- Schizophrenia. Delusional disorder. Schizotypal disorder

Содержание
- 2. DEFINITION Gr.. φρήν – mind, reason Schizophrenia - a progressive endogenous polymorphic mental disorder characterized by
- 3. HISTORY OF SCHIZOPHRENIA Emil Kraepelin:In 1883, separated schizophrenia (which he called dementia praecox) from bipolar disorder
- 4. HISTORY OF SCHIZOPHRENIA Eugen Bleuler "Schizophrenia" (1911) "Basic symptoms" Four "A": Autism Associate synthesis disorders Emotional
- 5. HISTORY OF SCHIZOPHRENIA Four «A» E.BIeuler AUTISM AMBIVALENCE APATHY ABULIA
- 6. Epidemiology of schizophrenia The prevalence of schizophrenia in the world is estimated at between 0.8 -
- 7. Psychological consequences of schizophrenia The most debilitating of all mental illnesses Reduced quality of life for
- 8. Etiology of schizophrenia Genetically inhereted Adverse impact of the environment Psychodynamic Infectious Autoimmune Neurotransmitter «Stress-diathesis» Hypotheses
- 9. Pathogenesis of schizophrenia Neurotransmitter disorders Morphological changes Serotonin theory The dopamine theory increase in dopaminergic activity
- 10. Pathogenesis of schizophrenia 2 types of schizophrenia Crow Т. (1985) hyper-dopaminergic activity Hypo dopaminergic activity Atrophy
- 11. CLINIC OF SCHIZOPHRENIA Emotional disorder NEGATIVE SYMPTOMS (Deficits) – define nosological diagnosis of schizophrenia POSITIVE SYMPTOMS
- 12. «SKHIZIS» The process of thinking is disrupted without connection between thoughts – "Splitting" is a violation
- 13. Classification Types of course Clinical forms F20.0 Paranoid schizophrenia F20.1 Hebephrenic schizophrenia F20.3 Undifferentiated schizophrenia F20.4
- 14. A simple form of schizophrenia There are no positive symptoms negative symptoms grow rapidly, reaching a
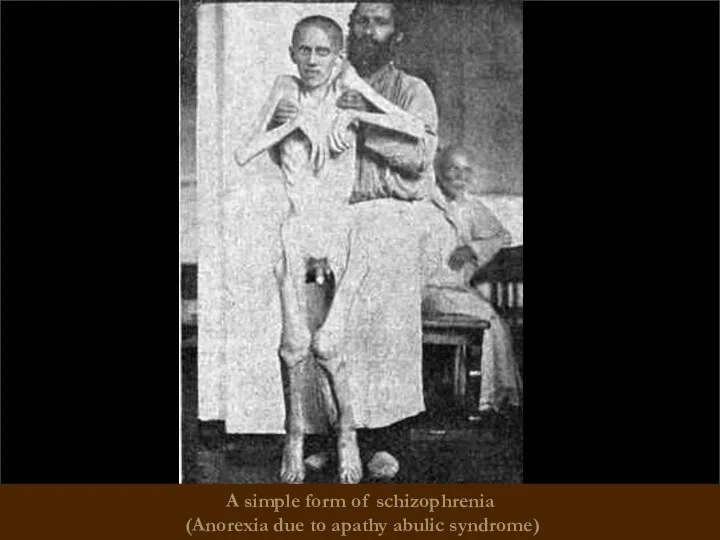
- 15. A simple form of schizophrenia (Anorexia due to apathy abulic syndrome)
- 16. Hebephrenic schizophrenia Starting at adolescence, young adulthood Hebephrenia syndrome dominate (including emotional and volitional and behavioral
- 17. hebephrenic schizophrenia (hebephrenic excitation)
- 18. Paranoid schizophrenia Hallucinatory-paranoid syndrome dominates. Possible transformation syndrome: paranoiac -> paranoid -> paraphrenic Duration is continuous
- 19. Paranoid schizophrenia (Pretentious posture, hallucinatory-paranoid syndrome)
- 20. Paranoid schizophrenia (Paraphrenic syndrome)
- 21. Catatonic schizophrenia It begins with an episode of psychomotor agitation. Leading syndrome – catatonic Meets basic
- 22. Catatonic schizophrenia (waxy flexibility)
- 23. Catatonic schizophrenia (waxy flexibility, a symptom of the proboscis)
- 24. Catatonic schizophrenia
- 25. Febrile schizophrenia oneiric bouts of catatonia, accompanied by a rise in temperature and the emergence of
- 26. Schizophrenic "defect" – irreversible personality changes occur during the course of the disease and combine negative
- 27. Types of schizophrenic "defect" Apatite-abulic - the most common defect of emotional and volitional spheres (passivity,
- 28. Types of schizophrenic "defect" Thymopathic - "acquired cyclothymia." Hyperesthenic - appearance after the attack before unusual
- 29. The prognosis for schizophrenia It depends on the type of disease The earlier debut, the worse
- 30. Treatment of SCHIZOPHRENIA
- 31. STAGES OF TREATMENT
- 32. Treatment of schizophrenia Biological methods (insulin-coma therapy, electro-convulsive therapy) psychopharmacology (Antipsychotics) psychotherapy
- 33. THERAPY BIOLOGICAL PSYCHOSOCIAL Psycho-educational sessions with patients' relatives Psychotherapy with patients Antipsychotics (chlorpromazine, galloperidol, risperon etc.).
- 34. The history of the development of biological therapy Pyrogenic therapy - (1918) for the treatment of
- 35. Electroshock treatment (EST) was suggested in 1938 by an Italian psychiatrist U. Cherletti and a neurophysiologist
- 36. Insulin coma treatment Consists in giving the patient on an empty stomach some individually selected dose
- 37. First Generation Antipsychotics (Neuroleptics) – typical neuroleptics Relieve only positive symptoms Chlorpromazine (Thorazine) phenothiazines primarily blocks
- 38. First Generation Antipsychotics (Neuroleptics) – typical neuroleptics Relieve only positive symptoms Chlorpromazine (Thorazine) phenothiazines primarily blocks
- 39. Major Side Effects Movement Effects (Extrapyramidal) Parkinsonism Akathisia Tardive Dyskinesia Agranulocytosis ↓ white blood cells (WBC)
- 40. Second Generation Antipsychotics (Atypical Neuroleptics) Relieve negative & positive symptoms Lower risk of Parkinsonism Akathisia Tardive
- 41. Clozapine Clozaril ↑ Agranulocytosis Risperidone Risperdal ↓↓ Agranulocytosis; Amisulpride (↑ level of prolactine) Aripiprazole (Abilify) ?
- 42. Common antipsychotic medication side effects Dry mouth Constipation Blurred vision Drowsiness
- 43. Serious antipsychotic medication side effects Restlessness Muscle stiffness Slurred speech Extremity tremors Agranulocytosis
- 44. CRITERIA FOR THE QUALITY OF TREATMENT Reduction of psychopathological symptoms for at least six months Clinical
- 45. Treatment of schizophrenia After treatment of acute schizophrenic psychosis long time maintain therapy: after 1 episod
- 46. Schizophrenia-like psychotic disorder Acute psychotic disorder in which the psychotic symptoms are relatively stable and meet
- 47. Treatment During the transient psychotic states small doses of neuroleptics are prescribed (eg, haloperidol 2-5 mg
- 48. Induced delusional disorder A rare delusional disorder, which is shared by two or more people with
- 49. Delusional disorder Every year there from 1 to 3 new cases of delusional disorders per 100
- 50. Delusional disorder Situations that contribute to the development of delusional disorders: 1) subject of exaggerated expectation
- 51. Classification of delirium Primary (Interpretative, primordial, verbal) Secondary (sensual and imaginative) Violation of thinking comes secondly
- 52. Delusional syndrome: Paranoiac syndrome - a systematic interpretative delirium. Most monothematic. There has been no intellectual-mental
- 53. Stages of development of delirium Delusional mood - the belief that there were some changes somewhere
- 54. Paraphrenia Greek. Involutionary paraphrenia - represents delusional psychosis of elderly people, it is manifested by delusions
- 55. The course and prognosis The diagnosis of schizophenia can never be withdrawn, but a long-term compensation
- 56. Schizotypal disorder Schizotypal disorder - a disorder is not suitable for diagnostic criteria of ICD-10 diagnosis
- 57. Schizotypal disorder In ukrainian psychiatry resemble the indolent (slow-) schizophrenia. Diagnosis is complicated. It is characterized
- 58. The criteria according to ICD-10 A. For at least two years continuously or periodically be detected
- 59. Louis Wayne (1860-1939) Creation of patients with schizophrenia
- 60. Mark Gudvolt (1980) Creation of patients with schizophrenia
- 61. Mark Gudvolt (1980) Arts of patients with schizophrenia
- 62. Salvador Felip Jacint Dalí Domenech Domenech and the Marquis de Pubol (1904 - 1989) Spanish surrealist
- 63. Salvador Dali. Untitled. Dovetail and cello (a series of accidents), 1983 Last picture painted by the
- 64. Francisco Jose de Goya (1746 - 1828) Self Portrait. Court painter of King of Spain, vice-director
- 65. Friedrich Wilhelm Nietzsche (1844 - 1900) German philosopher
- 66. John Forbes Nash Jr (1928 -) American mathematician, Nobel Laureate in Economics 1994
- 67. Mikhail Vrubel (1856 - 1910) Self Portrait. Russian modernist painter
- 68. Franz Kafka (1883 - 1924) Austrian writer
- 69. Vincent Van Gogh (1853 - 1890) Self Portrait. Dutch postimpressionist painter
- 70. Emanuel Swedenborg (1688 - 1772) The Swedish natural scientist, theosophist, inventor. In 2004, the collection of
- 71. Ludwig II (1845 - 1886) The King of Bavaria
- 72. Victor Kandinsky (1849 - 1889) The Russian psychiatrist and author of "On pseudohallucinations"
- 73. THANK YOU FOR YOUR ATTENTION!
- 79. Скачать презентацию
DEFINITION
Gr..
φρήν
– mind, reason
Schizophrenia - a progressive endogenous polymorphic mental disorder
DEFINITION
Gr..
φρήν
– mind, reason
Schizophrenia - a progressive endogenous polymorphic mental disorder
HISTORY OF SCHIZOPHRENIA
Emil Kraepelin:In 1883, separated schizophrenia (which he called dementia
HISTORY OF SCHIZOPHRENIA
Emil Kraepelin:In 1883, separated schizophrenia (which he called dementia
HISTORY OF SCHIZOPHRENIA
Eugen Bleuler
"Schizophrenia" (1911)
"Basic symptoms"
Four "A":
Autism
Associate synthesis disorders
Emotional and volitional
HISTORY OF SCHIZOPHRENIA
Eugen Bleuler
"Schizophrenia" (1911)
"Basic symptoms"
Four "A":
Autism
Associate synthesis disorders
Emotional and volitional
HISTORY OF SCHIZOPHRENIA
Four «A»
E.BIeuler
AUTISM
AMBIVALENCE
APATHY
ABULIA
HISTORY OF SCHIZOPHRENIA
Four «A»
E.BIeuler
AUTISM
AMBIVALENCE
APATHY
ABULIA
Epidemiology of schizophrenia
The prevalence of schizophrenia in the world is estimated
Epidemiology of schizophrenia
The prevalence of schizophrenia in the world is estimated
Psychological consequences of schizophrenia
The most debilitating of all mental illnesses
Reduced quality
Psychological consequences of schizophrenia
The most debilitating of all mental illnesses
Reduced quality
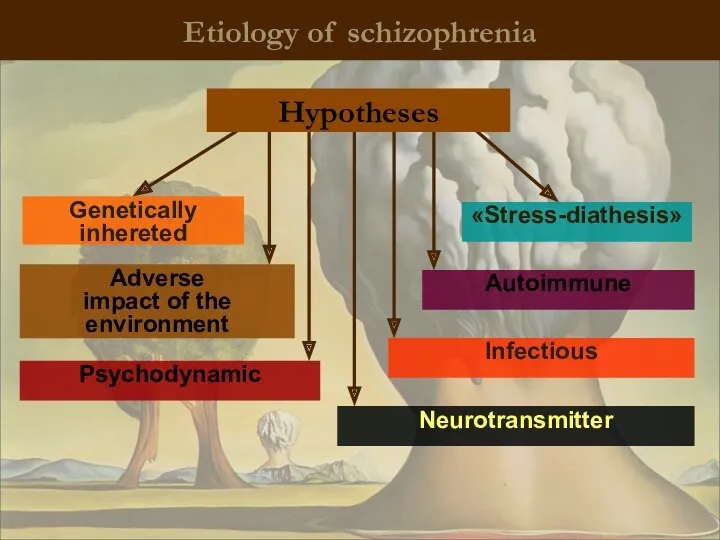
Etiology of schizophrenia
Genetically inhereted
Adverse
impact of the environment
Psychodynamic
Infectious
Autoimmune
Neurotransmitter
«Stress-diathesis»
Hypotheses
Etiology of schizophrenia
Genetically inhereted
Adverse
impact of the environment
Psychodynamic
Infectious
Autoimmune
Neurotransmitter
«Stress-diathesis»
Hypotheses
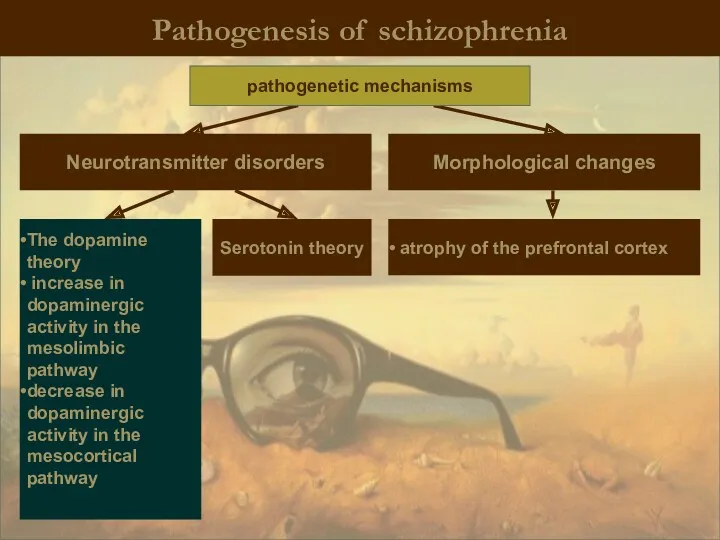
Pathogenesis of schizophrenia
Neurotransmitter disorders
Morphological changes
Serotonin theory
The dopamine theory
increase in dopaminergic
Pathogenesis of schizophrenia
Neurotransmitter disorders
Morphological changes
Serotonin theory
The dopamine theory
increase in dopaminergic
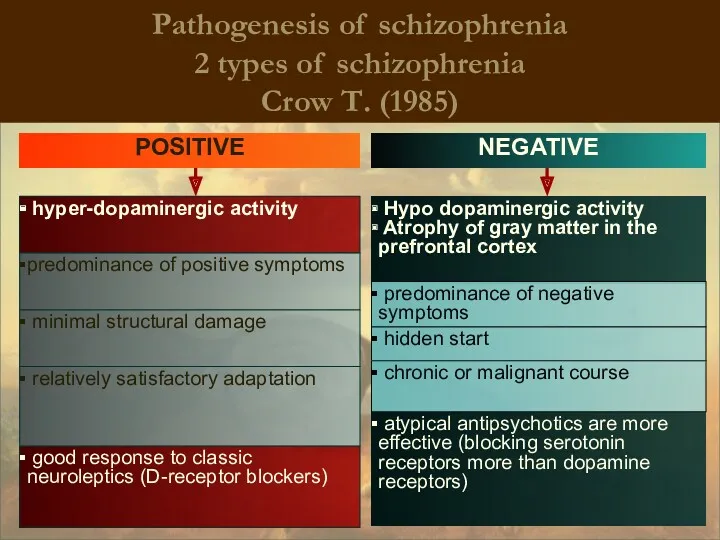
Pathogenesis of schizophrenia
2 types of schizophrenia
Crow Т. (1985)
hyper-dopaminergic activity
Hypo
Pathogenesis of schizophrenia
2 types of schizophrenia
Crow Т. (1985)
hyper-dopaminergic activity
Hypo
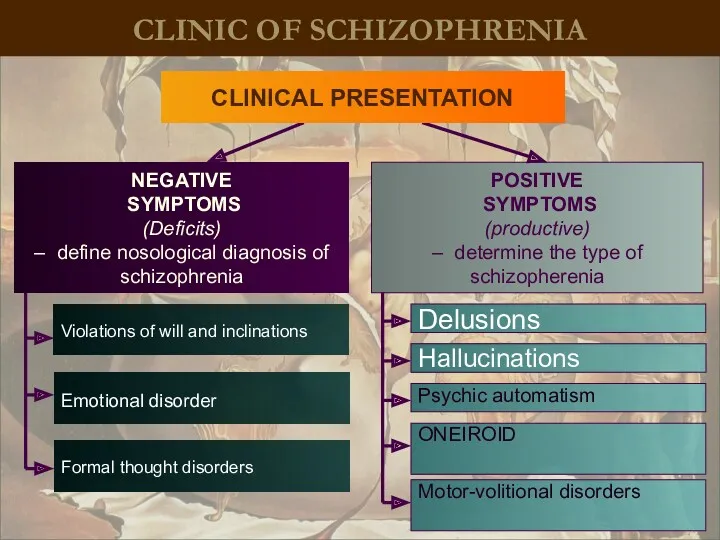
CLINIC OF SCHIZOPHRENIA
Emotional disorder
NEGATIVE
SYMPTOMS
(Deficits)
– define nosological diagnosis of schizophrenia
POSITIVE
SYMPTOMS
(productive)
–
CLINIC OF SCHIZOPHRENIA
Emotional disorder
NEGATIVE
SYMPTOMS
(Deficits)
– define nosological diagnosis of schizophrenia
POSITIVE
SYMPTOMS
(productive)
–
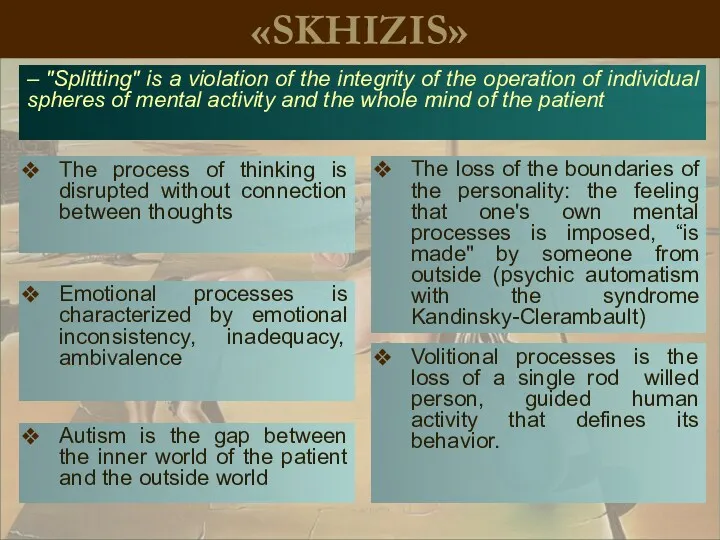
«SKHIZIS»
The process of thinking is disrupted without connection between thoughts
– "Splitting"
«SKHIZIS»
The process of thinking is disrupted without connection between thoughts
– "Splitting"
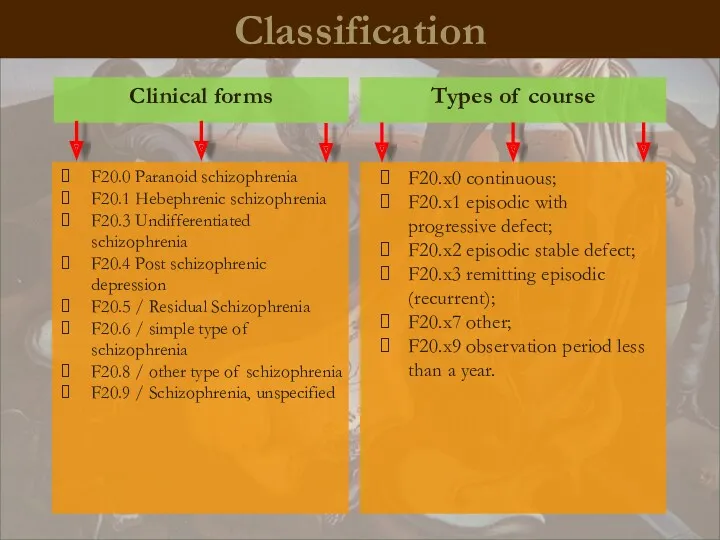
Classification
Types of course
Clinical forms
F20.0 Paranoid schizophrenia
F20.1 Hebephrenic schizophrenia
F20.3 Undifferentiated schizophrenia
F20.4
Classification
Types of course
Clinical forms
F20.0 Paranoid schizophrenia
F20.1 Hebephrenic schizophrenia
F20.3 Undifferentiated schizophrenia
F20.4
A simple form of schizophrenia
There are no positive symptoms
negative symptoms
A simple form of schizophrenia
There are no positive symptoms
negative symptoms
A simple form of schizophrenia
(Anorexia due to apathy abulic syndrome)
A simple form of schizophrenia
(Anorexia due to apathy abulic syndrome)
Hebephrenic schizophrenia
Starting at adolescence, young adulthood
Hebephrenia syndrome dominate (including emotional
Hebephrenic schizophrenia
Starting at adolescence, young adulthood
Hebephrenia syndrome dominate (including emotional
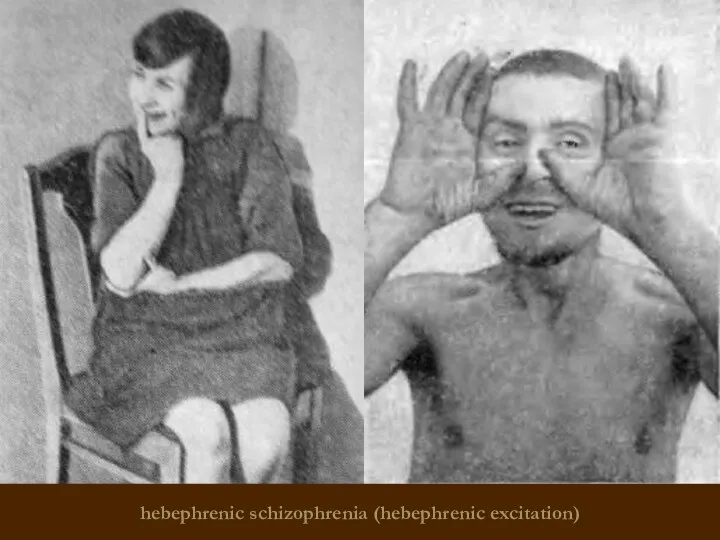
hebephrenic schizophrenia (hebephrenic excitation)
hebephrenic schizophrenia (hebephrenic excitation)
Paranoid schizophrenia
Hallucinatory-paranoid syndrome dominates.
Possible transformation syndrome: paranoiac -> paranoid -> paraphrenic
Duration
Paranoid schizophrenia
Hallucinatory-paranoid syndrome dominates.
Possible transformation syndrome: paranoiac -> paranoid -> paraphrenic
Duration
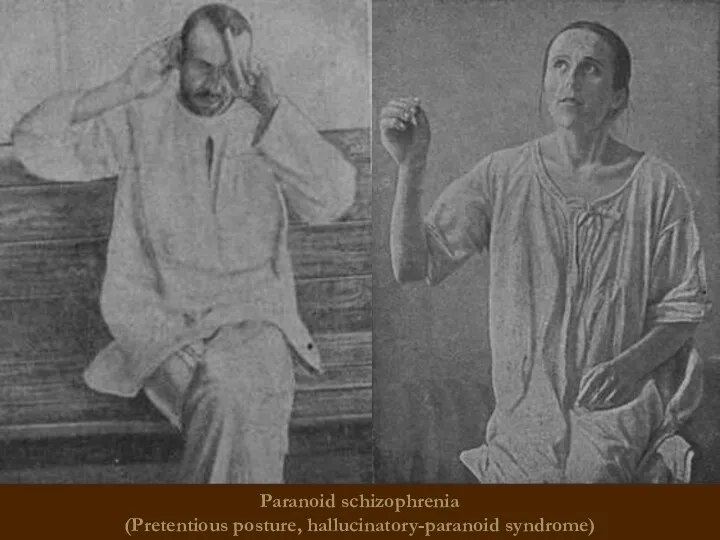
Paranoid schizophrenia
(Pretentious posture, hallucinatory-paranoid syndrome)
Paranoid schizophrenia
(Pretentious posture, hallucinatory-paranoid syndrome)
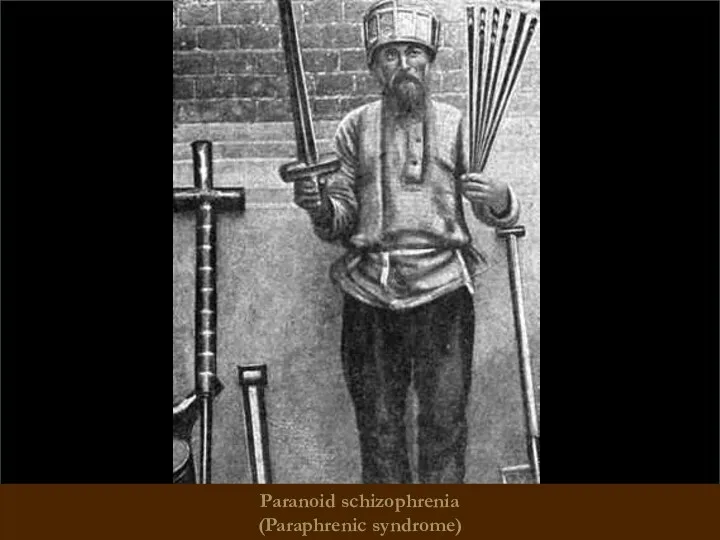
Paranoid schizophrenia
(Paraphrenic syndrome)
Paranoid schizophrenia
(Paraphrenic syndrome)
Catatonic schizophrenia
It begins with an episode of psychomotor agitation.
Leading syndrome –
Catatonic schizophrenia
It begins with an episode of psychomotor agitation.
Leading syndrome –
Catatonic schizophrenia (waxy flexibility)
Catatonic schizophrenia (waxy flexibility)
Catatonic schizophrenia (waxy flexibility, a symptom of the proboscis)
Catatonic schizophrenia (waxy flexibility, a symptom of the proboscis)
Catatonic schizophrenia
Catatonic schizophrenia
Febrile schizophrenia
oneiric bouts of catatonia, accompanied by a rise in
Febrile schizophrenia
oneiric bouts of catatonia, accompanied by a rise in
Schizophrenic "defect"
– irreversible personality changes occur during the course of the
Schizophrenic "defect"
– irreversible personality changes occur during the course of the
Types of schizophrenic "defect"
Apatite-abulic - the most common defect of emotional
Types of schizophrenic "defect"
Apatite-abulic - the most common defect of emotional
Types of schizophrenic "defect"
Thymopathic - "acquired cyclothymia."
Hyperesthenic - appearance after the
Types of schizophrenic "defect"
Thymopathic - "acquired cyclothymia."
Hyperesthenic - appearance after the
The prognosis for schizophrenia
It depends on the type of disease
The earlier
The prognosis for schizophrenia
It depends on the type of disease
The earlier
Treatment
of SCHIZOPHRENIA
Treatment
of SCHIZOPHRENIA
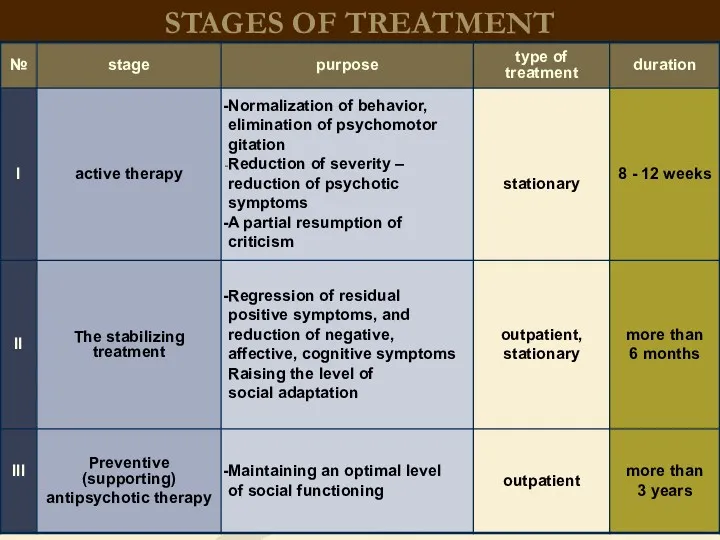
STAGES OF TREATMENT
STAGES OF TREATMENT
Treatment
of schizophrenia
Biological methods (insulin-coma therapy, electro-convulsive therapy)
psychopharmacology (Antipsychotics)
psychotherapy
Treatment
of schizophrenia
Biological methods (insulin-coma therapy, electro-convulsive therapy)
psychopharmacology (Antipsychotics)
psychotherapy
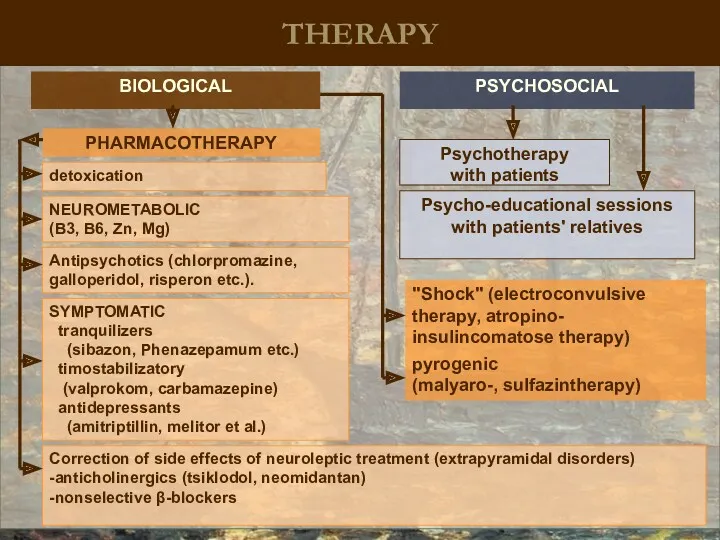
THERAPY
BIOLOGICAL
PSYCHOSOCIAL
Psycho-educational sessions with patients' relatives
Psychotherapy
with patients
Antipsychotics (chlorpromazine, galloperidol, risperon etc.).
detoxication
SYMPTOMATIC
tranquilizers
THERAPY
BIOLOGICAL
PSYCHOSOCIAL
Psycho-educational sessions with patients' relatives
Psychotherapy
with patients
Antipsychotics (chlorpromazine, galloperidol, risperon etc.).
detoxication
SYMPTOMATIC
tranquilizers
The history of the development
of biological therapy
Pyrogenic therapy - (1918)
The history of the development
of biological therapy
Pyrogenic therapy - (1918)
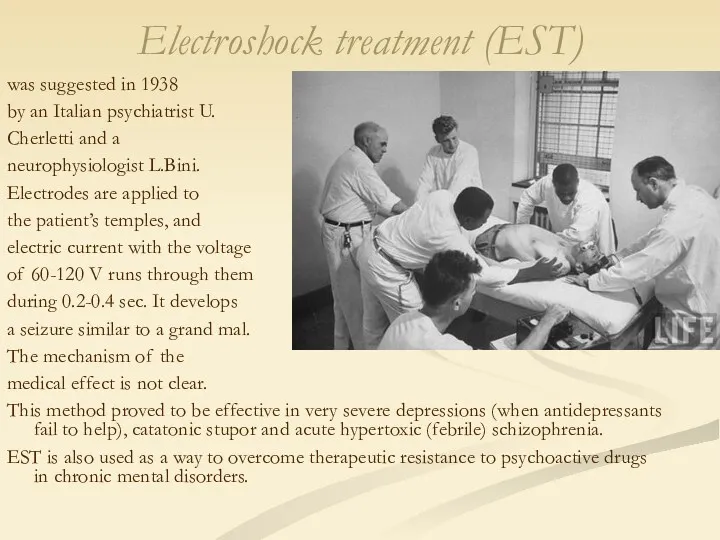
Electroshock treatment (EST)
was suggested in 1938
by an Italian psychiatrist U.
Electroshock treatment (EST)
was suggested in 1938
by an Italian psychiatrist U.
Insulin coma treatment
Consists in giving the patient on an empty stomach
Insulin coma treatment
Consists in giving the patient on an empty stomach
First Generation Antipsychotics (Neuroleptics) – typical neuroleptics
Relieve only positive symptoms
Chlorpromazine (Thorazine)
phenothiazines
primarily
First Generation Antipsychotics (Neuroleptics) – typical neuroleptics
Relieve only positive symptoms
Chlorpromazine (Thorazine)
phenothiazines
primarily
First Generation Antipsychotics (Neuroleptics) – typical neuroleptics
Relieve only positive symptoms
Chlorpromazine (Thorazine)
phenothiazines
primarily
First Generation Antipsychotics (Neuroleptics) – typical neuroleptics
Relieve only positive symptoms
Chlorpromazine (Thorazine)
phenothiazines
primarily
Major Side Effects
Movement Effects (Extrapyramidal)
Parkinsonism
Akathisia
Tardive Dyskinesia
Agranulocytosis
↓ white blood cells (WBC)
Not
Major Side Effects
Movement Effects (Extrapyramidal)
Parkinsonism
Akathisia
Tardive Dyskinesia
Agranulocytosis
↓ white blood cells (WBC)
Not
Second Generation Antipsychotics (Atypical Neuroleptics)
Relieve negative & positive symptoms
Lower risk of
Second Generation Antipsychotics (Atypical Neuroleptics)
Relieve negative & positive symptoms
Lower risk of
Clozapine Clozaril
↑ Agranulocytosis
Risperidone Risperdal
↓↓ Agranulocytosis;
Amisulpride (↑ level of prolactine)
Aripiprazole
↑ Agranulocytosis
Risperidone Risperdal
↓↓ Agranulocytosis;
Amisulpride (↑ level of prolactine)
Aripiprazole
Common antipsychotic medication side effects
Dry mouth
Constipation
Blurred vision
Drowsiness
Common antipsychotic medication side effects
Dry mouth
Constipation
Blurred vision
Drowsiness
Serious antipsychotic medication side effects
Restlessness
Muscle stiffness
Slurred speech
Extremity tremors
Agranulocytosis
Serious antipsychotic medication side effects
Restlessness
Muscle stiffness
Slurred speech
Extremity tremors
Agranulocytosis
CRITERIA FOR THE QUALITY OF TREATMENT
Reduction of psychopathological symptoms for at
CRITERIA FOR THE QUALITY OF TREATMENT
Reduction of psychopathological symptoms for at
Treatment
of schizophrenia
After treatment of acute schizophrenic psychosis long time maintain therapy:
after
Treatment
of schizophrenia
After treatment of acute schizophrenic psychosis long time maintain therapy:
after
Schizophrenia-like psychotic disorder
Acute psychotic disorder in which the psychotic symptoms are
Schizophrenia-like psychotic disorder
Acute psychotic disorder in which the psychotic symptoms are
Treatment
During the transient psychotic states small doses of neuroleptics are
Treatment
During the transient psychotic states small doses of neuroleptics are
Induced delusional disorder
A rare delusional disorder, which is shared by two
Induced delusional disorder
A rare delusional disorder, which is shared by two
Delusional disorder
Every year there from 1 to 3 new cases
Delusional disorder
Every year there from 1 to 3 new cases
Delusional disorder
Situations that contribute to the development of delusional disorders:
1)
Delusional disorder
Situations that contribute to the development of delusional disorders:
1)
Classification of delirium
Primary
(Interpretative, primordial, verbal)
Secondary (sensual and imaginative)
Violation of thinking
Classification of delirium
Primary
(Interpretative, primordial, verbal)
Secondary (sensual and imaginative)
Violation of thinking
Delusional syndrome:
Paranoiac syndrome - a systematic interpretative delirium. Most monothematic. There
Delusional syndrome:
Paranoiac syndrome - a systematic interpretative delirium. Most monothematic. There
Stages of development of delirium
Delusional mood - the belief that there
Stages of development of delirium
Delusional mood - the belief that there
Paraphrenia
Greek.
Involutionary paraphrenia - represents delusional psychosis of elderly people,
Paraphrenia
Greek.
Involutionary paraphrenia - represents delusional psychosis of elderly people,
The course and prognosis
The diagnosis of schizophenia can never be withdrawn,
The course and prognosis
The diagnosis of schizophenia can never be withdrawn,
Schizotypal disorder
Schizotypal disorder - a disorder is not suitable for
Schizotypal disorder
Schizotypal disorder - a disorder is not suitable for
Schizotypal disorder
In ukrainian psychiatry resemble the indolent (slow-) schizophrenia.
Diagnosis is
Schizotypal disorder
In ukrainian psychiatry resemble the indolent (slow-) schizophrenia.
Diagnosis is
The criteria according to ICD-10
A. For at least two years continuously
The criteria according to ICD-10
A. For at least two years continuously
Louis Wayne (1860-1939)
Creation of patients with schizophrenia
Louis Wayne (1860-1939)
Creation of patients with schizophrenia
Mark Gudvolt
(1980)
Creation of patients with schizophrenia
Mark Gudvolt
(1980)
Creation of patients with schizophrenia
Mark Gudvolt
(1980)
Arts of patients with schizophrenia
Mark Gudvolt
(1980)
Arts of patients with schizophrenia
Salvador Felip Jacint Dalí Domenech Domenech and the Marquis de Pubol
Salvador Felip Jacint Dalí Domenech Domenech and the Marquis de Pubol
Salvador Dali. Untitled. Dovetail and cello (a series of accidents), 1983
Salvador Dali. Untitled. Dovetail and cello (a series of accidents), 1983

Francisco Jose de Goya
(1746 - 1828)
Self Portrait. Court painter
Francisco Jose de Goya (1746 - 1828) Self Portrait. Court painter
Friedrich Wilhelm Nietzsche
(1844 - 1900)
German philosopher
Friedrich Wilhelm Nietzsche
(1844 - 1900)
German philosopher
John Forbes Nash Jr
(1928 -)
American mathematician, Nobel Laureate in
John Forbes Nash Jr (1928 -) American mathematician, Nobel Laureate in
Mikhail Vrubel
(1856 - 1910)
Self Portrait. Russian modernist painter
Mikhail Vrubel
(1856 - 1910)
Self Portrait. Russian modernist painter
Franz Kafka
(1883 - 1924)
Austrian writer
Franz Kafka
(1883 - 1924)
Austrian writer
Vincent Van Gogh
(1853 - 1890)
Self Portrait. Dutch postimpressionist painter
Vincent Van Gogh
(1853 - 1890)
Self Portrait. Dutch postimpressionist painter
Emanuel Swedenborg
(1688 - 1772)
The Swedish natural scientist, theosophist, inventor.
Emanuel Swedenborg (1688 - 1772) The Swedish natural scientist, theosophist, inventor.

Ludwig II
(1845 - 1886)
The King of Bavaria
Ludwig II
(1845 - 1886)
The King of Bavaria
Victor Kandinsky
(1849 - 1889)
The Russian psychiatrist and author of
Victor Kandinsky (1849 - 1889) The Russian psychiatrist and author of
THANK YOU FOR YOUR ATTENTION!
THANK YOU FOR YOUR ATTENTION!



 Инфузионная терапия и парентеральное питание
Инфузионная терапия и парентеральное питание Деструктивные формы туберкулеза легких
Деструктивные формы туберкулеза легких Артикуляция и окклюзия. Биомеханика нижней челюсти
Артикуляция и окклюзия. Биомеханика нижней челюсти Клінічні та ЕКГ-ознаки порушень збудливості та провідності
Клінічні та ЕКГ-ознаки порушень збудливості та провідності Самотропты гармонның бұзылысы
Самотропты гармонның бұзылысы Кадровая политика в области здравоохранения
Кадровая политика в области здравоохранения Механическая желтуха
Механическая желтуха Жіті коронарлық синдром
Жіті коронарлық синдром Диагностикалық лапароскопия әдістері
Диагностикалық лапароскопия әдістері Фитотерапия заболеваний мочевыделительной системы
Фитотерапия заболеваний мочевыделительной системы Нарушения поведения при аффективных расстройствах
Нарушения поведения при аффективных расстройствах Гормональные и антигормональные средства. Средства, регулирующие обмен веществ
Гормональные и антигормональные средства. Средства, регулирующие обмен веществ Методы исследования ЖКТ
Методы исследования ЖКТ Законы роста детей
Законы роста детей Синдром подразненого кишечника
Синдром подразненого кишечника Ожоги органа зрения
Ожоги органа зрения Сіреспеге қарсы қолданылатың дәрілік заттарға сипаттама
Сіреспеге қарсы қолданылатың дәрілік заттарға сипаттама Анализ деятельности стационара
Анализ деятельности стационара Клиникалық эпидемиологиядағы биологиялық статистиканың рөлі
Клиникалық эпидемиологиядағы биологиялық статистиканың рөлі АМСЭ – некоммерческая корпоративная организация, объединяющая врачей и специалистов медико-социальной экспертизы
АМСЭ – некоммерческая корпоративная организация, объединяющая врачей и специалистов медико-социальной экспертизы Маскүнемдік, уытқорлық, шылым шегудің патофизиологиялық негіздері
Маскүнемдік, уытқорлық, шылым шегудің патофизиологиялық негіздері Особенности проведения специальной оценки условий труда медицинских работников
Особенности проведения специальной оценки условий труда медицинских работников Демиелинизирующие заболевания нервной системы (ДЗНС)
Демиелинизирующие заболевания нервной системы (ДЗНС) Корь: клиническая диагностика. Противоэпидемические мероприятия
Корь: клиническая диагностика. Противоэпидемические мероприятия Сестринский уход при заболеваниях сердечно-сосудистой системы и системы крови у гериатрических пациентов
Сестринский уход при заболеваниях сердечно-сосудистой системы и системы крови у гериатрических пациентов Порушення гемостазу. Етіологія. Патогенез. Діагностика. Клініка. Принципи лікування
Порушення гемостазу. Етіологія. Патогенез. Діагностика. Клініка. Принципи лікування I.Introduction. Contact transmission mechanism. Prevention of contact infection
I.Introduction. Contact transmission mechanism. Prevention of contact infection Кардиотонические средства
Кардиотонические средства