- Детская рефракция. Очки детям

Содержание
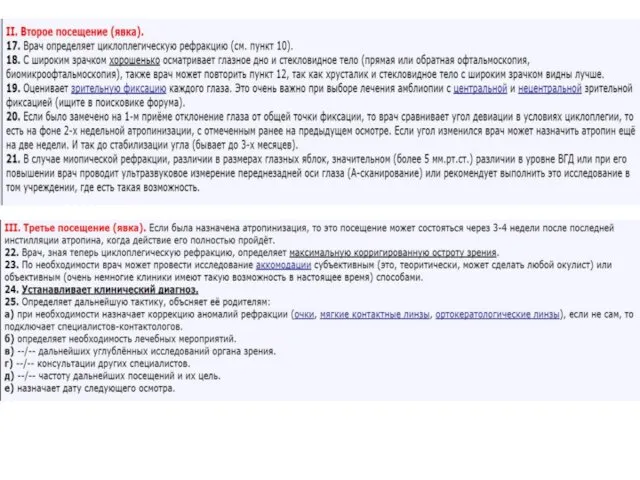
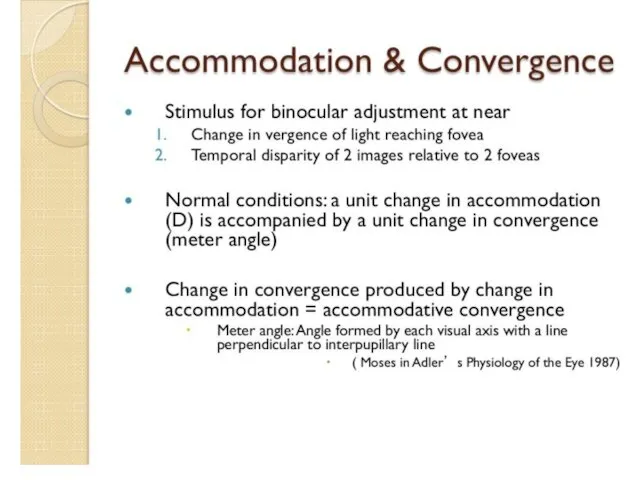
- 2. Первая встреча с дитём.
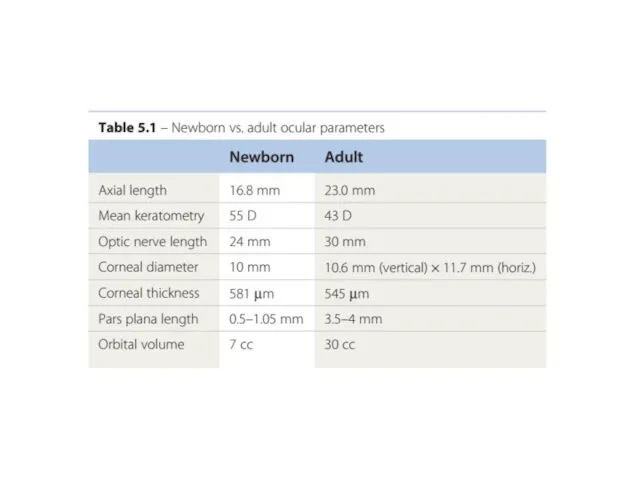
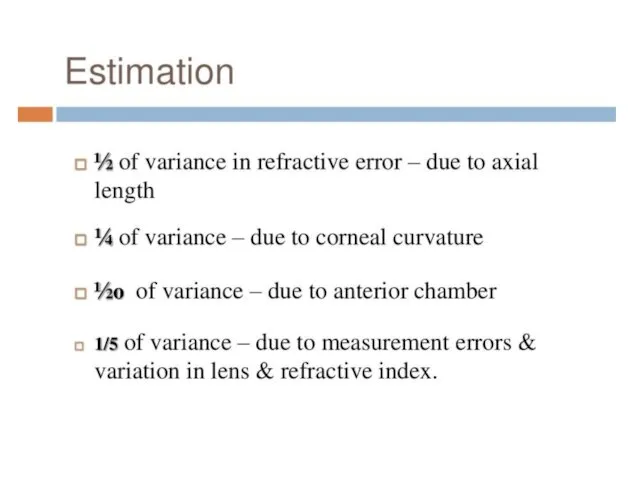
- 9. Поговорим об эмметропизации
- 14. The probability of reaching 2.00 D by 18 months of age as a function of the
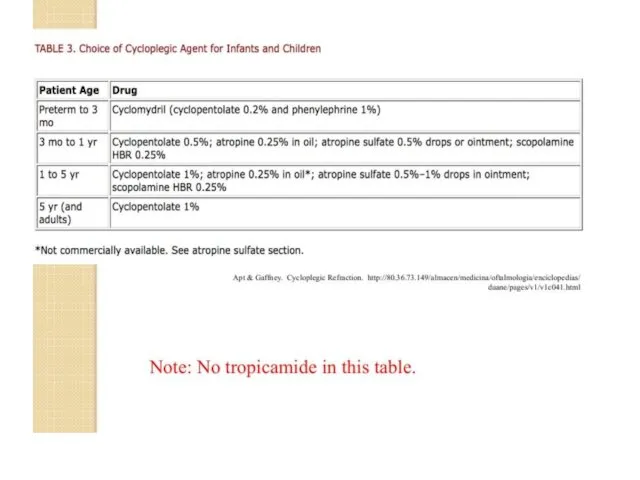
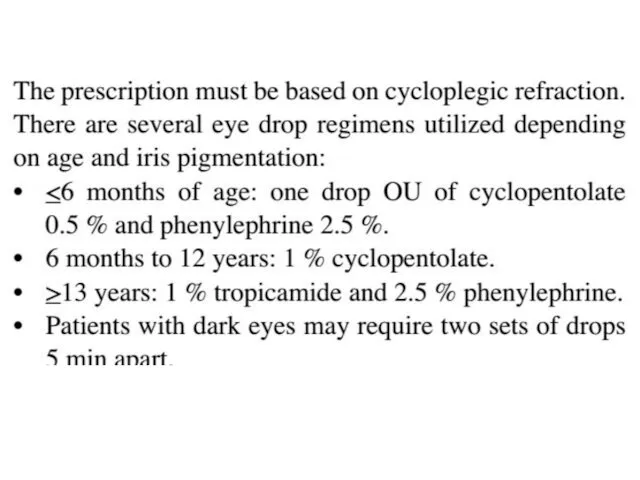
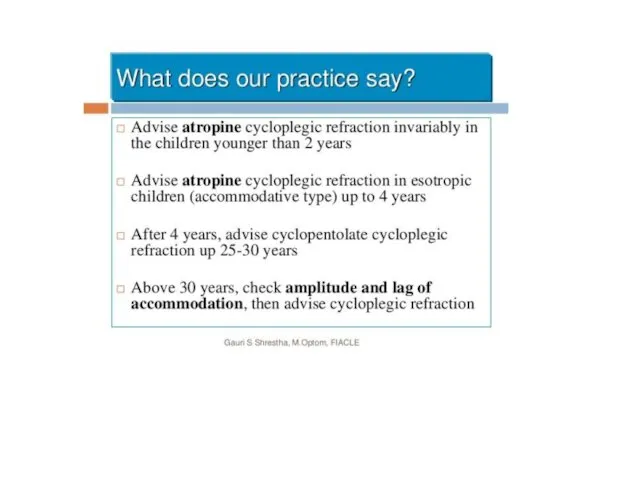
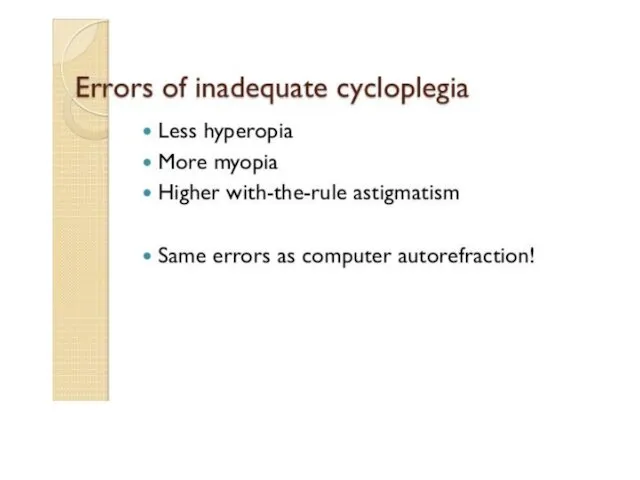
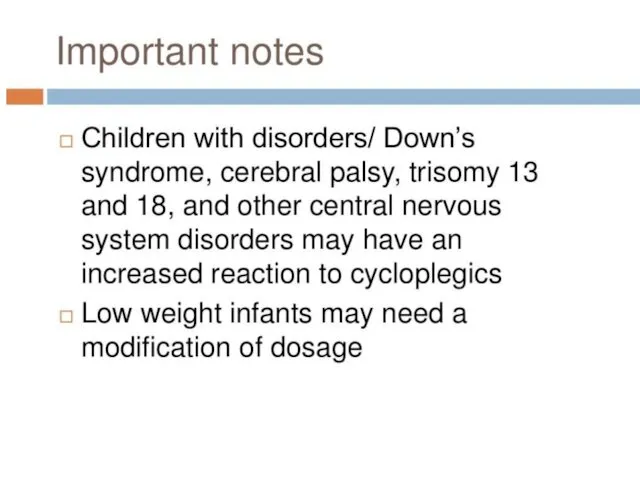
- 31. Поговорим о циклоплегии.
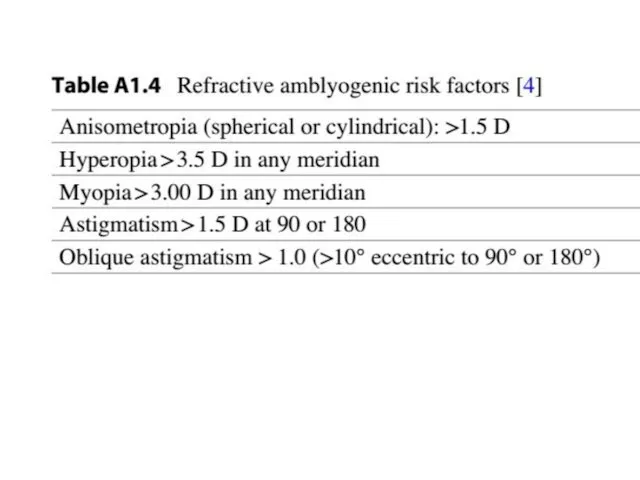
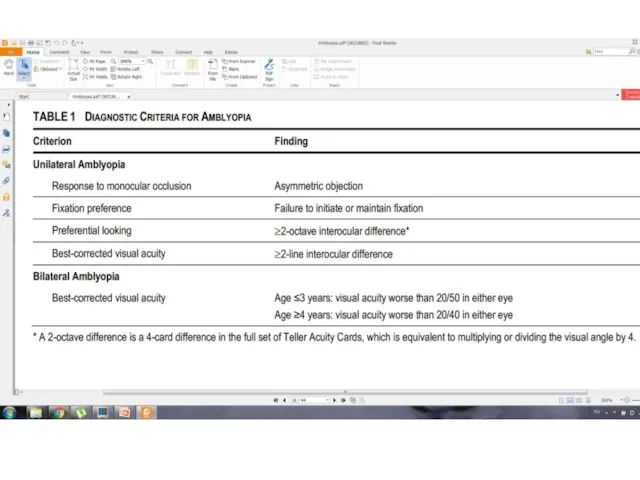
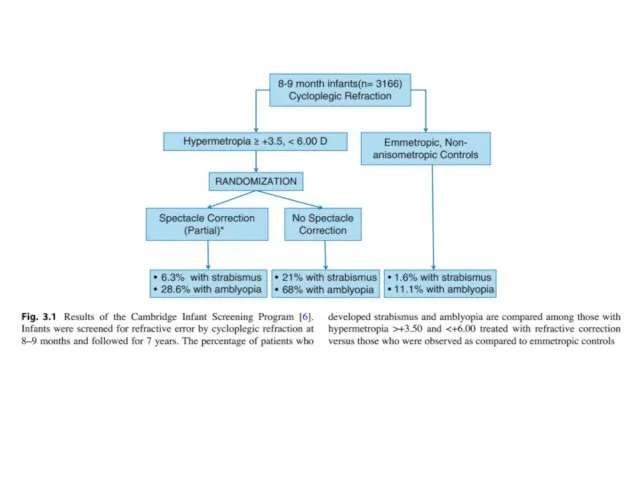
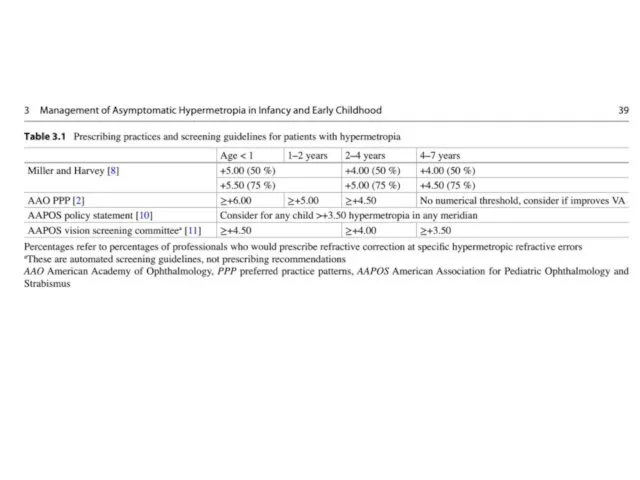
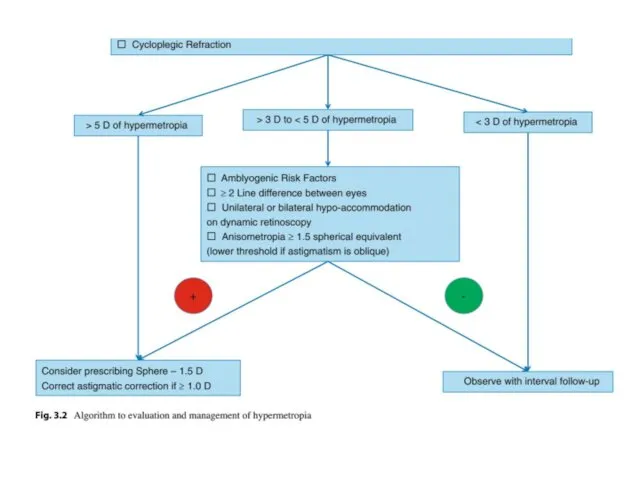
- 40. Поговорим об амблиогенных рефракциях
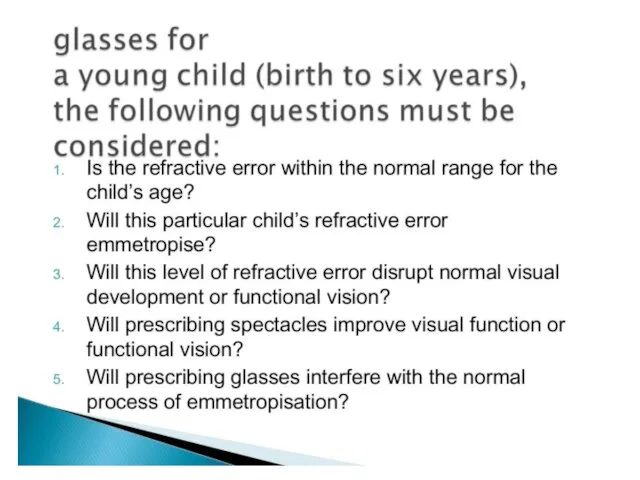
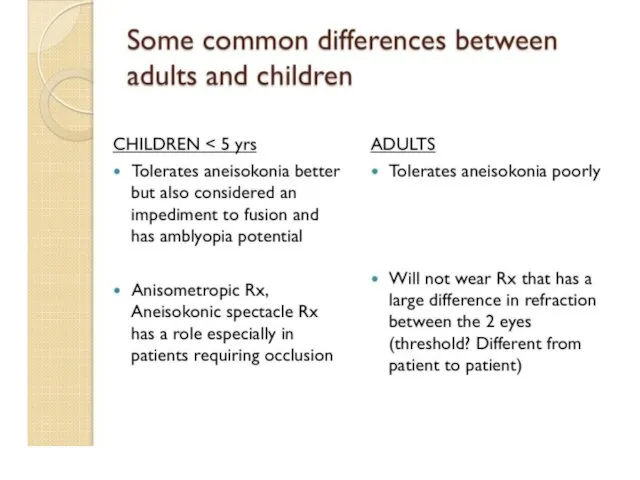
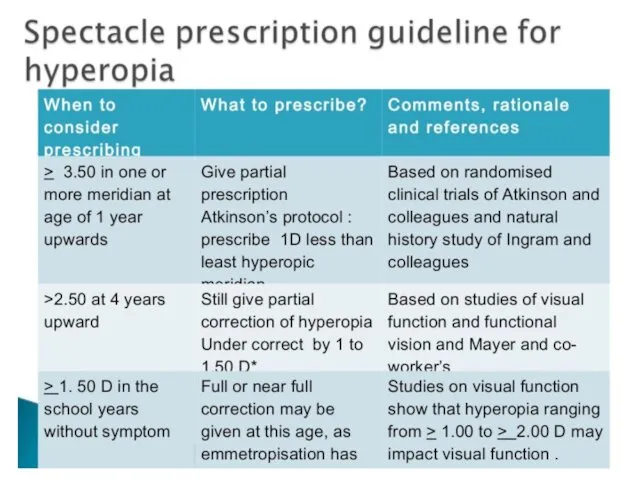
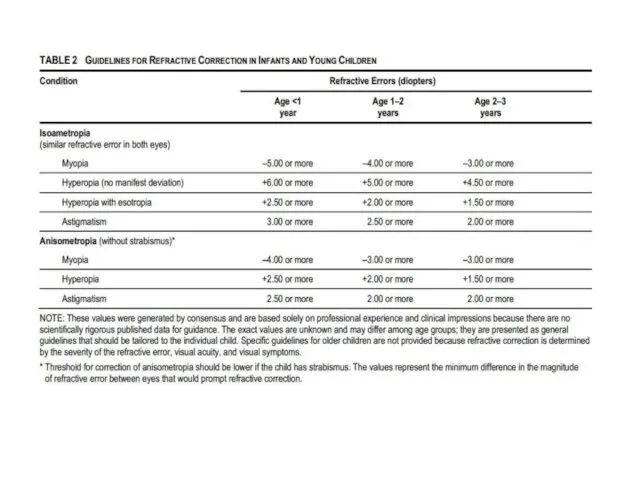
- 43. Когда назначать очки. Общие подходы.
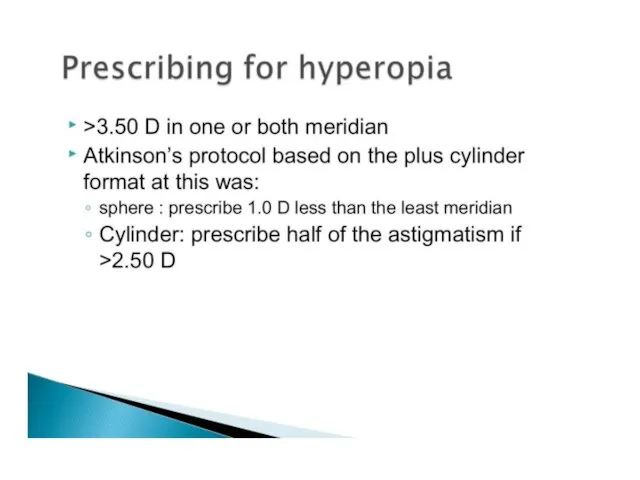
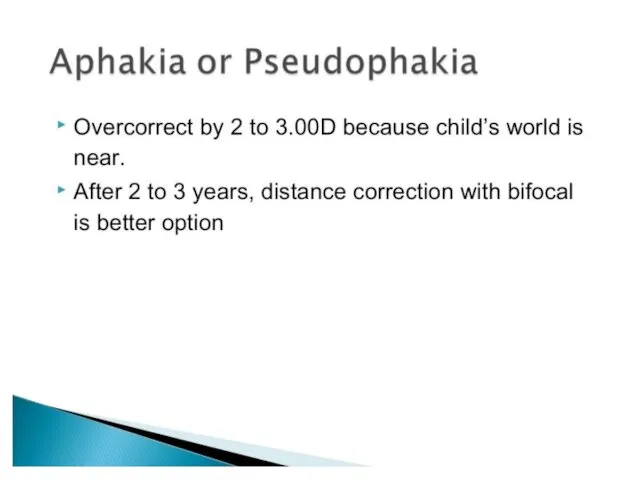
- 52. Очки при гиперметропии
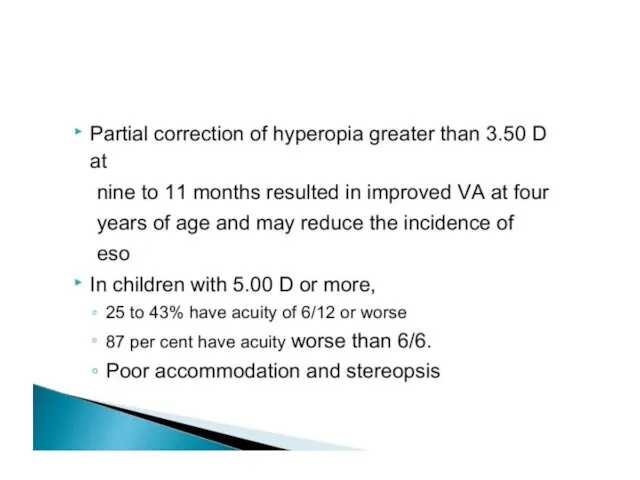
- 53. • Children have high accommodation amplitudes, and therefore, mild to moderate hypermetropia does not require correction
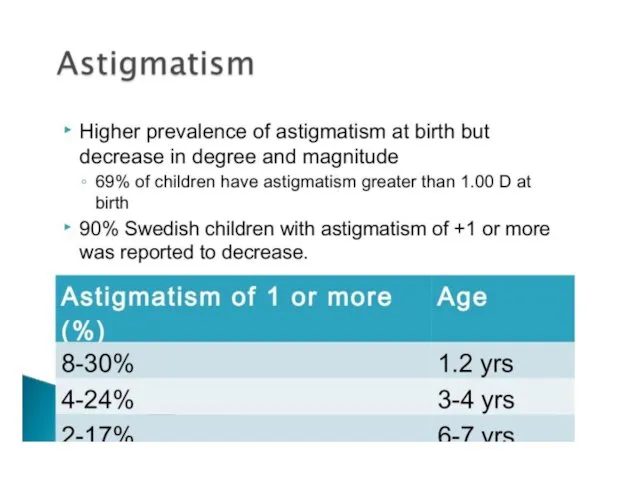
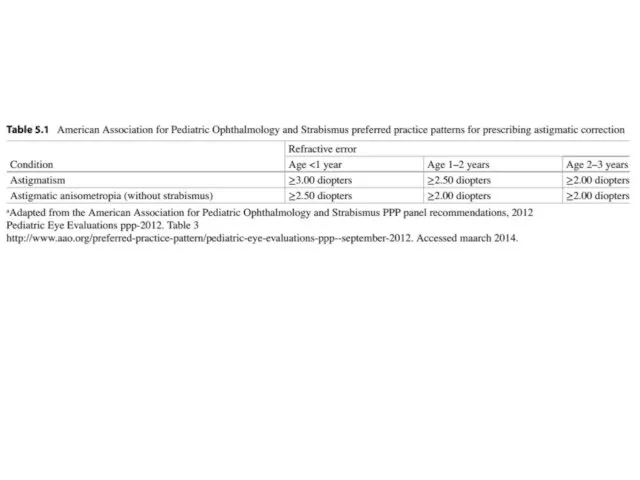
- 61. Очки при астигматизме
- 64. for oblique astigmatism—plus axis between 15° and 75° or 105° and 165°—it is probably preferable to
- 65. if astigmatic errors of magnitudes less than those listed above are present in conjunction with amblyogenic
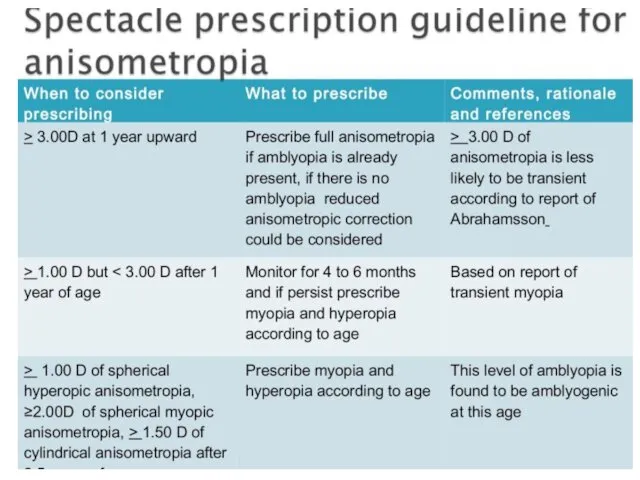
- 66. Очки при анизометропии
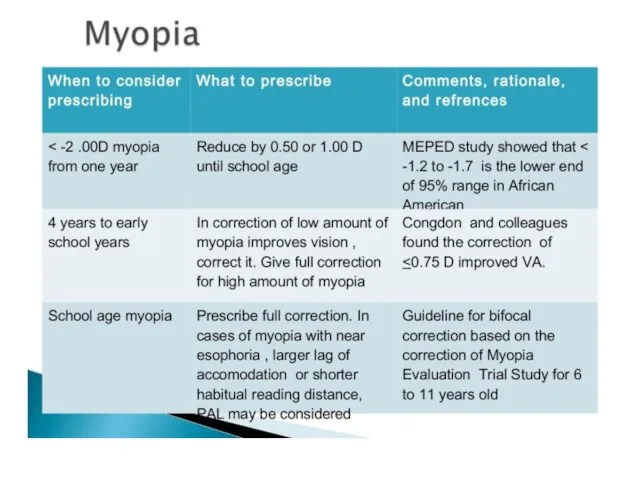
- 68. Очки при миопии
- 70. • Infants and very young children are most interested in objects at an arm’s length up
- 76. Итого.
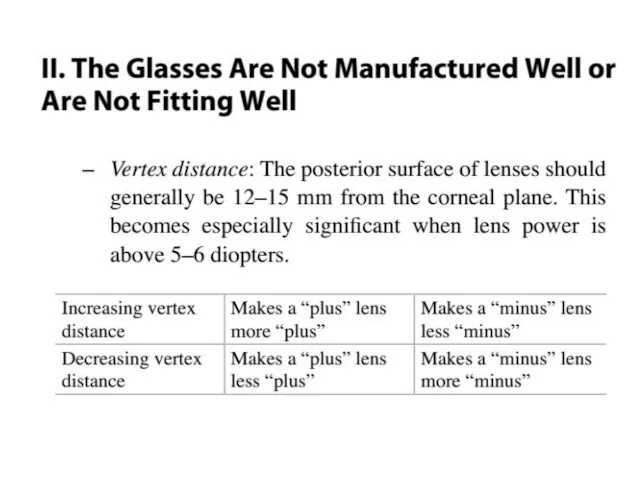
- 82. Что если ребёнок не переносит очки?
- 85. ?
- 86. ?
- 92. Скачать презентацию
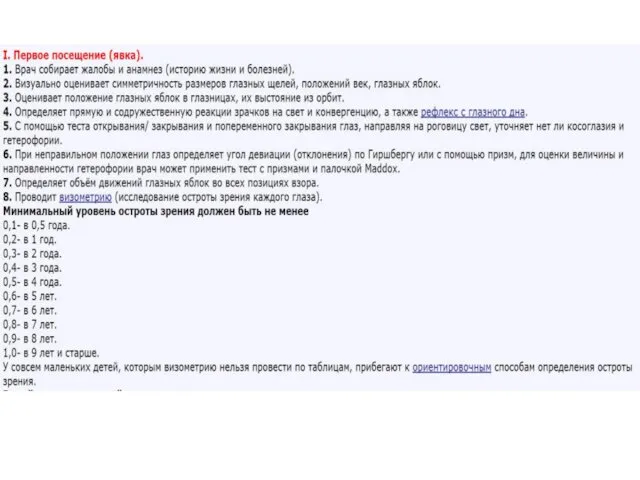
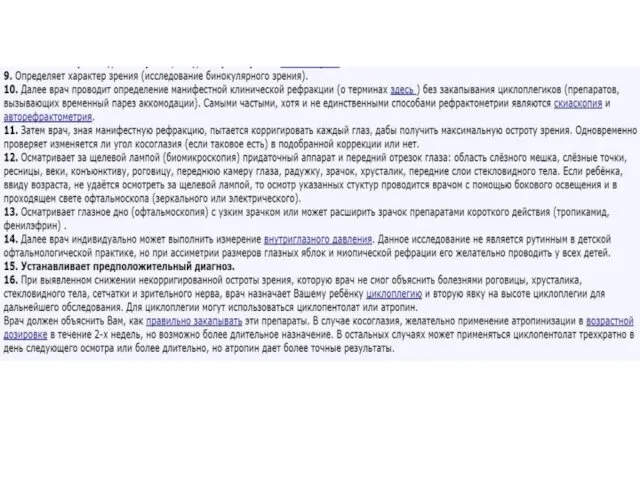
Первая встреча с дитём.
Первая встреча с дитём.
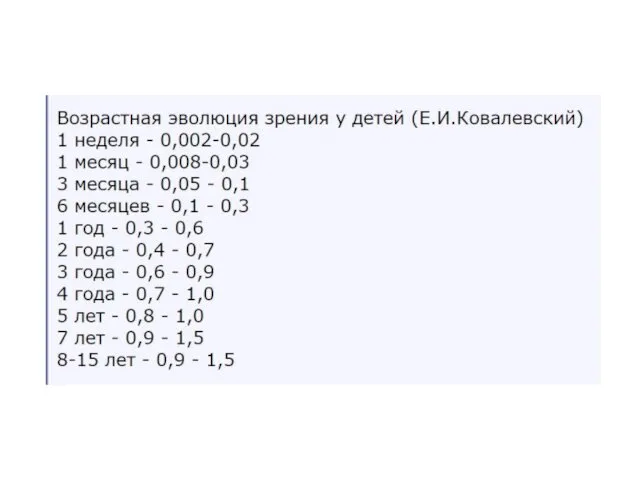
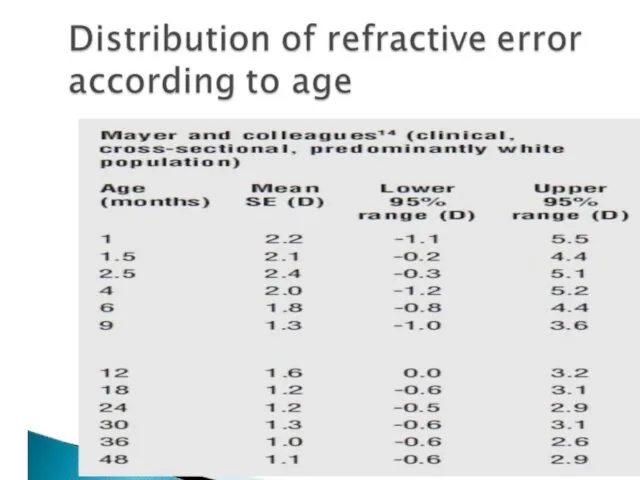
Поговорим об эмметропизации
Поговорим об эмметропизации
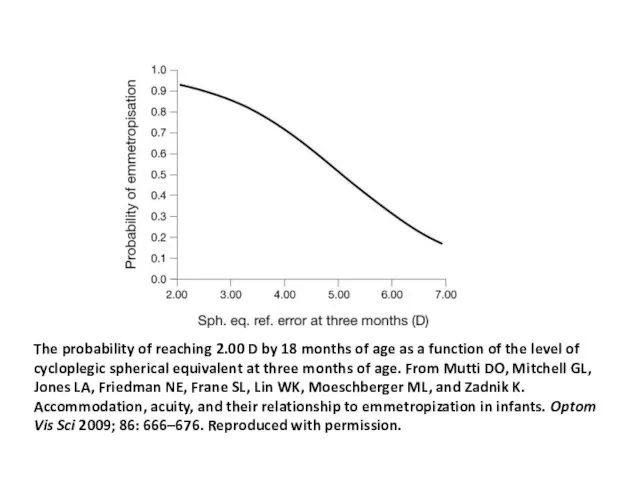
The probability of reaching 2.00 D by 18 months of age as a
The probability of reaching 2.00 D by 18 months of age as a

Поговорим о циклоплегии.
Поговорим о циклоплегии.
Поговорим об амблиогенных
рефракциях
Поговорим об амблиогенных
рефракциях
Когда назначать очки.
Общие подходы.
Когда назначать очки.
Общие подходы.
Очки при гиперметропии
Очки при гиперметропии
• Children have high accommodation amplitudes, and
therefore, mild to moderate hypermetropia
• Children have high accommodation amplitudes, and therefore, mild to moderate hypermetropia
Очки при астигматизме
Очки при астигматизме
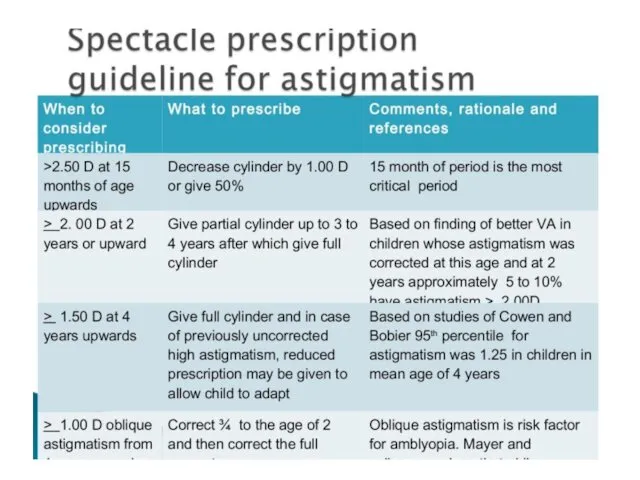
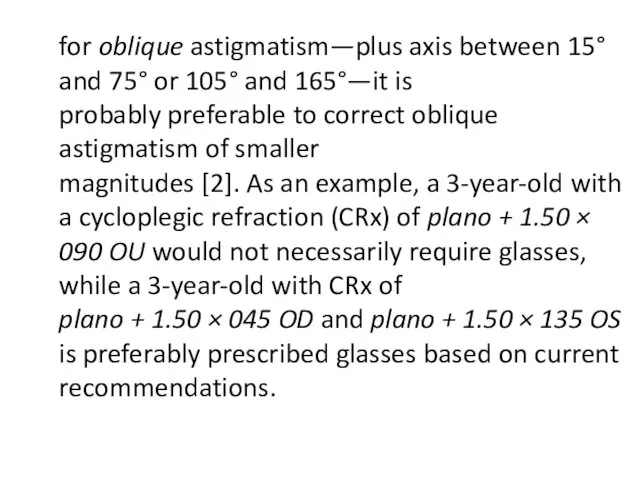
for oblique astigmatism—plus axis between 15° and 75° or 105° and
for oblique astigmatism—plus axis between 15° and 75° or 105° and
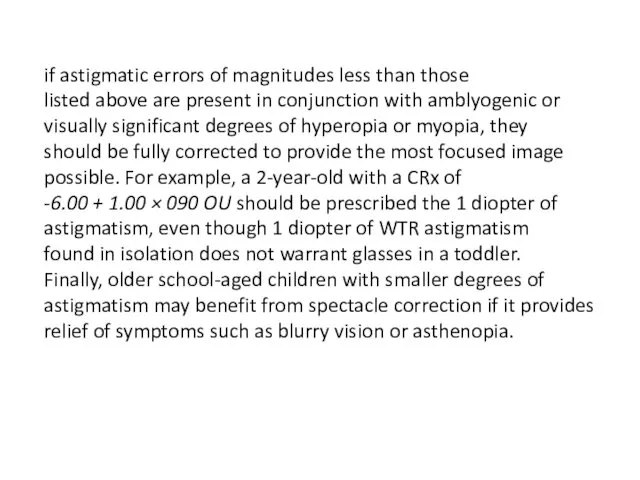
if astigmatic errors of magnitudes less than those
listed above are present
if astigmatic errors of magnitudes less than those listed above are present
Очки при анизометропии
Очки при анизометропии
Очки при миопии
Очки при миопии
• Infants and very young children are most interested in objects
• Infants and very young children are most interested in objects
Итого.
Итого.
Что если ребёнок не переносит очки?
Что если ребёнок не переносит очки?
?
?
?
?
 Международная торговля и услуги
Международная торговля и услуги Биосфера, как система, обеспечивающая существование человека
Биосфера, как система, обеспечивающая существование человека Универсальный дизайн в основной возрастной и профессиональной деятельности
Универсальный дизайн в основной возрастной и профессиональной деятельности Простейшие переборные задачи. Генерация подмножеств и перестановок
Простейшие переборные задачи. Генерация подмножеств и перестановок Синтетические противомикробные средства
Синтетические противомикробные средства Выжигание
Выжигание Презентация к уроку технологии Аппликация Осень в лесу
Презентация к уроку технологии Аппликация Осень в лесу Информационная безопасность и защита информации в медицинском учреждении
Информационная безопасность и защита информации в медицинском учреждении О профессиях для дошкольников
О профессиях для дошкольников класс. ЛР №5
класс. ЛР №5 Правовой режим информации, распространение которой ограничивается или запрещается
Правовой режим информации, распространение которой ограничивается или запрещается Черновая отделка. Группа компаний Удача
Черновая отделка. Группа компаний Удача Кавказ.
Кавказ. 7kl_ur1_piton
7kl_ur1_piton Мозаика народов. Россия – многонациональная страна
Мозаика народов. Россия – многонациональная страна Плата за негативное воздействие на окружающую среду
Плата за негативное воздействие на окружающую среду Портфолио учителя
Портфолио учителя Источники ошибок ГНСС-измерений. Режимы ГНСС-измерений
Источники ошибок ГНСС-измерений. Режимы ГНСС-измерений Расчёт теплового баланса реакционного узла. Лекция 4
Расчёт теплового баланса реакционного узла. Лекция 4 Оригами-танграм
Оригами-танграм Значение подвижных игр
Значение подвижных игр Умная телефония для оптимальной работы с клиентами
Умная телефония для оптимальной работы с клиентами Термообработка стали
Термообработка стали Der beruf – die berufe
Der beruf – die berufe Презентация к статье Формы взаимодействия педагога с детьми в условиях реализации образовательной программы Югорский трамплин
Презентация к статье Формы взаимодействия педагога с детьми в условиях реализации образовательной программы Югорский трамплин Концевые эффекты и их значение при измерениях фильтрационных характеристик
Концевые эффекты и их значение при измерениях фильтрационных характеристик Ранний возраст
Ранний возраст Атмосферное давление
Атмосферное давление