- Tuberculosis. Mycobacterium tuberculosis

Содержание
- 2. Tuberculosis (TB), which is caused by bacteria of the Mycobacterium tuberculosis complex, is one of the
- 3. If properly treated, TB caused by drug-susceptible strains is curable in the vast majority of cases.
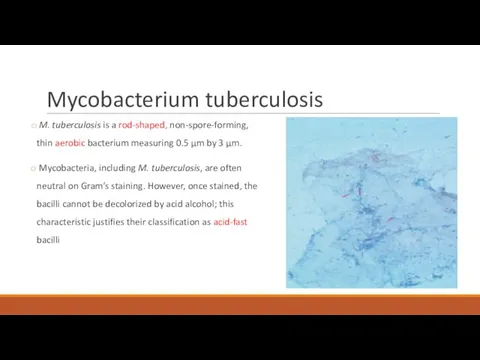
- 4. Mycobacterium tuberculosis M. tuberculosis is a rod-shaped, non-spore-forming, thin aerobic bacterium measuring 0.5 μm by 3
- 5. Transmission and infection Transmission usually takes place through the airborne spread of droplet nuclei produced by
- 6. Most infectious patients: Cavitary pulmonary disease or, much less common, laryngeal TB Patients with positive sputum
- 7. Natural history of the disease 10% of infected persons will eventually develop active TB in their
- 8. TB is classified as pulmonary, extrapulmonary, or both. Depending on several factors linked to different populations
- 9. Pulmonary TB
- 10. Primary Pulmonary TB Clinical illness directly following infection. Is common among children and immunocompromised persons. May
- 11. Symptoms May be asymptomatic or may present with fever and occasionally pleuritic chest pain. Most commonly
- 12. In young children and in persons with impaired immunity (e.g. malnutrition or HIV), primary pulmonary TB
- 13. Bronchiectasis may develop in any segment/lobe damaged by progressive caseating pneumonia. Occult hematogenous dissemination commonly follows
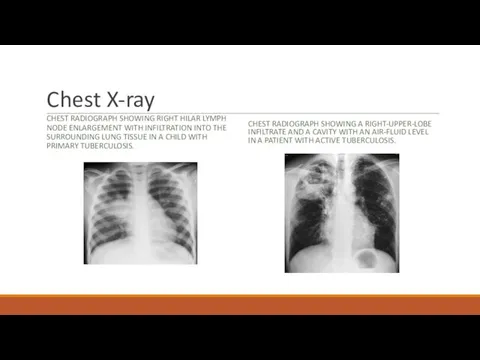
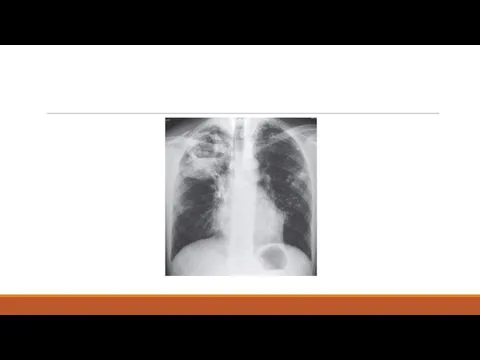
- 14. Chest X-ray CHEST RADIOGRAPH SHOWING RIGHT HILAR LYMPH NODE ENLARGEMENT WITH INFILTRATION INTO THE SURROUNDING LUNG
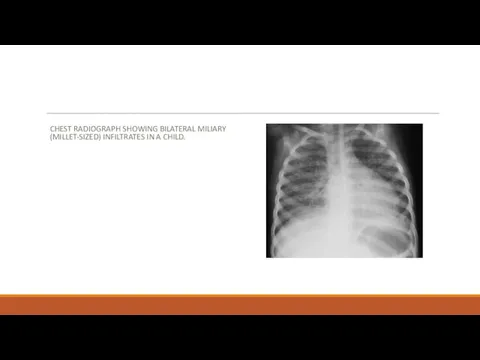
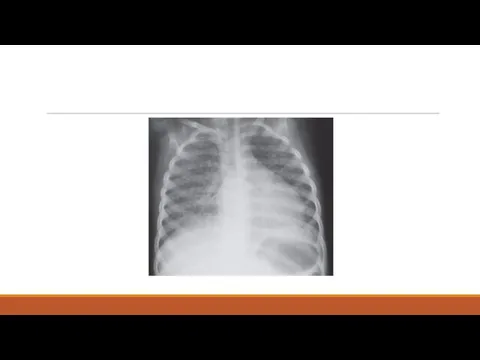
- 15. CHEST RADIOGRAPH SHOWING BILATERAL MILIARY (MILLET-SIZED) INFILTRATES IN A CHILD.
- 16. Secondary Pulmonary TB Bacilli may reactivate after many years because of frequent cavitation, is more often
- 17. Symptoms Early in the course of disease symptoms and signs are often nonspecific: fever, chills, night
- 19. Hemoptysis develops in 20-30% of cases, and massive hemoptysis may ensue as a consequence of the
- 20. Diagnosis Physical findings are of limited use in pulmonary TB. The most common hematologic findings are
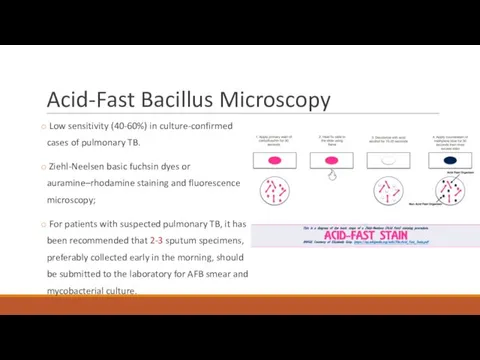
- 21. Acid-Fast Bacillus Microscopy Low sensitivity (40-60%) in culture-confirmed cases of pulmonary TB. Ziehl-Neelsen basic fuchsin dyes
- 22. Gene Xpert Fully automated amplification of mycobacterial nucleic acid (DNA PCR) Most useful for the rapid
- 23. Mycobacteria culture A low-cost Definitive diagnosis MGIT cultures usually become positive after a period ranging from
- 24. Drug Susceptibility testing Any initial isolate of M. tuberculosis should be tested for susceptibility to isoniazid
- 25. HIV-ASSOCIATED TB Likely main cause of infectious-related death in this population If CD4 is low (less
- 26. Treatment The two main aims of TB treatment: to prevent morbidity and death by curing TB
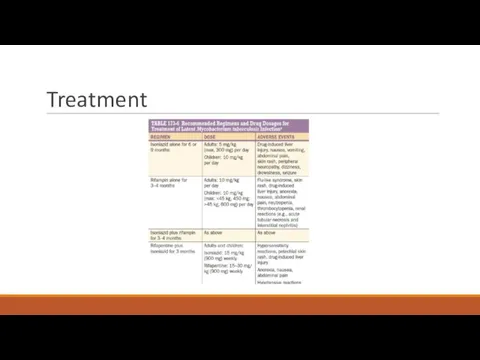
- 27. Isoniazid (H) – s/e liver toxicity, peripheral neuropathy (should be administered with pyridoxine) Rifampin (R) –
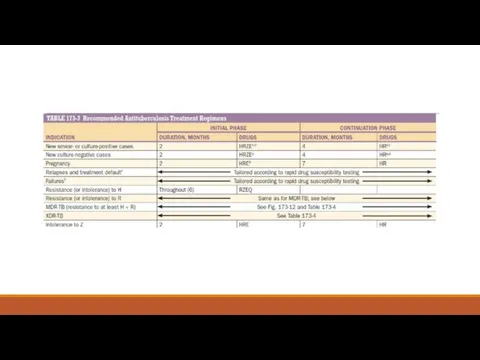
- 28. Treatment regimen Divided into 2 phases: An initial, or bactericidal phase - the majority of the
- 30. Patients with pulmonary disease should have their sputum examined monthly until cultures become negative to allow
- 31. Treatment failure and relapse Current isolate must be urgently tested for susceptibility to first- and second-line
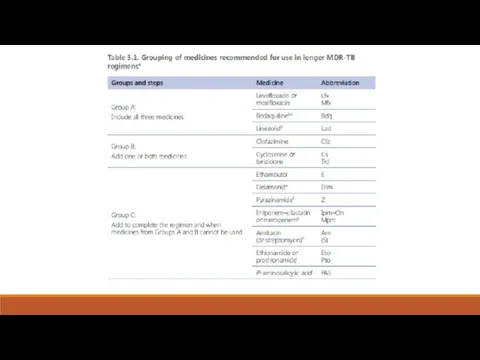
- 32. MDR-TB treatment For the treatment of patients with isoniazid-resistant disease, it is recommended to use a
- 33. In 2013 and 2014, respectively, bedaquiline and delamanid—the first two drugs specifically developed for TB during
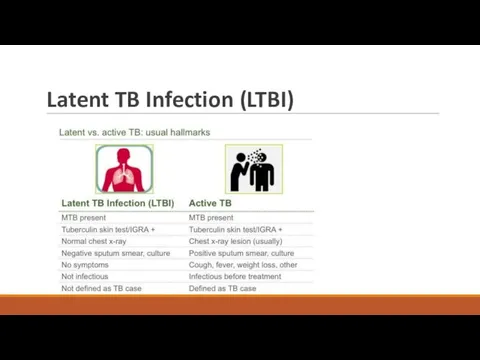
- 35. Latent TB Infection (LTBI)
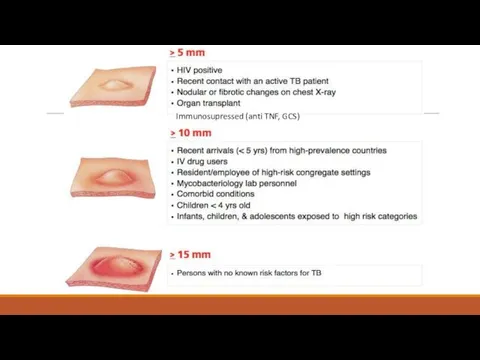
- 36. Tuberculin Skin Testing (Tuberculin purifed protein derivative (PPD) Measures the response to antigenic stimulation by T
- 38. Immunosupressed (anti TNF, GCS)
- 39. IFN- γ Release Assays (IGRA) Have usually replaced the TST for LTBI diagnosis in low-incidence, high-income
- 40. Treatment
- 41. PREVENTION The best way to prevent TB is to diagnose and isolate infectious cases rapidly and
- 42. Extrapulmonary TB
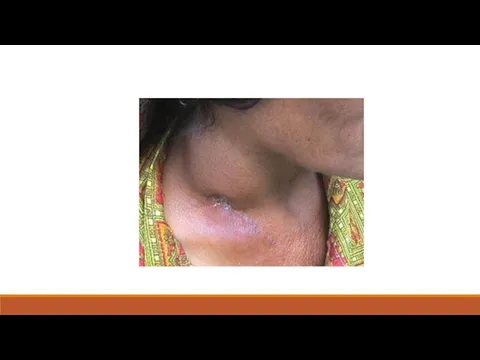
- 43. Tuberculous Lymphadenitis Most commo form of extrapulmonary TB (35-40%) Cervical adenopathy Peak age of onset of
- 45. Pleural Tuberculosis Cough, pleuritic chest pain, fever, or dyspnea. Small to moderate, unilateral pleural effusion About
- 46. TB of the Upper Airways Nearly always a complication of advanced cavitary pulmonary TB May involve
- 47. Genitourinary TB ~10–15% of all extrapulmonary cases Urinary frequency, dysuria, nocturia, hematuria, and flank or abdominal
- 48. Skeletal Tuberculosis ~10% of extrapulmonary cases. Most often involves the spine, arthritis in weight-bearing joints and
- 49. Surgery may be necessary to drain abscesses, debride infected tissue, or stabilize the spine and relieve
- 50. Meningitis ~5% of extrapulmonary cases Acute or subacute Headache and slight mental changes after a pro-drome
- 51. MILIARY TUBERCULOSIS Any progressive, disseminated form of tuberculosis; the disease can occur during primary dissemination or
- 54. THANK YOU!
- 55. QUESTIONS
- 56. Перед вами представлены факторы повышающие вероятность передачи активного туберкулеза, все ответы верны КРОМЕ: Продолжительность контакта с
- 57. 42-летний мужчина из Нигерии приезжает в отделение реанимации из-за высокой температуры, усталости, потери веса и кашля
- 59. Перевести пациента на воздушнокапельный карантин, пока три анализа мокроты не придут с признаками присутсвия кислотоустойчивых бацилл.
- 60. 18-летний молодой человек из Южной Африки пришел в клинику с жалобами из 2 недельного прогрессирующего недомогания
- 62. Диссеминированный Экстрапульмонарный Лимфаденит Плевральный Вторичный кавитарный
- 63. 50-летний человек госпитализирован в связи с активным легочным туберкулезом с положительным мазком мокроты на кислотоустойчивые бациллы.
- 64. Все следующие люди, получающие реакции PPD туберкулина кожи, должны лечиться с связи подозрением на скрытый туберкулез
- 66. Скачать презентацию
Tuberculosis (TB), which is caused by bacteria of the Mycobacterium tuberculosis
Tuberculosis (TB), which is caused by bacteria of the Mycobacterium tuberculosis
If properly treated, TB caused by drug-susceptible strains is curable
If properly treated, TB caused by drug-susceptible strains is curable
Mycobacterium tuberculosis
M. tuberculosis is a rod-shaped, non-spore-forming, thin aerobic bacterium
Mycobacterium tuberculosis
M. tuberculosis is a rod-shaped, non-spore-forming, thin aerobic bacterium
Transmission and infection
Transmission usually takes place through the airborne spread of
Transmission and infection
Transmission usually takes place through the airborne spread of
Most infectious patients:
Cavitary pulmonary disease or, much less common, laryngeal TB
Most infectious patients:
Cavitary pulmonary disease or, much less common, laryngeal TB
Natural history of the disease
10% of infected persons will eventually
Natural history of the disease
10% of infected persons will eventually
TB is classified as pulmonary, extrapulmonary, or both. Depending on
TB is classified as pulmonary, extrapulmonary, or both. Depending on
Pulmonary TB
Pulmonary TB
Primary Pulmonary TB
Clinical illness directly following infection.
Is common
Primary Pulmonary TB
Clinical illness directly following infection.
Is common
Symptoms
May be asymptomatic or may present with fever and occasionally
Symptoms
May be asymptomatic or may present with fever and occasionally

In young children and in persons with impaired immunity (e.g.
In young children and in persons with impaired immunity (e.g.

Bronchiectasis may develop in any segment/lobe damaged by progressive caseating
Bronchiectasis may develop in any segment/lobe damaged by progressive caseating
Chest X-ray
CHEST RADIOGRAPH SHOWING RIGHT HILAR LYMPH NODE ENLARGEMENT WITH INFILTRATION
Chest X-ray
CHEST RADIOGRAPH SHOWING RIGHT HILAR LYMPH NODE ENLARGEMENT WITH INFILTRATION
CHEST RADIOGRAPH SHOWING BILATERAL MILIARY (MILLET-SIZED) INFILTRATES IN A CHILD.
CHEST RADIOGRAPH SHOWING BILATERAL MILIARY (MILLET-SIZED) INFILTRATES IN A CHILD.
Secondary Pulmonary TB
Bacilli may reactivate after many years because of
Secondary Pulmonary TB
Bacilli may reactivate after many years because of
Symptoms
Early in the course of disease symptoms and signs are often
Symptoms
Early in the course of disease symptoms and signs are often

Hemoptysis develops in 20-30% of cases, and massive hemoptysis may
Hemoptysis develops in 20-30% of cases, and massive hemoptysis may
Diagnosis
Physical findings are of limited use in pulmonary TB.
The
Diagnosis
Physical findings are of limited use in pulmonary TB.
The
Acid-Fast Bacillus Microscopy
Low sensitivity (40-60%) in culture-confirmed cases of pulmonary
Acid-Fast Bacillus Microscopy
Low sensitivity (40-60%) in culture-confirmed cases of pulmonary
Gene Xpert
Fully automated amplification of mycobacterial nucleic acid (DNA PCR)
Gene Xpert
Fully automated amplification of mycobacterial nucleic acid (DNA PCR)
Mycobacteria culture
A low-cost
Definitive diagnosis
MGIT cultures usually become positive
Mycobacteria culture
A low-cost
Definitive diagnosis
MGIT cultures usually become positive
Drug Susceptibility testing
Any initial isolate of M. tuberculosis should be
Drug Susceptibility testing
Any initial isolate of M. tuberculosis should be
HIV-ASSOCIATED TB
Likely main cause of infectious-related death in this population
HIV-ASSOCIATED TB
Likely main cause of infectious-related death in this population
Treatment
The two main aims of TB treatment:
to prevent morbidity
Treatment
The two main aims of TB treatment:
to prevent morbidity
Isoniazid (H) – s/e liver toxicity, peripheral neuropathy (should be
Isoniazid (H) – s/e liver toxicity, peripheral neuropathy (should be
Treatment regimen
Divided into 2 phases:
An initial, or bactericidal phase
Treatment regimen
Divided into 2 phases:
An initial, or bactericidal phase
Patients with pulmonary disease should have their sputum examined monthly
Patients with pulmonary disease should have their sputum examined monthly
Treatment failure and relapse
Current isolate must be urgently tested for
Treatment failure and relapse
Current isolate must be urgently tested for
MDR-TB treatment
For the treatment of patients with isoniazid-resistant disease, it is
MDR-TB treatment
For the treatment of patients with isoniazid-resistant disease, it is

In 2013 and 2014, respectively, bedaquiline and delamanid—the first two drugs
In 2013 and 2014, respectively, bedaquiline and delamanid—the first two drugs
Latent TB Infection (LTBI)
Latent TB Infection (LTBI)
Tuberculin Skin Testing (Tuberculin purifed protein derivative (PPD)
Measures the response
Tuberculin Skin Testing (Tuberculin purifed protein derivative (PPD)
Measures the response
Immunosupressed (anti TNF, GCS)
Immunosupressed (anti TNF, GCS)
IFN- γ Release Assays (IGRA)
Have usually replaced the TST for
IFN- γ Release Assays (IGRA)
Have usually replaced the TST for
Treatment
Treatment
PREVENTION
The best way to prevent TB is to diagnose and
PREVENTION
The best way to prevent TB is to diagnose and
Extrapulmonary TB
Extrapulmonary TB
Tuberculous Lymphadenitis
Most commo form of extrapulmonary TB (35-40%)
Cervical adenopathy
Tuberculous Lymphadenitis
Most commo form of extrapulmonary TB (35-40%)
Cervical adenopathy
Pleural Tuberculosis
Cough, pleuritic chest pain, fever, or dyspnea.
Small to
Pleural Tuberculosis
Cough, pleuritic chest pain, fever, or dyspnea.
Small to
TB of the Upper Airways
Nearly always a complication of
TB of the Upper Airways
Nearly always a complication of
Genitourinary TB
~10–15% of all extrapulmonary cases
Urinary frequency,
Genitourinary TB
~10–15% of all extrapulmonary cases
Urinary frequency,
Skeletal Tuberculosis
~10% of extrapulmonary cases.
Most often involves the
Skeletal Tuberculosis
~10% of extrapulmonary cases.
Most often involves the
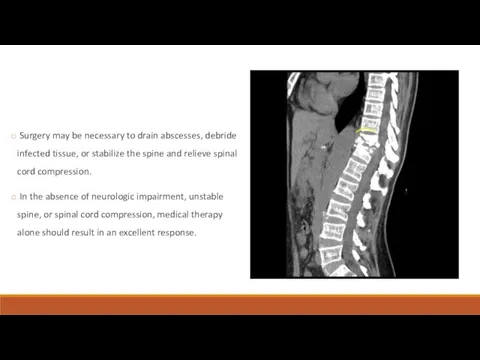
Surgery may be necessary to drain abscesses, debride infected tissue,
Surgery may be necessary to drain abscesses, debride infected tissue,
Meningitis
~5% of extrapulmonary cases
Acute or subacute
Headache and slight
Meningitis
~5% of extrapulmonary cases
Acute or subacute
Headache and slight
MILIARY TUBERCULOSIS
Any progressive, disseminated form of tuberculosis; the disease can
MILIARY TUBERCULOSIS
Any progressive, disseminated form of tuberculosis; the disease can

THANK YOU!
THANK YOU!

QUESTIONS
QUESTIONS
Перед вами представлены факторы повышающие вероятность передачи активного туберкулеза, все ответы
Перед вами представлены факторы повышающие вероятность передачи активного туберкулеза, все ответы

42-летний мужчина из Нигерии приезжает в отделение реанимации из-за высокой температуры,
42-летний мужчина из Нигерии приезжает в отделение реанимации из-за высокой температуры,
Перевести пациента на воздушнокапельный карантин, пока три анализа мокроты не придут
Перевести пациента на воздушнокапельный карантин, пока три анализа мокроты не придут

18-летний молодой человек из Южной Африки пришел в клинику с жалобами
18-летний молодой человек из Южной Африки пришел в клинику с жалобами

Диссеминированный
Экстрапульмонарный
Лимфаденит
Плевральный
Вторичный кавитарный
Диссеминированный
Экстрапульмонарный
Лимфаденит
Плевральный
Вторичный кавитарный
50-летний человек госпитализирован в связи с активным легочным туберкулезом с положительным
50-летний человек госпитализирован в связи с активным легочным туберкулезом с положительным

Все следующие люди, получающие реакции PPD туберкулина кожи, должны лечиться с
Все следующие люди, получающие реакции PPD туберкулина кожи, должны лечиться с
 Улучшение качества материнской и неонатальной помощи. (Модуль 15)
Улучшение качества материнской и неонатальной помощи. (Модуль 15) Синдром легочной диссеминации. Диссеминированный туберкулез легких
Синдром легочной диссеминации. Диссеминированный туберкулез легких Нейроофтальмологические нарушения при нейромышечных заболеваниях
Нейроофтальмологические нарушения при нейромышечных заболеваниях Острые пневмонии у детей
Острые пневмонии у детей Приклади хвороби органів ШКТ
Приклади хвороби органів ШКТ Введение в фитотерапию
Введение в фитотерапию Ранняя диагностика острого лейкоза у детей
Ранняя диагностика острого лейкоза у детей Синдром диабетической стопы
Синдром диабетической стопы О вреде абортов
О вреде абортов Рак слизистой оболочки полости рта. Клиника, диагностика, лечение
Рак слизистой оболочки полости рта. Клиника, диагностика, лечение Семиотика заболеваний мочевой системы у детей
Семиотика заболеваний мочевой системы у детей Автоматические поточные линии
Автоматические поточные линии ЭКГ
ЭКГ Педиатрия как наука о здоровом и больном ребёнке.Место педиатрии в системе общей медицины. Возрастная периодизация в педиатрии
Педиатрия как наука о здоровом и больном ребёнке.Место педиатрии в системе общей медицины. Возрастная периодизация в педиатрии Острая кишечная непроходимость у детей
Острая кишечная непроходимость у детей Гестационная трофобластическая болезнь
Гестационная трофобластическая болезнь Медицина в Средневековье
Медицина в Средневековье Кровообращение и гомеостаз
Кровообращение и гомеостаз Эпидемиология РМЖ
Эпидемиология РМЖ Метаболический синдром и НАЖБП в современных условиях. Актуальность коморбидности
Метаболический синдром и НАЖБП в современных условиях. Актуальность коморбидности Гигиена аптечных заведений
Гигиена аптечных заведений Клубные наркотики
Клубные наркотики Логопедия. Дизартрия
Логопедия. Дизартрия Координаторная сфера. Мозжечок. Синдромы поражения
Координаторная сфера. Мозжечок. Синдромы поражения Орально-мануальные техники
Орально-мануальные техники Анатомо-физиологические особенности лёгких. (Лекция 11)
Анатомо-физиологические особенности лёгких. (Лекция 11) Общественное здоровье-высшая ценность человечества
Общественное здоровье-высшая ценность человечества Ерте жастағы балалардағы сөйлеу тілінің тежелуінің алдын алудың ерекшеліктері
Ерте жастағы балалардағы сөйлеу тілінің тежелуінің алдын алудың ерекшеліктері