- Protein-energy malnutrition in children

Содержание
- 2. Plan of the lecture 1. The frequency of protein-energy malnutrition in children 2. Etiology 3. PATHOGENESIS
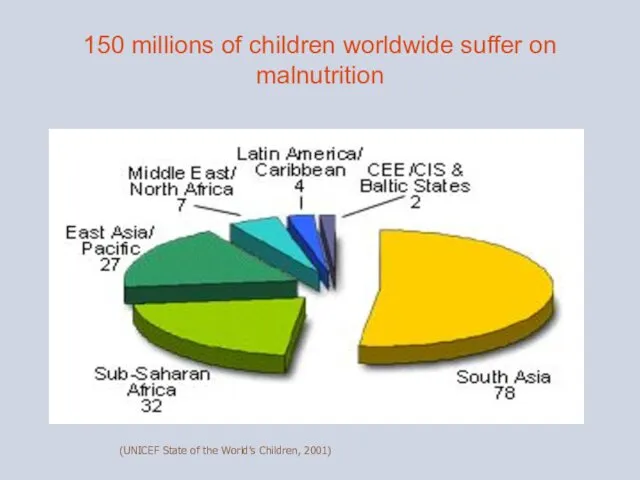
- 3. 150 millions of children worldwide suffer on malnutrition (UNICEF State of the World’s Children, 2001)
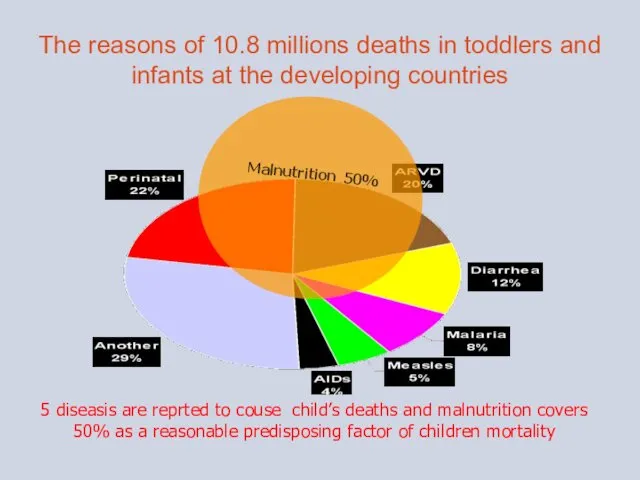
- 4. The reasons of 10.8 millions deaths in toddlers and infants at the developing countries 5 diseasis
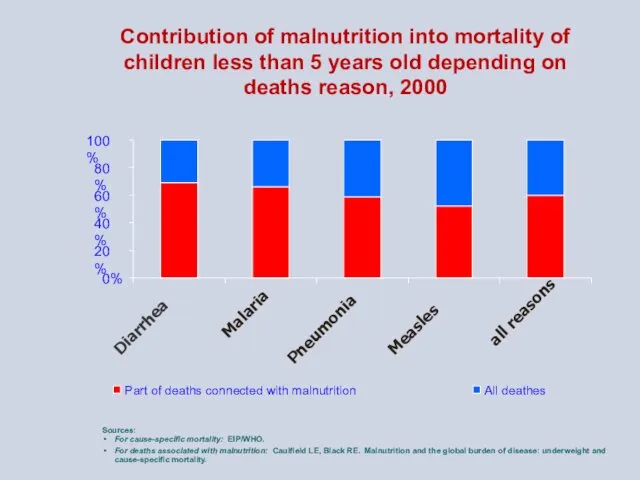
- 5. Contribution of malnutrition into mortality of children less than 5 years old depending on deaths reason,
- 6. ETIOLOGY Prenatal factors - Insufficient alimentation and diseases of mother (in early pregnancy term – gestosis;
- 7. b) infectious factors: intrauterine generalized infections like cytomegaloviruses, rubella, syphylis, toxoplasmosis etc., Intranatal infections, toxic-septic conditions,
- 8. 3. Endogene reasons: а) perinatal encephalopathies, bronchial and lung dysplasia; b) congenital and inborn malformations of
- 9. PATHOGENESIS Decreased secretory function of digestive glands - abnormality of food evacuation Decreased secretory function of
- 10. Protein-energy malnutrition (prenatal, postnatal malnutrition) –Insufficient child feeding characterised by failure to thrive or retardation of
- 11. Clean, pinkish smooth skin without signs of hypovitaminosis; Normal subcutaneous fat layer, good tissue turgor, proper
- 12. Prenatal, postnatal malnutrition types ( according to Worldwide disease register) Type Е 43 – Severe protein-energy
- 13. Classification of hypotrophy (protein-energy malnutrition - PEM): I degree PEM – weight deficiency 11 – 20
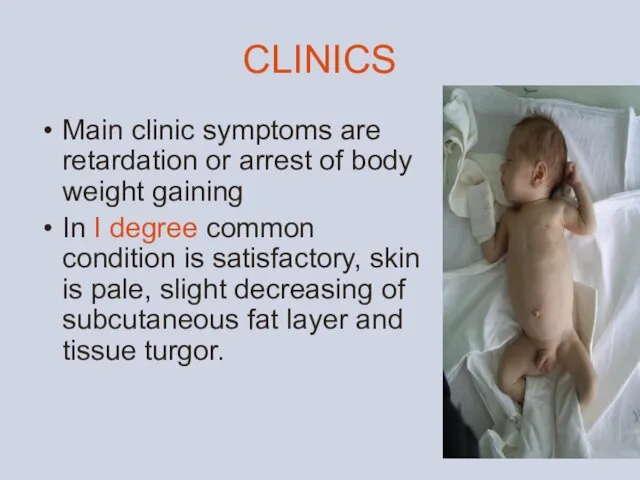
- 15. CLINICS Main clinic symptoms are retardation or arrest of body weight gaining In I degree common
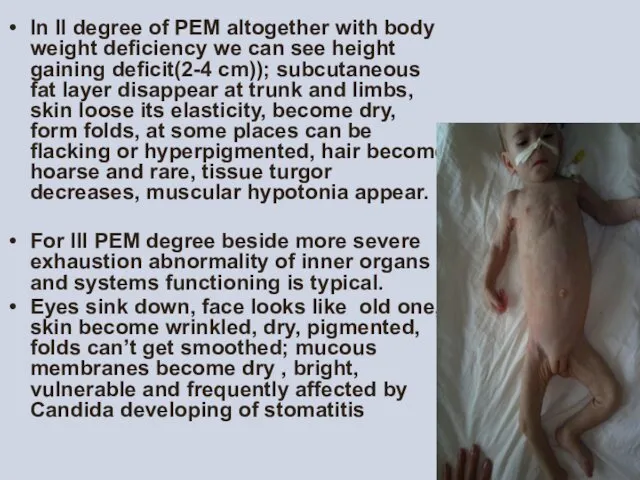
- 16. In II degree of PEM altogether with body weight deficiency we can see height gaining deficit(2-4
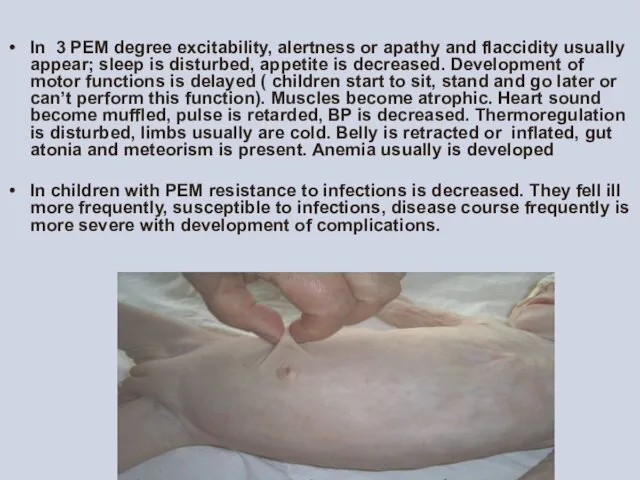
- 17. In 3 PEM degree excitability, alertness or apathy and flaccidity usually appear; sleep is disturbed, appetite
- 18. Kwashiorkor — is a type of PEM in infants and toddlers due to feeding predominantly by
- 19. · Laboratory tests а) obligatory: - common blood test - common urine test - stool test
- 20. Treatment must be complex: Eliminate etiologic factor, normalize diet, rational regimen, good care, treatment of all
- 21. Main diet approaches in PEM is triphase feeding : Period of food tolerance clarifying; Transient period;
- 22. In II and III PEM grade when metabolic disturbances are more expressed and therefore assimilation of
- 23. Diet of children with PEM must be of full value Infants must be supplied by breast
- 24. Efficacy criteria of dietetic treatment are: emotional status improvement, appetite normalizing, skin condition improvement, turgor normalizing,
- 25. Treatment In II and III PEM grade treatment is performed in hospital: - parenteral nutrition (
- 26. Hypovitaminosis Ascorbic acid (vit C) insuficiancy. Clinics. As another types of hypovitaminosis can start gradually. The
- 27. Thiamin defficiancy (vitamin BI). CLINICS. Disease is manifested by changes in muscles and nervous tissue. Fatigability,
- 28. Riboflavin deficiancy (vitamin В2). CLINICS Decreasing of weight, retardation in growth, weakness, prompt fatigability, decreased immune
- 29. Nicotinic acid deficiency (vitamin РР,niacyn, vitamin Вз). Clinics presents abnormalities of gut. Inflammatory changes of mucous
- 30. Pyridoxine deficiency (vitamin B6). Clinics Vitamin B6 influences for nervous system activity and hematopoiesis. In deficiency
- 31. Biotin deficiency (vitamin N). Clinics. In the case of vit N deficiency or insufficient synthesis of
- 32. Rutin deficiency (vitamin P). Clinics Vit P deficiency can cause fragility of vessels predominantly capillaries with
- 33. Folic acid deficiency (vitamin Bc). Clinics appears predominantly after antibiotic and sulfonamides treatment, due to malabsorption
- 34. Tocopherol deficiency (vitamin Е). CLINICS There can be observed fragility of capillaries, muscular dystrophy, liver affection.
- 36. Скачать презентацию
Plan of the lecture
1. The frequency of protein-energy malnutrition in
Plan of the lecture
1. The frequency of protein-energy malnutrition in
150 millions of children worldwide suffer on malnutrition
(UNICEF State of the
150 millions of children worldwide suffer on malnutrition
(UNICEF State of the
The reasons of 10.8 millions deaths in toddlers and infants at
The reasons of 10.8 millions deaths in toddlers and infants at
Contribution of malnutrition into mortality of children less than 5 years
Contribution of malnutrition into mortality of children less than 5 years
ETIOLOGY
Prenatal factors
- Insufficient alimentation and diseases of mother (in early pregnancy
ETIOLOGY
Prenatal factors
- Insufficient alimentation and diseases of mother (in early pregnancy
b) infectious factors:
intrauterine generalized infections like cytomegaloviruses, rubella, syphylis, toxoplasmosis
b) infectious factors:
intrauterine generalized infections like cytomegaloviruses, rubella, syphylis, toxoplasmosis
3. Endogene reasons:
а) perinatal encephalopathies, bronchial and lung dysplasia;
b) congenital and inborn
3. Endogene reasons: а) perinatal encephalopathies, bronchial and lung dysplasia; b) congenital and inborn
PATHOGENESIS
Decreased secretory function of digestive glands - abnormality of food evacuation
Decreased
PATHOGENESIS
Decreased secretory function of digestive glands - abnormality of food evacuation
Decreased
Protein-energy malnutrition (prenatal, postnatal malnutrition) –Insufficient child feeding characterised by
failure
Protein-energy malnutrition (prenatal, postnatal malnutrition) –Insufficient child feeding characterised by
failure
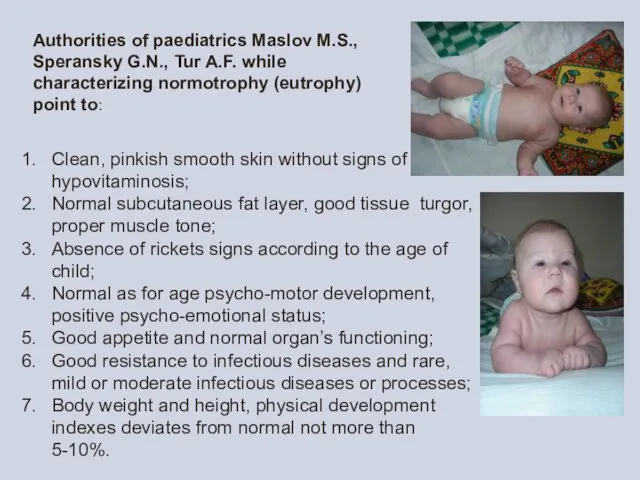
Clean, pinkish smooth skin without signs of hypovitaminosis;
Normal subcutaneous fat layer,
Normal subcutaneous fat layer,
Prenatal, postnatal malnutrition types ( according to Worldwide disease register)
Type
Prenatal, postnatal malnutrition types ( according to Worldwide disease register)
Type
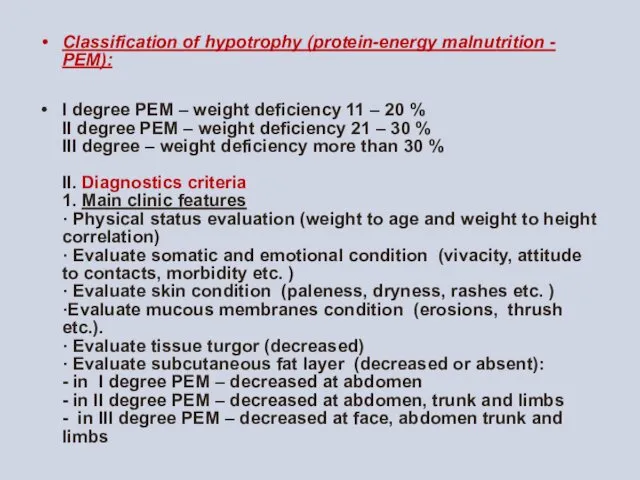
Classification of hypotrophy (protein-energy malnutrition - PEM):
I degree PEM –
Classification of hypotrophy (protein-energy malnutrition - PEM):
I degree PEM –

CLINICS
Main clinic symptoms are retardation or arrest of body weight gaining
In
CLINICS
Main clinic symptoms are retardation or arrest of body weight gaining
In
In II degree of PEM altogether with body weight deficiency we
In II degree of PEM altogether with body weight deficiency we
In 3 PEM degree excitability, alertness or apathy and flaccidity usually
Kwashiorkor — is a type of PEM in infants and toddlers
Kwashiorkor — is a type of PEM in infants and toddlers
·
Laboratory tests
а) obligatory:
- common blood test
- common
·
Laboratory tests а) obligatory: - common blood test - common
Treatment must be complex:
Eliminate etiologic factor, normalize diet, rational regimen, good
Treatment must be complex:
Eliminate etiologic factor, normalize diet, rational regimen, good
Main diet approaches in PEM is triphase feeding :
Period of food
Main diet approaches in PEM is triphase feeding :
Period of food
In II and III PEM grade when metabolic disturbances are more
In II and III PEM grade when metabolic disturbances are more
Diet of children with PEM must be of full value
Infants must
Diet of children with PEM must be of full value
Infants must
Efficacy criteria of dietetic treatment are:
emotional status improvement,
Efficacy criteria of dietetic treatment are:
emotional status improvement,
Treatment
In II and III PEM grade treatment is performed in hospital:
Treatment
In II and III PEM grade treatment is performed in hospital:
Hypovitaminosis
Ascorbic acid (vit C) insuficiancy.
Clinics. As another types of hypovitaminosis
Hypovitaminosis
Ascorbic acid (vit C) insuficiancy.
Clinics. As another types of hypovitaminosis
Thiamin defficiancy (vitamin BI).
CLINICS. Disease is manifested by changes in
Thiamin defficiancy (vitamin BI).
CLINICS. Disease is manifested by changes in
Riboflavin deficiancy (vitamin В2).
CLINICS Decreasing of weight, retardation in growth,
Riboflavin deficiancy (vitamin В2).
CLINICS Decreasing of weight, retardation in growth,
Nicotinic acid deficiency (vitamin РР,niacyn, vitamin Вз).
Clinics presents abnormalities of
Nicotinic acid deficiency (vitamin РР,niacyn, vitamin Вз).
Clinics presents abnormalities of
Pyridoxine deficiency (vitamin B6).
Clinics Vitamin B6 influences for nervous system
Pyridoxine deficiency (vitamin B6).
Clinics Vitamin B6 influences for nervous system
Biotin deficiency (vitamin N).
Clinics. In the case of vit N
Biotin deficiency (vitamin N).
Clinics. In the case of vit N
Rutin deficiency (vitamin P).
Clinics Vit P deficiency can cause fragility
Rutin deficiency (vitamin P).
Clinics Vit P deficiency can cause fragility
Folic acid deficiency (vitamin Bc).
Clinics appears predominantly after antibiotic and
Folic acid deficiency (vitamin Bc).
Clinics appears predominantly after antibiotic and
Tocopherol deficiency (vitamin Е).
CLINICS There can be observed fragility of
Tocopherol deficiency (vitamin Е).
CLINICS There can be observed fragility of
 Фармацевтическая опека пациентов при боли в горле и гортани
Фармацевтическая опека пациентов при боли в горле и гортани Қызыл жалпақ теміреткі. Жүйелі қызыл жегі. Күлдіреуікше. Ауыз қуысындағы көріністері
Қызыл жалпақ теміреткі. Жүйелі қызыл жегі. Күлдіреуікше. Ауыз қуысындағы көріністері Реабилитация больных, перенесших инсульт
Реабилитация больных, перенесших инсульт Бронхоэктатикалық ауру, диагностикасы және емдеу әдістері
Бронхоэктатикалық ауру, диагностикасы және емдеу әдістері Кровотечение из дистальных отделов желудочно-кишечного тракта у детей. Занятие № 4
Кровотечение из дистальных отделов желудочно-кишечного тракта у детей. Занятие № 4 Неопухолевые заболевания ободочной кишки. Часть № 2
Неопухолевые заболевания ободочной кишки. Часть № 2 Наркотические анальгетики
Наркотические анальгетики Диалектика. Диалектиканың негізгі заңдары
Диалектика. Диалектиканың негізгі заңдары Метаболический синдром
Метаболический синдром Жүкті әйелдің тамақтануы
Жүкті әйелдің тамақтануы Программа дифференциальной диагностики при суставном синдроме. Критерии диагностики ревматических заболеваний
Программа дифференциальной диагностики при суставном синдроме. Критерии диагностики ревматических заболеваний Пульпит. Клиническая классификация пульпита:
Пульпит. Клиническая классификация пульпита: Фракционная терапия лица
Фракционная терапия лица Методы обеспечения проходимости дыхательных путей. Коникотомия. Интубация трахеи
Методы обеспечения проходимости дыхательных путей. Коникотомия. Интубация трахеи Диагностикалық лапароскопия әдістері
Диагностикалық лапароскопия әдістері Закаливающие процедуры для детей дошкольного возраста
Закаливающие процедуры для детей дошкольного возраста Хирургическая инфекция
Хирургическая инфекция Острая ревматическая лихорадка
Острая ревматическая лихорадка Антибиотики. Синтетические противомикробные средства
Антибиотики. Синтетические противомикробные средства Жұқпалы аурулар
Жұқпалы аурулар Железы внешней, внутренней и смешанной секреции
Железы внешней, внутренней и смешанной секреции Фармакология кардиотонических препаратов
Фармакология кардиотонических препаратов Особенности вакцинации отдельных контингентов людей. Вакцины будущего
Особенности вакцинации отдельных контингентов людей. Вакцины будущего Плевриты
Плевриты Физиология родов
Физиология родов Дифференциальная диагностика заболеваний ВНЧС. Методы обследования при заболеваниях височно-нижнечелюстного сустава
Дифференциальная диагностика заболеваний ВНЧС. Методы обследования при заболеваниях височно-нижнечелюстного сустава Анатомо-физиологические особенности нервной системы у детей. Нервно-психическое развитие
Анатомо-физиологические особенности нервной системы у детей. Нервно-психическое развитие Ротова порожнина. Травлення в ротовій порожнині
Ротова порожнина. Травлення в ротовій порожнині