- Valvular Heart Diseases

Содержание
- 3. Stages of Progression of Valvular Heart Disease
- 4. Innocent Murmurs Common in asymptomatic adults Characterized by Grade I – II @ LSB Systolic ejection
- 5. Common Murmurs and Timing Systolic Murmurs Aortic stenosis Mitral insufficiency Mitral valve prolapse Tricuspid insufficiency Diastolic
- 6. Mitral Valve Stenosis
- 7. Mitral Stenosis Etiology Rheumatic Heart Disease -99.8% of cases Normal Valve area: >4 cm2 Critical MS:
- 9. Pathophysiology
- 10. Pathophysiology Left atrial dilatation Allows larger volume at low pressure Prone to A. Fib Thrombi may
- 11. Symptoms Left sided failure Hemoptysis, URI Systemic embolism Palpitations Fatigue Right sided failure Hoarseness
- 12. Signs Loud S1 Opening snap following S2 Narrow pulse pressure Diastolic murmur Atrial Fibrillation Pulmonary congestion;
- 13. Recognizing Mitral Stenosis Palpation: Small volume pulse Tapping apex-palpable S1 +/- palpable opening snap (OS) RV
- 14. Mitral stenosis murmur First heart sound (S1) is accentuated and snapping Opening snap (OS) after aortic
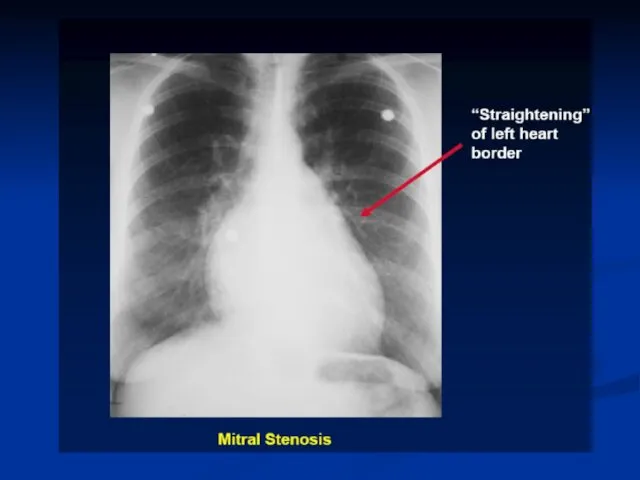
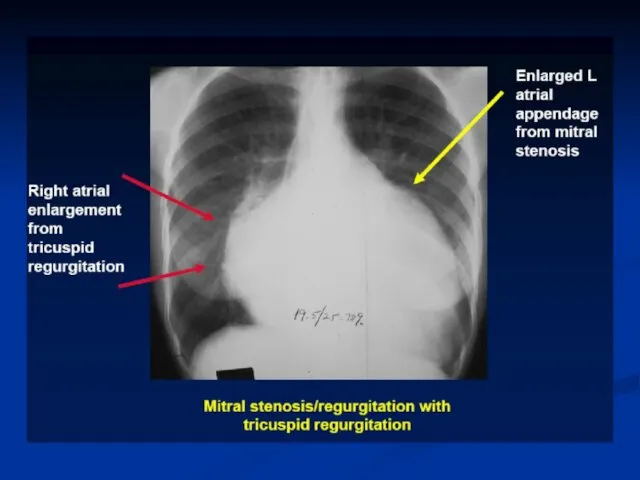
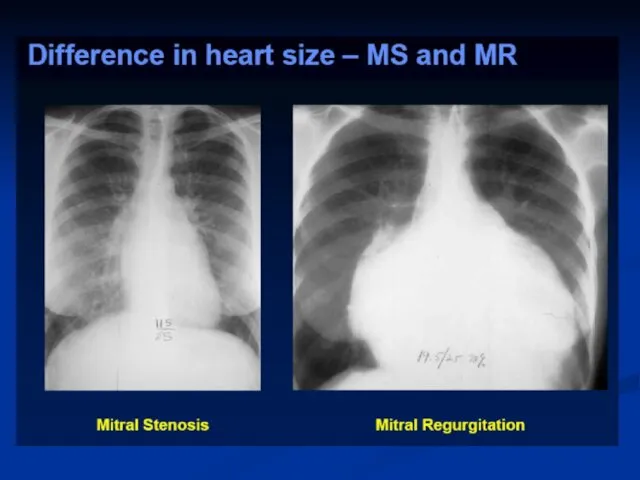
- 15. Lab Diagnosis EKG: A Fib, LAE, RVH CXR: Large LA, Pulm venous congestion, RV dilatation, interstitial/alveolar
- 18. Echo - TTE
- 19. LAE LV AO Echo - TEE
- 20. Therapy Medical Diuretics: For pulmonary congestion, dyspnea and orthopnea Rate control in A Fib: Beta blockers,
- 21. Mitral Valvuloplasty Percutaneous mitral balloon commissurotomy (PMBC) is recommended for symptomatic patients with severe MS (mitral
- 25. Therapy Surgical Mitral commissurotomy: Effective long term improvement Mitral Valve Replacement Mechanical Bioprosthetic
- 26. MV Surgery Mitral valve surgery (repair, commissurotomy, or valve replacement) is indicated in severely symptomatic patients
- 28. When to Perform Cardiac Catheterization in Valvular Patient? No “routine” cardiac catheterization Cardiac catheterization for hemodynamic
- 29. Frequency of Echo Exam
- 30. Secondary Prevention of Rheumatic Fever Secondary prevention of rheumatic fever is indicated in patients with rheumatic
- 31. Mitral Regurgitation
- 32. Etiology Valvular Myxomatous CT Disease Rheumatic Endocarditis Chordae Annulus Calcification Papillary Muscles CAD (Ischemia, Infarction) Infiltrative
- 33. Pathophysiology
- 34. Symptoms Similar to MS Dyspnea, Orthopnea, PND Fatigue Pulmonary HTN, Right sided failure Systemic embolization in
- 35. Signs Chronic MR Hyperdynamic, Displaced apex beat Apical holosystolic murmur Pounding pulse Variable Pulm. HTN Acute
- 36. Diagnosis EKG: LVH, LAE CXR: Cardiac enlargement Echo: Abnormal anatomy, chamber size, EF, Qualitative assessment of
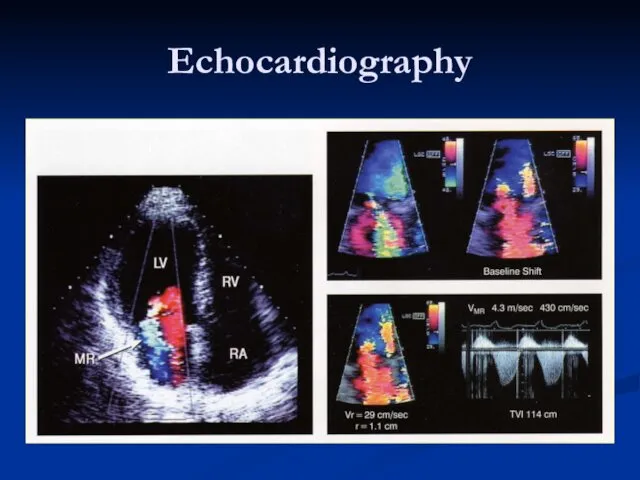
- 39. Echocardiography
- 40. Echo assessment of severity Color Doppler – may be misleading Calculations Effective regurgitant orifice Regurgitant Volume,
- 41. Therapy MEDICAL Diuretics: reduce vol. Overload Vasodilators: Increase forward output and decrease LV size Digitalis: Control
- 45. MV Repair 1. Mitral valve repair is performed at a lower operative mortality rate than MVR.
- 46. Mitral Valve Prolapse
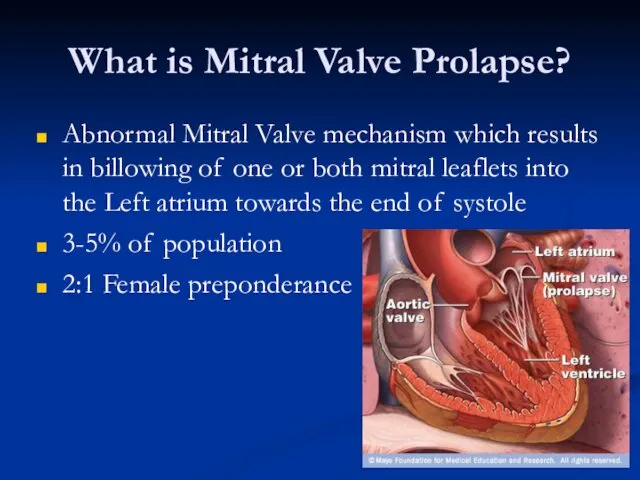
- 47. What is Mitral Valve Prolapse? Abnormal Mitral Valve mechanism which results in billowing of one or
- 48. Pathophysiology Forms Functional Common LV is small, Hyperdynamic Valve is normal Organic (Myxomatous Degeneration) Uncommon LV:
- 49. Symptoms Most patients: None Chest pain Palpitations Easy fatigability Arrhythmias TIA MR
- 50. Signs Mid-systolic Click Systolic murmur with co-existent MR Other connective tissue disorders
- 51. Diagnosis EKG: Non specific ST-T changes CXR: Usually normal Echo: Mitral valve anatomy, leaflet thickness, degree
- 53. Скачать презентацию

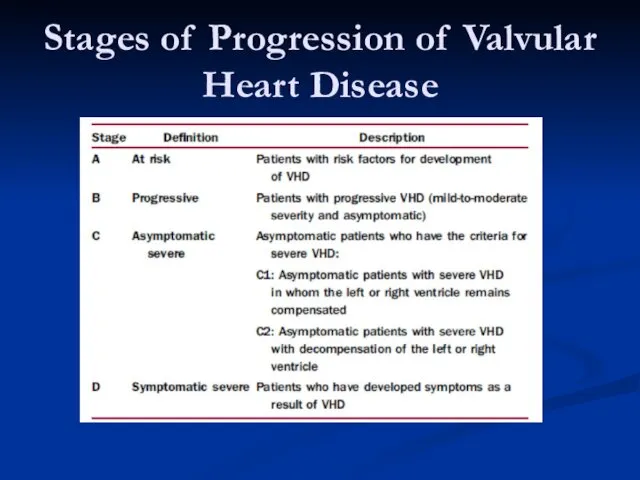
Stages of Progression of Valvular Heart Disease
Stages of Progression of Valvular Heart Disease
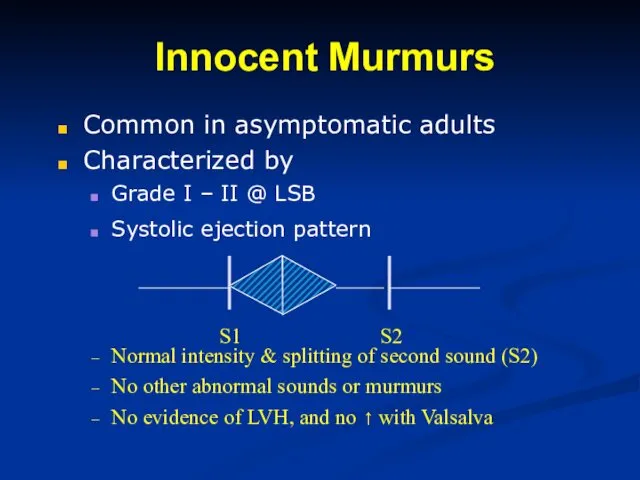
Innocent Murmurs
Common in asymptomatic adults
Characterized by
Grade I – II @ LSB
Systolic
Innocent Murmurs
Common in asymptomatic adults
Characterized by
Grade I – II @ LSB
Systolic
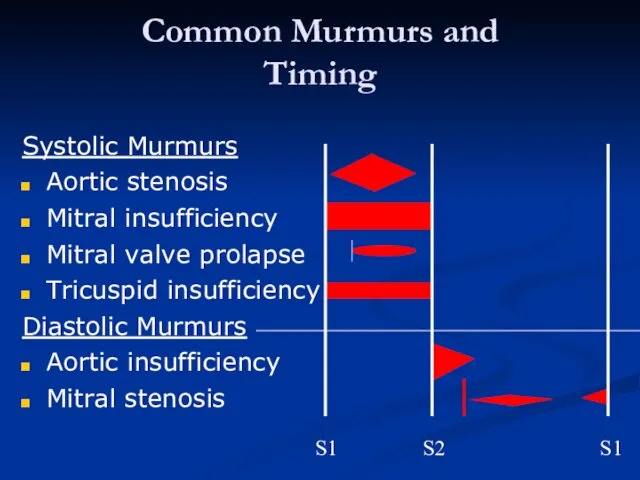
Common Murmurs and
Timing
Systolic Murmurs
Aortic stenosis
Mitral insufficiency
Mitral valve prolapse
Tricuspid insufficiency
Diastolic
Common Murmurs and
Timing
Systolic Murmurs
Aortic stenosis
Mitral insufficiency
Mitral valve prolapse
Tricuspid insufficiency
Diastolic
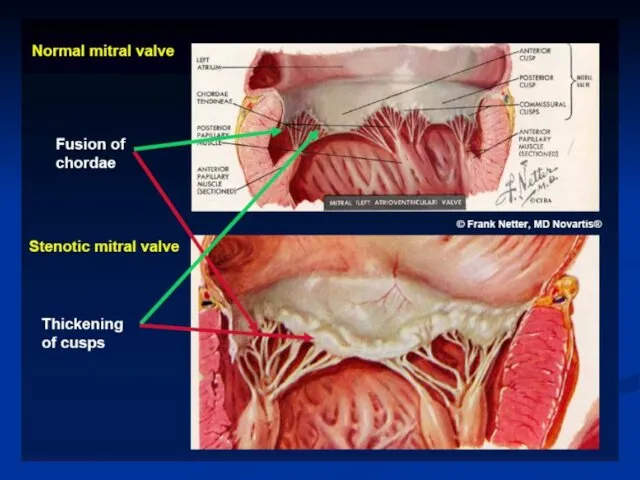
Mitral Valve Stenosis
Mitral Valve Stenosis
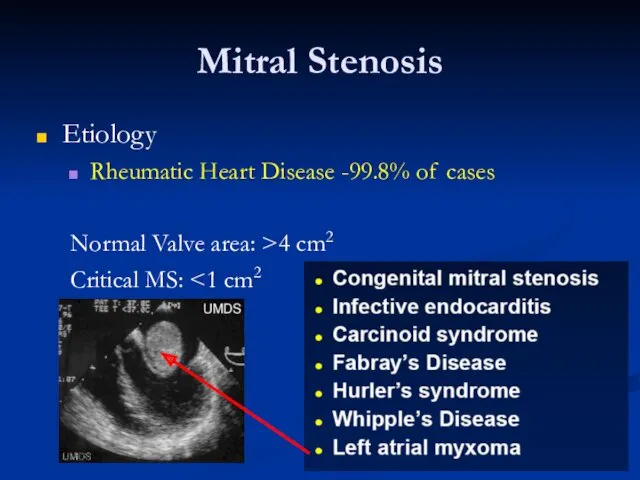
Mitral Stenosis
Etiology
Rheumatic Heart Disease -99.8% of cases
Normal Valve area: >4 cm2
Critical
Mitral Stenosis
Etiology
Rheumatic Heart Disease -99.8% of cases
Normal Valve area: >4 cm2
Critical
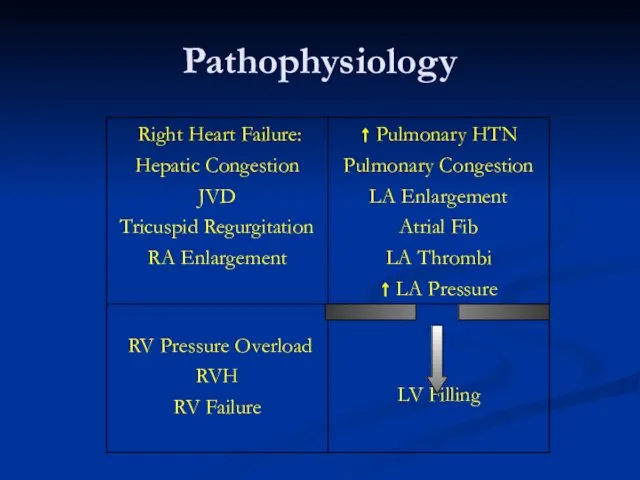
Pathophysiology
Pathophysiology
Pathophysiology
Left atrial dilatation
Allows larger volume at low pressure
Prone to A. Fib
Thrombi
Pathophysiology
Left atrial dilatation
Allows larger volume at low pressure
Prone to A. Fib
Thrombi
Symptoms
Left sided failure
Hemoptysis, URI
Systemic embolism
Palpitations
Fatigue
Right sided failure
Hoarseness
Symptoms
Left sided failure
Hemoptysis, URI
Systemic embolism
Palpitations
Fatigue
Right sided failure
Hoarseness
Signs
Loud S1
Opening snap following S2
Narrow pulse pressure
Diastolic murmur
Atrial Fibrillation
Pulmonary congestion; Right
Signs
Loud S1
Opening snap following S2
Narrow pulse pressure
Diastolic murmur
Atrial Fibrillation
Pulmonary congestion; Right
Recognizing Mitral
Stenosis
Palpation:
Small volume pulse
Tapping apex-palpable S1
+/- palpable opening snap (OS)
RV
Recognizing Mitral
Stenosis
Palpation:
Small volume pulse
Tapping apex-palpable S1
+/- palpable opening snap (OS)
RV
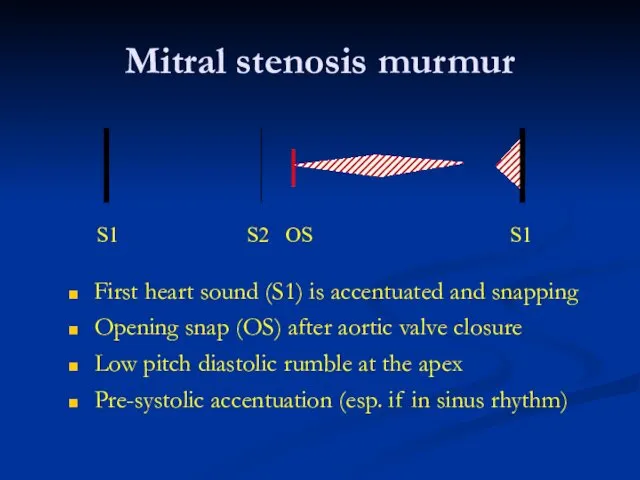
Mitral stenosis murmur
First heart sound (S1) is accentuated and snapping
Opening snap
Mitral stenosis murmur
First heart sound (S1) is accentuated and snapping
Opening snap
Lab Diagnosis
EKG: A Fib, LAE, RVH
CXR: Large LA, Pulm venous congestion,
Lab Diagnosis
EKG: A Fib, LAE, RVH
CXR: Large LA, Pulm venous congestion,
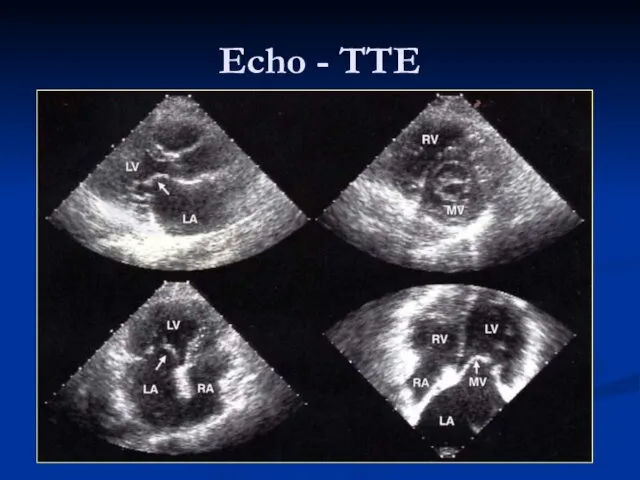
Echo - TTE
Echo - TTE
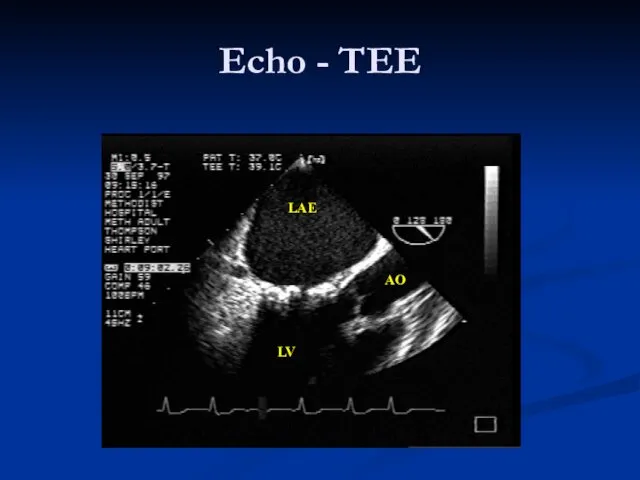
LAE
LV
AO
Echo - TEE
LAE
LV
AO
Echo - TEE
Therapy
Medical
Diuretics: For pulmonary congestion, dyspnea and orthopnea
Rate control in A Fib:
Therapy
Medical
Diuretics: For pulmonary congestion, dyspnea and orthopnea
Rate control in A Fib:
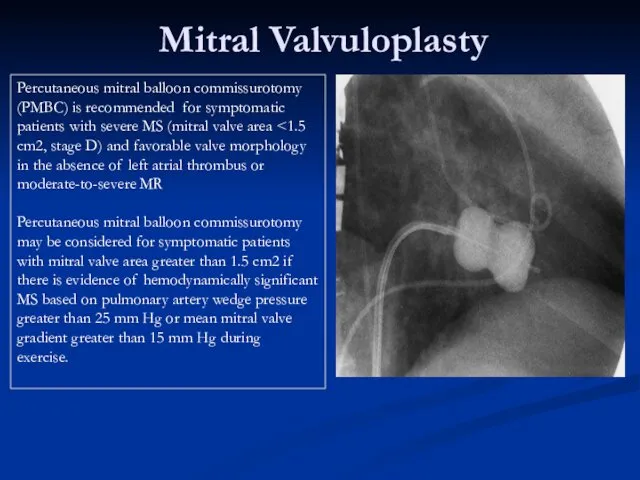
Mitral Valvuloplasty
Percutaneous mitral balloon commissurotomy (PMBC) is recommended for symptomatic patients
Mitral Valvuloplasty
Percutaneous mitral balloon commissurotomy (PMBC) is recommended for symptomatic patients

Therapy
Surgical
Mitral commissurotomy:
Effective long term improvement
Mitral Valve Replacement
Mechanical
Bioprosthetic
Therapy
Surgical
Mitral commissurotomy:
Effective long term improvement
Mitral Valve Replacement
Mechanical
Bioprosthetic
MV Surgery
Mitral valve surgery (repair, commissurotomy, or valve
replacement) is indicated in
MV Surgery
Mitral valve surgery (repair, commissurotomy, or valve
replacement) is indicated in
When to Perform Cardiac Catheterization in Valvular Patient?
No “routine” cardiac
When to Perform Cardiac Catheterization in Valvular Patient?
No “routine” cardiac
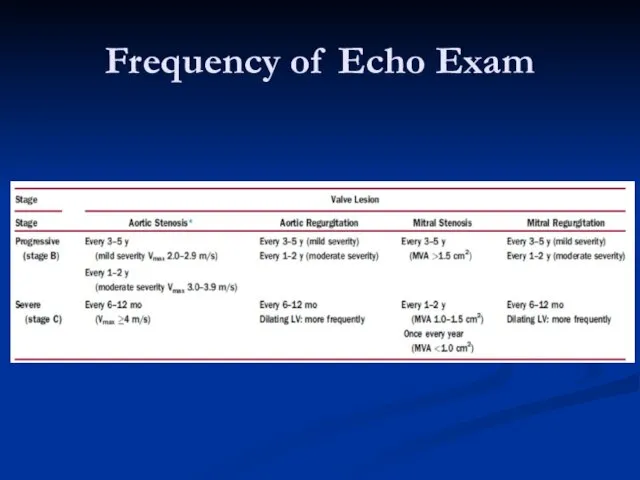
Frequency of Echo Exam
Frequency of Echo Exam
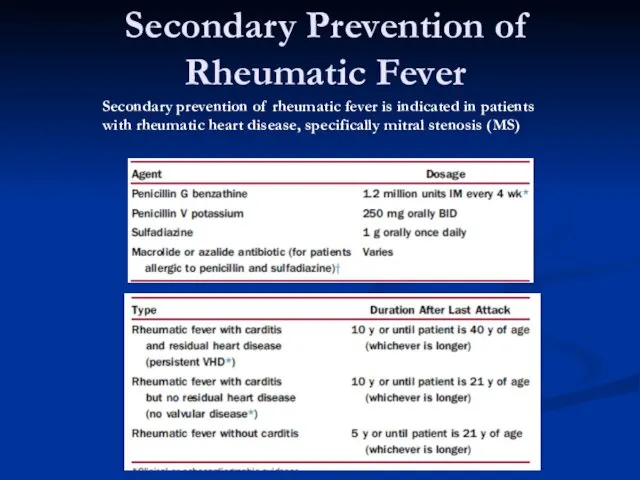
Secondary Prevention of Rheumatic Fever
Secondary prevention of rheumatic fever is indicated
Secondary Prevention of Rheumatic Fever
Secondary prevention of rheumatic fever is indicated

Mitral Regurgitation
Mitral Regurgitation
Etiology
Valvular
Myxomatous CT Disease
Rheumatic
Endocarditis
Chordae
Annulus
Calcification
Papillary Muscles
CAD (Ischemia, Infarction)
Infiltrative disorders
LV Dilatation & Functional Prolapse
Etiology
Valvular
Myxomatous CT Disease
Rheumatic
Endocarditis
Chordae
Annulus
Calcification
Papillary Muscles
CAD (Ischemia, Infarction)
Infiltrative disorders
LV Dilatation & Functional Prolapse
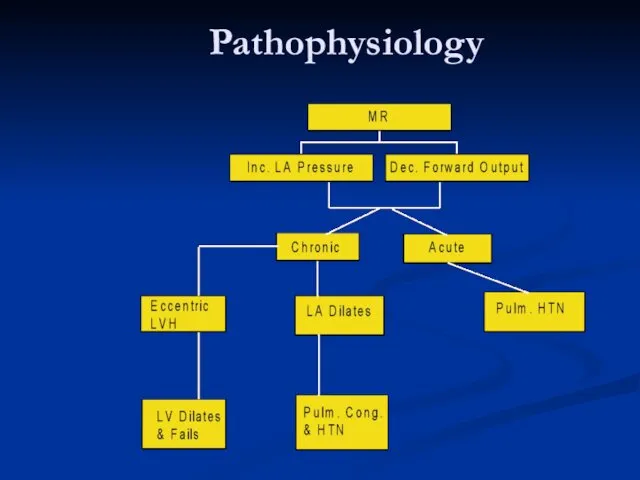
Pathophysiology
Pathophysiology
Symptoms
Similar to MS
Dyspnea, Orthopnea, PND
Fatigue
Pulmonary HTN, Right sided failure
Systemic embolization in
Symptoms
Similar to MS
Dyspnea, Orthopnea, PND
Fatigue
Pulmonary HTN, Right sided failure
Systemic embolization in
Signs
Chronic MR
Hyperdynamic, Displaced apex beat
Apical holosystolic murmur
Pounding pulse
Variable Pulm. HTN
Acute
Signs
Chronic MR
Hyperdynamic, Displaced apex beat
Apical holosystolic murmur
Pounding pulse
Variable Pulm. HTN
Acute
Diagnosis
EKG: LVH, LAE
CXR: Cardiac enlargement
Echo: Abnormal anatomy, chamber size, EF, Qualitative assessment of MR
Diagnosis
EKG: LVH, LAE
CXR: Cardiac enlargement
Echo: Abnormal anatomy, chamber size, EF, Qualitative assessment of MR

Echocardiography
Echocardiography
Echo assessment of severity
Color Doppler – may be misleading
Calculations
Effective regurgitant orifice
Regurgitant
Echo assessment of severity
Color Doppler – may be misleading
Calculations
Effective regurgitant orifice
Regurgitant

Therapy
MEDICAL
Diuretics: reduce vol. Overload
Vasodilators: Increase forward output and decrease LV size
Digitalis:
Therapy
MEDICAL
Diuretics: reduce vol. Overload
Vasodilators: Increase forward output and decrease LV size
Digitalis:


MV Repair
1. Mitral valve repair is performed at a lower operative
MV Repair
1. Mitral valve repair is performed at a lower operative
Mitral Valve Prolapse
Mitral Valve Prolapse
What is Mitral Valve Prolapse?
Abnormal Mitral Valve mechanism which results in
What is Mitral Valve Prolapse?
Abnormal Mitral Valve mechanism which results in
Pathophysiology
Forms
Functional
Common
LV is small, Hyperdynamic
Valve is normal
Organic (Myxomatous Degeneration)
Uncommon
LV: Nl to Large
Thickened
Pathophysiology
Forms
Functional
Common
LV is small, Hyperdynamic
Valve is normal
Organic (Myxomatous Degeneration)
Uncommon
LV: Nl to Large
Thickened
Symptoms
Most patients: None
Chest pain
Palpitations
Easy fatigability
Arrhythmias
TIA
MR
Symptoms
Most patients: None
Chest pain
Palpitations
Easy fatigability
Arrhythmias
TIA
MR
Signs
Mid-systolic Click
Systolic murmur with co-existent MR
Other connective tissue disorders
Signs
Mid-systolic Click
Systolic murmur with co-existent MR
Other connective tissue disorders
Diagnosis
EKG: Non specific ST-T changes
CXR: Usually normal
Echo: Mitral valve anatomy, leaflet thickness, degree of
Diagnosis
EKG: Non specific ST-T changes
CXR: Usually normal
Echo: Mitral valve anatomy, leaflet thickness, degree of
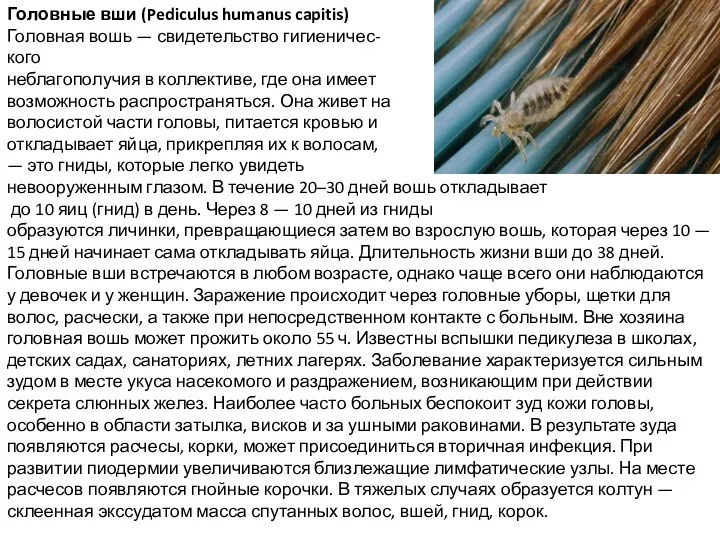 Головные вши (Pediculus humanus capitis)
Головные вши (Pediculus humanus capitis) Гипоплазия эмали: этиология, патогенез, клиника, диагностика, лечение. Наследственные пороки развития твердых тканей зубов
Гипоплазия эмали: этиология, патогенез, клиника, диагностика, лечение. Наследственные пороки развития твердых тканей зубов Көз туберкулезі
Көз туберкулезі Анализ результатов лечения гидроцефалии у детей
Анализ результатов лечения гидроцефалии у детей Основные принципы асептики в терапевтической стоматологии. Инфекционный контроль
Основные принципы асептики в терапевтической стоматологии. Инфекционный контроль Организация ортопедического отделения. Зуботехническая лаборатория
Организация ортопедического отделения. Зуботехническая лаборатория Лечебная физкультура
Лечебная физкультура Стационарлық көмек деңгейіндегі заманауи автоматтандырылған деректер базасымен таныстыру
Стационарлық көмек деңгейіндегі заманауи автоматтандырылған деректер базасымен таныстыру Обеспечение безопасного пространства для пациента и персонала в медицинских организациях
Обеспечение безопасного пространства для пациента и персонала в медицинских организациях Рациональное питание
Рациональное питание Закаливание организма
Закаливание организма Служение больницы и учреждения. Анонимные Наркоманы
Служение больницы и учреждения. Анонимные Наркоманы Одонтогенді гайморит
Одонтогенді гайморит Firearm injuries
Firearm injuries Прививка против гриппа
Прививка против гриппа Особенности сестринского ухода в гериатрии. Болезни органов дыхания у гериатрических пациентов
Особенности сестринского ухода в гериатрии. Болезни органов дыхания у гериатрических пациентов Компенсаторно-приспособительные реакции
Компенсаторно-приспособительные реакции Правила постановки периферического венозного катетера
Правила постановки периферического венозного катетера Тағамдық және санитарлы микробиология
Тағамдық және санитарлы микробиология Особо опасные инфекции (ООИ)
Особо опасные инфекции (ООИ) Гангрена, некроз, язвы, свищи
Гангрена, некроз, язвы, свищи Жүктілік кезіндегі гипертензивті жағдайлар
Жүктілік кезіндегі гипертензивті жағдайлар Дүниежүзілік денсаулық сақтау ұйымы (ДДҰ) Қазақстанда
Дүниежүзілік денсаулық сақтау ұйымы (ДДҰ) Қазақстанда Оқу кестелері мен муляждарды қолдану арқылы ауыз қуысы мен ауыз қуысы құрылымдарының функцияларын зерттеу
Оқу кестелері мен муляждарды қолдану арқылы ауыз қуысы мен ауыз қуысы құрылымдарының функцияларын зерттеу Патогенна дія хімічних та біологічних факторів на організм. Роль спадковості в патології. (Лекція 4)
Патогенна дія хімічних та біологічних факторів на організм. Роль спадковості в патології. (Лекція 4) Средства, влияющие на афферентную нервную систему
Средства, влияющие на афферентную нервную систему Хірургічні захворювання прямої кишки
Хірургічні захворювання прямої кишки Алгоритм манипуляций по оказанию больным первой медицинской помощи при возникновении неотложных ситуаций
Алгоритм манипуляций по оказанию больным первой медицинской помощи при возникновении неотложных ситуаций