The anatomical and physiological particularities of cardiovascular system in children and their clinical importance презентация
- The anatomical and physiological particularities of cardiovascular system in children and their clinical importance

Содержание
- 2. The heart and large blood vessels appears at the 3-rd week of the embrionic phase. The
- 3. Briefly the process of heart and large blood vessels embryogenesis can be described as a complex
- 4. In this time the simultaneous embrionic heart migration proseedes from the neck`s area of embryo into
- 5. Heart congenital abnormalities It is important to confess that embryo heart during at list the 1-st
- 6. Embryopathyes. Develop within first 9 weeks of gastation Are usually severe diseases Show huge anatomical abnormalities
- 7. Heart ecthopia Newborn male with thoracoabdominal ectopia cordis (Cantrell pentalogy). Flaring of the lower thoracic cavity
- 9. dextrocardy
- 10. Ultrasound investigation in utero By means of ultrasound investigation method it is possible to define embryo
- 11. Fethophaties The 3-rd month old normal fetus has an already wholly formed heart. If congenital heart
- 12. The existence of Fethophaties may by explained from position of the fetus blood circulation.
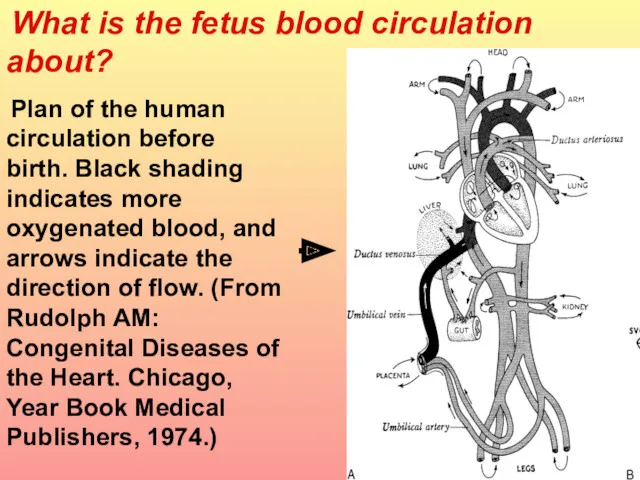
- 13. What is the fetus blood circulation about? Plan of the human circulation before birth. Black shading
- 14. The fetus type of blood circulation is defined by placenta existence before the birth. Placenta is
- 15. The pump function of fetus heart and two arteries connected with fetus aorta in place of
- 16. After delivery the umbilical cord crossing (cut) usually has to be done. Immediately after the umbilical
- 17. The abnormalities of the umbilical cord are indicative for different congenital internal organs abnormalities especially kidneys.
- 18. The first phenomenon is a splitting umbilical vein on two venous vessels. One falls into portal
- 19. The second phenomenon: in right atrium the umbilical blood flow by miraculous reason does not mingle
- 20. The third phenomenon: in the rising aorta and big arteries leaving from it there is an
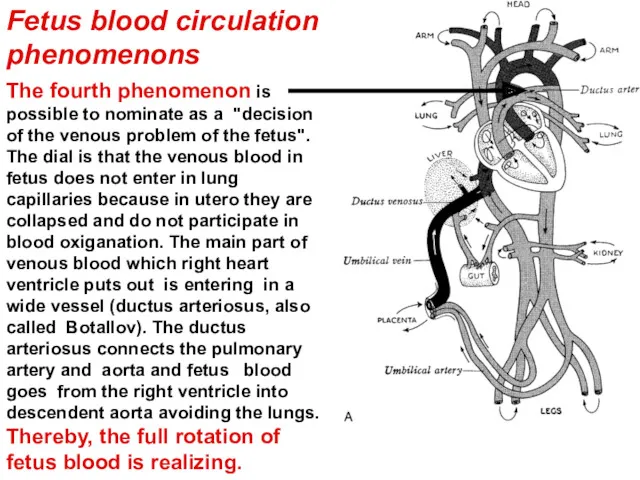
- 21. Fetus blood circulation phenomenons The fourth phenomenon is possible to nominate as a "decision of the
- 22. After birth the ductus venosus and umbilical vessels obliterate and from the second week of life
- 23. The ductus arteriosus and foramen ovale close for several seconds or minutes after birth. Their complete
- 24. Morphological and functional particularities of the heart and blood vessels in children.
- 25. The heart size The heart of the fetus or newborn is comparatively greater that one in
- 26. The myocardial infarction in children is a casuistry Heart coronary arteries before age two are distributed
- 27. The myocardium. In small children the heart myocytes are fine, have not transverse lines and contain
- 28. The nerviouse system supplementation of the heart is realized through surface and deep plexuses combination formed
- 29. The premature heart bites The premature heart bites (extrasystoles) if they are not occurring often also
- 30. The heart rate In children the heart rate is very changeable due to different physiological and
- 31. Characterizing anatomical and physiological particularities of children heart it is necessary to underline its high level
- 32. The vessels conduct and distribute the blood on organ and tissues. The acute difficiency of blood
- 33. By origin the shock can be cardiogenic connected with low heart out-put looks like a deficiency
- 34. The clinical study of cardiovascular system.
- 35. The cardiovascular dependent complaints in children are very unspecific. Especially they are doubtful when the child
- 36. The physical load intolerance complaint In children the big clinical importance in diagnostics of cardiovascular diseases
- 37. The heart rate, arterial blood pressure The clinical characteristics of cardiovascular system pertain to vitality-important signs
- 38. The normal frequency of pulse is changing depending on age: - in newborns 120 - 140
- 39. Pulse count An important practical remark consists in necessary to create for the patient a standard
- 40. Pulse count The pulse rate also depends on the body temperature. In fever the pulse usually
- 41. In children the arterial blood pressure (BP) is measured less often then in adults. It is
- 42. The Normal values of arterial blood pressure depend on the child age and should be approximately
- 43. Current cardiac examination is made in 4 steps.
- 45. I. The inspection of heart area allows to reveal following symptoms: Precordial bulge, which is indicative
- 46. II. Palpation is important for determination: Apex beat. It is shifted downwards and outwards in LVH
- 47. III. Percussion. The percussion of cardiac borders is obsolete now in modern cardiology. It can not
- 48. It should be made on the four cardiac areas and on the left parasternal area (see
- 49. The clinical comment of auscultation shold include next characteristics: The heart sounds. Normal heart sounds can
- 50. The clinical comment of auscultation shold include next characteristics: Murmurs. Their comment should include the next
- 51. The clinical comment of auscultation shold include next characteristics: Pericardial rub. It is a friction sound
- 52. The heart sounds can be visualized in paper or electronic screen by phonocardiography method. Phonocardiogram allows
- 53. For successful diagnostics of cardiovascular diseases in children it is necessary to master several acceptances of
- 54. Cyanosis is defined as skin or mucosa bluishness. Acute cyanosis with respiratory distress is observed in
- 55. A femoral pulsation or palpation of the pulse on hip artery is important sign. Weak or
- 56. The syndrome of congestive heart failure is formed from specific signs. It can be acute or
- 57. In acute failure, the cardinal triad is tachycardia, tachypnea and enlarged and tender liver. 1. Tachycardia
- 58. In chronic failure: 1. Exertional dyspnea is present. The breathlessness appears in response to physical load,
- 59. The Semiotics of the commonest diseases of cardiovascular system in children.
- 60. The Fallot`s Tetralogy is a one of the commonest congenital heart diseases being accompanied by cyanosis.
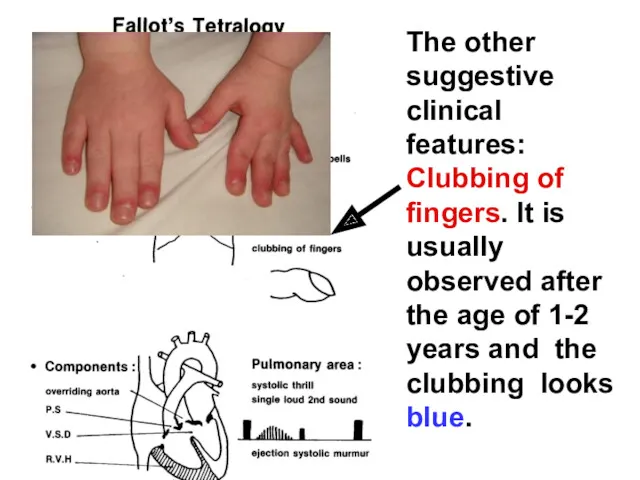
- 61. The Biological heart defects of this congenital abnormality are the following: 1. Intermediate position of the
- 62. The semiotics reflect pathophysiological changes occurring in this congenital heart disease. In advanced stage of disease
- 63. High hemoglobin The compensaroty hemoglobin and erythrocytes elevation reachs the level nearly double exceeding the normal.
- 64. Hypercyanotic spells They are attacks of deep cyanosis and respiratory distress which may by precipitated by
- 65. The other suggestive clinical features: Clubbing of fingers. It is usually observed after the age of
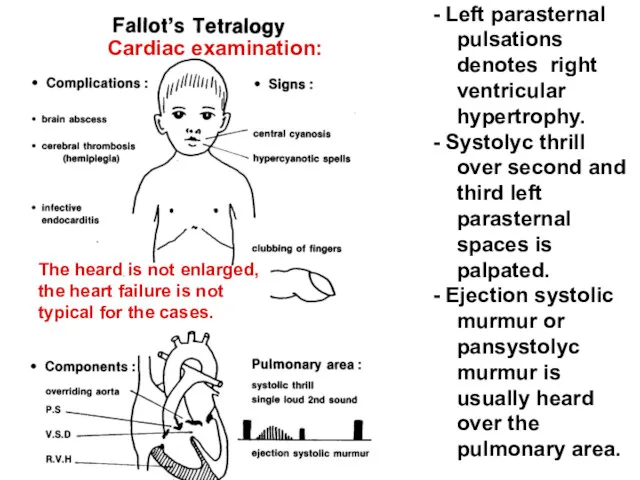
- 66. - Left parasternal pulsations denotes right ventricular hypertrophy. - Systolyc thrill over second and third left
- 67. The additional clinical investigations. Chest X-ray shows pulmonary oligemia, normal sized heart, prominent right ventricle with
- 68. The guidelines of care for the sick children. When the hypercyanotic spell happens it is necessary
- 69. The Ventricular septal defect (VSD) is the most spread congenital heart disease as it accounts 30%
- 70. Patients with VSD are frequently asymptomatic and the condition is accidentally discovers on routine cardiac examination.
- 71. Murmur, VSD! Healthy!
- 72. Semiotics of V.S.D. Characteristic murmur is pansystolic, loud, harsh, and left parasternal mainly over 3rd and
- 73. The manifestations of CHF may by chronic or acute. Chronic CHF appears gradually in the form
- 74. Other diagnostic approaches Diagnostic echocardiography demonstrates the septal defect, its size as well as the degree
- 75. Presence of cardiomegaly or congestive heart failure in infancy is an indication for early surgical intervention
- 76. A) Preoperative roentgenogram in a ventricular septal defect with a large left-to-right shunt and pulmonary hypertension.
- 77. The guidelines of care for sick children. The children sufferring from VSD with chronic congestive heart
- 78. The atrial septal defect (ASD) The atrial septal defect (ASD) is other one of the wide-spread
- 79. Symptoms of ASD 1. The systolic murmur over the pulmonary area is usually heard. It is
- 81. The other causes of ejection systolic murmur 1. Innocent (functional, non-malignant) systolic murmur is faint, soft
- 82. The guidelines of care for sick children with ASD. They are the same as discussing before
- 83. Symptoms PDA. - Continuous machinery murmur. It is maximally heard over the pulmonary area and may
- 84. Other diagnostic approaches Echcardiography reveals increased left atrial and left ventricular sizes. UltraSound-Scanning from the suprasternal
- 85. Chest X-Ray in a patient with PDA. The heart size is normal, the pulmonary artery segment
- 86. The Rheumatism (rheumatic fever) is an autoimmune disease, which develops as complication of streptococcal infections (pharyngitis
- 87. Jones`s criteria 5 Jones`s criterias (or clinical manifestations) are generally used for diagnosis of rheumatic fever.
- 88. Major criteria (Jones`s criteria or manifestations) of rheumatic fever. 1/ Polyarthritis occurs in 75% of cases.
- 89. Major criteria (Jones`s criteria or manifestations) of rheumatic fever. 2/ Carditis occurs in 50% of cases.
- 90. Major criteria (Jones`s criteria or manifestations) of rheumatic fever. 3/ Reumatic chorea. The chorea is the
- 91. Major criteria (Jones`s criteria or manifestations) of rheumatic fever. 4/ Erythema marginatum (annular erythema) revels in
- 92. Major criteria (Jones`s criteria or manifestations) of rheumatic fever. 5/ Subcutaneous nodules. It can be found
- 93. The Chronic rheumatic heart disease is a continuation of the acute rheumatic fever and is characterized
- 94. Recognition of the valvular lesions depends on auscultation of the characteristic murmur. Mitral incompetence (M.I.). An
- 95. Mitral stenosis (M.S.). An apical mid-diastolic rumbling murmur is present. Simultaneously the right ventricular hypertrophy (RVH)
- 96. Aortic incompetence. A soft and bloving diastolic murmur is heard over aortic area. The left ventricular
- 97. Aortic stenosis. A harsh and loud ejection systolic murmur is heard over aortic area. It usually
- 98. Atrial flatter
- 99. Ventricular premature bites (exstrasystols)
- 100. AV - block
- 101. ABC program of cardio-pulmonary and cerebral resuscitation The sudden cardial arrest for several minutes leads a
- 102. The principles of resuscitation are: to restore air-ways ability for air pass (A), organize artificial lung
- 103. to make rhythmic squeexing of the thorax capable to provide blood circulation in a heart chambers
- 105. Скачать презентацию
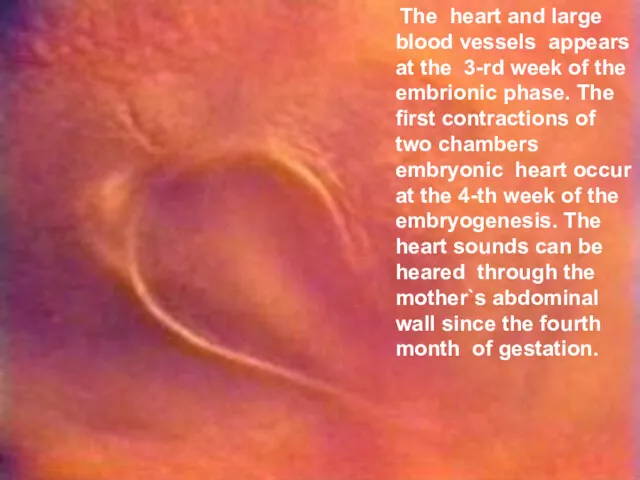
The heart and large blood vessels appears at the
The heart and large blood vessels appears at the
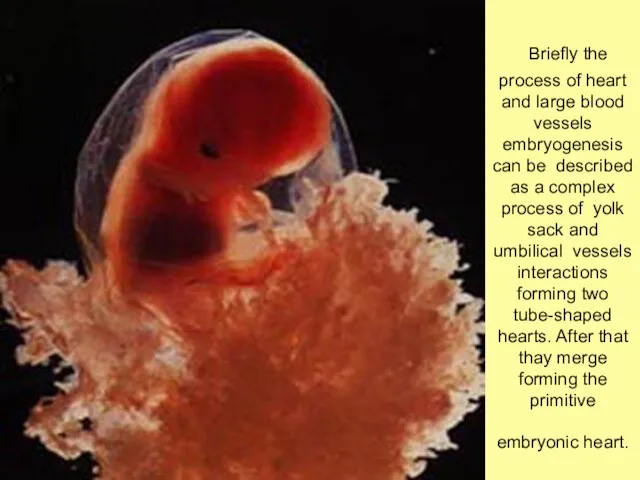
Briefly the process of heart and large blood vessels embryogenesis
Briefly the process of heart and large blood vessels embryogenesis
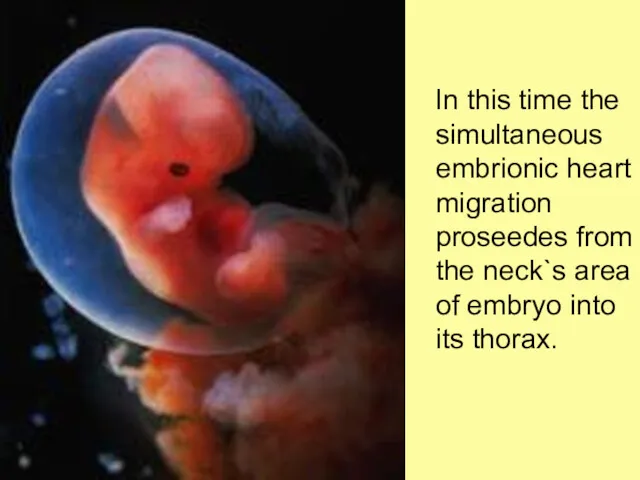
In this time the simultaneous embrionic heart migration proseedes from the
Heart congenital abnormalities
It is important to confess that embryo heart during
Heart congenital abnormalities
It is important to confess that embryo heart during
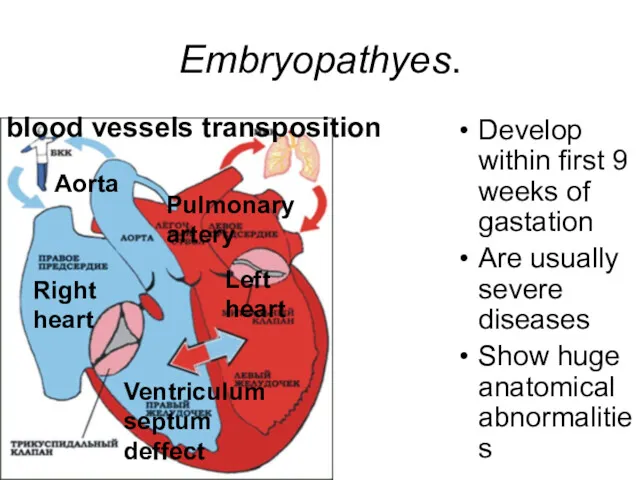
Embryopathyes.
Develop within first 9 weeks of gastation
Are usually severe diseases
Show
Embryopathyes.
Develop within first 9 weeks of gastation
Are usually severe diseases
Show
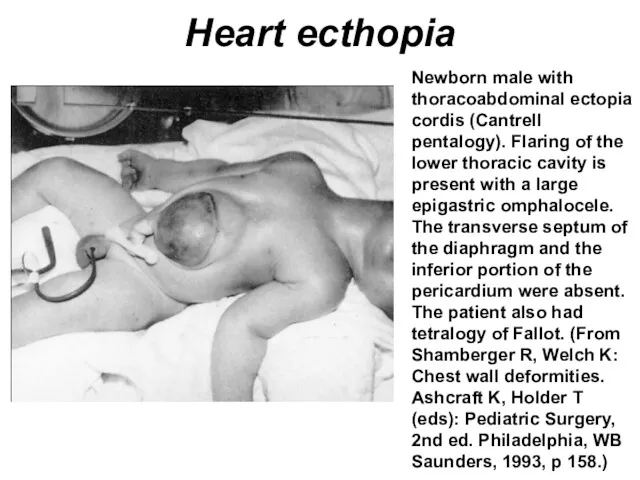
Heart ecthopia
Newborn male with thoracoabdominal ectopia cordis (Cantrell pentalogy). Flaring
Heart ecthopia
Newborn male with thoracoabdominal ectopia cordis (Cantrell pentalogy). Flaring

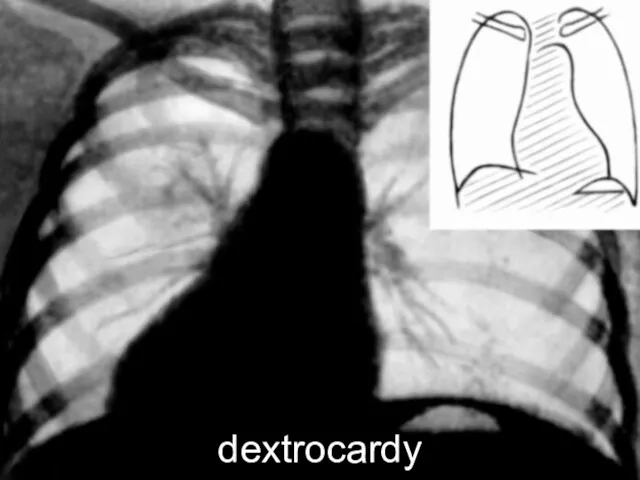
dextrocardy
dextrocardy
Ultrasound investigation in utero
By means of ultrasound investigation method it is
Ultrasound investigation in utero
By means of ultrasound investigation method it is
Fethophaties
The 3-rd month old normal fetus has an already wholly formed
Fethophaties
The 3-rd month old normal fetus has an already wholly formed
The existence of Fethophaties may by explained from position of
The existence of Fethophaties may by explained from position of
What is the fetus blood circulation about?
Plan of the
What is the fetus blood circulation about?
Plan of the
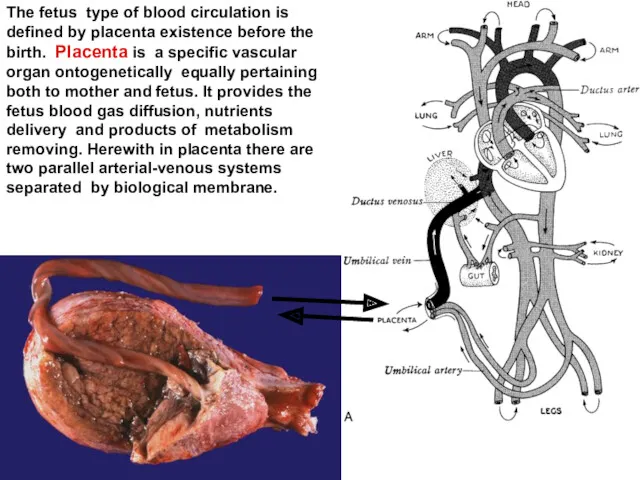
The fetus type of blood circulation is defined by placenta existence
The fetus type of blood circulation is defined by placenta existence
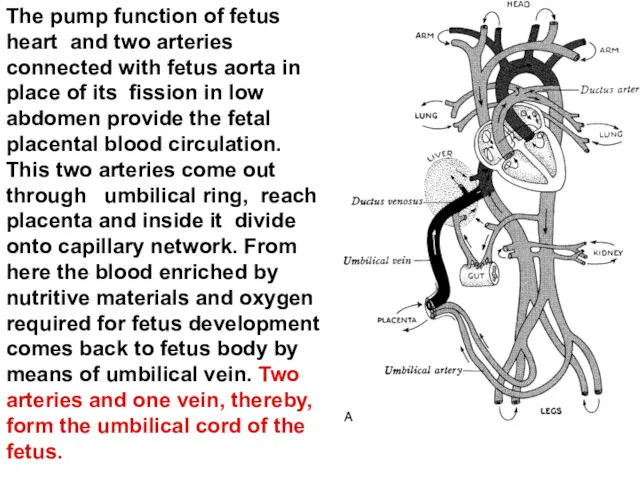
The pump function of fetus heart and two arteries connected with
The pump function of fetus heart and two arteries connected with
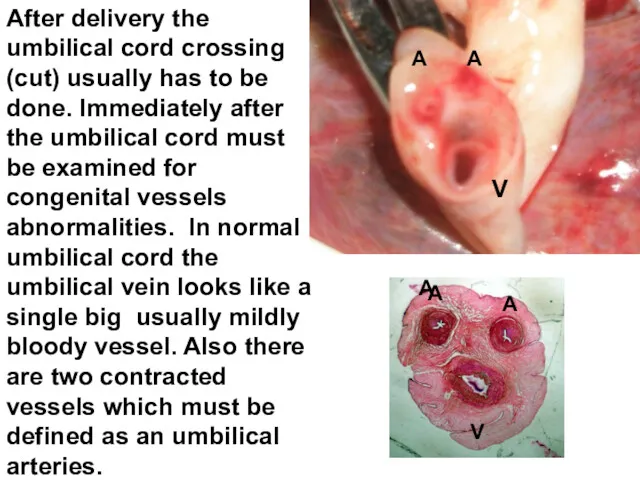
After delivery the umbilical cord crossing (cut) usually has to be
After delivery the umbilical cord crossing (cut) usually has to be
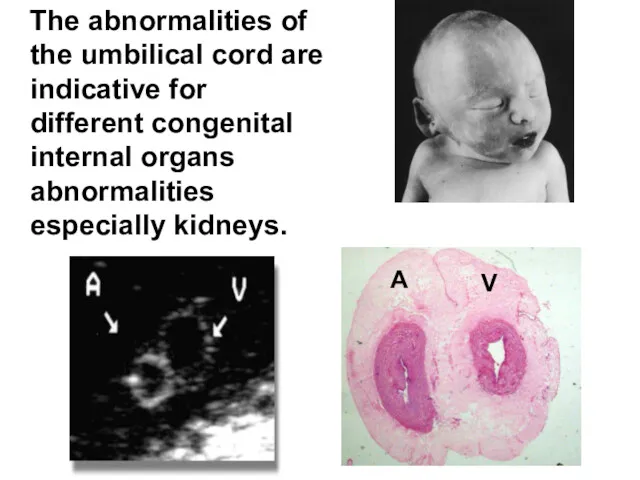
The abnormalities of the umbilical cord are indicative for different
The abnormalities of the umbilical cord are indicative for different
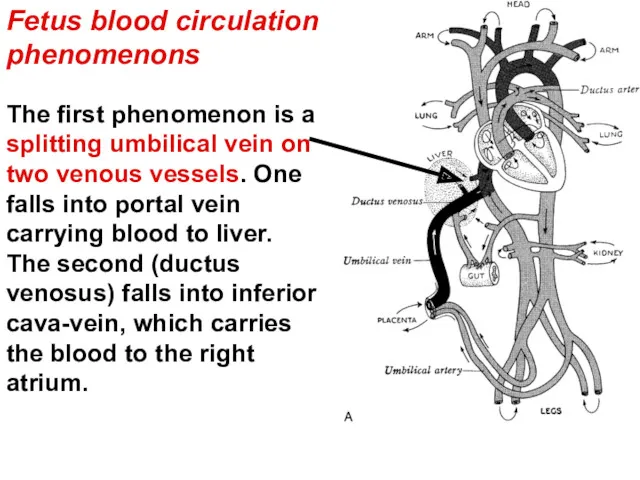
The first phenomenon is a splitting umbilical vein on two venous
The first phenomenon is a splitting umbilical vein on two venous
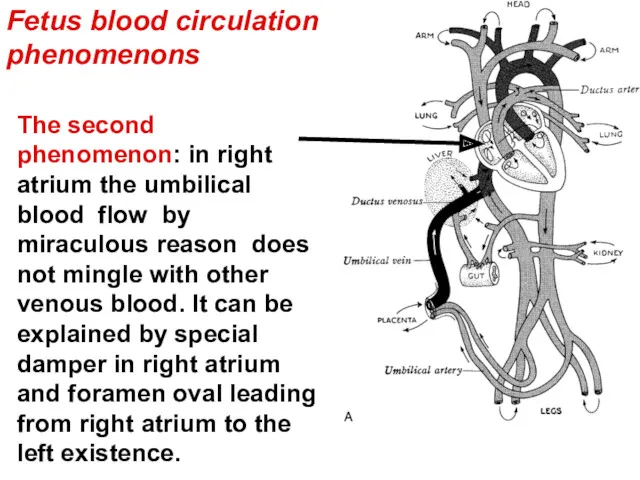
The second phenomenon: in right atrium the umbilical blood flow by
The second phenomenon: in right atrium the umbilical blood flow by
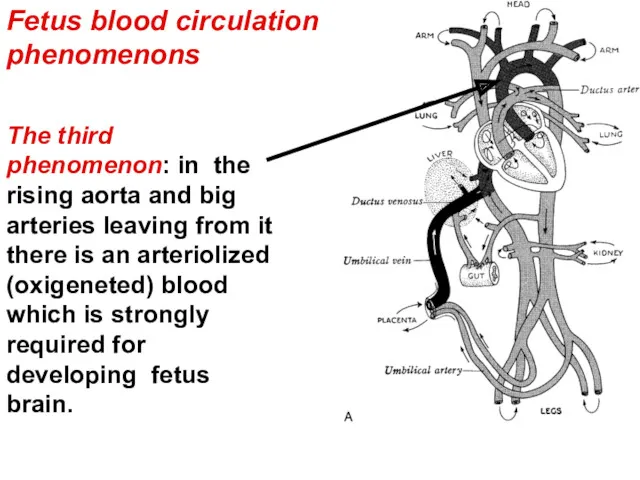
The third phenomenon: in the rising aorta and big arteries leaving
The third phenomenon: in the rising aorta and big arteries leaving
Fetus blood circulation phenomenons
The fourth phenomenon is possible to nominate as
Fetus blood circulation phenomenons
The fourth phenomenon is possible to nominate as
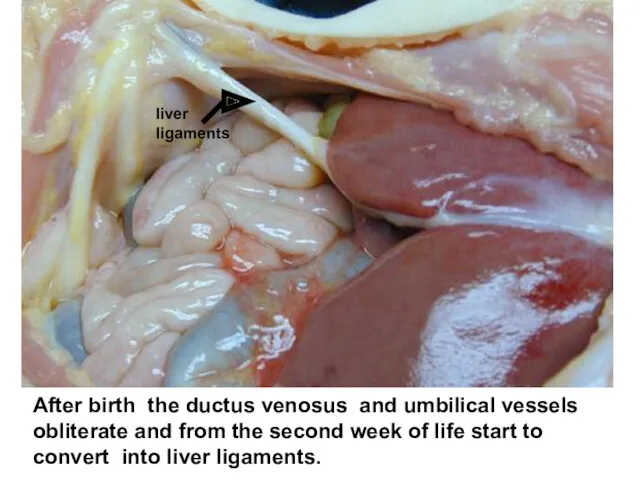
After birth the ductus venosus and umbilical vessels obliterate and from
After birth the ductus venosus and umbilical vessels obliterate and from
The ductus arteriosus and foramen ovale close for several seconds or
The ductus arteriosus and foramen ovale close for several seconds or
Morphological and functional particularities of the heart and blood vessels in
Morphological and functional particularities of the heart and blood vessels in
The heart size
The heart of the fetus or newborn is
The heart size
The heart of the fetus or newborn is
The myocardial infarction in children is a casuistry
Heart coronary arteries
The myocardial infarction in children is a casuistry
Heart coronary arteries
The myocardium.
In small children the heart myocytes are fine, have
The myocardium.
In small children the heart myocytes are fine, have
The nerviouse system supplementation of the heart
is realized through surface
The nerviouse system supplementation of the heart
is realized through surface
The premature heart bites
The premature heart bites (extrasystoles) if they are
The premature heart bites
The premature heart bites (extrasystoles) if they are
The heart rate
In children the heart rate is very changeable due
The heart rate
In children the heart rate is very changeable due
Characterizing anatomical and physiological particularities of children heart
it is necessary
Characterizing anatomical and physiological particularities of children heart
it is necessary
The vessels
conduct and distribute the blood on organ and tissues.
The vessels
conduct and distribute the blood on organ and tissues.
By origin the shock can be
cardiogenic connected with low heart out-put
By origin the shock can be
cardiogenic connected with low heart out-put
The clinical study of
cardiovascular system.
The clinical study of
cardiovascular system.
The cardiovascular dependent complaints
in children are very unspecific. Especially they are
The cardiovascular dependent complaints
in children are very unspecific. Especially they are
The physical load intolerance complaint
In children the big clinical importance
The physical load intolerance complaint
In children the big clinical importance
The heart rate, arterial blood pressure
The clinical characteristics of cardiovascular
The heart rate, arterial blood pressure
The clinical characteristics of cardiovascular
The normal frequency of pulse is changing depending on age:
- in
The normal frequency of pulse is changing depending on age:
- in
Pulse count
An important practical remark consists in necessary to create for
Pulse count
An important practical remark consists in necessary to create for
Pulse count
The pulse rate also depends on the body temperature. In
Pulse count
The pulse rate also depends on the body temperature. In
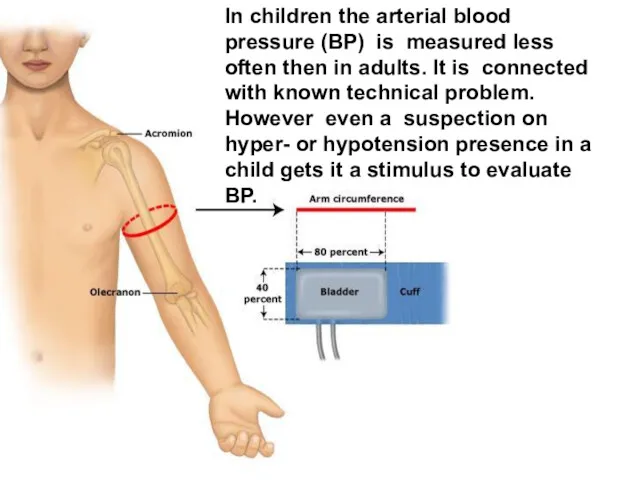
In children the arterial blood pressure (BP) is measured less often
In children the arterial blood pressure (BP) is measured less often
The Normal values of arterial blood pressure
depend on the child age
The Normal values of arterial blood pressure
depend on the child age
Current cardiac examination is made in 4 steps.
Current cardiac examination is made in 4 steps.
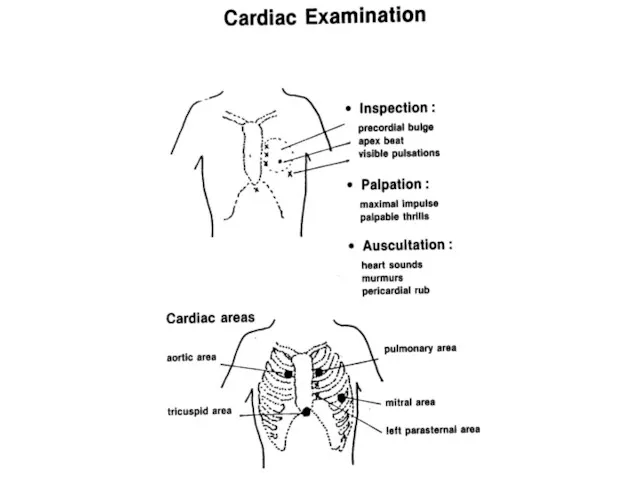
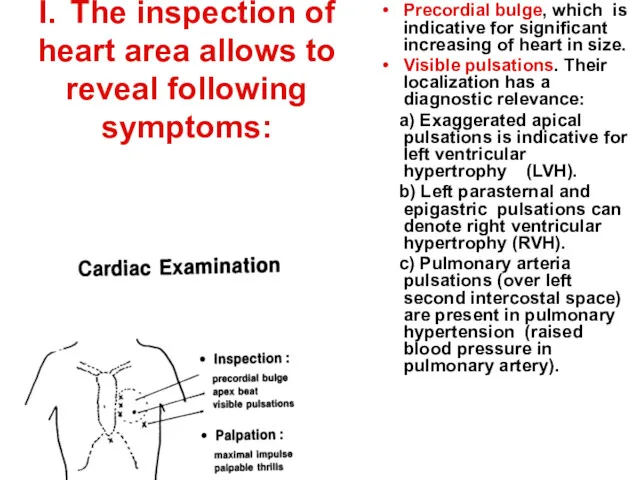
I. The inspection of heart area allows to reveal following symptoms:
Precordial bulge,
I. The inspection of heart area allows to reveal following symptoms:
Precordial bulge,
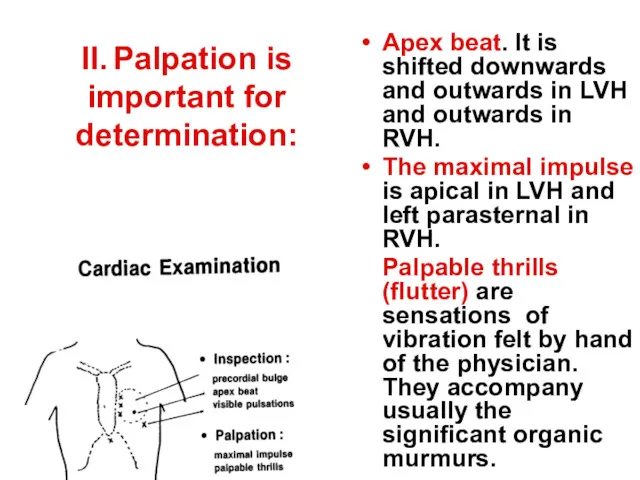
II. Palpation is important for determination:
Apex beat. It is shifted downwards and
II. Palpation is important for determination:
Apex beat. It is shifted downwards and
III. Percussion.
The percussion of cardiac borders is obsolete now in modern
III. Percussion.
The percussion of cardiac borders is obsolete now in modern
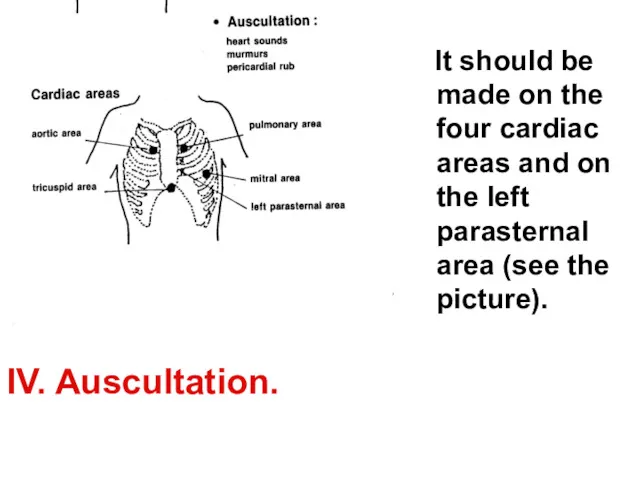
It should be made on the four cardiac areas and on
The clinical comment of auscultation shold include next characteristics:
The heart
The clinical comment of auscultation shold include next characteristics:
The heart
The clinical comment of auscultation shold include next characteristics:
Murmurs. Their comment
The clinical comment of auscultation shold include next characteristics:
Murmurs. Their comment
The clinical comment of auscultation shold include next characteristics:
Pericardial rub. It
The clinical comment of auscultation shold include next characteristics:
Pericardial rub. It
The heart sounds can be visualized in paper or electronic screen
The heart sounds can be visualized in paper or electronic screen
For successful diagnostics of cardiovascular diseases in children it is necessary
For successful diagnostics of cardiovascular diseases in children it is necessary
Cyanosis
is defined as skin or mucosa bluishness.
Acute cyanosis with respiratory
Cyanosis
is defined as skin or mucosa bluishness.
Acute cyanosis with respiratory
A femoral pulsation
or palpation of the pulse on hip artery
A femoral pulsation
or palpation of the pulse on hip artery
The syndrome of congestive heart failure
is formed from specific signs.
The syndrome of congestive heart failure
is formed from specific signs.
In acute failure, the cardinal triad is tachycardia, tachypnea and enlarged
In acute failure, the cardinal triad is tachycardia, tachypnea and enlarged
In chronic failure:
1. Exertional dyspnea is present. The breathlessness appears in
In chronic failure:
1. Exertional dyspnea is present. The breathlessness appears in
The Semiotics of the commonest diseases of cardiovascular system in children.
The Semiotics of the commonest diseases of cardiovascular system in children.
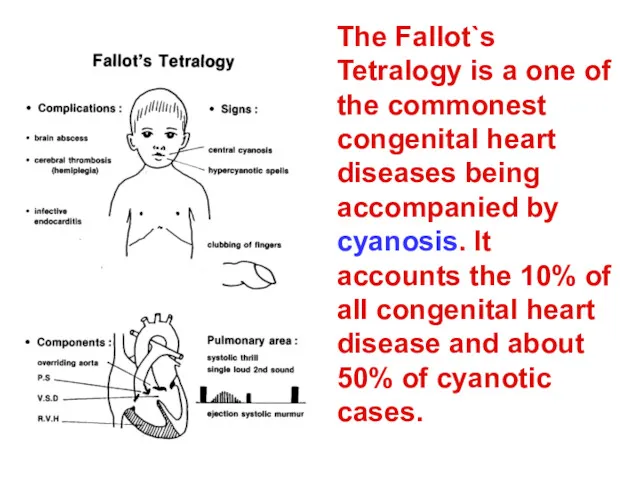
The Fallot`s Tetralogy is a one of the commonest congenital heart
The Fallot`s Tetralogy is a one of the commonest congenital heart
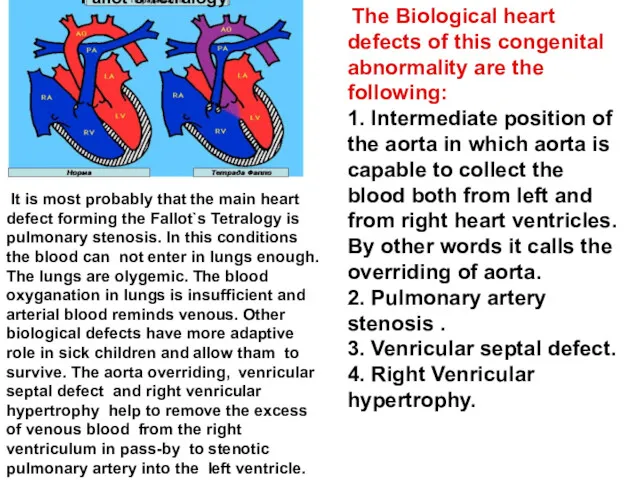
The Biological heart defects of this congenital abnormality are the
The Biological heart defects of this congenital abnormality are the
The semiotics reflect pathophysiological changes occurring in this congenital heart disease.
In
The semiotics reflect pathophysiological changes occurring in this congenital heart disease.
In
High hemoglobin
The compensaroty hemoglobin and erythrocytes elevation reachs the level nearly
High hemoglobin
The compensaroty hemoglobin and erythrocytes elevation reachs the level nearly
Hypercyanotic spells
They are attacks of deep cyanosis and respiratory distress
Hypercyanotic spells
They are attacks of deep cyanosis and respiratory distress
The other suggestive clinical features:
Clubbing of fingers. It is usually
The other suggestive clinical features:
Clubbing of fingers. It is usually
- Left parasternal pulsations denotes right ventricular hypertrophy.
- Systolyc thrill
- Left parasternal pulsations denotes right ventricular hypertrophy.
- Systolyc thrill
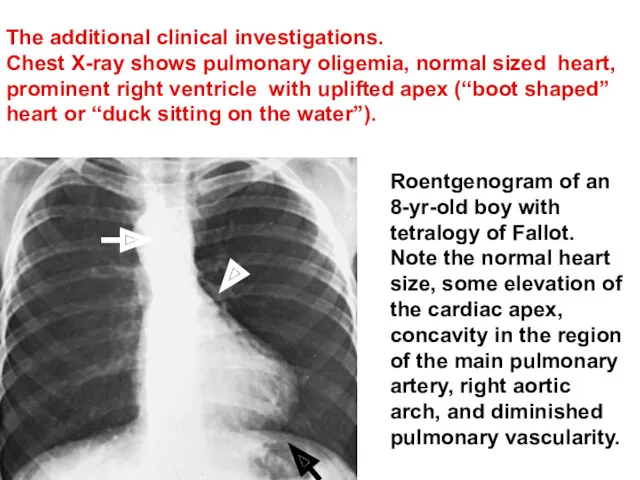
The additional clinical investigations.
Chest X-ray shows pulmonary oligemia, normal sized heart,
The additional clinical investigations. Chest X-ray shows pulmonary oligemia, normal sized heart,
The guidelines of care for the sick children.
When the hypercyanotic
The guidelines of care for the sick children.
When the hypercyanotic
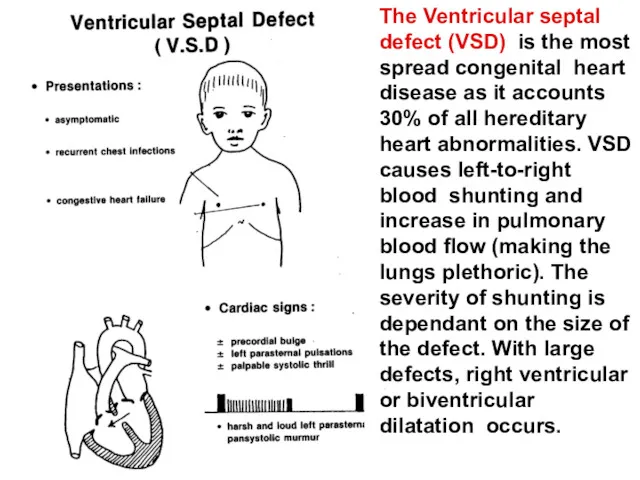
The Ventricular septal defect (VSD) is the most spread congenital heart
The Ventricular septal defect (VSD) is the most spread congenital heart
Patients with VSD are frequently asymptomatic and the condition is accidentally
Patients with VSD are frequently asymptomatic and the condition is accidentally

Murmur, VSD!
Healthy!
Murmur, VSD!
Healthy!
Semiotics of V.S.D.
Characteristic murmur is pansystolic, loud, harsh, and left
Semiotics of V.S.D.
Characteristic murmur is pansystolic, loud, harsh, and left
The manifestations of CHF may by chronic or acute.
Chronic CHF
The manifestations of CHF may by chronic or acute.
Chronic CHF
Other diagnostic approaches
Diagnostic echocardiography demonstrates the septal defect, its size
Other diagnostic approaches
Diagnostic echocardiography demonstrates the septal defect, its size
Presence of cardiomegaly or congestive heart failure in infancy is an
Presence of cardiomegaly or congestive heart failure in infancy is an
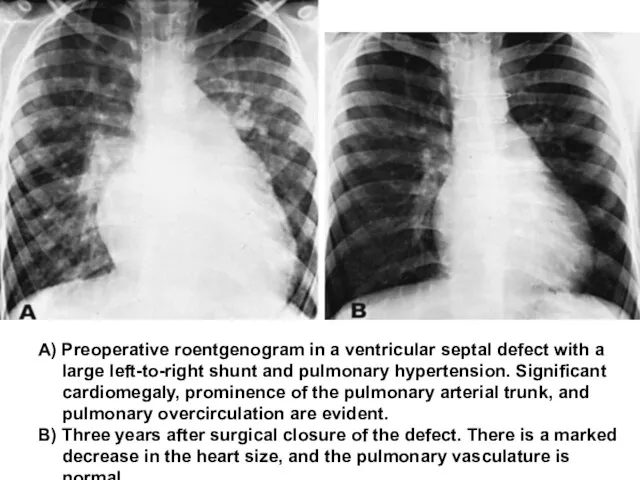
A) Preoperative roentgenogram in a ventricular septal defect with a large
A) Preoperative roentgenogram in a ventricular septal defect with a large
The guidelines of care for sick children.
The children sufferring from
The guidelines of care for sick children.
The children sufferring from
The atrial septal defect (ASD)
The atrial septal defect (ASD) is other
The atrial septal defect (ASD)
The atrial septal defect (ASD) is other
Symptoms of ASD
1. The systolic murmur over the pulmonary area is usually
Symptoms of ASD
1. The systolic murmur over the pulmonary area is usually
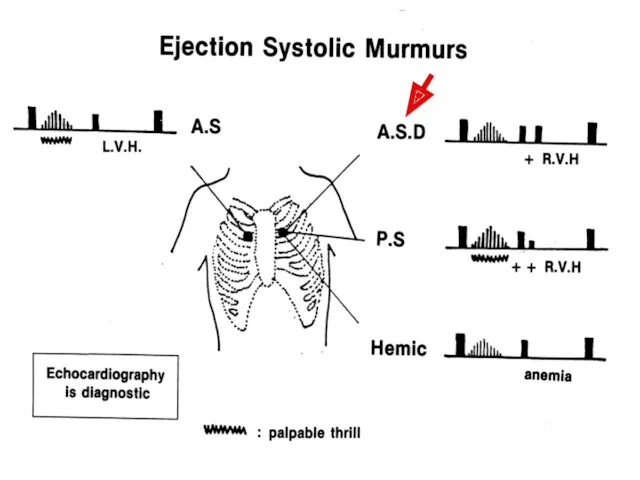
The other causes of ejection systolic murmur
1. Innocent (functional, non-malignant) systolic murmur
The other causes of ejection systolic murmur
1. Innocent (functional, non-malignant) systolic murmur
The guidelines of care for sick children with ASD.
They
The guidelines of care for sick children with ASD.
They
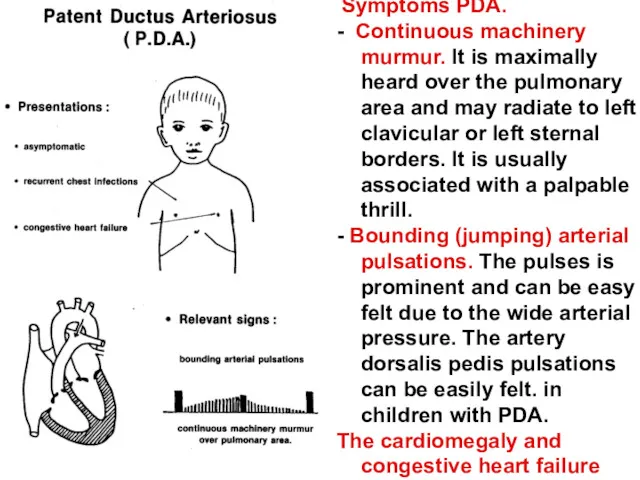
Symptoms PDA.
- Continuous machinery murmur. It is maximally heard
Symptoms PDA.
- Continuous machinery murmur. It is maximally heard
Other diagnostic approaches
Echcardiography reveals increased left atrial and left ventricular sizes.
Other diagnostic approaches
Echcardiography reveals increased left atrial and left ventricular sizes.
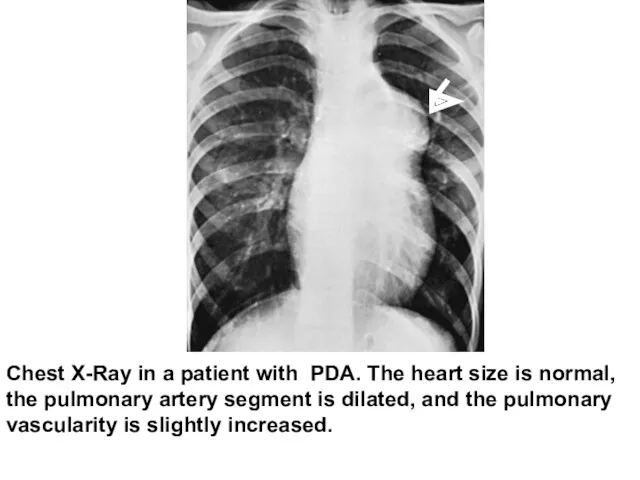
Chest X-Ray in a patient with PDA. The heart size is
Chest X-Ray in a patient with PDA. The heart size is
The Rheumatism (rheumatic fever) is an autoimmune disease, which develops as
The Rheumatism (rheumatic fever) is an autoimmune disease, which develops as
Jones`s criteria
5 Jones`s criterias (or clinical manifestations) are generally used for
Jones`s criteria
5 Jones`s criterias (or clinical manifestations) are generally used for
Major criteria (Jones`s criteria or manifestations) of rheumatic fever.
1/ Polyarthritis occurs
Major criteria (Jones`s criteria or manifestations) of rheumatic fever.
1/ Polyarthritis occurs
Major criteria (Jones`s criteria or manifestations) of rheumatic fever.
2/ Carditis occurs
Major criteria (Jones`s criteria or manifestations) of rheumatic fever.
2/ Carditis occurs
Major criteria (Jones`s criteria or manifestations) of rheumatic fever.
3/ Reumatic chorea.
Major criteria (Jones`s criteria or manifestations) of rheumatic fever.
3/ Reumatic chorea.
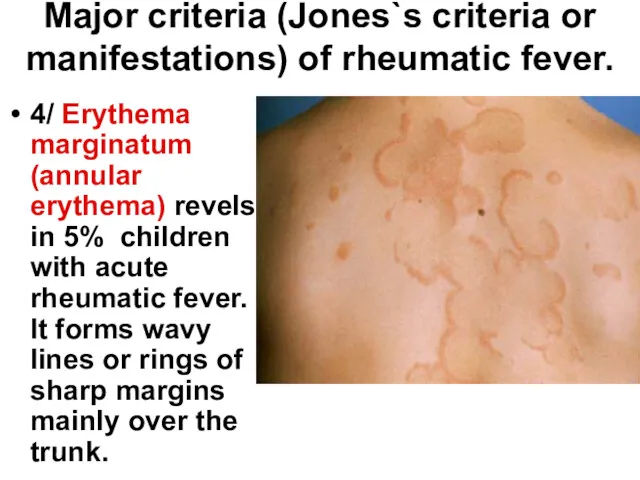
Major criteria (Jones`s criteria or manifestations) of rheumatic fever.
4/ Erythema marginatum
Major criteria (Jones`s criteria or manifestations) of rheumatic fever.
4/ Erythema marginatum
Major criteria (Jones`s criteria or manifestations) of rheumatic fever.
5/ Subcutaneous nodules.
Major criteria (Jones`s criteria or manifestations) of rheumatic fever.
5/ Subcutaneous nodules.
The Chronic rheumatic heart disease is a continuation of the acute
The Chronic rheumatic heart disease is a continuation of the acute
Recognition of the valvular lesions depends on auscultation of the characteristic
Recognition of the valvular lesions depends on auscultation of the characteristic
Mitral stenosis (M.S.).
An apical mid-diastolic rumbling murmur is present.
Mitral stenosis (M.S.).
An apical mid-diastolic rumbling murmur is present.
Aortic incompetence.
A soft and bloving diastolic murmur is heard
Aortic incompetence.
A soft and bloving diastolic murmur is heard
Aortic stenosis.
A harsh and loud ejection systolic murmur is
Aortic stenosis.
A harsh and loud ejection systolic murmur is
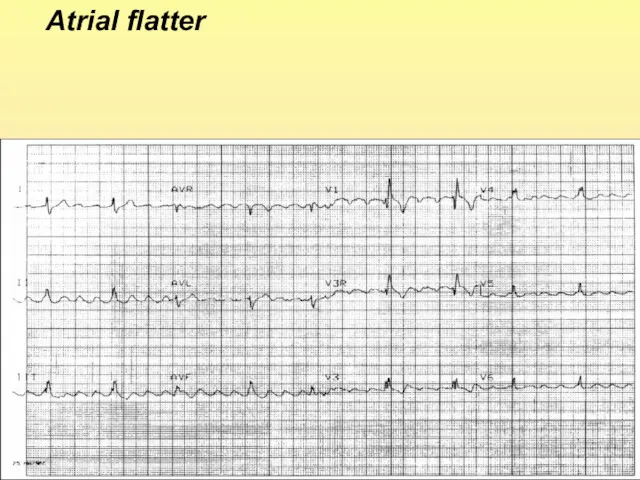
Atrial flatter
Atrial flatter
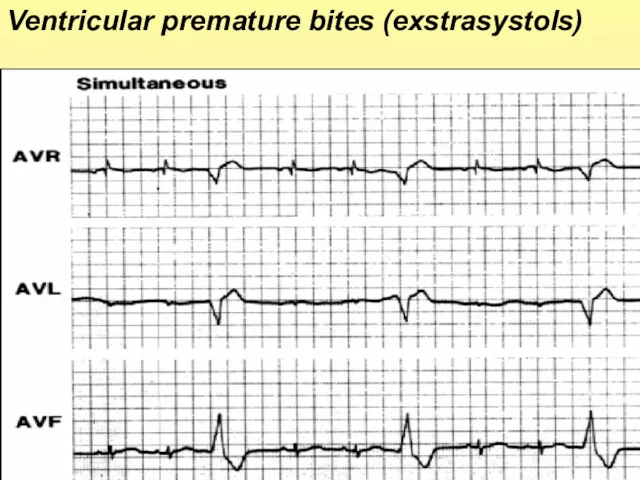
Ventricular premature bites (exstrasystols)
Ventricular premature bites (exstrasystols)
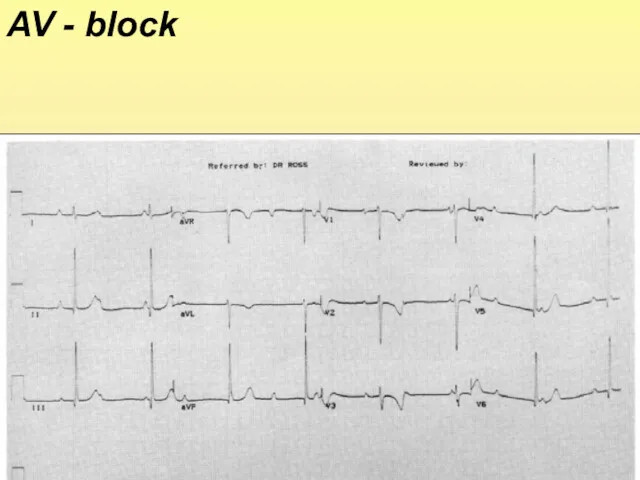
AV - block
AV - block
ABC program of cardio-pulmonary and cerebral resuscitation
The sudden cardial arrest
ABC program of cardio-pulmonary and cerebral resuscitation
The sudden cardial arrest
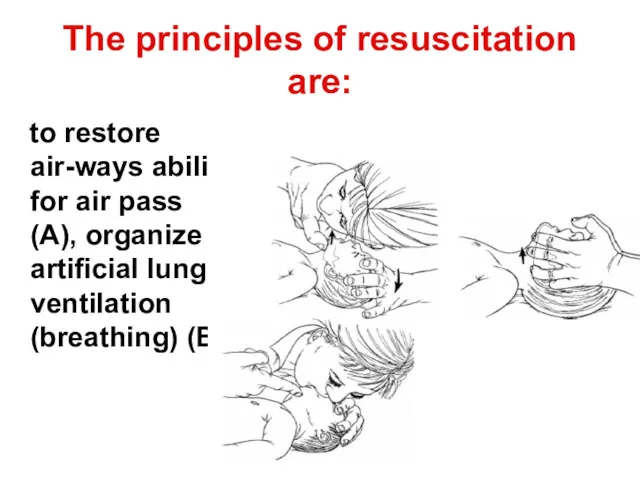
The principles of resuscitation are:
to restore air-ways ability for air
The principles of resuscitation are:
to restore air-ways ability for air
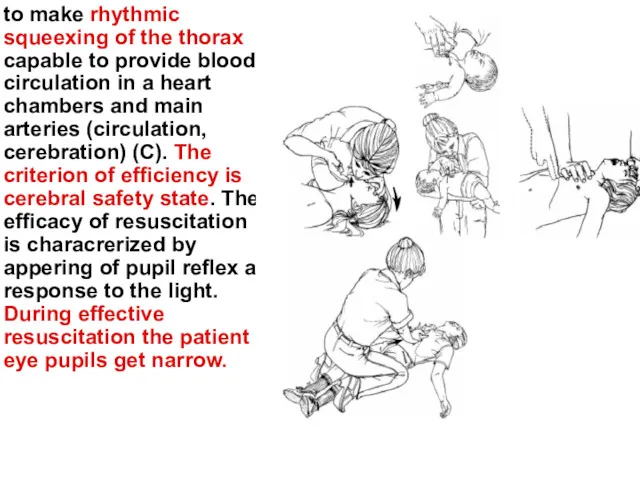
to make rhythmic squeexing of the thorax capable to provide blood
to make rhythmic squeexing of the thorax capable to provide blood
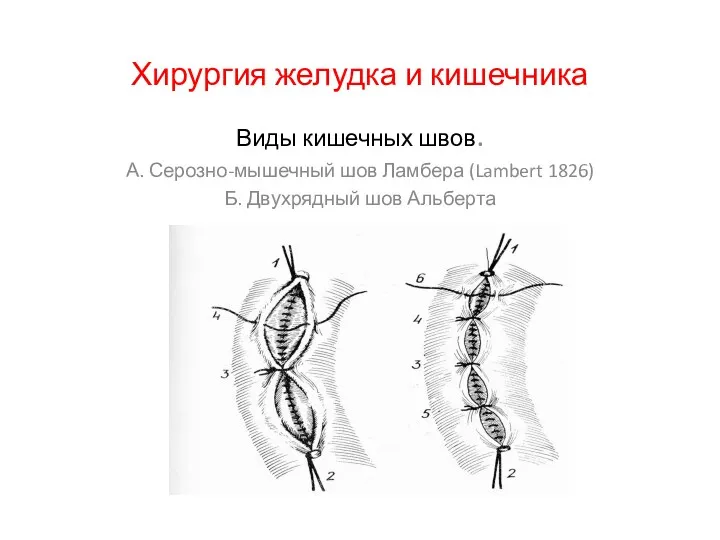 Хирургия желудка и кишечника
Хирургия желудка и кишечника Рациональное питание
Рациональное питание Общая синдесмология
Общая синдесмология Mondino de Luzzi
Mondino de Luzzi Интоксикация промышленными ядами. Формы свинцовой интоксикации
Интоксикация промышленными ядами. Формы свинцовой интоксикации Дезинфицирующие средства компании ООО “Дезнэт”
Дезинфицирующие средства компании ООО “Дезнэт” Инфекционные заболевания
Инфекционные заболевания Смерть и умирание. Правовые и морально-этические аспекты эвтаназии
Смерть и умирание. Правовые и морально-этические аспекты эвтаназии Медицина и этика. Биоэтика. Профессиональная этика
Медицина и этика. Биоэтика. Профессиональная этика Анафилактический шок. Этиология. Патогенез. Лечение
Анафилактический шок. Этиология. Патогенез. Лечение Переливание крови
Переливание крови Подагра – болезнь 21 века?
Подагра – болезнь 21 века? Қабыну. Ауыру. Оның құрылымы, механизмі, өткізу жолдары, ағзаның ауыру сезіміне реакциясы
Қабыну. Ауыру. Оның құрылымы, механизмі, өткізу жолдары, ағзаның ауыру сезіміне реакциясы Тағамдық токсикоинфекция
Тағамдық токсикоинфекция Аутоимунный гепатит
Аутоимунный гепатит Ауыз қуысының жеке басының тазалығы. Ауыз қуысының кәсіби тазалығы
Ауыз қуысының жеке басының тазалығы. Ауыз қуысының кәсіби тазалығы Основы хирургии пороков развития
Основы хирургии пороков развития Асқазанның зертханалық және аспаптық зерттеу әдістері
Асқазанның зертханалық және аспаптық зерттеу әдістері Отек легких
Отек легких Распорядок дня
Распорядок дня Бесплодный брак
Бесплодный брак Нейроиммунология. Стресс. История проблемы
Нейроиммунология. Стресс. История проблемы Острые отравления этанолом
Острые отравления этанолом Абдоминальная хирургия. Кишечный шов
Абдоминальная хирургия. Кишечный шов Клиническая психология. Формирование базовых знаний по теории, методологии и практике клинической психологии,
Клиническая психология. Формирование базовых знаний по теории, методологии и практике клинической психологии, Нарушения памяти при локальных поражениях мозга
Нарушения памяти при локальных поражениях мозга Особености травматологии детского возраста
Особености травматологии детского возраста Алгоритм диагностики суставного синдрома. Основные заболевания
Алгоритм диагностики суставного синдрома. Основные заболевания