- Radiology and imaging of the mammаry gland

Содержание
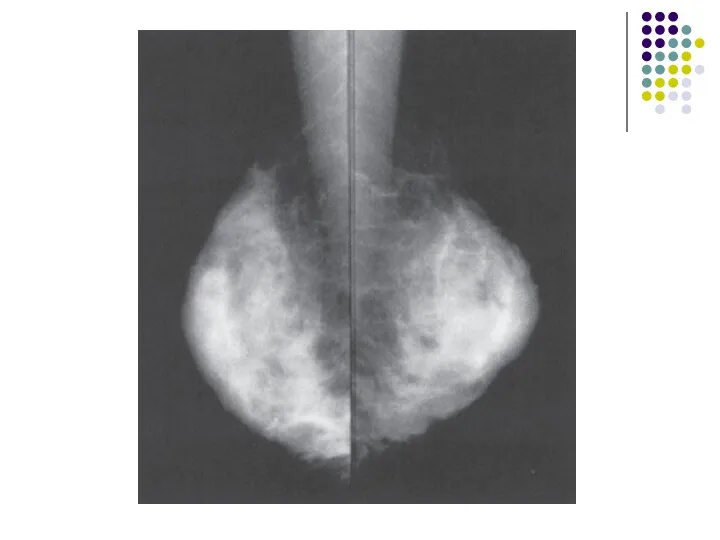
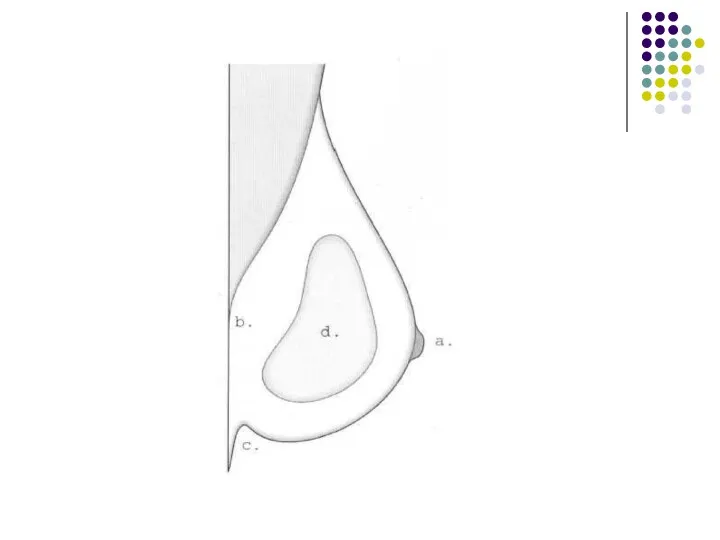
- 2. Normal anatomy Normal Structures Normal breast is composed: mainly of parenchyma (lobules and ducts) connective tissue
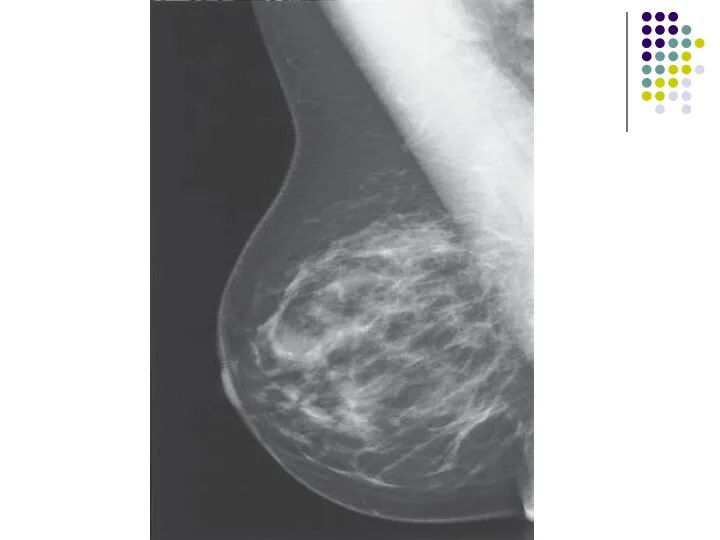
- 3. Parenchyma The lobules are glandular units and are seen as ill-defined, splotchy opacities of medium density.
- 4. . The breast lobes are intertwined and are therefore not discretely identifiable. This parenchymal tissue is
- 7. Connective tissue Trabecular structures, which are condensations of connective tissue, appear as thin (1 mm) linear
- 8. Fat The breast is composed of a large amount of fat, which is lucent, or almost
- 9. Lymph Nodes Lymph nodes are seen in the axillae and occasionally in the breast itself.
- 10. Veins Veins are seen traversing the breast as uniform, linear opacities, about 1 to 5 mm
- 11. Arteries Arteries appear as slightly thinner, uniform, linear densities and are best seen when calcified, as
- 12. Skin Skin lines are normally thin and are not easily seen without the aid of a
- 13. Normal variants The normal anatomical variants of the brest result from the embryological development of the
- 15. The dense breast Diffuse increase in the density of the breast tissue is caused by oedema
- 16. The increased density of the parenchyma seen as a result of HRT has been shown to
- 17. Mammography The film-screen mammogram is created with x-rays, radiographic film, and intensifying screens adjacent to the
- 18. The routine examination consists of two views of each breast: the craniocaudal (C-C) view the mediolateraloblique
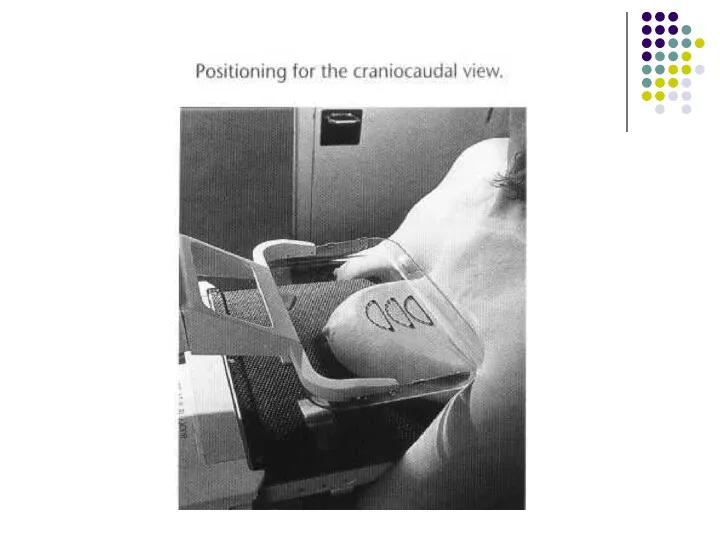
- 19. The C-C view can be considered the “top-down” view, and the MLO an angled view from
- 20. A flat, plastic compression paddle is then gently but firmly lowered onto the breast surface to
- 23. Compression may be uncomfortable, and may even be painful in a small proportion of patients. However,
- 24. Compression Firm compression is essential for high-quality mammograms and is applied using a powered system operated
- 25. The effects of compression are: (i) reduced dose; (ii) reduced scatter-improved contrast; (iii) reduced geometric unsharpness;
- 26. Mammography projections and normal appearances The standard examination for women undergoing either symptomatic mammography or their
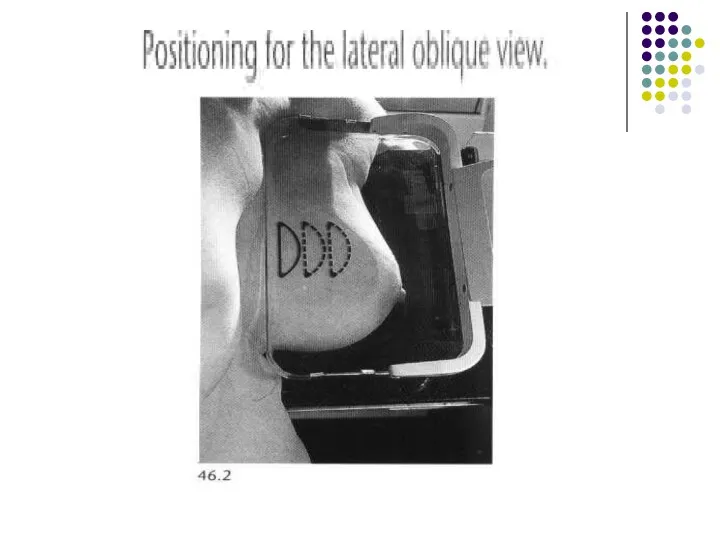
- 27. More breast tissue is demonstrated on the lateral oblique projection than on any other projection. Careful
- 28. The standard craniocaudal film is obtained with a vertical X-ray beam and the nipple should be
- 29. Supplementary views For demonstration of tissue in the most posterolateral part of the breast, an extended
- 30. Magnification views Magnification views are obtained by increasing the object-film distance, producing an `air gap', and
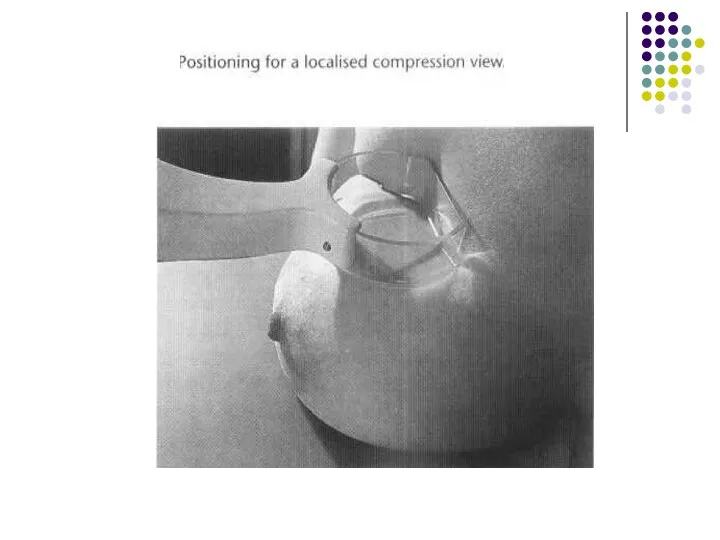
- 31. Localized compression views Localized compression views are obtained by using a small paddle compression device and
- 33. Screening Mammography The standard mammogram (along with appropriate history taking) makes up the entire screening mammogram.
- 34. Diagnostic Mammography The diagnostic mammogram begins with the two-view standard mammogram. Additional maneuvers are then used
- 35. Indications for diagnostic mammography are: (1) a palpable mass or other symptom or sign (e.g., skin
- 36. Indications of mammography • Screening asymptomatic women aged 50 years and over • Screening asymptomatic women
- 37. • Investigation of symptomatic women aged 35 years and over with a breast lump or other
- 38. Patient Preparation For the mammogram, two-piece clothing is most convenient as the patient will need to
- 39. Mammography is generally limited to ambulatory, cooperative patients because of the difficulties in proper positioning and
- 40. Computer-Aided Detection Computer-aided detection (CAD) utilizes complex algorithms to analyze the data from a mammogram for
- 41. _ Ultrasonography Technique High-quality images of the normal and abnormal breast can be obtained with modern
- 42. The side being examined is raised and the arm placed above the head to ensure that
- 43. The indications for ultrasonography are: (1) a mammographically detected mass, the nature of which is indeterminate
- 44. Ultrasonography is a highly reliable technique for differentiating cystic from solid masses. Although certain features have
- 45. A limitation A limitation of ultrasonography is that it is very operatordependent. Also, it images only
- 46. Normal breast ultrasound: 1 = skin; 2 = subcutaneous fat; 3 = glandular tissue; 4 =
- 47. Magnetic Resonance Imaging The role of MRI in mammography continues to expand, with common applications including:
- 48. (5) screening of high-risk patients (6) evaluating implants (7) evaluating difficult (dense or fibrous) breasts In
- 50. Axial T1 -weighted (A) and T2 -weighted (B) i mages in a patient with bilateral single
- 51. _ Ductography Ductography, or galactography, uses mammographic imaging with contrast injection into the breast ducts.
- 52. The indication The indication for use is a profuse, spontaneous, nonmilky nipple discharge from a single
- 53. The patient lies in supine position while the discharging duct is cannulated with a blunt-tipped needle
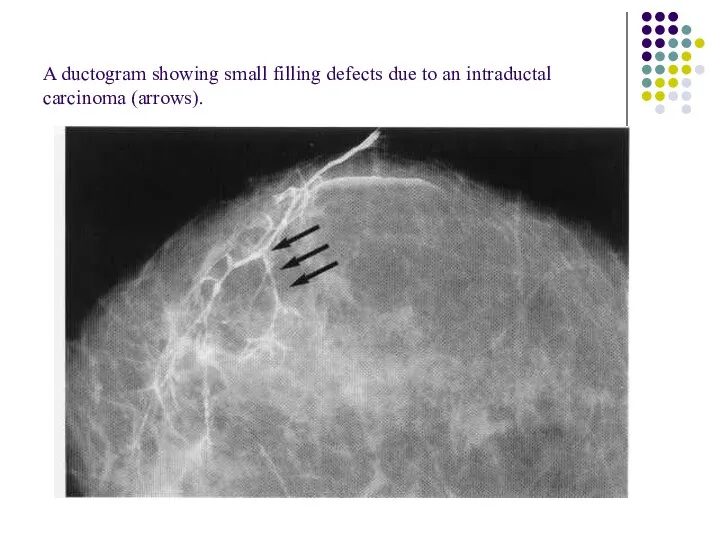
- 54. A ductogram showing small filling defects due to an intraductal carcinoma (arrows).
- 55. Image-Guided Needle Aspiration and Biopsy The first indication is aspiration of cystic lesions to confirm diagnosis,
- 56. Needle biopsy is used in this case (1) to confirm benignity of a lesion carrying a
- 57. 1 4G needle and automated biopsy device used for ultrasound and stereotactic core breast biopsy.
- 58. Stereotactic-guided fine needle aspiration. The check pair of films shows the tip of the needle positioned
- 59. Stereotactic core biopsy. Stereo film pair showing 'post fire' position of needle during biopsy of microcalcification
- 60. Image-Guided Needle Localization When a nonpalpable breast lesion must be excised, imaging is used to guide
- 61. Once the needle is in the appropriate position, a hook wire is inserted through the needle
- 62. Wire localisation and surgical excision of a nonpalpable carcinoma. (A) The position of a spiculate mass
- 63. Patient Preparation Patients for whom stereotactic biopsy is being considered should be able to lie in
- 64. Approach to the Palpable Lump When a breast lump is found, several questions must be answered
- 65. Second, is the lump new or enlarged? A new lump is more suspicious than a lump
- 66. Third, how big is the lump? Tiny pea-sized or smaller lumps, particularly in young women, are
- 67. Fourth, how old is the patient? If the patient is less than 35 years of age,
- 68. If the patient is below 35 years of age, a significant lump is usually first examined
- 69. For women between the ages of 30 and 40 years, judgment is needed as to whether
- 70. Bi - rads assessment categories category 0 - need additional imaging evaluation category 1 - negative
- 71. Circumscribed mass A circumscribed mass is analysed according to the following features: I. Density: (i) radiolucent
- 72. Radiolucent lesions Lipoma Oil cyst Galactocele.
- 73. Mixed density lesions adenolipoma hamartoma galactocele hematoma lymph node
- 74. Radiopaque (soft-tissue density) lesions Benign lesions * Cyst * Fibroadenoma * Papilloma *Phyllodes tumour * Abscess
- 75. Malignant lesions * Mucinous carcinoma * Medullary carcinoma * Papillary carcinoma * Invasive ductal carcinoma *
- 76. Calcifications Arterial: curvilinear, parallel line calcifications along the course of a blood vessel. Skin calcification: multiple
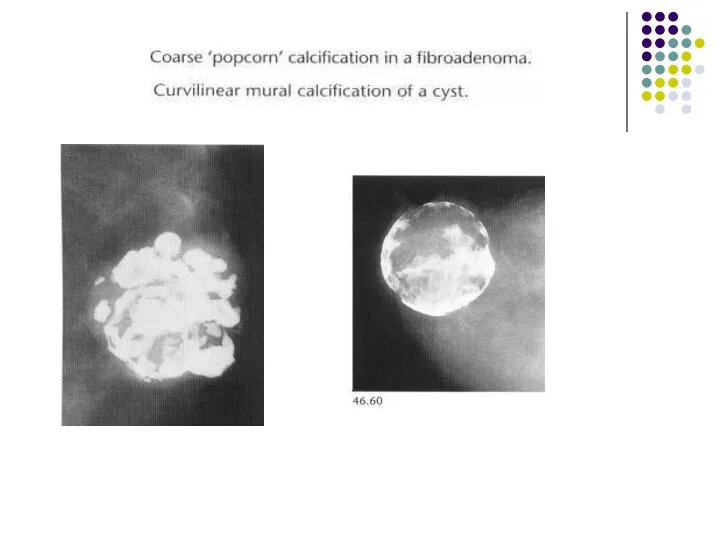
- 77. Cyst: curvilinear calcification may occur in the wall of a cyst. Carcinoma: the calcification particles of
- 78. Ductal carcinoma in situ. Irregular pleomorphic microcalcification
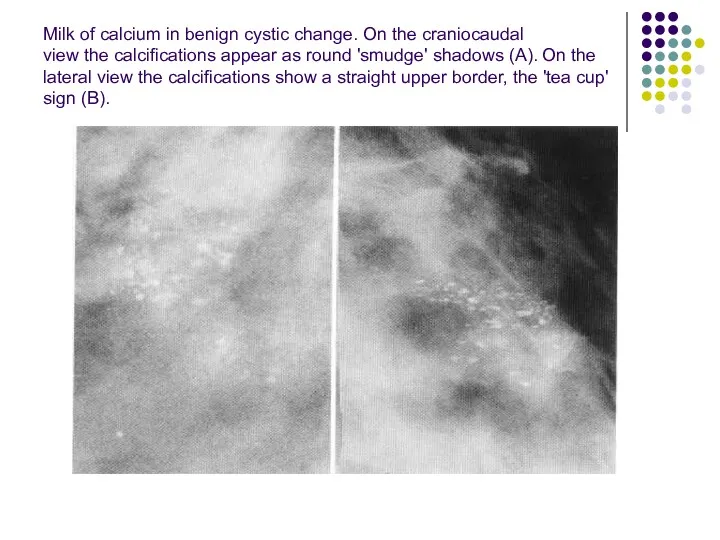
- 79. Milk of calcium in benign cystic change. On the craniocaudal view the calcifications appear as round
- 80. Skin calcification. Multiple small ring-shaped calcifications
- 81. Course calcification due to fat necrosis from previous surgery
- 82. Renal failure. Extensive stromal and vascular calcification.
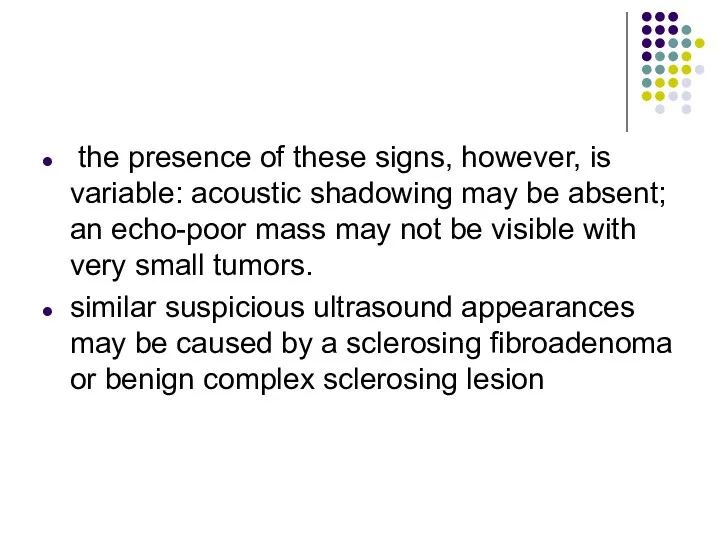
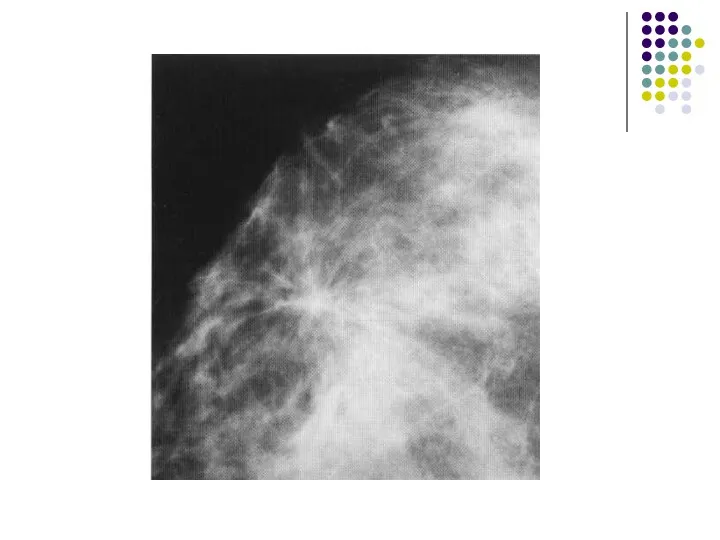
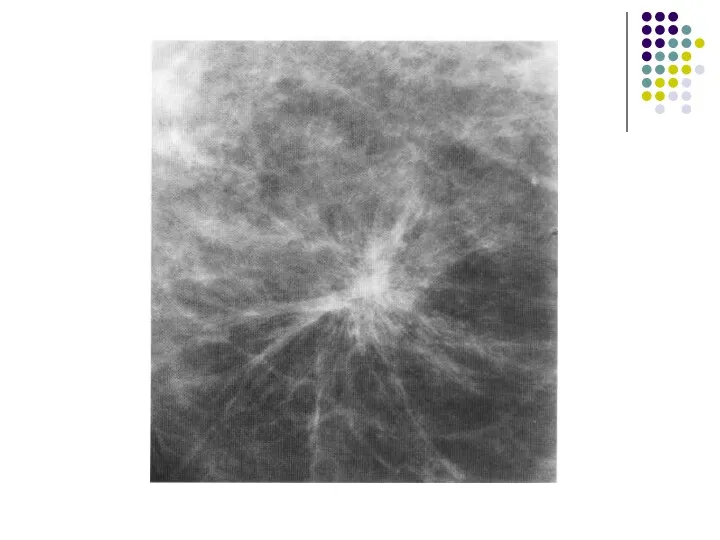
- 84. Spiculate mass A spiculate mass is the commonest mammographic appearance of invasive breast carcinoma. 1. It
- 85. 2. Large or superficially positioned tumors may be associated with localized skin thickening and retraction. 3.
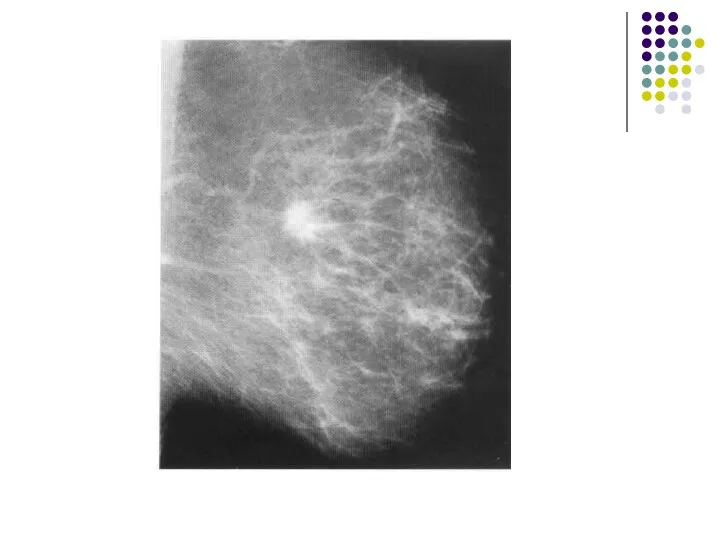
- 86. The typical ultrasound features are Most spiculate carcinomas of I cm diameter or more can be
- 87. the presence of these signs, however, is variable: acoustic shadowing may be absent; an echo-poor mass
- 93. Non-invasive intracystic carcinoma.
- 94. Ductal carcinoma in situ-high-grade comedo type. (A-C) Irregular linear branching microcalcification.
- 95. Interval cancers are classified radiologically as follows: I. True interval: there is no evidence of the
- 96. 4. Minimal sign: there are subtle features on the screening mammograms which correspond to the position
- 97. Fibroadenoma Fibroadenoma are characteristically sharply outlined low soft tissue density lesions, sometimes with a lobulated outline
- 98. The typical ultrasound appearance of a fibroadenoma is a well circumscribed round or oval mass showing
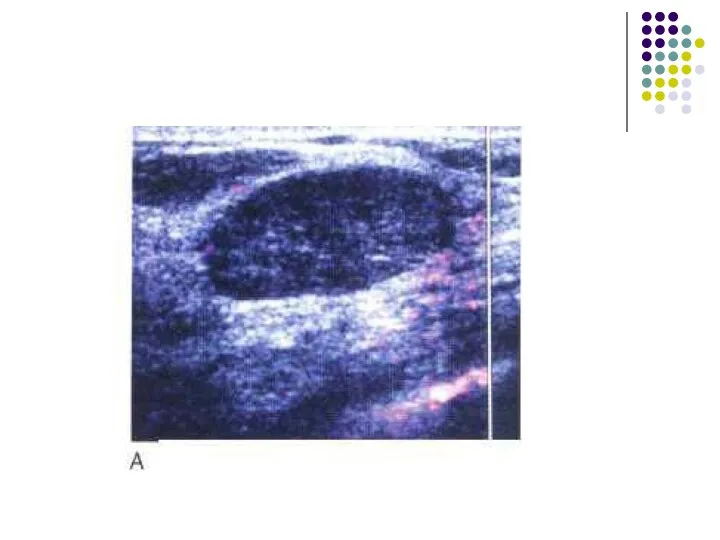
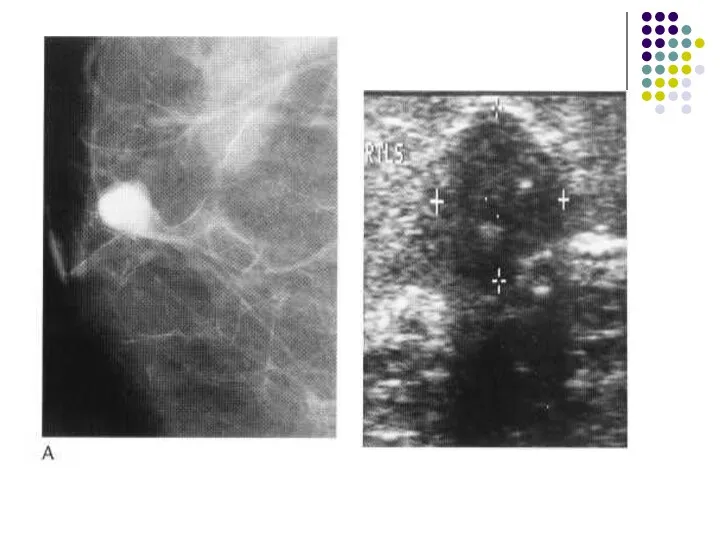
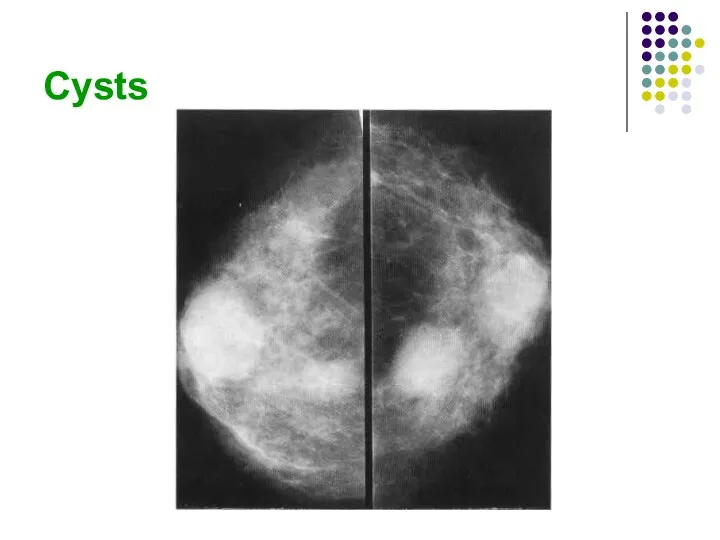
- 101. Cyst Cyst are the most common cause of a discrete breast mass. they are often multiple
- 102. Cysts can be readily diagnosed with ultrasound. They have: well-defined margins are oval or round in
- 103. When these features are present, a cyst can be diagnosed with certainty. Aspiration is easily performed
- 104. Cysts
- 106. Скачать презентацию
Normal anatomy
Normal Structures
Normal breast is composed:
mainly of parenchyma (lobules and ducts)
Normal anatomy
Normal Structures
Normal breast is composed:
mainly of parenchyma (lobules and ducts)
Parenchyma
The lobules are glandular units and are seen as ill-defined, splotchy
Parenchyma
The lobules are glandular units and are seen as ill-defined, splotchy
. The breast lobes are intertwined and are therefore not discretely
. The breast lobes are intertwined and are therefore not discretely
Connective tissue
Trabecular structures, which are condensations of connective tissue, appear as
Connective tissue
Trabecular structures, which are condensations of connective tissue, appear as
Fat
The breast is composed of a large amount of fat, which
Fat
The breast is composed of a large amount of fat, which
Lymph Nodes
Lymph nodes are seen in the axillae and occasionally in
Lymph Nodes
Lymph nodes are seen in the axillae and occasionally in
Veins
Veins are seen traversing the breast as uniform, linear opacities, about
Veins
Veins are seen traversing the breast as uniform, linear opacities, about
Arteries
Arteries appear as slightly thinner, uniform, linear densities and are best
Arteries
Arteries appear as slightly thinner, uniform, linear densities and are best
Skin
Skin lines are normally thin and are not easily seen without
Skin
Skin lines are normally thin and are not easily seen without
Normal variants
The normal anatomical variants of the brest result from the
Normal variants
The normal anatomical variants of the brest result from the
The dense breast
Diffuse increase in the density of the breast tissue
The dense breast
Diffuse increase in the density of the breast tissue
The increased density of the parenchyma seen as a result of
The increased density of the parenchyma seen as a result of
Mammography
The film-screen mammogram is created with x-rays, radiographic film, and intensifying
Mammography
The film-screen mammogram is created with x-rays, radiographic film, and intensifying
The routine examination consists of two views of each breast:
the craniocaudal
The routine examination consists of two views of each breast:
the craniocaudal
The C-C view can be considered the “top-down” view, and
The C-C view can be considered the “top-down” view, and
A flat, plastic compression paddle is then gently but firmly lowered
A flat, plastic compression paddle is then gently but firmly lowered
Compression may be uncomfortable, and may even be painful in a
Compression may be uncomfortable, and may even be painful in a
Compression
Firm compression is essential for high-quality mammograms and is applied
Compression
Firm compression is essential for high-quality mammograms and is applied
The effects of compression are:
(i) reduced dose;
(ii) reduced scatter-improved contrast;
(iii) reduced
The effects of compression are:
(i) reduced dose;
(ii) reduced scatter-improved contrast;
(iii) reduced
Mammography projections and normal appearances
The standard examination for women undergoing either
Mammography projections and normal appearances
The standard examination for women undergoing either
More breast tissue is demonstrated on the lateral oblique projection than
More breast tissue is demonstrated on the lateral oblique projection than
The standard craniocaudal film is obtained with a vertical X-ray beam
The standard craniocaudal film is obtained with a vertical X-ray beam
Supplementary views
For demonstration of tissue in the most posterolateral part of
Supplementary views
For demonstration of tissue in the most posterolateral part of
Magnification views
Magnification views are obtained by increasing the object-film distance,
Magnification views
Magnification views are obtained by increasing the object-film distance,
Localized compression views
Localized compression views are obtained by using a
Localized compression views
Localized compression views are obtained by using a
Screening Mammography
The standard mammogram (along with appropriate history taking) makes up
Screening Mammography
The standard mammogram (along with appropriate history taking) makes up
Diagnostic Mammography
The diagnostic mammogram begins with the two-view standard mammogram. Additional
Diagnostic Mammography
The diagnostic mammogram begins with the two-view standard mammogram. Additional
Indications for diagnostic mammography are:
(1) a palpable mass or
Indications for diagnostic mammography are:
(1) a palpable mass or
Indications of mammography
• Screening asymptomatic women aged 50 years and over
•
Indications of mammography
• Screening asymptomatic women aged 50 years and over
•
• Investigation of symptomatic women aged 35 years and over with
• Investigation of symptomatic women aged 35 years and over with
Patient Preparation
For the mammogram, two-piece clothing is most convenient as the
Patient Preparation
For the mammogram, two-piece clothing is most convenient as the
Mammography is generally limited to ambulatory, cooperative patients because of the
Mammography is generally limited to ambulatory, cooperative patients because of the
Computer-Aided Detection
Computer-aided detection (CAD) utilizes complex algorithms to analyze the data
Computer-Aided Detection
Computer-aided detection (CAD) utilizes complex algorithms to analyze the data
_ Ultrasonography
Technique
High-quality images of the normal and abnormal breast can be
_ Ultrasonography
Technique
High-quality images of the normal and abnormal breast can be
The side being examined is raised and the arm placed
The side being examined is raised and the arm placed
The indications for ultrasonography are:
(1) a mammographically detected mass, the nature
The indications for ultrasonography are:
(1) a mammographically detected mass, the nature
Ultrasonography is a highly reliable technique for differentiating cystic from solid
Ultrasonography is a highly reliable technique for differentiating cystic from solid
A limitation
A limitation of ultrasonography is that it is very
A limitation
A limitation of ultrasonography is that it is very
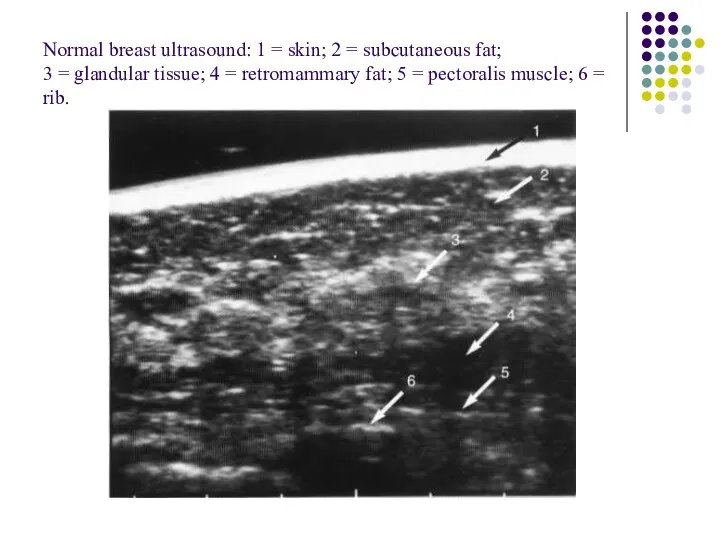
Normal breast ultrasound: 1 = skin; 2 = subcutaneous fat;
3 =
Normal breast ultrasound: 1 = skin; 2 = subcutaneous fat; 3 =
Magnetic Resonance Imaging
The role of MRI in mammography continues to
Magnetic Resonance Imaging
The role of MRI in mammography continues to
(5) screening of high-risk patients
(6) evaluating implants
(7) evaluating difficult
(5) screening of high-risk patients
(6) evaluating implants
(7) evaluating difficult
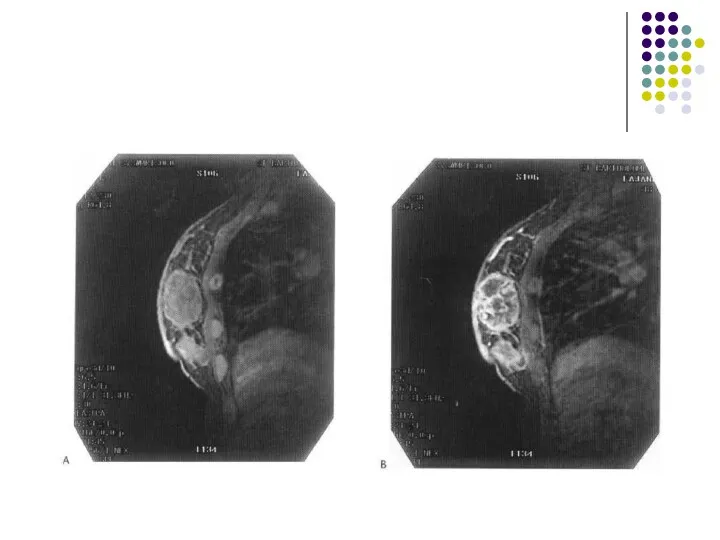
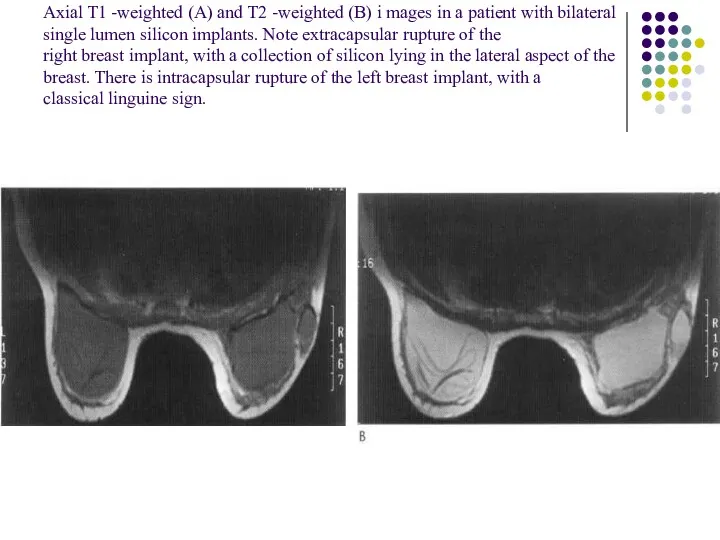
Axial T1 -weighted (A) and T2 -weighted (B) i mages in
Axial T1 -weighted (A) and T2 -weighted (B) i mages in
_ Ductography
Ductography, or galactography, uses mammographic imaging with contrast injection into
_ Ductography
Ductography, or galactography, uses mammographic imaging with contrast injection into
The indication
The indication for use is a profuse,
The indication
The indication for use is a profuse,
The patient lies in supine position while the discharging duct is
The patient lies in supine position while the discharging duct is
A ductogram showing small filling defects due to an intraductal
carcinoma (arrows).
A ductogram showing small filling defects due to an intraductal
carcinoma (arrows).
Image-Guided Needle Aspiration and Biopsy
The first indication is aspiration of cystic
Image-Guided Needle Aspiration and Biopsy
The first indication is aspiration of cystic
Needle biopsy is used in this case
(1) to confirm benignity
Needle biopsy is used in this case
(1) to confirm benignity
1 4G needle and automated biopsy device used for ultrasound
and stereotactic
1 4G needle and automated biopsy device used for ultrasound and stereotactic
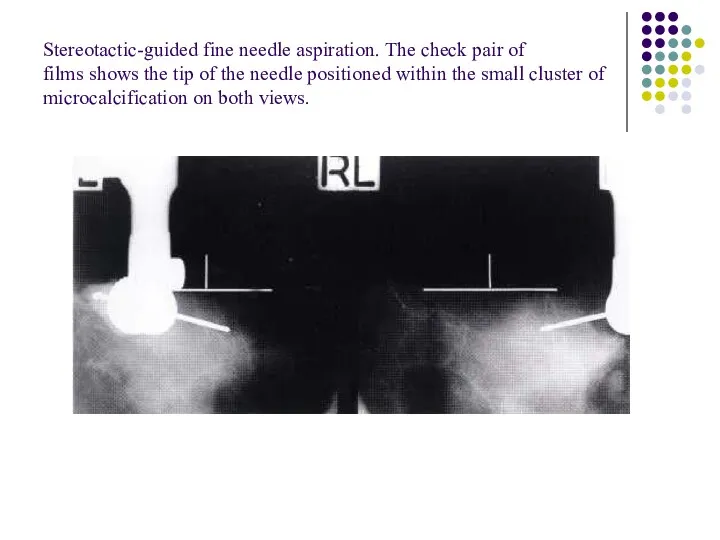
Stereotactic-guided fine needle aspiration. The check pair of
films shows the tip
Stereotactic-guided fine needle aspiration. The check pair of films shows the tip
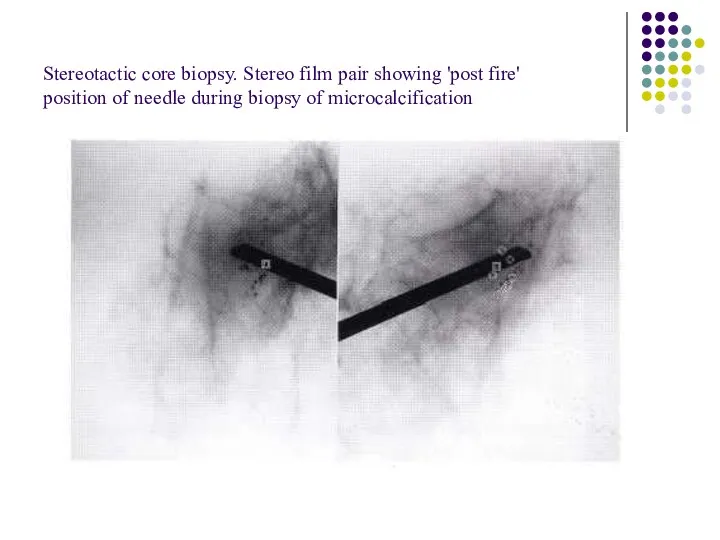
Stereotactic core biopsy. Stereo film pair showing 'post fire'
position of needle
Stereotactic core biopsy. Stereo film pair showing 'post fire' position of needle
Image-Guided Needle Localization
When a nonpalpable breast lesion must be excised, imaging
Image-Guided Needle Localization
When a nonpalpable breast lesion must be excised, imaging
Once the needle is in the appropriate position, a hook wire
Once the needle is in the appropriate position, a hook wire
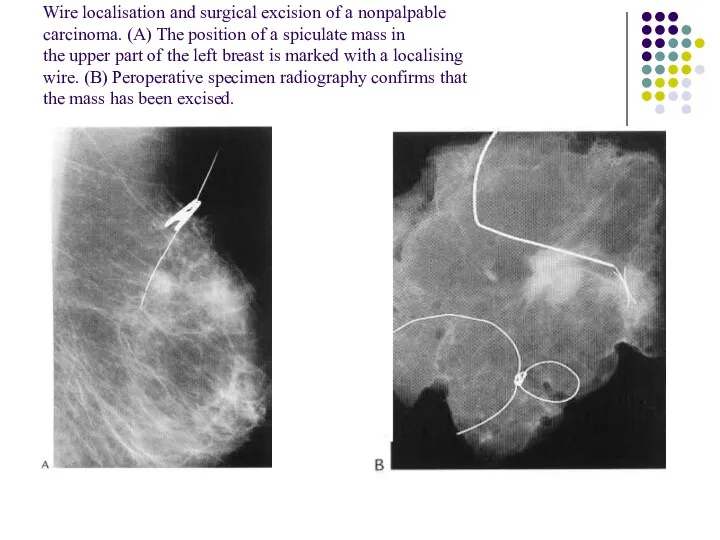
Wire localisation and surgical excision of a nonpalpable
carcinoma. (A) The position
Wire localisation and surgical excision of a nonpalpable carcinoma. (A) The position
Patient Preparation
Patients for whom stereotactic biopsy is being considered should be
Patient Preparation
Patients for whom stereotactic biopsy is being considered should be

Approach to the Palpable Lump
When a breast lump is found, several
Approach to the Palpable Lump
When a breast lump is found, several
Second, is the lump new or enlarged? A new lump is
Second, is the lump new or enlarged? A new lump is
Third, how big is the lump? Tiny pea-sized or smaller lumps,
Third, how big is the lump? Tiny pea-sized or smaller lumps,
Fourth, how old is the patient? If the patient is less
Fourth, how old is the patient? If the patient is less
If the patient is below 35 years of age, a significant
If the patient is below 35 years of age, a significant
For women between the ages of 30 and 40 years, judgment
For women between the ages of 30 and 40 years, judgment
Bi - rads assessment categories
category 0 - need additional imaging
Bi - rads assessment categories
category 0 - need additional imaging
Circumscribed mass
A circumscribed mass is analysed according to the following features:
I.
Circumscribed mass
A circumscribed mass is analysed according to the following features:
I.
Radiolucent lesions
Lipoma
Oil cyst
Galactocele.
Radiolucent lesions
Lipoma
Oil cyst
Galactocele.
Mixed density lesions
adenolipoma hamartoma
galactocele
hematoma
lymph node
Mixed density lesions
adenolipoma hamartoma
galactocele
hematoma
lymph node
Radiopaque (soft-tissue density) lesions
Benign lesions
* Cyst
* Fibroadenoma
* Papilloma
*Phyllodes tumour
* Abscess
* Lymph
Radiopaque (soft-tissue density) lesions
Benign lesions
* Cyst
* Fibroadenoma
* Papilloma
*Phyllodes tumour
* Abscess
* Lymph
Malignant lesions
* Mucinous carcinoma
* Medullary carcinoma
* Papillary carcinoma
* Invasive ductal carcinoma
*
Malignant lesions
* Mucinous carcinoma
* Medullary carcinoma
* Papillary carcinoma
* Invasive ductal carcinoma
*
Calcifications
Arterial: curvilinear, parallel line calcifications along the course of a blood
Calcifications
Arterial: curvilinear, parallel line calcifications along the course of a blood
Cyst: curvilinear calcification may occur in the wall of a cyst.
Carcinoma:
Cyst: curvilinear calcification may occur in the wall of a cyst.
Carcinoma:
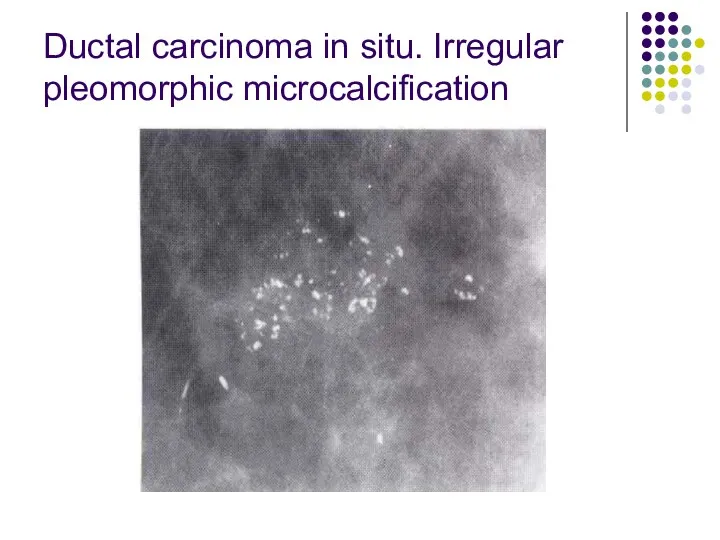
Ductal carcinoma in situ. Irregular pleomorphic microcalcification
Ductal carcinoma in situ. Irregular pleomorphic microcalcification
Milk of calcium in benign cystic change. On the craniocaudal
view the
Milk of calcium in benign cystic change. On the craniocaudal view the
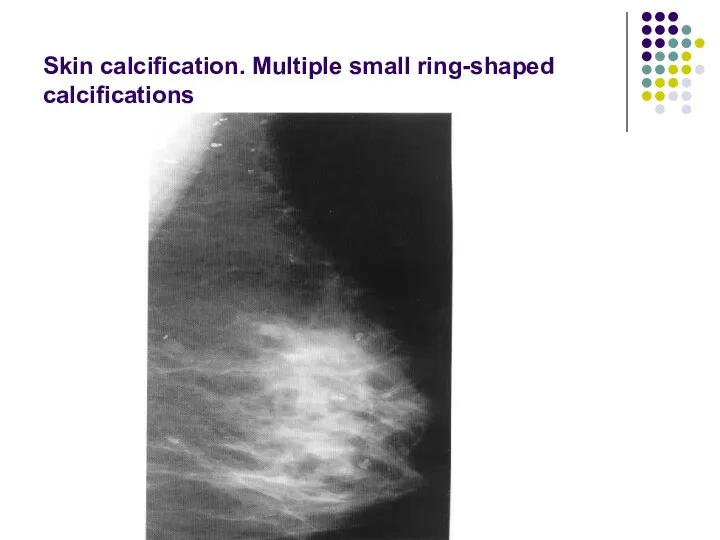
Skin calcification. Multiple small ring-shaped calcifications
Skin calcification. Multiple small ring-shaped calcifications
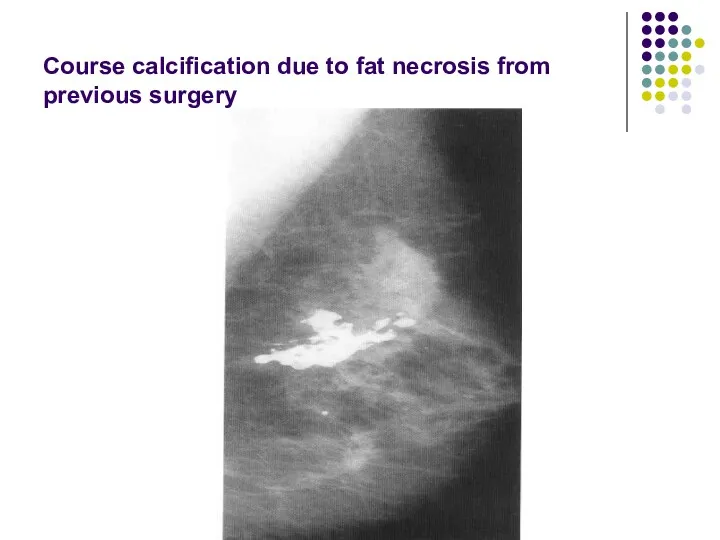
Course calcification due to fat necrosis from previous surgery
Course calcification due to fat necrosis from previous surgery
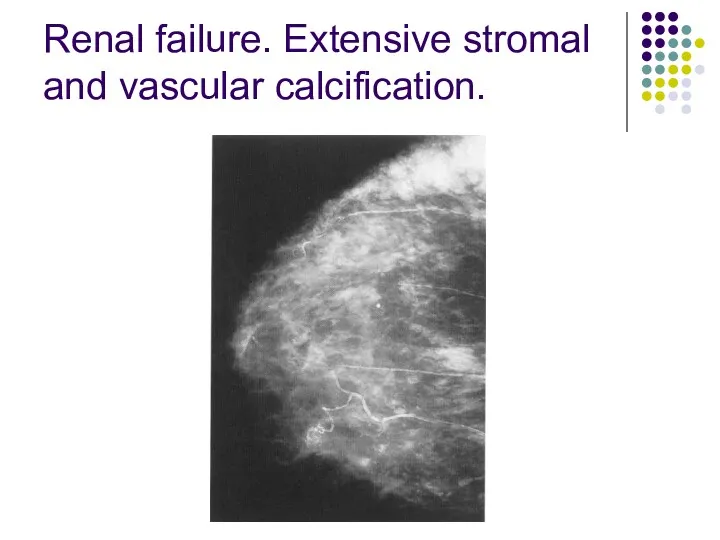
Renal failure. Extensive stromal and vascular calcification.
Renal failure. Extensive stromal and vascular calcification.
Spiculate mass
A spiculate mass is the commonest mammographic appearance of invasive
Spiculate mass
A spiculate mass is the commonest mammographic appearance of invasive
2. Large or superficially positioned tumors may be associated with localized
2. Large or superficially positioned tumors may be associated with localized
The typical ultrasound features are
Most spiculate carcinomas of I cm diameter
The typical ultrasound features are
Most spiculate carcinomas of I cm diameter
the presence of these signs, however, is variable: acoustic shadowing
the presence of these signs, however, is variable: acoustic shadowing
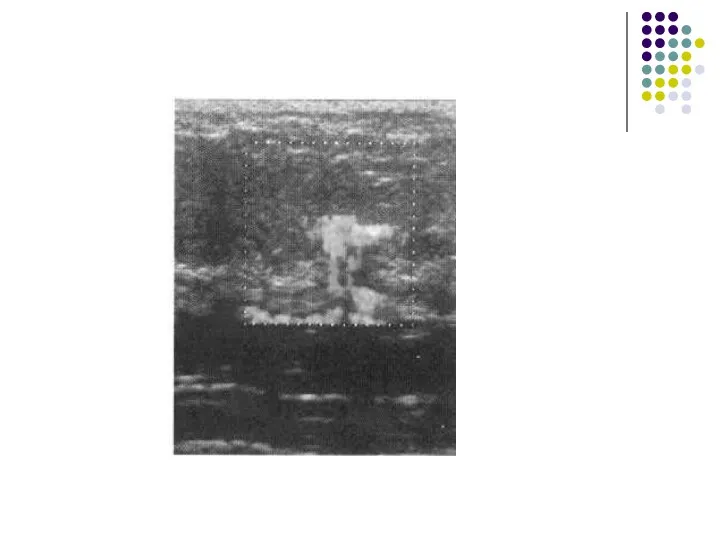
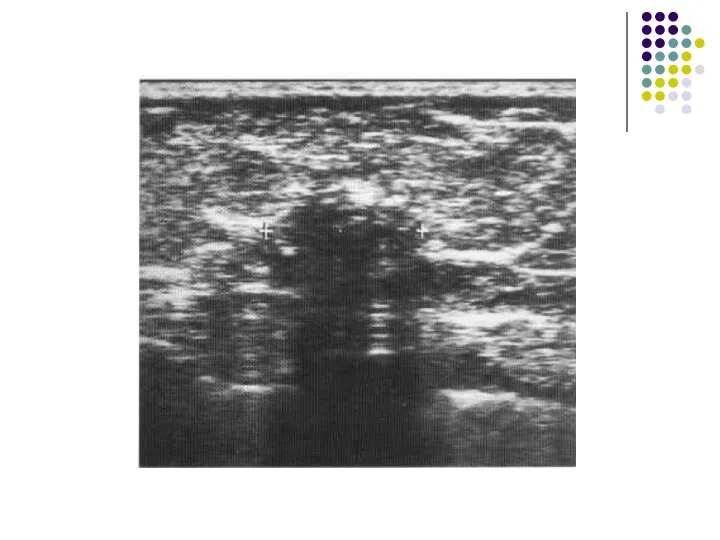
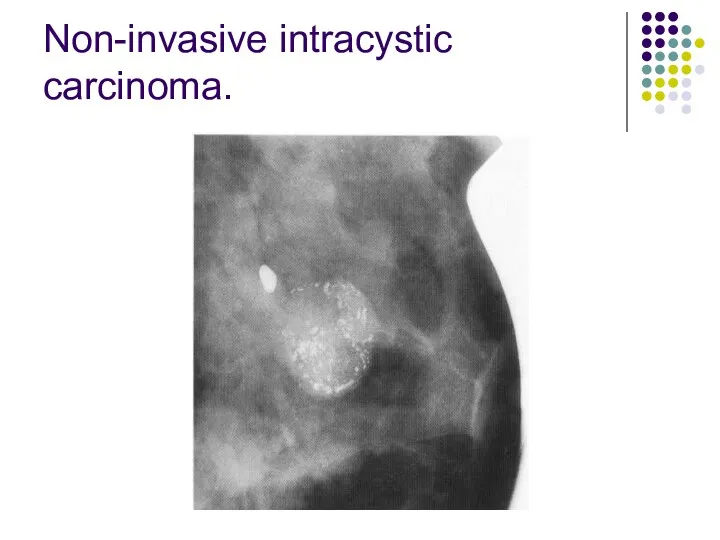
Non-invasive intracystic carcinoma.
Non-invasive intracystic carcinoma.
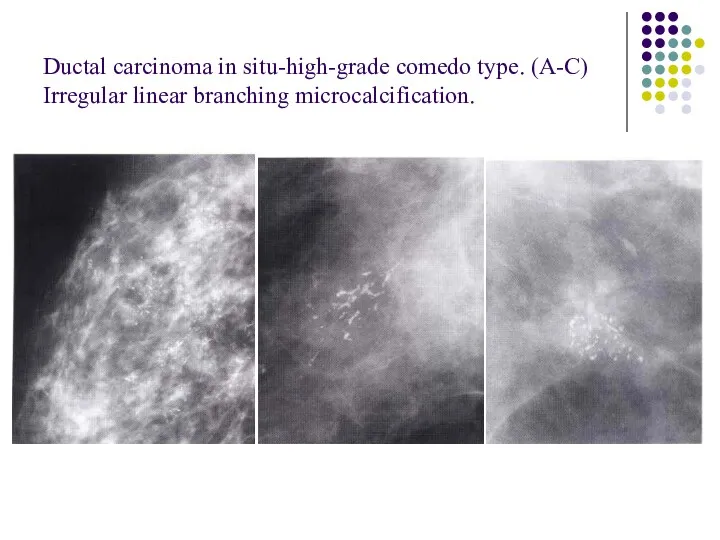
Ductal carcinoma in situ-high-grade comedo type. (A-C) Irregular linear branching microcalcification.
Ductal carcinoma in situ-high-grade comedo type. (A-C) Irregular linear branching microcalcification.
Interval cancers are classified radiologically as follows:
I. True interval: there is
Interval cancers are classified radiologically as follows:
I. True interval: there is
4. Minimal sign: there are subtle features on the screening mammograms
4. Minimal sign: there are subtle features on the screening mammograms
Fibroadenoma
Fibroadenoma are characteristically
sharply outlined
low soft tissue density
Fibroadenoma
Fibroadenoma are characteristically
sharply outlined
low soft tissue density
The typical ultrasound appearance of a fibroadenoma is
a well circumscribed round
The typical ultrasound appearance of a fibroadenoma is
a well circumscribed round
Cyst
Cyst are the most common cause of a discrete breast mass.
they
Cyst
Cyst are the most common cause of a discrete breast mass.
they
Cysts can be readily diagnosed with ultrasound.
They have:
well-defined margins
are
Cysts can be readily diagnosed with ultrasound.
They have:
well-defined margins
are
When these features are present, a cyst can be diagnosed with
When these features are present, a cyst can be diagnosed with
Cysts
Cysts
 Тыныс алу жолдарының инфекциясы немесе ауа –тамшы инфекциялары
Тыныс алу жолдарының инфекциясы немесе ауа –тамшы инфекциялары О вреде абортов
О вреде абортов Диагностика и лечение артериальной гипертензии на уровне ПМСП
Диагностика и лечение артериальной гипертензии на уровне ПМСП Роль медицинской сестры в подготовке пациента к плановой операции
Роль медицинской сестры в подготовке пациента к плановой операции Гигиенические основы физического воспитания и закаливания детей и подростков
Гигиенические основы физического воспитания и закаливания детей и подростков Шашыранды склероз
Шашыранды склероз Диагностика ишемической болезни сердца
Диагностика ишемической болезни сердца Осложнения сахарного диабета. Кома кетоацидотическая
Осложнения сахарного диабета. Кома кетоацидотическая Туа біткен кардиттер. Эластофиброз
Туа біткен кардиттер. Эластофиброз Халық денсаулығы және денсаулық сақтау жүйесі туралы
Халық денсаулығы және денсаулық сақтау жүйесі туралы Тики. Этиология
Тики. Этиология Рак щитовидной железы
Рак щитовидной железы Ерте жастағы аутизм
Ерте жастағы аутизм Особенности клинического течения заболеваний пародонта у детей
Особенности клинического течения заболеваний пародонта у детей Гигиенические требования к размещению войск в полевых условиях. Типы полевых жилищ, их характеристика
Гигиенические требования к размещению войск в полевых условиях. Типы полевых жилищ, их характеристика Ортодонтическое лечение. Общий план
Ортодонтическое лечение. Общий план Сахарный диабет. Заболевания щитовидной железы. Ожирение
Сахарный диабет. Заболевания щитовидной железы. Ожирение Цементы. Амальгамы. Компомеры. Ормокеры. Состав, свойства и особенности клинического применения
Цементы. Амальгамы. Компомеры. Ормокеры. Состав, свойства и особенности клинического применения Особливості медико-соціального забезпечення населення літнього віку. Організація паліативної та хоспісної допомоги населенню
Особливості медико-соціального забезпечення населення літнього віку. Організація паліативної та хоспісної допомоги населенню Ортодонтическое лечение. Стоматология
Ортодонтическое лечение. Стоматология Диф.діагностика жовтяниць у новонародженних дітей. Тема 17
Диф.діагностика жовтяниць у новонародженних дітей. Тема 17 Десмургия. Иммобилизация
Десмургия. Иммобилизация Пневмомикозы. Первичные и вторичные пневмомикозы
Пневмомикозы. Первичные и вторичные пневмомикозы Сестринские манипуляции. Постановка очистительной клизмы
Сестринские манипуляции. Постановка очистительной клизмы Макулодистрофия. Макулярная дистрофия сетчатки глаза
Макулодистрофия. Макулярная дистрофия сетчатки глаза Медицина катастроф
Медицина катастроф Задние афазии
Задние афазии Диагностика и лечение ХСН
Диагностика и лечение ХСН