- Anxiety Disorders

Содержание
- 2. חרדה- הגדרה מצב בעל ביטויים פיזיים, קוגניטיביים ורגשיים הגורמים לחווה אותם לתחושה לא נעימה של פחד
- 3. Определение понятия Тревога Это душевное состояние , характеризующееся психологическими, физиологическими и когнитивными изменениями, вызывающие у того,
- 4. Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa Не всякая Тревога патологична Патологическая Тревога
- 5. Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 6. תפקידה החיובי של חרדה מוכנות- אנו נוטים להגיב יותר לאיומים המוכרים לנו מאלפי שנות אבולוציה (נחש,
- 7. Что хорошего в Тревоге? Готовность – мы легко реагируем на угрозы, знакомые нам в процессе тысячелетней
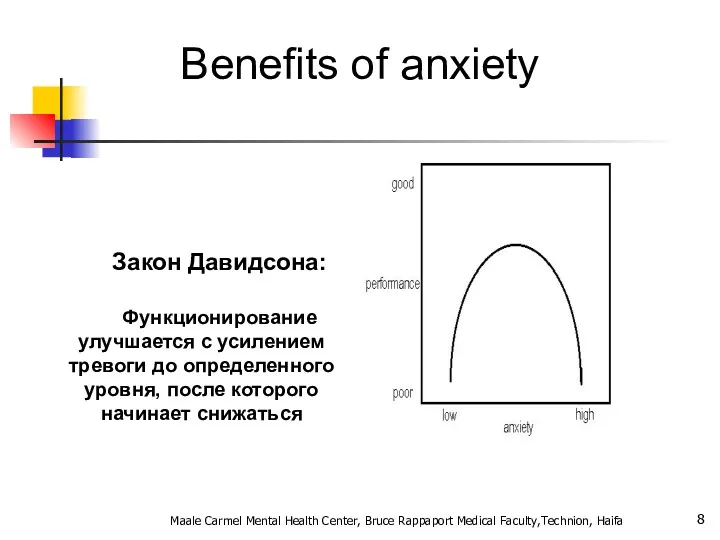
- 8. Benefits of anxiety Закон Давидсона: Функционирование улучшается с усилением тревоги до определенного уровня, после которого начинает
- 9. General considerations for anxiety disorders Often have an early onset- teens or early twenties Show 2:1
- 10. The differential diagnosis of anxiety. Psychiatric and Medical disorders. Psychiatr Clin North Am 1985 Mar;8(1):3-23 Primary
- 11. What characteristics of primary anxiety disorders predict subsequent major depressive disorder. J Clin Psychiatry 2004 May;65(5):618-25
- 12. Anxiety disorders Specific phobia Social anxiety disorder (SAD) Panic disorder (PD) Agoraphobia Generalized anxiety disorder (GAD)
- 13. הבסיס הביולוגי של חרדה מבנים מעורבים: קורטקס פרונטלי מערכת לימבית היפוטלמוס, היפוקמפוס אמיגדלה גזע המוח ההיפופיזה
- 14. Биологическая база Тревоги Замешанные структуры: Логбные доли Лимьическая система Гипоталамус, Гипокампус Амигдала Ствол мога Гипофиз Adrenal
- 15. חרדה- מודלים ביולוגיים אמנם המחקר העכשווי מתמקד במבנים אנטומיים כגון האמיגדלה, ההיפוקמפוס ומסלולים נוירואנדוקרינים אבל... תגובות
- 16. אריק קנדל, חתן פרס נובל לרפואה/פיזיולוגיה לשנת 2000 Maale Carmel Mental Health Center, Bruce Rappaport Medical
- 17. האפליזיה קליפורניקה, רכיכת ים בעלת מערכת עצבים פרימיטיבית המורכבת מ- 20,000 נוירונים בלבד, חלקם הגדול עבים
- 18. נגיעה בסיפון של האפליזיה גורמת לרתיעה נגיעה חוזרת בסיפון של האפליזיה מפחיתה את הרתיעה = הביטואציה
- 19. נגיעה בחישני מגע נקלטת ב SN ה SN מעורר תגובה מוטורית ב MN הביטואציה= ירידה בכמות
- 20. תגובת דחק Fight or Flight תגובה פיזיולוגית לדחק מווסתת דרך ההיפותלמוס ומבנים נוספים מאפשרת להתגונן בפני
- 21. Fight or Flight Физиологическая реакция на стресс Адаптируется с помощью гипоталамуса и других мозговоых структур Позволяет
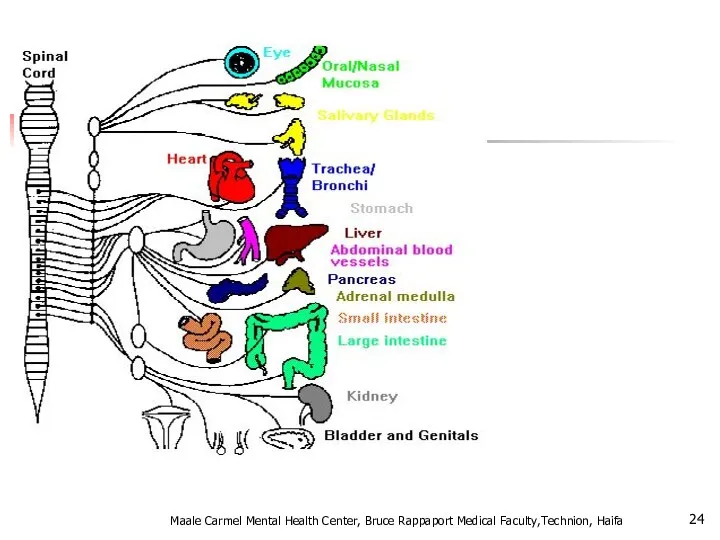
- 22. מה קורה בתגובה הסימפתטית? מתרחשת על ידי אדרנלין ונוראדרנלין מעלה קצב לב והתכווצות הלב קצב נשימה
- 23. Что происходи при реакции симпатической системы? Происходит с помошью адреналина и норадреналина Усиливает частоту и силу
- 24. Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 25. Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa Pierre Janet לכל אדם יש כבאנטום
- 26. Sigmund Freud דחפים מיניים ואגרסיביים מסולקים מעל פני השטח בגלל מוסכמות ואיסורים (סופר אגו) והקונפליקט יוצר
- 27. A Developmental Hierarchy of Anxiety Superego anxiety Castration anxiety Fear of loss of love Separation anxiety
- 28. Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 29. Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 30. Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 31. Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 32. Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 33. אהרון בק: "בבסיס כל פסיכופתולוגיה עומדת הכללת יתר" דיכאון אופוריה, מאניה פאראנויה הפרעת חרדה עצבות שמחה
- 34. А. Барак: "В основе любой патологии лежит чрезмерное и необоснованное обобщение» Депрессия Мания, эйфория Паранойя Паника
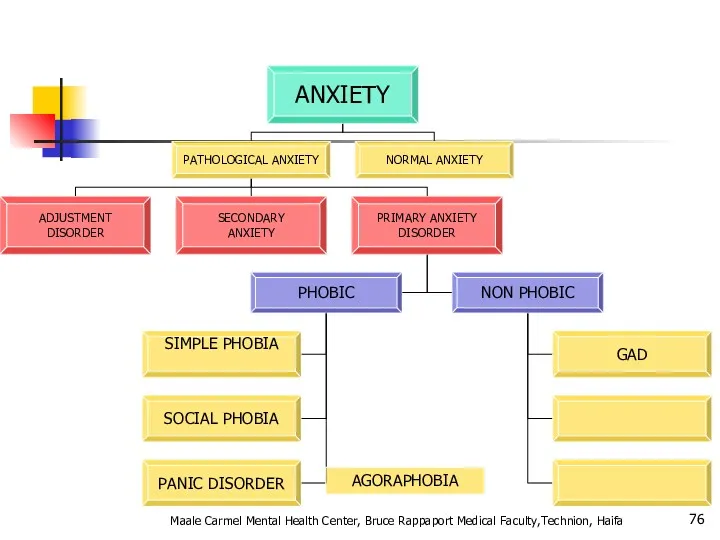
- 35. Pathological Anxiety כחלק מהפרעת הסתגלות כחלק ממחלה / הפרעה נפשית אחרת הפרעת חרדה ראשונית Maale Carmel
- 36. Pathological Anxiety Как часть патологической адаптивной реакции Часть другого патологического расстройства Первичная патологическая реакция Maale Carmel
- 37. Primary Anxiety Disorders הפרעות חרדה לא פוביות: GENERAILIZED ANXIETY DISORDER OCD הפרעות חרדה פוביות: SIMPLE PHOBIA
- 38. Primary Anxiety Disorders Нефобические тревожные реакции: GENERAILIZED ANXIETY DISORDER Фобические тревожные реакии: SIMPLE PHOBIA SOCIAL PHOBIA
- 39. אפידמיולוגיה ברוב המקרים נשים סובלות יותר, במיוחד בגילים בין 16 ל – 40. פחד קהל פי
- 40. Эпидемиология В большинстве своем женщины страдают чаще мужчин, в основном в возрасте 16-40 лет Социофобия в
- 41. Kessler et al. Arch Gen Psychiatry. 1995;52:1048. Kessler et al. Arch Gen Psychiatry. 1994;51:8. Prevalence of
- 42. Genetic Epidemiology of Anxiety Disorders There is significant familial aggregation for PD, GAD, OCD and phobias
- 43. Anxiety Disorders “The anxiety must be out of proportion to the actual danger or threat in
- 44. Agoraphobia , Specific Phobia, and Social Anxiety Disorder Changes in criteria : Clients over 18 do
- 45. Panic Attacks and Agoraphobia are “unlinked” in DSM- 5 DSM- IV terminology describing different types of
- 46. Specific Phobia Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 47. Animal Type Natural Environment Type (e.g., heights, storms, water) Blood-Injection-Injury Type Situational Type (e.g., airplanes, elevators,
- 48. Specific Phobia Marked or persistent fear (>6 months) that is excessive or unreasonable cued by the
- 49. SPECIFIC PHOBIA בשאר הזמן תפקוד נורמאלי המנעות מאפשרת חיים נורמאליים שכיחות גבוהה –עד 20% מהאוכלוסייה בד"כ
- 50. SOCIAL PHOBIA בדומה לפוביה פשוטה אך כאן הפחד חסר הגיון מאינטראקציה חברתית, ומכאן: יותר פגיעה תפקודית
- 51. Incidence of social anxiety disorders and the consistent risk for secondary depression in the first three
- 52. אבחנה יותר בעייתית (הפרעת אישיות?? ) שני סוגים: LIMITED PERVASIVE Maale Carmel Mental Health Center, Bruce
- 53. What is going on in their brains?? Study of 16 SAD patients and 16 matched controls
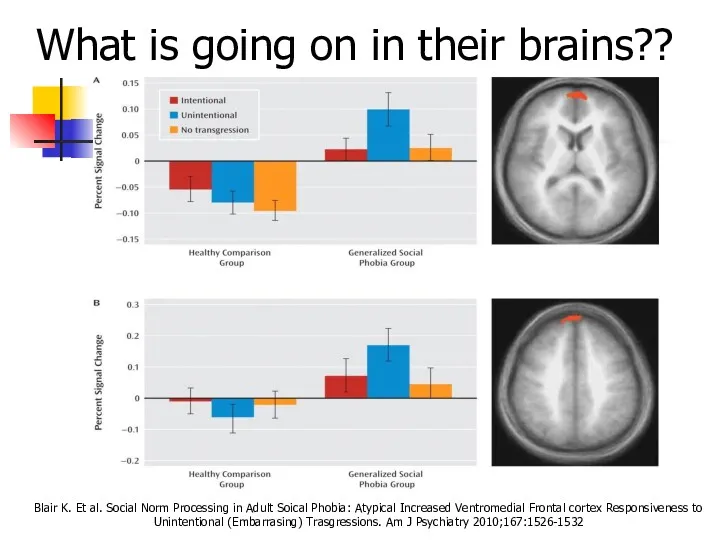
- 54. What is going on in their brains?? Both groups ↑ medial prefrontal cortex activity in response
- 55. What is going on in their brains?? Blair K. Et al. Social Norm Processing in Adult
- 56. Functional imaging studies in SAD Several studies have found hyperactivity of the amygdala even with a
- 57. Social Anxiety Disorder treatment Social skills training, behavior therapy, cognitive therapy Medication – SSRIs, SNRIs, MAOIs,
- 58. סיבוכים: דיכאון שימוש בחומרים ממכרים Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 59. PANIC DISORDER התקף אימה, חרדה בעוצמה קיצונית מופיע ספונטאנית (לפחות בתחילת המחלה) הכללת אירועים חרדה מטרימהANTICIPATION
- 60. Panic Disorder Recurrent unexpected panic attacks and for a one month period or more of: Persistent
- 61. A Panic Attack is: Palpitations or rapid heart rate Sweating Trembling or shaking Shortness of breath
- 62. Panic disorder epidemiology 2-3% of general population; 5-10% of primary care patients.Onset in teens or early
- 63. Things to keep in mind A panic attack ≠ panic disorder Panic disorder often has a
- 64. With Agoraphobia פחד או המנעות להיות במקומות או במצבים בהם יש קושי לברוח או לקבל עזרה.
- 65. טיפול: שילוב של טיפול CBT ותרופות: נוגדי דיכאון נוגדי חרדה לשלב הראשון סיבוכים : דיכאון עד
- 66. Panic Disorder Comorbidity 50-60% have lifetime major depression One third have current depression 20-25% have history
- 67. Panic Disorder Etiology Drug/Alcohol Genetics Social learning Cognitive theories Neurobiology/conditioned fear Psychosocial stressors Prior separation anxiety
- 68. Treatment See 70% or better treatment response Education, reassurance, elimination of caffeine, alcohol, drugs, OTC stimulants
- 69. Agoraphobia Marked fear or anxiety for more than 6 months about two or more of the
- 70. Agoraphobia The individual fears or avoids these situations because escape might be difficult or help might
- 71. Prevalence 2% of the population Females to males:2:1 Mean onset is 17 years 30% of persons
- 72. Generalized Anxiety פחד או חרדה מוגזמים, ללא כל אחיזה במציאות, מלווים בביטוים של מתח מוטורי, פעילות
- 73. Generalized Anxiety Disorder Excessive worry more days than not for at least 6 months about a
- 74. GAD Comorbidity 90% have at least one other lifetime Axis I Disorder 66% have another current
- 75. Long-Term Treatment Of GAD Need to treat long-term Full relapse in approximately 25% of patients 1
- 76. Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa AGORAPHOBIA
- 77. Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 78. Pharmacotherapy for Anxiety Disorders Antidepressants Serotonin Selective Reuptake Inhibitors (SSRIs) Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) Atypical Antidepressants
- 79. Benzodiazepines Other Agents Azaspirones Beta blockers Anticonvulsants Other strategies Maale Carmel Mental Health Center, Bruce Rappaport
- 80. Discontinuation of Treatment for Anxiety Disorders Withdrawal/rebound more common with Bzd than other anxiolytic treatment Relapse:
- 81. Strategies for Anxiolytic Discontinuation Slow taper Switch to longer-acting agent for taper Cognitive-Behavioral therapy Adjunctive Antidepressant
- 82. Strategies for Refractory Anxiety Disorder Maximize dose Combine antidepressant and benzodiazepine Administer cognitive-behavioral therapy Attend to
- 83. Strategies for Refractory Anxiety Disorders Augmentation Anticonvulsants Gabapentin Valproate Topiramate Beta blocker Buspirone Clonidine/Guanfacine Pindolol -nonselective
- 84. סיכום: Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa AGORAPHOBIA
- 85. Screening questions How ever experienced a panic attack? (Panic) Do you consider yourself a worrier? (GAD)
- 86. Take home points Anxiety, Obsessive-Compulsive and Related, and Trauma and Stressor-related disorders are common, common, common!
- 87. Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa Question
- 89. Trauma- and Stressor-Related Disorders New chapter in DSM-5 brings together anxiety disorders that are preceded by
- 90. Disinhibited Social Engagement Disorder “The essential feature of disorder is a pattern of behavior that involves
- 91. A. PTSD A Criterion B. No mandatory (e.g., dissociative, etc.) symptoms from any cluster C. Nine
- 92. Adjustment Disorders are redefined as an array of stress-response syndromes occurring after exposure to a distressing
- 93. Chronic Adjustment Disorder Omitted by mistake from DSM-5 Acute AD – less than 6 months Chronic
- 94. Other Specified Trauma/Stressor-Related Disorder (309.89) AD with duration more than 6 months without prolonged duration of
- 95. Reactive Attachment Disorder Emotionally withdrawn behavior Social/emotional disturbance - reduced responsiveness, limited affect &/or irritability, sadness
- 96. Persistent Complex Bereavement Disorder Onset > 12 months after death of loved one Yearning/Sorrow/Pre-occupation with deceased
- 97. Persistent Complex Bereavement Disorder (PCBD) Diagnostic Criteria-ICD The person experienced the death of a close relative
- 98. Persistent Complex Bereavement Disorder (PCBD) Preoccupation with the circumstances of the death. In children, this preoccupation
- 99. Reactive Distress to the Death Marked difficulty accepting the death. In children, this is dependent on
- 100. Social/Identity Disruption A desire to die in order to be with the deceased. Difficulty trusting other
- 101. Specify if: With Traumatic Bereavement: Following a death that occurred under traumatic circumstances (e.g. homicide, suicide,
- 102. Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 103. Changes in PTSD Criteria Four symptom clusters, rather than three -Re-experiencing -Avoidance -Persistent negative alterations in
- 104. Changes in PTSD Criteria DSM-5 more clearly defines what constitutes a traumatic event Sexual assault is
- 105. Changes in PTSD Criteria Recognition of PTSD in Young children Developmentally sensitive: Criteria have been modified
- 106. DSM-5: PTSD Criterion A A. The person was exposed to: death, threatened death, actual or threatened
- 107. Criterion A (continued): 3. Indirectly, by learning that a close relative or close friend was exposed
- 108. CRITERION B - Intrusion (5 Sx – Need 1) Recurrent, involuntary and intrusive recollections * *
- 109. C. Persistent effortful avoidance of distressing trauma-related stimuli after the event (1/2 symptoms needed): Trauma-related thoughts
- 110. CRITERION D – negative alterations in cognition & Mood (7 Sx – Need 2) Inability to
- 111. CRITERION E – Trauma-related alterations in arousal and reactivity that began or worsened after the traumatic
- 112. PTSD Criteria for DSM-5 F. Persistence of symptoms (in Criteria B, C, D and E) for
- 113. Preschool Subtype: 6 Years or Younger Relative to broader diagnosis for adults (or those over 6
- 114. A. In children (younger than 6 years), exposure to actual or threatened death, serious injury, or
- 115. DSM-5: Preschool PTSD Criterion B B. Presence of one or more intrusion symptoms associated with the
- 116. Preschool PTSD Criterion C One or more symptoms from either Criterion C or D below: C.
- 117. Preschool PTSD Criterion E E. Alterations in arousal and reactivity associated with the traumatic event,, as
- 118. Preschool PTSD for DSM-5 F. Duration (of Criteria B, C, D and E) is more than
- 119. Summary: PTSD in DSM-5 Perhaps PTSD should be re-conceptualized as a spectrum disorder in which several
- 120. Dissociative Subtype of PTSD New subtype for both age groupings of PTSD diagnosis: Meets PTSD diagnostic
- 121. specifiers Specify whether: With dissociative symptoms: The individual’s symptoms meet the criteria for PTSD, and in
- 122. CAPS Clinician Administered PTSD Scale National Center for PTSD (www.ptsd.va.gov) 20 item structured clinical interview Primarily
- 123. 1. (B1) Recurrent, involuntary, and intrusive distressing memories of the traumatic event(s). Note: In children older
- 124. PCL Posttraumatic Check List National Center for PTSD (www.ptsd.va.gov) Simple, easy to administer Self-report or clinician
- 125. TRS Trauma Recovery Scale Gentry, 1996 Developed as an outcome instrument Good psychometrics (Chronbach’s a =
- 126. Early Sessions Graphic Time Line of life including ALL significant traumatic experiences Verbal Narrative using GTL
- 127. PTSD Epidemiology 7-9% of general population 60-80% of trauma victims 30% of combat veterans 50-80% of
- 128. PTSD Epidemiology בין אבחנות בודדות ב DSM שמדברת על אטיולוגיה זוהי תגובה נפשית קשה הנגרמת כתגובה
- 129. Comorbidities Depression Other anxiety disorders Substance use disorders Somatization Dissociative disorders Maale Carmel Mental Health Center,
- 130. Acute PTSD - symptoms less than three months Chronic PTSD - symptoms more than three months
- 131. Can occur at any age, including childhood, and can affect anyone. Individuals who have recently immigrated
- 132. Onset Symptoms usually begin within the first 3 months after the trauma, although there may be
- 133. Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 134. Course The symptoms and the relative predominance of re-experiencing, avoidance, and increased arousal symptoms may vary
- 135. Course Continued The severity, duration, and proximity of an individual’s exposure to a traumatic event are
- 136. Rape (49%) Severe beating or physical assault (31.9%) Other sexual assault (23.7%) Serious accident or injury
- 137. Differential Diagnosis Differential diagnosis of the disorder or problem; that is, what other disorders or problems
- 138. While the symptoms of posttraumatic stress disorder (PTSD) may seem similar to those of other disorders,
- 139. Differences between Acute Stress Disorder In general, the symptoms of acute stress disorder must occur within
- 140. Differences between PTSD and Obsessive-Compulsive Disorder Both have recurrent, intrusive thoughts as a symptom, but the
- 141. Differences Between PTSD and Adjustment Disorder PTSD symptoms can also seem similar to adjustment disorder because
- 142. Differences Between PTSD and Depression Depression after trauma and PTSD both may present numbing and avoidance
- 143. מי מיועד יותר? עוצמה של סטרסור פתאומיות (לא צפוי) חוסר יכולת לשלוט על מתרחש sexual as
- 144. An adult's risk for psychological distress will increase as the number of the following factors increases:
- 145. For women, the presence of a spouse, especially if he is significantly distressed Psychiatric history Severe
- 146. Why PTSD Victims Might Be Resistant to Getting Help Sometimes hard because people expect to be
- 147. During a Traumatic Event Norepinephrine- Mobilizing fear, the flight response, sympathetic activation, consolidating memory Too much
- 148. Causal Attributions “PTSD is typified by both automatic, involuntary symptoms, (e.g. flashbacks, intrusive thoughts, autonomic hyperarousal)
- 149. Treatment Individual Therapy Group Support (especially for Chronic PTSD) Medication
- 150. Treatment Continued For PTSD in children, adolescents, and geriatrics the preferred treatment is psychotherapy Acute PTSD
- 151. Treatment Continued Exposure Therapy- Education about common reactions to trauma, breathing retraining, and repeated exposure to
- 152. Treatment Continued “Cognitive Restructuring involved teaching and reinforcing self-monitoring or thoughts and emotions, identifying automatic thoughts
- 153. Medications approved for the treatment of Anxiety Disorders including PTSD SSRIs – Sertraline (Zoloft), Paroxetine (Paxil),
- 154. Tricyclic Antidepressants- Clomiprimine (Anafranil), Doxepin (Sinequan) Nortriptyline (Aventyl), Amitriptyline (Elavil), Maprotiline (Ludiomil) Desipramine (Norpramin) Affects concentration
- 155. Treatment With treatment, symptoms should improve after 3 months In Chronic PTSD cases, 1-2 years
- 156. Noradrenergic Agents Beta Blockers – Propranolol Future Direction of Treatment
- 157. PTSD - Treatment שילוב של טיפול תרופתי בנוגדי דיכאון וחרדה בפועל מגיעים לכל הספקטרום של התרופות
- 158. Future Direction of Treatment Continued “Early Diagnosis and intervention- either psychotherapeutic or pharmacological- following trauma may
- 159. PTSD Myths PTSD is a complex disorder that often is misunderstood. Not everyone who experiences a
- 160. PTSD Myths Continued MYTH: People should be able to move on with their lives after a
- 161. PTSD Myths Continued MYTH: People suffer from PTSD right after they experience a traumatic event. FACT:
- 162. What is Prolonged Exposure? PE is a type of CBT, which is designed to specifically target
- 163. education about common reactions to trauma breathing retraining (or relaxation training) prolonged (repeated) exposure to trauma
- 164. Post-treatment data from a study conducted by Foa and colleagues (1999) comparing prolonged exposure (PE), stress
- 165. Combat Reaction Combat stress reaction, better known as "Shell Shock" is the post traumatic reaction of
- 166. The Background of Combat Reaction The transition from civilian life to military life is acute. The
- 167. In wartime, a new and even more acute transition is added - the transition from conditions
- 168. On the other hand the soldier feels solidarity with his unit, pride and honor and a
- 169. Risk Factors Risk factors for Combat Reaction are all the factors that influence the incidence of
- 170. Enforced passivity. When the soldier is deprived of activity and is in a state of waiting
- 171. PIE principles Proximity - treat the casualties close to the front and within sound of the
- 172. The US services now use the more recently developed BICEPS principles: Brevity Immediacy Centrality or Contact
- 173. Treatment results Data from the 1982 Lebanon war showed that with proximal treatment 90% of CSR
- 174. Controversy Throughout wars but notably during the Vietnam War there has been a conflict amongst doctors
- 175. תסמונת שואה דור ראשון דור שני Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
- 176. Re-experiencing Intrusive thoughts Nightmares flashbacks Avoidance Hyperarousal Reminders Hyperarousal Angry outbursts Startle response Lacks concentration Disomnia
- 178. Скачать презентацию
חרדה- הגדרה
מצב בעל ביטויים פיזיים, קוגניטיביים ורגשיים הגורמים לחווה אותם לתחושה
חרדה- הגדרה
מצב בעל ביטויים פיזיים, קוגניטיביים ורגשיים הגורמים לחווה אותם לתחושה
Определение понятия Тревога
Это душевное состояние , характеризующееся психологическими, физиологическими и когнитивными
Определение понятия Тревога
Это душевное состояние , характеризующееся психологическими, физиологическими и когнитивными
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Не
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Не

Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
תפקידה החיובי של חרדה
מוכנות- אנו נוטים להגיב יותר לאיומים המוכרים לנו
תפקידה החיובי של חרדה
מוכנות- אנו נוטים להגיב יותר לאיומים המוכרים לנו
Что хорошего в Тревоге?
Готовность – мы легко реагируем на угрозы,
Что хорошего в Тревоге?
Готовность – мы легко реагируем на угрозы,
Benefits of anxiety
Закон Давидсона:
Функционирование улучшается с усилением тревоги до определенного уровня,
Benefits of anxiety
Закон Давидсона:
Функционирование улучшается с усилением тревоги до определенного уровня,

General considerations for anxiety disorders
Often have an early onset- teens or
General considerations for anxiety disorders
Often have an early onset- teens or
The differential diagnosis of anxiety. Psychiatric and Medical disorders. Psychiatr Clin
The differential diagnosis of anxiety. Psychiatric and Medical disorders. Psychiatr Clin
What characteristics of primary anxiety disorders predict subsequent major depressive disorder.
What characteristics of primary anxiety disorders predict subsequent major depressive disorder.
Anxiety disorders
Specific phobia
Social anxiety disorder (SAD)
Panic disorder (PD)
Agoraphobia
Generalized anxiety disorder
Anxiety disorders
Specific phobia
Social anxiety disorder (SAD)
Panic disorder (PD)
Agoraphobia
Generalized anxiety disorder

הבסיס הביולוגי של חרדה
מבנים מעורבים:
קורטקס פרונטלי
מערכת לימבית
היפוטלמוס, היפוקמפוס אמיגדלה
גזע המוח
ההיפופיזה
Adrenal Axis
המערכת
הבסיס הביולוגי של חרדה
מבנים מעורבים:
קורטקס פרונטלי
מערכת לימבית
היפוטלמוס, היפוקמפוס אמיגדלה
גזע המוח
ההיפופיזה
Adrenal Axis
המערכת
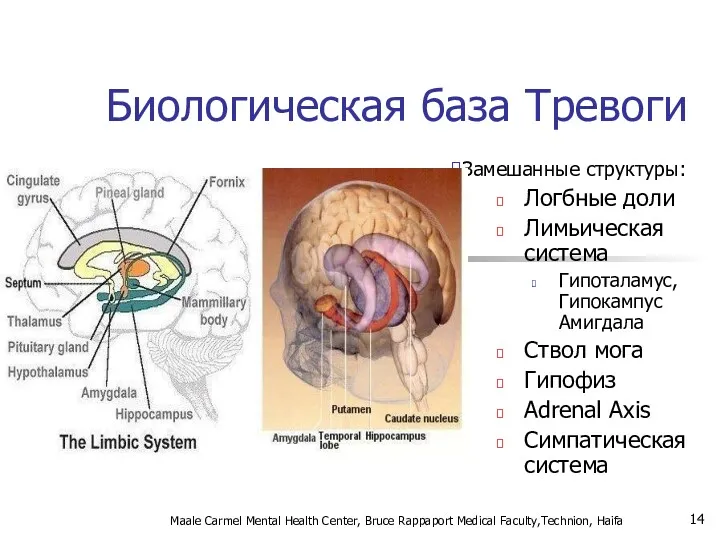
Биологическая база Тревоги
Замешанные структуры:
Логбные доли
Лимьическая система
Гипоталамус, Гипокампус Амигдала
Ствол мога
Гипофиз
Adrenal Axis
Симпатическая система
Maale
Биологическая база Тревоги
Замешанные структуры:
Логбные доли
Лимьическая система
Гипоталамус, Гипокампус Амигдала
Ствол мога
Гипофиз
Adrenal Axis
Симпатическая система
Maale
חרדה- מודלים ביולוגיים
אמנם המחקר העכשווי מתמקד במבנים אנטומיים כגון האמיגדלה, ההיפוקמפוס
חרדה- מודלים ביולוגיים
אמנם המחקר העכשווי מתמקד במבנים אנטומיים כגון האמיגדלה, ההיפוקמפוס
אריק קנדל, חתן פרס נובל לרפואה/פיזיולוגיה לשנת 2000
Maale Carmel Mental Health
אריק קנדל, חתן פרס נובל לרפואה/פיזיולוגיה לשנת 2000
Maale Carmel Mental Health
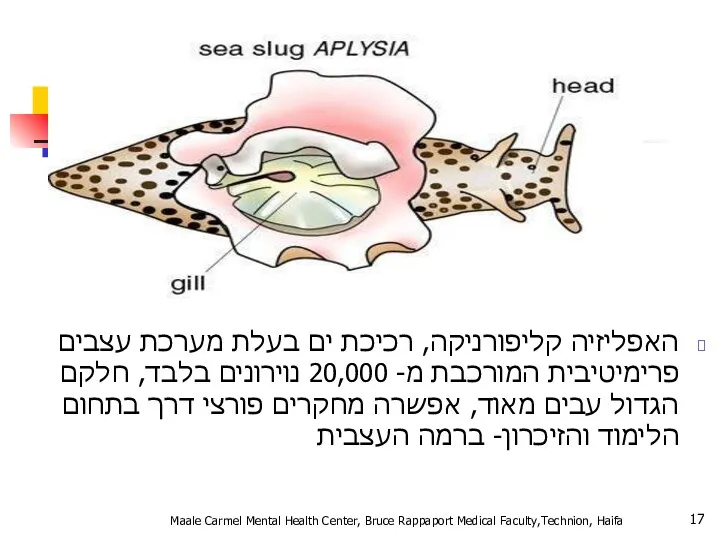
האפליזיה קליפורניקה, רכיכת ים בעלת מערכת עצבים פרימיטיבית המורכבת מ- 20,000
האפליזיה קליפורניקה, רכיכת ים בעלת מערכת עצבים פרימיטיבית המורכבת מ- 20,000
נגיעה בסיפון של האפליזיה גורמת לרתיעה
נגיעה חוזרת בסיפון של האפליזיה מפחיתה
נגיעה בסיפון של האפליזיה גורמת לרתיעה
נגיעה חוזרת בסיפון של האפליזיה מפחיתה
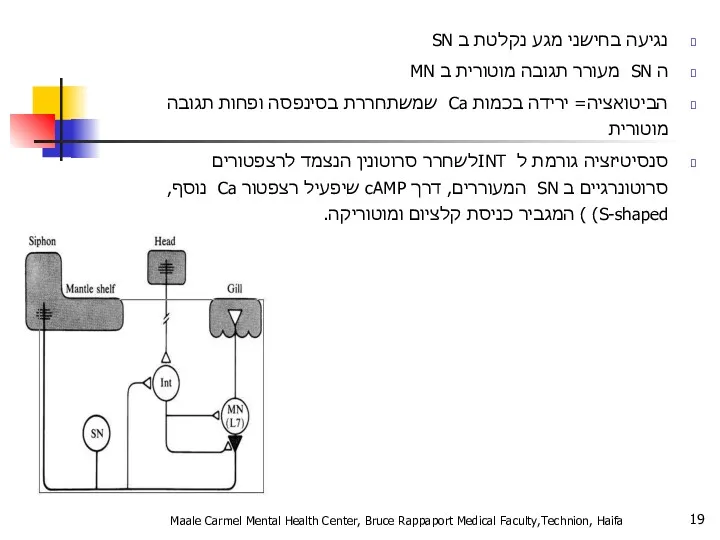
נגיעה בחישני מגע נקלטת ב SN
ה SN מעורר תגובה מוטורית ב
נגיעה בחישני מגע נקלטת ב SN
ה SN מעורר תגובה מוטורית ב
תגובת דחק
Fight or Flight
תגובה פיזיולוגית לדחק
מווסתת דרך ההיפותלמוס ומבנים נוספים
מאפשרת להתגונן
תגובת דחק
Fight or Flight
תגובה פיזיולוגית לדחק
מווסתת דרך ההיפותלמוס ומבנים נוספים
מאפשרת להתגונן
Fight or Flight
Физиологическая реакция на стресс
Адаптируется с помощью гипоталамуса и других
Fight or Flight
Физиологическая реакция на стресс
Адаптируется с помощью гипоталамуса и других
מה קורה בתגובה הסימפתטית?
מתרחשת על ידי אדרנלין ונוראדרנלין
מעלה קצב לב
מה קורה בתגובה הסימפתטית?
מתרחשת על ידי אדרנלין ונוראדרנלין
מעלה קצב לב
Что происходи при реакции симпатической системы?
Происходит с помошью адреналина и норадреналина
Усиливает
Что происходи при реакции симпатической системы?
Происходит с помошью адреналина и норадреналина
Усиливает
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Pierre
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Pierre
Sigmund Freud
דחפים מיניים ואגרסיביים מסולקים מעל פני השטח בגלל מוסכמות ואיסורים
Sigmund Freud
דחפים מיניים ואגרסיביים מסולקים מעל פני השטח בגלל מוסכמות ואיסורים
A Developmental Hierarchy of Anxiety
Superego anxiety
Castration anxiety
Fear of
A Developmental Hierarchy of Anxiety
Superego anxiety
Castration anxiety
Fear of

Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa

Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa

Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa

Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
אהרון בק:
"בבסיס כל פסיכופתולוגיה עומדת הכללת יתר"
דיכאון
אופוריה, מאניה
פאראנויה
הפרעת חרדה
עצבות
שמחה
חשד
חרדה
Maale Carmel
אהרון בק:
"בבסיס כל פסיכופתולוגיה עומדת הכללת יתר"
דיכאון
אופוריה, מאניה
פאראנויה
הפרעת חרדה
עצבות
שמחה
חשד
חרדה
Maale Carmel
А. Барак:
"В основе любой патологии лежит чрезмерное и необоснованное обобщение»
Депрессия
Мания, эйфория
Паранойя
Паника
Сниженое
А. Барак:
"В основе любой патологии лежит чрезмерное и необоснованное обобщение»
Депрессия
Мания, эйфория
Паранойя
Паника
Сниженое
Pathological Anxiety
כחלק מהפרעת הסתגלות
כחלק ממחלה / הפרעה נפשית אחרת
הפרעת חרדה ראשונית
Maale
Pathological Anxiety
כחלק מהפרעת הסתגלות
כחלק ממחלה / הפרעה נפשית אחרת
הפרעת חרדה ראשונית
Maale
Pathological Anxiety
Как часть патологической адаптивной реакции
Часть другого патологического расстройства
Первичная патологическая
Pathological Anxiety
Как часть патологической адаптивной реакции
Часть другого патологического расстройства
Первичная патологическая
Primary Anxiety Disorders
הפרעות חרדה לא פוביות:
GENERAILIZED ANXIETY DISORDER
OCD
הפרעות חרדה פוביות:
SIMPLE PHOBIA
SOCIAL
Primary Anxiety Disorders
הפרעות חרדה לא פוביות:
GENERAILIZED ANXIETY DISORDER
OCD
הפרעות חרדה פוביות:
SIMPLE PHOBIA
SOCIAL
Primary Anxiety Disorders
Нефобические тревожные реакции:
GENERAILIZED ANXIETY DISORDER
Фобические тревожные реакии:
SIMPLE PHOBIA
SOCIAL PHOBIA
PANIC
Primary Anxiety Disorders
Нефобические тревожные реакции:
GENERAILIZED ANXIETY DISORDER
Фобические тревожные реакии:
SIMPLE PHOBIA
SOCIAL PHOBIA
PANIC

אפידמיולוגיה
ברוב המקרים נשים סובלות יותר, במיוחד בגילים בין 16 ל –
אפידמיולוגיה
ברוב המקרים נשים סובלות יותר, במיוחד בגילים בין 16 ל –
Эпидемиология
В большинстве своем женщины страдают чаще мужчин, в основном в возрасте
Эпидемиология
В большинстве своем женщины страдают чаще мужчин, в основном в возрасте
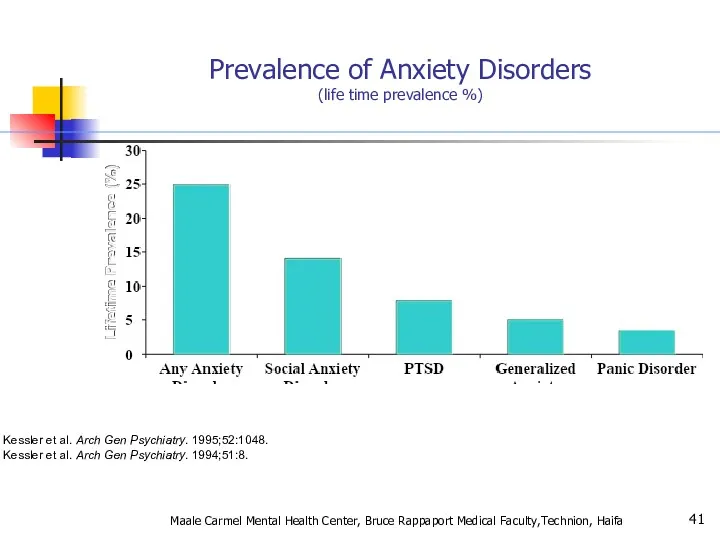
Kessler et al. Arch Gen Psychiatry. 1995;52:1048.
Kessler et al. Arch Gen
Kessler et al. Arch Gen Psychiatry. 1995;52:1048.
Kessler et al. Arch Gen
Genetic Epidemiology of Anxiety Disorders
There is significant familial aggregation for PD,
Genetic Epidemiology of Anxiety Disorders
There is significant familial aggregation for PD,
Anxiety Disorders
“The anxiety must be out of proportion to the actual
Anxiety Disorders
“The anxiety must be out of proportion to the actual
Agoraphobia ,
Specific Phobia, and
Social Anxiety Disorder
Changes in criteria :
Agoraphobia ,
Specific Phobia, and
Social Anxiety Disorder
Changes in criteria :
Panic Attacks and Agoraphobia are “unlinked” in DSM- 5
DSM- IV terminology
Panic Attacks and Agoraphobia are “unlinked” in DSM- 5
DSM- IV terminology
Specific Phobia
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Specific Phobia
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Animal Type
Natural Environment Type (e.g., heights, storms, water)
Blood-Injection-Injury Type
Animal Type
Natural Environment Type (e.g., heights, storms, water)
Blood-Injection-Injury Type
Specific Phobia
Marked or persistent fear (>6 months) that is excessive or
Specific Phobia
Marked or persistent fear (>6 months) that is excessive or
SPECIFIC PHOBIA
בשאר הזמן תפקוד נורמאלי
המנעות מאפשרת חיים נורמאליים
שכיחות גבוהה –עד 20%
SPECIFIC PHOBIA
בשאר הזמן תפקוד נורמאלי
המנעות מאפשרת חיים נורמאליים
שכיחות גבוהה –עד 20%
SOCIAL PHOBIA
בדומה לפוביה פשוטה אך כאן הפחד חסר הגיון מאינטראקציה חברתית,
SOCIAL PHOBIA
בדומה לפוביה פשוטה אך כאן הפחד חסר הגיון מאינטראקציה חברתית,
Incidence of social anxiety disorders and the consistent risk for secondary
Incidence of social anxiety disorders and the consistent risk for secondary
אבחנה יותר בעייתית (הפרעת אישיות?? )
שני סוגים:
LIMITED
PERVASIVE
Maale Carmel Mental Health Center,
אבחנה יותר בעייתית (הפרעת אישיות?? )
שני סוגים:
LIMITED
PERVASIVE
Maale Carmel Mental Health Center,
What is going on in their brains??
Study of 16 SAD patients
What is going on in their brains??
Study of 16 SAD patients
What is going on in their brains??
Both groups ↑ medial
What is going on in their brains??
Both groups ↑ medial
What is going on in their brains??
Blair K. Et al. Social
What is going on in their brains??
Blair K. Et al. Social
Functional imaging studies in SAD
Several studies have found hyperactivity of the
Functional imaging studies in SAD
Several studies have found hyperactivity of the
Social Anxiety Disorder treatment
Social skills training, behavior therapy, cognitive therapy
Medication –
Social Anxiety Disorder treatment
Social skills training, behavior therapy, cognitive therapy
Medication –

סיבוכים:
דיכאון
שימוש בחומרים ממכרים
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion,
סיבוכים:
דיכאון
שימוש בחומרים ממכרים
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion,

PANIC DISORDER
התקף אימה, חרדה בעוצמה קיצונית
מופיע ספונטאנית (לפחות בתחילת המחלה)
PANIC DISORDER
התקף אימה, חרדה בעוצמה קיצונית
מופיע ספונטאנית (לפחות בתחילת המחלה)
Panic Disorder
Recurrent unexpected panic attacks and for a one month period
Panic Disorder
Recurrent unexpected panic attacks and for a one month period
A Panic Attack is:
Palpitations or rapid heart rate
Sweating
Trembling or shaking
Shortness
A Panic Attack is:
Palpitations or rapid heart rate
Sweating
Trembling or shaking
Shortness
Panic disorder epidemiology
2-3% of general population; 5-10% of primary care patients.Onset
Panic disorder epidemiology
2-3% of general population; 5-10% of primary care patients.Onset
Things to keep in mind
A panic attack ≠ panic disorder
Panic disorder
Things to keep in mind
A panic attack ≠ panic disorder
Panic disorder
With Agoraphobia
פחד או המנעות להיות במקומות או במצבים בהם יש קושי
With Agoraphobia
פחד או המנעות להיות במקומות או במצבים בהם יש קושי
טיפול:
שילוב של טיפול CBT ותרופות:
נוגדי דיכאון
נוגדי חרדה לשלב הראשון
סיבוכים :
דיכאון
טיפול:
שילוב של טיפול CBT ותרופות:
נוגדי דיכאון
נוגדי חרדה לשלב הראשון
סיבוכים :
דיכאון
Panic Disorder Comorbidity
50-60% have lifetime major depression
One third have current depression
20-25%
Panic Disorder Comorbidity
50-60% have lifetime major depression
One third have current depression
20-25%
Panic Disorder Etiology
Drug/Alcohol
Genetics
Social learning
Cognitive theories
Neurobiology/conditioned fear
Psychosocial stressors
Prior separation anxiety
Maale Carmel Mental
Panic Disorder Etiology
Drug/Alcohol
Genetics
Social learning
Cognitive theories
Neurobiology/conditioned fear
Psychosocial stressors
Prior separation anxiety
Maale Carmel Mental

Treatment
See 70% or better treatment response
Education, reassurance, elimination of caffeine, alcohol,
Treatment
See 70% or better treatment response
Education, reassurance, elimination of caffeine, alcohol,
Agoraphobia
Marked fear or anxiety for more than 6 months about two
Agoraphobia
Marked fear or anxiety for more than 6 months about two
Agoraphobia
The individual fears or avoids these situations because escape might be
Agoraphobia
The individual fears or avoids these situations because escape might be

Prevalence
2% of the population
Females to males:2:1
Mean onset is 17 years
30% of
Prevalence
2% of the population
Females to males:2:1
Mean onset is 17 years
30% of
Generalized Anxiety
פחד או חרדה מוגזמים, ללא כל אחיזה במציאות, מלווים בביטוים
Generalized Anxiety
פחד או חרדה מוגזמים, ללא כל אחיזה במציאות, מלווים בביטוים
Generalized Anxiety Disorder
Excessive worry more days than not for at least
Generalized Anxiety Disorder
Excessive worry more days than not for at least
GAD Comorbidity
90% have at least one other lifetime Axis I Disorder
66%
GAD Comorbidity
90% have at least one other lifetime Axis I Disorder
66%
Long-Term Treatment Of GAD
Need to treat long-term
Full relapse in approximately
Long-Term Treatment Of GAD
Need to treat long-term
Full relapse in approximately
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
AGORAPHOBIA
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
AGORAPHOBIA
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Pharmacotherapy for Anxiety Disorders
Antidepressants
Serotonin Selective Reuptake Inhibitors (SSRIs)
Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
Atypical
Pharmacotherapy for Anxiety Disorders
Antidepressants
Serotonin Selective Reuptake Inhibitors (SSRIs)
Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
Atypical
Benzodiazepines
Other Agents
Azaspirones
Beta blockers
Anticonvulsants
Other strategies
Maale Carmel Mental Health Center, Bruce Rappaport
Benzodiazepines
Other Agents
Azaspirones
Beta blockers
Anticonvulsants
Other strategies
Maale Carmel Mental Health Center, Bruce Rappaport
Discontinuation of Treatment
for Anxiety Disorders
Withdrawal/rebound more common with Bzd than
Discontinuation of Treatment
for Anxiety Disorders
Withdrawal/rebound more common with Bzd than
Strategies for Anxiolytic Discontinuation
Slow taper
Switch to longer-acting agent for taper
Cognitive-Behavioral therapy
Adjunctive
Antidepressant
Anticonvulsant
clonidine,
Strategies for Anxiolytic Discontinuation
Slow taper
Switch to longer-acting agent for taper
Cognitive-Behavioral therapy
Adjunctive
Antidepressant
Anticonvulsant
clonidine,
Strategies for Refractory Anxiety Disorder
Maximize dose
Combine antidepressant and benzodiazepine
Administer cognitive-behavioral therapy
Attend
Strategies for Refractory Anxiety Disorder
Maximize dose
Combine antidepressant and benzodiazepine
Administer cognitive-behavioral therapy
Attend
Strategies for Refractory Anxiety Disorders
Augmentation
Anticonvulsants
Gabapentin
Valproate
Topiramate
Beta blocker
Buspirone
Clonidine/Guanfacine
Pindolol -nonselective beta blocker
Dopaminergic
Strategies for Refractory Anxiety Disorders
Augmentation
Anticonvulsants
Gabapentin
Valproate
Topiramate
Beta blocker
Buspirone
Clonidine/Guanfacine
Pindolol -nonselective beta blocker
Dopaminergic
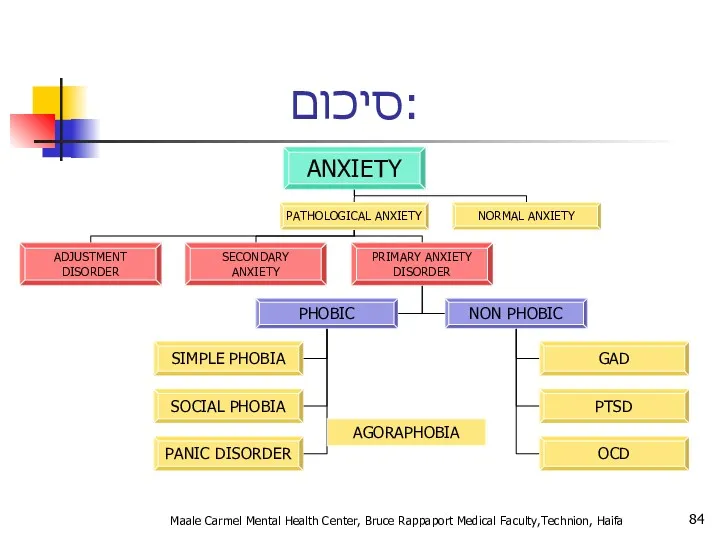
סיכום:
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
סיכום:
Maale Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Screening questions
How ever experienced a panic attack? (Panic)
Do you consider yourself
Screening questions
How ever experienced a panic attack? (Panic)
Do you consider yourself
Take home points
Anxiety, Obsessive-Compulsive and Related, and Trauma and Stressor-related disorders
Take home points
Anxiety, Obsessive-Compulsive and Related, and Trauma and Stressor-related disorders

Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Question
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Question

Trauma- and Stressor-Related Disorders
New chapter in DSM-5 brings together anxiety disorders
Trauma- and Stressor-Related Disorders
New chapter in DSM-5 brings together anxiety disorders
Disinhibited Social Engagement Disorder
“The essential feature of disorder is a pattern
Disinhibited Social Engagement Disorder
“The essential feature of disorder is a pattern
A. PTSD A Criterion
B. No mandatory (e.g., dissociative, etc.) symptoms from
A. PTSD A Criterion
B. No mandatory (e.g., dissociative, etc.) symptoms from
Adjustment Disorders are redefined as an array of stress-response syndromes
Adjustment Disorders are redefined as an array of stress-response syndromes
Chronic Adjustment Disorder
Omitted by mistake from DSM-5
Acute AD – less than
Chronic Adjustment Disorder
Omitted by mistake from DSM-5
Acute AD – less than
Other Specified Trauma/Stressor-Related Disorder (309.89)
AD with duration more than 6 months
Other Specified Trauma/Stressor-Related Disorder (309.89)
AD with duration more than 6 months
Reactive Attachment Disorder
Emotionally withdrawn behavior
Social/emotional disturbance
- reduced responsiveness, limited affect &/or
Reactive Attachment Disorder
Emotionally withdrawn behavior
Social/emotional disturbance
- reduced responsiveness, limited affect &/or
Persistent Complex Bereavement Disorder
Onset > 12 months after death of loved
Persistent Complex Bereavement Disorder
Onset > 12 months after death of loved
Persistent Complex Bereavement Disorder (PCBD)
Diagnostic Criteria-ICD
The person experienced the death of
Persistent Complex Bereavement Disorder (PCBD)
Diagnostic Criteria-ICD
The person experienced the death of
Persistent Complex Bereavement Disorder (PCBD)
Preoccupation with the circumstances of the death.
Persistent Complex Bereavement Disorder (PCBD)
Preoccupation with the circumstances of the death.
Reactive Distress to the Death
Marked difficulty accepting the death. In children,
Reactive Distress to the Death
Marked difficulty accepting the death. In children,
Social/Identity Disruption
A desire to die in order to be with the
Social/Identity Disruption
A desire to die in order to be with the
Specify if:
With Traumatic Bereavement: Following a death that occurred under traumatic
Specify if:
With Traumatic Bereavement: Following a death that occurred under traumatic
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Changes in PTSD Criteria
Four symptom clusters, rather than three
-Re-experiencing
-Avoidance
-Persistent negative alterations
Changes in PTSD Criteria
Four symptom clusters, rather than three
-Re-experiencing
-Avoidance
-Persistent negative alterations
Changes in PTSD Criteria
DSM-5 more clearly defines what constitutes a traumatic
Changes in PTSD Criteria
DSM-5 more clearly defines what constitutes a traumatic
Changes in PTSD Criteria
Recognition of PTSD in Young children
Developmentally sensitive:
Criteria have
Changes in PTSD Criteria
Recognition of PTSD in Young children
Developmentally sensitive:
Criteria have
DSM-5: PTSD Criterion A
A. The person was exposed to: death, threatened
DSM-5: PTSD Criterion A
A. The person was exposed to: death, threatened
Criterion A (continued):
3. Indirectly, by learning that a close relative or
Criterion A (continued):
3. Indirectly, by learning that a close relative or
CRITERION B - Intrusion (5 Sx – Need 1)
Recurrent, involuntary and
CRITERION B - Intrusion (5 Sx – Need 1)
Recurrent, involuntary and
C. Persistent effortful avoidance of distressing trauma-related stimuli after the event
C. Persistent effortful avoidance of distressing trauma-related stimuli after the event
CRITERION D – negative alterations in cognition & Mood (7 Sx
CRITERION D – negative alterations in cognition & Mood (7 Sx
CRITERION E – Trauma-related alterations in arousal and reactivity that began
CRITERION E – Trauma-related alterations in arousal and reactivity that began
PTSD Criteria for DSM-5
F. Persistence of symptoms (in Criteria B,
PTSD Criteria for DSM-5
F. Persistence of symptoms (in Criteria B,
Preschool Subtype: 6 Years or Younger
Relative to broader diagnosis for adults
Preschool Subtype: 6 Years or Younger Relative to broader diagnosis for adults
A. In children (younger than 6 years), exposure to actual or
A. In children (younger than 6 years), exposure to actual or
DSM-5: Preschool PTSD Criterion B
B. Presence of one or more intrusion
DSM-5: Preschool PTSD Criterion B
B. Presence of one or more intrusion
Preschool PTSD Criterion C
One or more symptoms from either Criterion C
Preschool PTSD Criterion C
One or more symptoms from either Criterion C
Preschool PTSD Criterion E
E. Alterations in arousal and reactivity associated with
Preschool PTSD Criterion E
E. Alterations in arousal and reactivity associated with
Preschool PTSD for DSM-5
F. Duration (of Criteria B, C, D and
Preschool PTSD for DSM-5
F. Duration (of Criteria B, C, D and
Summary: PTSD in DSM-5
Perhaps PTSD should be re-conceptualized as a spectrum
Summary: PTSD in DSM-5
Perhaps PTSD should be re-conceptualized as a spectrum
Dissociative Subtype of PTSD
New subtype for both age groupings of PTSD
Dissociative Subtype of PTSD
New subtype for both age groupings of PTSD
specifiers
Specify whether:
With dissociative symptoms: The individual’s symptoms meet the criteria for
specifiers
Specify whether:
With dissociative symptoms: The individual’s symptoms meet the criteria for
CAPS
Clinician Administered PTSD Scale
National Center for PTSD (www.ptsd.va.gov)
20 item structured clinical
CAPS
Clinician Administered PTSD Scale
National Center for PTSD (www.ptsd.va.gov)
20 item structured clinical
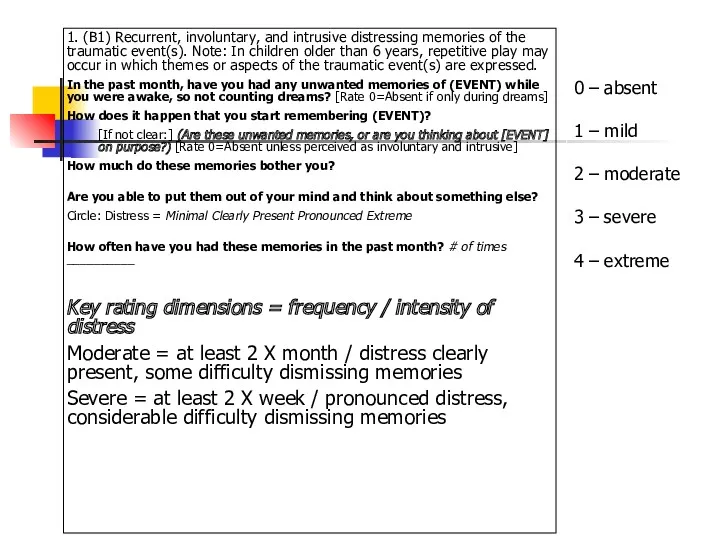
1. (B1) Recurrent, involuntary, and intrusive distressing memories of the traumatic
1. (B1) Recurrent, involuntary, and intrusive distressing memories of the traumatic
PCL
Posttraumatic Check List
National Center for PTSD (www.ptsd.va.gov)
Simple, easy to administer
Self-report or
PCL
Posttraumatic Check List
National Center for PTSD (www.ptsd.va.gov)
Simple, easy to administer
Self-report or
TRS
Trauma Recovery Scale
Gentry, 1996
Developed as an outcome instrument
Good psychometrics (Chronbach’s a
TRS
Trauma Recovery Scale
Gentry, 1996
Developed as an outcome instrument
Good psychometrics (Chronbach’s a
Early Sessions
Graphic Time Line of life including ALL significant traumatic experiences
Verbal
Early Sessions
Graphic Time Line of life including ALL significant traumatic experiences
Verbal
PTSD Epidemiology
7-9% of general population
60-80% of trauma victims
30% of combat veterans
50-80%
PTSD Epidemiology
7-9% of general population
60-80% of trauma victims
30% of combat veterans
50-80%
PTSD Epidemiology
בין אבחנות בודדות ב DSM שמדברת על אטיולוגיה
זוהי תגובה נפשית
PTSD Epidemiology
בין אבחנות בודדות ב DSM שמדברת על אטיולוגיה
זוהי תגובה נפשית
Comorbidities
Depression
Other anxiety disorders
Substance use disorders
Somatization
Dissociative disorders
Maale Carmel Mental Health Center,
Comorbidities
Depression
Other anxiety disorders
Substance use disorders
Somatization
Dissociative disorders
Maale Carmel Mental Health Center,
Acute PTSD - symptoms less than three months
Chronic PTSD - symptoms
Acute PTSD - symptoms less than three months
Chronic PTSD - symptoms
Can occur at any age, including childhood, and can affect anyone.
Individuals
Can occur at any age, including childhood, and can affect anyone.
Individuals

Onset
Symptoms usually begin within the first 3 months after the trauma,
Onset
Symptoms usually begin within the first 3 months after the trauma,
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
Tirat Carmel Mental Health Center, Bruce Rappaport Medical Faculty,Technion, Haifa
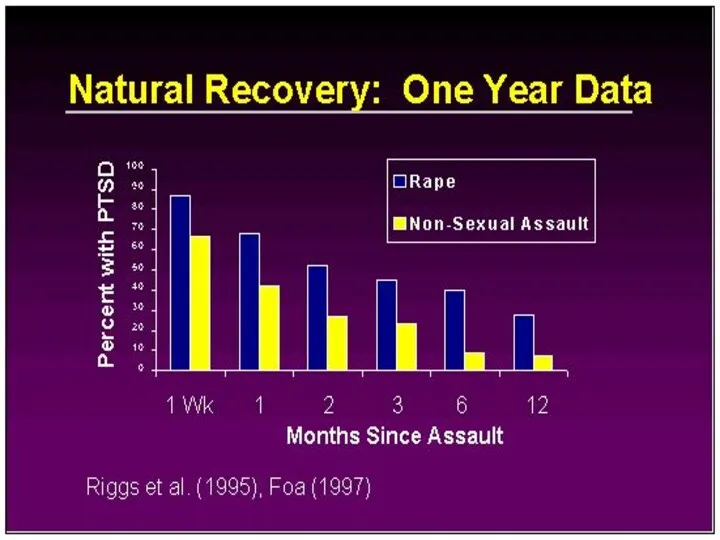
Course
The symptoms and the relative predominance of re-experiencing, avoidance, and increased
Course
The symptoms and the relative predominance of re-experiencing, avoidance, and increased

Course Continued
The severity, duration, and proximity of an individual’s exposure to
Course Continued
The severity, duration, and proximity of an individual’s exposure to

Rape (49%)
Severe beating or physical assault (31.9%)
Other sexual assault (23.7%)
Serious accident
Rape (49%)
Severe beating or physical assault (31.9%)
Other sexual assault (23.7%)
Serious accident
Differential Diagnosis
Differential diagnosis of the disorder or problem; that is, what
Differential Diagnosis
Differential diagnosis of the disorder or problem; that is, what

While the symptoms of posttraumatic stress disorder (PTSD) may seem similar
While the symptoms of posttraumatic stress disorder (PTSD) may seem similar
Differences between Acute Stress Disorder
In general, the symptoms of acute stress
Differences between Acute Stress Disorder
In general, the symptoms of acute stress
Differences between PTSD and Obsessive-Compulsive Disorder
Both have recurrent, intrusive thoughts as
Differences between PTSD and Obsessive-Compulsive Disorder
Both have recurrent, intrusive thoughts as
Differences Between PTSD and Adjustment Disorder
PTSD symptoms can also seem similar
Differences Between PTSD and Adjustment Disorder
PTSD symptoms can also seem similar
Differences Between PTSD and Depression
Depression after trauma and PTSD both may
Differences Between PTSD and Depression
Depression after trauma and PTSD both may
מי מיועד יותר?
עוצמה של סטרסור
פתאומיות (לא צפוי)
חוסר יכולת לשלוט על מתרחש
sexual
מי מיועד יותר?
עוצמה של סטרסור
פתאומיות (לא צפוי)
חוסר יכולת לשלוט על מתרחש
sexual
An adult's risk for psychological distress will increase as the number
An adult's risk for psychological distress will increase as the number
For women, the presence of a spouse, especially if he is
For women, the presence of a spouse, especially if he is
Why PTSD Victims Might Be Resistant to Getting Help
Sometimes hard because
Why PTSD Victims Might Be Resistant to Getting Help
Sometimes hard because
During a Traumatic Event
Norepinephrine- Mobilizing fear, the flight response, sympathetic activation,
During a Traumatic Event
Norepinephrine- Mobilizing fear, the flight response, sympathetic activation,
Causal Attributions
“PTSD is typified by both automatic, involuntary symptoms, (e.g. flashbacks,
Causal Attributions
“PTSD is typified by both automatic, involuntary symptoms, (e.g. flashbacks,
Treatment
Individual Therapy
Group Support (especially for Chronic PTSD)
Medication
Treatment
Individual Therapy
Group Support (especially for Chronic PTSD)
Medication
Treatment Continued
For PTSD in children, adolescents, and geriatrics the preferred treatment
Treatment Continued
For PTSD in children, adolescents, and geriatrics the preferred treatment
Treatment Continued
Exposure Therapy- Education about common reactions to trauma, breathing retraining,
Treatment Continued
Exposure Therapy- Education about common reactions to trauma, breathing retraining,
Treatment Continued
“Cognitive Restructuring involved teaching and reinforcing self-monitoring or thoughts and
Treatment Continued
“Cognitive Restructuring involved teaching and reinforcing self-monitoring or thoughts and
Medications
approved for the treatment of Anxiety Disorders including PTSD
SSRIs –
Medications
approved for the treatment of Anxiety Disorders including PTSD
SSRIs –
Tricyclic Antidepressants- Clomiprimine (Anafranil), Doxepin (Sinequan) Nortriptyline (Aventyl), Amitriptyline (Elavil), Maprotiline
Tricyclic Antidepressants- Clomiprimine (Anafranil), Doxepin (Sinequan) Nortriptyline (Aventyl), Amitriptyline (Elavil), Maprotiline
Treatment
With treatment, symptoms should improve after 3 months
In Chronic PTSD cases,
Treatment
With treatment, symptoms should improve after 3 months
In Chronic PTSD cases,
Noradrenergic Agents
Beta Blockers – Propranolol
Future Direction of Treatment
Beta Blockers – Propranolol
Future Direction of Treatment
PTSD - Treatment
שילוב של טיפול תרופתי בנוגדי דיכאון וחרדה
בפועל מגיעים
PTSD - Treatment
שילוב של טיפול תרופתי בנוגדי דיכאון וחרדה
בפועל מגיעים
Future Direction of Treatment Continued
“Early Diagnosis and intervention- either psychotherapeutic or
Future Direction of Treatment Continued
“Early Diagnosis and intervention- either psychotherapeutic or
PTSD Myths
PTSD is a complex disorder that often is misunderstood. Not
PTSD Myths
PTSD is a complex disorder that often is misunderstood. Not
PTSD Myths Continued
MYTH:
People should be able to move on with their
PTSD Myths Continued
MYTH:
People should be able to move on with their
PTSD Myths Continued
MYTH:
People suffer from PTSD right after they experience a
PTSD Myths Continued
MYTH:
People suffer from PTSD right after they experience a
What is Prolonged Exposure?
PE is a type of CBT, which is
What is Prolonged Exposure?
PE is a type of CBT, which is
education about common reactions to trauma
breathing retraining (or relaxation training)
breathing retraining (or relaxation training)
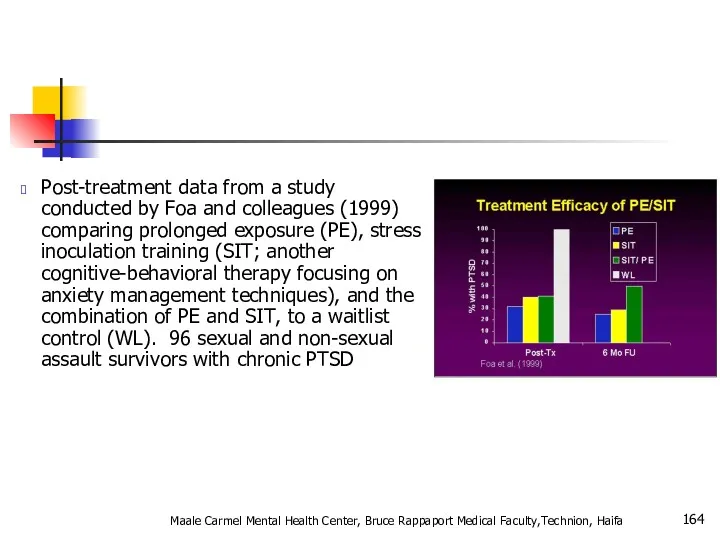
Post-treatment data from a study conducted by Foa and colleagues (1999)
Post-treatment data from a study conducted by Foa and colleagues (1999)
Combat Reaction
Combat stress reaction, better known as "Shell Shock" is
Combat Reaction
Combat stress reaction, better known as "Shell Shock" is
The Background of Combat Reaction
The transition from civilian life to
The Background of Combat Reaction
The transition from civilian life to
In wartime, a new and even more acute transition is added
In wartime, a new and even more acute transition is added

On the other hand the soldier feels solidarity with his unit,
On the other hand the soldier feels solidarity with his unit,

Risk Factors
Risk factors for Combat Reaction are all the factors
Risk Factors
Risk factors for Combat Reaction are all the factors
Enforced passivity. When the soldier is deprived of activity and is
Enforced passivity. When the soldier is deprived of activity and is
PIE principles
Proximity - treat the casualties close to the front and
PIE principles
Proximity - treat the casualties close to the front and
The US services now use the more recently developed BICEPS principles:
Brevity
The US services now use the more recently developed BICEPS principles:
Brevity
Treatment results
Data from the 1982 Lebanon war showed that with proximal
Treatment results
Data from the 1982 Lebanon war showed that with proximal
Controversy
Throughout wars but notably during the Vietnam War there has been
Controversy
Throughout wars but notably during the Vietnam War there has been
תסמונת שואה
דור ראשון
דור שני
Maale Carmel Mental Health Center, Bruce Rappaport Medical
תסמונת שואה
דור ראשון
דור שני
Maale Carmel Mental Health Center, Bruce Rappaport Medical
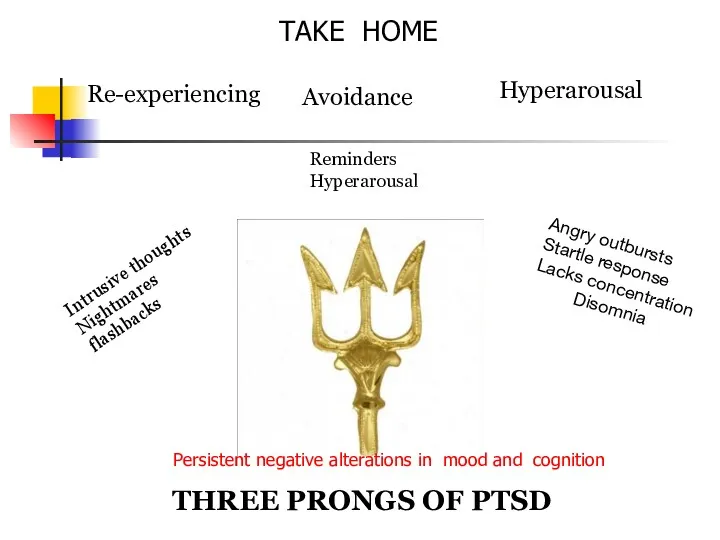
Re-experiencing
Intrusive thoughts
Nightmares
flashbacks
Avoidance
Hyperarousal
Reminders
Hyperarousal
Angry outbursts
Startle response
Lacks concentration
Disomnia
THREE PRONGS OF PTSD
TAKE HOME
Persistent negative
Re-experiencing
Intrusive thoughts
Nightmares
flashbacks
Avoidance
Hyperarousal
Reminders
Hyperarousal
Angry outbursts
Startle response
Lacks concentration
Disomnia
THREE PRONGS OF PTSD
TAKE HOME
Persistent negative
 Невербальные средства общения
Невербальные средства общения Манипуляции
Манипуляции Деловые и межкультурные коммуникации. Типы конфликтных личностей
Деловые и межкультурные коммуникации. Типы конфликтных личностей Вербальные и невербальные средства коммуникации
Вербальные и невербальные средства коммуникации Методы диагностики конфликтных ситуаций в ОО
Методы диагностики конфликтных ситуаций в ОО Профессиональный отбор
Профессиональный отбор Представление о внимании в современной когнитивной психологии
Представление о внимании в современной когнитивной психологии Профессиональное самоопределение личности
Профессиональное самоопределение личности Общая характеристика одаренности в психологии
Общая характеристика одаренности в психологии Невербальное общение. Язык жестов
Невербальное общение. Язык жестов Психологиялық тесттер
Психологиялық тесттер Комп'ютерна залежність - ознаки, стадії, причини виникнення та профілактика. Селфіманія - хвороба чи спосіб самовираження
Комп'ютерна залежність - ознаки, стадії, причини виникнення та профілактика. Селфіманія - хвороба чи спосіб самовираження Особенности развития психологической готовности подростка к разрешению конфликтов
Особенности развития психологической готовности подростка к разрешению конфликтов Особенности общения с пациентами с нарушениями слуха, зрения, речи, с асоциальным рискованным поведением
Особенности общения с пациентами с нарушениями слуха, зрения, речи, с асоциальным рискованным поведением Когнитивные стили и социально-психологические характеристики руководителей (часть 2)
Когнитивные стили и социально-психологические характеристики руководителей (часть 2) Психология ребёнка и взаимоотношений
Психология ребёнка и взаимоотношений Тұлға . Басқару жүйесіндегі жеке тұлға
Тұлға . Басқару жүйесіндегі жеке тұлға Професиограмма, психограмма
Професиограмма, психограмма Синектика. Метод поиска творческих решений
Синектика. Метод поиска творческих решений Характер и темперамент личности
Характер и темперамент личности Психология конфликта
Психология конфликта Структура психологической службы в учреждениях и органах исполняющих уголовные наказания и нормативно-правовые документы
Структура психологической службы в учреждениях и органах исполняющих уголовные наказания и нормативно-правовые документы Психокоррекционная работа детского практического психолога
Психокоррекционная работа детского практического психолога Управление человеческими ресурсами: инструкция по применению для специалистов муниципальных органов управления образованием
Управление человеческими ресурсами: инструкция по применению для специалистов муниципальных органов управления образованием Психологические особенности обучения взрослых
Психологические особенности обучения взрослых Общение и речь. Коммуникативные барьеры
Общение и речь. Коммуникативные барьеры Ораторская речь и её особенности
Ораторская речь и её особенности Готовность ребёнка к школьному обучению
Готовность ребёнка к школьному обучению