- Surgical Emergencies in the Newborn

Содержание
- 2. Emergencies Types Airway/Respiratory Intestinal Obstruction Intestinal Perforation Signs Respiratory distress Abdominal distension Peritonitis Pneumoperitoneum
- 3. Airway/Respiratory Neck Masses Cystic Hygromas Tracheal anomalies Thoracic masses/pulmonary lesions Congenital lobar emphysema Overdistension of one
- 4. Cystic Hygroma Multiloculated cystic spaces lined by endothelial cells Separated by fine walls containing numerous smooth
- 5. Cystic Hygroma Complications Respiratory—large hygromas can extend into oropharynx and trachea Inflammation/Infection Hemorrhage Treatment Dependent on
- 6. Cystic Hygroma
- 7. Cystic Hygroma
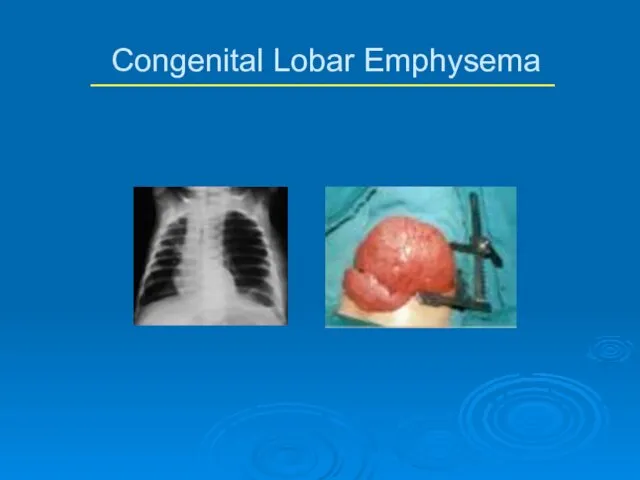
- 8. Postnatal overdistension of one or more lobes of histologically normal lung Probably due to cartilaginous deficiency
- 9. Congenital Lobar Emphysema Diagnosis Usually can be made by plain CXR; Chest CT and V/P scans
- 10. Congenital Lobar Emphysema
- 11. Congenital Cystic Adenomatous Malformation (CCAM) Mass of cysts lined by ciliated cuboidal or columnar pseudostratified epithelium
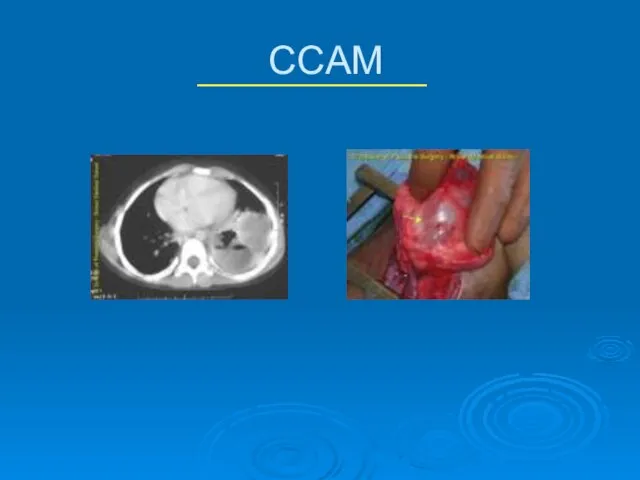
- 12. CCAM Diagnosis CT scan allows differentiation of types Some can be diagnosed on prenatal US Treatment
- 13. CCAM
- 14. Congenital Diaphragmatic Hernia Intro 1 in 200-5000 live births, females >males Etiology unknown Large percentage of
- 16. Tracheoesophageal Fistula and Esophageal Atresia
- 19. Intestinal Obstruction Incidence approx 1 per 500-1000 live births Approx 50% due to atresia or stenosis
- 20. Anatomic Differentiation Upper GI Duodenal atresias/webs small bowel atresias malrotation/midgut volvulus GERD Meconium ileus pyloric stenosis
- 21. Lower GI Colonic atresia Meconium plug Hirschsprung’s Small Left Colon Syndrome Magalocystis-Microcolon-Intestinal Hypoperistalsis Syndrome Imperforate anus
- 22. Urgency to Treat Emergencies Free air on KUB Peritonitis Acute increase in abd distension Clinical deterioration
- 23. Urgency to Treat Further workup Contrast enemas for distal obstructions KUB/Cross-table lateral Milk Scans for GERD
- 24. Common Disorders NEC Duodenal Atresia Small Bowel Atresia Malrotation/Volvulus Hirschsprung’s
- 25. NEC Con’t Presentation distension, tachycardia, lethargy, bilious output, heme pos stools, oliguria DX clinical KUB may
- 26. NEC Treatment Medical NPO, sump tube, Broad Abx after cx’s drawn, serial KUB/lateral x-rays, frequent abd
- 27. NEC Outcomes Overall survival ~ 80%, improving in LBW In pts w/perforation, 65% perioperative mortality, no
- 28. Pneumatosis
- 29. Pneumoperitoneum
- 30. NEC--Abd Distension/Erythema
- 31. Necrotic Segment Ileum
- 32. Resection
- 33. Specimen--Ileocecectomy
- 34. Ileostomy
- 35. Common Disorders NEC Duodenal Atresia Small Bowel Atresia Malrotation Hirschsprung’s
- 36. Duodenal Atresia Incidence--1 in 5,000 to 10,000 live births 75% of stenoses and 40% of atresias
- 37. Duodenal Atresia Con’t Associated Anomalies Down’s (30%) Malrotation Congenital Heart Disease Esophageal Atresia Urinary Tract Malformations
- 38. Duodenal Atresia Diagnosis Radiographs “Double-Bubble” Pyloric dimple sign Absence of “beak” sign seen in pyloric obstruction
- 39. “Double Bubble”
- 40. Duodenal Atresia Treatment Nasogastric decompression, hydration Surgery Double diamond duodenoduodenostomy Con’t prolonged NG decompression, sometimes more
- 41. Common Disorders NEC Duodenal Atresia Small Bowel Atresia Malrotation Hirschsprung’s
- 42. Small Bowel Atresia Jejunal is most common, about 1 per 2,000 live births Atresia due to
- 43. Intestinal Atresia Classification
- 44. Small Bowel Atresia Con’t Associated Anomalies other atresias Hirschsprung’s Biliary atresia polysplenia syndrome (situs inversus, cardiac
- 45. Atresia--Diagnosis and Treatment Plain films show dilated loops small bowel Contrast enema shows small unused colon
- 46. Common Disorders NEC Duodenal Atresia Small Bowel Atresia Malrotation/Volvulus Hirschsprung’s
- 47. Malrotation 1 per 6,000 live births can be asymptomatic throughout life Usually presents in first 6
- 48. Normal Embryology
- 49. Malrotation Classification Nonrotation when neither duodenojejunal or cecocolic limbs undergo correct rotation Abn Rotation of Duodenojejunal
- 50. Abnormal Rotation/Fixation
- 51. Malrotation Diagnosis Varying symptoms from very mild to catastrophic **Bilious emesis is Volvulus until proven otherwise**
- 52. Malrotation UGI
- 53. Intraop Volvulus
- 54. Bowel Necrosis--Volvulus
- 55. Malrotation--Treatment Surgical--Ladd’s Procedure Evisceration Untwisting of volvulus (counterclockwise) Division of Ladd’s Bands Widening mesenteric base Relief
- 56. Common Disorders NEC Duodenal Atresia Small Bowel Atresia Malrotation Hirschsprung’s
- 57. Hirschsprung’s Disease Migratory failure of neural crest cells Incidence 1 in 5,000 live births, males affected
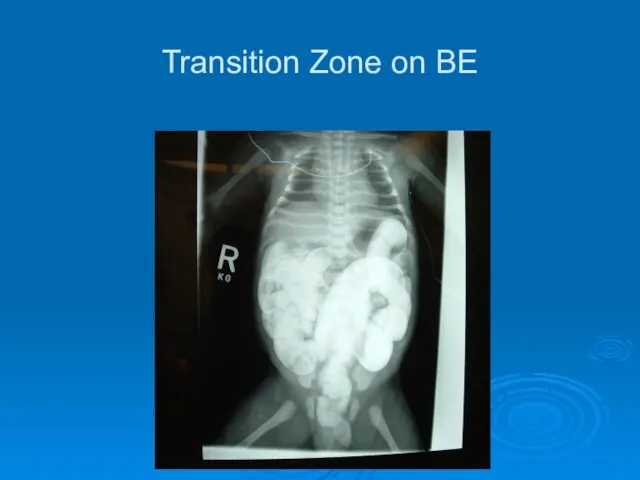
- 58. Hirschsprung’s Diagnosis Barium Enema Transition zone Anorectal Manometry shows failure of reflexive relaxation not very helpful
- 59. Transition Zone on BE
- 60. Hirschsprung’s Treatment In neonates, can do primary pull-through--bringing normal colon down to anorectal junction In older
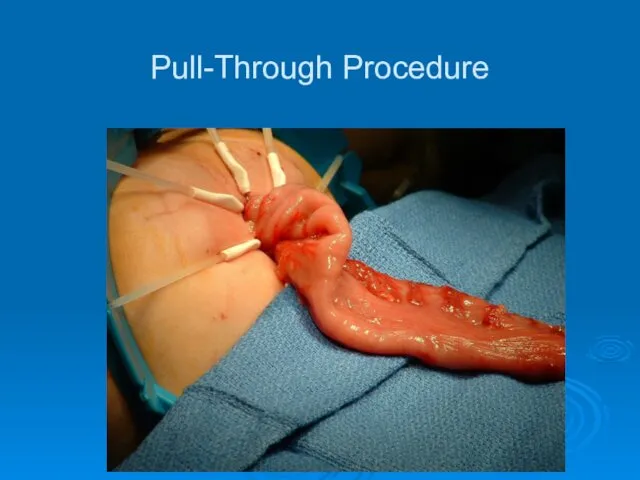
- 61. Pull-Through Procedure
- 64. Скачать презентацию
Emergencies
Types
Airway/Respiratory
Intestinal Obstruction
Intestinal Perforation
Signs
Respiratory distress
Abdominal distension
Peritonitis
Pneumoperitoneum
Emergencies
Types
Airway/Respiratory
Intestinal Obstruction
Intestinal Perforation
Signs
Respiratory distress
Abdominal distension
Peritonitis
Pneumoperitoneum
Airway/Respiratory
Neck Masses
Cystic Hygromas
Tracheal anomalies
Thoracic masses/pulmonary lesions
Congenital lobar emphysema
Overdistension of one or
Airway/Respiratory
Neck Masses
Cystic Hygromas
Tracheal anomalies
Thoracic masses/pulmonary lesions
Congenital lobar emphysema
Overdistension of one or
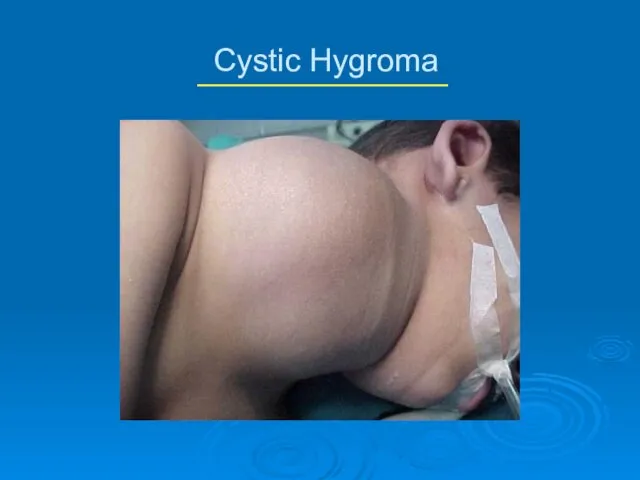
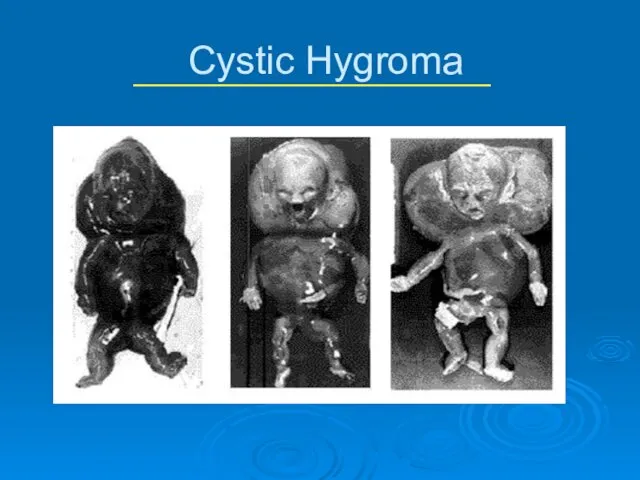
Cystic Hygroma
Multiloculated cystic spaces lined by endothelial cells
Separated by fine walls
Cystic Hygroma
Multiloculated cystic spaces lined by endothelial cells
Separated by fine walls
Cystic Hygroma
Complications
Respiratory—large hygromas can extend into oropharynx and trachea
Inflammation/Infection
Hemorrhage
Treatment
Dependent on size,
Cystic Hygroma
Complications
Respiratory—large hygromas can extend into oropharynx and trachea
Inflammation/Infection
Hemorrhage
Treatment
Dependent on size,
Cystic Hygroma
Cystic Hygroma
Cystic Hygroma
Cystic Hygroma
Postnatal overdistension of one or more lobes of histologically normal lung
Probably
Postnatal overdistension of one or more lobes of histologically normal lung
Probably
Congenital Lobar Emphysema
Diagnosis
Usually can be made by plain CXR; Chest CT
Congenital Lobar Emphysema
Diagnosis
Usually can be made by plain CXR; Chest CT
Congenital Lobar Emphysema
Congenital Lobar Emphysema
Congenital Cystic Adenomatous Malformation (CCAM)
Mass of cysts lined by ciliated cuboidal
Congenital Cystic Adenomatous Malformation (CCAM)
Mass of cysts lined by ciliated cuboidal
CCAM
Diagnosis
CT scan allows differentiation of types
Some can be diagnosed on prenatal
CCAM
Diagnosis
CT scan allows differentiation of types
Some can be diagnosed on prenatal
CCAM
CCAM
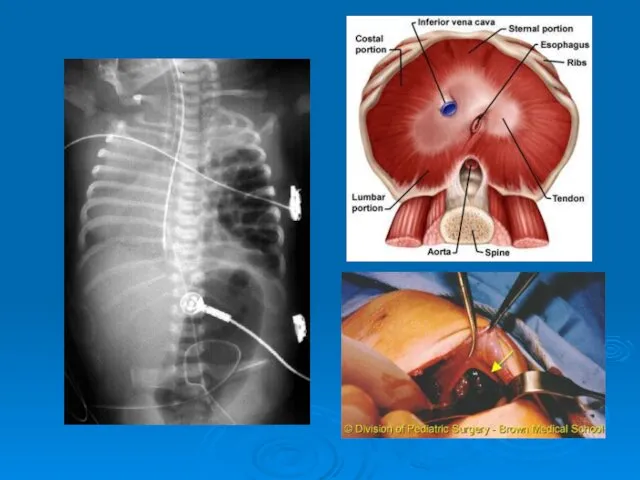
Congenital Diaphragmatic Hernia
Intro
1 in 200-5000 live births, females >males
Etiology unknown
Large percentage
Congenital Diaphragmatic Hernia
Intro
1 in 200-5000 live births, females >males
Etiology unknown
Large percentage
Tracheoesophageal Fistula and Esophageal Atresia
Tracheoesophageal Fistula and Esophageal Atresia


Intestinal Obstruction
Incidence approx 1 per 500-1000 live births
Approx 50% due to
Intestinal Obstruction
Incidence approx 1 per 500-1000 live births
Approx 50% due to
Anatomic Differentiation
Upper GI
Duodenal atresias/webs
small bowel atresias
malrotation/midgut volvulus
GERD
Meconium ileus
pyloric stenosis
Inguinal hernia
NEC
Anatomic Differentiation
Upper GI
Duodenal atresias/webs
small bowel atresias
malrotation/midgut volvulus
GERD
Meconium ileus
pyloric stenosis
Inguinal hernia
NEC
Lower GI
Colonic atresia
Meconium plug
Hirschsprung’s
Small Left Colon Syndrome
Magalocystis-Microcolon-Intestinal Hypoperistalsis Syndrome
Imperforate anus
Anatomic Differentiation
Lower GI
Colonic atresia
Meconium plug
Hirschsprung’s
Small Left Colon Syndrome
Magalocystis-Microcolon-Intestinal Hypoperistalsis Syndrome
Imperforate anus
Anatomic Differentiation
Urgency to Treat
Emergencies
Free air on KUB
Peritonitis
Acute increase in abd distension
Clinical deterioration
Urgency to Treat
Emergencies
Free air on KUB
Peritonitis
Acute increase in abd distension
Clinical deterioration
Urgency to Treat
Further workup
Contrast enemas for distal obstructions
KUB/Cross-table lateral
Milk Scans
Urgency to Treat
Further workup
Contrast enemas for distal obstructions
KUB/Cross-table lateral
Milk Scans
Common Disorders
NEC
Duodenal Atresia
Small Bowel Atresia
Malrotation/Volvulus
Hirschsprung’s
Common Disorders
NEC
Duodenal Atresia
Small Bowel Atresia
Malrotation/Volvulus
Hirschsprung’s
NEC Con’t
Presentation
distension, tachycardia, lethargy, bilious output, heme pos stools, oliguria
DX
clinical
KUB may
NEC Con’t
Presentation
distension, tachycardia, lethargy, bilious output, heme pos stools, oliguria
DX
clinical
KUB may
NEC Treatment
Medical
NPO, sump tube, Broad Abx after cx’s drawn, serial KUB/lateral
NEC Treatment
Medical
NPO, sump tube, Broad Abx after cx’s drawn, serial KUB/lateral
NEC Outcomes
Overall survival ~ 80%, improving in LBW
In pts w/perforation, 65%
NEC Outcomes
Overall survival ~ 80%, improving in LBW
In pts w/perforation, 65%
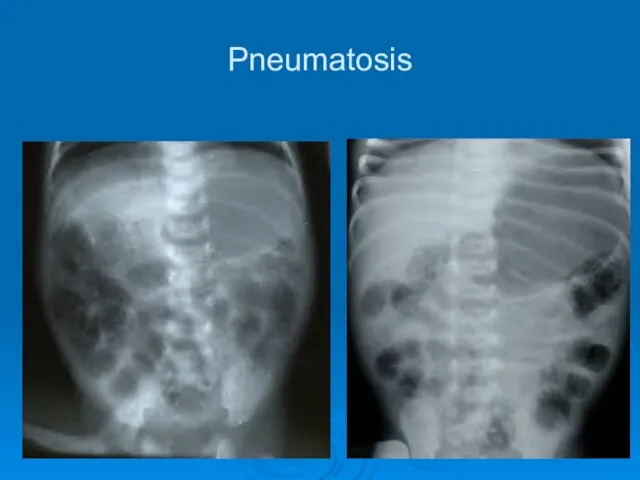
Pneumatosis
Pneumatosis
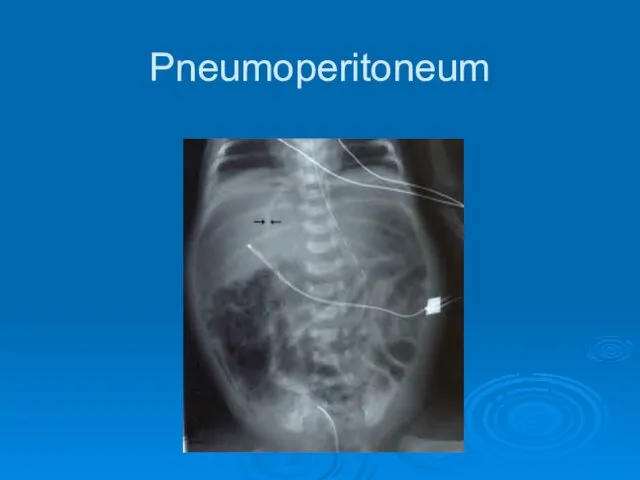
Pneumoperitoneum
Pneumoperitoneum
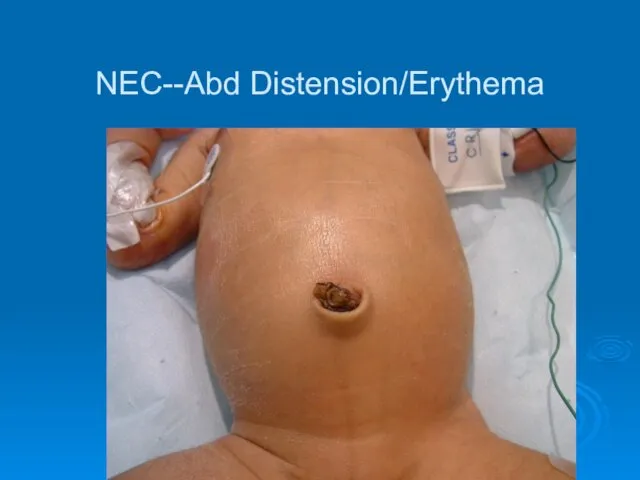
NEC--Abd Distension/Erythema
NEC--Abd Distension/Erythema
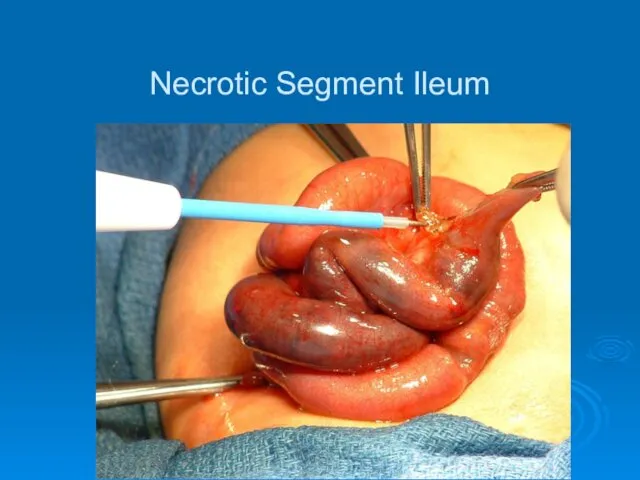
Necrotic Segment Ileum
Necrotic Segment Ileum

Resection
Resection
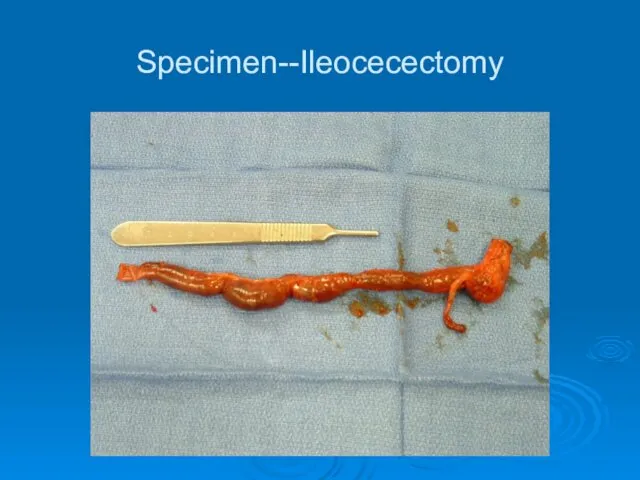
Specimen--Ileocecectomy
Specimen--Ileocecectomy

Ileostomy
Ileostomy
Common Disorders
NEC
Duodenal Atresia
Small Bowel Atresia
Malrotation
Hirschsprung’s
Common Disorders
NEC
Duodenal Atresia
Small Bowel Atresia
Malrotation
Hirschsprung’s
Duodenal Atresia
Incidence--1 in 5,000 to 10,000 live births
75% of stenoses and
Duodenal Atresia
Incidence--1 in 5,000 to 10,000 live births
75% of stenoses and
Duodenal Atresia Con’t
Associated Anomalies
Down’s (30%)
Malrotation
Congenital Heart Disease
Esophageal Atresia
Urinary Tract Malformations
Anorectal malformations
VACTERL
Duodenal Atresia Con’t
Associated Anomalies
Down’s (30%)
Malrotation
Congenital Heart Disease
Esophageal Atresia
Urinary Tract Malformations
Anorectal malformations
VACTERL
Duodenal Atresia Diagnosis
Radiographs
“Double-Bubble”
Pyloric dimple sign
Absence of “beak” sign seen in pyloric
Duodenal Atresia Diagnosis
Radiographs
“Double-Bubble”
Pyloric dimple sign
Absence of “beak” sign seen in pyloric
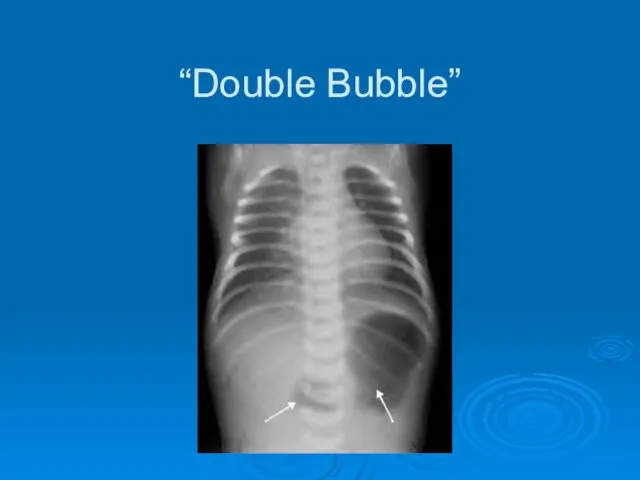
“Double Bubble”
“Double Bubble”
Duodenal Atresia Treatment
Nasogastric decompression, hydration
Surgery
Double diamond duodenoduodenostomy
Con’t prolonged NG decompression, sometimes
Duodenal Atresia Treatment
Nasogastric decompression, hydration
Surgery
Double diamond duodenoduodenostomy
Con’t prolonged NG decompression, sometimes
Common Disorders
NEC
Duodenal Atresia
Small Bowel Atresia
Malrotation
Hirschsprung’s
Common Disorders
NEC
Duodenal Atresia
Small Bowel Atresia
Malrotation
Hirschsprung’s
Small Bowel Atresia
Jejunal is most common, about 1 per 2,000 live
Small Bowel Atresia
Jejunal is most common, about 1 per 2,000 live
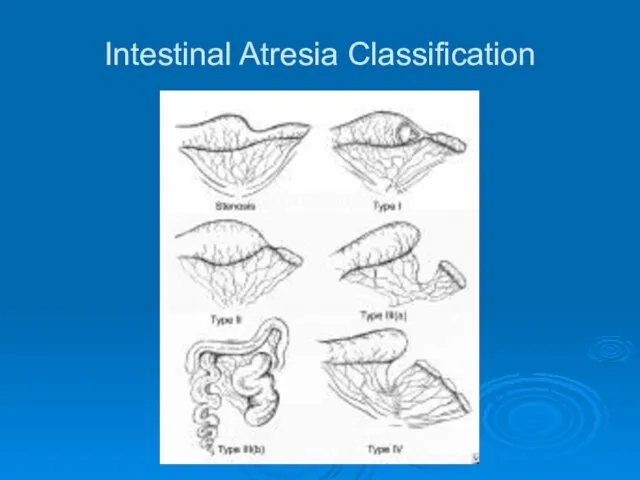
Intestinal Atresia Classification
Intestinal Atresia Classification
Small Bowel Atresia Con’t
Associated Anomalies
other atresias
Hirschsprung’s
Biliary atresia
polysplenia syndrome (situs inversus, cardiac
Small Bowel Atresia Con’t
Associated Anomalies
other atresias
Hirschsprung’s
Biliary atresia
polysplenia syndrome (situs inversus, cardiac
Atresia--Diagnosis and Treatment
Plain films show dilated loops small bowel
Contrast enema shows
Atresia--Diagnosis and Treatment
Plain films show dilated loops small bowel
Contrast enema shows
Common Disorders
NEC
Duodenal Atresia
Small Bowel Atresia
Malrotation/Volvulus
Hirschsprung’s
Common Disorders
NEC
Duodenal Atresia
Small Bowel Atresia
Malrotation/Volvulus
Hirschsprung’s
Malrotation
1 per 6,000 live births
can be asymptomatic throughout life
Usually presents in
Malrotation
1 per 6,000 live births
can be asymptomatic throughout life
Usually presents in
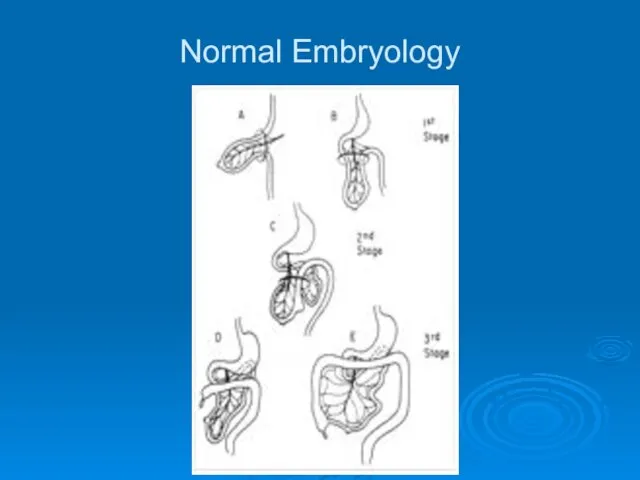
Normal Embryology
Normal Embryology
Malrotation Classification
Nonrotation
when neither duodenojejunal or cecocolic limbs undergo correct rotation
Abn Rotation
Malrotation Classification
Nonrotation
when neither duodenojejunal or cecocolic limbs undergo correct rotation
Abn Rotation
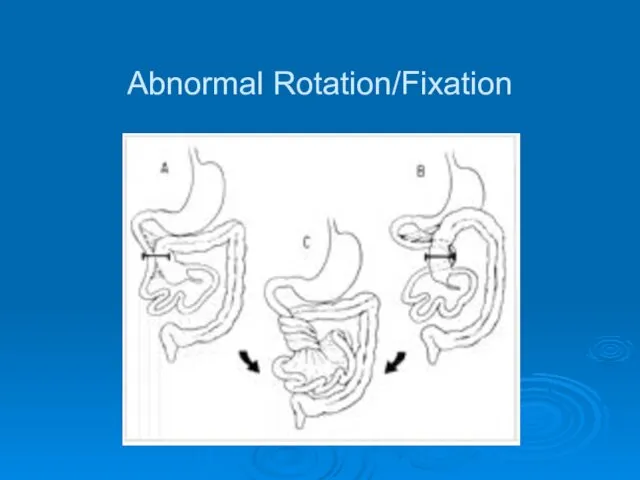
Abnormal Rotation/Fixation
Abnormal Rotation/Fixation
Malrotation Diagnosis
Varying symptoms from very mild to catastrophic
**Bilious emesis is Volvulus
Malrotation Diagnosis
Varying symptoms from very mild to catastrophic
**Bilious emesis is Volvulus
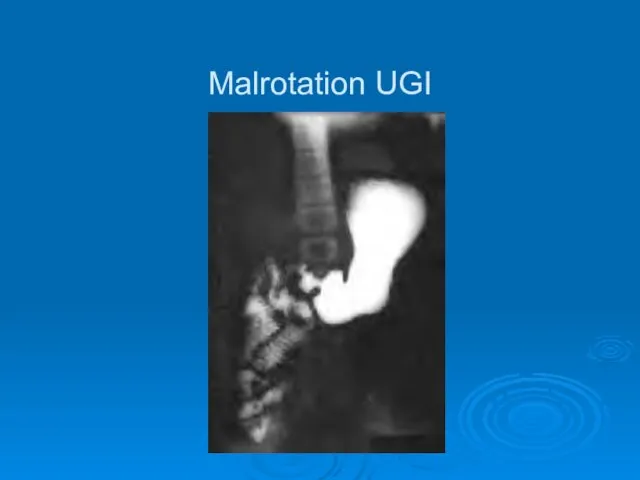
Malrotation UGI
Malrotation UGI
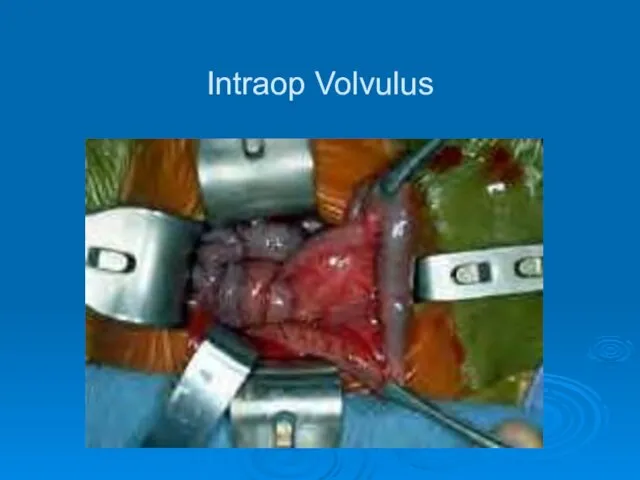
Intraop Volvulus
Intraop Volvulus
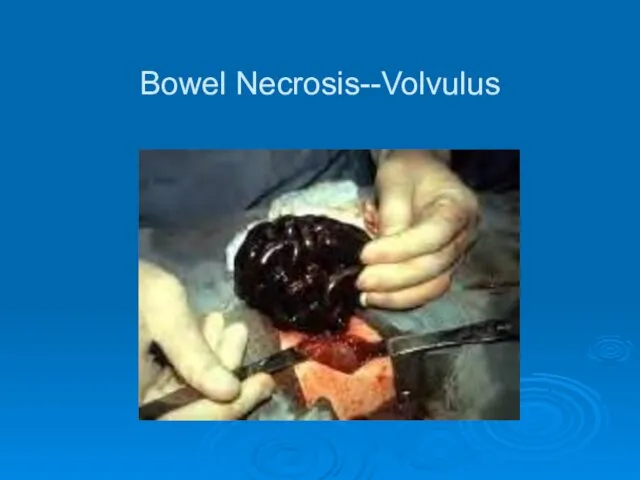
Bowel Necrosis--Volvulus
Bowel Necrosis--Volvulus

Malrotation--Treatment
Surgical--Ladd’s Procedure
Evisceration
Untwisting of volvulus (counterclockwise)
Division of Ladd’s Bands
Widening mesenteric base
Relief of
Malrotation--Treatment
Surgical--Ladd’s Procedure
Evisceration
Untwisting of volvulus (counterclockwise)
Division of Ladd’s Bands
Widening mesenteric base
Relief of
Common Disorders
NEC
Duodenal Atresia
Small Bowel Atresia
Malrotation
Hirschsprung’s
Common Disorders
NEC
Duodenal Atresia
Small Bowel Atresia
Malrotation
Hirschsprung’s
Hirschsprung’s Disease
Migratory failure of neural crest cells
Incidence 1 in 5,000 live
Hirschsprung’s Disease
Migratory failure of neural crest cells
Incidence 1 in 5,000 live
Hirschsprung’s Diagnosis
Barium Enema
Transition zone
Anorectal Manometry
shows failure of reflexive relaxation
not very helpful
Hirschsprung’s Diagnosis
Barium Enema
Transition zone
Anorectal Manometry
shows failure of reflexive relaxation
not very helpful
Transition Zone on BE
Transition Zone on BE
Hirschsprung’s Treatment
In neonates, can do primary pull-through--bringing normal colon down to
Hirschsprung’s Treatment
In neonates, can do primary pull-through--bringing normal colon down to
Pull-Through Procedure
Pull-Through Procedure

 Психологические особенности женщин на этапе подготовки ЭКО (психоаналитический подход)
Психологические особенности женщин на этапе подготовки ЭКО (психоаналитический подход) Клиническая эпидемиология
Клиническая эпидемиология Язвенно-некротический энтероколит новорожденных
Язвенно-некротический энтероколит новорожденных Первичные вирусные энцефалиты у детей
Первичные вирусные энцефалиты у детей Анатомо-физиологические особенности строения полости рта новорожденного
Анатомо-физиологические особенности строения полости рта новорожденного Вірус віспи
Вірус віспи Принципы гигиенической регламентации химических веществ
Принципы гигиенической регламентации химических веществ Биологические эффекты воздействия ионизирующего излучения на организм человека
Биологические эффекты воздействия ионизирующего излучения на организм человека Смерть клиническая и биологическая
Смерть клиническая и биологическая Алгоритмы диагностики в общей врачебной практике, семейной медицине
Алгоритмы диагностики в общей врачебной практике, семейной медицине КОГБУЗ Яранская центральная районная больница
КОГБУЗ Яранская центральная районная больница Тромбоз. Причины, диагностика
Тромбоз. Причины, диагностика Трихоцефалёз. Этиология. Клиника. Диагностика. Лечение
Трихоцефалёз. Этиология. Клиника. Диагностика. Лечение Технология гомеопатических таблеток. Викторина
Технология гомеопатических таблеток. Викторина Воспалительные заболевания женских половых органов
Воспалительные заболевания женских половых органов Методы оценки удовлетворенности пациента качеством предоставленных медицинских услуг
Методы оценки удовлетворенности пациента качеством предоставленных медицинских услуг Пролиферациялық қабыну
Пролиферациялық қабыну Бешенство
Бешенство Профилактика ОРВИ и гриппа
Профилактика ОРВИ и гриппа Ұйқы физилогиясы.Ұйқы фазасы,бұзылысы және емдеу әдісі
Ұйқы физилогиясы.Ұйқы фазасы,бұзылысы және емдеу әдісі Развитие глотки, пищевода, желудка, кишечника
Развитие глотки, пищевода, желудка, кишечника Ретинобластома – злокачественная опухоль сетчатки глаза
Ретинобластома – злокачественная опухоль сетчатки глаза Внебольничные пневмонии и грипп
Внебольничные пневмонии и грипп Терминальные состояния
Терминальные состояния Трансвагинальная эхография в первом триместре беременности
Трансвагинальная эхография в первом триместре беременности Лучевое исследование легких
Лучевое исследование легких ДВС-синдром. ТЭЛА
ДВС-синдром. ТЭЛА