- Acute Pancreatitis

Содержание
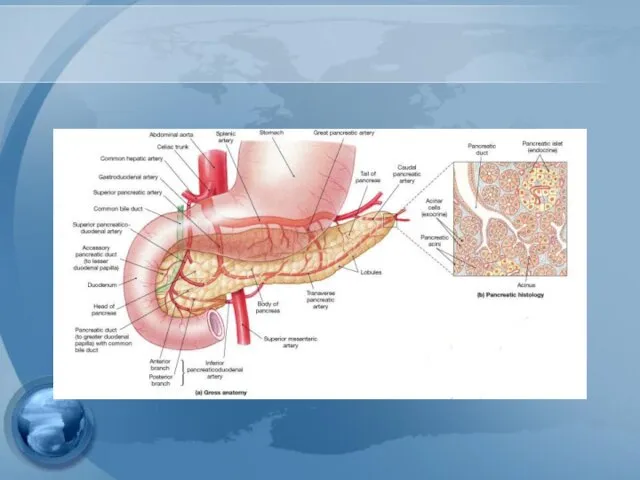
- 2. Anatomy
- 4. Introduction Water & Electrolyte Secretion Bicarbonate – most important Na, K, Cl, Ca, Zn, PO4, SO4
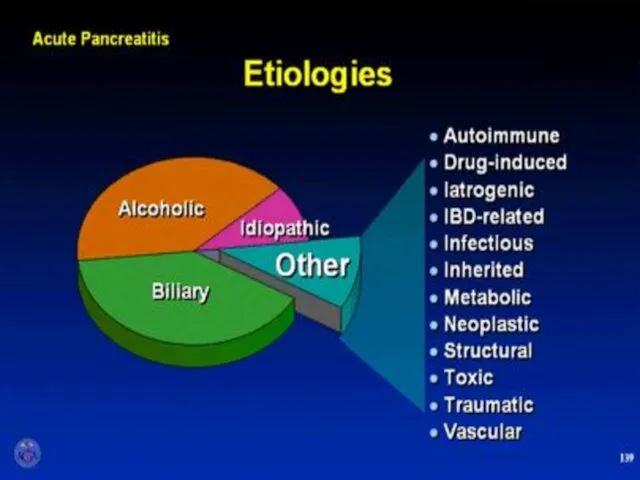
- 5. What are the two most common etiologies for acute pancreatitis in the western civilization? Drugs and
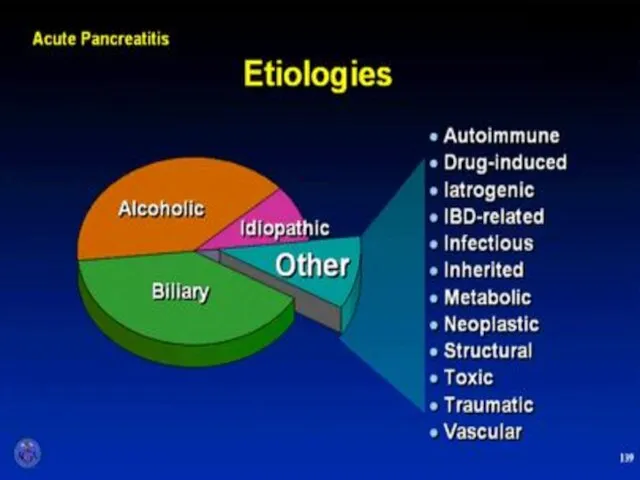
- 6. Etiology
- 8. Gallstone pancreatitis Mechanism is not entirely clear Common-channel theory “Blockage below junction of biliary and pancreatic
- 9. Mechanism??? Ductal hypertension Cause rupture of small ducts and leakage of pancreatic juice pH in pancreatic
- 10. Alcoholic pancreatitis Common in pt. alcohol drinking > 2yr. Often much longer up to 10 yr.
- 12. Which of the following drugs is well known for it’s ability to induce pancreatitis? Propranolol Erythromycin
- 14. AGA Institute
- 15. Diagnosis
- 16. Diagnostic criteria Two of following three features Upper abd. pain of acute onset often radiating to
- 17. Physical exam Grey Turner’s Sign - ecchymosis in 1 or both flanks Cullen’s sign - ecchymosis
- 18. Grey Turner’s Sign
- 19. Cullen’s Sign
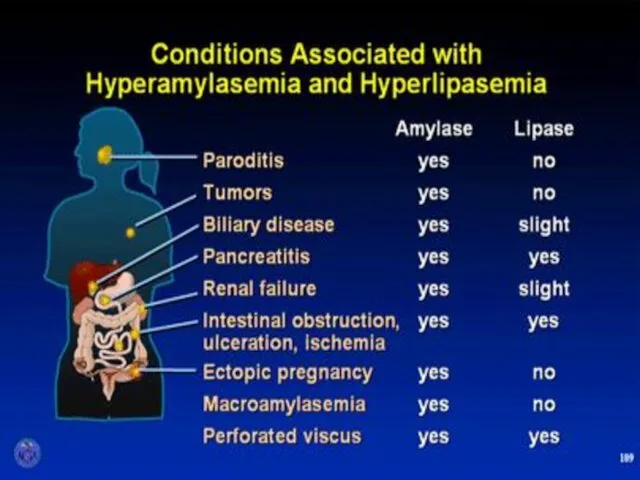
- 20. Serum markers
- 21. Serum amylase Elevates within HOURS and can remain elevated for 3-5 days High specificity when level
- 22. Urine amylase urinary levels may be more sensitive than serum levels. Urinary amylase levels usually remain
- 23. Serum lipase The preferred test for diagnosis Begins to increase 4-8H after onset of symptoms and
- 25. Plain Abdominal Radiograph
- 26. Plain Abdominal Radiograph Bowel ileus “Sentinel Loop” “Colon cut off sign” Loss of psoas shadow Helps
- 27. Radiologic Findings Plain radiographs contribute little Ultrasound may show the pancreas in only 25-50% CT scan
- 28. Assessment of severity
- 29. Classification of severity - Mild : lack of organ failure or systemic complications - Moderate :
- 30. Complication
- 31. Which of the following is not considered adverse prognostic feature in acute pancreatitis? 1. WBC> 16,000
- 32. Early prognostic signs Ranson’s score APACHE II
- 34. Ranson’s Criteria (GB Pancreatitis) At Admission Age > 70 yr WBC > 18,000/mm3 Blood glucose >
- 35. APACHE II Measure at during the first 24 hours after admission Using a cutoff of ≥8
- 36. APACHE II
- 37. Biochemical marker CRP at 48hr cutoff 150mg/L Sens. 80% Spec. 76% TAP Interleukins ???
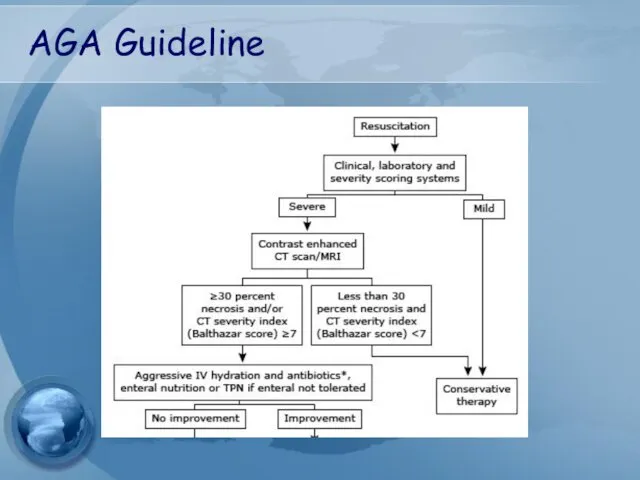
- 38. CT severity score (Balthazar score) ≥6 = severe disease.
- 40. Treatment
- 41. Treatment General Considerations - adequate IV hydration and analgesia - NPO - NG tube: not routinely
- 42. Treatment Metabolic Complications - Correction of electrolyte imbalance - Ca,Mg - Cautiously for hyperglycemia Cardiovascular Care
- 43. Prophylactic antibiotics Although this is still an area of debate Not indicated for mild attack suggest
- 44. TREATMENT OF ASSOCIATED CONDITIONS Gallstone pancreatitis ERCP should be performed within 72 hours in those with
- 45. Cholecystectomy?? should be performed after recovery in all patient with gallstone pancreatitis Failure to perform a
- 46. Cholecystectomy In mild pancreatitis case, can usually be performed safely within 7 days after recovery In
- 47. Complications
- 48. Local Complications Pseudocyst Abscess Necrosis Sterile Infected Mild pancreatitis severe pancreatitis Pseudocyst abscess Pancreatic necrosis
- 49. Infected pancreatic necrosis. The most common organisms include E.coli, Pseudomonas, Klebsiella, and Enterococcus
- 50. Guideline management of severe pancreatitis
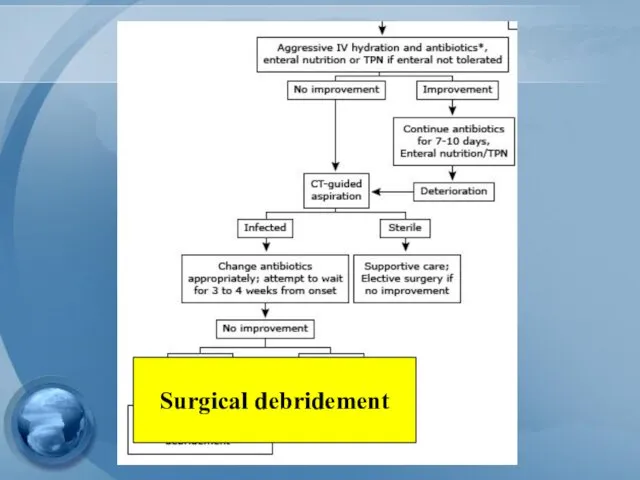
- 51. AGA Guideline
- 52. Surgical debridement
- 53. Management of pseudocyst
- 54. Management of pseudocyst Watchful waiting: Operative intervention was recommended following an observation period of 6 wks
- 55. Management of pseudocyst Surgical drainage – gold standard Open vs endoscopic cystgastrostomy Cystenterostomy Cystojejunostomy, Cystoduodenostomy Ressection
- 56. Management of pseudocyst Percutaneous catheter drainage As effective as surgery in draining and closing both sterile
- 57. Management of local complication of pancreatitis
- 58. Indication for pancreatic debridement Infected pancreatic necrosis Symptomatic sterile pancreatic necrosis chronic low grade fever Nausea
- 59. Timing of debridement The optimal timing is at least 3-4wks following the onset of acute pancreatitis.
- 61. Скачать презентацию
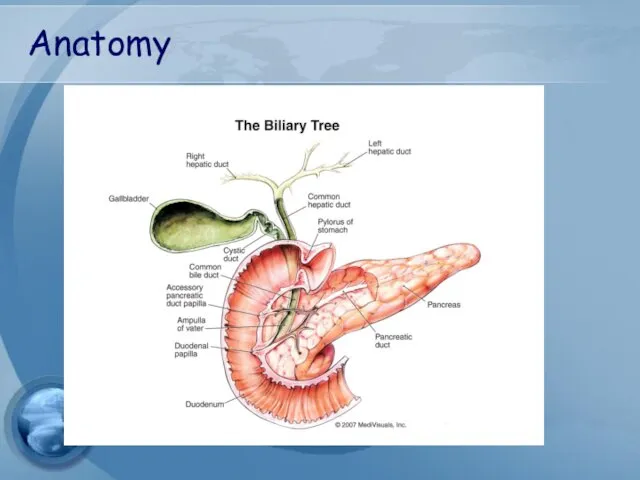
Anatomy
Anatomy
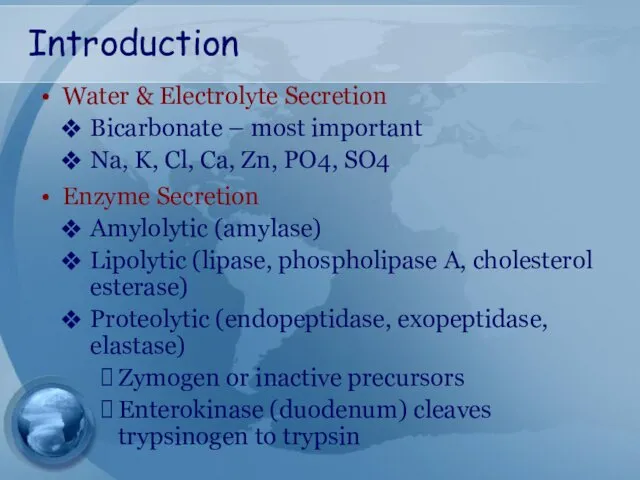
Introduction
Water & Electrolyte Secretion
Bicarbonate – most important
Na, K, Cl, Ca, Zn,
Introduction
Water & Electrolyte Secretion
Bicarbonate – most important
Na, K, Cl, Ca, Zn,
What are the two most common etiologies for acute pancreatitis in
What are the two most common etiologies for acute pancreatitis in

Etiology
Etiology
Gallstone pancreatitis
Mechanism is not entirely clear
Common-channel theory
“Blockage below junction of
Gallstone pancreatitis
Mechanism is not entirely clear
Common-channel theory
“Blockage below junction of
Mechanism???
Ductal hypertension
Cause rupture of small ducts and leakage of pancreatic
Mechanism???
Ductal hypertension
Cause rupture of small ducts and leakage of pancreatic
Alcoholic pancreatitis
Common in pt. alcohol drinking > 2yr.
Often much longer
Alcoholic pancreatitis
Common in pt. alcohol drinking > 2yr.
Often much longer
Which of the following drugs is well known for it’s ability
Which of the following drugs is well known for it’s ability
AGA Institute
AGA Institute

Diagnosis
Diagnosis
Diagnostic criteria
Two of following three features
Upper abd. pain of acute onset
Diagnostic criteria
Two of following three features
Upper abd. pain of acute onset
Physical exam
Grey Turner’s Sign
- ecchymosis in 1 or both flanks
Cullen’s sign
-
Physical exam
Grey Turner’s Sign
- ecchymosis in 1 or both flanks
Cullen’s sign
-

Grey Turner’s Sign
Grey Turner’s Sign

Cullen’s Sign
Cullen’s Sign

Serum markers
Serum markers
Serum amylase
Elevates within HOURS and can remain elevated for 3-5 days
High
Serum amylase
Elevates within HOURS and can remain elevated for 3-5 days
High
Urine amylase
urinary levels may be more sensitive than serum levels.
Urinary amylase
Urine amylase
urinary levels may be more sensitive than serum levels.
Urinary amylase
Serum lipase
The preferred test for diagnosis
Begins to increase 4-8H after onset
Serum lipase
The preferred test for diagnosis
Begins to increase 4-8H after onset
Plain Abdominal Radiograph
Plain Abdominal Radiograph
Plain Abdominal Radiograph
Bowel ileus
“Sentinel Loop”
“Colon cut off sign”
Loss of
Plain Abdominal Radiograph
Bowel ileus
“Sentinel Loop”
“Colon cut off sign”
Loss of
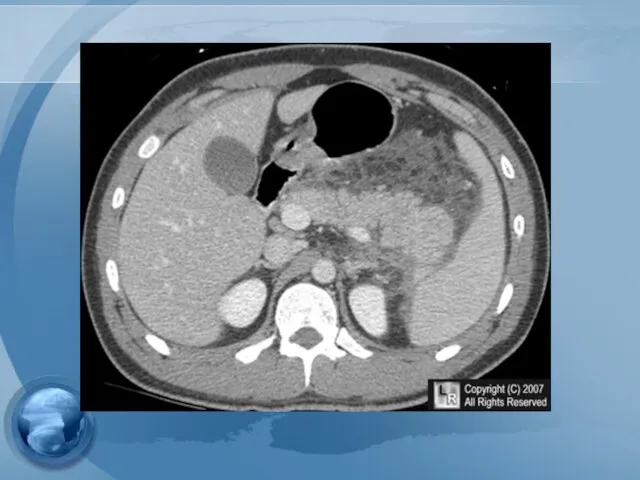
Radiologic Findings
Plain radiographs contribute little
Ultrasound may show the pancreas in only
Radiologic Findings
Plain radiographs contribute little
Ultrasound may show the pancreas in only

Assessment of severity
Assessment of severity
Classification of severity
- Mild : lack of organ failure or systemic
Classification of severity
- Mild : lack of organ failure or systemic
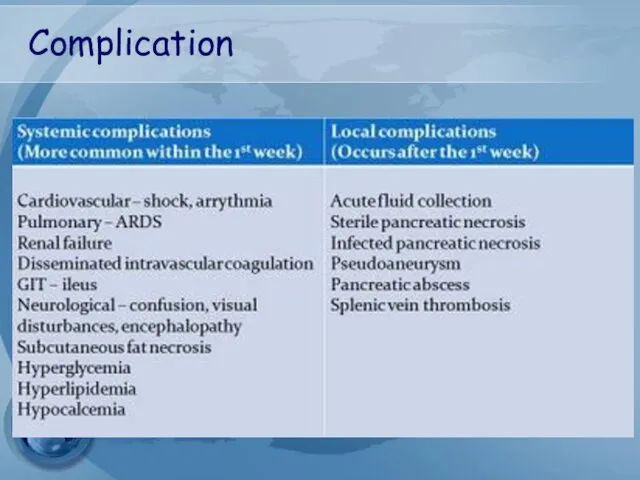
Complication
Complication
Which of the following is not considered adverse prognostic feature in
Which of the following is not considered adverse prognostic feature in

Early prognostic signs
Ranson’s score
APACHE II
Early prognostic signs
Ranson’s score
APACHE II
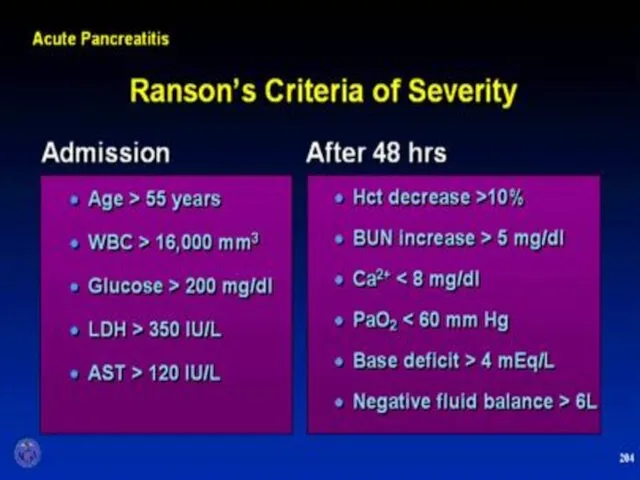
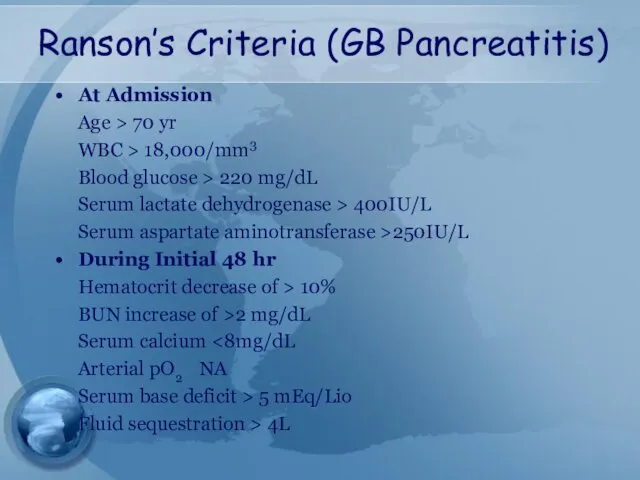
Ranson’s Criteria (GB Pancreatitis)
At Admission
Age > 70 yr
WBC > 18,000/mm3
Blood glucose
Ranson’s Criteria (GB Pancreatitis)
At Admission
Age > 70 yr
WBC > 18,000/mm3
Blood glucose
APACHE II
Measure at during the first 24 hours after admission
Using a
APACHE II
Measure at during the first 24 hours after admission
Using a
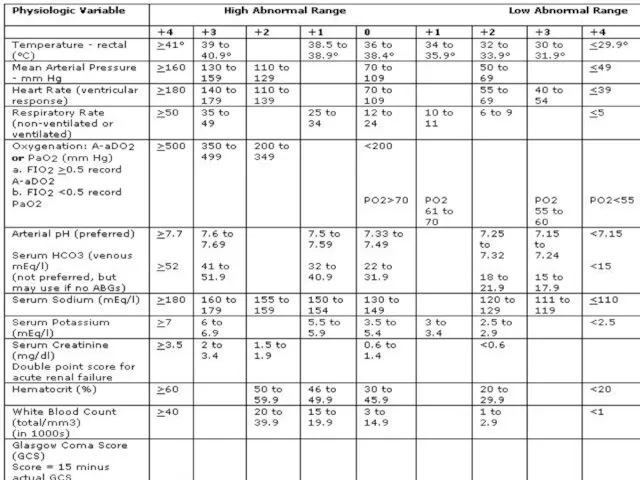
APACHE II
APACHE II
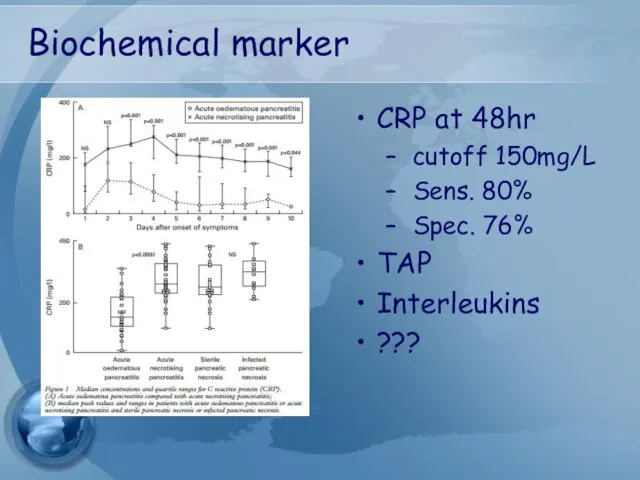
Biochemical marker
CRP at 48hr
cutoff 150mg/L
Sens. 80%
Spec. 76%
TAP
Interleukins
???
Biochemical marker
CRP at 48hr
cutoff 150mg/L
Sens. 80%
Spec. 76%
TAP
Interleukins
???
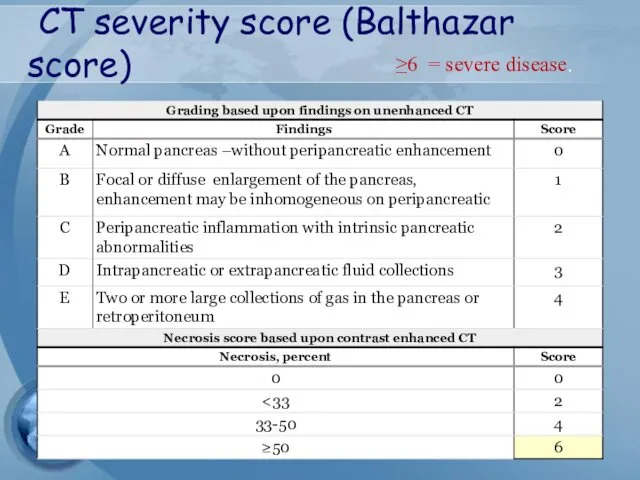
CT severity score (Balthazar score)
≥6 = severe disease.
CT severity score (Balthazar score)
≥6 = severe disease.

Treatment
Treatment
Treatment
General Considerations
- adequate IV hydration and analgesia
- NPO
- NG tube:
Treatment
General Considerations
- adequate IV hydration and analgesia
- NPO
- NG tube:
Treatment
Metabolic Complications
- Correction of electrolyte imbalance - Ca,Mg
- Cautiously for
Treatment
Metabolic Complications
- Correction of electrolyte imbalance - Ca,Mg
- Cautiously for
Prophylactic antibiotics
Although this is still an area of debate
Not indicated for
Prophylactic antibiotics
Although this is still an area of debate
Not indicated for
TREATMENT OF
ASSOCIATED CONDITIONS
Gallstone pancreatitis
ERCP should be performed within 72 hours
TREATMENT OF
ASSOCIATED CONDITIONS
Gallstone pancreatitis
ERCP should be performed within 72 hours
Cholecystectomy??
should be performed after recovery in all patient with gallstone pancreatitis
Failure
Cholecystectomy??
should be performed after recovery in all patient with gallstone pancreatitis
Failure
Cholecystectomy
In mild pancreatitis case, can usually be performed safely within 7
Cholecystectomy
In mild pancreatitis case, can usually be performed safely within 7

Complications
Complications
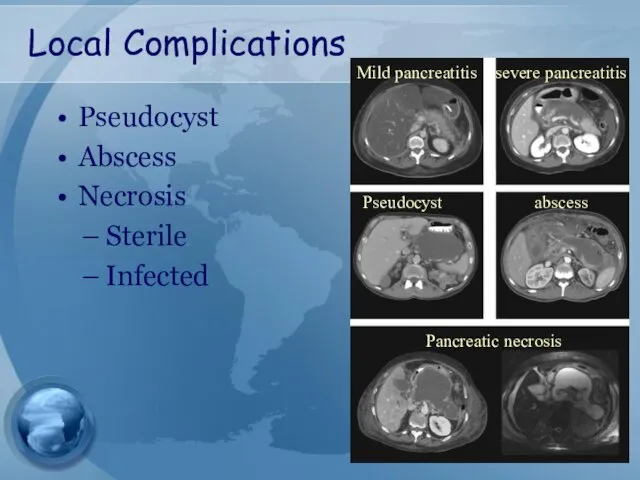
Local Complications
Pseudocyst
Abscess
Necrosis
Sterile
Infected
Mild pancreatitis
severe pancreatitis
Pseudocyst
abscess
Pancreatic necrosis
Local Complications
Pseudocyst
Abscess
Necrosis
Sterile
Infected
Mild pancreatitis
severe pancreatitis
Pseudocyst
abscess
Pancreatic necrosis
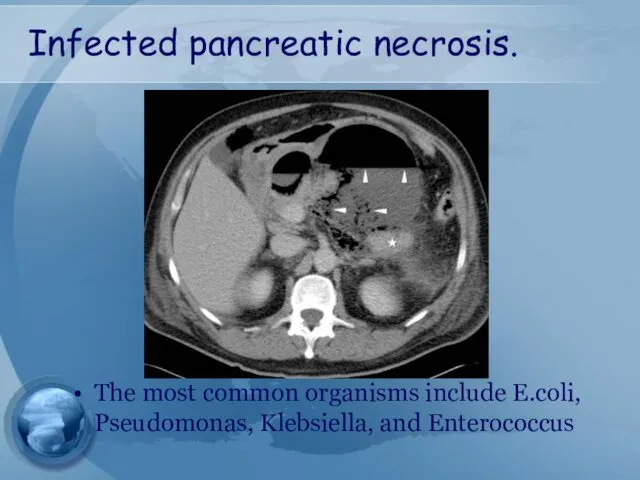
Infected pancreatic necrosis.
The most common organisms include E.coli, Pseudomonas, Klebsiella,
Infected pancreatic necrosis.
The most common organisms include E.coli, Pseudomonas, Klebsiella,
Guideline management of
severe pancreatitis
Guideline management of
severe pancreatitis
AGA Guideline
AGA Guideline
Surgical debridement
Surgical debridement
Management of pseudocyst
Management of pseudocyst
Management of pseudocyst
Watchful waiting:
Operative intervention was recommended following an observation
Management of pseudocyst
Watchful waiting:
Operative intervention was recommended following an observation
Management of pseudocyst
Surgical drainage – gold standard
Open vs endoscopic
cystgastrostomy
Cystenterostomy
Cystojejunostomy, Cystoduodenostomy
Ressection
Management of pseudocyst
Surgical drainage – gold standard
Open vs endoscopic
cystgastrostomy
Cystenterostomy
Cystojejunostomy, Cystoduodenostomy
Ressection
Management of pseudocyst
Percutaneous catheter drainage
As effective as surgery in draining and
Management of pseudocyst
Percutaneous catheter drainage
As effective as surgery in draining and

Management of local complication of pancreatitis
Management of local complication of pancreatitis
Indication for
pancreatic debridement
Infected pancreatic necrosis
Symptomatic sterile pancreatic necrosis
chronic low grade fever
Nausea
Lethargy
Inability
Indication for
pancreatic debridement
Infected pancreatic necrosis
Symptomatic sterile pancreatic necrosis
chronic low grade fever
Nausea
Lethargy
Inability
Timing of debridement
The optimal timing is at least 3-4wks following the
Timing of debridement
The optimal timing is at least 3-4wks following the
 Общая семиотика экстрапирамидных нарушений
Общая семиотика экстрапирамидных нарушений Лікарські засоби промислового виробництва, що проявляють гепатопротекторну дію
Лікарські засоби промислового виробництва, що проявляють гепатопротекторну дію Гнойные заболевания костей и суставов. (Лекция 26)
Гнойные заболевания костей и суставов. (Лекция 26) Здоровый образ жизни. Медико – профилактическое направление здравоохранения. Виды профилактики
Здоровый образ жизни. Медико – профилактическое направление здравоохранения. Виды профилактики Гинекологиядағы нейроэндокринді синдромдар
Гинекологиядағы нейроэндокринді синдромдар ОМП. Бактериологическое оружие
ОМП. Бактериологическое оружие Болевой синдром
Болевой синдром Федеральный закон Об обращении лекарственные средств. (Лекции 7,8)
Федеральный закон Об обращении лекарственные средств. (Лекции 7,8) Протезирование дефектов зубных рядов пластмассовыми комбинированными и цельнокерамическими коронками
Протезирование дефектов зубных рядов пластмассовыми комбинированными и цельнокерамическими коронками Воспаление. Флогогены
Воспаление. Флогогены Braster pro-иновационная система обследования молочной железы
Braster pro-иновационная система обследования молочной железы Клиническая анатомия головы. Хирургическая анатомия мозгового отдела головы
Клиническая анатомия головы. Хирургическая анатомия мозгового отдела головы Пищевые отравления и их профилактика
Пищевые отравления и их профилактика Легочная гипертензия
Легочная гипертензия Роль питания в профилактике и лечении рака. Клиника иммунопатологии Мира
Роль питания в профилактике и лечении рака. Клиника иммунопатологии Мира Анатомо-фізіологічні особливості шлунково-кишкового тракту. Методика обстеження ШКТ. (Лекція 4)
Анатомо-фізіологічні особливості шлунково-кишкового тракту. Методика обстеження ШКТ. (Лекція 4) Ларинготрахеит у детей
Ларинготрахеит у детей Биоптрон 2014
Биоптрон 2014 Рациональная антибиотикотерапия при бактериальных осложнениях ОРВИ
Рациональная антибиотикотерапия при бактериальных осложнениях ОРВИ Санитарная микробиология
Санитарная микробиология Этика в психиатрии и психотерапии
Этика в психиатрии и психотерапии Концепция здоровья Coral Club
Концепция здоровья Coral Club Гранулематоз Вегенера
Гранулематоз Вегенера Острые гастродуоденальные кровотечения. Принципы диагностики и лечения
Острые гастродуоденальные кровотечения. Принципы диагностики и лечения Аневризма сердца
Аневризма сердца Іріңді-септикалық асқынулар кезіндегі интенсивті терапия
Іріңді-септикалық асқынулар кезіндегі интенсивті терапия Туберкульоз. Історія боротьби
Туберкульоз. Історія боротьби Организация стоматологического терапевтического кабинета
Организация стоматологического терапевтического кабинета