- Жүректің туа пайда болған ақауының алдын алуда поливитаминдердің тиімділігін бағалау

Содержание
- 2. Өзектілігі: Жүректің туа пайда болған ақауы – жүректің анатомиялық құрылымының өзгеруі. Барлық туа пайда болған аномалиялардың
- 3. Мақсаты: Жүректің туа пайда болған ақауын төмендетуде поливитамин мен моновитаминнің эффективтілігін салыстыру
- 4. Сұрақ: Қауіп тобындағы жүкті әйелдерге дуовитті қабылдау фолий қышқылына қарағанда ұрықтың туа пайда болған жүрек ақауын
- 5. Patient – жүректің даму қаупі бар жүкті әйелдер Interventoin – дуовит Compare – фолий қышқылы Outcome
- 6. Зерттеу дизайны:
- 7. Генеральная совокупность – себебі қауіп тобындағы жүкті әйелдер алынды. Таңдау: қарапайым кездейсоқ таңдау Зерттеуге ұрықтың ТПЖА
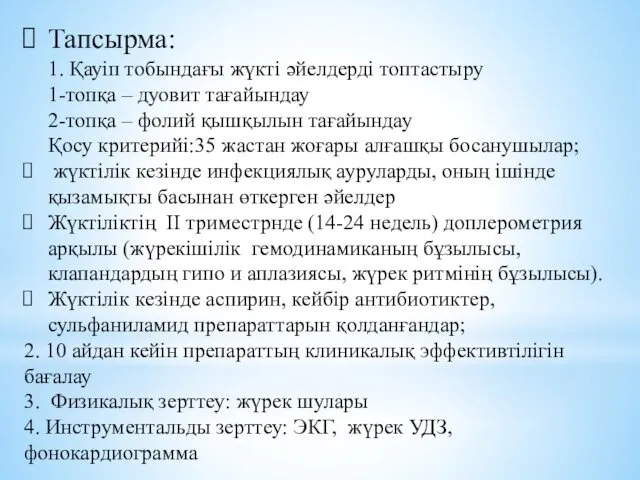
- 8. Тапсырма: 1. Қауіп тобындағы жүкті әйелдерді топтастыру 1-топқа – дуовит тағайындау 2-топқа – фолий қышқылын тағайындау
- 9. Этикалық аспектілер Этикалық Комитетпен бекітілді Сыйластық: науқастарға препараттарды тағайындамас бұрын ақпараттандырылды Шынайылық: эксперимент өту барысын түсіндірілді.
- 10. Prophylactic milrinone for the prevention of low cardiac output syndrome and mortality in children undergoing surgery
- 11. Abstract Background Children with congenital heart disease often undergo heart surgery at a young age. They
- 12. Main results Three of the five included studies compared milrinone versus levosimendan, one study compared milrinone
- 13. Authors' conclusions There is insufficient evidence of the effectiveness of prophylactic milrinone in preventing death or
- 14. : Мақсаты Жүректің туа пайда болған ақауына байланысты операцияны бастан өткізген балаларға өлімнің және LCOS жүрек
- 15. Сұрақ: 12 жасқа дейінгі балаларға ТПЖА байланысты жасалған операциядан кейінгі кезеңде милринонды тағайындау жүрек айдауының төмендеу
- 16. Patient – жүректің туа пайда болған ақауына байланысты паллиативті немесе коррекциялық операцияны басынан өткізген 12жасқа дейінгі
- 17. Зерттеу дизайны:
- 19. Скачать презентацию
Өзектілігі:
Жүректің туа пайда болған ақауы – жүректің анатомиялық құрылымының өзгеруі. Барлық
Өзектілігі:
Жүректің туа пайда болған ақауы – жүректің анатомиялық құрылымының өзгеруі. Барлық
Мақсаты:
Жүректің туа пайда болған ақауын төмендетуде поливитамин мен моновитаминнің эффективтілігін
Мақсаты:
Жүректің туа пайда болған ақауын төмендетуде поливитамин мен моновитаминнің эффективтілігін
Сұрақ:
Қауіп тобындағы жүкті әйелдерге дуовитті қабылдау фолий қышқылына қарағанда ұрықтың
Сұрақ:
Қауіп тобындағы жүкті әйелдерге дуовитті қабылдау фолий қышқылына қарағанда ұрықтың
Patient – жүректің даму қаупі бар жүкті әйелдер
Interventoin – дуовит
Compare
Patient – жүректің даму қаупі бар жүкті әйелдер
Interventoin – дуовит
Compare
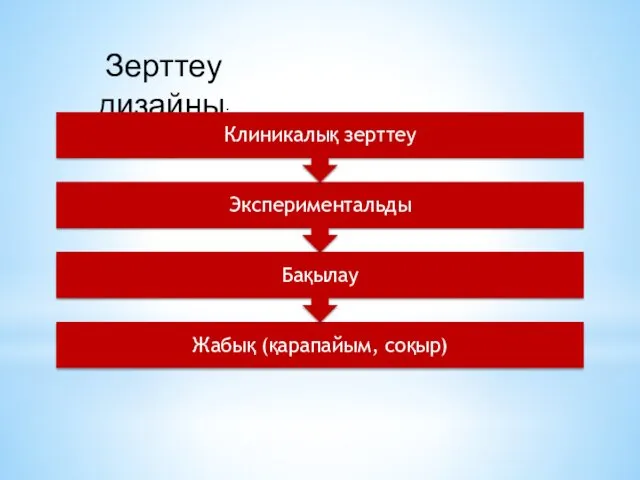
Зерттеу дизайны:
Зерттеу дизайны:
Генеральная совокупность – себебі қауіп тобындағы жүкті әйелдер алынды.
Таңдау: қарапайым
Генеральная совокупность – себебі қауіп тобындағы жүкті әйелдер алынды.
Таңдау: қарапайым
Тапсырма:
1. Қауіп тобындағы жүкті әйелдерді топтастыру
1-топқа – дуовит тағайындау
2-топқа – фолий
Тапсырма: 1. Қауіп тобындағы жүкті әйелдерді топтастыру 1-топқа – дуовит тағайындау 2-топқа – фолий
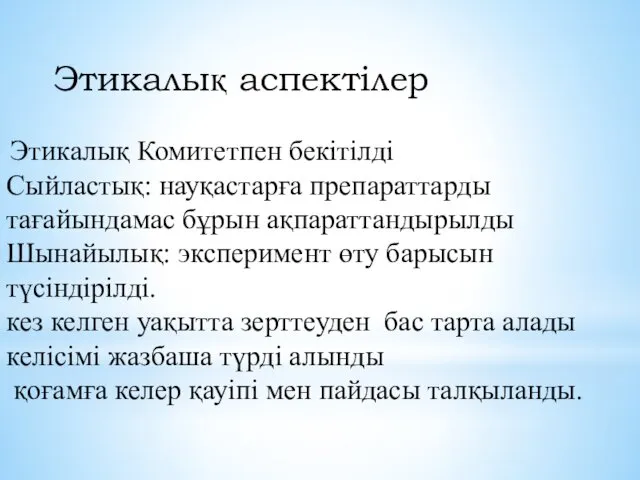
Этикалық аспектілер
Этикалық Комитетпен бекітілді
Сыйластық: науқастарға препараттарды тағайындамас бұрын ақпараттандырылды
Шынайылық: эксперимент
Этикалық аспектілер
Этикалық Комитетпен бекітілді
Сыйластық: науқастарға препараттарды тағайындамас бұрын ақпараттандырылды
Шынайылық: эксперимент
Prophylactic milrinone for the prevention of low cardiac output syndrome
and
Prophylactic milrinone for the prevention of low cardiac output syndrome
and
Abstract
Background
Children with congenital heart disease often undergo heart surgery at a
Abstract
Background
Children with congenital heart disease often undergo heart surgery at a
Main results
Three of the five included studies compared milrinone versus levosimendan,
Main results
Three of the five included studies compared milrinone versus levosimendan,
Authors' conclusions
There is insufficient evidence of the effectiveness of prophylactic milrinone
Authors' conclusions
There is insufficient evidence of the effectiveness of prophylactic milrinone
:
Мақсаты
Жүректің туа пайда болған ақауына байланысты операцияны бастан өткізген балаларға өлімнің
:
Мақсаты
Жүректің туа пайда болған ақауына байланысты операцияны бастан өткізген балаларға өлімнің
Сұрақ:
12 жасқа дейінгі балаларға ТПЖА байланысты жасалған операциядан кейінгі кезеңде милринонды
Сұрақ:
12 жасқа дейінгі балаларға ТПЖА байланысты жасалған операциядан кейінгі кезеңде милринонды
Patient – жүректің туа пайда болған ақауына байланысты паллиативті немесе коррекциялық
Patient – жүректің туа пайда болған ақауына байланысты паллиативті немесе коррекциялық
Зерттеу дизайны:
Зерттеу дизайны:
 в Лекция 6
в Лекция 6 презентация Формирование связной речи у детей с заиканием
презентация Формирование связной речи у детей с заиканием Український модерн
Український модерн Реконструкция и реновация особняков России
Реконструкция и реновация особняков России Конструктивные особенности самоходных опрыскивателей серии SP
Конструктивные особенности самоходных опрыскивателей серии SP Воздух и его состав
Воздух и его состав Принципы построения параллельных вычислительных систем
Принципы построения параллельных вычислительных систем Сочинение-описание по картине Т. Н. Яблонской Утро
Сочинение-описание по картине Т. Н. Яблонской Утро Технология разработки СБИС типа СнК на отечественной платформе по заданным алгоритмам
Технология разработки СБИС типа СнК на отечественной платформе по заданным алгоритмам Конспект урока по математике Решение примеров на нахождение неизвестного слагаемого
Конспект урока по математике Решение примеров на нахождение неизвестного слагаемого Организация торговли на борту ВС. Обучение бортпроводников
Организация торговли на борту ВС. Обучение бортпроводников Организация работы банковской системы в области противодействия легализации (отмыванию) доходов, полученных преступным путем
Организация работы банковской системы в области противодействия легализации (отмыванию) доходов, полученных преступным путем Характеристика карьерных дорог
Характеристика карьерных дорог Европейская и русская культурологическая мысль XIX века
Европейская и русская культурологическая мысль XIX века Развитие кооперации в Липецкой области
Развитие кооперации в Липецкой области РМО учителей географии
РМО учителей географии Компания Петро-Композит. Проект Зеленый город
Компания Петро-Композит. Проект Зеленый город Каждой пичужке кормушка. Краевая Акция Экологический марафон
Каждой пичужке кормушка. Краевая Акция Экологический марафон Веселые старты, посвященные Дню Защитника Отечества. Выше голову будущий солдат
Веселые старты, посвященные Дню Защитника Отечества. Выше голову будущий солдат Скелетная травма
Скелетная травма Проект моя Родина
Проект моя Родина Прекращение трудового договора по инициативе работодателя
Прекращение трудового договора по инициативе работодателя Сортировка в массивах. Методы сортировки
Сортировка в массивах. Методы сортировки Сказка как средство развития эмоциональной сферы у дошкольников
Сказка как средство развития эмоциональной сферы у дошкольников Классный час 2014 год - год культуры России Диск
Классный час 2014 год - год культуры России Диск Аркадий и Борис Стругацкие
Аркадий и Борис Стругацкие She/from. He/from
She/from. He/from Презентация к родительскому собранию на тему: Фейерверки и пиротехника. Друзья или враги?
Презентация к родительскому собранию на тему: Фейерверки и пиротехника. Друзья или враги?