- Radiology and imaging the biliary, liver and pancreas

Содержание
- 2. The biliary tract These include: 1. Simple X-ray 2. Oral Cholecystography 3. Intravenous Cholangiography 4. Operative
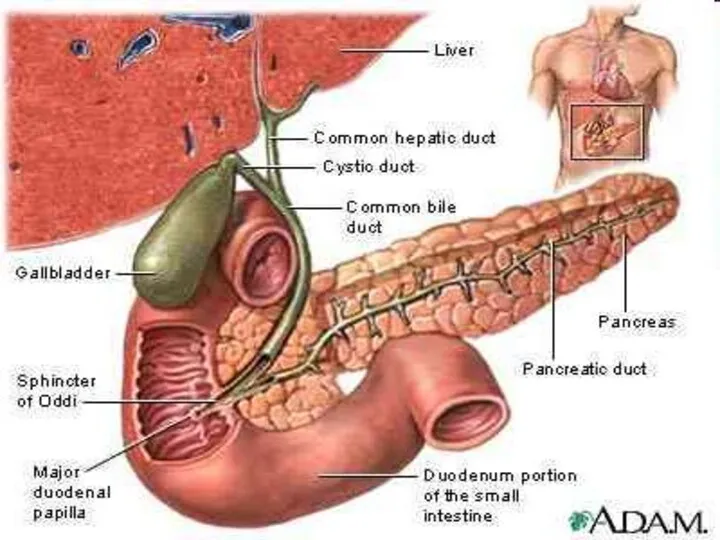
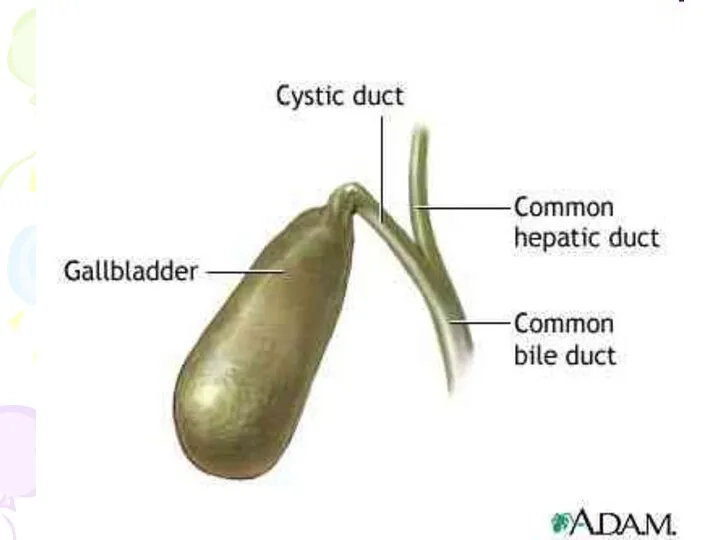
- 3. Gall Bladder The normal gall bladder is composed of four parts: fundus body infundibulum and a
- 4. Smooth muscle fibers are found in the wall of the fundus and infundibulum but are completely
- 5. The gall bladder concentrates this bile and when the pressure in gall bladder falls below that
- 8. Cholecystitis Acute Cholecystitis In acute cholecystitis cholecystography is contraindication because: opaque medium may aggravate the inflammation
- 9. Chronic cholecystitis Chronic cholecystitis may follow acute cholecystitis with or without stones. Chronically inflamed gall bladder
- 10. Cholecystography In cholecystography we see the following three points by which we can estimate the biliary
- 11. Technique After a light fat-free dinner the patient is given 3 or 6gm of telepaque; next
- 12. Occasionally nausea may be complained or mild diarrhea may develop as side reaction. Sensitivity to iodine
- 13. The amount of iodine in bile then becomes sufficient to make it radio-opaque and a dense
- 14. Cause of Non- visualization of Gall Bladder The patient could not take drug or could not
- 15. There may be faulty absorption from the intestine Obstruction of cystic duct may prevent entrance of
- 16. Normal Cholecystography Gall bladder is visualized with uniform density There is no filling defect suggestive of
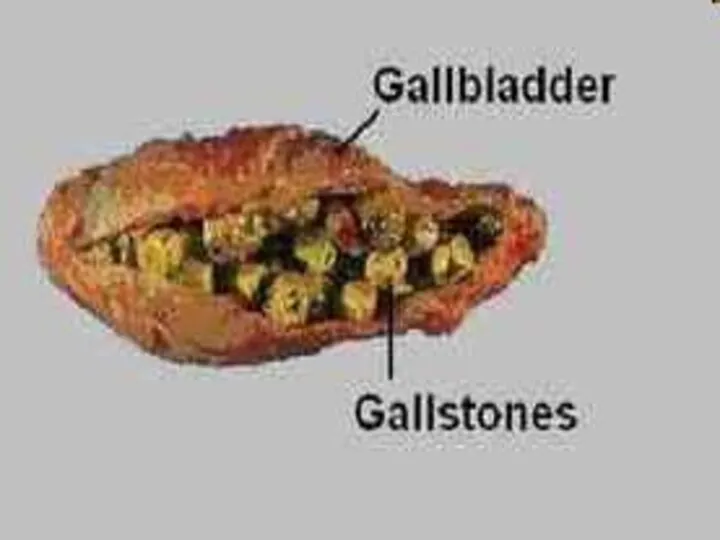
- 18. Non Functioning Gall bladder Common cause for non-functioning gall bladder is chronic cholecystitis with stones. Multiple
- 19. When gall bladder is sub normally functional a shadow of the gall bladder is visible but
- 20. Simple X-ray of the biliary tract Opaque gall stones will be readily shown. These vary in
- 21. Non-opaque gall-stones, for instance large cholesterol stones, will not be diagnosed by plain x-rays and will
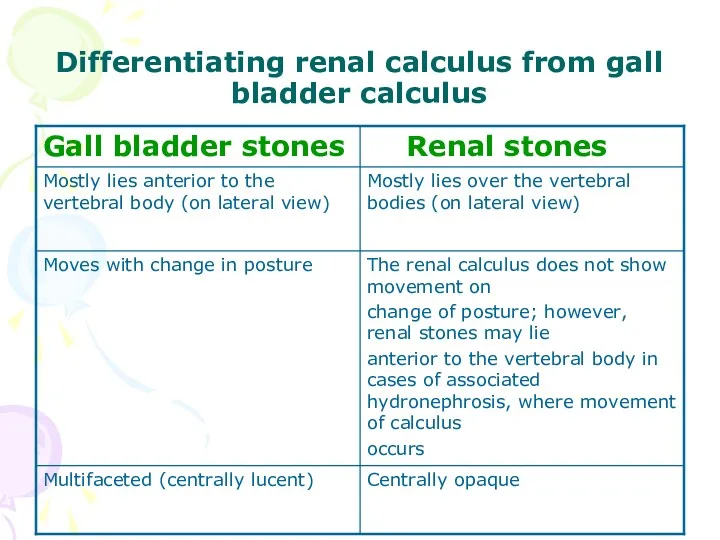
- 22. Differentiating renal calculus from gall bladder calculus
- 28. Gas in the biliary tract Usually in the hepatic ducts, is only occasionally noted at plain
- 29. It is important to remember that both oral and intravenous cholecystography are unlikely to be successful
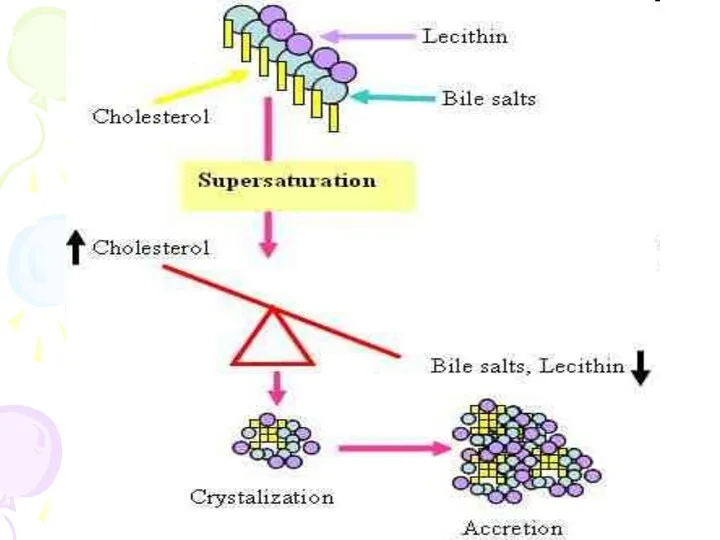
- 30. Cholesterols [strawberry gall bladder] There is diffuse deposition of cholesterol on the mucosa of the gall
- 31. Cholesterosis are: small round translucent defects attached to the gall bladder wall these vary in size
- 32. A cholesterol polyp is not a tumor but consists of small collection of cholesterol crystals. It
- 36. Calcification of walls of Gall Bladder This is a rare condition. It cannot occur without existing
- 40. Milk of Calcium Gall Bladder Milk of calcium bile is a condition in which the gall
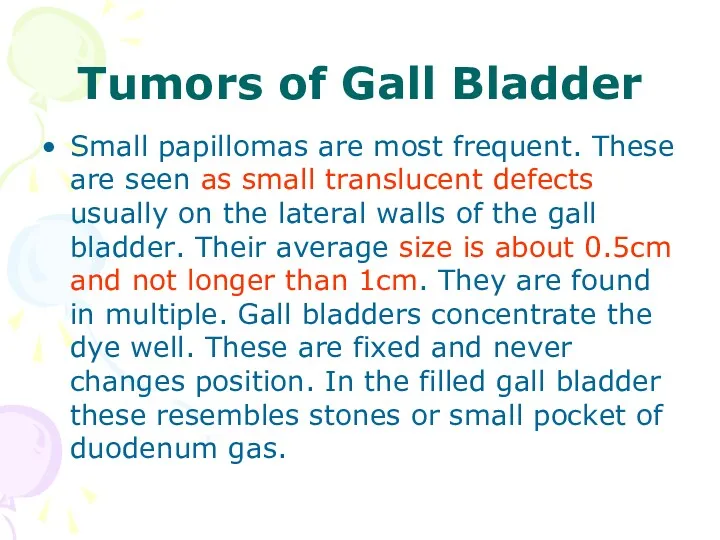
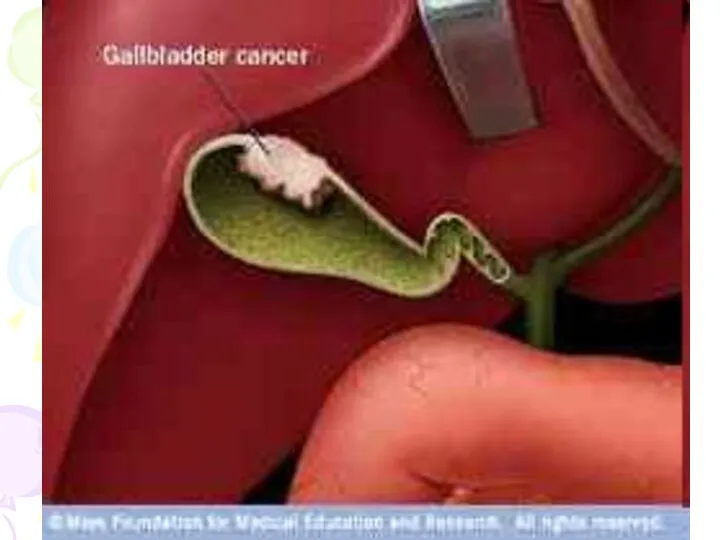
- 41. Tumors of Gall Bladder Small papillomas are most frequent. These are seen as small translucent defects
- 42. Adenoma of gall bladder is rear. It looks like single small semi -circular or circular translucent
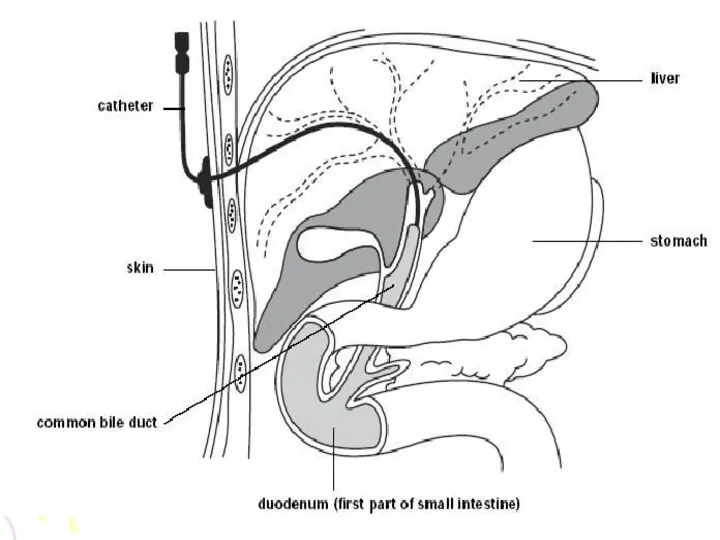
- 45. Percutaneous Cholangiography Indications are: • To differentiate between obstructive and non obstructive jaundice. • To determine
- 46. Contraindications are: • Hemorrhagic diathesis • Vitamin K resistant hypoprothrombinemia • Febrile cholangitis
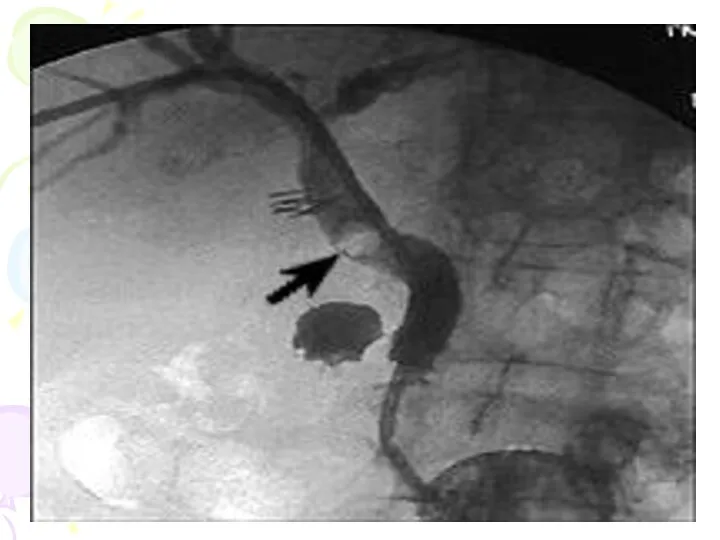
- 47. Interpretation of Percutaneous Cholangiography • Calculi producing filling defects. • Obstructed duct is usually due to
- 48. • Dilatation of duct with an uneven and ragged obstruction pattern indicates carcinoma in the ampulla
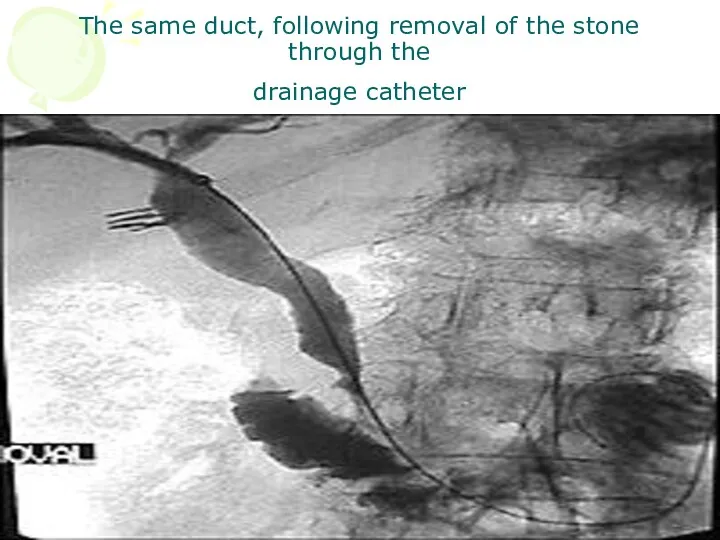
- 51. The same duct, following removal of the stone through the drainage catheter
- 52. Ultrasound This view is widely used as the preliminary examination in suspected gall bladder or billiary
- 53. Gall stones characteristically produce high density echoes and cast acoustic shadows appearing dark bands. Ultrasound will
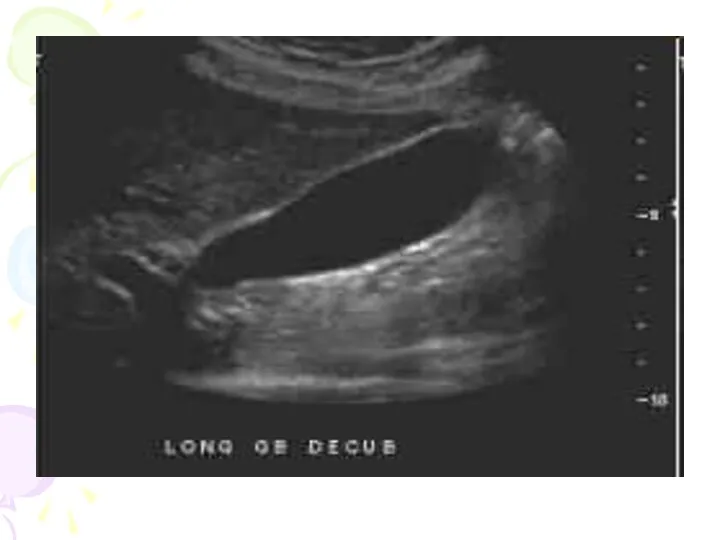
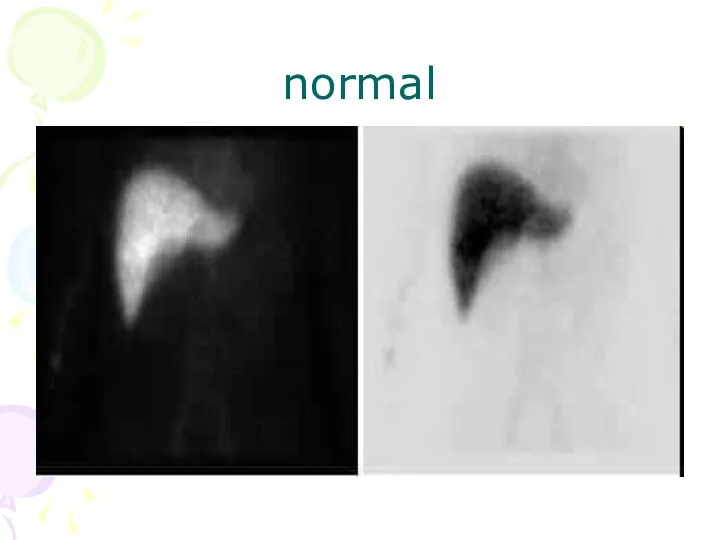
- 54. normal
- 57. stones
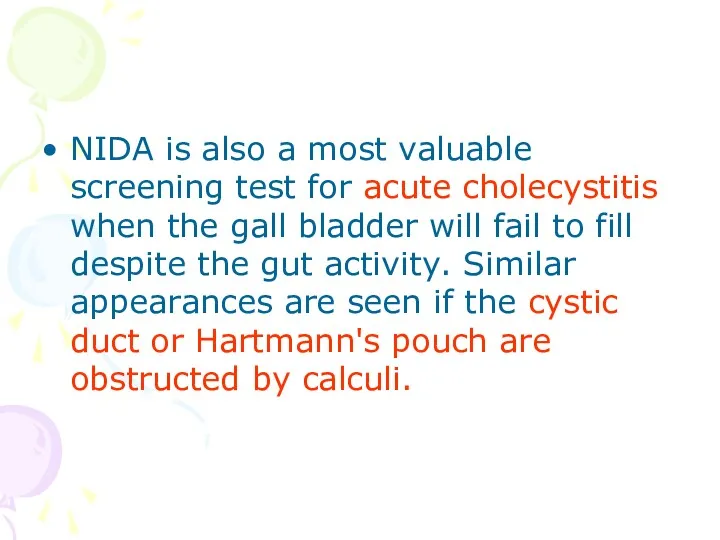
- 58. Isotope scanning 99 Tc HIDA (a derivative of iminodiacetic acid (IDA)) is a drug which is
- 59. NIDA is also a most valuable screening test for acute cholecystitis when the gall bladder will
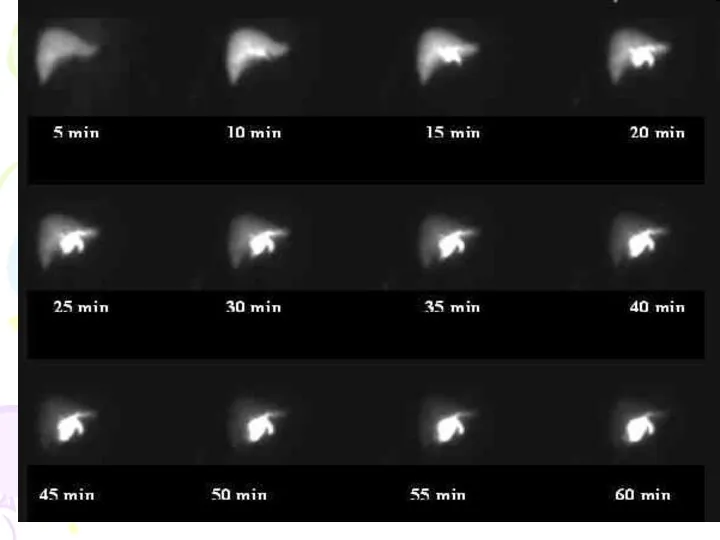
- 60. normal
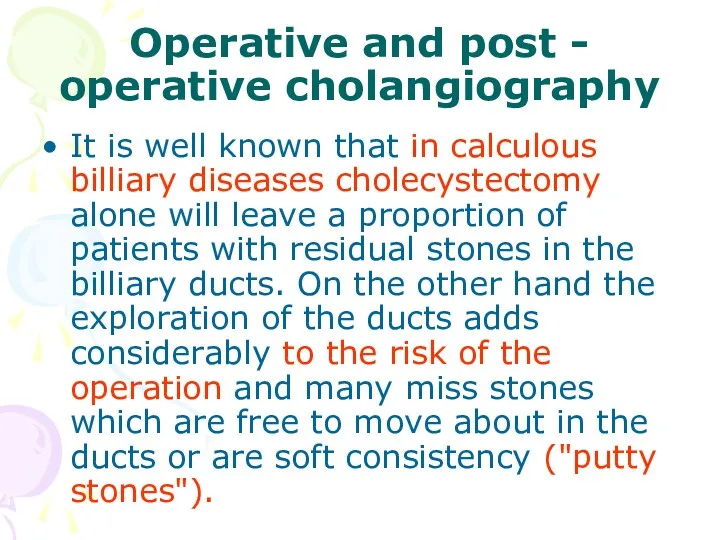
- 62. Operative and post - operative cholangiography It is well known that in calculous billiary diseases cholecystectomy
- 63. Many surgeons now perform operative cholangiography as a routine at operations for billiary stones. A small
- 64. Operative cholangiography Operative cholangiography, if skillfully performed, adds little to the operative time and will ensure
- 65. Post - operative cholangiography Post - operative cholangiography is carried out in the immediate post operative
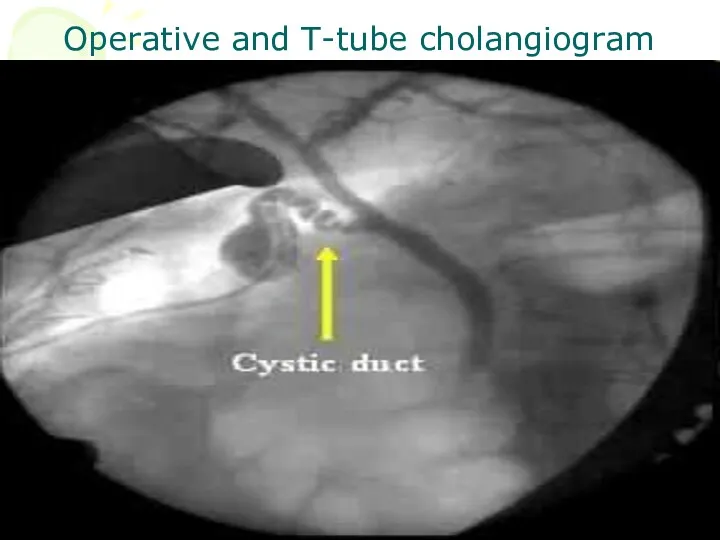
- 66. Operative and T-tube cholangiogram
- 67. post operative study
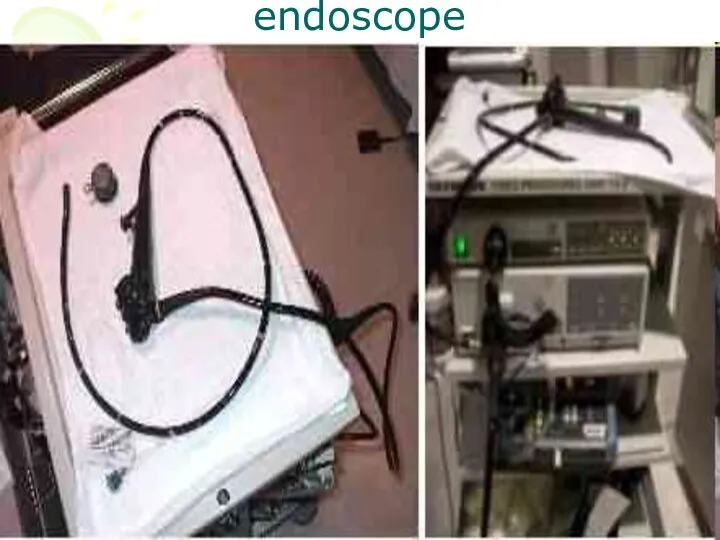
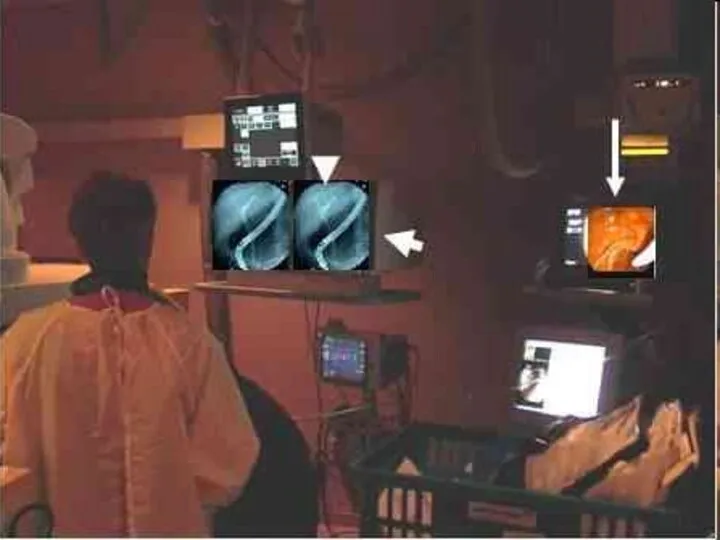
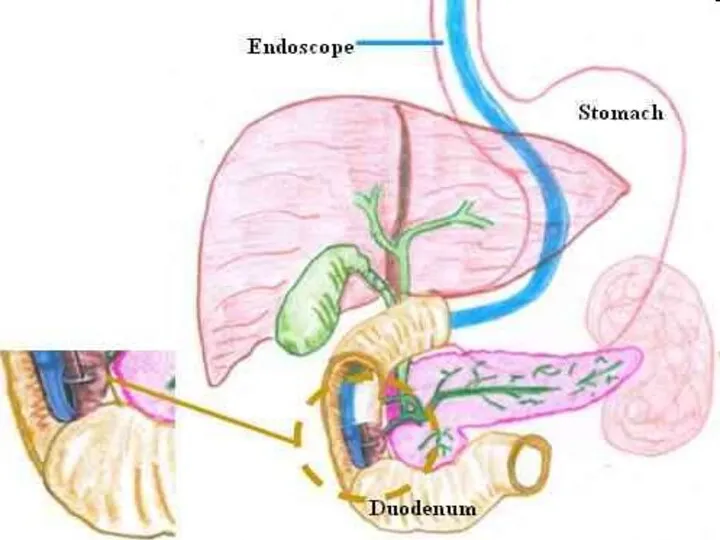
- 68. Endoscopic retrograde cholangio pancreatography (ERCP) Under radiological control, the ampulla of Vater is cannulated and the
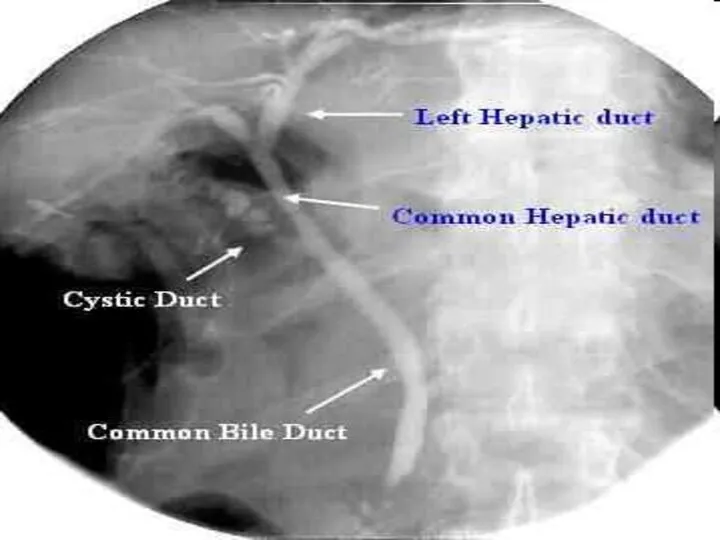
- 69. Biliary obstruction due to stone or neoplasm can be visualized or alternatively a normal biliary tree
- 70. For this examination the patient is usually fasting and lightly sedated. A side viewing duodenoscope or
- 72. endoscope
- 76. Stricture of the cystic duct
- 77. stones
- 78. The Liver The main indication or the investigation of the liver by imaging are the diagnosis
- 79. The techniques available include: • Simple X ray • Ultra sound • CT • Isotope scanning
- 80. Simple X ray provides little information apart from the confirming enlargement of the liver and showing
- 81. Indications are: the liver cysts abscess Hematomas and neoplasm both primary and secondary are readily identified
- 82. Tumors usually show as rounded areas with diminished echoes. Cysts are completely transonic. As already noted
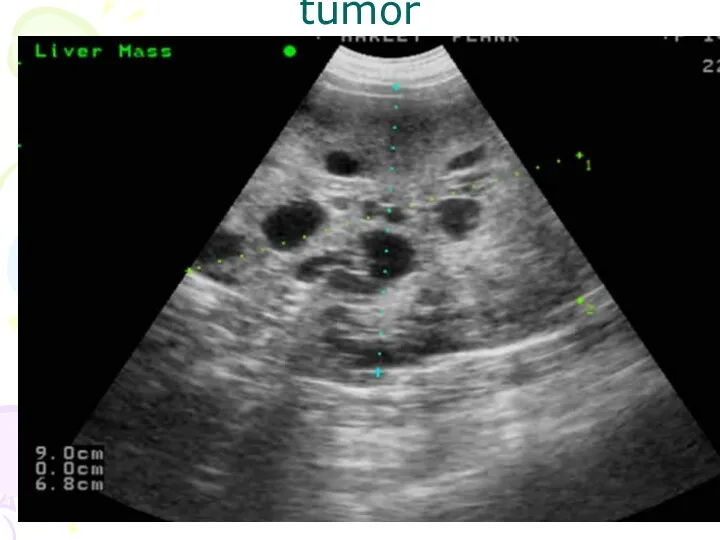
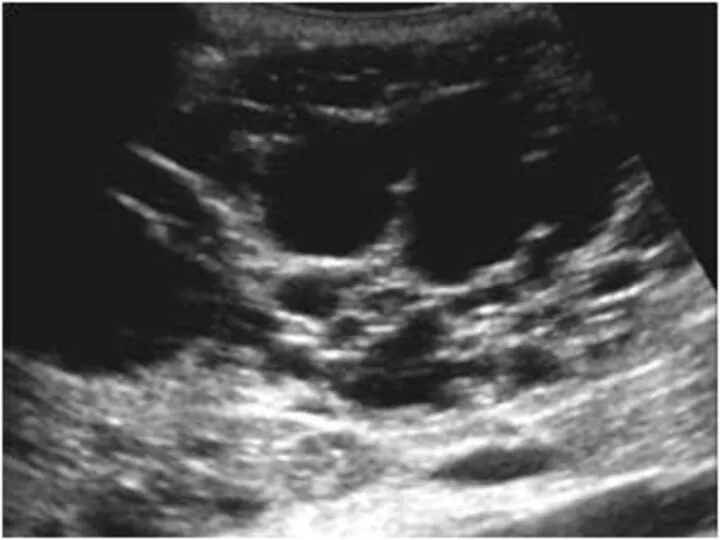
- 83. tumor
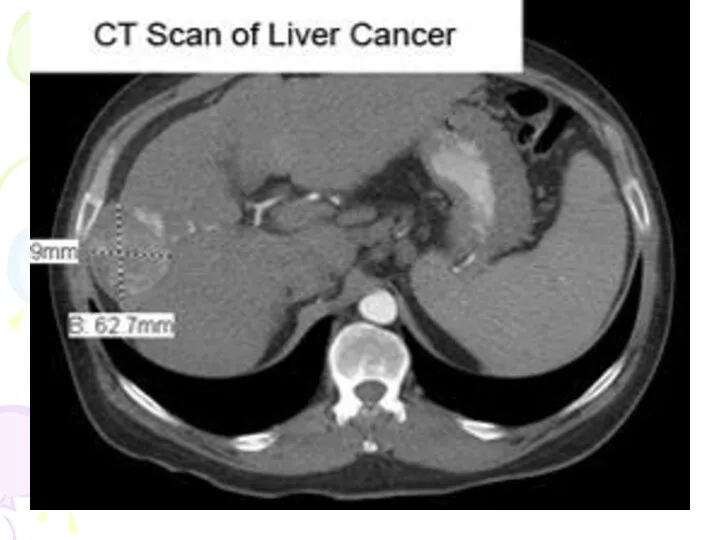
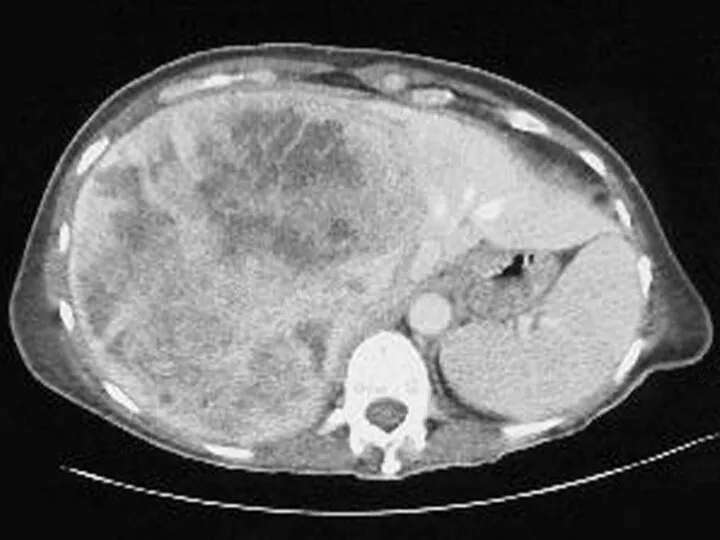
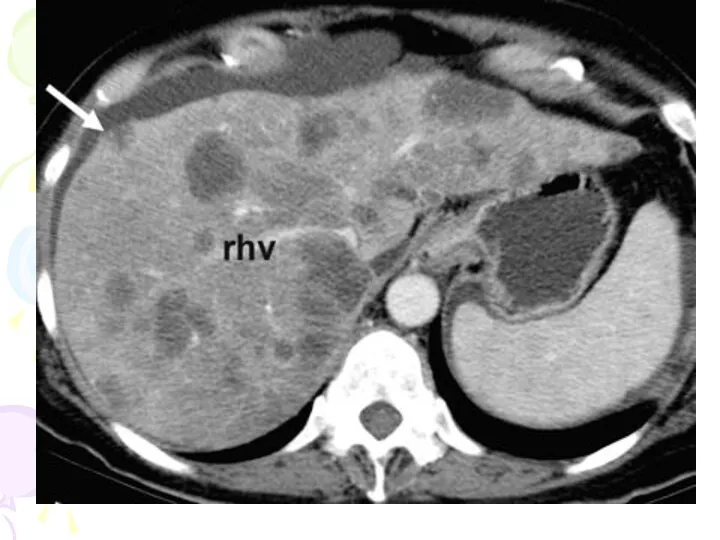
- 87. CT scanning CT shows the liver in axial sections with high resolution. Primary and secondary neoplasm
- 88. cyst
- 92. mts
- 94. stone
- 95. Necrotic gall bladder
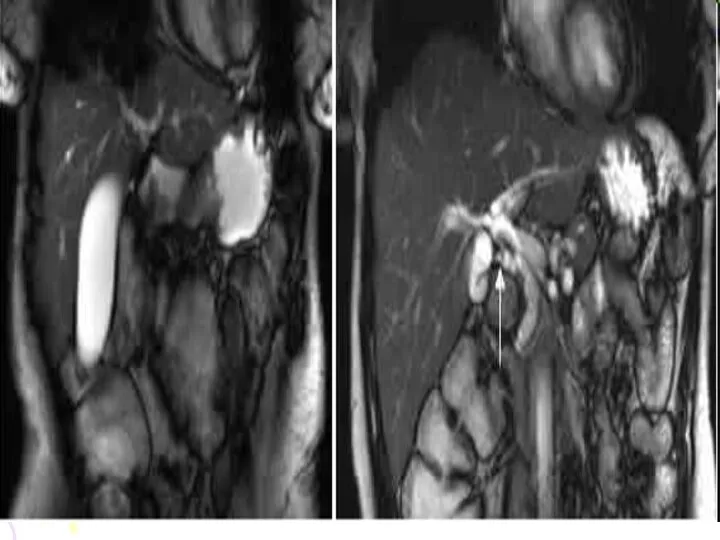
- 96. MRI MRI is similar to CT in the accuracy of showing focal lesions in the liver.
- 98. 3-D image
- 99. Angiography Hepatic angiography is performed by percutaneous transfemoral catheterization of the coeliac axis or superselective catheterization
- 100. The technique uses: for the diagnosis of tumors angiomas aneurysms and other vascular lesions for the
- 101. liver tumor during embolizations
- 103. hemangioma
- 104. Isotope scanning The study is usually performed 15-30 minutes after injection with radiopharmaceutical substent since 10-15
- 105. Following are the indications of liver imaging: • Evaluation of the liver size, shape and position.
- 107. CHOICE OF EXAMINATION IN BILIARY AND LIVER DISEASE Suspected liver masses (tumors, primary or secondary, cysts
- 108. CT and MRI will also perform this function but are more expansive investigations and CT involves
- 109. In suspected obstructive jaundice, ultrasound is the primary investigation of choice, though biliary isotope scanning will
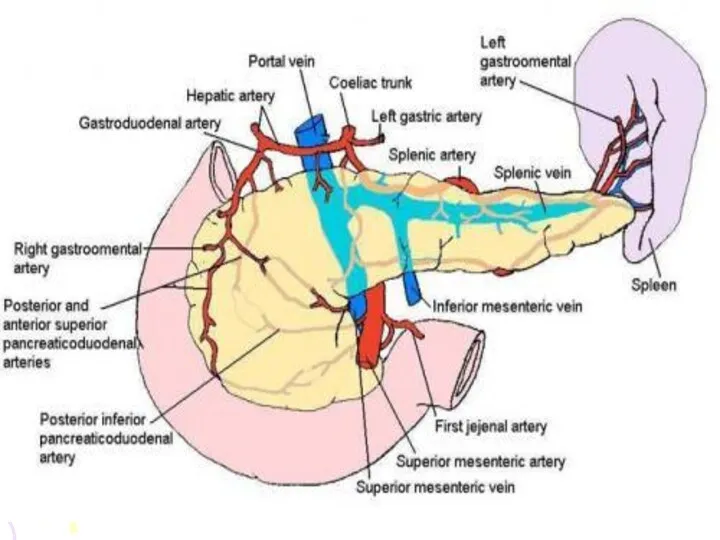
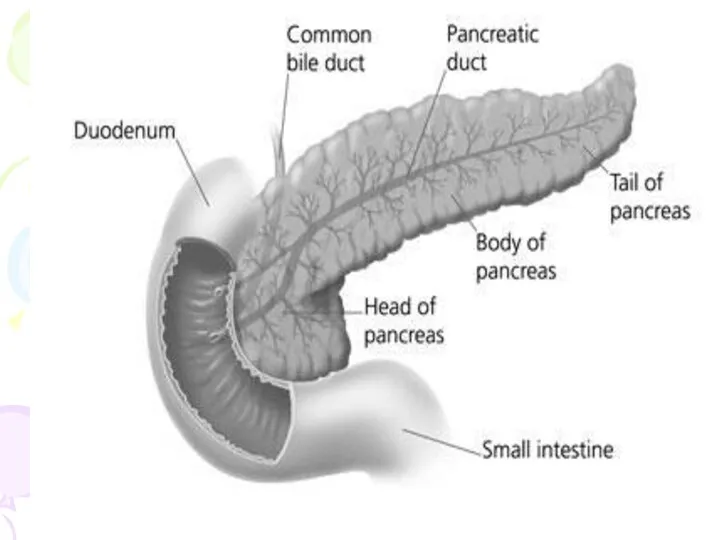
- 110. PANCREAS Pancreas lies in the posterior abdominal wall in the epigastrium and left hypochondrium. Head is
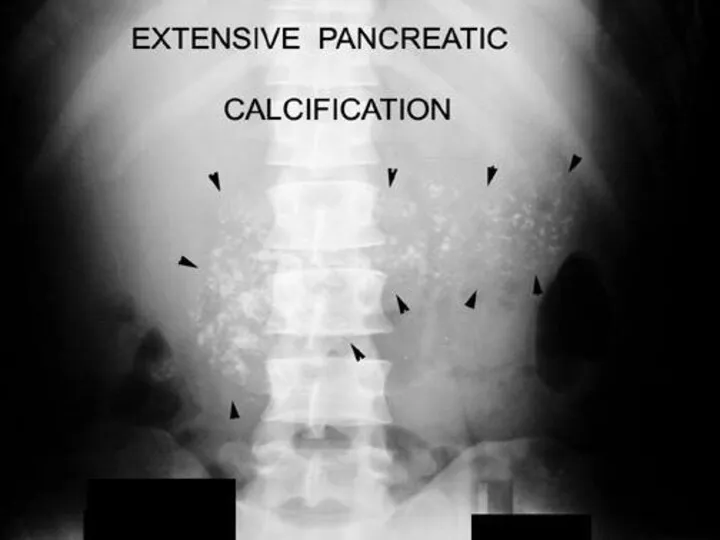
- 113. Simple X ray will occasionally show extensive nodules of calcification in the pancreas associated with chronic
- 116. Barium studies will show: distortion of the duodenal loop by masses in the head of the
- 119. Ultrasound: the normal pancreas may be partly obscured by bowel gas but when well seen appears
- 120. In acute pancreatitis, the whole organ is enlarged and edematous appearing more transonic than normal. Abscess
- 121. Rupture of pancreas
- 122. CT scan CT is now the method most widely used for the demonstration of the pancreatic
- 123. Small tumors such as islet cell adenomas are more difficult to diagnose. Acute pancreatitis may be
- 124. cyst
- 126. MRI MRI can also show the pancreas well but has no advantage over CT, which is
- 127. ERCP ERCP is the method of choice for demonstrating the pancreatic duct and its obstruction or
- 128. These include: 1. Stone extraction from pancreatic and bile ducts 2. Sphincterectomy 3. Biopsy of ampulla
- 129. Choice of examination CT is probably the best method for speedy demonstration of the pancreas. The
- 131. Скачать презентацию
The biliary tract
These include:
1. Simple X-ray
2. Oral Cholecystography
3. Intravenous Cholangiography
4.
The biliary tract
These include:
1. Simple X-ray
2. Oral Cholecystography
3. Intravenous Cholangiography
4.
Gall Bladder
The normal gall bladder is composed of four parts:
fundus
body
Gall Bladder
The normal gall bladder is composed of four parts:
fundus
body
Smooth muscle fibers are found in the wall of the
Smooth muscle fibers are found in the wall of the
The gall bladder concentrates this bile and when the pressure in
The gall bladder concentrates this bile and when the pressure in
Cholecystitis
Acute Cholecystitis
In acute cholecystitis cholecystography is contraindication because:
opaque medium
Cholecystitis
Acute Cholecystitis
In acute cholecystitis cholecystography is contraindication because:
opaque medium
Chronic cholecystitis
Chronic cholecystitis may follow acute cholecystitis with or without stones.
Chronic cholecystitis
Chronic cholecystitis may follow acute cholecystitis with or without stones.
Cholecystography
In cholecystography we see the following three points by which
Cholecystography
In cholecystography we see the following three points by which
Technique
After a light fat-free dinner the patient is given 3 or
Technique
After a light fat-free dinner the patient is given 3 or
Occasionally nausea may be complained or mild diarrhea may develop as
Occasionally nausea may be complained or mild diarrhea may develop as
The amount of iodine in bile then becomes sufficient to
The amount of iodine in bile then becomes sufficient to
Cause of Non- visualization of Gall Bladder
The patient could not
Cause of Non- visualization of Gall Bladder
The patient could not
There may be faulty absorption from the intestine
Obstruction of cystic duct
There may be faulty absorption from the intestine
Obstruction of cystic duct
Normal Cholecystography
Gall bladder is visualized with uniform density
There is
Normal Cholecystography
Gall bladder is visualized with uniform density
There is

Non Functioning Gall bladder
Common cause for non-functioning gall bladder is chronic
Non Functioning Gall bladder
Common cause for non-functioning gall bladder is chronic
When gall bladder is sub normally functional a shadow of the
When gall bladder is sub normally functional a shadow of the
Simple X-ray of the biliary tract
Opaque gall stones will be readily
Simple X-ray of the biliary tract
Opaque gall stones will be readily
Non-opaque gall-stones, for instance large cholesterol stones, will not be diagnosed
Non-opaque gall-stones, for instance large cholesterol stones, will not be diagnosed
Differentiating renal calculus from gall bladder calculus
Differentiating renal calculus from gall bladder calculus



Gas in the biliary tract
Usually in the hepatic ducts, is only
Gas in the biliary tract
Usually in the hepatic ducts, is only
It is important to remember that both oral and intravenous cholecystography
It is important to remember that both oral and intravenous cholecystography
![Cholesterols [strawberry gall bladder] There is diffuse deposition of cholesterol](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/202241/slide-29.jpg)
Cholesterols [strawberry gall bladder]
There is diffuse deposition of cholesterol on the
Cholesterols [strawberry gall bladder]
There is diffuse deposition of cholesterol on the
Cholesterosis are:
small round translucent defects attached to the gall bladder
Cholesterosis are:
small round translucent defects attached to the gall bladder
A cholesterol polyp is not a tumor but consists of small
A cholesterol polyp is not a tumor but consists of small



Calcification of walls of Gall Bladder
This is a rare condition.
Calcification of walls of Gall Bladder
This is a rare condition.



Milk of Calcium Gall Bladder
Milk of calcium bile is a condition
Milk of Calcium Gall Bladder
Milk of calcium bile is a condition
Tumors of Gall Bladder
Small papillomas are most frequent. These are seen
Tumors of Gall Bladder
Small papillomas are most frequent. These are seen
Adenoma of gall bladder is rear. It looks like single small
Adenoma of gall bladder is rear. It looks like single small
Percutaneous Cholangiography
Indications are:
• To differentiate between obstructive and non obstructive jaundice.
•
Percutaneous Cholangiography
Indications are:
• To differentiate between obstructive and non obstructive jaundice.
•
Contraindications are:
• Hemorrhagic diathesis
• Vitamin K resistant hypoprothrombinemia
• Febrile cholangitis
Contraindications are:
• Hemorrhagic diathesis
• Vitamin K resistant hypoprothrombinemia
• Febrile cholangitis
Interpretation of Percutaneous Cholangiography
• Calculi producing filling defects.
• Obstructed duct
Interpretation of Percutaneous Cholangiography
• Calculi producing filling defects.
• Obstructed duct
• Dilatation of duct with an uneven and ragged obstruction pattern
• Dilatation of duct with an uneven and ragged obstruction pattern
The same duct, following removal of the stone through the
drainage
The same duct, following removal of the stone through the drainage
Ultrasound
This view is widely used as the preliminary examination in suspected
Ultrasound
This view is widely used as the preliminary examination in suspected
Gall stones characteristically produce high density echoes and cast acoustic shadows
Gall stones characteristically produce high density echoes and cast acoustic shadows
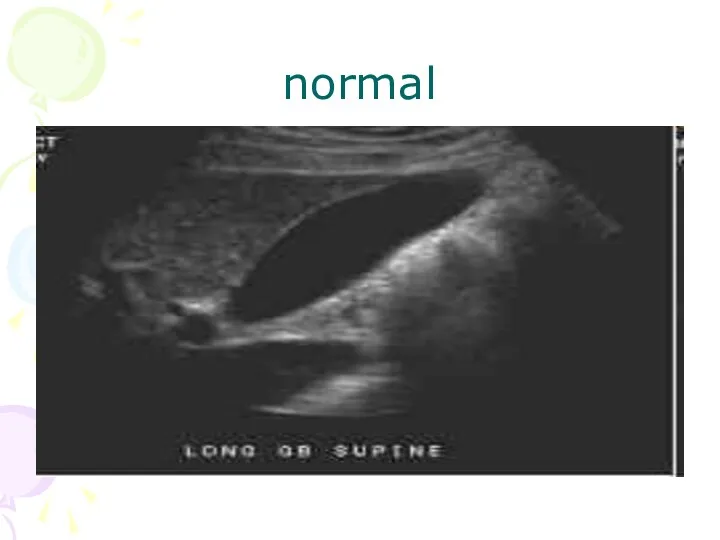
normal
normal


stones
stones
Isotope scanning
99 Tc HIDA (a derivative of iminodiacetic acid (IDA)) is
Isotope scanning
99 Tc HIDA (a derivative of iminodiacetic acid (IDA)) is
NIDA is also a most valuable screening test for acute cholecystitis
NIDA is also a most valuable screening test for acute cholecystitis
normal
normal
Operative and post - operative cholangiography
It is well known that in
Operative and post - operative cholangiography
It is well known that in
Many surgeons now perform operative cholangiography as a routine at operations
Many surgeons now perform operative cholangiography as a routine at operations
Operative cholangiography
Operative cholangiography, if skillfully performed, adds little to the
Operative cholangiography
Operative cholangiography, if skillfully performed, adds little to the
Post - operative cholangiography
Post - operative cholangiography is carried out
Post - operative cholangiography
Post - operative cholangiography is carried out
Operative and T-tube cholangiogram
Operative and T-tube cholangiogram
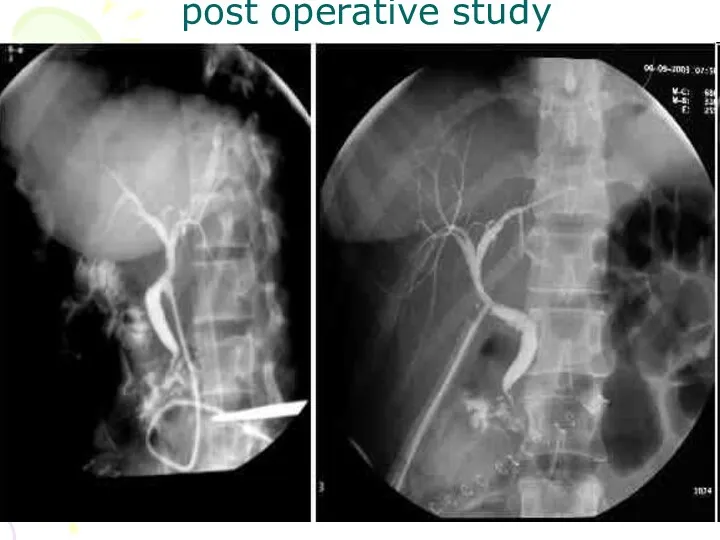
post operative study
post operative study
Endoscopic retrograde cholangio pancreatography (ERCP)
Under radiological control, the ampulla of Vater
Endoscopic retrograde cholangio pancreatography (ERCP)
Under radiological control, the ampulla of Vater
Biliary obstruction due to stone or neoplasm can be visualized or
Biliary obstruction due to stone or neoplasm can be visualized or
For this examination the patient is usually fasting and lightly sedated.

endoscope
endoscope
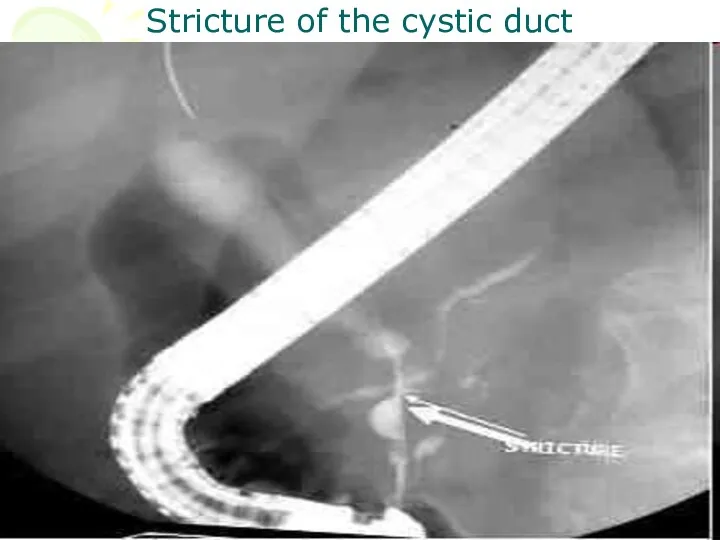
Stricture of the cystic duct
Stricture of the cystic duct

stones
stones
The Liver
The main indication or the investigation of the liver by
The Liver
The main indication or the investigation of the liver by
The techniques available include:
• Simple X ray
• Ultra sound
• CT
• Isotope scanning
• MRI
• Hepatic angiography
• Splenic and arterial
The techniques available include:
• Simple X ray
• Ultra sound
• CT
• Isotope scanning
• MRI
• Hepatic angiography
• Splenic and arterial
Simple X ray provides little information apart from the confirming enlargement
Simple X ray provides little information apart from the confirming enlargement
Indications are:
the liver cysts
abscess
Hematomas
and neoplasm both primary and
Indications are:
the liver cysts
abscess
Hematomas
and neoplasm both primary and
Tumors usually show as rounded areas with diminished echoes.
Cysts are
Tumors usually show as rounded areas with diminished echoes.
Cysts are
tumor
tumor


CT scanning
CT shows the liver in axial sections with high resolution.
Primary
CT scanning
CT shows the liver in axial sections with high resolution.
Primary

cyst
cyst

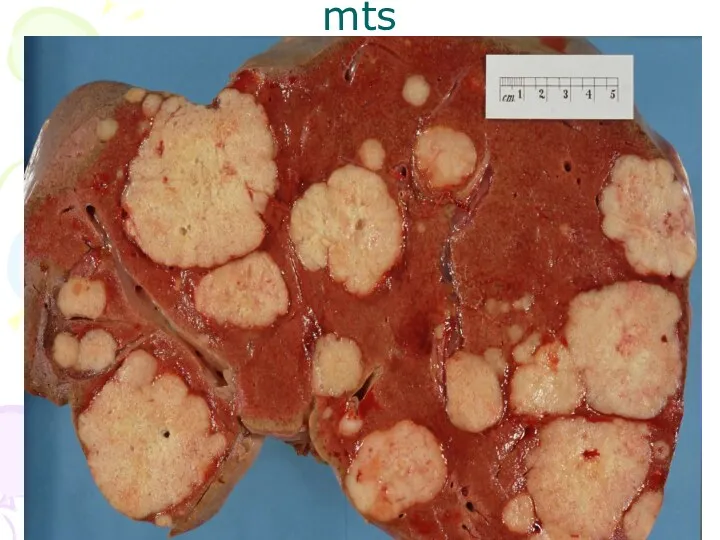
mts
mts

stone
stone
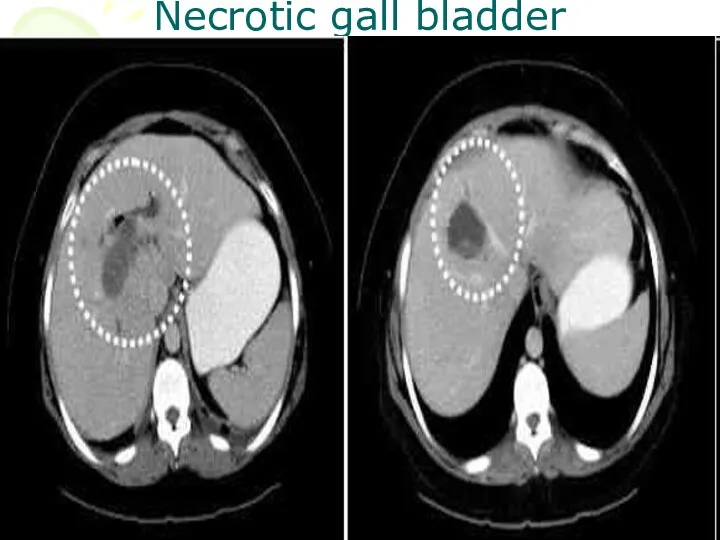
Necrotic gall bladder
Necrotic gall bladder
MRI
MRI is similar to CT in the accuracy of showing focal
MRI
MRI is similar to CT in the accuracy of showing focal
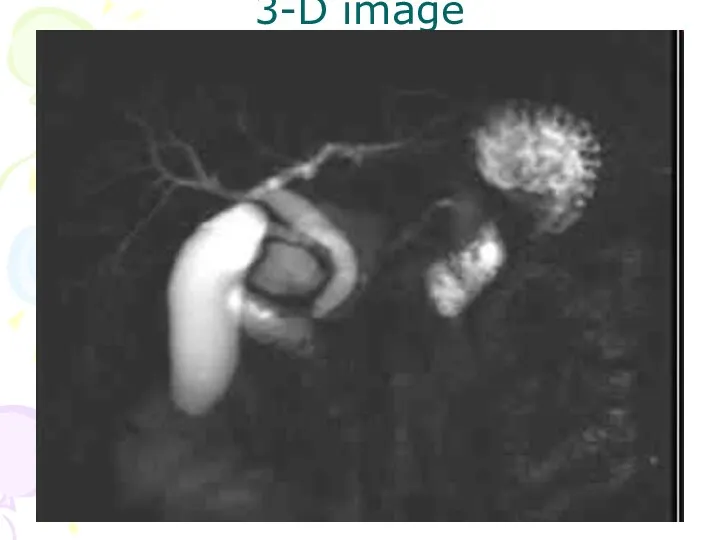
3-D image
3-D image
Angiography
Hepatic angiography is performed by percutaneous transfemoral catheterization of the coeliac
Angiography
Hepatic angiography is performed by percutaneous transfemoral catheterization of the coeliac
The technique uses:
for the diagnosis of tumors
angiomas
aneurysms
and other vascular lesions
for the
The technique uses:
for the diagnosis of tumors
angiomas
aneurysms
and other vascular lesions
for the
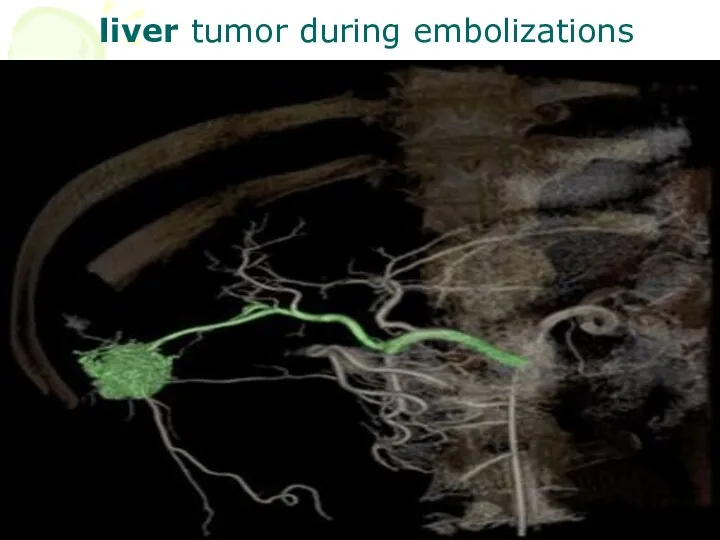
liver tumor during embolizations
liver tumor during embolizations
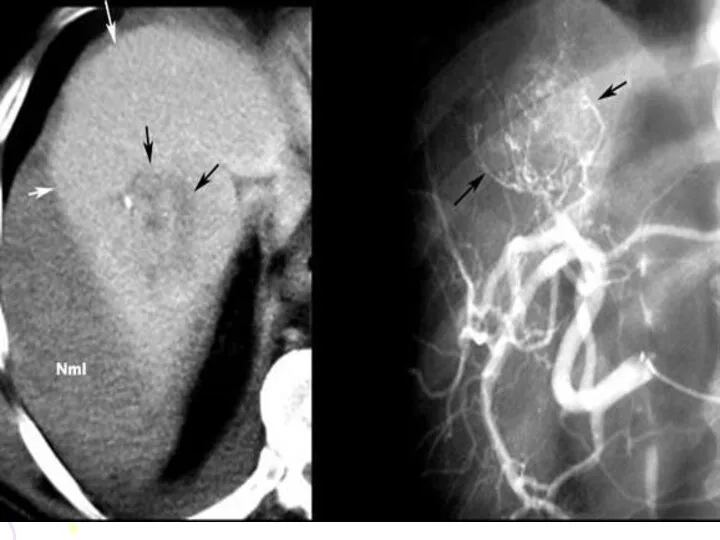

hemangioma
hemangioma
Isotope scanning
The study is usually performed 15-30 minutes after injection with
Isotope scanning
The study is usually performed 15-30 minutes after injection with
Following are the indications of liver imaging:
• Evaluation of the liver
Following are the indications of liver imaging:
• Evaluation of the liver
CHOICE OF EXAMINATION IN BILIARY AND LIVER DISEASE
Suspected liver masses (tumors,
CHOICE OF EXAMINATION IN BILIARY AND LIVER DISEASE
Suspected liver masses (tumors,
CT and MRI will also perform this function but are more
CT and MRI will also perform this function but are more
In suspected obstructive jaundice, ultrasound is the primary investigation of choice,
In suspected obstructive jaundice, ultrasound is the primary investigation of choice,
PANCREAS
Pancreas lies in the posterior abdominal wall in the epigastrium and
PANCREAS
Pancreas lies in the posterior abdominal wall in the epigastrium and
Simple X ray will occasionally show extensive nodules of calcification in
Simple X ray will occasionally show extensive nodules of calcification in

Barium studies will show:
distortion of the duodenal loop by masses in
Barium studies will show:
distortion of the duodenal loop by masses in


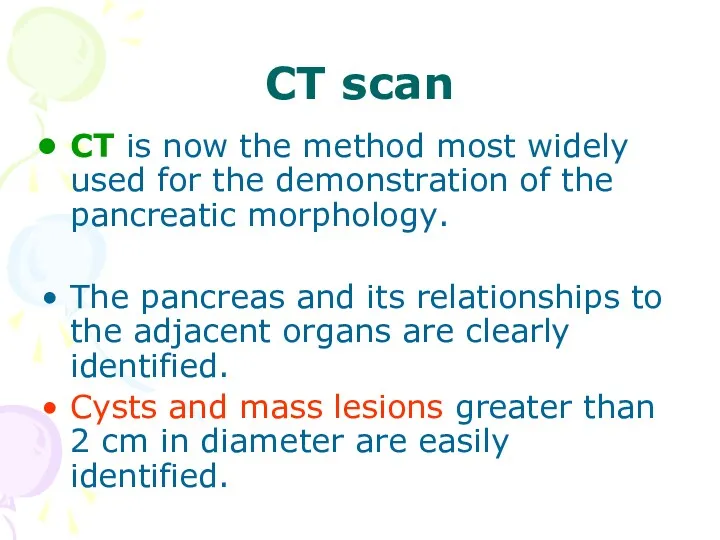
Ultrasound: the normal pancreas may be partly obscured by bowel gas
In acute pancreatitis, the whole organ is enlarged and edematous
In acute pancreatitis, the whole organ is enlarged and edematous
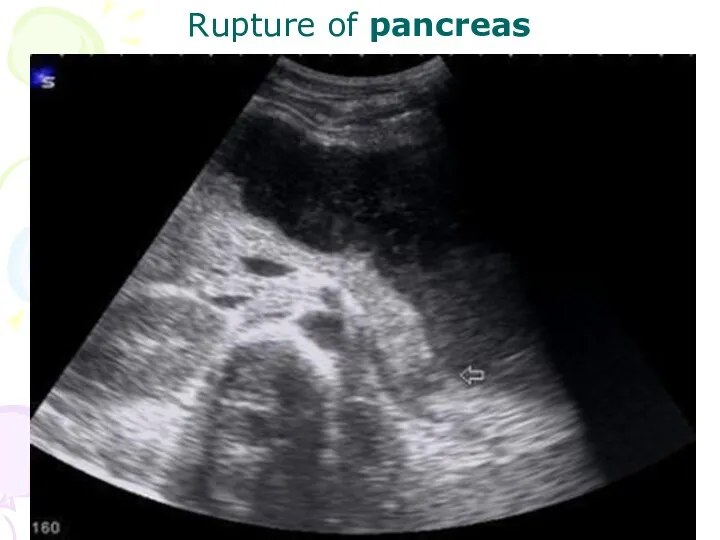
Rupture of pancreas
Rupture of pancreas
CT scan
CT is now the method most widely used for the
CT scan
CT is now the method most widely used for the
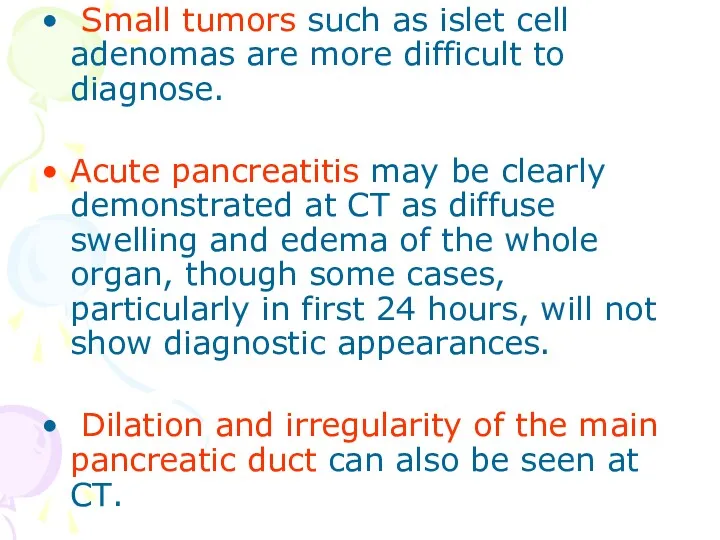
Small tumors such as islet cell adenomas are more difficult
Small tumors such as islet cell adenomas are more difficult
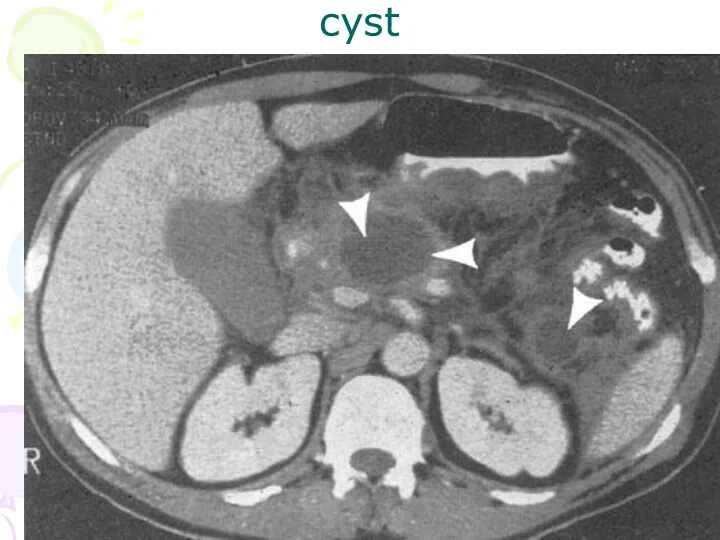
cyst
cyst
MRI
MRI can also show the pancreas well but has no advantage
MRI
MRI can also show the pancreas well but has no advantage
ERCP
ERCP is the method of choice for demonstrating the pancreatic
ERCP
ERCP is the method of choice for demonstrating the pancreatic
These include:
1. Stone extraction from pancreatic and bile ducts
2. Sphincterectomy
3. Biopsy of ampulla
4. Cytology of
These include:
1. Stone extraction from pancreatic and bile ducts
2. Sphincterectomy
3. Biopsy of ampulla
4. Cytology of
Choice of examination
CT is probably the best method for speedy demonstration
Choice of examination
CT is probably the best method for speedy demonstration
 Бронхиальная астма
Бронхиальная астма Феохромоцитома. Симптомы. Диагностика
Феохромоцитома. Симптомы. Диагностика Нарушение кровообращения. Лекция
Нарушение кровообращения. Лекция Пневмония. Клинико-этиологическая классификация пневмонии
Пневмония. Клинико-этиологическая классификация пневмонии История отечественного здравоохранения. Характеристика дисциплины Общественное здоровье и здравоохранение
История отечественного здравоохранения. Характеристика дисциплины Общественное здоровье и здравоохранение Позвоночник. Грудная клетка
Позвоночник. Грудная клетка Менопаузадан кейін сүт безі ісігінің жоғары қаупін алдын алу үшін көк шай пайдалану
Менопаузадан кейін сүт безі ісігінің жоғары қаупін алдын алу үшін көк шай пайдалану Психофизиология эмоций
Психофизиология эмоций Особливості туберкульозу у ВІЛ-інфікованих і хворих на СНІД
Особливості туберкульозу у ВІЛ-інфікованих і хворих на СНІД Научные работы в области косноязычия (А. Куссмауль), афазиологии (Либман, К. Вернике и другие)
Научные работы в области косноязычия (А. Куссмауль), афазиологии (Либман, К. Вернике и другие) Хронический панкреатит. Хронический холецистит
Хронический панкреатит. Хронический холецистит Острый аппендицит
Острый аппендицит Тиреотоксикоз жаңа туған балалардан бастап
Тиреотоксикоз жаңа туған балалардан бастап Arodmedicīna. Darba higiēna, vides medicīna
Arodmedicīna. Darba higiēna, vides medicīna Трансплантология. Тіндерді қондырудың биологиялық жағдайлары. Ағзаларды қондыру. Иммунодепрессивті әсері бар дәрілерді қолдану
Трансплантология. Тіндерді қондырудың биологиялық жағдайлары. Ағзаларды қондыру. Иммунодепрессивті әсері бар дәрілерді қолдану Хронический лимфолейкоз
Хронический лимфолейкоз Профилактика гриппа и коронавирусной инфекции. Короновирус под микроскопом
Профилактика гриппа и коронавирусной инфекции. Короновирус под микроскопом Ана сүтімен қоректендірудің маңызы
Ана сүтімен қоректендірудің маңызы Иммунобиологические лекарственные препараты
Иммунобиологические лекарственные препараты Психические и поведенческие расстройства, вызванные употреблением опиоидов
Психические и поведенческие расстройства, вызванные употреблением опиоидов Ангины. Виды ангин
Ангины. Виды ангин Нейротропные АГС центрального действия. Локализация и механизм антигипертензивного действия
Нейротропные АГС центрального действия. Локализация и механизм антигипертензивного действия Общественное здоровье. Основные понятия. (Лекция 2)
Общественное здоровье. Основные понятия. (Лекция 2) Реабилитация больных с заболеваниями ЖКТ
Реабилитация больных с заболеваниями ЖКТ Зрительные вызванные потенциалы
Зрительные вызванные потенциалы Астмалық статус
Астмалық статус Мұрыннан қан кету
Мұрыннан қан кету Қария науқастардың күтімі
Қария науқастардың күтімі