития женской половой системы Кисты и свищи поджелудочной железы, классификация, диагностика, современные методы лечения
Кисты и свищи поджелудочной железы, классификация, диагностика, современные методы лечения Оказание первой медицинской помощи пострадавшим от действия электрического тока
Оказание первой медицинской помощи пострадавшим от действия электрического тока Әлеуметтік диагностика
Әлеуметтік диагностика Основы иммунитета
Основы иммунитета Подготовка к лабораторным исследованиям (2)
Подготовка к лабораторным исследованиям (2) Оказание медицинской помощи при остром коронарном синдроме (ОКС)
Оказание медицинской помощи при остром коронарном синдроме (ОКС) Аллергические состояния, проявления в полости рта. Клиника, диагностика, лечение
Аллергические состояния, проявления в полости рта. Клиника, диагностика, лечение № 2 Симптомдық артериальды гипертензия. № 3 вариант: Иценко-Кушинг синдромы кезіндегі
№ 2 Симптомдық артериальды гипертензия. № 3 вариант: Иценко-Кушинг синдромы кезіндегі Синдром уплотнения легочной ткани. Пневмония
Синдром уплотнения легочной ткани. Пневмония