Применение трициклических антидепрессантов (Амитриптиллин) и психотерапии у пациентов с постинсультной депрессии презентация
- Применение трициклических антидепрессантов (Амитриптиллин) и психотерапии у пациентов с постинсультной депрессии

Содержание
- 2. АКТУАЛЬНОСТЬ Депрессия - развивается примерно у каждого 3-го больного, перенесшего инсульт, и может негативно влиять на
- 3. Депрессия ухудшает качество жизни как самих пациентов, так и членов их семьи и ухаживающих за ними
- 4. ЦЕЛЬ ИССЛЕДОВАНИЯ Сравнить эффективность трициклических антидепрессантов (Амитриптиллина) и психотерапии при постинсультной депрессии
- 5. ГИПОТЕЗА Нулевая - лечение постинсультной депрессии с Амитриптиллином и психотерапии не отмечает эффекта. Альтернативная- лечение постинсультной
- 6. ЗАДАЧИ Произвести литературный обзор . Определение групп пациентов генеральной совокупности для формирования выборки. Путем рандомизации распределить
- 7. ДИЗАЙН ИССЛЕДОВАНИЯ Открытое рандомизированное контралируемое исследование
- 8. ВЫБОРКА Исследование проводилось в городской поликлинике №3 в г. Актобе. В исследование были взяты те пациенты
- 9. КРИТЕРИИ ВКЛЮЧЕНИЯ Пациенты после инсульта в возрасте 30-70 лет, независимо от пола которые по шкале Гамильтона
- 10. КРИТЕРИИ ИСКЛЮЧЕНИЯ Пациенты после инсульта у которых по шкале Гамильтона набирают 19-22 баллов. Пациенты которые по
- 11. ИССЛЕДОВАТЕЛЬСКИЙ ВОПРОС Приведет ли к снижению тяжести депрессии у постинсультных больных с депрессии средней степени тяжести?
- 12. ЭТИЧЕСКИЕ АСПЕКТЫ Одобрено КЭ Информированное согласие с полным раскрытием всей необходимой информацией на понятном языке (на
- 13. ИССЛЕДОВАТЕЛЬСКИЙ ВОПРОС ПО СТАТЬЕ Оценить эффективность антидепрессантов у больных с постинсультной депрессии (по шкале Монсгомери) Р
- 14. ДИЗАЙН ИССЛЕДОВАНИЯ ПО СТАТЬЕ Окрытое рандомизированное контролируемое многоцентровое исследование.
- 15. ВЫБОРКА ПО СТАТЬЕ Систематическая
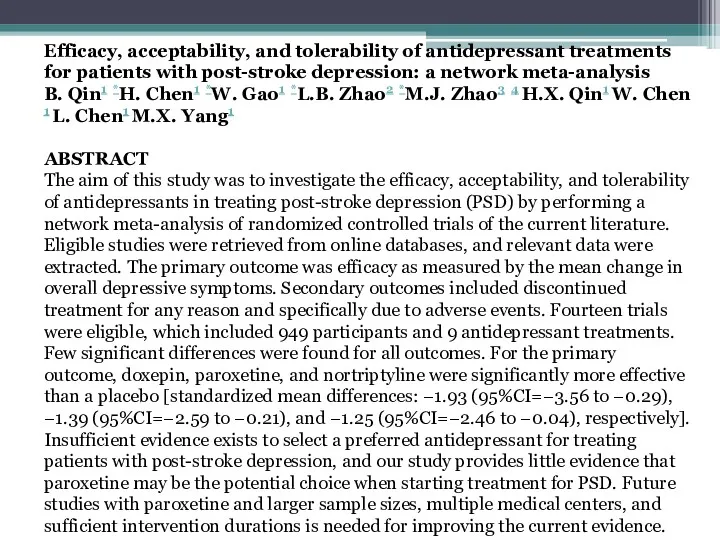
- 16. Efficacy, acceptability, and tolerability of antidepressant treatments for patients with post-stroke depression: a network meta-analysis B.
- 17. MATERIAL AND METHODS Data sources and search strategy We conducted a systematic search of the PubMed,
- 18. Outcome measures The primary outcome was the mean change in overall depressive symptoms, which was assessed
- 19. DISCUSSION This study performed a comprehensive comparison of the efficacy, tolerability, and acceptability of antidepressants using
- 20. The most important clinical implication of the results presented here is that paroxetine might be the
- 24. Скачать презентацию
АКТУАЛЬНОСТЬ
Депрессия - развивается примерно у каждого 3-го больного, перенесшего инсульт,
АКТУАЛЬНОСТЬ
Депрессия - развивается примерно у каждого 3-го больного, перенесшего инсульт,
Депрессия ухудшает качество жизни как самих пациентов, так и членов их
Депрессия ухудшает качество жизни как самих пациентов, так и членов их
ЦЕЛЬ ИССЛЕДОВАНИЯ
Сравнить эффективность трициклических антидепрессантов (Амитриптиллина) и психотерапии при постинсультной
ЦЕЛЬ ИССЛЕДОВАНИЯ
Сравнить эффективность трициклических антидепрессантов (Амитриптиллина) и психотерапии при постинсультной
ГИПОТЕЗА
Нулевая - лечение постинсультной депрессии с Амитриптиллином и психотерапии не
ГИПОТЕЗА
Нулевая - лечение постинсультной депрессии с Амитриптиллином и психотерапии не
ЗАДАЧИ
Произвести литературный обзор .
Определение групп пациентов генеральной совокупности для формирования
ЗАДАЧИ
Произвести литературный обзор .
Определение групп пациентов генеральной совокупности для формирования
ДИЗАЙН ИССЛЕДОВАНИЯ
Открытое рандомизированное контралируемое исследование
ДИЗАЙН ИССЛЕДОВАНИЯ
Открытое рандомизированное контралируемое исследование
ВЫБОРКА
Исследование проводилось в городской поликлинике №3 в г. Актобе. В
ВЫБОРКА
Исследование проводилось в городской поликлинике №3 в г. Актобе. В
КРИТЕРИИ ВКЛЮЧЕНИЯ
Пациенты после инсульта в возрасте 30-70 лет, независимо от
КРИТЕРИИ ВКЛЮЧЕНИЯ
Пациенты после инсульта в возрасте 30-70 лет, независимо от
КРИТЕРИИ ИСКЛЮЧЕНИЯ
Пациенты после инсульта у которых по шкале Гамильтона набирают
КРИТЕРИИ ИСКЛЮЧЕНИЯ
Пациенты после инсульта у которых по шкале Гамильтона набирают
ИССЛЕДОВАТЕЛЬСКИЙ ВОПРОС
Приведет ли к снижению тяжести депрессии у постинсультных больных
ИССЛЕДОВАТЕЛЬСКИЙ ВОПРОС
Приведет ли к снижению тяжести депрессии у постинсультных больных
ЭТИЧЕСКИЕ АСПЕКТЫ
Одобрено КЭ
Информированное согласие с полным раскрытием всей необходимой информацией
ЭТИЧЕСКИЕ АСПЕКТЫ
Одобрено КЭ
Информированное согласие с полным раскрытием всей необходимой информацией
ИССЛЕДОВАТЕЛЬСКИЙ ВОПРОС ПО СТАТЬЕ
Оценить эффективность антидепрессантов у больных с постинсультной
ИССЛЕДОВАТЕЛЬСКИЙ ВОПРОС ПО СТАТЬЕ
Оценить эффективность антидепрессантов у больных с постинсультной
ДИЗАЙН ИССЛЕДОВАНИЯ ПО СТАТЬЕ
Окрытое рандомизированное контролируемое многоцентровое исследование.
ДИЗАЙН ИССЛЕДОВАНИЯ ПО СТАТЬЕ
Окрытое рандомизированное контролируемое многоцентровое исследование.
ВЫБОРКА ПО СТАТЬЕ
Систематическая
ВЫБОРКА ПО СТАТЬЕ
Систематическая
Efficacy, acceptability, and tolerability of antidepressant treatments for patients with post-stroke
MATERIAL AND METHODS
Data sources and search strategy
We conducted a systematic search
MATERIAL AND METHODS
Data sources and search strategy
We conducted a systematic search
Outcome measures
The primary outcome was the mean change in overall depressive
Outcome measures
The primary outcome was the mean change in overall depressive
DISCUSSION
This study performed a comprehensive comparison of the efficacy, tolerability, and
DISCUSSION
This study performed a comprehensive comparison of the efficacy, tolerability, and
The most important clinical implication of the results presented here is
The most important clinical implication of the results presented here is
 Радиобиология пәні, мақсаты, міндеттері. Иондаушы сәулелердің түрлері және олардың қасиеттері
Радиобиология пәні, мақсаты, міндеттері. Иондаушы сәулелердің түрлері және олардың қасиеттері Эпизоотическая ситуация по бешенству на территории г. Вологда
Эпизоотическая ситуация по бешенству на территории г. Вологда Ишемическая болезнь сердца
Ишемическая болезнь сердца Кариес. Этиология, патогенез, клиника, лечение
Кариес. Этиология, патогенез, клиника, лечение Регенерация. Физиологиялық, репаративтік, патологиялық
Регенерация. Физиологиялық, репаративтік, патологиялық Нарушения психического развития у детей
Нарушения психического развития у детей Пероральные лекарственные формы с модифицированным высвобождением
Пероральные лекарственные формы с модифицированным высвобождением Жансыздандыру кезіндегі жергілікті асқынулар
Жансыздандыру кезіндегі жергілікті асқынулар Введение в фармокологию
Введение в фармокологию Сердечно-легочная реанимация
Сердечно-легочная реанимация Геморрагиялық шок
Геморрагиялық шок Заболеваемость населения как медико-социальная проблема. Эпидемиологические методы изучения заболеваемости
Заболеваемость населения как медико-социальная проблема. Эпидемиологические методы изучения заболеваемости Ревматическая болезнь сердца
Ревматическая болезнь сердца Лечение неотложных состояний при сахарном диабете
Лечение неотложных состояний при сахарном диабете Неотложные состояния у детей
Неотложные состояния у детей Брюшной тиф
Брюшной тиф Збудник туберкульозу. Патогенні мікобактерії
Збудник туберкульозу. Патогенні мікобактерії Рентгенодиагностика пневмоний
Рентгенодиагностика пневмоний Инструментальные методы исследования гинекологических заболеваний
Инструментальные методы исследования гинекологических заболеваний Профессиональные заболевания людей. Диагностика и лечение
Профессиональные заболевания людей. Диагностика и лечение ВИЧ. Этиология, клиника, диагностика, лечение
ВИЧ. Этиология, клиника, диагностика, лечение Қосымша репродуктивтік технология
Қосымша репродуктивтік технология Особенности межличностного общения с коллегами. Врачи Скорой помощи
Особенности межличностного общения с коллегами. Врачи Скорой помощи Железодефицитная анемия у детей
Железодефицитная анемия у детей Врожденная кишечная непроходимость
Врожденная кишечная непроходимость Солнечные и воздушные ванны
Солнечные и воздушные ванны Баға экономикалық категориясы: мағынасы, жүйелері, жіктелуі. Дәрілік заттардың бағасының түрлері
Баға экономикалық категориясы: мағынасы, жүйелері, жіктелуі. Дәрілік заттардың бағасының түрлері Жедел жәрдем станциясында диспетчерлік жұмыс ұйымдастыру
Жедел жәрдем станциясында диспетчерлік жұмыс ұйымдастыру