- Surgical operation and post-operation period

Содержание
- 2. Surgical operation is a traumatic intervention on organs or tissues with the aim of treatment or
- 3. According to the term of performance: urgent emergency, or fixed-term planned According to the aim: Radical
- 4. The operation consists of 3 stages: operative approach (incision) operative method consummation of the operation.
- 5. The operation consists of 3 stages: operative approach (incision), operative method, consummation of the operation
- 6. Demands for the operative approach: it must provide a comfortable performance of the main stage of
- 7. Operative methods can be: removing the whole organ (ectomia) removing an injured part of the organ
- 8. Absolute indications are diseases, which are dangerous for the patient's life & may be removed only
- 9. Relative indications may be divided into 2 groups: diseases which can be cured only with the
- 10. Types of longitudinal, transverse & oblique laparotomy (I - median, 2 -paramedian, 3 - transrectal, 4
- 11. The general state of the organism is valued by physical examination : Palpation Percussion Auscultation; minimal
- 12. Absolute contraindications are: Shock (besides hemorrhagic shock in continuing bleeding) acute myocardial infarction disorders of brain
- 13. Preparation Psychological preparation includes convincing a patient that the operation is necessary & inspiring with the
- 14. The doctor must determine the risk of the operation which depends on many factors: patient's age,
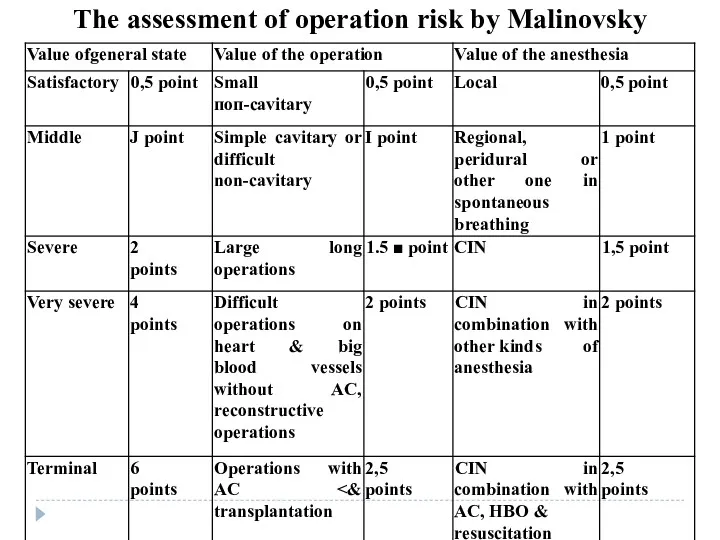
- 15. The assessment of operation risk by Malinovsky
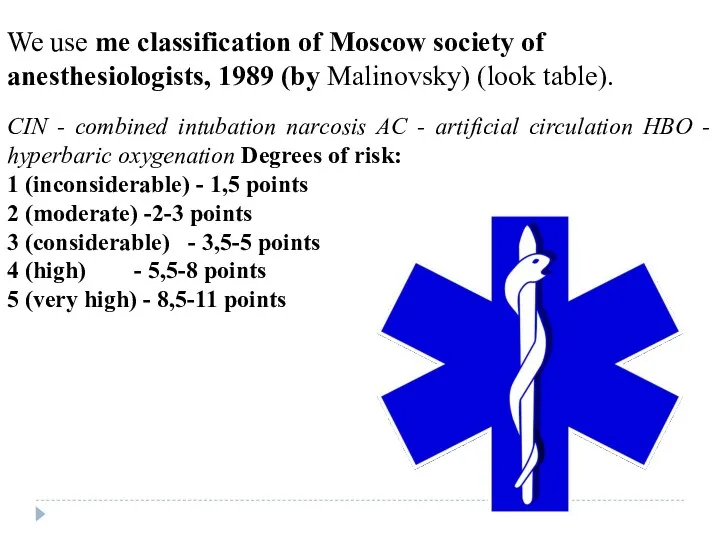
- 16. We use me classification of Moscow society of anesthesiologists, 1989 (by Malinovsky) (look table). CIN -
- 17. Postoperative period
- 18. Everything dealing with the operation & the influence of anesthesia is determined like an operative stress
- 19. In cases of non-complicated course of postoperative period intensive therapy includes: struggle against pain the restoration
- 20. The complications of early postoperative period take place due to 3 main factors: the presence of
- 21. Methods of prophylaxis of cardiovascular disorders: early activation of patients the treatment of chronic diseases of
- 22. Methods of prophylaxis of pulmonary disorders: early activation of patients antibiotics adequate posture in bed respiratory
- 23. Methods of prophylaxis of intestinal disorders: early activation of patients rational diet therapy draining a stomach
- 24. When complications occur in the recovery room or in the perioperative period the importance of consultation
- 25. Postoperative respiratory depression is most commonly due to opiates used for pain relief. However, other causes
- 26. When respiratory depression is severe, immediate respiratory support is necessary, using an Ambu bag or similar-device.
- 27. Cardiovascular system Cardiac failure occurs when reduced myocardial contractility is unable to cope with the additional
- 28. Management involves optimization of oxygenation, posture, and diuretics and in severe cases intermittent positive pressure ventilation
- 29. Postoperative hypertension may be due to pain, or to the withdrawal of preoperative antihypertensive medication. Optimal
- 30. Hypotension is most commonly due to inadequate fluid replacement. Drain tubes should be checked for correct
- 31. In the absence of demonstrable fluid problems, ischemia, arrhythmia, and drug-induced myocardial depression should be excluded.
- 32. Following ECG confirmation of the arrhythmia, specific therapy should be commenced. Rapid atrial fibrillation with haemodynamic
- 33. Pre-existing disease, pain, poorly controlled hypotension, intraoperative events, and suboptimal oxygenation, especially in combination with hypertension
- 34. Nervous system Confusion is common in the perioperative period, especially in the elderly. Diagnosis is frequently
- 35. Hypoxia must be excluded, either by oximetry or blood gas estimation. Review of the anaesthetic chart
- 36. The anaesthetized patient is vulnerable to nerve injury because of the loss of protective reflexes. Nerves
- 37. Catheter-related problems, and postoperative urinary tract infections, although not relevant to the anaesthetic management, need careful
- 38. Postoperative jaundice is an uncommon problem. Full clinical and biochemical assessment is important. Flalothane hepatitis is
- 39. Thus the incidence of jaundice is significantly lower than that following halothane anesthesia and the mortality
- 40. Management in the operating theatre should be supportive until other metabolic pathways eliminate the suxamethonium. Sedation
- 41. This is one of the most common and distressing postoperative complications. The incidence of vomiting ranges
- 42. Skin rashes may be caused by reaction to anaesthetic agents, antibiotics, adhesive dressings, or skin prep
- 43. The incidence of sore throat following endotracheal intubation varies between 2 and 70% of cases. Predisposing
- 44. The development of muscle pains is common in fit, ambulant, muscular young subjects given suxamethonium to
- 46. Скачать презентацию
Surgical operation is a traumatic intervention on organs or tissues with
Surgical operation is a traumatic intervention on organs or tissues with
According to the term of performance:
urgent
emergency, or fixed-term planned
According to
According to the term of performance:
urgent
emergency, or fixed-term planned
According to
The operation consists
of 3 stages:
operative approach (incision)
operative method
consummation of the
The operation consists
of 3 stages:
operative approach (incision)
operative method
consummation of the
The operation consists of 3 stages:
operative approach (incision), operative method,
The operation consists of 3 stages:
operative approach (incision), operative method,

Demands for the operative approach: it must provide a comfortable performance
Demands for the operative approach: it must provide a comfortable performance
Operative methods can be:
removing the whole organ (ectomia)
removing an injured
Operative methods can be:
removing the whole organ (ectomia)
removing an injured
Absolute indications are diseases, which are dangerous for the patient's life
Absolute indications are diseases, which are dangerous for the patient's life
Relative indications may be divided into 2 groups:
diseases which can
Relative indications may be divided into 2 groups:
diseases which can
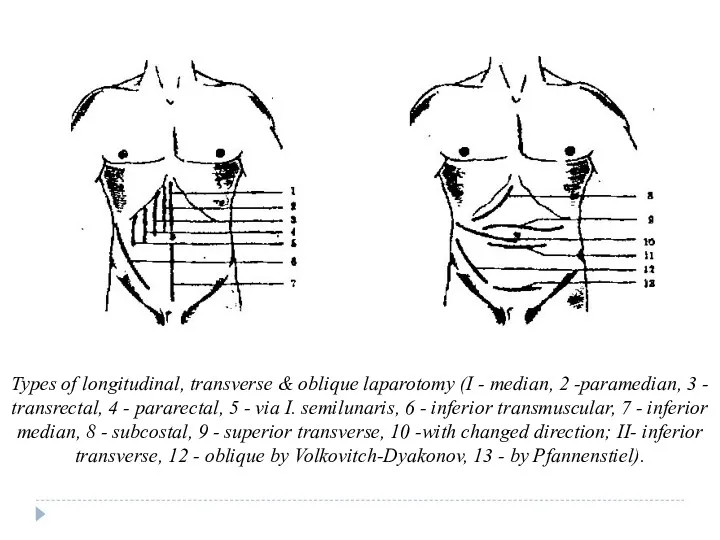
Types of longitudinal, transverse & oblique laparotomy (I - median, 2
Types of longitudinal, transverse & oblique laparotomy (I - median, 2
The general state of the organism is valued by physical examination
The general state of the organism is valued by physical examination
Absolute contraindications are:
Shock (besides hemorrhagic shock in continuing bleeding)
acute myocardial infarction
disorders
Absolute contraindications are:
Shock (besides hemorrhagic shock in continuing bleeding)
acute myocardial infarction
disorders
Preparation
Psychological preparation includes convincing a patient that the operation is necessary
Preparation
Psychological preparation includes convincing a patient that the operation is necessary
The doctor must determine the risk of the operation which depends
The doctor must determine the risk of the operation which depends
The assessment of operation risk by Malinovsky
The assessment of operation risk by Malinovsky
We use me classification of Moscow society of anesthesiologists, 1989 (by
We use me classification of Moscow society of anesthesiologists, 1989 (by
Postoperative period
Postoperative period
Everything dealing with the operation & the influence of anesthesia is
Everything dealing with the operation & the influence of anesthesia is
In cases of non-complicated course of postoperative period intensive therapy includes:
struggle
In cases of non-complicated course of postoperative period intensive therapy includes:
struggle
The complications of early postoperative period take place due to 3
The complications of early postoperative period take place due to 3
Methods of prophylaxis of cardiovascular disorders:
early activation of patients
the treatment of
Methods of prophylaxis of cardiovascular disorders:
early activation of patients
the treatment of
Methods of prophylaxis of pulmonary disorders:
early activation of patients
antibiotics
adequate posture in
Methods of prophylaxis of pulmonary disorders:
early activation of patients
antibiotics
adequate posture in
Methods of prophylaxis of intestinal disorders:
early activation of patients
rational diet therapy
draining
Methods of prophylaxis of intestinal disorders:
early activation of patients
rational diet therapy
draining
When complications occur in the recovery room or in the perioperative
When complications occur in the recovery room or in the perioperative
Postoperative respiratory depression is most commonly due to opiates used for
Postoperative respiratory depression is most commonly due to opiates used for
When respiratory depression is severe, immediate respiratory support is necessary, using
When respiratory depression is severe, immediate respiratory support is necessary, using
Cardiovascular system
Cardiac failure occurs when reduced myocardial contractility is unable to
Cardiovascular system
Cardiac failure occurs when reduced myocardial contractility is unable to
Management involves optimization of oxygenation, posture, and diuretics and in severe
Management involves optimization of oxygenation, posture, and diuretics and in severe
Postoperative hypertension may be due to pain, or to the withdrawal
Postoperative hypertension may be due to pain, or to the withdrawal
Hypotension is most commonly due to inadequate fluid replacement. Drain tubes
Hypotension is most commonly due to inadequate fluid replacement. Drain tubes
In the absence of demonstrable fluid problems, ischemia, arrhythmia, and drug-induced
In the absence of demonstrable fluid problems, ischemia, arrhythmia, and drug-induced
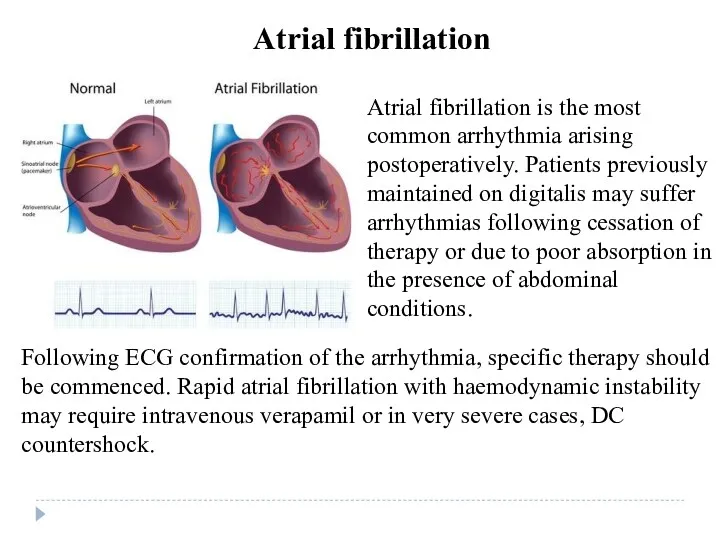
Following ECG confirmation of the arrhythmia, specific therapy should be commenced.
Following ECG confirmation of the arrhythmia, specific therapy should be commenced.
Pre-existing disease,
pain,
poorly controlled hypotension,
intraoperative events,
and suboptimal oxygenation,
especially in combination
Pre-existing disease,
pain,
poorly controlled hypotension,
intraoperative events,
and suboptimal oxygenation,
especially in combination
Nervous system
Confusion is common in the perioperative period, especially in the
Nervous system
Confusion is common in the perioperative period, especially in the
Hypoxia must be excluded, either by oximetry or blood gas estimation.
Hypoxia must be excluded, either by oximetry or blood gas estimation.
The anaesthetized patient is vulnerable to nerve injury because of the
The anaesthetized patient is vulnerable to nerve injury because of the
Catheter-related problems, and postoperative urinary tract infections, although
not relevant to the
Catheter-related problems, and postoperative urinary tract infections, although
not relevant to the
Postoperative jaundice is an uncommon problem. Full clinical and biochemical assessment
Postoperative jaundice is an uncommon problem. Full clinical and biochemical assessment
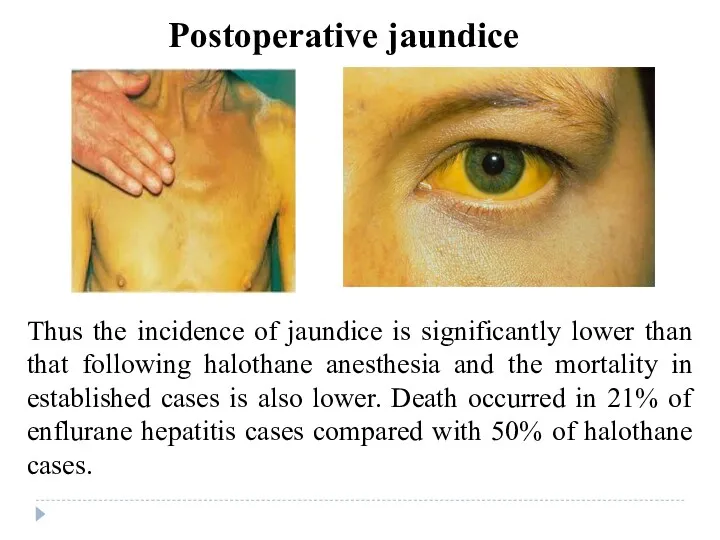
Thus the incidence of jaundice is significantly lower than that following
Thus the incidence of jaundice is significantly lower than that following
Management in the operating theatre should be supportive until other metabolic
Management in the operating theatre should be supportive until other metabolic
This is one of the most common and distressing postoperative complications.
This is one of the most common and distressing postoperative complications.
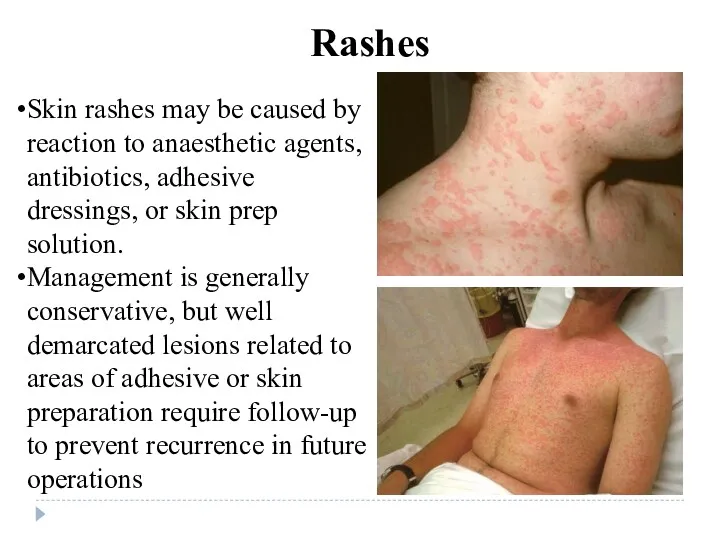
Skin rashes may be caused by reaction to anaesthetic agents, antibiotics,
Skin rashes may be caused by reaction to anaesthetic agents, antibiotics,
The incidence of sore throat following endotracheal intubation varies between 2
The incidence of sore throat following endotracheal intubation varies between 2
The development of muscle pains is common in fit, ambulant, muscular
The development of muscle pains is common in fit, ambulant, muscular
 Металлокерамика. Монолитная гипсовая модель
Металлокерамика. Монолитная гипсовая модель Лептоспироз диагностикасы мен күресу шаралары
Лептоспироз диагностикасы мен күресу шаралары Судебно-медицинская токсикология
Судебно-медицинская токсикология Tetralogy of Fallot
Tetralogy of Fallot Современные шкалы в оценке тяжести хирургических больных с SIRS
Современные шкалы в оценке тяжести хирургических больных с SIRS Антисептики и дезинфицирующие средства. Антибактериальные химиотерапевтические средства
Антисептики и дезинфицирующие средства. Антибактериальные химиотерапевтические средства Ауруханаішілік инфекция
Ауруханаішілік инфекция Физиотерапия заболеваний нервной системы
Физиотерапия заболеваний нервной системы Беременность и роды высокого риска
Беременность и роды высокого риска Алгоритм диагностики, оказания скорой и неотложной медицинской помощи и порядок госпитализации пациентов с ОНМК
Алгоритм диагностики, оказания скорой и неотложной медицинской помощи и порядок госпитализации пациентов с ОНМК Хранение лекарственных средств. Специалистам аптечных организаций
Хранение лекарственных средств. Специалистам аптечных организаций Открытый прикус
Открытый прикус Естественное вскармливание ребенка первого года жизни
Естественное вскармливание ребенка первого года жизни Сахарный диабет. Ожирение. Лекция №30
Сахарный диабет. Ожирение. Лекция №30 Бауме бойынша тістесу түрлері
Бауме бойынша тістесу түрлері Механизмы трофического действия физических упражнений
Механизмы трофического действия физических упражнений Нарушение ритма
Нарушение ритма Страхование здоровья в Грузии. Страховая компания Полис Меди
Страхование здоровья в Грузии. Страховая компания Полис Меди Гериатрические аспекты заболеваний опорно-двигательного аппарата
Гериатрические аспекты заболеваний опорно-двигательного аппарата Развертывание, оборудование и свертывание медицинской роты бригады. Тема № 19-1
Развертывание, оборудование и свертывание медицинской роты бригады. Тема № 19-1 Әйел жыныс мүшелерінің қабыну аурулары
Әйел жыныс мүшелерінің қабыну аурулары Лекарственная безопасность
Лекарственная безопасность Ведение беременности и родов у ВИЧ-инфицированных
Ведение беременности и родов у ВИЧ-инфицированных Улану кезіндегі шұғыл көмек
Улану кезіндегі шұғыл көмек Гепатит A (Болезнью Боткин)
Гепатит A (Болезнью Боткин)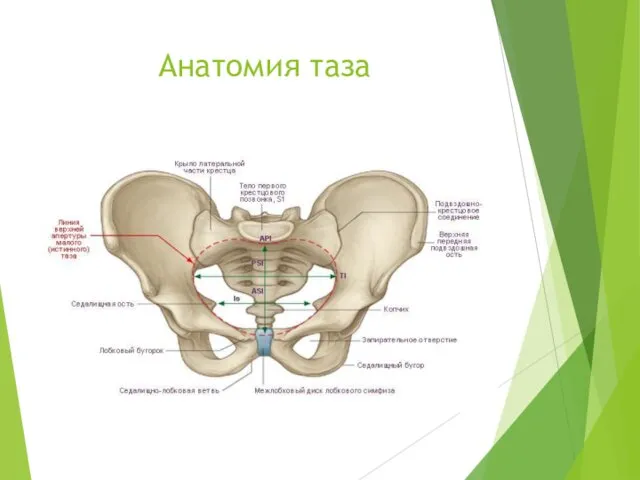 Анатомия таза
Анатомия таза Биоэтика. Исторические модели моральной медицины
Биоэтика. Исторические модели моральной медицины Постинъекционные осложнения. Вирусные гепатиты и ВИЧ-инфекция
Постинъекционные осложнения. Вирусные гепатиты и ВИЧ-инфекция