- Uterine sarcoma

Содержание
- 2. The uterine sarcomas form a group of malignant tumors that arises from the smooth muscle or
- 4. Risk factors Exposure to estrogen is a key risk factor Risk is increased with dose and
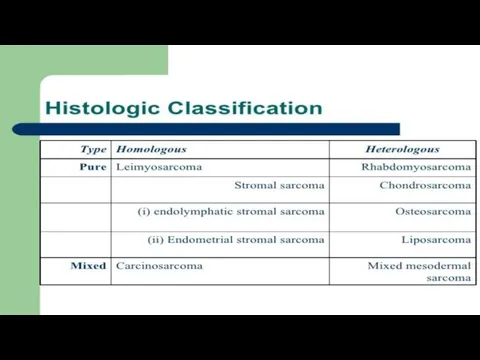
- 5. (THE HISTOLOGICAL SUBTYPE) Tumoral entities include: - Leiomyosarcomas (30%) - endometrial stromal sarcomas(15%) - carcinosarcomas (10%)
- 6. ESS /LMS/Adenosarcoma FIGO 2009 staging
- 7. CLASSIFICATION Leiomyosarcomas are now staged using the 2009 FIGO staging system[2] (previously they were staged like
- 10. Clinical symptoms Bleeding or discharge not related to menstruation (periods) Bleeding after menopause Irregular bleeding in
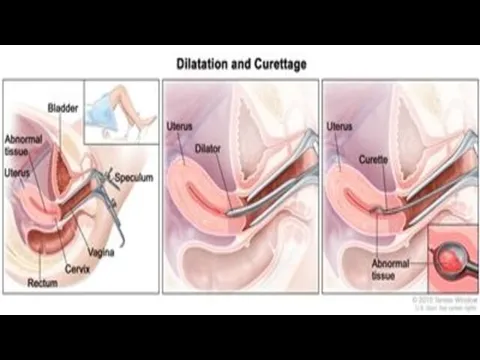
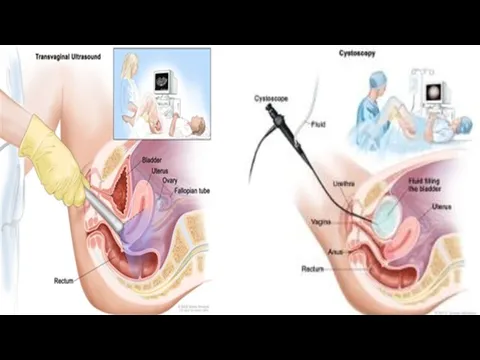
- 11. DIAGNOSTICS Anamnesis (complaints, an objective examination) General blood analysis, blood chemistry, CA 125 assay Gynecological examination
- 12. Pelvic exam PAP test
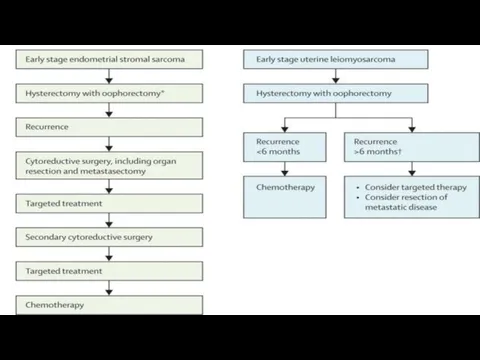
- 15. Treatment Treatment for this disease will vary, based on: • The size and location of the
- 16. Treatment for leiomyosarcoma Stage I - radical therapy, total abdominal hysterectomy with appendages Stage II, III
- 17. Treatment for endometrial stromal sarcoma Stage I - hysterectomy with appendages of the upper third of
- 18. Operations Leiomyosarcoma of reproductive age - hysterectomy without appendages pre and postmenopause - hysterectomy with appendages
- 19. Hormone terapy Appropriate in patients that desire fertility preservation - young parient - well differentiated cancer
- 23. REFERENCES * Zagouri F, Dimopoulos AM, Fotiou S, Kouloulias V, Papadimitriou CA (2009). "Treatment of early
- 25. Скачать презентацию
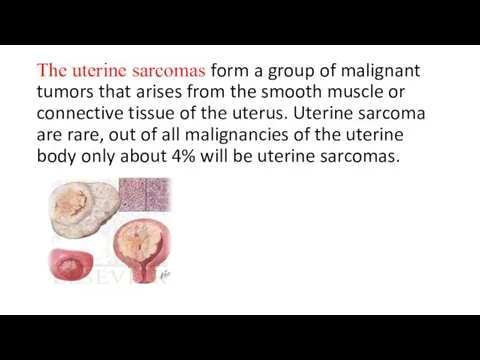
The uterine sarcomas form a group of malignant tumors that arises
The uterine sarcomas form a group of malignant tumors that arises
Risk factors
Exposure to estrogen is a key risk factor
Risk is
Risk factors
Exposure to estrogen is a key risk factor
Risk is
(THE HISTOLOGICAL SUBTYPE)
Tumoral entities include:
- Leiomyosarcomas (30%)
- endometrial stromal sarcomas(15%)
(THE HISTOLOGICAL SUBTYPE)
Tumoral entities include:
- Leiomyosarcomas (30%)
- endometrial stromal sarcomas(15%)
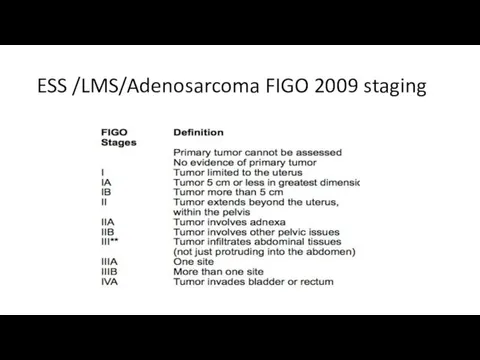
ESS /LMS/Adenosarcoma FIGO 2009 staging
ESS /LMS/Adenosarcoma FIGO 2009 staging
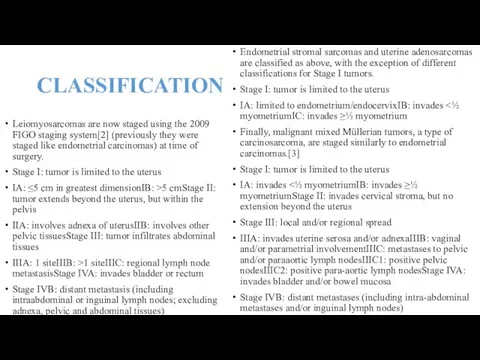
CLASSIFICATION
Leiomyosarcomas are now staged using the 2009 FIGO staging system[2] (previously
CLASSIFICATION
Leiomyosarcomas are now staged using the 2009 FIGO staging system[2] (previously
Clinical symptoms
Bleeding or discharge not related to menstruation (periods)
Bleeding after
Clinical symptoms
Bleeding or discharge not related to menstruation (periods)
Bleeding after
DIAGNOSTICS
Anamnesis (complaints, an objective examination)
General blood analysis, blood chemistry, CA 125
DIAGNOSTICS
Anamnesis (complaints, an objective examination)
General blood analysis, blood chemistry, CA 125
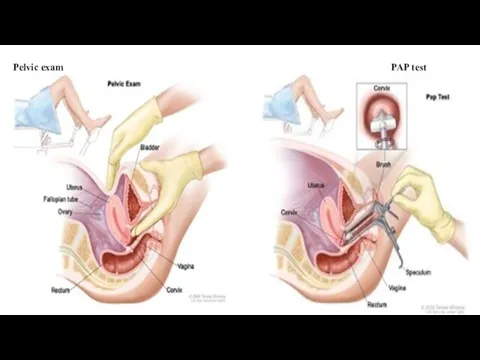
Pelvic exam PAP test
Pelvic exam PAP test
Treatment
Treatment for this disease will vary, based on:
• The size and location
Treatment
Treatment for this disease will vary, based on:
• The size and location
Treatment for leiomyosarcoma
Stage I - radical therapy, total abdominal hysterectomy
Treatment for leiomyosarcoma
Stage I - radical therapy, total abdominal hysterectomy
Treatment for endometrial stromal sarcoma
Stage I - hysterectomy with appendages
Treatment for endometrial stromal sarcoma
Stage I - hysterectomy with appendages
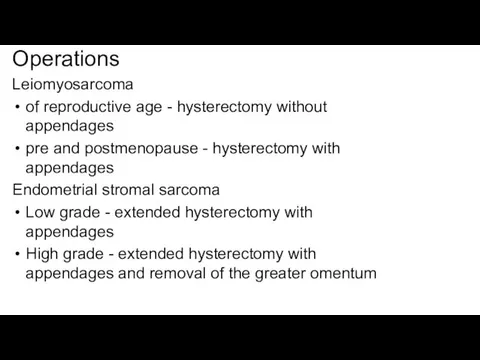
Operations
Leiomyosarcoma
of reproductive age - hysterectomy without appendages
pre and postmenopause -
Operations
Leiomyosarcoma
of reproductive age - hysterectomy without appendages
pre and postmenopause -
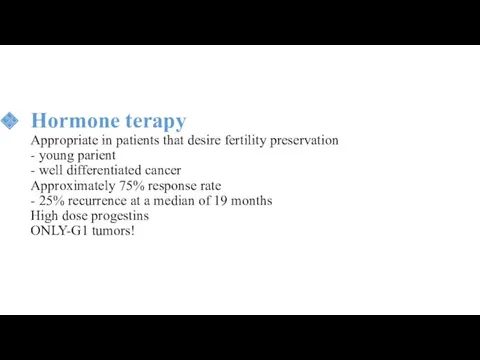
Hormone terapy
Appropriate in patients that desire fertility preservation
- young parient
- well
Hormone terapy Appropriate in patients that desire fertility preservation - young parient - well
REFERENCES
* Zagouri F, Dimopoulos AM, Fotiou S, Kouloulias V, Papadimitriou CA
REFERENCES * Zagouri F, Dimopoulos AM, Fotiou S, Kouloulias V, Papadimitriou CA
 Классный час Ежели Вы вежливы
Классный час Ежели Вы вежливы Система питания двигателя от впрыска топлива
Система питания двигателя от впрыска топлива физкультминутки
физкультминутки Социально-экономическое развитие Руси в XI веке
Социально-экономическое развитие Руси в XI веке Болезни желудка и двенадцатиперстной кишки
Болезни желудка и двенадцатиперстной кишки Презентация Наши земляки - Герои Советского Союза (О брасовцах)
Презентация Наши земляки - Герои Советского Союза (О брасовцах) Презентация к празднику День матери Диск
Презентация к празднику День матери Диск Презентация к занятию Давайте разберемся! (программа Планета здоровья)
Презентация к занятию Давайте разберемся! (программа Планета здоровья) Дошкольное образование в Великобритании.
Дошкольное образование в Великобритании. Налог на имущество физических лиц
Налог на имущество физических лиц CREDO бағдарламасы. Konverter
CREDO бағдарламасы. Konverter обобщение знаний по теме Главные особенности природы Земли презентация
обобщение знаний по теме Главные особенности природы Земли презентация Предпринимательство. Защита нематериальных благ. Причинение и возмещение вреда
Предпринимательство. Защита нематериальных благ. Причинение и возмещение вреда Урок Земля отцов - моя земля!
Урок Земля отцов - моя земля! Хранение лекарственных средств
Хранение лекарственных средств Родительское собрание Подростковый алкоголизм
Родительское собрание Подростковый алкоголизм Текст и предложение
Текст и предложение Диалог между верами в целях религиозного плюрализма
Диалог между верами в целях религиозного плюрализма Презентация для работы гражданско-патриотического клуба Моя Россия
Презентация для работы гражданско-патриотического клуба Моя Россия ОСОБЕННОСТИ РАЗВИТИЯ И ВОСПИТАНИЯ ДЕТЕЙ ОТ 3 ДО 4 ЛЕТ
ОСОБЕННОСТИ РАЗВИТИЯ И ВОСПИТАНИЯ ДЕТЕЙ ОТ 3 ДО 4 ЛЕТ Дидактические системы и модели обучения, факторы и цели
Дидактические системы и модели обучения, факторы и цели Рождество
Рождество Организация медицинской помощи сельскому населению
Организация медицинской помощи сельскому населению Урок химии для 8 класса на тему Ковалентная связь.ФГОС.
Урок химии для 8 класса на тему Ковалентная связь.ФГОС. России милый уголок (презентация)
России милый уголок (презентация) Компьютерная графика
Компьютерная графика Ортопедиялық стоматологияда қолданылатын анестезия препараттары. Олардың сипаттамасы
Ортопедиялық стоматологияда қолданылатын анестезия препараттары. Олардың сипаттамасы Негізгі макроэкономикалық көрсеткіштер (мұнайға баррельіне $90 бағасы кезінде)
Негізгі макроэкономикалық көрсеткіштер (мұнайға баррельіне $90 бағасы кезінде)