Importance of tuberculosis as scientific and practical problem. Tuberculosis epidemiology in the world. (Lecture 1) презентация
- Importance of tuberculosis as scientific and practical problem. Tuberculosis epidemiology in the world. (Lecture 1)

Содержание
- 2. Tuberculosis is defined as an infectious disease caused by a bacterium; that most commonly affects the
- 3. These numbers are expected to increase in the coming years because of the acquired immune deficiency
- 4. People who have healthy immune systems can often fight off a tuberculosis infection after breathing in
- 5. The magnitude of the problem: Tuberculosis kills more than 3 million people per year Tuberculosis produces
- 6. Tuberculosis uniqueness: the most ancient among known infection the most ubiquitous infection infection which can coexist
- 7. Main reasons for tuberculosis reappearance as a global challenge: Drug-resistance Human immunodeficiency virus (HIV) Social disturbances
- 8. EPIDEMIOLOGY
- 10. 5 PRIORITIES TO ELIMINATE TB Reaching the “missed” cases (3 million not in the system) Address
- 11. Reaching the "missed" cases early means cutting transmission Share of total missed cases
- 12. Addressing MDR-TB as a crisis Percentage of new TB cases with MDR-TB
- 13. Five priority actions to address the global MDR-TB crisis
- 14. Accelerating response to TB/HIV means cutting transmission and mortality Estimated HIV prevalence in new TB cases,
- 15. 67th World Health Assembly, Geneva, May 2014
- 16. The End TB Strategy – Components 1. INTEGRATED, PATIENT-CENTRED CARE AND PREVENTION A. Early diagnosis of
- 17. 2. BOLD POLICIES AND SUPPORTIVE SYSTEMS A. Political commitment with adequate resources for tuberculosis care and
- 18. Mycobacteria types M. causing tuberculosis M. tuberculosis (human) M. bovis. M. Africans. Non-patogenous M. M.avium-intracellulare. M.smegmaticus.
- 19. Important Mycobacterium Mycobacterium tuberculosis, along with M. bovis, M. africanum, and M. microti all cause the
- 20. The Causative agent of tuberculosis is opened by R. Kokh on March, 24, 1892
- 21. Morphology of Mycobacterium tuberculosis Straight, slightly curved Rod shaped 3 x 0.3microns May be single, in
- 22. Atypical Mycobacterium Photochromogens Scotochromogens Non Photochromogens Rapid growers
- 23. The lungs are the basic organs affected by tuberculosis. The lungs are comprised of lobes. The
- 24. Each lung segment contains a bronchus and artery that are almost arranged in a parallel order.
- 25. Bronchial Airways The two bronchi proceed from the bifurcation of the trachea opposite to the 4-th
- 26. The structure of the lung parenchyma The finniest, independent functional unit of the lung parenchyma is
- 27. Pleura Each lung is enclosed and its structure supported by a serous membrane, the pleura, which
- 28. The lymphatic lung system The lung surface is formed of a thin sub-pleural network of lymphatic
- 29. Transmission of tuberculosis TB is spread from person to person through the air. The dots in
- 30. The ways of the transmission: Inhalation (about 90%) Dusty Droplet Alimentary Contact Vertical
- 31. Factors that determine the probability of transmission of M. Tuberculosis
- 32. Characteristics of a patient with TB disease that are associated with Infectiousness
- 33. Proximity and length of exposure factors that can affect transmission of M. Tuberculosis
- 34. Pathogenesis of TB Droplet nuclei containing tubercle bacilli are inhaled, enter the lungs, and travel to
- 35. Tubercle bacilli multiply in the alveoli.
- 36. A small number of tubercle bacilli enter the bloodstream and spread throughout the body. The tubercle
- 37. Within 2 to 8 weeks, special immune cells called macrophages ingest and surround the tubercle bacilli.
- 38. If the immune system cannot keep the tubercle bacilli under control, the bacilli begin to multiply
- 39. Latent Tuberculosis Infection (LTBI) Persons with LTBI have M. tuberculosis in their bodies, but do not
- 40. TB Disease In some people, the tubercle bacilli overcome the immune system and multiply, resulting in
- 41. Risk of developing TB disease over a lifetime Without treatment, approximately 5% of persons who have
- 42. Risk of LTBI Progressing to TB Disease Anyone who has LTBI can develop TB disease, but
- 43. Persons at Increased Risk for Progression of LTBI to TB Disease
- 44. The tubercular inflammation The tubercular inflammation, like any other inflammation is a manifestation of alteration, exudation,
- 45. Participate in the formation of tubercular granuloma hematogenic elements (lymphocytes, monocytes, polymorphonuclear leucocytes), histiogenic elements (histocytes,
- 46. The tubercular granuloma has the following structure: The center consists of amorphous tissue detritus (due to
- 47. Diagram of a Granuloma NOTE: ultimately a fibrin layer develops around granuloma (fibrosis), further “walling off”
- 49. The tuberculum histogenesis depends on the development of the inflammation process, which is either progressive or
- 50. Various foci of different sizes of cheesy necrosis arise during the further progression of specific tubercular
- 51. The particular danger is represented by vascular blood erosion supplying sites of lungs where caseous degeneration
- 52. The morphological and biochemical components of microbial cells cause various reactions in the host. The basic
- 53. Delayed-type hypersensitivity (DTH) The substances, which are included in the MBT wall structure, induce tissue specific
- 54. In general, term DTH is used for characteristics of a type IV immune response (induration at
- 55. The cycle of tuberculosis development from MBT contamination till the occurrence of its clinical manifestations and
- 56. Primary tuberculosis Primary tuberculosis develops after the first contact of macroorganism with MBT. MBT fill in
- 57. In the primary lung focus, alveolitis develops, which is quickly replaced by the typical development of
- 58. Perifocal inflammation around the lymph nodes will spread in the mediastinum and surround the lung tissues.
- 59. The dynamic study of primary pulmonary processes among children has allowed to allot 4 phases of
- 60. phase 1 (pneumonic) In the first phase (pneumatic) the focus of broncho-lobular pneumonia (3) is determined
- 61. phase 2 of dissolving (bipolarity) In the second phase of dissolving (bipolarity) the reduction of the
- 62. the phase 3 – condensation In the third phase, the phase of condensation: the primary focus
- 63. phase 4 formation of Gohn’s focus In the fourth phase, in the place of broncho-lobular pneumonia
- 64. Outcomes of the primary tubercular complex may be in the following way: 1) healing with encapsulation,
- 65. There are 2 types of generalization of the tubercular complex progression: 1) hematogenic; 2) lymphogenic 3)
- 66. At progression of hematogenous disseminated tuberculosis the cavities are formed. The formation of cavities is the
- 67. Immunity at tuberculosis Natural resistance to tuberculosis is inherited. It involves non-specific antimicrobial humoral factors (non-immunological
- 68. Phagocytosis plays special role in natural resistance. Primary contact MBT and the host triggers phagocytosis of
- 69. Fagocitosis Completed phagocytosis Uncompleted phagocytosis It is one of mechanisms The result of him is education
- 70. Results of phagocytosis
- 71. Immunity in tuberculosis consists from five basic reactions: cell reaction, humoral factor, allergy, immune memory and
- 72. Only under these conditions T-helper (CD4+) may recognize antigen peptide of MBT. - At the same
- 73. Proof of the role of T- lymphocytes in anti-tubercular immunity: injection of T- lymphocytes suspension from
- 74. As immune response builds up multiplication of Mycobacteria slows down, their general number decreases, as specific
- 75. Remaining MBT are located within cells and prevent formation of phagolysosome, thus becoming inaccessible to enzymes
- 77. Скачать презентацию
Tuberculosis is defined as an infectious disease caused by a bacterium;
Tuberculosis is defined as an infectious disease caused by a bacterium;
These numbers are expected to increase in
the coming years because of
These numbers are expected to increase in
the coming years because of
People who have healthy immune systems can often fight off a
People who have healthy immune systems can often fight off a
The magnitude of the problem:
Tuberculosis kills more than 3 million people
The magnitude of the problem:
Tuberculosis kills more than 3 million people
Tuberculosis uniqueness:
the most ancient among known infection
the most ubiquitous infection
infection
Tuberculosis uniqueness:
the most ancient among known infection
the most ubiquitous infection
infection
Main reasons for tuberculosis reappearance as a global challenge:
Drug-resistance
Human immunodeficiency virus
Main reasons for tuberculosis reappearance as a global challenge:
Drug-resistance
Human immunodeficiency virus
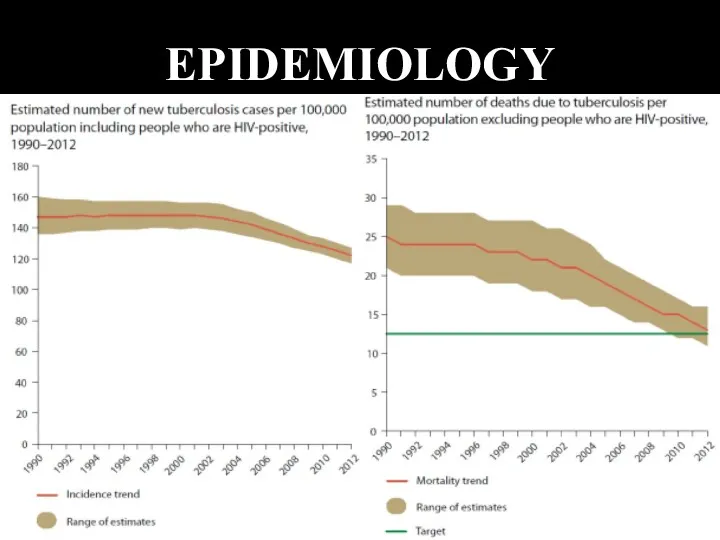
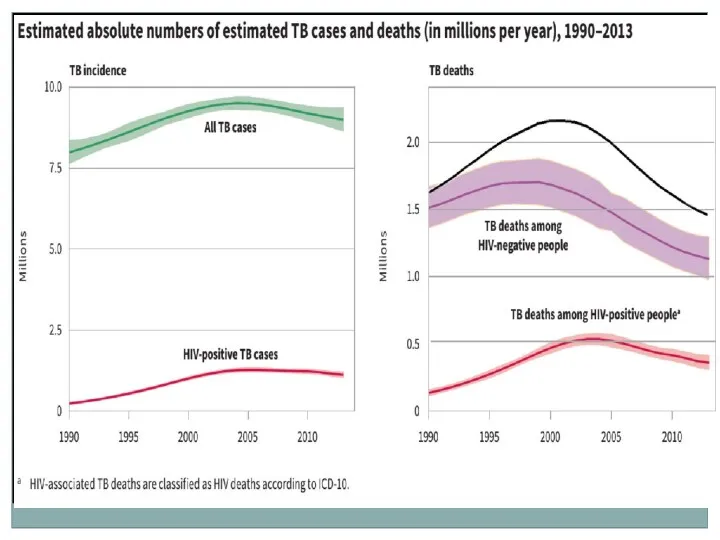
EPIDEMIOLOGY
EPIDEMIOLOGY
5 PRIORITIES TO ELIMINATE TB
Reaching the “missed” cases (3 million
5 PRIORITIES TO ELIMINATE TB
Reaching the “missed” cases (3 million
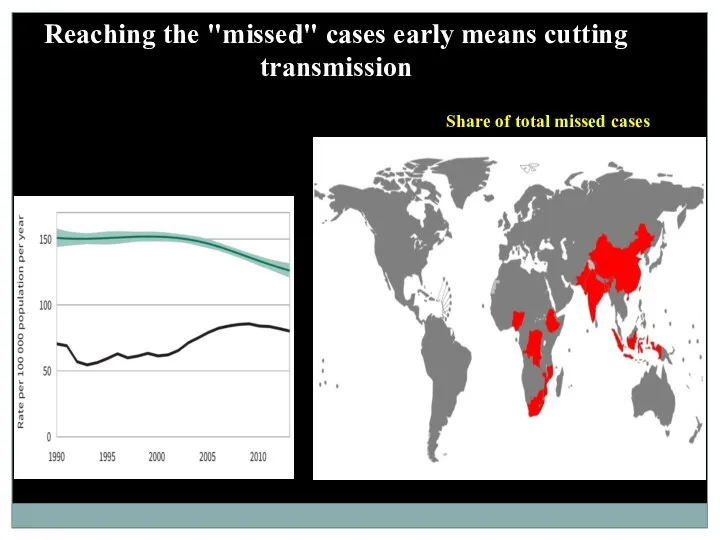
Reaching the "missed" cases early means cutting transmission
Share of total missed
Reaching the "missed" cases early means cutting transmission
Share of total missed
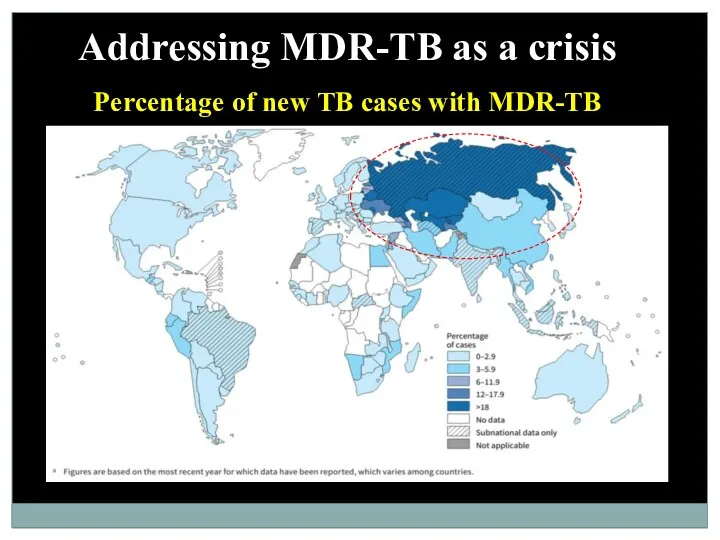
Addressing MDR-TB as a crisis
Percentage of new TB cases with MDR-TB
Addressing MDR-TB as a crisis
Percentage of new TB cases with MDR-TB
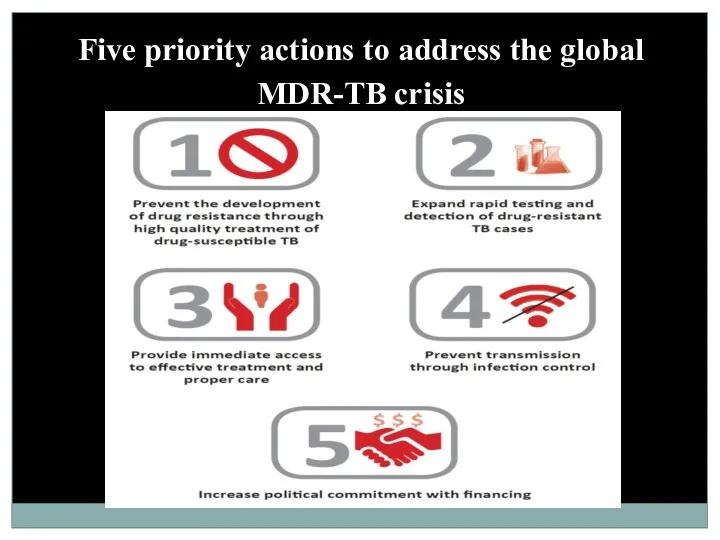
Five priority actions to address the global MDR-TB crisis
Five priority actions to address the global MDR-TB crisis
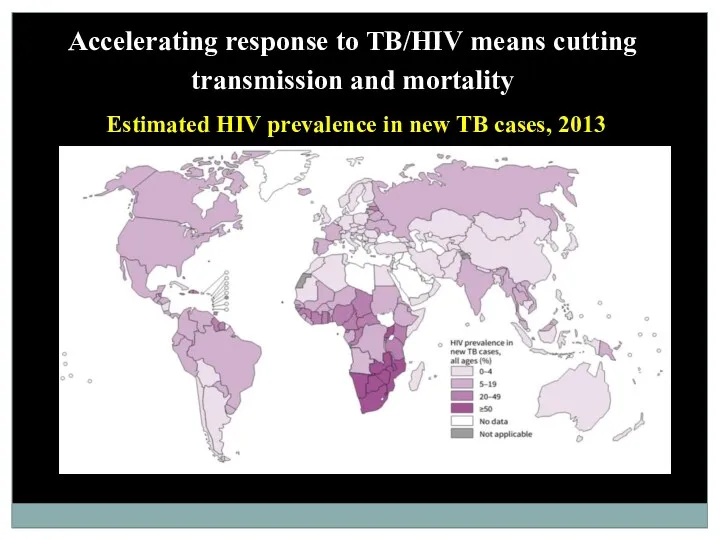
Accelerating response to TB/HIV means cutting transmission and mortality
Estimated HIV prevalence
Accelerating response to TB/HIV means cutting transmission and mortality
Estimated HIV prevalence
67th World Health Assembly, Geneva, May 2014
67th World Health Assembly, Geneva, May 2014
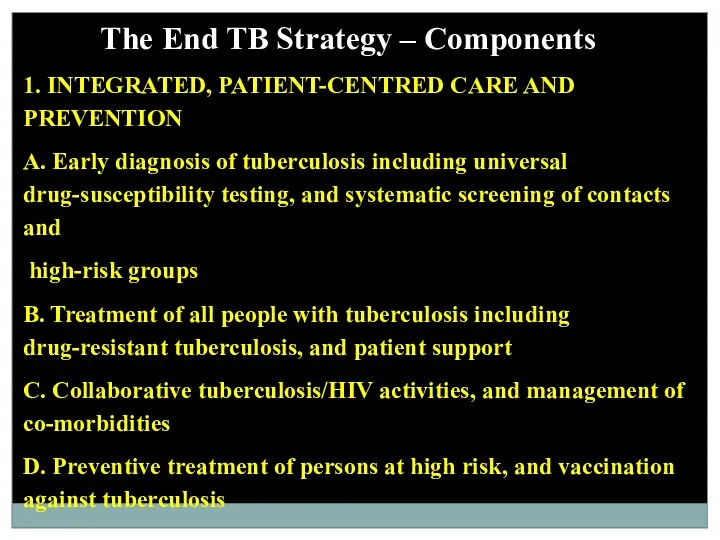
The End TB Strategy – Components
1. INTEGRATED, PATIENT-CENTRED CARE AND PREVENTION
A.
The End TB Strategy – Components
1. INTEGRATED, PATIENT-CENTRED CARE AND PREVENTION
A.
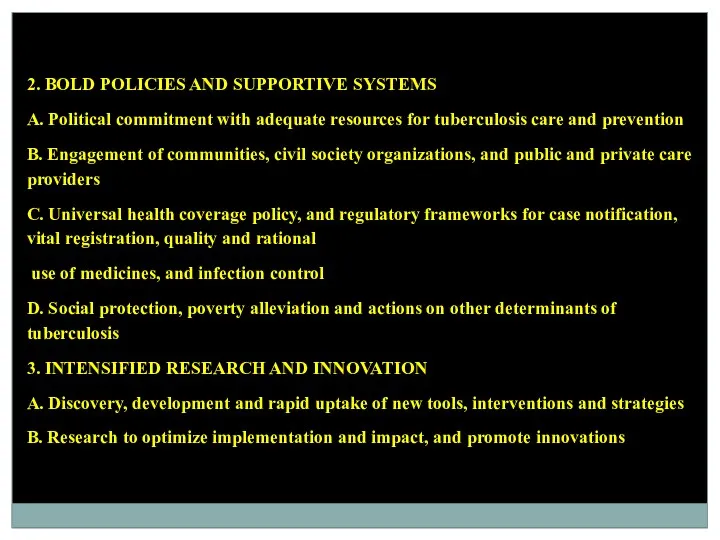
2. BOLD POLICIES AND SUPPORTIVE SYSTEMS
A. Political commitment with adequate resources
2. BOLD POLICIES AND SUPPORTIVE SYSTEMS
A. Political commitment with adequate resources
Mycobacteria types
M. causing tuberculosis
M. tuberculosis (human)
M. bovis.
M. Africans.
Non-patogenous M.
M.avium-intracellulare.
M.smegmaticus.
M. xenopi
M. scrofulaceum.
M.
Mycobacteria types
M. causing tuberculosis
M. tuberculosis (human)
M. bovis.
M. Africans.
Non-patogenous M.
M.avium-intracellulare.
M.smegmaticus.
M. xenopi
M. scrofulaceum.
M.
Important Mycobacterium
Mycobacterium tuberculosis, along with M. bovis, M. africanum, and M.
Important Mycobacterium
Mycobacterium tuberculosis, along with M. bovis, M. africanum, and M.
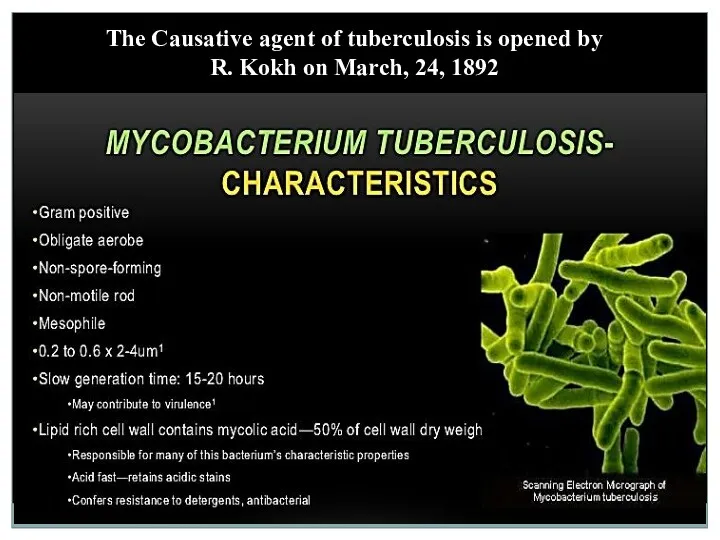
The Causative agent of tuberculosis is opened by
R. Kokh on
The Causative agent of tuberculosis is opened by
R. Kokh on
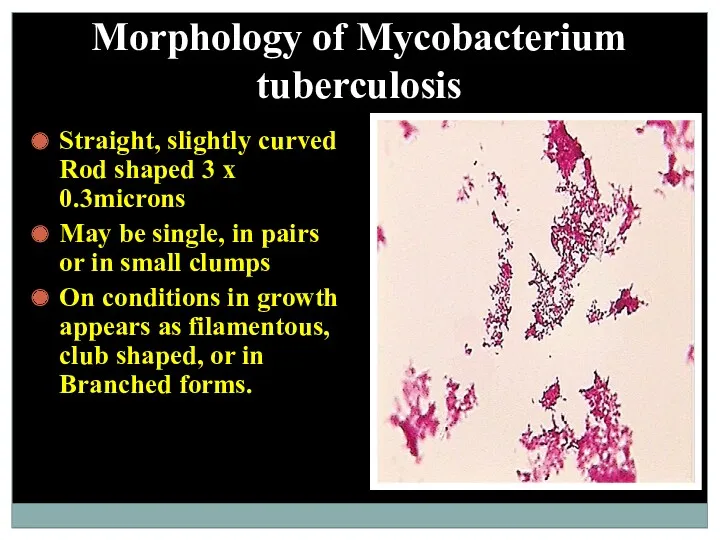
Morphology of Mycobacterium tuberculosis
Straight, slightly curved Rod shaped 3 x 0.3microns
May
Morphology of Mycobacterium tuberculosis
Straight, slightly curved Rod shaped 3 x 0.3microns
May
Atypical Mycobacterium
Photochromogens
Scotochromogens
Non Photochromogens
Rapid growers
Atypical Mycobacterium
Photochromogens
Scotochromogens
Non Photochromogens
Rapid growers
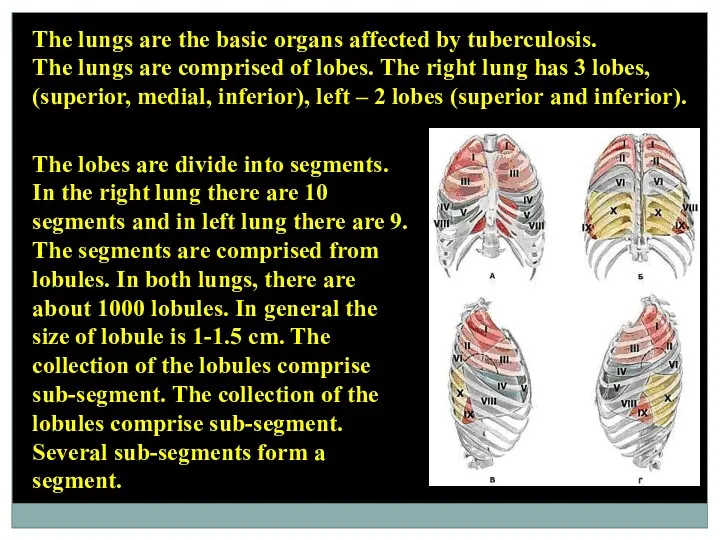
The lungs are the basic organs affected by tuberculosis.
The lungs are
The lungs are the basic organs affected by tuberculosis.
The lungs are
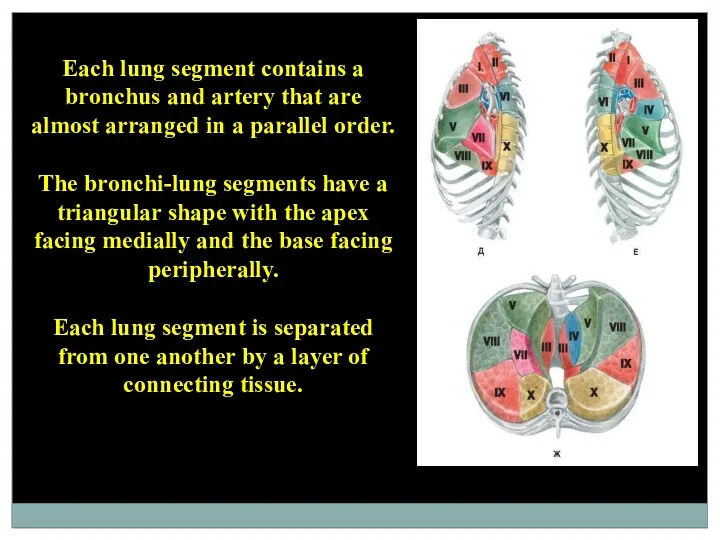
Each lung segment contains a bronchus and artery that are almost
Each lung segment contains a bronchus and artery that are almost
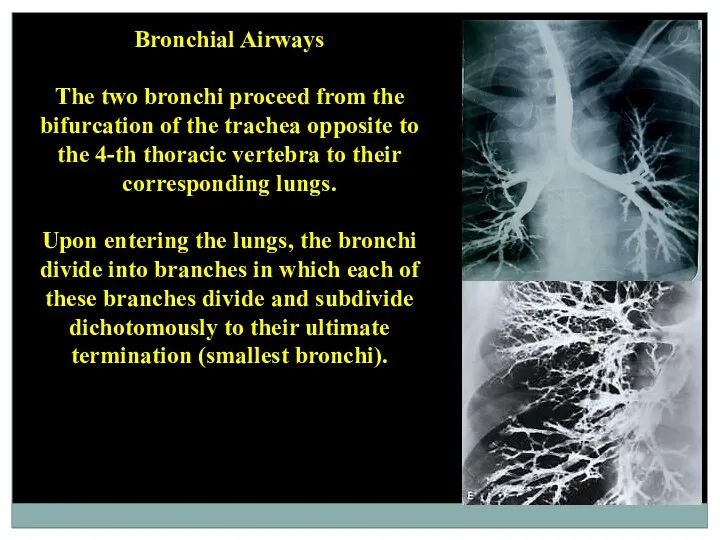
Bronchial Airways
The two bronchi proceed from the bifurcation of the
Bronchial Airways
The two bronchi proceed from the bifurcation of the
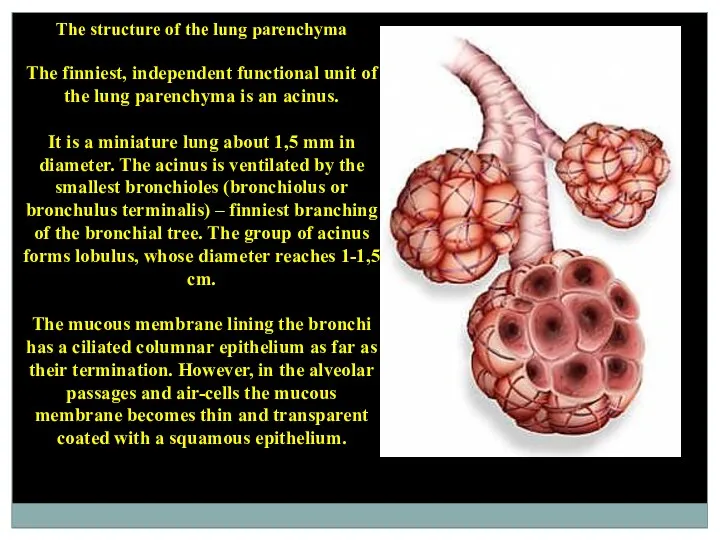
The structure of the lung parenchyma
The finniest, independent functional unit
The structure of the lung parenchyma
The finniest, independent functional unit
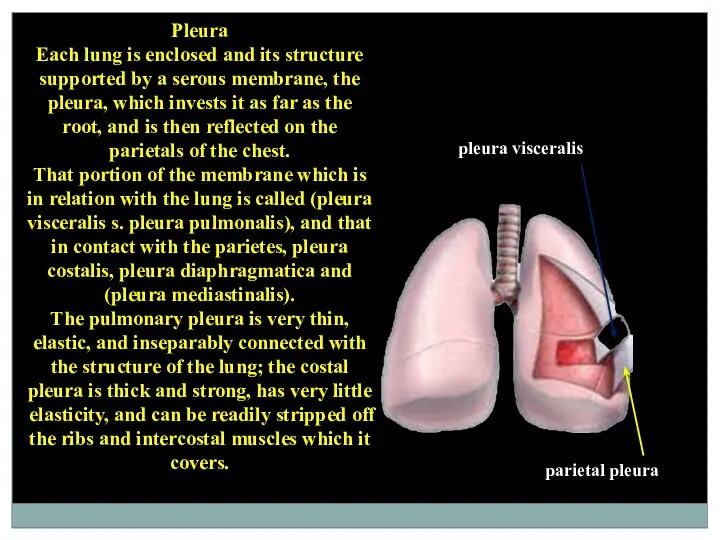
Pleura
Each lung is enclosed and its structure supported by a
Pleura
Each lung is enclosed and its structure supported by a
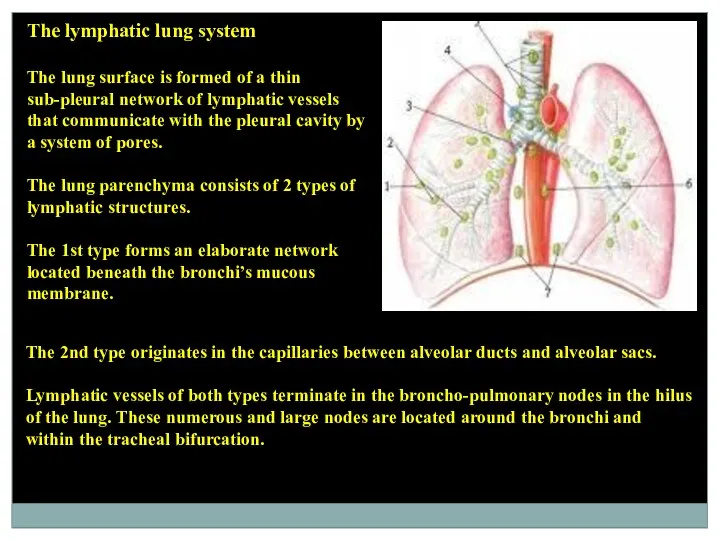
The lymphatic lung system
The lung surface is formed of a
The lymphatic lung system
The lung surface is formed of a
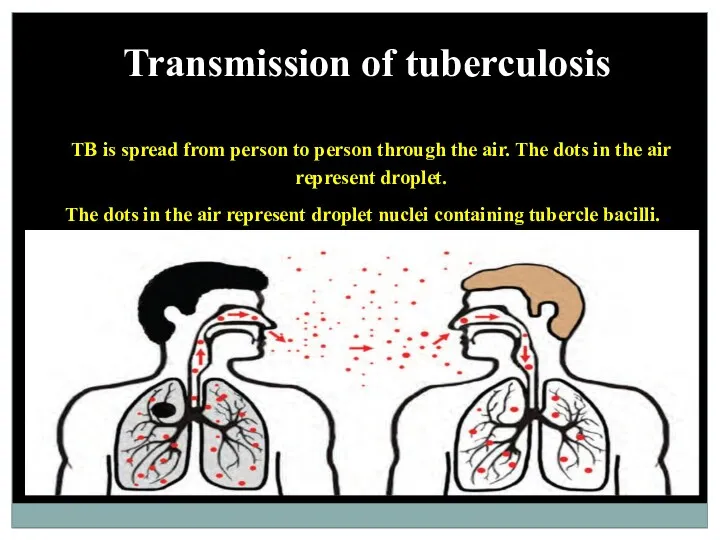
Transmission of tuberculosis
TB is spread from person to person through the
Transmission of tuberculosis
TB is spread from person to person through the
The ways of the transmission:
Inhalation (about 90%)
Dusty
Droplet
Alimentary
Contact
Vertical
The ways of the transmission:
Inhalation (about 90%)
Dusty
Droplet
Alimentary
Contact
Vertical
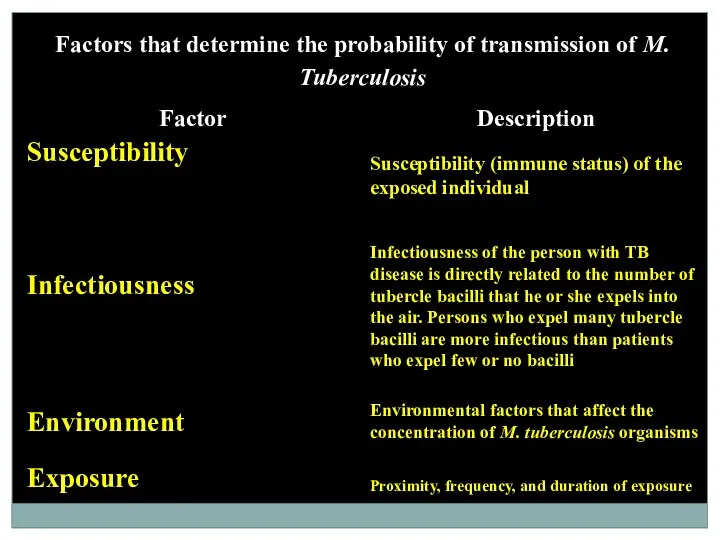
Factors that determine the probability of transmission of M. Tuberculosis
Factors that determine the probability of transmission of M. Tuberculosis
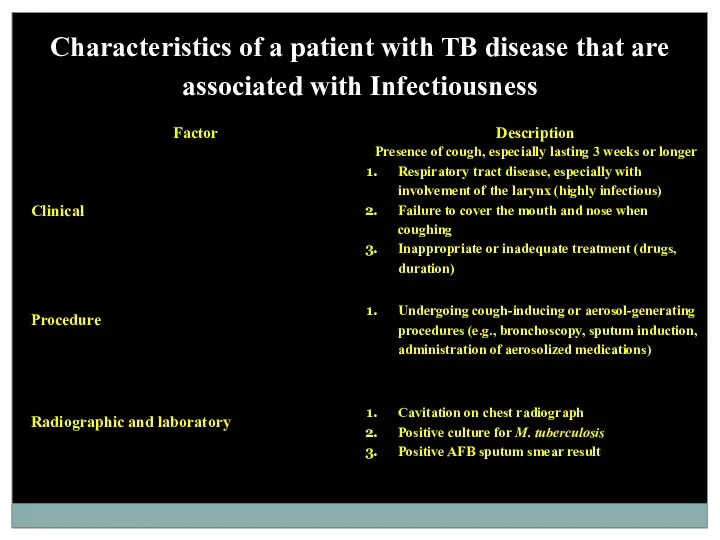
Characteristics of a patient with TB disease that are associated with
Characteristics of a patient with TB disease that are associated with
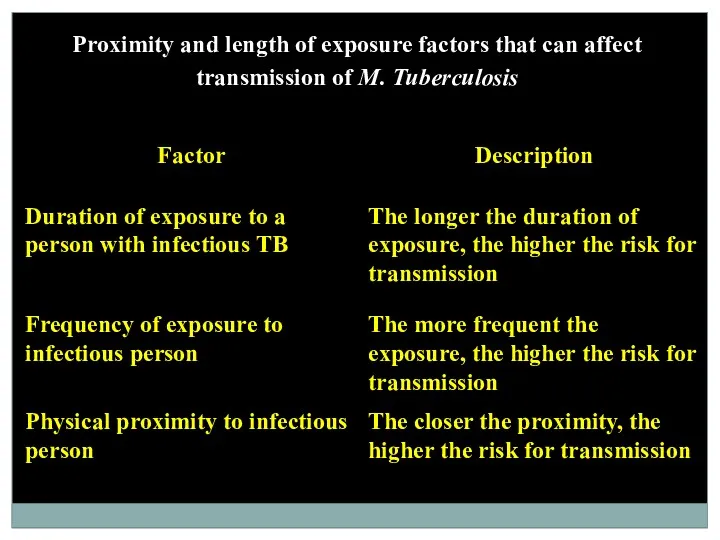
Proximity and length of exposure factors that can affect transmission of
Proximity and length of exposure factors that can affect transmission of
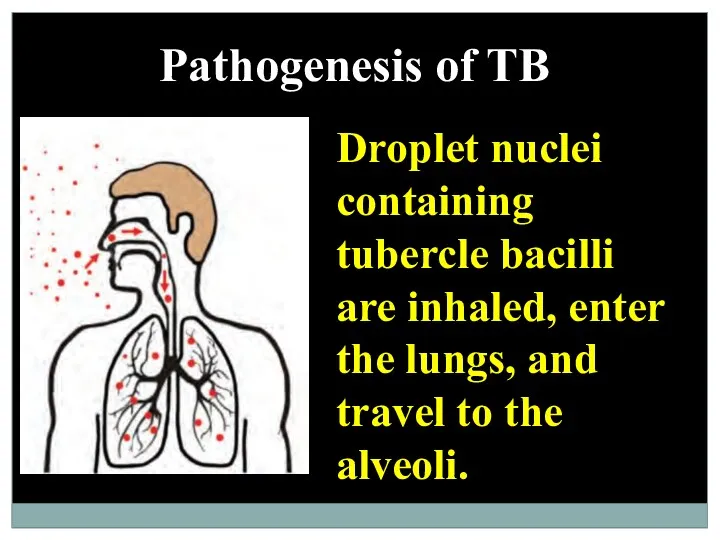
Pathogenesis of TB
Droplet nuclei containing tubercle bacilli are inhaled, enter the
Pathogenesis of TB
Droplet nuclei containing tubercle bacilli are inhaled, enter the
Tubercle bacilli multiply in the alveoli.
Tubercle bacilli multiply in the alveoli.
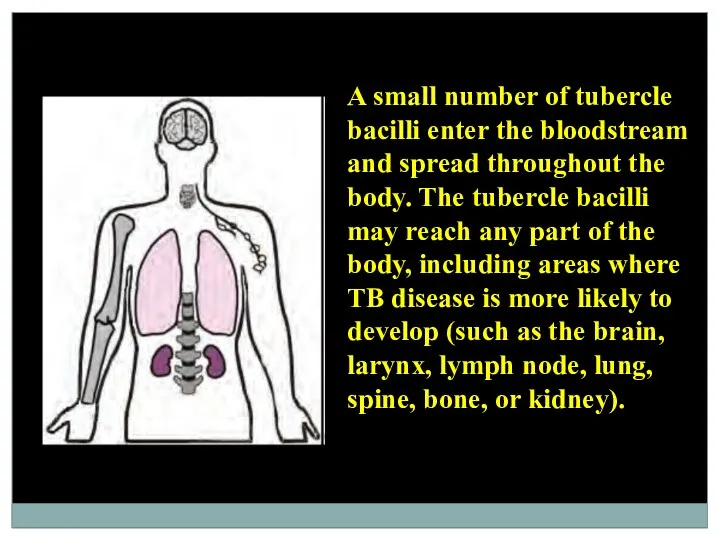
A small number of tubercle bacilli enter the bloodstream and spread
A small number of tubercle bacilli enter the bloodstream and spread
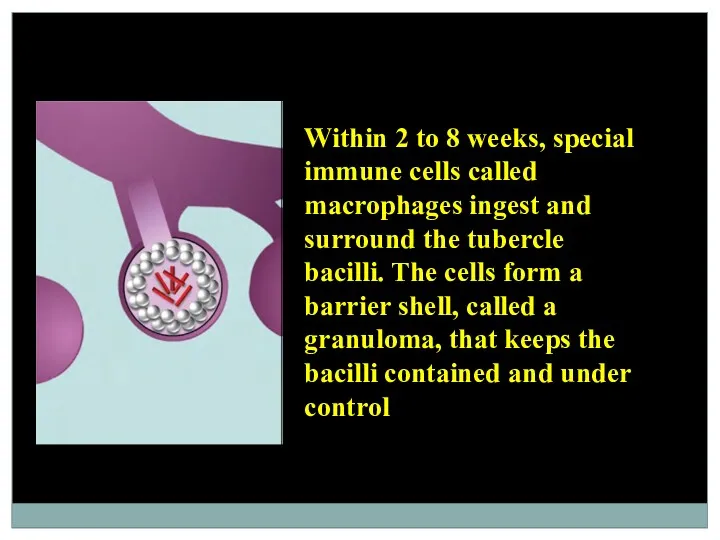
Within 2 to 8 weeks, special immune cells called macrophages ingest
Within 2 to 8 weeks, special immune cells called macrophages ingest
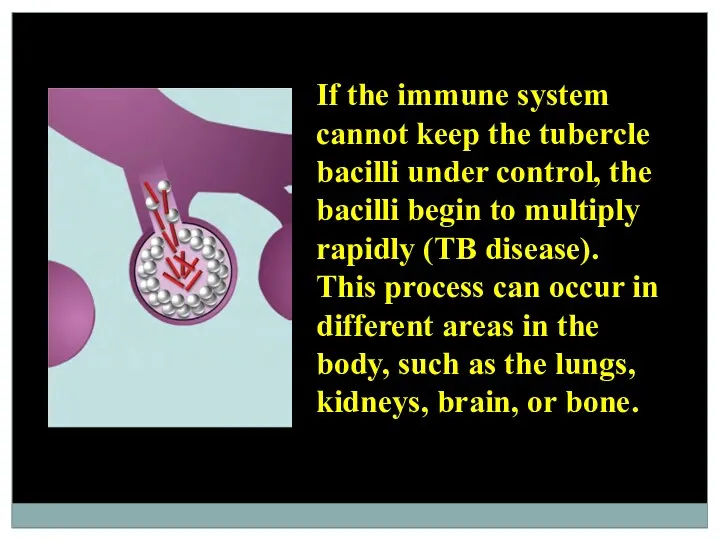
If the immune system cannot keep the tubercle bacilli under control,
If the immune system cannot keep the tubercle bacilli under control,
Latent Tuberculosis Infection (LTBI)
Persons with LTBI have M. tuberculosis in their
Latent Tuberculosis Infection (LTBI)
Persons with LTBI have M. tuberculosis in their
TB Disease
In some people, the tubercle bacilli overcome the immune system
TB Disease
In some people, the tubercle bacilli overcome the immune system
Risk of developing TB disease over a lifetime
Without treatment, approximately
Risk of developing TB disease over a lifetime
Without treatment, approximately
Risk of LTBI Progressing to TB Disease
Anyone who has LTBI can
Risk of LTBI Progressing to TB Disease
Anyone who has LTBI can
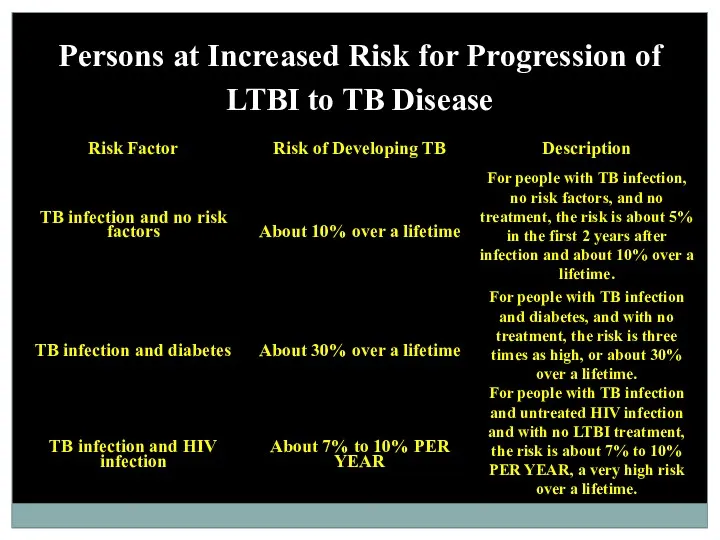
Persons at Increased Risk for Progression of LTBI to TB Disease
Persons at Increased Risk for Progression of LTBI to TB Disease
The tubercular inflammation
The tubercular inflammation, like any other inflammation is a
The tubercular inflammation
The tubercular inflammation, like any other inflammation is a
Participate in the formation of tubercular granuloma
hematogenic elements (lymphocytes, monocytes, polymorphonuclear
Participate in the formation of tubercular granuloma
hematogenic elements (lymphocytes, monocytes, polymorphonuclear
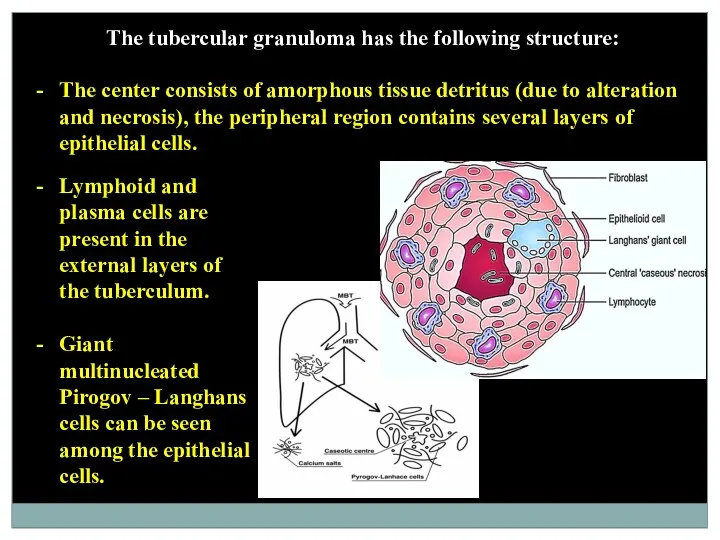
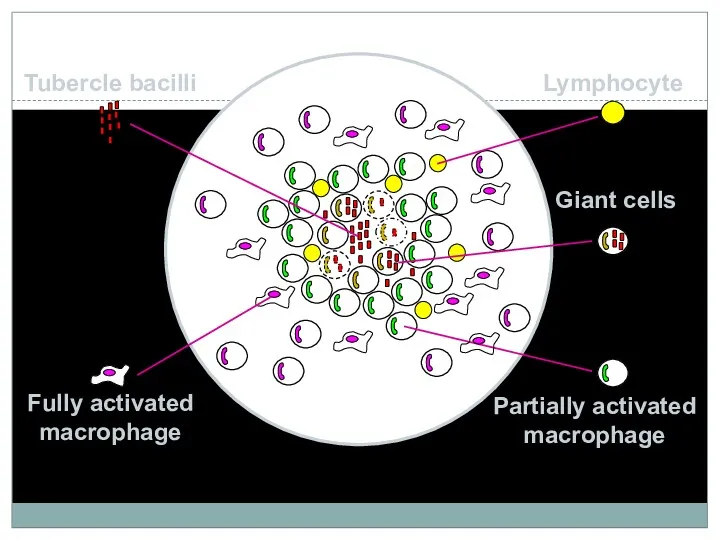
The tubercular granuloma has the following structure:
The center consists of amorphous
The tubercular granuloma has the following structure:
The center consists of amorphous
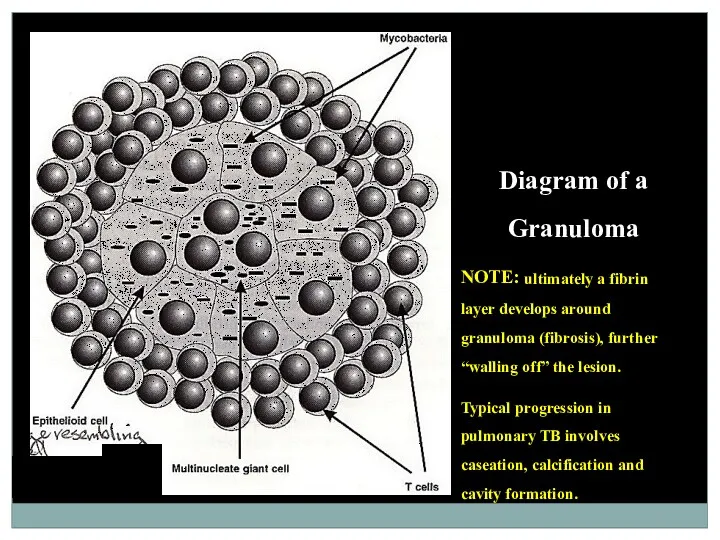
Diagram of a Granuloma
NOTE: ultimately a fibrin layer develops around granuloma
Diagram of a Granuloma
NOTE: ultimately a fibrin layer develops around granuloma
The tuberculum histogenesis depends on the development of the inflammation process,
The tuberculum histogenesis depends on the development of the inflammation process,
Various foci of different sizes of cheesy necrosis arise during the
Various foci of different sizes of cheesy necrosis arise during the
The particular danger is represented by vascular blood erosion supplying sites
The particular danger is represented by vascular blood erosion supplying sites
The morphological and biochemical components of microbial cells cause various reactions
The morphological and biochemical components of microbial cells cause various reactions
Delayed-type hypersensitivity (DTH)
The substances, which are included in the MBT wall
Delayed-type hypersensitivity (DTH)
The substances, which are included in the MBT wall
In general, term DTH is used for characteristics of a type
In general, term DTH is used for characteristics of a type
The cycle of tuberculosis development from MBT contamination till the occurrence
The cycle of tuberculosis development from MBT contamination till the occurrence
Primary tuberculosis
Primary tuberculosis develops after the first contact of macroorganism with
Primary tuberculosis
Primary tuberculosis develops after the first contact of macroorganism with
In the primary lung focus, alveolitis develops, which is quickly replaced
In the primary lung focus, alveolitis develops, which is quickly replaced
Perifocal inflammation around the lymph nodes will spread in the mediastinum
Perifocal inflammation around the lymph nodes will spread in the mediastinum
The dynamic study of primary pulmonary processes among children has allowed
The dynamic study of primary pulmonary processes among children has allowed
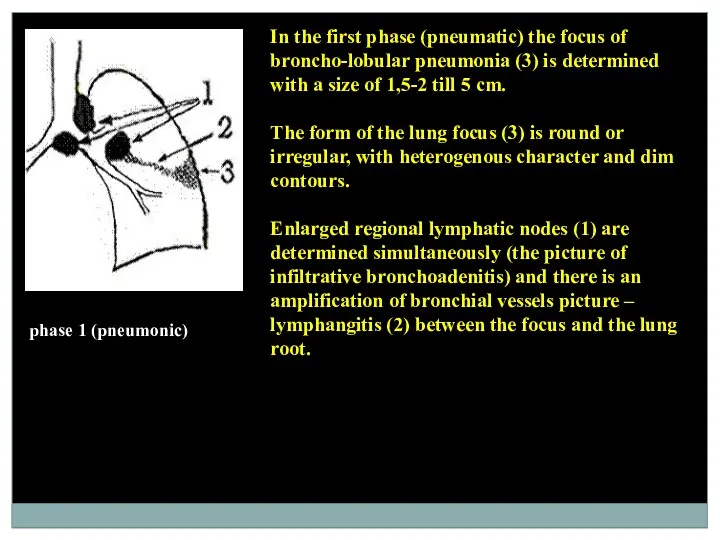
phase 1 (pneumonic)
In the first phase (pneumatic) the focus of broncho-lobular
phase 1 (pneumonic)
In the first phase (pneumatic) the focus of broncho-lobular
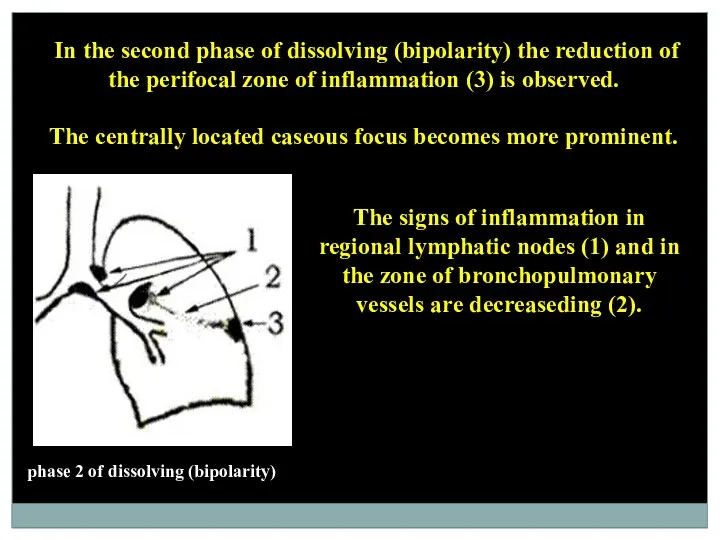
phase 2 of dissolving (bipolarity)
In the second phase of dissolving
phase 2 of dissolving (bipolarity)
In the second phase of dissolving
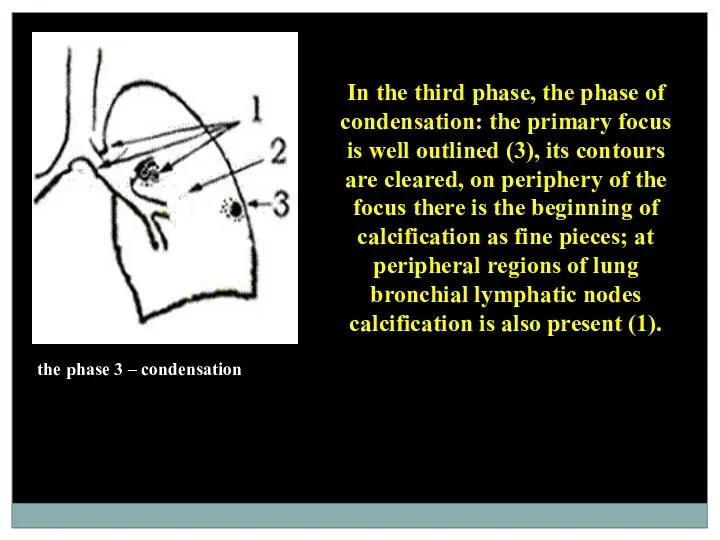
the phase 3 – condensation
In the third phase, the phase of
the phase 3 – condensation
In the third phase, the phase of
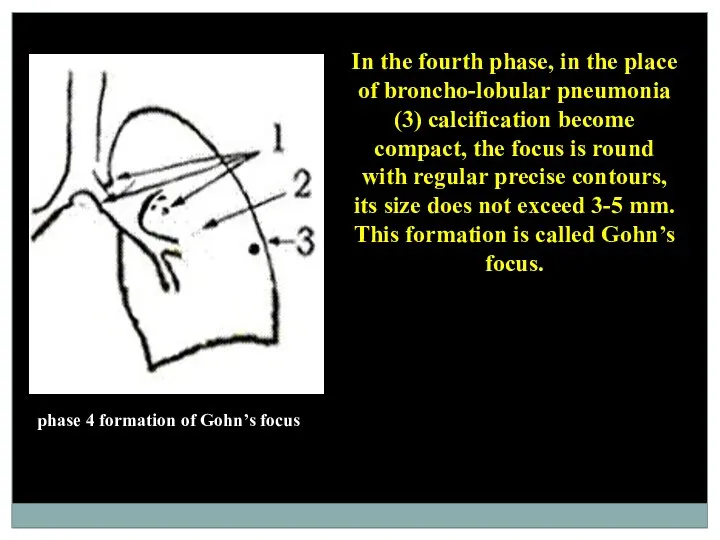
phase 4 formation of Gohn’s focus
In the fourth phase, in the
phase 4 formation of Gohn’s focus
In the fourth phase, in the
Outcomes of the primary tubercular complex may be in the following
Outcomes of the primary tubercular complex may be in the following
There are 2 types of generalization of the tubercular complex progression:
There are 2 types of generalization of the tubercular complex progression:
At progression of hematogenous disseminated tuberculosis the cavities are formed.
The
At progression of hematogenous disseminated tuberculosis the cavities are formed.
The
Immunity at tuberculosis
Natural resistance to tuberculosis is inherited. It involves non-specific
Immunity at tuberculosis
Natural resistance to tuberculosis is inherited. It involves non-specific
Phagocytosis plays special role in natural resistance. Primary contact MBT and
Phagocytosis plays special role in natural resistance. Primary contact MBT and
Fagocitosis
Completed phagocytosis Uncompleted phagocytosis
It is one of mechanisms The result of
Fagocitosis
Completed phagocytosis Uncompleted phagocytosis
It is one of mechanisms The result of
Results of phagocytosis
Results of phagocytosis
Immunity in tuberculosis consists from five basic reactions: cell reaction, humoral
Immunity in tuberculosis consists from five basic reactions: cell reaction, humoral
Only under these conditions T-helper (CD4+) may recognize antigen peptide of
Only under these conditions T-helper (CD4+) may recognize antigen peptide of
Proof of the role of T- lymphocytes in anti-tubercular immunity:
injection of
Proof of the role of T- lymphocytes in anti-tubercular immunity:
injection of
As immune response builds up multiplication of Mycobacteria slows down, their
As immune response builds up multiplication of Mycobacteria slows down, their
Remaining MBT are located within cells and prevent formation of phagolysosome,
Remaining MBT are located within cells and prevent formation of phagolysosome,
 Перикардиты. Анатомия перикарда
Перикардиты. Анатомия перикарда Спадкові захворювання нервової системи
Спадкові захворювання нервової системи ВИЧ: вопросы и ответы
ВИЧ: вопросы и ответы Нейтропении у детей
Нейтропении у детей Николай Иванович Пирогов Русский хирург и анатом
Николай Иванович Пирогов Русский хирург и анатом Информационные технологии для фармацевтов
Информационные технологии для фармацевтов Периоды детства
Периоды детства Антипсихотики (нейролептики)
Антипсихотики (нейролептики) Глобальные риски и новейшие медицинские технологии
Глобальные риски и новейшие медицинские технологии Компрессионные синдромы шейного отдела позвоночника
Компрессионные синдромы шейного отдела позвоночника Жанұямен қарым – қатынаста жеткен жетістіктерді және қиыншылықтарды талдау
Жанұямен қарым – қатынаста жеткен жетістіктерді және қиыншылықтарды талдау Інсульт. Причини, симптоми інсульту, перша допомога, поради
Інсульт. Причини, симптоми інсульту, перша допомога, поради Крон ауруы
Крон ауруы Pancreatic Cancer
Pancreatic Cancer Особенности фармакокинетики и фармакодинамики при лечении аллергий
Особенности фармакокинетики и фармакодинамики при лечении аллергий ИБС. Стенокардия
ИБС. Стенокардия Нәрестелердің асфиксиясы
Нәрестелердің асфиксиясы Опухолевый рост
Опухолевый рост Кілегейлі қабықтар мен мүшелерде эпителий тінінің мамандануы
Кілегейлі қабықтар мен мүшелерде эпителий тінінің мамандануы Нарушения сна у младенцев и детей раннего возраста
Нарушения сна у младенцев и детей раннего возраста Анастезия задних верхних и нижнего луночкого нерва по П.М. Егорову
Анастезия задних верхних и нижнего луночкого нерва по П.М. Егорову Токсикология фосфорорганических соединений (ФОС)
Токсикология фосфорорганических соединений (ФОС) Анатомо-фізіологічні особливості сечовидільної системи у дітей
Анатомо-фізіологічні особливості сечовидільної системи у дітей Өлім, өлім белгілері
Өлім, өлім белгілері Ми қыртысының анатомиялық-гистологиялық құрылымы
Ми қыртысының анатомиялық-гистологиялық құрылымы Воспалительные процессы органов женской половой системы специфической этиологии
Воспалительные процессы органов женской половой системы специфической этиологии Болезнь Крона
Болезнь Крона Respiratory system
Respiratory system