- Bronchial asthma in children

Содержание
- 2. Plan of the lecture 1. Definition of bronchial asthma 2. Factors of development 3. Bronchial asthma
- 3. What do we know about asthma? Bronchial asthma is a chronic inflammatory disorder of the airways
- 4. Asthma is a problem worldwide with an estimated 300 million affected individuals BA morbidity increased twice
- 5. Predisposing Factors: Genes pre-disposing to allergic reactions Airway hyperresponsiveness– The characteristic functional abnormality of asthma results
- 6. Sensibilization Factors : Indoor: domestic mites, domestic and library dust, cockroaches allergenes, fish fodder, feather of
- 7. Family Glycyphagidae Mites Dermatophagoides rodens Stock mites Acarus siro Healthy BA Mild course BA moderate course
- 8. Resolution factors ( triggers): Pollutants – compounds of serum, nickel, Cobalt etc.-result of industrial plants activity,
- 9. Extrinsic asthma The asthma episode is typically initiated by the type1hypersensitivity reaction induced by exposure to
- 10. Intrinsic asthma The triggering mechanisms are non-immune in this form a number of stimuli that have
- 11. Drug induced asthma Is seen most commonly with 1.NSAID’S (COX-1 inhibitors) 2.Aspirin, Ibuprofen 3.Propranolol (because non
- 12. Bronchial Asthma Pathogenesis Early phase Allergen Fixation on mast cells, eosinophils, basophils, thrombocytes Cell activation Hyperproduction
- 13. Bronchial Asthma Pathogenesis Late phasePathophysiological stage) Releasing of primary mediators (PG, Tx, PAF, LT) Eosinophils, neutrophils,
- 14. Bronchial Asthma Pathogenesis Late stage (Pathophysiological stage) Bronchoobstruc- tive syndrome Microvasculature impairment Bronchial spasm and hyperreactivity
- 15. MUCOUS EDEMA Sputum hyperproduction Bronchial spasm
- 16. Slice of normal bronchi Slice of Spasmodic bronchi
- 17. Neutrophil
- 18. Smooth muscle dysfunction Inflammation ПАТОГЕНЕЗ БРОНХИАЛЬНОЙ АСТМЫ Bronchial Asthma two component disease
- 19. Bronchial asthma – two component disease Exacerbation symptoms
- 20. Clinics of asthma exacerbation cough typical attacks of chest tightness, exhalative dyspnea, wheezing, dry cough, viscous
- 21. Sputum analysis 1.curschman’s spirals: Refers to finding in sputum of spiral shaped mucus plugs Airway epithelium
- 22. Sputum analysis Creole bodies: Found in a patient’s sputum they are ciliated columnar cells sluggshed from
- 23. Blood analysis Neutrophiles (band cells increased) Eosinophils also increased Serum IgE increased (Extrinsic asthma)
- 24. Skin allergy test: (prick test) Is a method for medical diagnosis of allergies that attempts to
- 25. Skin allergy test
- 26. It is very important that the subject should stay in the observation of physician for at
- 27. Peakflow meter Used to measure a persons maximum speed of expiration.
- 28. Pulmonary function test are carried out mostly by using spirometer The air in the lungs is
- 29. spirometer
- 30. spirometer
- 31. Late diagnostics of bronchial asthma Complicate bronchial asthma course prognosis Worsen life quality in bronchial asthma
- 32. What can be achieved due to full asthma control
- 33. Classification of Asthma severity Протокол по лечению и диагностке астмы у детей GINA 2003
- 34. The goal of asthma treatment is to achieve and maintain clinical control Treatment of asthma is
- 35. Step approach of BA treatment means increasing of medication according to severity of asthma. Physician can
- 36. BA treatment in acute period: Termination of the contact with allergen Oxygen therapy Inhaled В2-adrenomymetics (salbutamol
- 37. Medications for basic BA therapy Cromoglycium acid derivates Glucocorticosteroids (systemic, inhaled) Long acting inhaled b2-agonists Leukotriene
- 38. Antiinflammatory medications- derivates of cromoglycium acid Inhibit mast cells degranulation process Retard IgE- linked secretion of
- 39. Derivates of cromoglycium acid Mast cells membranes stabilizers: cromoglycium acid (intal,chromohexal,chromogenum) Nedocromyl sodium (tailed,tailed-mint)
- 40. Inhaled corticosteroids Inhaled corticosteroids (ICS) has the most manifested anti-inflammatory activity Reduce BA symptoms Decrease quantity
- 41. Systemic corticosteroids (hydrocortisone,dexamethasone, methylprednisolone, prednisolone, polcortolone) Inhaled corticosteroids Beclomethasone (becodisk, becotide, aldecine ) Fluticasone propionate (seretide,
- 42. Leukotriene modifiers Acolad (Zaferlucast) Singular (Montelucast)
- 43. Long acting b-2-agonistsагонисты: Salmeterol (Serevent,Serevent rotadisk) Clenbutirole (Spiropent) Formoterol (Formoteroloxis, Foradil)
- 44. Reliever Medications Broncholytic medications (bronchospasmolytics) Short acting b –adrenomymetics Salbutamol ( ventolin- nebulas,ventolin, bolmax, salomol, salben,
- 45. Reliever Medication Methylxantines (euphylline, theophylline) M-cholynoblockers - Ipratropium bromide (Atrovent)
- 46. Combined medications: Phenoterol + Ipratropium bromide = berodual Salbutamol + Ipratropium bromide = combivent Cromoglycate sodium
- 47. Medications for Nebulizer therapy Nebulizer – is inhalation device for spraying aerosol into very small disperse
- 48. The main goal of nebulizer therapy Delivering of medication therapeutic dosage in aerosol form Gaining of
- 49. Indications for nebulizer therapy It is used for intensive care in obstructive lung diseases, changed secretory
- 50. Advantages of nebulizer treatment It isn’t necessary coordinate respiratory with aerosole puffs Possibility to use high
- 51. Medications for nebulizer therapy Ventolin ( in nebulas 2,5 ml/2,5 mg nondeluted form) Berodual (solution for
- 52. Allergen specific immunotherapy Nowadays this method is the most effective treatment because of opportunity to influence
- 53. To decrease efficacy of BA therapy Educational programs ( for affected children and their parents in
- 54. Key statements of BA treatment The most efficient BA treatment is causative allergen elimination Asthma can
- 56. Скачать презентацию
Plan of the lecture
1. Definition of bronchial asthma
2. Factors of
Plan of the lecture
1. Definition of bronchial asthma
2. Factors of
What do we know about asthma?
Bronchial asthma is a chronic
What do we know about asthma?
Bronchial asthma is a chronic
Asthma is a problem worldwide with an estimated 300 million affected
Asthma is a problem worldwide with an estimated 300 million affected
Predisposing Factors:
Genes pre-disposing to allergic reactions
Airway hyperresponsiveness– The characteristic functional abnormality
Predisposing Factors:
Genes pre-disposing to allergic reactions
Airway hyperresponsiveness– The characteristic functional abnormality

Sensibilization Factors :
Indoor: domestic mites, domestic and library dust, cockroaches allergenes,
Sensibilization Factors :
Indoor: domestic mites, domestic and library dust, cockroaches allergenes,
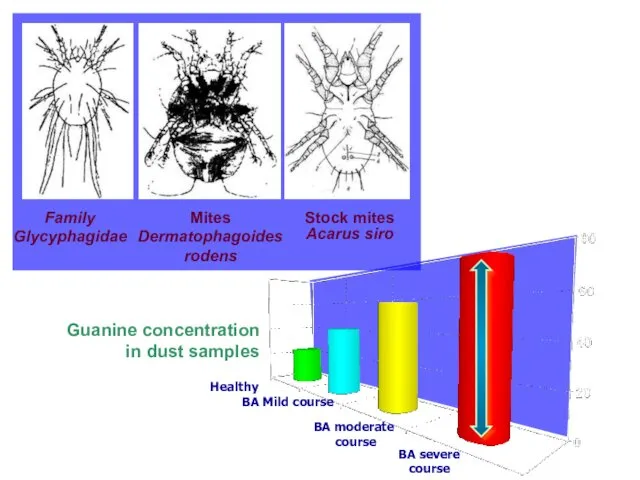
Family Glycyphagidae
Mites Dermatophagoides rodens
Stock mites
Acarus siro
Healthy
BA Mild course
BA moderate
course
BA severe
Family Glycyphagidae
Mites Dermatophagoides rodens
Stock mites
Acarus siro
Healthy
BA Mild course
BA moderate
course
BA severe
Resolution factors ( triggers):
Pollutants – compounds of serum, nickel, Cobalt etc.-result
Resolution factors ( triggers):
Pollutants – compounds of serum, nickel, Cobalt etc.-result
Extrinsic asthma
The asthma episode is typically initiated by the type1hypersensitivity reaction
Extrinsic asthma
The asthma episode is typically initiated by the type1hypersensitivity reaction
Intrinsic asthma
The triggering mechanisms are non-immune in this form a number
Intrinsic asthma
The triggering mechanisms are non-immune in this form a number
Drug induced asthma
Is seen most commonly with
1.NSAID’S (COX-1 inhibitors)
2.Aspirin, Ibuprofen
3.Propranolol
Drug induced asthma
Is seen most commonly with
1.NSAID’S (COX-1 inhibitors)
2.Aspirin, Ibuprofen
3.Propranolol
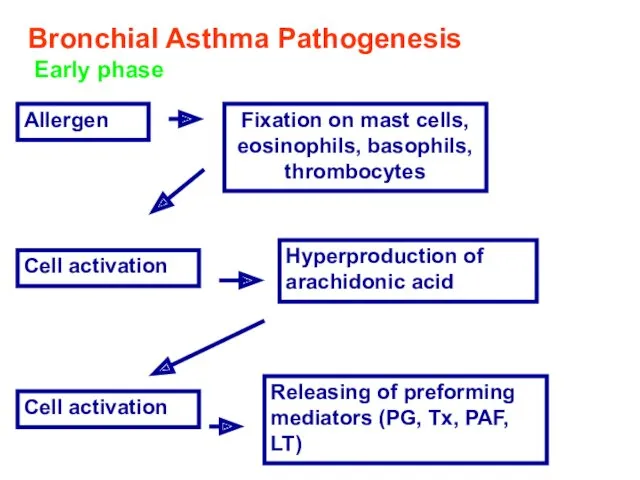
Bronchial Asthma Pathogenesis
Early phase
Allergen
Fixation on mast cells, eosinophils, basophils, thrombocytes
Cell
Bronchial Asthma Pathogenesis
Early phase
Allergen
Fixation on mast cells, eosinophils, basophils, thrombocytes
Cell
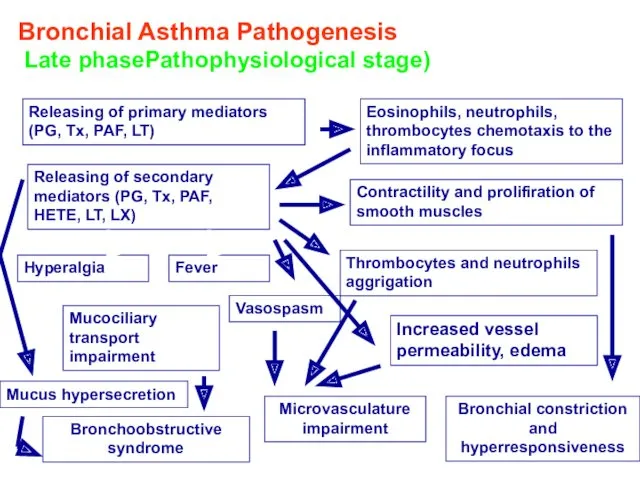
Bronchial Asthma Pathogenesis
Late phasePathophysiological stage)
Releasing of primary mediators (PG, Tx,
Bronchial Asthma Pathogenesis
Late phasePathophysiological stage)
Releasing of primary mediators (PG, Tx,
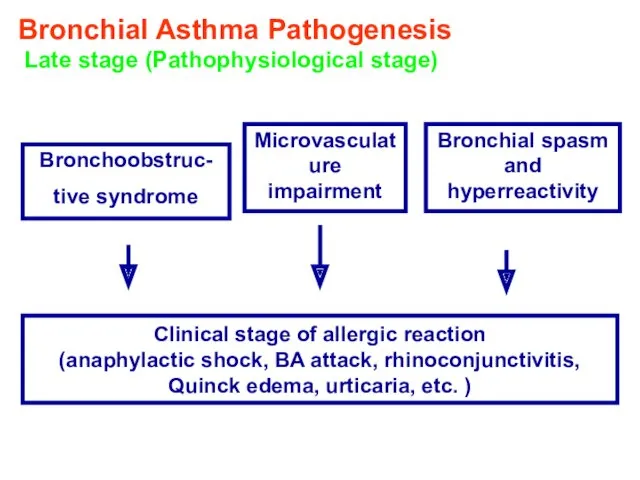
Bronchial Asthma Pathogenesis
Late stage (Pathophysiological stage)
Bronchoobstruc-
tive syndrome
Microvasculature impairment
Bronchial spasm and
Bronchial Asthma Pathogenesis
Late stage (Pathophysiological stage)
Bronchoobstruc-
tive syndrome
Microvasculature impairment
Bronchial spasm and
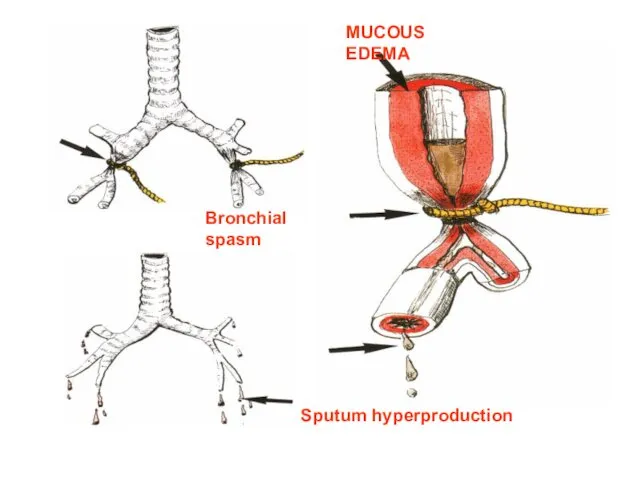
MUCOUS EDEMA
Sputum hyperproduction
Bronchial spasm
MUCOUS EDEMA
Sputum hyperproduction
Bronchial spasm
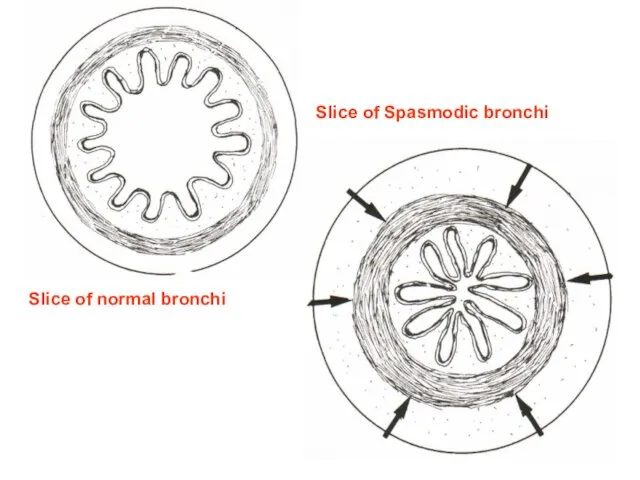
Slice of normal bronchi
Slice of Spasmodic bronchi
Slice of normal bronchi
Slice of Spasmodic bronchi
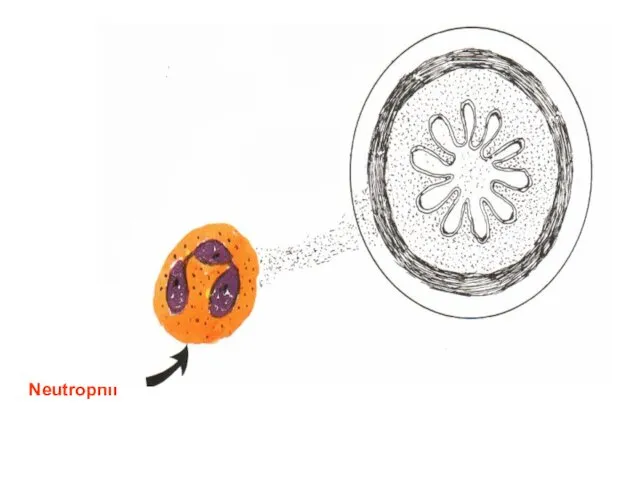
Neutrophil
Neutrophil
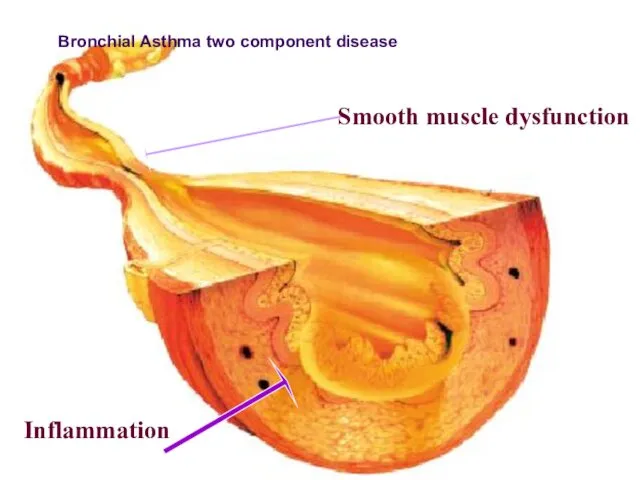
Smooth muscle dysfunction
Inflammation
ПАТОГЕНЕЗ БРОНХИАЛЬНОЙ АСТМЫ
Bronchial Asthma two component disease
Smooth muscle dysfunction
Inflammation
ПАТОГЕНЕЗ БРОНХИАЛЬНОЙ АСТМЫ
Bronchial Asthma two component disease
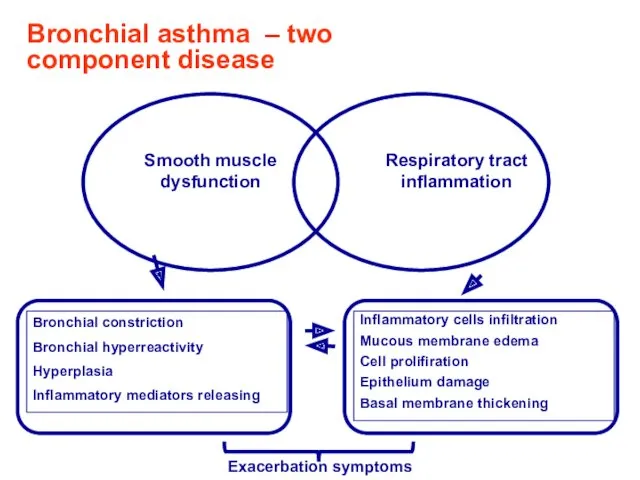
Bronchial asthma – two component disease
Exacerbation symptoms
Bronchial asthma – two component disease
Exacerbation symptoms
Clinics of asthma exacerbation
cough
typical attacks of chest tightness, exhalative dyspnea, wheezing,
Clinics of asthma exacerbation
cough
typical attacks of chest tightness, exhalative dyspnea, wheezing,
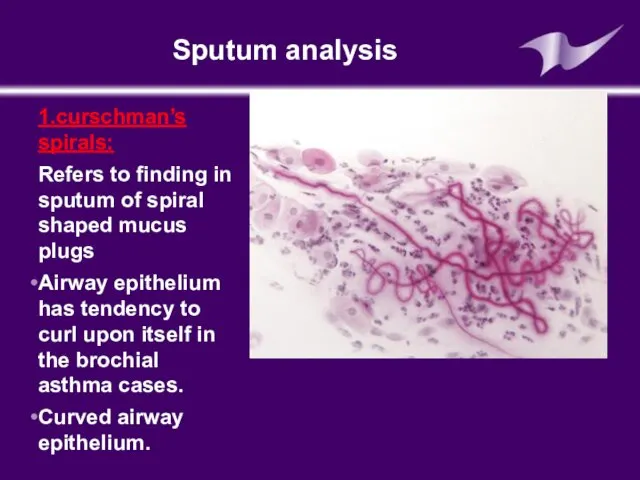
Sputum analysis
1.curschman’s spirals:
Refers to finding in sputum of spiral shaped
Sputum analysis
1.curschman’s spirals:
Refers to finding in sputum of spiral shaped
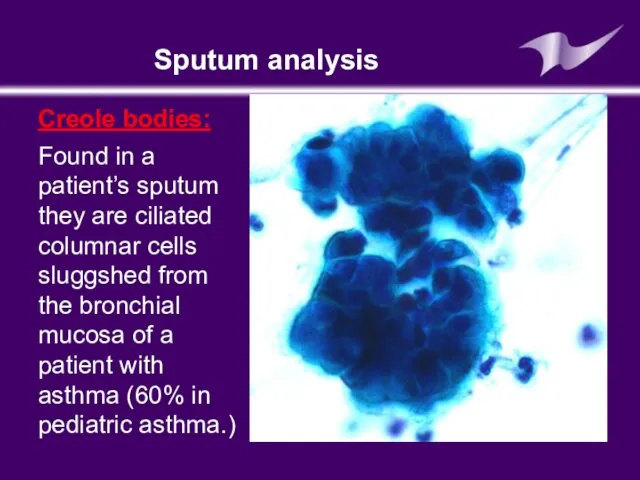
Sputum analysis
Creole bodies:
Found in a patient’s sputum they are ciliated columnar
Sputum analysis
Creole bodies:
Found in a patient’s sputum they are ciliated columnar
Blood analysis
Neutrophiles (band cells increased)
Eosinophils also increased
Serum IgE increased (Extrinsic asthma)
Blood analysis
Neutrophiles (band cells increased)
Eosinophils also increased
Serum IgE increased (Extrinsic asthma)
Skin allergy test: (prick test)
Is a method for medical diagnosis of
Skin allergy test: (prick test)
Is a method for medical diagnosis of

Skin allergy test
Skin allergy test
It is very important that the subject should stay in the
It is very important that the subject should stay in the
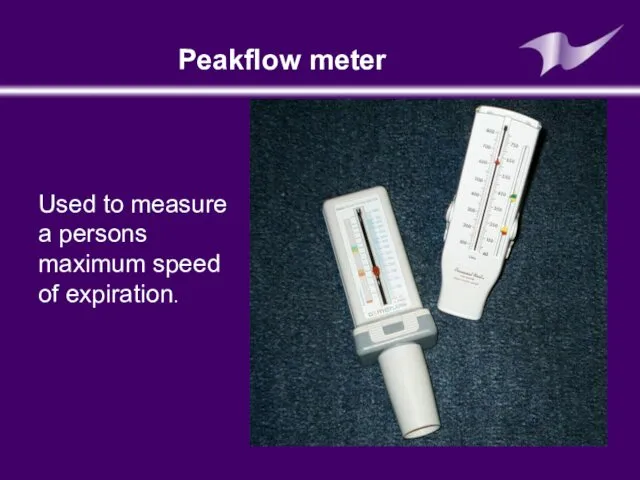
Peakflow meter
Used to measure a persons maximum speed of expiration.
Peakflow meter
Used to measure a persons maximum speed of expiration.
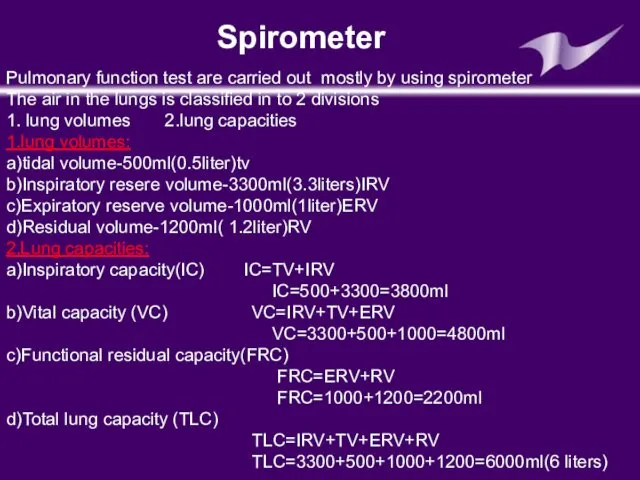
Pulmonary function test are carried out mostly by using spirometer
The air
Pulmonary function test are carried out mostly by using spirometer The air
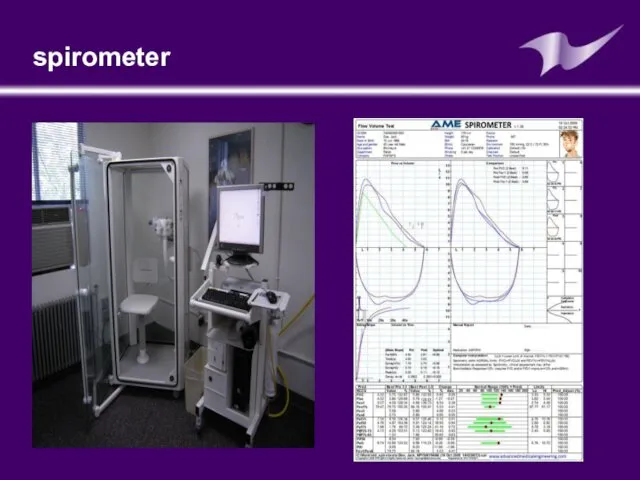
spirometer
spirometer
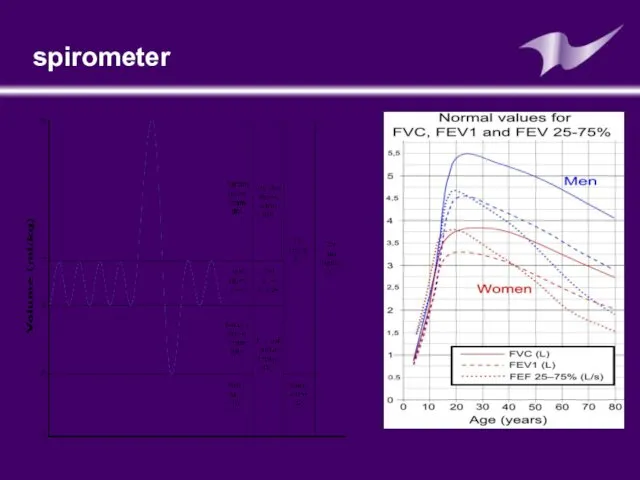
spirometer
spirometer
Late diagnostics of bronchial asthma
Complicate bronchial asthma course prognosis
Worsen life quality
Late diagnostics of bronchial asthma
Complicate bronchial asthma course prognosis
Worsen life quality
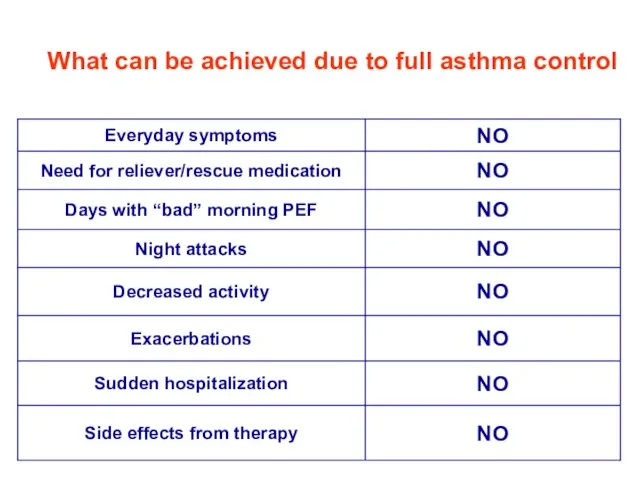
What can be achieved due to full asthma control
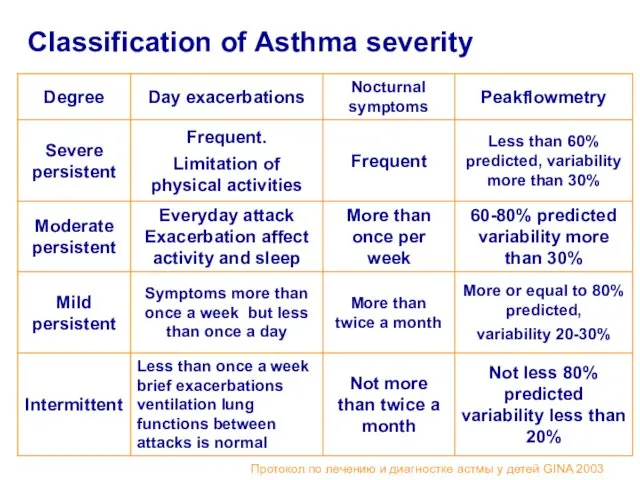
Classification of Asthma severity
Протокол по лечению и диагностке астмы у детей
Classification of Asthma severity
Протокол по лечению и диагностке астмы у детей
The goal of asthma treatment is to achieve and maintain clinical
The goal of asthma treatment is to achieve and maintain clinical
Step approach of BA treatment means increasing of medication according to
Step approach of BA treatment means increasing of medication according to
BA treatment in acute period:
Termination of the contact with allergen
Oxygen therapy
Inhaled
BA treatment in acute period:
Termination of the contact with allergen
Oxygen therapy
Inhaled
Medications for basic BA therapy
Cromoglycium acid derivates
Glucocorticosteroids (systemic, inhaled)
Long acting inhaled
Medications for basic BA therapy
Cromoglycium acid derivates
Glucocorticosteroids (systemic, inhaled)
Long acting inhaled
Antiinflammatory medications- derivates of cromoglycium acid
Inhibit mast cells degranulation process
Retard IgE-
Antiinflammatory medications- derivates of cromoglycium acid
Inhibit mast cells degranulation process
Retard IgE-
Derivates of cromoglycium acid
Mast cells membranes stabilizers: cromoglycium acid (intal,chromohexal,chromogenum)
Nedocromyl sodium
Derivates of cromoglycium acid
Mast cells membranes stabilizers: cromoglycium acid (intal,chromohexal,chromogenum)
Nedocromyl sodium
Inhaled corticosteroids
Inhaled corticosteroids (ICS) has the most manifested anti-inflammatory activity
Reduce BA
Inhaled corticosteroids
Inhaled corticosteroids (ICS) has the most manifested anti-inflammatory activity
Reduce BA
Systemic corticosteroids (hydrocortisone,dexamethasone, methylprednisolone, prednisolone, polcortolone)
Inhaled corticosteroids
Beclomethasone (becodisk, becotide, aldecine )
Fluticasone
Systemic corticosteroids (hydrocortisone,dexamethasone, methylprednisolone, prednisolone, polcortolone)
Inhaled corticosteroids
Beclomethasone (becodisk, becotide, aldecine )
Fluticasone
Leukotriene modifiers
Acolad (Zaferlucast)
Singular (Montelucast)
Leukotriene modifiers
Acolad (Zaferlucast)
Singular (Montelucast)
Long acting b-2-agonistsагонисты:
Salmeterol (Serevent,Serevent rotadisk)
Clenbutirole (Spiropent)
Formoterol (Formoteroloxis, Foradil)
Long acting b-2-agonistsагонисты:
Salmeterol (Serevent,Serevent rotadisk)
Clenbutirole (Spiropent)
Formoterol (Formoteroloxis, Foradil)

Reliever Medications
Broncholytic medications (bronchospasmolytics)
Short acting b –adrenomymetics
Salbutamol ( ventolin- nebulas,ventolin, bolmax,
Reliever Medications
Broncholytic medications (bronchospasmolytics)
Short acting b –adrenomymetics
Salbutamol ( ventolin- nebulas,ventolin, bolmax,

Reliever Medication
Methylxantines
(euphylline, theophylline)
M-cholynoblockers
- Ipratropium bromide (Atrovent)
Reliever Medication
Methylxantines
(euphylline, theophylline)
M-cholynoblockers
- Ipratropium bromide (Atrovent)
Combined medications:
Phenoterol + Ipratropium bromide = berodual
Salbutamol + Ipratropium bromide =
Combined medications:
Phenoterol + Ipratropium bromide = berodual
Salbutamol + Ipratropium bromide =
Medications for Nebulizer therapy
Nebulizer – is inhalation device for spraying aerosol
Medications for Nebulizer therapy
Nebulizer – is inhalation device for spraying aerosol
The main goal of nebulizer therapy
Delivering of medication therapeutic dosage in
The main goal of nebulizer therapy
Delivering of medication therapeutic dosage in
Indications for nebulizer therapy
It is used for intensive care in obstructive
Indications for nebulizer therapy
It is used for intensive care in obstructive
Advantages of nebulizer treatment
It isn’t necessary coordinate respiratory with aerosole puffs
Possibility
Advantages of nebulizer treatment
It isn’t necessary coordinate respiratory with aerosole puffs
Possibility
Medications for nebulizer therapy
Ventolin ( in nebulas 2,5 ml/2,5 mg
Medications for nebulizer therapy
Ventolin ( in nebulas 2,5 ml/2,5 mg
Allergen specific immunotherapy
Nowadays this method is the most effective treatment because
Allergen specific immunotherapy
Nowadays this method is the most effective treatment because
To decrease efficacy of BA therapy
Educational programs ( for affected children
To decrease efficacy of BA therapy
Educational programs ( for affected children
Key statements of BA treatment
The most efficient BA treatment is causative
Key statements of BA treatment
The most efficient BA treatment is causative
 Дискинезии желчевыводящих путей у детей
Дискинезии желчевыводящих путей у детей Врожденные аномалии роговицы
Врожденные аномалии роговицы Рак шейки матки
Рак шейки матки Эхинококкоз
Эхинококкоз Электроэнцефалография: применение в практике
Электроэнцефалография: применение в практике Противоаллергические ЛС, иммунотропные ЛС, биостимуляторы
Противоаллергические ЛС, иммунотропные ЛС, биостимуляторы Влияние алкоголя на ребенка в период беременности
Влияние алкоголя на ребенка в период беременности Патологиялық анатомия
Патологиялық анатомия Медицинское страхование
Медицинское страхование Атрезия пищевода и пилоростеноз
Атрезия пищевода и пилоростеноз Роль кожи в терморегуляции. Гигиена кожи
Роль кожи в терморегуляции. Гигиена кожи Несостоятельность тазового дна
Несостоятельность тазового дна Синдром раздражённого кишечника
Синдром раздражённого кишечника Возбудители пищевых интоксикаций
Возбудители пищевых интоксикаций Медико-демографические показатели населения Горноуральского городского округа
Медико-демографические показатели населения Горноуральского городского округа Телекоммуникационные системы в медицине. (Лекция 7)
Телекоммуникационные системы в медицине. (Лекция 7) Кардиогенный шок и его причины
Кардиогенный шок и его причины Митральный стеноз
Митральный стеноз Санитарно-гигиенические обработка больных
Санитарно-гигиенические обработка больных Рецепт: структура, правила выписывания и отпуска лекарственных средств
Рецепт: структура, правила выписывания и отпуска лекарственных средств ДВС-синдром (диссеминированное внутрисосудистое свёртывание) у беременных. Геморагический шок. Эмболия околоплодными водами
ДВС-синдром (диссеминированное внутрисосудистое свёртывание) у беременных. Геморагический шок. Эмболия околоплодными водами Инструментальные методы исследования в работе врача общей практики (семейного врача). Электрокардиография. Нормальная ЭКГ
Инструментальные методы исследования в работе врача общей практики (семейного врача). Электрокардиография. Нормальная ЭКГ Болезни и травмы органов дыхания
Болезни и травмы органов дыхания Правила предупреждения заражения глистами
Правила предупреждения заражения глистами Тромбофилия в кардиологической практике
Тромбофилия в кардиологической практике Сахарный диабет у детей
Сахарный диабет у детей Око. Будова ока
Око. Будова ока Грипп и другие острые респираторные вирусные инфекции
Грипп и другие острые респираторные вирусные инфекции