- The Structure and Funding of the U.S. Health Care System

Содержание
- 2. Goals of this module After this module, participants should be able to: Describe the structure of
- 3. Is this pertinent to ME? Survival in “real world” practice “You eat what you kill…..” Physicians
- 4. Is this pertinent to ME? The Ongoing/Impending Problems “Access”/”Rights”/”Justice”/”Fairness” All have very different meanings to different
- 5. Is this pertinent to ME? If you care about nothing else….. Federal & State governments face
- 6. A snapshot of some of the problems… Quality of care U.S. residents receive about 50% of
- 7. A snapshot of some of the problems… National expenditures 16% of GNP is health care1 25%
- 8. Leading Causes of Premature Deaths McGinnis JM et al. The case for more active policy attention
- 9. Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States,
- 10. Leading causes of death How do physicians address these causes? Do you expand office hours to
- 11. “The health care System”? – What it DOES… One Perspective Provides services: Somatic – medical, dental
- 12. The health care System – 5 Main Components Education and Research: professional schools Suppliers : drugs,
- 13. The health care System – Provider Groups Preventive Care: Primary Care Providers (PCPs), state/city health departments
- 14. The health care System – Provider Groups Acute Care – Hospitals, “Urgent Care” Auxiliary Services –
- 15. Public Health health care System Environmental Health Biostatistics Nutrition Physical Fitness Pharmacology “Basic Sciences” Inpatient Care
- 16. Health - Conceptual Framework U.S. Department of Health and Human Services. Healthy People 2010. 2nd ed.
- 17. “Medicaid HMO” “Individual coverage” “Uninsured” “Medicare” A lot of money is exchanging hands. Who is accountable
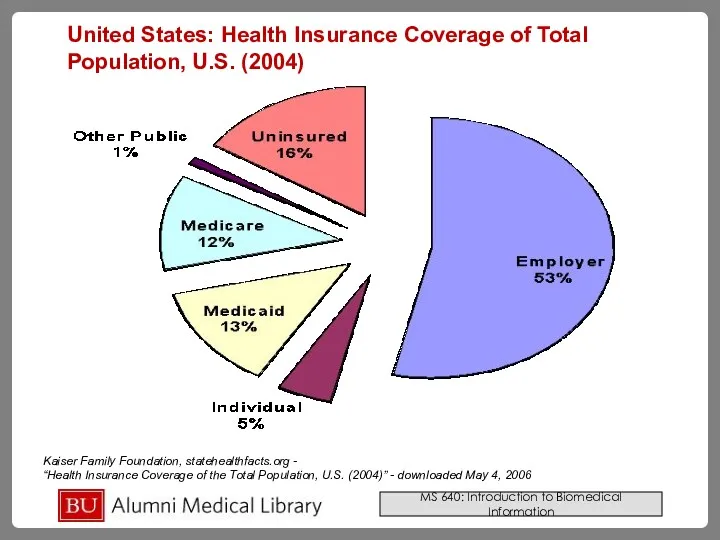
- 18. Kaiser Family Foundation, statehealthfacts.org - “Health Insurance Coverage of the Total Population, U.S. (2004)” - downloaded
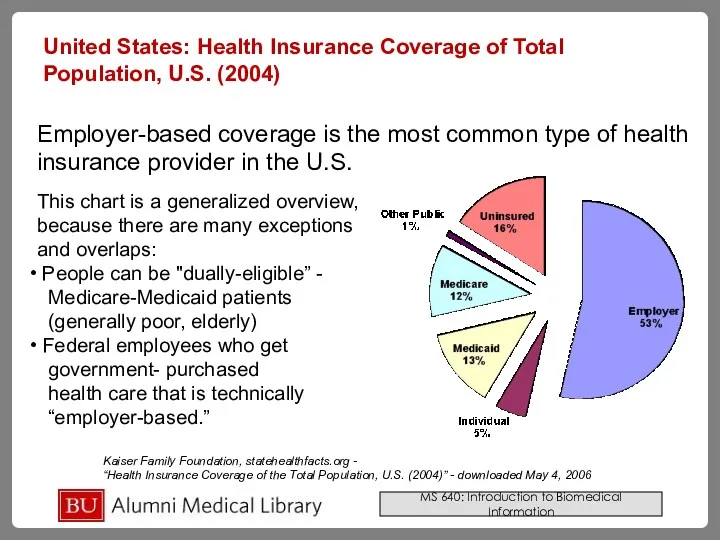
- 19. Kaiser Family Foundation, statehealthfacts.org - “Health Insurance Coverage of the Total Population, U.S. (2004)” - downloaded
- 20. Employer-Based and Individual 53% - Employer-based, 5% individual-purchased Dependants/spouses Government employees included Most will have DIFFERENT
- 21. Employer-Based and Individual Tax policy favors employee-based benefit Companies that spend money in employee health benefits
- 22. Medicare – “Elderly” 42 Million recipients – $325 Billion in 2003 Federally-funded > 65 years old
- 23. Medicare – “Elderly” Parts A, B, C, D A: Hospital and Skilled nursing care B: Outpatient,
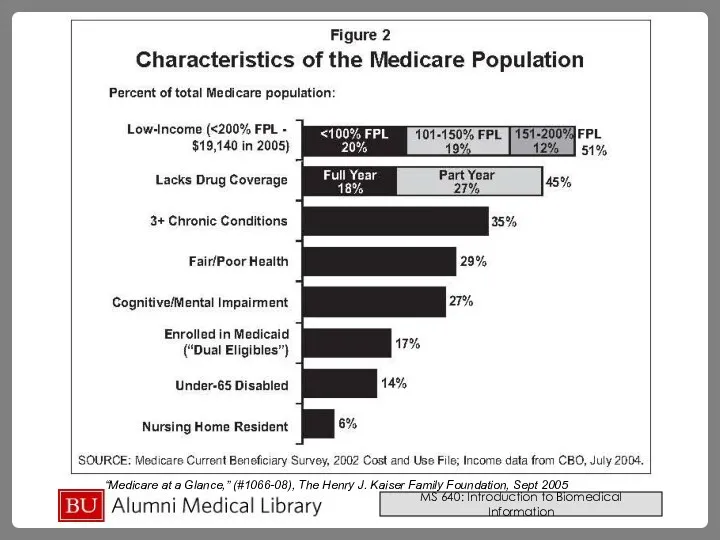
- 24. “Medicare at a Glance,” (#1066-08), The Henry J. Kaiser Family Foundation, Sept 2005
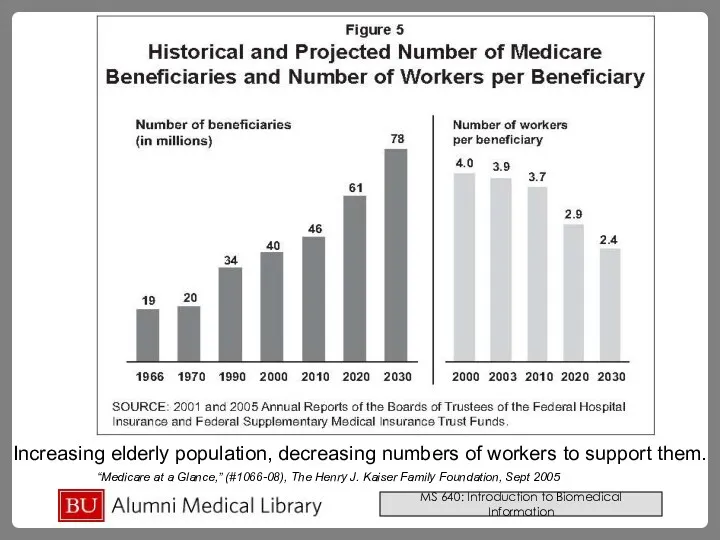
- 25. “Medicare at a Glance,” (#1066-08), The Henry J. Kaiser Family Foundation, Sept 2005 Increasing elderly population,
- 26. Medicaid – “Poor” 52 million recipients - $266 Billion in 2003 Federal-State Partnership Eligibility – varies
- 27. Medicaid – “Poor” May contract as “Medicaid HMO” with non-government entity Future – more cost limiting.
- 28. “The Medicaid Program at a Glance,” (#7235), The Henry J. Kaiser Family Foundation, Jan 2005
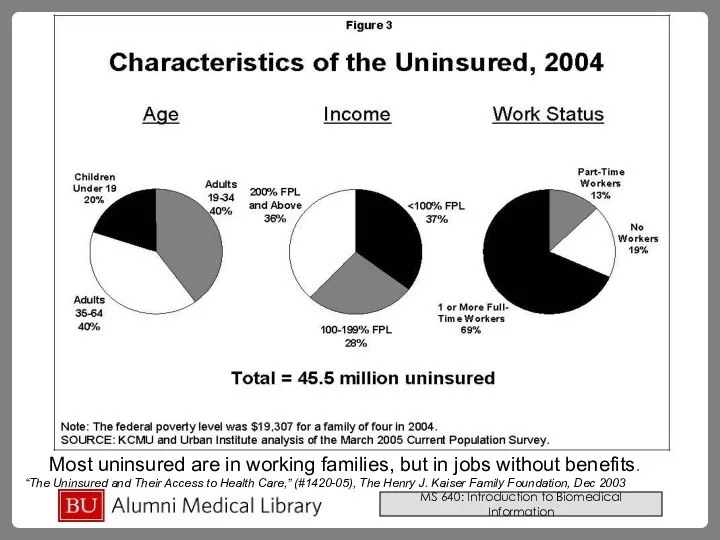
- 29. The Uninsured Over 45 million in 2004 Coverage = services. No coverage = no services. “But
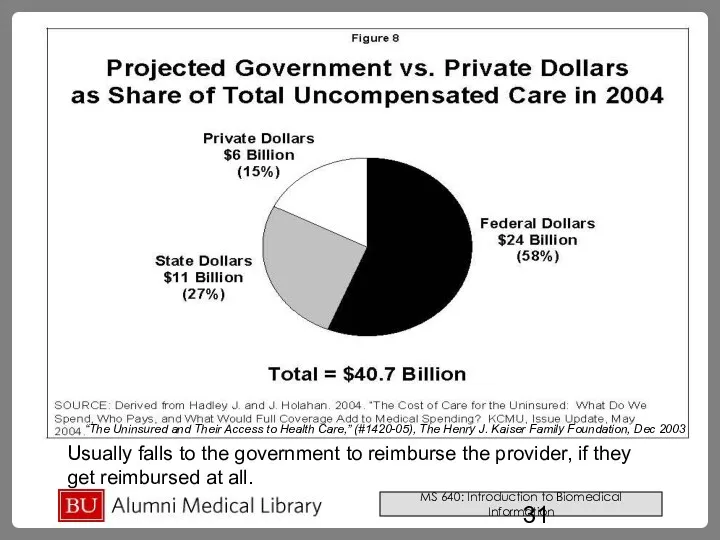
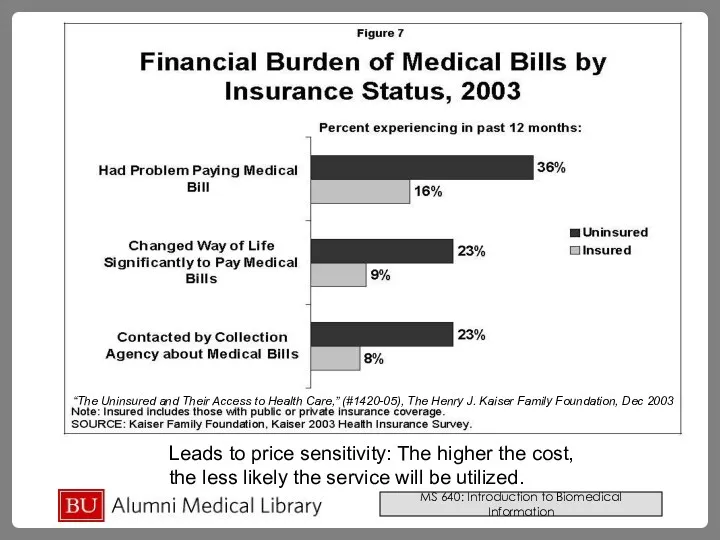
- 30. Most uninsured are in working families, but in jobs without benefits. “The Uninsured and Their Access
- 31. “The Uninsured and Their Access to Health Care,” (#1420-05), The Henry J. Kaiser Family Foundation, Dec
- 32. Leads to price sensitivity: The higher the cost, the less likely the service will be utilized.
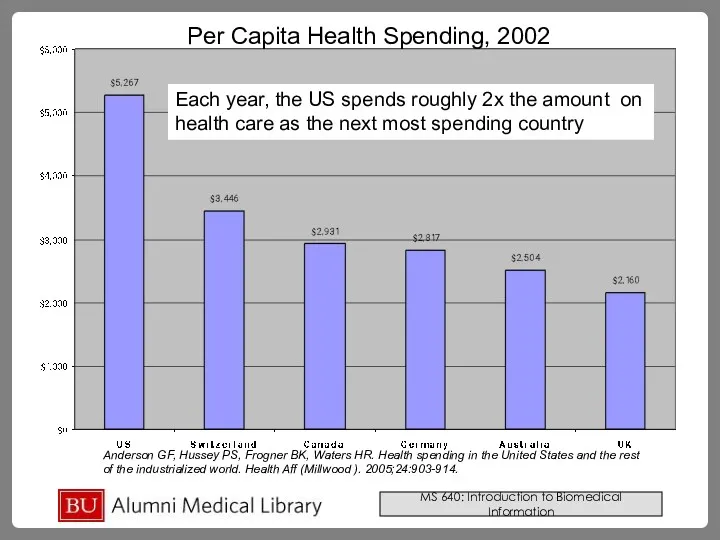
- 33. Anderson GF, Hussey PS, Frogner BK, Waters HR. Health spending in the United States and the
- 34. Summary Health, itself, is not simply a function of health care, but rather a complex interplay
- 35. Massachusetts Health Care Reform Plan Passed April 12, 2006 Aims to provide universal health care coverage
- 36. Looking up Information on the health care system Different types of Information: Background Gray literature Statistics
- 37. Background Resources that offer descriptive and consumer level information on various health care issues and topics
- 38. Books Good for explanations that integrate interdisciplinary factors of the health care system (cultural, medical, historical)
- 39. Gray Literature A lot of material concerning health care issues can be found outside of traditional
- 40. Finding Gray Literature Policy Institutes/Think Tanks: National Health Policy Forum Commonwealth Foundation Kaiser Family Foundation Institute
- 41. Looking up Statistics – US Government AHRQ: Agency for health care research and quality Includes MEPS
- 42. Looking up Statistics – Other sources Dartmouth Atlas of Health Care Massachusetts Health and Human Services
- 43. Research and Journal Articles Databases Medline: PubMed In PubMed can search Health Services Queries (see next
- 44. PubMed Health Services Queries A search interface to find PubMed citations relating to health care quality
- 45. Healthy People 2010 Pre-formulated PubMed searches based on objectives of a preventative health initiative Some searches
- 46. International Health Care Global Health Facts From the Kaiser Family Foundation Includes data and facts regarding
- 48. Скачать презентацию
Goals of this module
After this module, participants should be able to:
Goals of this module
After this module, participants should be able to:
Is this pertinent to ME?
Survival in “real world” practice
“You eat what
Is this pertinent to ME?
Survival in “real world” practice
“You eat what
Is this pertinent to ME?
The Ongoing/Impending Problems
“Access”/”Rights”/”Justice”/”Fairness”
All have very different meanings
Is this pertinent to ME?
The Ongoing/Impending Problems
“Access”/”Rights”/”Justice”/”Fairness”
All have very different meanings
Is this pertinent to ME?
If you care about nothing else…..
Federal &
Is this pertinent to ME?
If you care about nothing else…..
Federal &
A snapshot of some of the problems…
Quality of care
U.S. residents receive
A snapshot of some of the problems…
Quality of care
U.S. residents receive
A snapshot of some of the problems…
National expenditures
16% of GNP is
A snapshot of some of the problems…
National expenditures
16% of GNP is
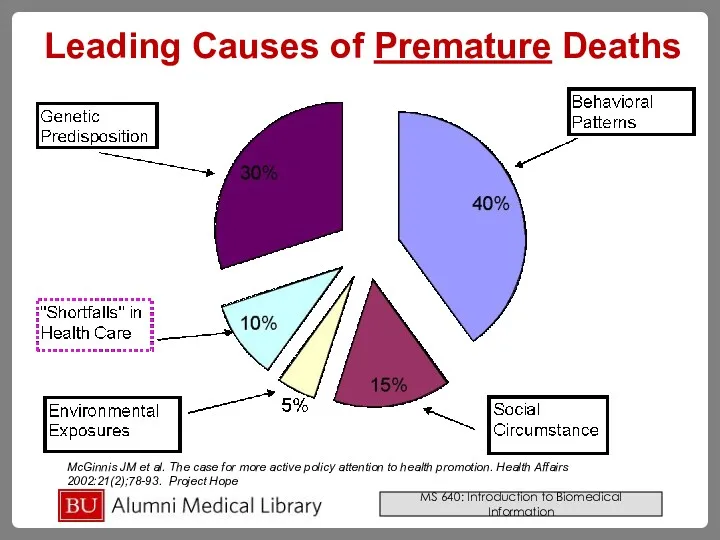
Leading Causes of Premature Deaths
McGinnis JM et al. The case for
Leading Causes of Premature Deaths
McGinnis JM et al. The case for
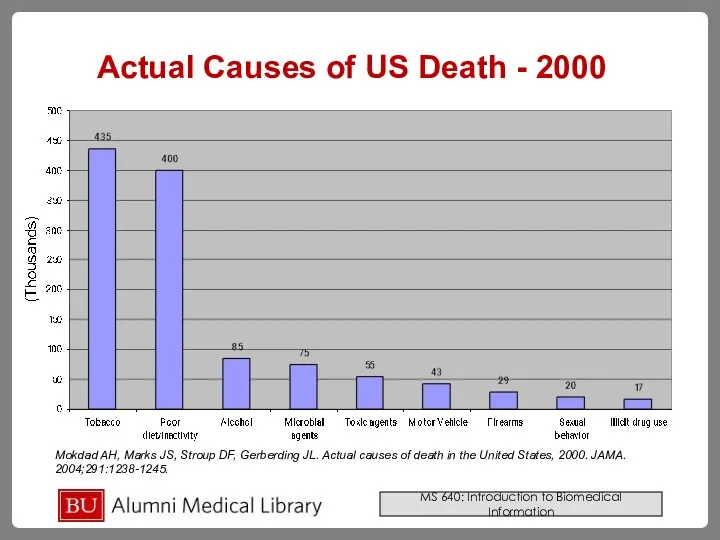
Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of
Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of
Leading causes of death
How do physicians address these causes?
Do you expand
Leading causes of death
How do physicians address these causes?
Do you expand
“The health care System”? – What it DOES…
One Perspective
Provides services:
Somatic
“The health care System”? – What it DOES…
One Perspective
Provides services:
Somatic
The health care System –
5 Main Components
Education and Research: professional
The health care System –
5 Main Components
Education and Research: professional
The health care System – Provider Groups
Preventive Care: Primary Care Providers
The health care System – Provider Groups
Preventive Care: Primary Care Providers
The health care System – Provider Groups
Acute Care – Hospitals, “Urgent
The health care System – Provider Groups
Acute Care – Hospitals, “Urgent
Public Health
health care
System
Environmental Health
Biostatistics
Nutrition
Physical
Fitness
Pharmacology
“Basic Sciences”
Inpatient Care
Cancer
“Disparities”
?
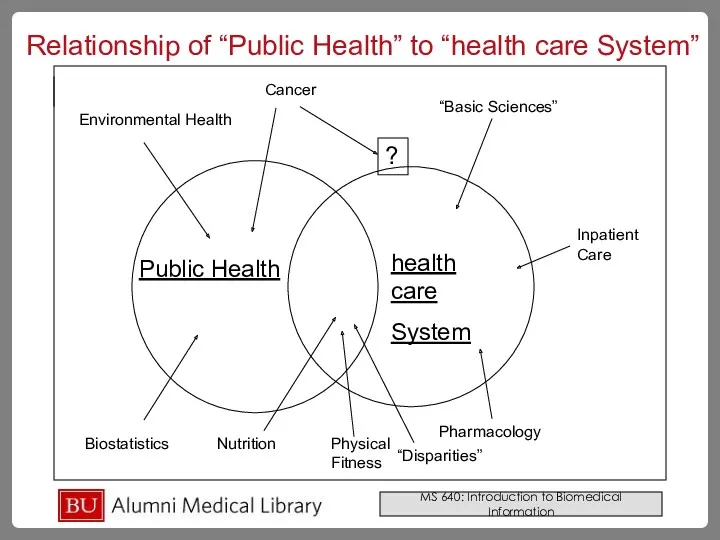
Relationship of “Public Health” to
Public Health
health care
System
Environmental Health
Biostatistics
Nutrition
Physical
Fitness
Pharmacology
“Basic Sciences”
Inpatient Care
Cancer
“Disparities”
?
Relationship of “Public Health” to
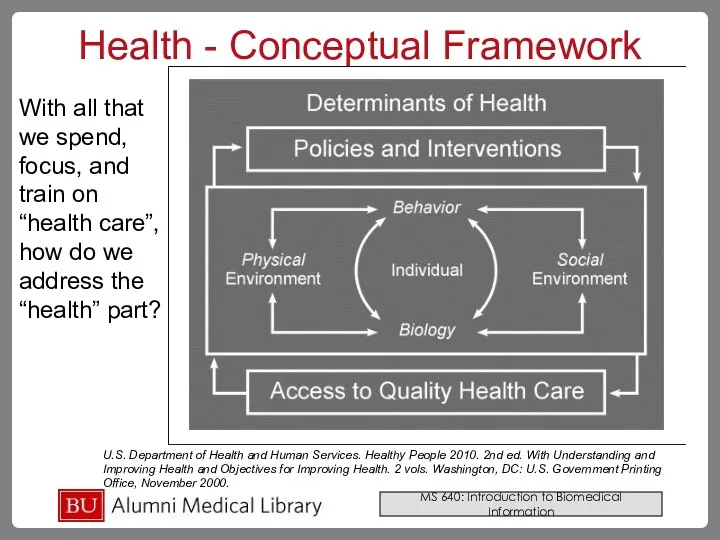
Health - Conceptual Framework
U.S. Department of Health and Human Services. Healthy
Health - Conceptual Framework
U.S. Department of Health and Human Services. Healthy
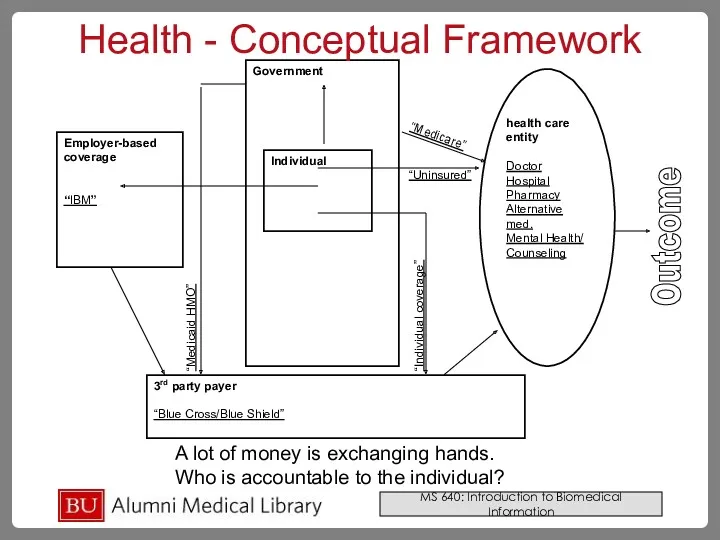
“Medicaid HMO”
“Individual coverage”
“Uninsured”
“Medicare”
A lot of money is exchanging hands.
Who is
“Medicaid HMO”
“Individual coverage”
“Uninsured”
“Medicare”
A lot of money is exchanging hands.
Who is
Kaiser Family Foundation, statehealthfacts.org -
“Health Insurance Coverage of the Total
Kaiser Family Foundation, statehealthfacts.org - “Health Insurance Coverage of the Total
Kaiser Family Foundation, statehealthfacts.org -
“Health Insurance Coverage of the Total
Kaiser Family Foundation, statehealthfacts.org - “Health Insurance Coverage of the Total
Employer-Based and Individual
53% - Employer-based, 5% individual-purchased
Dependants/spouses
Government employees included
Most will have
Employer-Based and Individual
53% - Employer-based, 5% individual-purchased
Dependants/spouses
Government employees included
Most will have
Employer-Based and Individual
Tax policy favors employee-based benefit
Companies that spend money in
Employer-Based and Individual
Tax policy favors employee-based benefit
Companies that spend money in
Medicare – “Elderly”
42 Million recipients – $325 Billion in 2003
Federally-funded
> 65
Medicare – “Elderly”
42 Million recipients – $325 Billion in 2003
Federally-funded
> 65
Medicare – “Elderly”
Parts A, B, C, D
A: Hospital and Skilled nursing
Medicare – “Elderly”
Parts A, B, C, D
A: Hospital and Skilled nursing
“Medicare at a Glance,” (#1066-08), The Henry J. Kaiser Family Foundation,
“Medicare at a Glance,” (#1066-08), The Henry J. Kaiser Family Foundation,
“Medicare at a Glance,” (#1066-08), The Henry J. Kaiser Family Foundation,
“Medicare at a Glance,” (#1066-08), The Henry J. Kaiser Family Foundation,
Medicaid – “Poor”
52 million recipients - $266 Billion in 2003
Federal-State Partnership
Eligibility
Medicaid – “Poor”
52 million recipients - $266 Billion in 2003
Federal-State Partnership
Eligibility
Medicaid – “Poor”
May contract as “Medicaid HMO” with non-government entity
Future –
Medicaid – “Poor”
May contract as “Medicaid HMO” with non-government entity
Future –
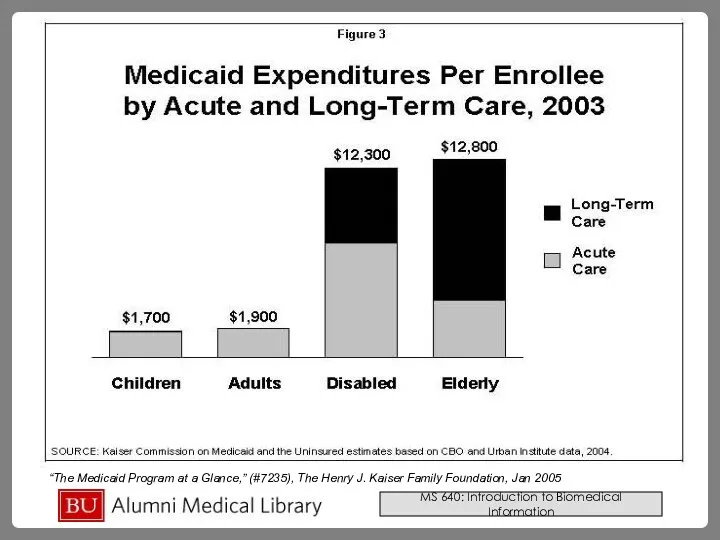
“The Medicaid Program at a Glance,” (#7235), The Henry J. Kaiser
“The Medicaid Program at a Glance,” (#7235), The Henry J. Kaiser
The Uninsured
Over 45 million in 2004
Coverage = services. No coverage =
The Uninsured
Over 45 million in 2004
Coverage = services. No coverage =
Most uninsured are in working families, but in jobs without benefits.
“The
Most uninsured are in working families, but in jobs without benefits.
“The
“The Uninsured and Their Access to Health Care,” (#1420-05), The Henry
“The Uninsured and Their Access to Health Care,” (#1420-05), The Henry
Leads to price sensitivity: The higher the cost,
the less likely
Leads to price sensitivity: The higher the cost,
the less likely
Anderson GF, Hussey PS, Frogner BK, Waters HR. Health spending in
Anderson GF, Hussey PS, Frogner BK, Waters HR. Health spending in
Summary
Health, itself, is not simply a function of health care, but
Summary
Health, itself, is not simply a function of health care, but
Massachusetts Health Care Reform Plan
Passed April 12, 2006
Aims to provide universal
Massachusetts Health Care Reform Plan
Passed April 12, 2006
Aims to provide universal
Looking up Information on the
health care system
Different types of Information:
Background
Gray
Looking up Information on the
health care system
Different types of Information:
Background
Gray
Background
Resources that offer descriptive and consumer level information on various health
Background
Resources that offer descriptive and consumer level information on various health
Books
Good for explanations that integrate interdisciplinary factors of the health care
Books
Good for explanations that integrate interdisciplinary factors of the health care
Gray Literature
A lot of material concerning health care issues can
Gray Literature
A lot of material concerning health care issues can
Finding Gray Literature
Policy Institutes/Think Tanks:
National Health Policy Forum
Commonwealth
Finding Gray Literature
Policy Institutes/Think Tanks:
National Health Policy Forum
Commonwealth
Looking up Statistics – US Government
AHRQ: Agency for health care
Looking up Statistics – US Government
AHRQ: Agency for health care
Looking up Statistics – Other sources
Dartmouth Atlas of Health Care
Looking up Statistics – Other sources
Dartmouth Atlas of Health Care
Research and Journal Articles
Databases
Medline: PubMed
In PubMed can
Research and Journal Articles
Databases
Medline: PubMed
In PubMed can
PubMed Health Services Queries
A search interface to find PubMed citations
PubMed Health Services Queries
A search interface to find PubMed citations
Healthy People 2010
Pre-formulated PubMed searches based on objectives of a
Healthy People 2010
Pre-formulated PubMed searches based on objectives of a
International Health Care
Global Health Facts
From the Kaiser Family Foundation
International Health Care
Global Health Facts
From the Kaiser Family Foundation
 Halloween monsters
Halloween monsters Infinitive and ingforms
Infinitive and ingforms Cognitive stylistics. Theory of cognitive metaphor. (Lecture 5)
Cognitive stylistics. Theory of cognitive metaphor. (Lecture 5) Plan for today
Plan for today Perm National Research Polytechnic University
Perm National Research Polytechnic University Food containers. Vocabulary
Food containers. Vocabulary Famous people of New Zealand
Famous people of New Zealand The words. (Unit 2)
The words. (Unit 2) Let’s cook!
Let’s cook! Some , Any, How much or How many?
Some , Any, How much or How many? Autecology (idioecology) or Individual Ecology
Autecology (idioecology) or Individual Ecology Auxiliary verb game
Auxiliary verb game ЕГЭ. Английский язык. Вариант 1
ЕГЭ. Английский язык. Вариант 1 Способы выражения будущего времени. 6 класс
Способы выражения будущего времени. 6 класс Пассивный залог
Пассивный залог History Gothic
History Gothic Spring Framework
Spring Framework Англоязычная публикация международного уровня: структура, содержание, стиль (Часть 1)
Англоязычная публикация международного уровня: структура, содержание, стиль (Часть 1) Day tour in Georgia
Day tour in Georgia Class assignment
Class assignment Present continious (basics)
Present continious (basics) Skeleton
Skeleton Comparison
Comparison Types of questions. Типы вопросов
Types of questions. Типы вопросов Ethical perspectives and corporate social responsibility. Utilitarianism
Ethical perspectives and corporate social responsibility. Utilitarianism Living plants
Living plants Классификация местоимений
Классификация местоимений Настоящее совершенное
Настоящее совершенное