- Adrenergic agents

Содержание
- 2. Adrenergic Synapses the main mediator of sympathetic nervous system is Nоradrenaline (Norepinephrine), so sympathetic innervation is
- 3. Adrenergic synapses Adrenergic neurones are located in the CNS (locus coeruleus of midbrain, pons Varolii, medulla
- 4. Sympathetic synapses Centers of pre- gangli- onic fibers N-ChR АR
- 5. Adrenergic agents Noradrenaline is the main mediator at postganglionic sympathetic site (except sweet glands, hair follicles
- 6. Uptake of CAs After dissociation of complex “noradrenalin-adrenoceptor”, the mediator is inactivated by a few mechanisms.
- 7. NET – norepinephrine transporter
- 8. Uptake of CAs Extraneuronal uptake (uptake-2) with neuroglia, fibroblasts, cardiomyocytes, endothelial cells and myocytes of blood
- 9. Metabolism of CAs МАО (monoamine oxydase) inactivates CAs in synapse. Part of NA leaking out from
- 10. Adrenergic agents change activity of sympathetic nervous system How? There are 2 big groups: adrenergic agonists
- 11. Adrenergic receptors R. Ahlquist (1948) classified them into two types α- and β. Molecular cloning in
- 12. Adrenergic receptors α1B/1D – in blood vessels of skin, mucosa and internal organs. α1 - receptors
- 13. α – adrenoceptors: α2-adrenoreceptors can be located both on postsynaptic and on presynaptic membrane of adrenergic
- 14. α – adrenoceptors: out-synaptic (non-innervated, extrajunctional) α2-receptors they are located in blood vessels, on platelets, in
- 15. β-adrenoceptors: β1-adrenoreceptors are located on postsynaptic membrane of myocardium cells in juxtaglomerular apparatus stimulation of β1-receptors
- 16. β-adrenoreceptors: β2-adrenoceptors can be located presynaptically, postsynaptically and extrasynaptically: Extrasynaptic β2-adrenoceptors are located in Smooth muscles
- 17. β-adrenoceptors: stimulation of β2-receptors causes Bronchodilation and decrease in bronchial secretion, Inhibition of platelet aggregation Increase
- 18. β-adrenoceptors: β3-adrenoreceptors have been found on membranes of adipocytes high concentration of catecholamines excite them what
- 19. TRANSDUCER MECHANISMS OF ADRENOCEPTORS Adrenergic receptors are membrane bound G-protein coupled receptors which function primarily by
- 20. TRANSDUCER MECHANISMS OF ADRENOCEPTORS α1-receptors via G-protein are coupled to phospholipase C. Activation of membrane phospholipases
- 21. TRANSDUCER MECHANISMS OF ADRENOCEPTORS β1 receptors via Gs-proteins stimulate phosphorilation of calcium channels that leads to
- 22. CLASSIFICATION OF ADRENERGIC AGONISTS increase transmission of nerve impulse in adrenergic synapses Adrenergic agonists of direct
- 23. α-adrenergic agonists: α2- agonists: Clonidine α-Methyldopa Apraclonidine Brimonidine
- 24. CLASSIFICATION OF ADRENERGIC AGONISTS β-adrenergic agonists: β1 -β2 –adrenergic agonists: Isoprenaline Orciprenaline β2-adrenergic agonists: Salbutamol ,
- 25. CLASSIFICATION OF ADRENERGIC AGONISTS Adrenergic agonists of indirect action (indirect sympathomimetics): Ephedrine hydrochloride Phenylpropanolamine Combined preparations:
- 26. Classification of direct adrenergic agonists according to origin Cathecholamines Endogenous Dopamine Adrenaline Dopamine Exogenous Dobutamine Isoprenaline
- 27. α-,β-adrenergic agonists The main representatives: Adrenaline & Noradrenaline PHARMACOLOGICAL EFFECTS: Influence on vascular tone Noradrenaline mostly
- 28. PHARMACOLOGICAL EFFECTS OF α-,β-ADRENERGIC AGONISTS Influence on vascular tone Adrenaline takes marked stimulant action on α1-
- 29. PHARMACOLOGICAL EFFECTS OF α-,β-ADRENERGIC AGONISTS Influence on the heart Noradrenaline stimulates β1-receptors and increases myocardium contractility
- 30. PHARMACOLOGICAL EFFECTS OF α-,β-ADRENERGIC AGONISTS An influence on the heart Adrenaline takes more marked action on
- 31. PHARMACOLOGICAL EFFECTS OF α-,β-ADRENERGIC AGONISTS Influence on eye dilate pupil due to contraction of radial muscle
- 32. PHARMACOLOGICAL EFFECTS OF α-,β-ADRENERGIC AGONISTS Influence on GIT a tone and motility of g.i.t. are decreased
- 33. Indications for administration of α-,β-adrenomimetics They are used only parenterally as they are destroyed in the
- 34. Indications for administration of α-,β-adrenomimetics Adrenaline can be used for elimination of A-V block and in
- 35. Adverse effects At administration of Noradrenaline: headache respiratory disorders cardiac arrhythmia necrosis of tissues at the
- 36. α1-adrenergic agonists α1-adrenergic agonists: Phenylephrine, Midodrine stimulate α1-adrenoreceptors of blood vessels mainly these cause longer vasoconstrictive
- 37. α2-adrenergic agonists Clonidine and α-Methyldopa, Guanfacin, Guanabenz can be used for hypertension Apraclonidine and Brimonidine are
- 38. α1, α2- ADRENERGIC AGONISTS α1-,α2-adrenergic agonists: Naphazoline, Xylometazoline,etc. stimulate simultaneously synaptic α1-receptors and extrasynaptic α2- receptors
- 39. ADMINISTRATION OF α- ADRENERGIC AGONISTS α1-adrenergic agonists are used as vasoconstrictants at hypotension Phenylephrine is also
- 40. β1–, β2-adrenergic agonists Representatives: Isoprenaline (Isadrinum), Orciprenaline salfate (Alupent) have stimulant action on the heart due
- 41. Indications for administration of β1–, β2-adrenomimetics For prophylaxis and relief of bronchial asthma attacks Isoprenaline is
- 42. β1 –adrenergic agonists A representative is Dobutamine It takes vigorous inotropic action (increases contractility of myocardium
- 43. β2 –adrenergic agonists Representatives: Salbutamol, Fenoterol, Terbutaline, Salmeterol, Pirbuterol, Bambuterol they are selective stimulants of β2-adrenoreceptors
- 44. Use of β2 –adrenergic agonists they are widely used as bronchodilatory agents for relief of bronchial
- 45. Adverse effects of β-adrenomimetics anxiety palpitation tremor of fingers giddiness, headache hyperhidrosis in such cases a
- 46. ADRENERGIC AGONISTS OF INDIRECT ACTION (INDIRECT SYMPATHOMIMETICS) Representatives: Ephedrine hydrochloride and Phenylpropanolamine (Trimex) Ephedrine is an
- 47. Ephedra disthachya
- 48. INDIRECT SYMPATHOMIMETICS Ephedrine also has direct stimulant action on β- adrenoreceptors mainly it narrows vessels and
- 49. INDIRECT SYMPATHOMIMETICS Ephedrine dilates pupil (due to stimulation of α1-receptors of radial muscle) it does not
- 50. Administration of sympathomimetics in hypotension, collapse to increase ABP Pseudoephedrine is administered orally as decongestant in
- 51. Adverse effects of sympathomimetics excitement sleeplessness tremor loss of appetite increase in ABP palpitation
- 52. Combined preparations: Combined preparations are frequently used (they contain preparations with с synergetic action): BERODUAL (fenoterol
- 53. DOPAMINOMIMETICS Dopamine is the main neuromediator for dopamine receptors, which differ from α- and β-adrenoreceptors different
- 54. Pharmacological characteristics of Dopamine At dose 0.5-2.0 mcg dopamine stimulates D1-receptors in blood vessels Causes dilation
- 55. Indications for administration dopaminomimetics are used in cardiogenic or septic shock to improve the heart work
- 57. Скачать презентацию
Adrenergic Synapses
the main mediator of sympathetic nervous system is Nоradrenaline (Norepinephrine),
Adrenergic Synapses
the main mediator of sympathetic nervous system is Nоradrenaline (Norepinephrine),
Adrenergic synapses
Adrenergic neurones are located in the CNS (locus coeruleus of
Adrenergic synapses
Adrenergic neurones are located in the CNS (locus coeruleus of
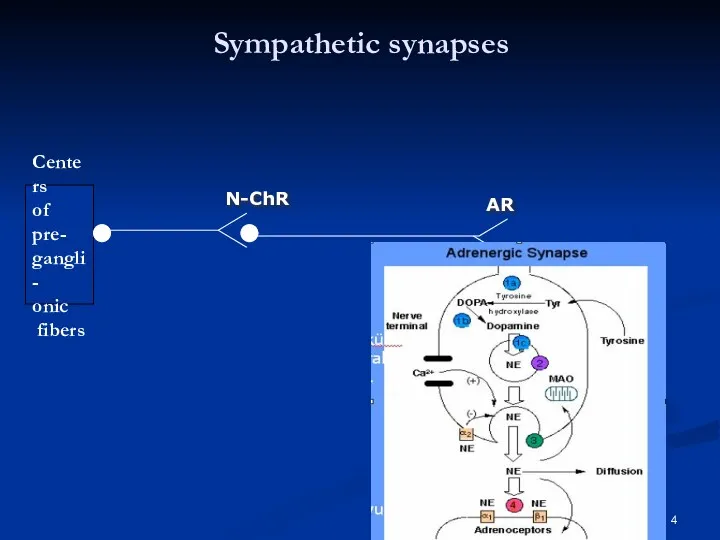
Sympathetic synapses
Centers
of pre-
gangli-
onic
fibers
N-ChR
АR
Sympathetic synapses
Centers
of pre-
gangli-
onic
fibers
N-ChR
АR
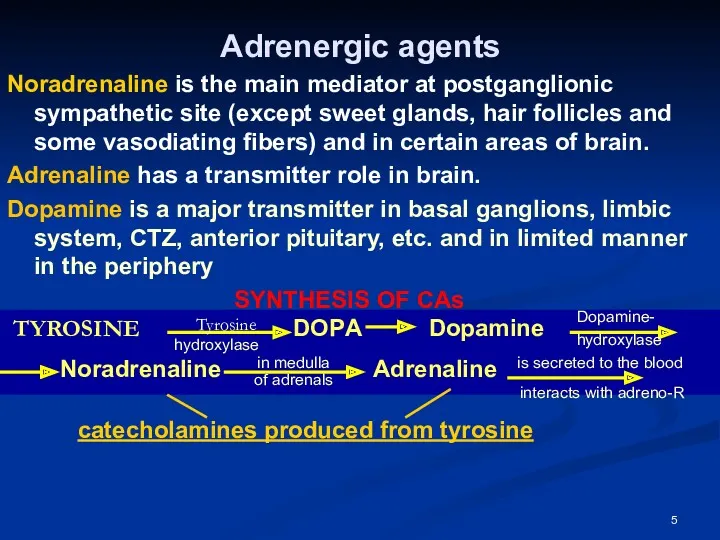
Adrenergic agents
Noradrenaline is the main mediator at postganglionic sympathetic site (except
Adrenergic agents
Noradrenaline is the main mediator at postganglionic sympathetic site (except
Uptake of CAs
After dissociation of complex “noradrenalin-adrenoceptor”, the mediator is inactivated
Uptake of CAs
After dissociation of complex “noradrenalin-adrenoceptor”, the mediator is inactivated
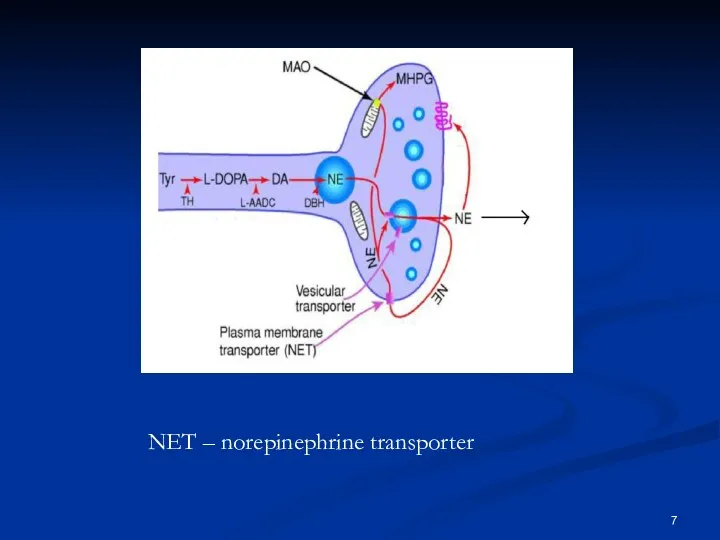
NET – norepinephrine transporter
NET – norepinephrine transporter
Uptake of CAs
Extraneuronal uptake (uptake-2) with neuroglia, fibroblasts, cardiomyocytes, endothelial cells
Uptake of CAs
Extraneuronal uptake (uptake-2) with neuroglia, fibroblasts, cardiomyocytes, endothelial cells
Metabolism of CAs
МАО (monoamine oxydase) inactivates CAs in synapse.
Part of
Metabolism of CAs
МАО (monoamine oxydase) inactivates CAs in synapse.
Part of
Adrenergic agents
change activity of sympathetic nervous system
How?
There are 2 big groups:
Adrenergic agents
change activity of sympathetic nervous system
How?
There are 2 big groups:
Adrenergic receptors
R. Ahlquist (1948) classified them into two types α-
Adrenergic receptors
R. Ahlquist (1948) classified them into two types α-
Adrenergic receptors
α1B/1D – in blood vessels of skin, mucosa and
Adrenergic receptors
α1B/1D – in blood vessels of skin, mucosa and
α – adrenoceptors:
α2-adrenoreceptors can be located both on postsynaptic and
α – adrenoceptors:
α2-adrenoreceptors can be located both on postsynaptic and
α – adrenoceptors:
out-synaptic (non-innervated, extrajunctional) α2-receptors
they are located in blood vessels,
α – adrenoceptors:
out-synaptic (non-innervated, extrajunctional) α2-receptors
they are located in blood vessels,
β-adrenoceptors:
β1-adrenoreceptors are located
on postsynaptic membrane of myocardium cells
in juxtaglomerular
β-adrenoceptors:
β1-adrenoreceptors are located
on postsynaptic membrane of myocardium cells
in juxtaglomerular
β-adrenoreceptors:
β2-adrenoceptors can be located presynaptically, postsynaptically and extrasynaptically:
Extrasynaptic β2-adrenoceptors
β-adrenoreceptors:
β2-adrenoceptors can be located presynaptically, postsynaptically and extrasynaptically:
Extrasynaptic β2-adrenoceptors
β-adrenoceptors:
stimulation of β2-receptors causes
Bronchodilation and decrease in bronchial secretion,
Inhibition of
β-adrenoceptors:
stimulation of β2-receptors causes
Bronchodilation and decrease in bronchial secretion,
Inhibition of
β-adrenoceptors:
β3-adrenoreceptors have been found on membranes of adipocytes
high concentration of
β-adrenoceptors:
β3-adrenoreceptors have been found on membranes of adipocytes
high concentration of
TRANSDUCER MECHANISMS OF ADRENOCEPTORS
Adrenergic receptors are membrane bound G-protein coupled receptors
TRANSDUCER MECHANISMS OF ADRENOCEPTORS
Adrenergic receptors are membrane bound G-protein coupled receptors
TRANSDUCER MECHANISMS OF ADRENOCEPTORS
α1-receptors via G-protein are coupled to phospholipase C.
TRANSDUCER MECHANISMS OF ADRENOCEPTORS
α1-receptors via G-protein are coupled to phospholipase C.
TRANSDUCER MECHANISMS OF ADRENOCEPTORS
β1 receptors via Gs-proteins stimulate phosphorilation of calcium
TRANSDUCER MECHANISMS OF ADRENOCEPTORS
β1 receptors via Gs-proteins stimulate phosphorilation of calcium
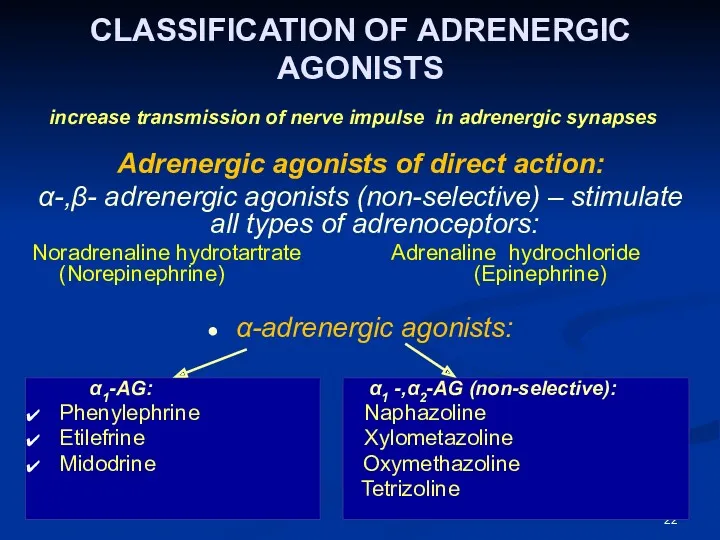
CLASSIFICATION OF ADRENERGIC AGONISTS
increase transmission of nerve impulse in adrenergic
CLASSIFICATION OF ADRENERGIC AGONISTS
increase transmission of nerve impulse in adrenergic
α-adrenergic agonists:
α2- agonists:
Clonidine
α-Methyldopa
Apraclonidine
Brimonidine
α-adrenergic agonists:
α2- agonists:
Clonidine
α-Methyldopa
Apraclonidine
Brimonidine
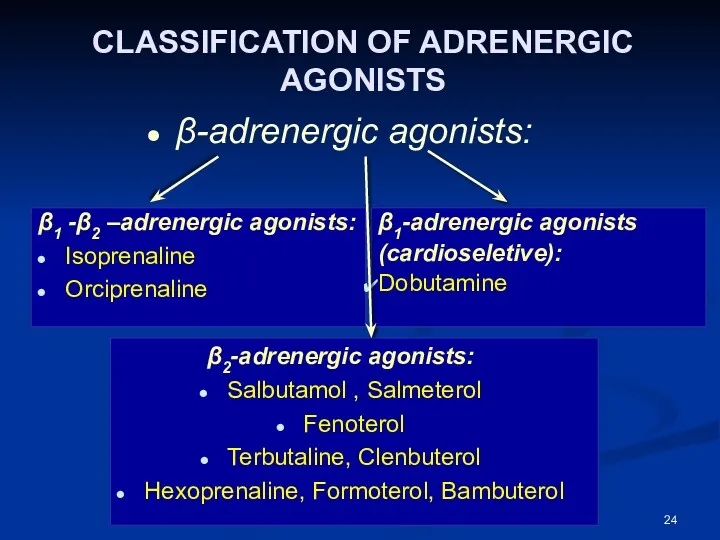
CLASSIFICATION OF ADRENERGIC AGONISTS
β-adrenergic agonists:
β1 -β2 –adrenergic agonists:
Isoprenaline
Orciprenaline
β2-adrenergic
CLASSIFICATION OF ADRENERGIC AGONISTS
β-adrenergic agonists:
β1 -β2 –adrenergic agonists:
Isoprenaline
Orciprenaline
β2-adrenergic
CLASSIFICATION OF ADRENERGIC AGONISTS
Adrenergic agonists of indirect action (indirect sympathomimetics):
Ephedrine hydrochloride
Phenylpropanolamine
Combined
CLASSIFICATION OF ADRENERGIC AGONISTS
Adrenergic agonists of indirect action (indirect sympathomimetics):
Ephedrine hydrochloride
Phenylpropanolamine
Combined
Classification of direct adrenergic agonists according to origin
Cathecholamines
Endogenous
Dopamine
Adrenaline
Dopamine
Exogenous
Dobutamine
Isoprenaline
Non-cathecholamines
Classification of direct adrenergic agonists according to origin
Cathecholamines
Endogenous
Dopamine
Adrenaline
Dopamine
Exogenous
Dobutamine
Isoprenaline
Non-cathecholamines
α-,β-adrenergic agonists
The main representatives:
Adrenaline & Noradrenaline
PHARMACOLOGICAL EFFECTS:
Influence on vascular
α-,β-adrenergic agonists
The main representatives:
Adrenaline & Noradrenaline
PHARMACOLOGICAL EFFECTS:
Influence on vascular
PHARMACOLOGICAL EFFECTS OF
α-,β-ADRENERGIC AGONISTS
Influence on vascular tone
Adrenaline takes
PHARMACOLOGICAL EFFECTS OF
α-,β-ADRENERGIC AGONISTS
Influence on vascular tone
Adrenaline takes
PHARMACOLOGICAL EFFECTS OF
α-,β-ADRENERGIC AGONISTS
Influence on the heart
Noradrenaline stimulates
PHARMACOLOGICAL EFFECTS OF
α-,β-ADRENERGIC AGONISTS
Influence on the heart
Noradrenaline stimulates
PHARMACOLOGICAL EFFECTS OF
α-,β-ADRENERGIC AGONISTS
An influence on the heart
Adrenaline takes
PHARMACOLOGICAL EFFECTS OF
α-,β-ADRENERGIC AGONISTS
An influence on the heart
Adrenaline takes
PHARMACOLOGICAL EFFECTS OF
α-,β-ADRENERGIC AGONISTS
Influence on eye
dilate pupil due to
PHARMACOLOGICAL EFFECTS OF
α-,β-ADRENERGIC AGONISTS
Influence on eye
dilate pupil due to
PHARMACOLOGICAL EFFECTS OF
α-,β-ADRENERGIC AGONISTS
Influence on GIT
a tone and motility of
PHARMACOLOGICAL EFFECTS OF
α-,β-ADRENERGIC AGONISTS
Influence on GIT
a tone and motility of
Indications for administration of
α-,β-adrenomimetics
They are used only parenterally as
Indications for administration of
α-,β-adrenomimetics
They are used only parenterally as
Indications for administration of
α-,β-adrenomimetics
Adrenaline can be used for elimination of
Indications for administration of
α-,β-adrenomimetics
Adrenaline can be used for elimination of
Adverse effects
At administration of Noradrenaline:
headache
respiratory disorders
cardiac arrhythmia
necrosis of tissues at
Adverse effects
At administration of Noradrenaline:
headache
respiratory disorders
cardiac arrhythmia
necrosis of tissues at
α1-adrenergic agonists
α1-adrenergic agonists:
Phenylephrine, Midodrine stimulate α1-adrenoreceptors of blood vessels mainly
these
α1-adrenergic agonists
α1-adrenergic agonists:
Phenylephrine, Midodrine stimulate α1-adrenoreceptors of blood vessels mainly
these
α2-adrenergic agonists
Clonidine and α-Methyldopa, Guanfacin, Guanabenz can be used for hypertension
α2-adrenergic agonists
Clonidine and α-Methyldopa, Guanfacin, Guanabenz can be used for hypertension
α1, α2- ADRENERGIC AGONISTS
α1-,α2-adrenergic agonists:
Naphazoline, Xylometazoline,etc. stimulate simultaneously synaptic α1-receptors
α1, α2- ADRENERGIC AGONISTS
α1-,α2-adrenergic agonists:
Naphazoline, Xylometazoline,etc. stimulate simultaneously synaptic α1-receptors
ADMINISTRATION OF α- ADRENERGIC AGONISTS
α1-adrenergic agonists are used as vasoconstrictants at
ADMINISTRATION OF α- ADRENERGIC AGONISTS
α1-adrenergic agonists are used as vasoconstrictants at
β1–, β2-adrenergic agonists
Representatives: Isoprenaline (Isadrinum),
Orciprenaline salfate (Alupent)
have stimulant
β1–, β2-adrenergic agonists
Representatives: Isoprenaline (Isadrinum),
Orciprenaline salfate (Alupent)
have stimulant
Indications for administration of
β1–, β2-adrenomimetics
For prophylaxis and relief of
Indications for administration of
β1–, β2-adrenomimetics
For prophylaxis and relief of
β1 –adrenergic agonists
A representative is Dobutamine
It takes vigorous inotropic action
β1 –adrenergic agonists
A representative is Dobutamine
It takes vigorous inotropic action
β2 –adrenergic agonists
Representatives: Salbutamol, Fenoterol, Terbutaline, Salmeterol, Pirbuterol, Bambuterol
they are
β2 –adrenergic agonists
Representatives: Salbutamol, Fenoterol, Terbutaline, Salmeterol, Pirbuterol, Bambuterol
they are
Use of β2 –adrenergic agonists
they are widely used as bronchodilatory agents
Use of β2 –adrenergic agonists
they are widely used as bronchodilatory agents
Adverse effects of
β-adrenomimetics
anxiety
palpitation
tremor of fingers
giddiness, headache
hyperhidrosis
in such cases a
Adverse effects of
β-adrenomimetics
anxiety
palpitation
tremor of fingers
giddiness, headache
hyperhidrosis
in such cases a
ADRENERGIC AGONISTS OF INDIRECT ACTION (INDIRECT SYMPATHOMIMETICS)
Representatives: Ephedrine hydrochloride and
ADRENERGIC AGONISTS OF INDIRECT ACTION (INDIRECT SYMPATHOMIMETICS)
Representatives: Ephedrine hydrochloride and
Ephedra disthachya
Ephedra disthachya
INDIRECT SYMPATHOMIMETICS
Ephedrine also has direct stimulant action on β- adrenoreceptors mainly
it
INDIRECT SYMPATHOMIMETICS
Ephedrine also has direct stimulant action on β- adrenoreceptors mainly
it
INDIRECT SYMPATHOMIMETICS
Ephedrine dilates pupil (due to stimulation of α1-receptors of radial
INDIRECT SYMPATHOMIMETICS
Ephedrine dilates pupil (due to stimulation of α1-receptors of radial
Administration of sympathomimetics
in hypotension, collapse to increase ABP
Pseudoephedrine is administered
Administration of sympathomimetics
in hypotension, collapse to increase ABP
Pseudoephedrine is administered
Adverse effects of sympathomimetics
excitement
sleeplessness
tremor
loss of appetite
increase in ABP
palpitation
Adverse effects of sympathomimetics
excitement
sleeplessness
tremor
loss of appetite
increase in ABP
palpitation
Combined preparations:
Combined preparations are frequently used
(they contain preparations with с
Combined preparations:
Combined preparations are frequently used
(they contain preparations with с
DOPAMINOMIMETICS
Dopamine is the main neuromediator for dopamine receptors, which differ
DOPAMINOMIMETICS
Dopamine is the main neuromediator for dopamine receptors, which differ
Pharmacological characteristics of Dopamine
At dose 0.5-2.0 mcg dopamine stimulates D1-receptors
Pharmacological characteristics of Dopamine
At dose 0.5-2.0 mcg dopamine stimulates D1-receptors
Indications for administration
dopaminomimetics are used in cardiogenic or septic shock
Indications for administration
dopaminomimetics are used in cardiogenic or septic shock
 Профилактическая медицина
Профилактическая медицина Боль и обезболивание
Боль и обезболивание Егде жастағы және қарт адамдардың тамақтануы
Егде жастағы және қарт адамдардың тамақтануы Улучшение качества медицинской помощи на основе информационных технологий
Улучшение качества медицинской помощи на основе информационных технологий Жапонияның денсаулық сақтау жүйесі
Жапонияның денсаулық сақтау жүйесі Налоги и налогообложение в здравоохранении
Налоги и налогообложение в здравоохранении Гнойно-воспалительные заболевания мягких тканей у детей
Гнойно-воспалительные заболевания мягких тканей у детей Кариес зубов. Причины и механизм образования. Основные теории и гипотезы кариеса (Миллер, Лукомский, Энтин, Шарпенак, Боровский)
Кариес зубов. Причины и механизм образования. Основные теории и гипотезы кариеса (Миллер, Лукомский, Энтин, Шарпенак, Боровский) Дифференциальная диагностика при легочных инфильтратах. Принципы лечения
Дифференциальная диагностика при легочных инфильтратах. Принципы лечения Коронавирус 2019-nCoV
Коронавирус 2019-nCoV Металло керамикалық сауыт дайындаудың бірінші лабораториялық кезеңінде қолданылатын құрал саймандар мен апараттар
Металло керамикалық сауыт дайындаудың бірінші лабораториялық кезеңінде қолданылатын құрал саймандар мен апараттар Доброкачественные органоспецифические опухоли челюстей, лица, шеи
Доброкачественные органоспецифические опухоли челюстей, лица, шеи Fizika kafedrasi
Fizika kafedrasi Невроз. Психотравма высшей нервной деятельности с конфликтом в ценостеях, ориентации, отношениях
Невроз. Психотравма высшей нервной деятельности с конфликтом в ценостеях, ориентации, отношениях Қазіргі кездегі өнеркәсіптік қала тұрғындарының денсаулығы
Қазіргі кездегі өнеркәсіптік қала тұрғындарының денсаулығы Ішек өтімсіздігі (инвагинация)
Ішек өтімсіздігі (инвагинация) СПИД – что это такое?
СПИД – что это такое? Течение и ведение послеродового периода. Становление лактации. Послеродовая контрацепция
Течение и ведение послеродового периода. Становление лактации. Послеродовая контрацепция Oral cavity
Oral cavity Malignant Melanoma
Malignant Melanoma Вещества, влияющие на эфферентную иннервацию. Адренергические средства
Вещества, влияющие на эфферентную иннервацию. Адренергические средства Основы здорового образа жизни студентов
Основы здорового образа жизни студентов Болезни желчного пузыря и желчевыводящих путей. Желчно-каменная болезнь. Хронический панкреатит
Болезни желчного пузыря и желчевыводящих путей. Желчно-каменная болезнь. Хронический панкреатит Неоадъювантное лечение II-III стадии HER2-положительного рака молочной железы
Неоадъювантное лечение II-III стадии HER2-положительного рака молочной железы Туберкулинодиагностика
Туберкулинодиагностика Тромболитики. Механизм действия
Тромболитики. Механизм действия Стахиботриотоксикоз
Стахиботриотоксикоз Защита медицинского персонала от ВБИ
Защита медицинского персонала от ВБИ