- Appendectomy By Mohan Krishna Redlapalle

Содержание
- 2. Outline Let us revise vermiform Appendix Definition of Appendectomy Indications Types Open Appendectomy Laparoscopic (Key hole)
- 3. The appendix The vermiform or worm like appendix, arising from the posteromedial wall of the caecum,
- 4. Positions The appendix lies in the right iliac fossa. Although the base of the appendix is
- 5. Peritoneal relations The appendix is suspended by a small, triangular fold of peritoneum, called the mesoappendix,
- 6. Arterial blood supply
- 7. Venous blood supply
- 8. Nerve supply Sympathetic nerves are derived from segments T9 to T10 through the celiac plexus. Parasympathetic
- 9. Now, What is Appendectomy?
- 10. What is an Appendectomy? An appendectomy, also termed appendicectomy, is a surgical operation in which the
- 11. Types of Appendectomy Open Laparoscopic General anesthesia. Laparoscopic: nasogastric tube & empty bladder. Palpation for mass
- 12. INDICATIONS Acute appendicitis Recurrent appendicitis, Stump Appendicitis As Interval appendectomy after drainage of abscess or in
- 13. Contraindications Extensive adhesions Radiation or immunosuppressive therapy, severe portal hypertension Gross coagulopathies. Laparoscopic appendectomy is contraindicated
- 14. If an acutely inflamed appendix had been found and removed, the rest of the abdomen does
- 15. Open Appendectomy (Conventional)- An overview Under general anesthesia, skin is incised. Two layers of superficial fascia
- 16. Special circumstances: -Edema of the cecal wall. -Base of the app. severely inflamed. -Gangrenous app. base.
- 17. PRE-OP PREPARATION INVESTIGATION Urinalysis- exclude infection Full blood count- leukocytosis Ultrasound scan – non compressible diameter
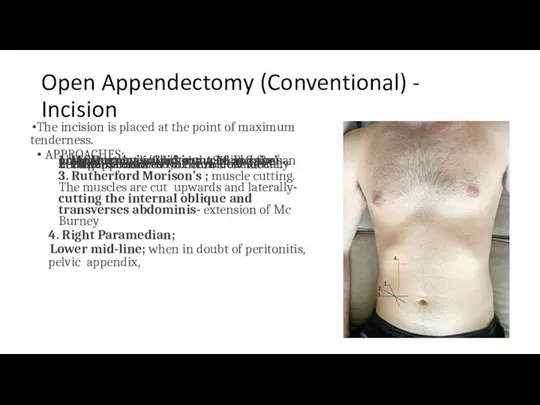
- 18. Open Appendectomy (Conventional) - Incision The incision is placed at the point of maximum tenderness. APPROACHES;
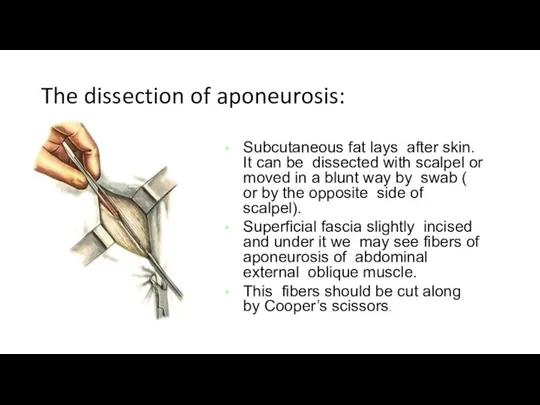
- 19. The dissection of aponeurosis: Subcutaneous fat lays after skin. It can be dissected with scalpel or
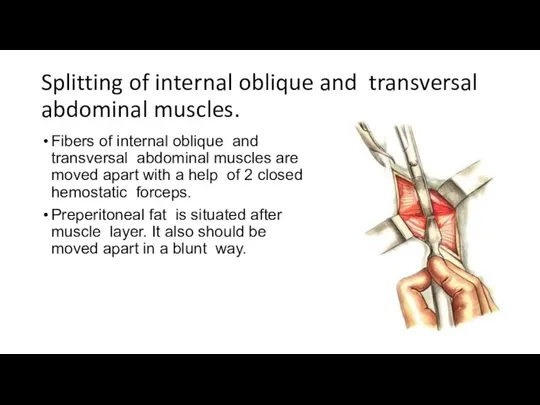
- 20. Splitting of internal oblique and transversal abdominal muscles. Fibers of internal oblique and transversal abdominal muscles
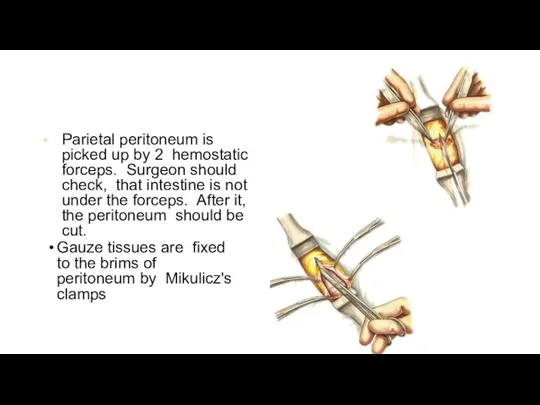
- 21. Parietal peritoneum is picked up by 2 hemostatic forceps. Surgeon should check, that intestine is not
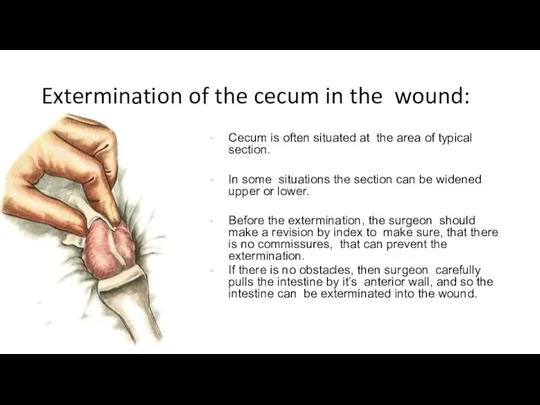
- 22. Extermination of the cecum in the wound: Cecum is often situated at the area of typical
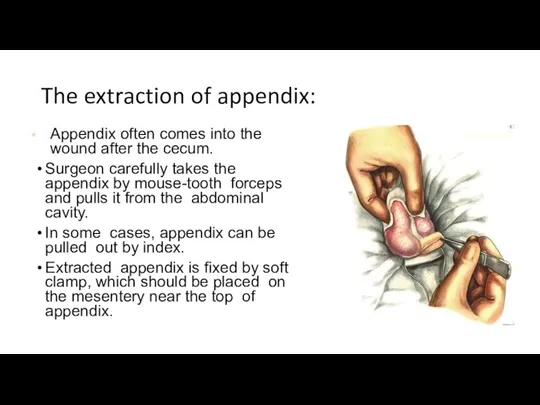
- 23. The extraction of appendix: Appendix often comes into the wound after the cecum. Surgeon carefully takes
- 24. Methods of appendectomy Antegrade (in the case of mobile cecum) Retrograde (in the case of immobile
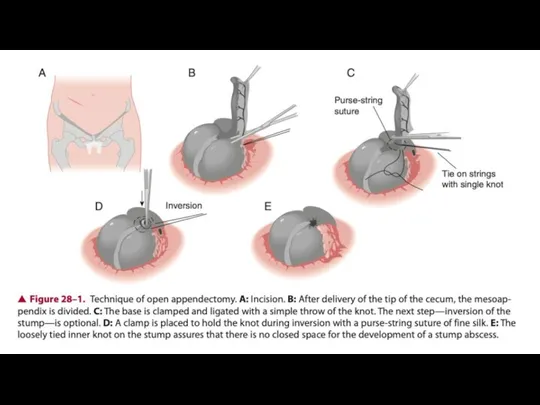
- 25. Anterograde Open Appendectomy
- 26. Bandaging of the appendix’s mesentery: The mesentery is bandaged by thick silk or catgut thread near
- 27. Putting in a purse-string suture: A seromuscular purse-string suture is put on the cecum at the
- 28. Bandaging of the appendix: Surgeon puts 2 clamps near the base of appendix and removes one
- 29. Cutting of the appendix Appendix is cut between the ligature and another clamp. The stump of
- 30. Dipping of the stump into the purse-string suture
- 31. Putting in a Z-shaped suture Sometimes a seromuscular Z-shaped suture is put over the purse-string suture
- 33. Retrograde Open Appendectomy
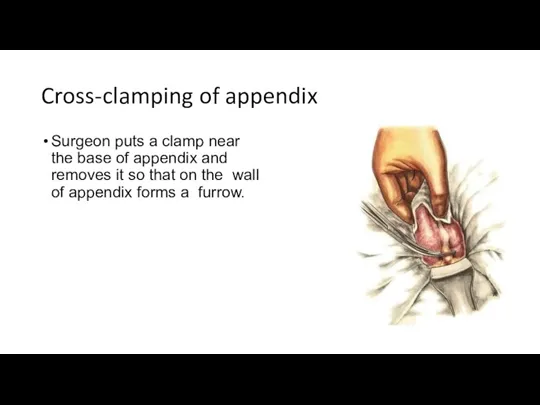
- 34. Cross-clamping of appendix Surgeon puts a clamp near the base of appendix and removes it so
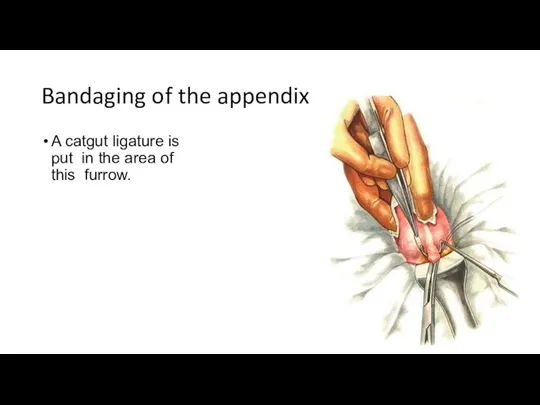
- 35. Bandaging of the appendix A catgut ligature is put in the area of this furrow.
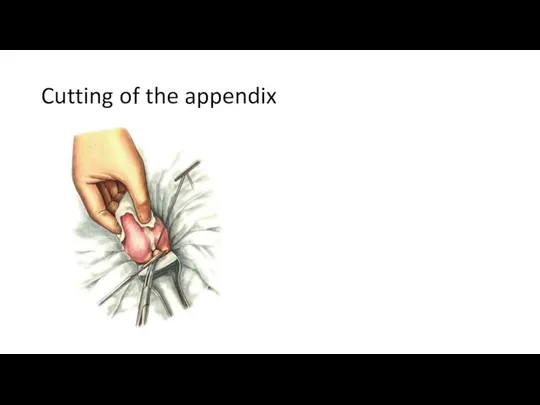
- 36. Cutting of the appendix
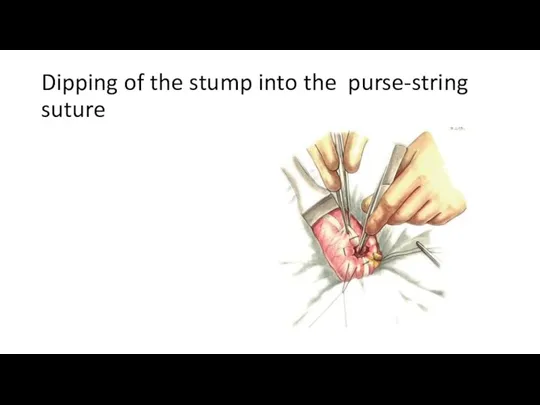
- 37. Dipping of the stump into the purse-string suture
- 38. Cutting of the appendix’s mesentery between the hemostatic clamps a surgeon starts a bandaging of mesentery,
- 39. Sewing and bandaging of the mesentery
- 40. Putting in a Z-shaped suture Sometimes a seromuscular Z-shaped suture is put over the purse-string suture
- 41. Appendectomy. Retroperitoneal position of appendix If there is no commissures in the abdominal cavity and the
- 42. The section line of parietal peritoneum: Surgeon cuts the parietal peritoneum for a distance of 10-
- 43. Bringing of gauze handle under the base of appendix: Cecum should be moved inside, founding the
- 44. Ligation of appendix vessels:
- 45. Cutting of the appendix: Appendix is cut under the clamp
- 46. Dipping the stump of appendix. Appendix stump is dipped in the purse- string suture
- 47. Sewing of parietal peritoneum: After moving off the appendix the intestine is laid back and the
- 48. CLOSURE The peritoneum is grasped with curved Kelly clamps and approximated with 3-0 continuous absorbable sutures.
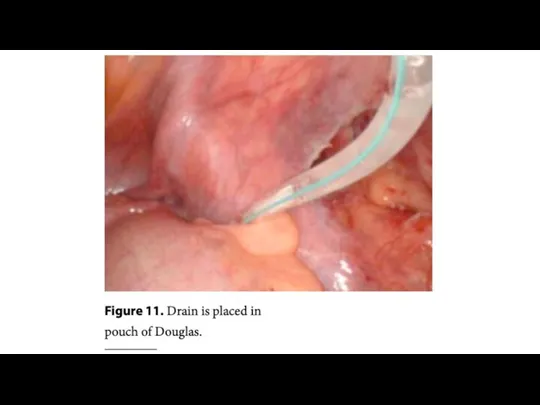
- 49. The final stage: After moving out the appendix cecum moves back in the abdominal cavity. Surgeon
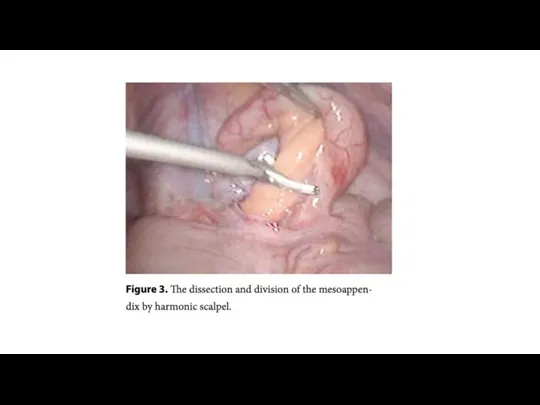
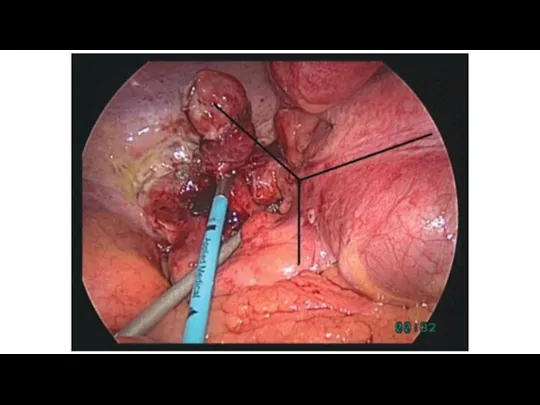
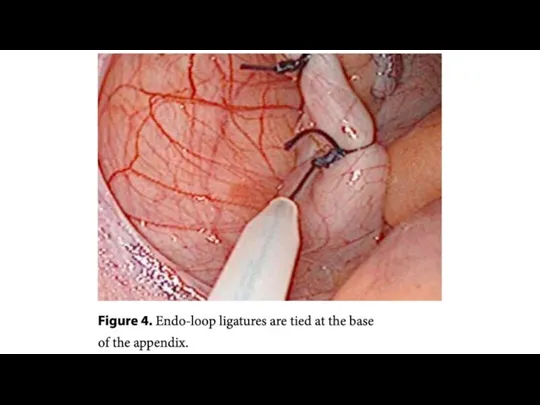
- 51. Nowadays, laparoscopic appendectomy becomes very popular. This variant is considered to be less traumatically, but not
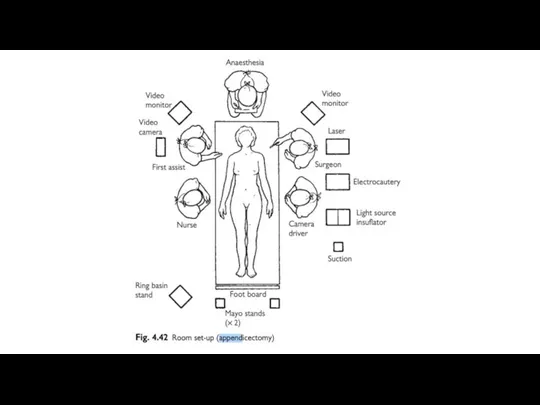
- 52. The Set up – position of the patient and the surgical team Place the patient in
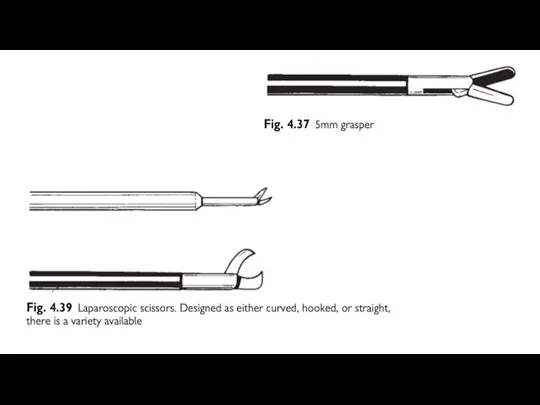
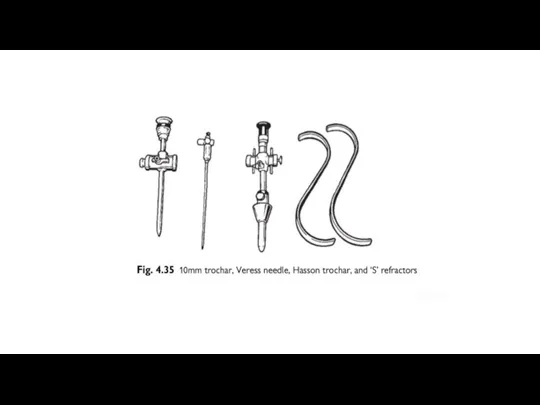
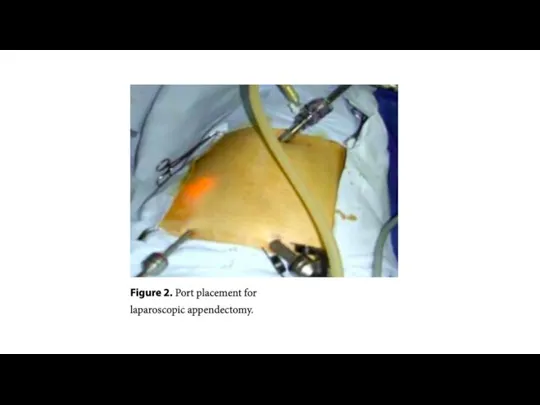
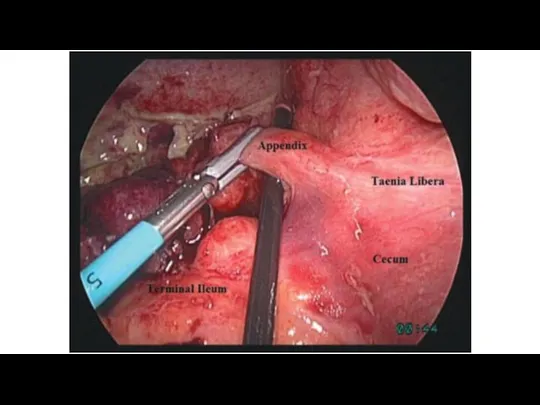
- 53. Position of trocars and instruments
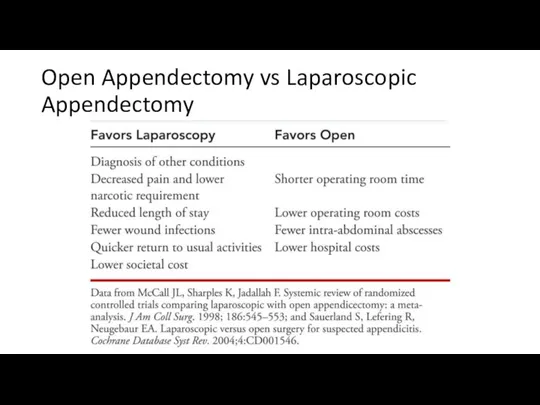
- 72. Open Appendectomy vs Laparoscopic Appendectomy
- 73. POST-OP MANAGEMENT In uncomplicated case, antibiotics should be continued up to 24 hours post-operatively ,oral fluid
- 74. Post operative Complications Wound infection (Most common) 5-10% of patient 4-5th day Intra- abdominal abscess -8%
- 75. Alternative Methods of Appendectomy Laparoscopic Single-Incision Appendectomy Natural orifice transluminal endoscopic surgery (NOTES)
- 76. Laparoscopic Single-Incision Appendectomy With laparoscopic single-incision appendectomy, the patient is prepared similarly to laparoscopic appendectomy. Under
- 77. Natural Orifice Transluminal Endoscopic Surgery Natural orifice transluminal endoscopic surgery (NOTES) is a new surgical procedure
- 78. REFERENCES Schwartz's Principles of Surgery ;Textbook by F. Charles Brunicardi and Seymour I. Schwartz SRB's Manual
- 80. Скачать презентацию
Outline
Let us revise vermiform Appendix
Definition of Appendectomy
Indications
Types
Open Appendectomy
Laparoscopic (Key hole) Appendectomy
Complications
References
Outline
Let us revise vermiform Appendix
Definition of Appendectomy
Indications
Types
Open Appendectomy
Laparoscopic (Key hole) Appendectomy
Complications
References
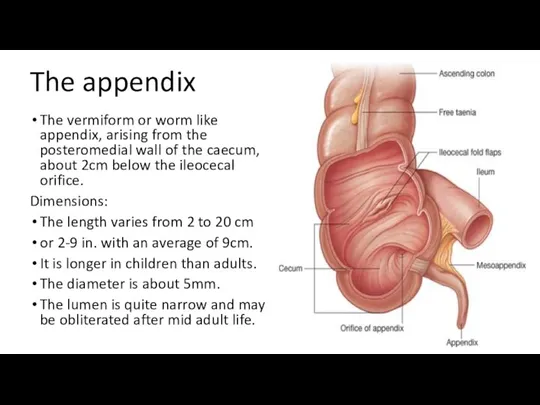
The appendix
The vermiform or worm like appendix, arising from the
The appendix
The vermiform or worm like appendix, arising from the
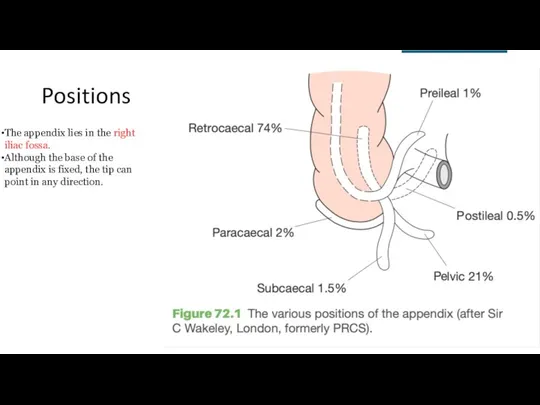
Positions
The appendix lies in the right iliac fossa.
Although the base of
Positions
The appendix lies in the right iliac fossa.
Although the base of
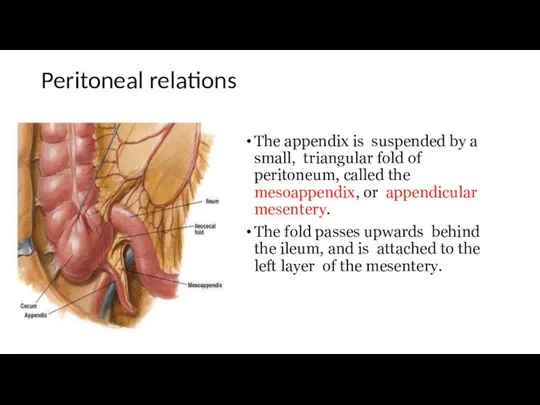
Peritoneal relations
The appendix is suspended by a small, triangular fold of
Peritoneal relations
The appendix is suspended by a small, triangular fold of
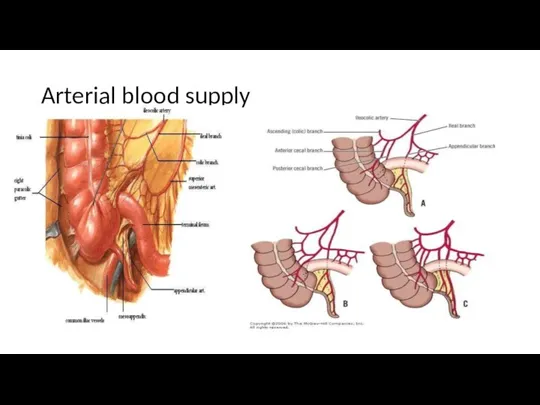
Arterial blood supply
Arterial blood supply
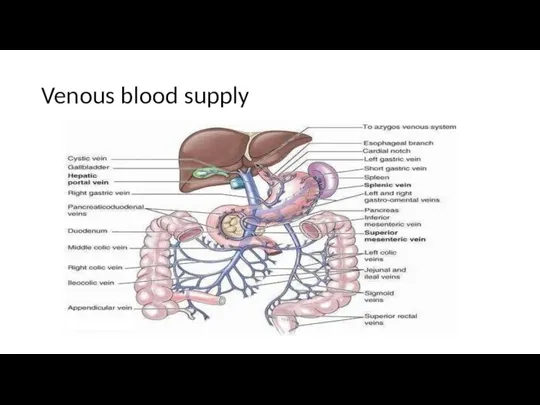
Venous blood supply
Venous blood supply
Nerve supply
Sympathetic nerves are derived from segments T9 to T10 through
Nerve supply
Sympathetic nerves are derived from segments T9 to T10 through
Now,
What is Appendectomy?
Now,
What is Appendectomy?
What is an Appendectomy?
An appendectomy, also termed appendicectomy, is a surgical
What is an Appendectomy?
An appendectomy, also termed appendicectomy, is a surgical
Types of Appendectomy
Open
Laparoscopic
General anesthesia.
Laparoscopic: nasogastric tube & empty bladder.
Palpation
Types of Appendectomy
Open
Laparoscopic
General anesthesia.
Laparoscopic: nasogastric tube & empty bladder.
Palpation
INDICATIONS
Acute appendicitis
Recurrent appendicitis, Stump Appendicitis
As Interval appendectomy after drainage of abscess
INDICATIONS
Acute appendicitis
Recurrent appendicitis, Stump Appendicitis
As Interval appendectomy after drainage of abscess
Contraindications
Extensive adhesions
Radiation or immunosuppressive therapy,
severe portal hypertension
Gross coagulopathies.
Laparoscopic appendectomy is contraindicated
Contraindications
Extensive adhesions
Radiation or immunosuppressive therapy,
severe portal hypertension
Gross coagulopathies.
Laparoscopic appendectomy is contraindicated
If an acutely inflamed appendix had been found and removed, the
If an acutely inflamed appendix had been found and removed, the
Open Appendectomy (Conventional)- An overview
Under general anesthesia, skin is incised. Two
Open Appendectomy (Conventional)- An overview
Under general anesthesia, skin is incised. Two
Special circumstances:
-Edema of the cecal wall.
-Base of the app. severely inflamed.
-Gangrenous
Special circumstances:
-Edema of the cecal wall.
-Base of the app. severely inflamed.
-Gangrenous
PRE-OP PREPARATION
INVESTIGATION
Urinalysis- exclude infection
Full blood count- leukocytosis
Ultrasound scan – non
PRE-OP PREPARATION
INVESTIGATION
Urinalysis- exclude infection
Full blood count- leukocytosis
Ultrasound scan – non
Open Appendectomy (Conventional) - Incision
The incision is placed at the point
Open Appendectomy (Conventional) - Incision
The incision is placed at the point
The dissection of aponeurosis:
Subcutaneous fat lays after skin. It can be
The dissection of aponeurosis:
Subcutaneous fat lays after skin. It can be
Splitting of internal oblique and transversal abdominal muscles.
Fibers of internal oblique
Splitting of internal oblique and transversal abdominal muscles.
Fibers of internal oblique
Parietal peritoneum is picked up by 2 hemostatic forceps. Surgeon should
Parietal peritoneum is picked up by 2 hemostatic forceps. Surgeon should
Extermination of the cecum in the wound:
Cecum is often situated at
Extermination of the cecum in the wound:
Cecum is often situated at
The extraction of appendix:
Appendix often comes into the wound after the
The extraction of appendix:
Appendix often comes into the wound after the
Methods of appendectomy
Antegrade (in the case of mobile cecum)
Retrograde (in the
Methods of appendectomy
Antegrade (in the case of mobile cecum)
Retrograde (in the
Anterograde Open Appendectomy
Anterograde Open Appendectomy
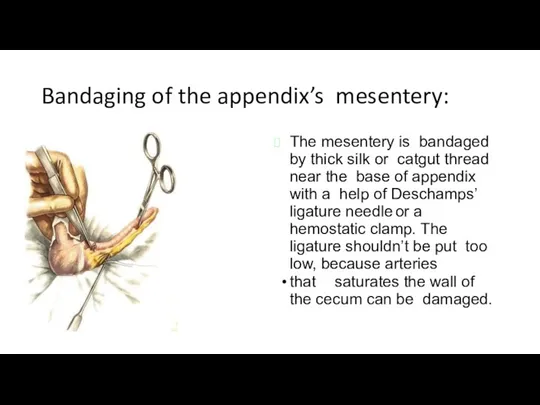
Bandaging of the appendix’s mesentery:
The mesentery is bandaged by thick silk
Bandaging of the appendix’s mesentery:
The mesentery is bandaged by thick silk
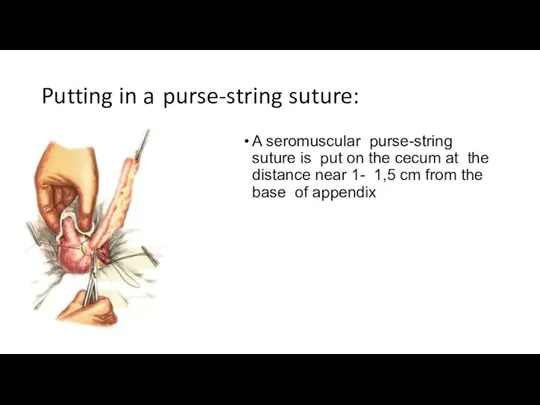
Putting in a purse-string suture:
A seromuscular purse-string suture is put on the
Putting in a purse-string suture:
A seromuscular purse-string suture is put on the
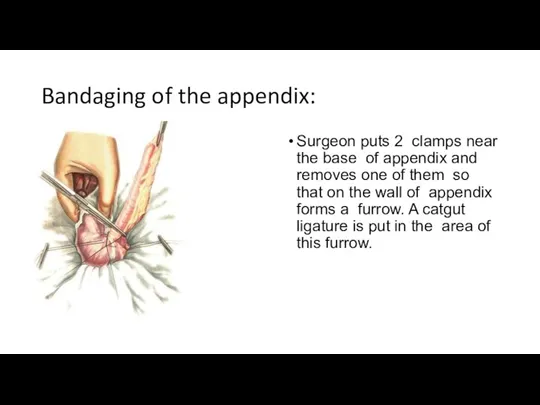
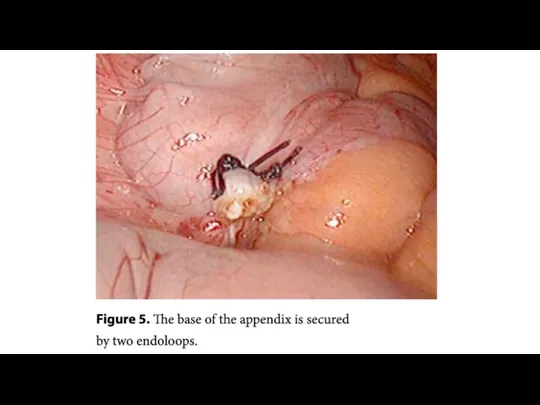
Bandaging of the appendix:
Surgeon puts 2 clamps near the base of
Bandaging of the appendix:
Surgeon puts 2 clamps near the base of
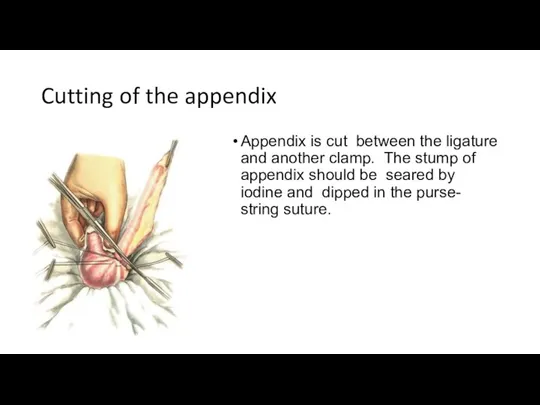
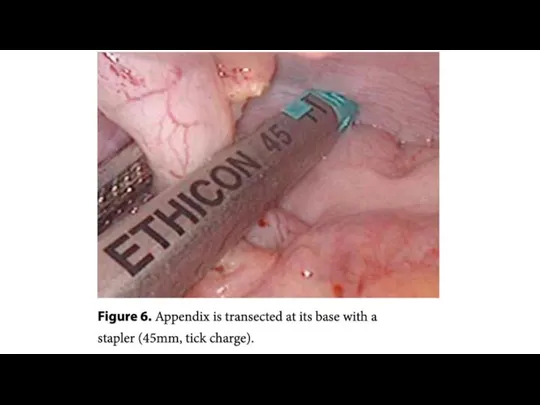
Cutting of the appendix
Appendix is cut between the ligature and another
Cutting of the appendix
Appendix is cut between the ligature and another
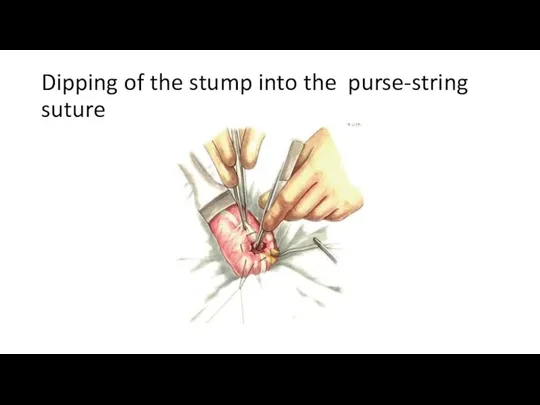
Dipping of the stump into the purse-string suture
Dipping of the stump into the purse-string suture
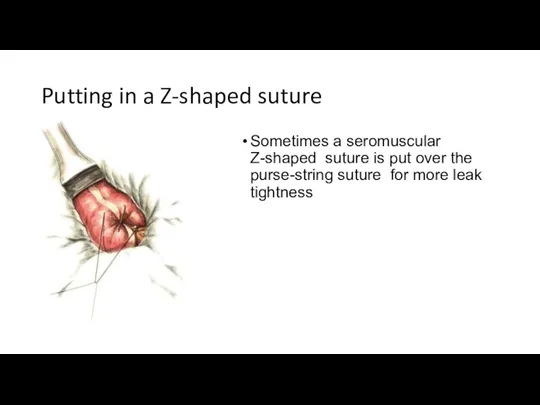
Putting in a Z-shaped suture
Sometimes a seromuscular Z-shaped suture is put
Putting in a Z-shaped suture
Sometimes a seromuscular Z-shaped suture is put
Retrograde Open Appendectomy
Retrograde Open Appendectomy
Cross-clamping of appendix
Surgeon puts a clamp near the base of appendix
Cross-clamping of appendix
Surgeon puts a clamp near the base of appendix
Bandaging of the appendix
A catgut ligature is put in the area
Bandaging of the appendix
A catgut ligature is put in the area
Cutting of the appendix
Cutting of the appendix
Dipping of the stump into the purse-string suture
Dipping of the stump into the purse-string suture
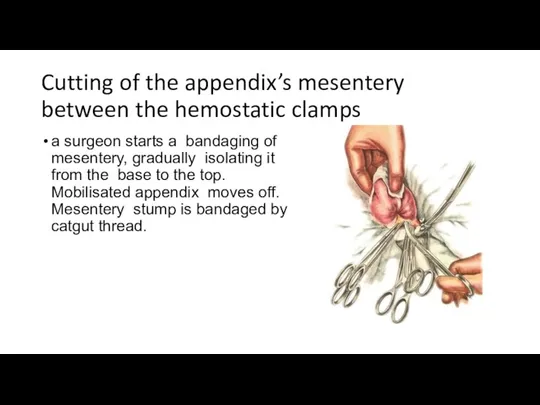
Cutting of the appendix’s mesentery between the hemostatic clamps
a surgeon starts
Cutting of the appendix’s mesentery between the hemostatic clamps
a surgeon starts
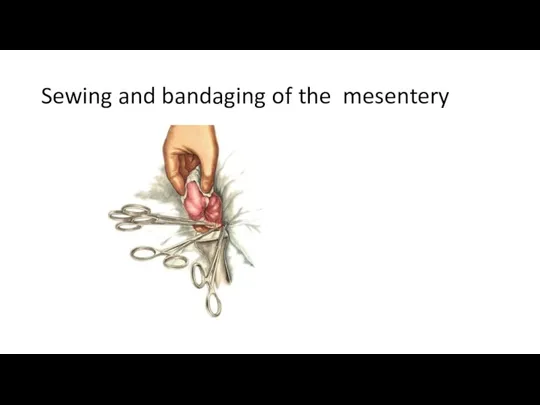
Sewing and bandaging of the mesentery
Sewing and bandaging of the mesentery
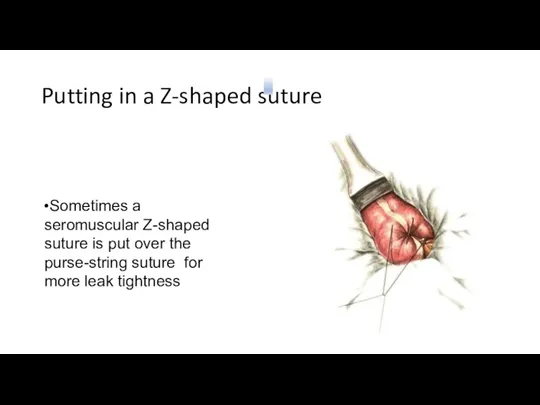
Putting in a Z-shaped suture
Sometimes a seromuscular Z-shaped suture is put
Putting in a Z-shaped suture
Sometimes a seromuscular Z-shaped suture is put
Appendectomy. Retroperitoneal position of appendix
If there is no commissures in the
Appendectomy. Retroperitoneal position of appendix
If there is no commissures in the
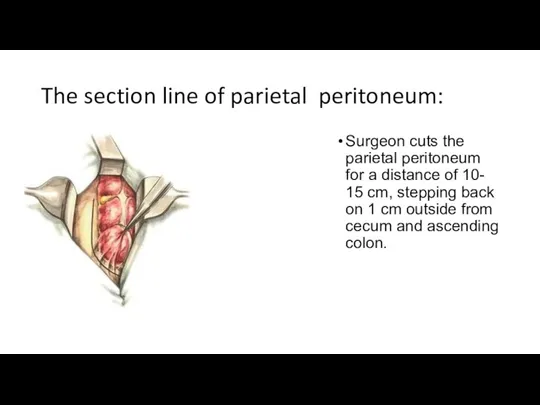
The section line of parietal peritoneum:
Surgeon cuts the parietal peritoneum for
The section line of parietal peritoneum:
Surgeon cuts the parietal peritoneum for
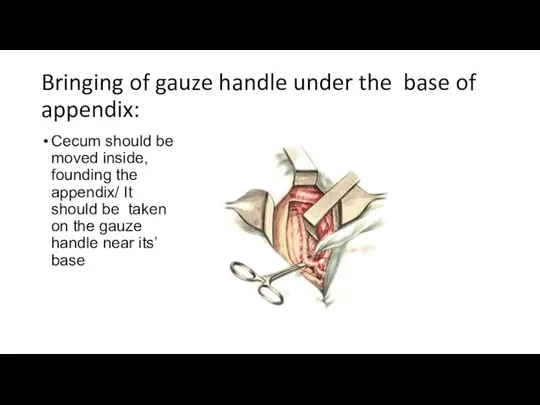
Bringing of gauze handle under the base of appendix:
Cecum should be
Bringing of gauze handle under the base of appendix:
Cecum should be
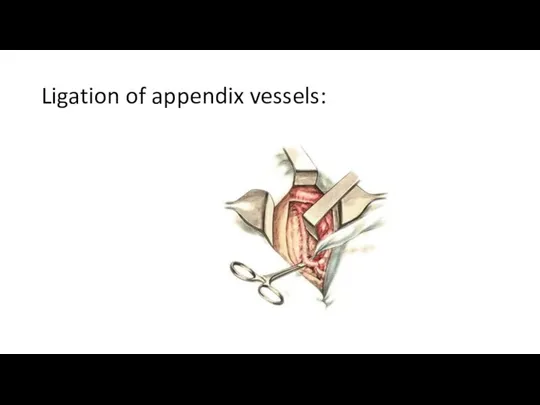
Ligation of appendix vessels:
Ligation of appendix vessels:
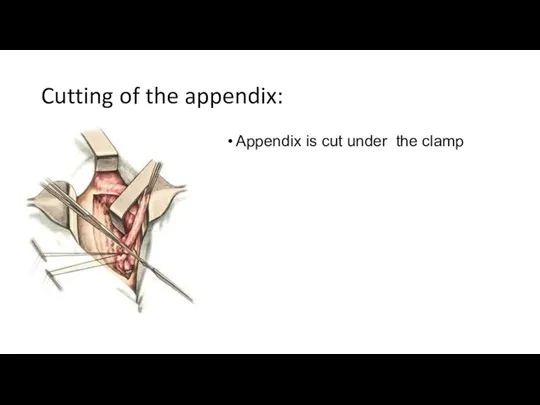
Cutting of the appendix:
Appendix is cut under the clamp
Cutting of the appendix:
Appendix is cut under the clamp
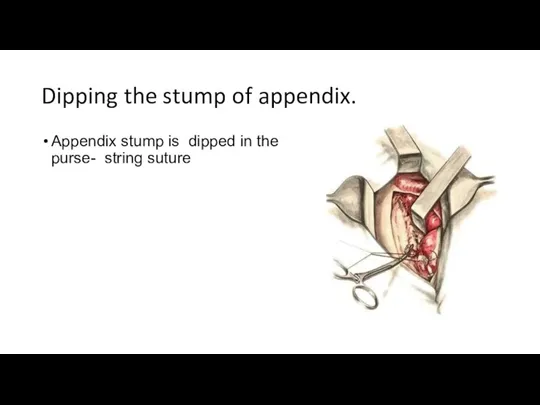
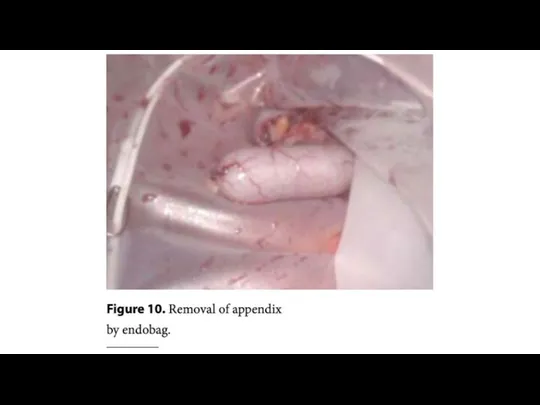
Dipping the stump of appendix.
Appendix stump is dipped in the purse-
Dipping the stump of appendix.
Appendix stump is dipped in the purse-
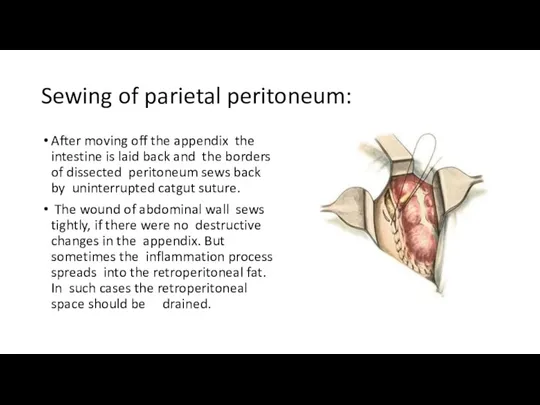
Sewing of parietal peritoneum:
After moving off the appendix the intestine is
Sewing of parietal peritoneum:
After moving off the appendix the intestine is
CLOSURE
The peritoneum is grasped with curved Kelly clamps and approximated with
CLOSURE
The peritoneum is grasped with curved Kelly clamps and approximated with
The final stage:
After moving out the appendix cecum moves back in
The final stage:
After moving out the appendix cecum moves back in
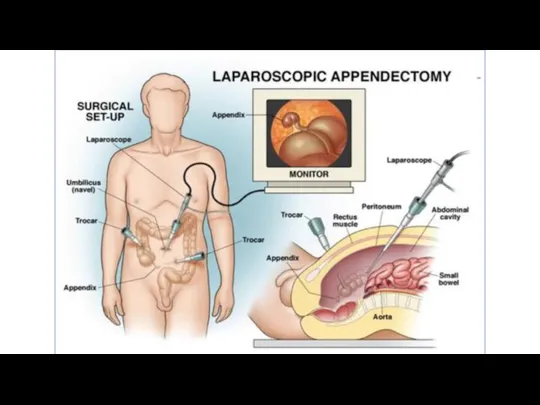
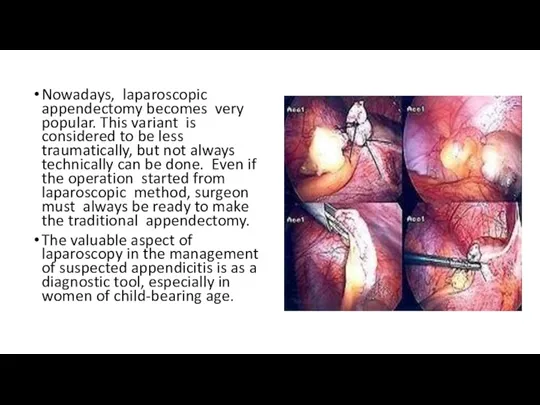
Nowadays, laparoscopic appendectomy becomes very popular. This variant is considered to
Nowadays, laparoscopic appendectomy becomes very popular. This variant is considered to
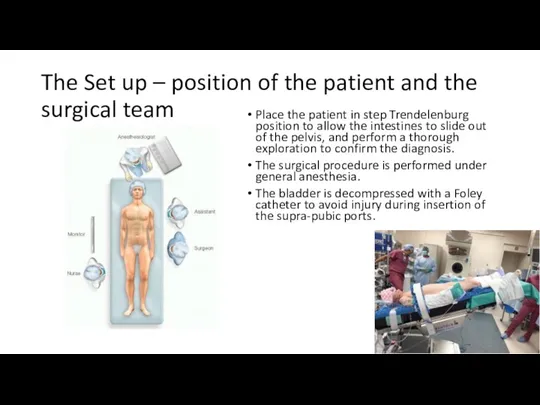
The Set up – position of the patient and the surgical
The Set up – position of the patient and the surgical
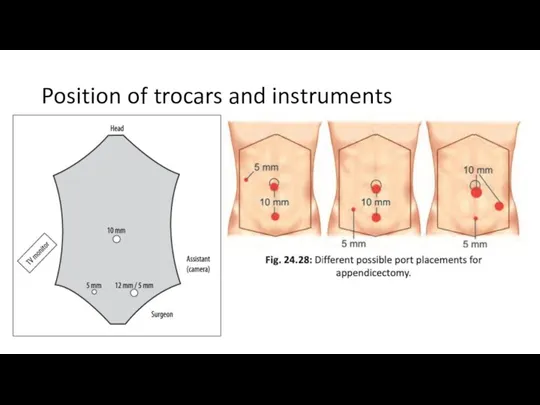
Position of trocars and instruments
Position of trocars and instruments





Open Appendectomy vs Laparoscopic Appendectomy
Open Appendectomy vs Laparoscopic Appendectomy
POST-OP MANAGEMENT
In uncomplicated case, antibiotics should be continued up to 24
POST-OP MANAGEMENT
In uncomplicated case, antibiotics should be continued up to 24

Post operative Complications
Wound infection (Most common)
5-10% of patient
4-5th day
Intra- abdominal abscess
Post operative Complications
Wound infection (Most common)
5-10% of patient
4-5th day
Intra- abdominal abscess
Alternative Methods of Appendectomy
Laparoscopic Single-Incision Appendectomy
Natural orifice transluminal endoscopic surgery
Alternative Methods of Appendectomy
Laparoscopic Single-Incision Appendectomy
Natural orifice transluminal endoscopic surgery
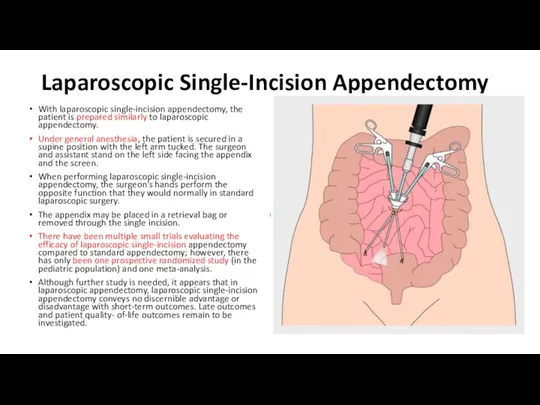
Laparoscopic Single-Incision Appendectomy
With laparoscopic single-incision appendectomy, the patient is prepared
Laparoscopic Single-Incision Appendectomy
With laparoscopic single-incision appendectomy, the patient is prepared
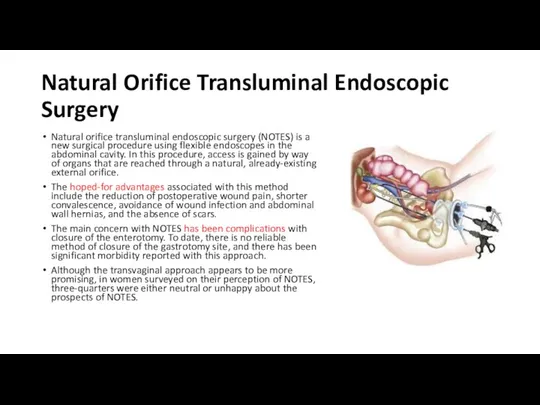
Natural Orifice Transluminal Endoscopic Surgery
Natural orifice transluminal endoscopic surgery (NOTES)
Natural Orifice Transluminal Endoscopic Surgery
Natural orifice transluminal endoscopic surgery (NOTES)
REFERENCES
Schwartz's Principles of Surgery ;Textbook by F. Charles Brunicardi and Seymour
REFERENCES
Schwartz's Principles of Surgery ;Textbook by F. Charles Brunicardi and Seymour
 Земская медицина
Земская медицина Острое воспаление
Острое воспаление Сегментмассаж
Сегментмассаж Интенсивная терапия тяжелой травмы
Интенсивная терапия тяжелой травмы ВИЧ-инфекция
ВИЧ-инфекция Әлеуметтік көмектер
Әлеуметтік көмектер Гипертоническая болезнь
Гипертоническая болезнь Цирроз печени
Цирроз печени Накостный остеосинтез. Виды пластин, показания, осложнения
Накостный остеосинтез. Виды пластин, показания, осложнения Проблема ожирения
Проблема ожирения Нестероидные противовоспалительные препараты
Нестероидные противовоспалительные препараты Респираторлық дистресс синдромы
Респираторлық дистресс синдромы Интерфероны. Биологическая природа интерферонов
Интерфероны. Биологическая природа интерферонов Серде́чная недоста́точность
Серде́чная недоста́точность Аллергодерматозы. Синдром Стивенса-Джонсона. Микозы
Аллергодерматозы. Синдром Стивенса-Джонсона. Микозы Туляремия. Возбудитель туляремии
Туляремия. Возбудитель туляремии Зубные имплантаты
Зубные имплантаты Этиология и патогенез пульпита. Классификация. Патологическая анатомия пульпита. Клиника. Диагностика
Этиология и патогенез пульпита. Классификация. Патологическая анатомия пульпита. Клиника. Диагностика Цитологическая диагностика заболеваний легких
Цитологическая диагностика заболеваний легких Функциональная анатомия мышц туловища
Функциональная анатомия мышц туловища Первая доврачебная помощь. Тепловой удар
Первая доврачебная помощь. Тепловой удар Weight Loss Challenge. Бросьте вызов лишнему весу. Углеводы, сахар и гликемический индекс
Weight Loss Challenge. Бросьте вызов лишнему весу. Углеводы, сахар и гликемический индекс Гелиос. Ваш доктор на связи. Страхование
Гелиос. Ваш доктор на связи. Страхование Особенности сестринского процесса при уходе за пациентом с ротавирусной инфекцией
Особенности сестринского процесса при уходе за пациентом с ротавирусной инфекцией Заболевания глотки. Ангина и хронический тонзиллит
Заболевания глотки. Ангина и хронический тонзиллит Комбинированная терапия L-тироксином и Lтрийодтиронином по сравнению с только Lтироксином при лечении первичного гипотиреоза
Комбинированная терапия L-тироксином и Lтрийодтиронином по сравнению с только Lтироксином при лечении первичного гипотиреоза Заболевания с фекально-оральным механизмом передачи возбудителя. Дизентерия, вирусные гепатиты, полиомиелит, туберкулёз
Заболевания с фекально-оральным механизмом передачи возбудителя. Дизентерия, вирусные гепатиты, полиомиелит, туберкулёз Микроэлементы и их роль в организме человека
Микроэлементы и их роль в организме человека