- Breast cancer

Содержание
- 2. The most frequent cancer in women
- 4. Ashkenazi Jewish 1:40, compared with 1:500 in the general population
- 5. + prostate and pancreatic
- 8. Cowden’s syndrome Hamartomas on the skin and mucous membranes. Enlarged head, a rare noncancerous brain tumor
- 12. Irradiation for the treatment of Hodgkin lymphoma before age 30 years.
- 14. Magnitude of Risk of Known Breast Cancer Risk Factors
- 15. + PBSO
- 16. Prevention for BRCA patients Tamoxifen ↓contralater - 40-50%, ↓ Risk BC in unaffected only in BRCA
- 17. Chemoprevention with Tamoxifen + RR 50% (0.51) (47 treated - 1 BC prevented) ADH - RR
- 18. Screening Mammography Recommendations Biannually or annually in 40-49 y/o Annually in >50 y/o 15% relative risk
- 19. Biopsy techniques FNA Diagnostic and therapeutic in cystic lesions Core needle U/S guided or sterotatic 90%
- 20. Risk of Future Invasive Breast Carcinoma Based on Histologic Diagnosis from Breast Biopsies No Increase Adenosis
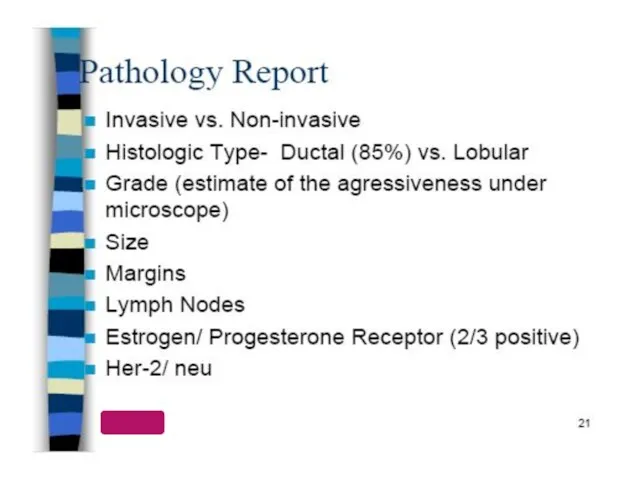
- 21. Benign Breast Masses Cysts Fibroadenoma Hamartoma/Adenoma Abscess Papillomas Sclerosing adenosis Radial scar Fat necrosis Papilloma
- 22. Maligant Breast Masses Ductal carcinoma DCIS Invasive Lobular carcinoma LCIS Invasive Inflammatory carcinoma Paget’s disease Phyllodes
- 25. BC Receptors
- 26. BC Receptors
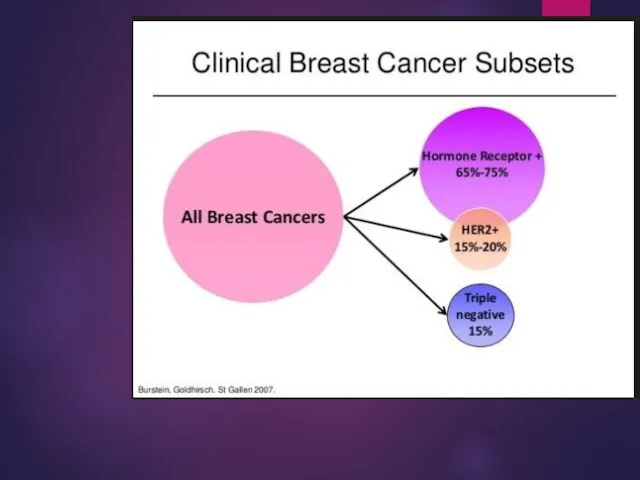
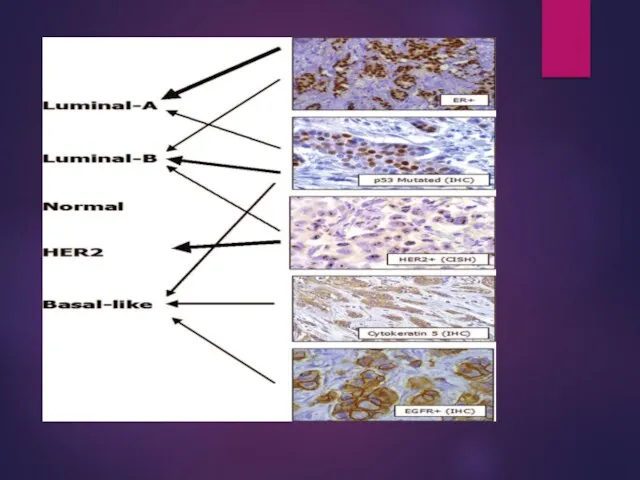
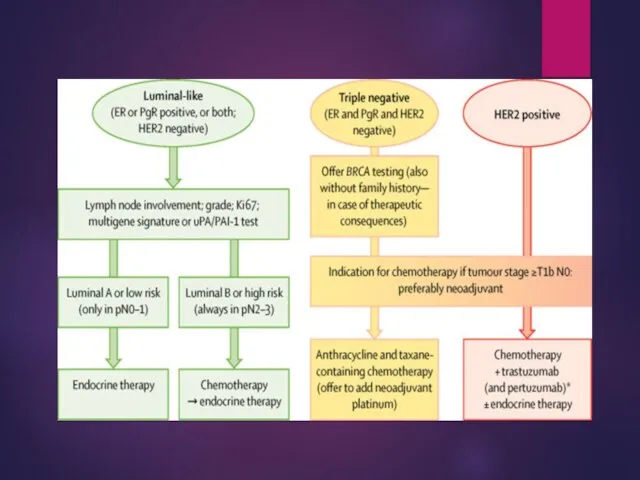
- 27. Biological subtypes
- 29. STAGING
- 30. STAGING cont.
- 31. DS Mammography US MRI CT (chest/abdomen) Bone scan or PET CT CT/MRI head Tumor markers
- 32. Systemic therapy: Hormonal therapy Chemotherapy Targeted therapies Local therapy: Surgery Radiation therapy Treatment of breast cancer
- 33. Surgery In the patient with clinical stage I, II, and T3N1 disease, the initial management is
- 34. Axilla ALND
- 35. Axilla SLNB (less lymphedema) - Majority of stage I-II BC pts - Contraindications to the procedure:
- 39. Adjuvant radiation therapy: 5 - 6.5 weeks Local control rates > 90% Minimal toxicity Adjuvant radiation
- 40. Breast cancer treatment Radiotherapy
- 41. Postmastectomy RT All women with > 3 positive nodes. a tumor larger than 5 cm. spreading
- 42. APPROACH TO BC MEDICAL TREATMENT
- 43. HORMONAL THERAPY IN LOW-RISK HORMONE POSITIVE BREAST CA- FOR 5 YEARS IN HIGH-RISK HORMONE POSITIVE BC-FOR
- 44. AI VS TAMOXIFEN –SIDE EFFECTS SSRI?
- 45. FISH hybridization test for HER 2+
- 46. APPROACH TO BC MEDICAL TREATMENT
- 47. For 1 year every 3 weeks
- 48. Trastuzumab emtansine (TDM1= KADCYLA) Her 2 pos BC Trastuzumab emtansine Conjugant therapy
- 49. Neoadjuvant chemotherapy Indications T4 cN pos Inflamatory BC Rationale Tumor shrinkage Opportunity for BCS Early treating
- 50. mBC
- 51. THERAPEUTIC ENDPOINTS OVERALL SURVIVAL QUALITY OF LIFE RESPONSE RATE TIME TO PROGRESSION TIME TO TREATMENT FAILURE
- 52. mBC approach( example)
- 54. Triple Negative Breast Cancer: Triple negative breast cancer (TNBC) is clinically characterized by the lack of
- 55. Lapatinib Her 2 pos BC A tyrosine kinase inhibitor A potent and selective oral dual inhibitor
- 56. Other breast cancers Phyllodes tumor Age 30-45 Similar in appearance to fibroadenoma 4% recurrence after excision
- 57. Inflammatory BC T4 1% to 5% of all cases Aggressive Neoadjuvant CMT +/- RT Surgery is
- 58. Paget disease 1 to 4.3% of all breast cancers Ca in situ in the nipple epidermis.
- 59. Angiosarcoma Risk factors Radiation Lymphedema Treatment Excision, radiation
- 60. Male breast cancer 90% are invasive at time of diagnosis 80% ER+, 75% PR+, 30% HER2/neu
- 61. CASE 1 03.2021 Diagnosis INCIDENTAL IMAGING TEST CT CHEST AGE-76 Y.O.
- 62. FNL BY US –clip and tumor
- 63. RT BREAST MAMMOGRAPHY
- 64. PATHOLOGICAL TEST INVASIVE BREAST CARCINOMA STAGE I G1 0.8 CM 0/2 LN NO PNI OR LVI
- 65. STAGE?
- 68. CT CHEST- DD?
- 69. CASE 2 AGE -48 SELF EXAMINATION- BREAST TUMOR
- 70. AFTER LN POS. TEST AND BREAST IMAJING
- 71. RT BREAST CA WITH RIB5 OLIGPMTS- STAGE IV
- 73. Скачать презентацию
The most frequent cancer in women
The most frequent cancer in women
Ashkenazi Jewish 1:40, compared with 1:500 in the general population
Ashkenazi Jewish 1:40, compared with 1:500 in the general population
+ prostate and pancreatic
+ prostate and pancreatic

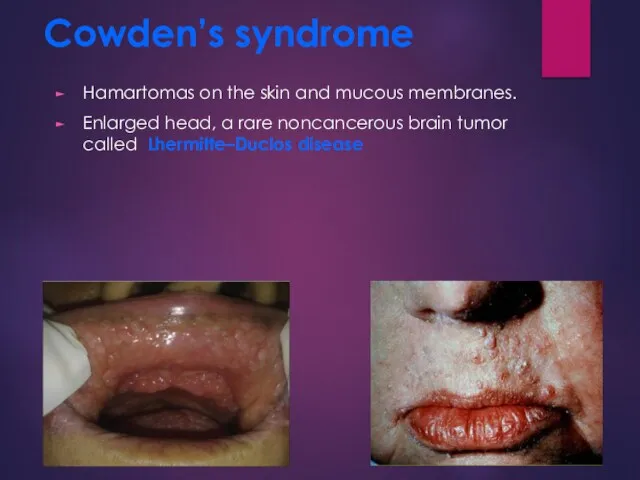
Cowden’s syndrome
Hamartomas on the skin and mucous membranes.
Enlarged head, a rare
Cowden’s syndrome
Hamartomas on the skin and mucous membranes.
Enlarged head, a rare
Irradiation for the treatment of Hodgkin lymphoma before age 30 years.
Irradiation for the treatment of Hodgkin lymphoma before age 30 years.
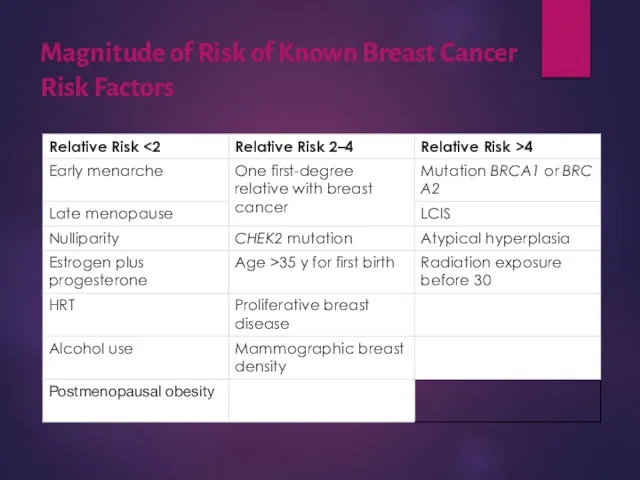
Magnitude of Risk of Known Breast Cancer Risk Factors
Magnitude of Risk of Known Breast Cancer Risk Factors
+ PBSO
+ PBSO

Prevention for BRCA patients
Tamoxifen ↓contralater - 40-50%,
↓ Risk
Prevention for BRCA patients
Tamoxifen ↓contralater - 40-50%,
↓ Risk
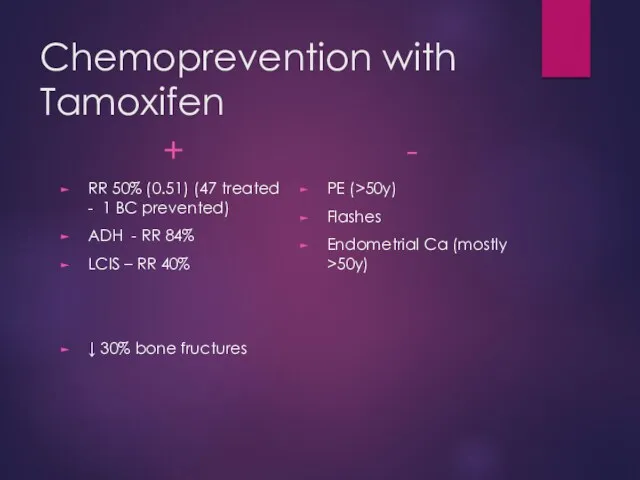
Chemoprevention with Tamoxifen
+
RR 50% (0.51) (47 treated - 1 BC prevented)
ADH
Chemoprevention with Tamoxifen
+
RR 50% (0.51) (47 treated - 1 BC prevented)
ADH
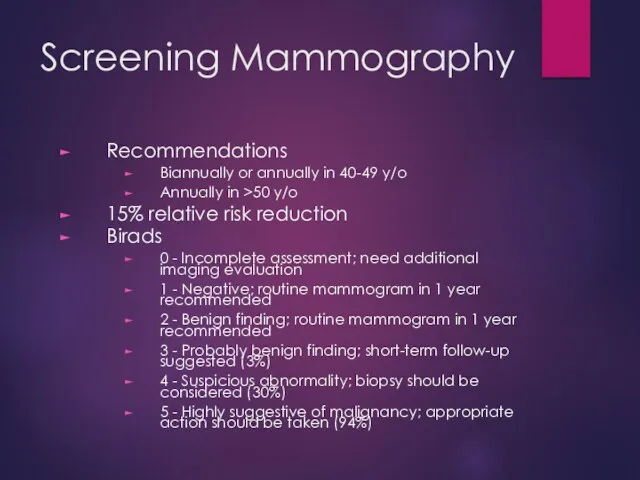
Screening Mammography
Recommendations
Biannually or annually in 40-49 y/o
Annually in >50 y/o
15% relative
Screening Mammography
Recommendations
Biannually or annually in 40-49 y/o
Annually in >50 y/o
15% relative
Biopsy techniques
FNA
Diagnostic and therapeutic in cystic lesions
Core needle
U/S guided or sterotatic
90%
Biopsy techniques
FNA
Diagnostic and therapeutic in cystic lesions
Core needle
U/S guided or sterotatic
90%
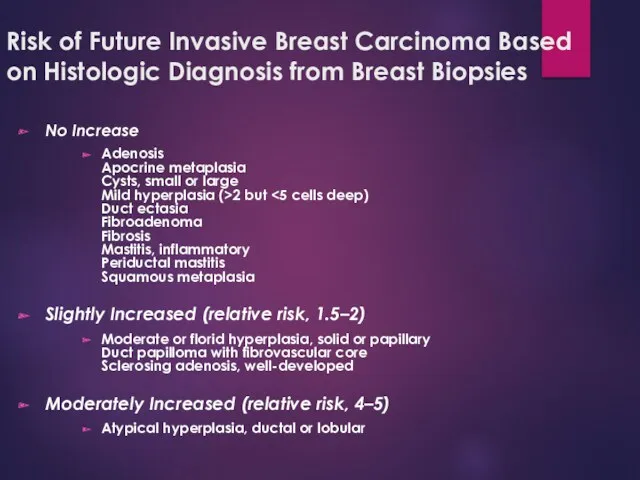
Risk of Future Invasive Breast Carcinoma Based on Histologic Diagnosis from
Risk of Future Invasive Breast Carcinoma Based on Histologic Diagnosis from
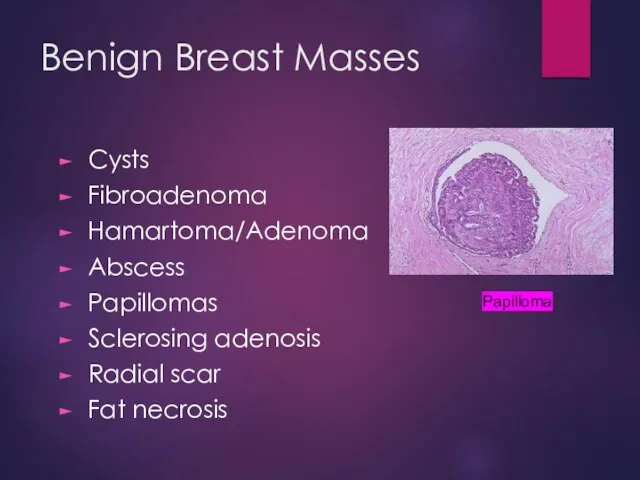
Benign Breast Masses
Cysts
Fibroadenoma
Hamartoma/Adenoma
Abscess
Papillomas
Sclerosing adenosis
Radial scar
Fat necrosis
Papilloma
Benign Breast Masses
Cysts
Fibroadenoma
Hamartoma/Adenoma
Abscess
Papillomas
Sclerosing adenosis
Radial scar
Fat necrosis
Papilloma
Maligant Breast Masses
Ductal carcinoma
DCIS
Invasive
Lobular carcinoma
LCIS
Invasive
Inflammatory carcinoma
Paget’s disease
Phyllodes tumor
Angiosarcoma
Maligant Breast Masses
Ductal carcinoma
DCIS
Invasive
Lobular carcinoma
LCIS
Invasive
Inflammatory carcinoma
Paget’s disease
Phyllodes tumor
Angiosarcoma
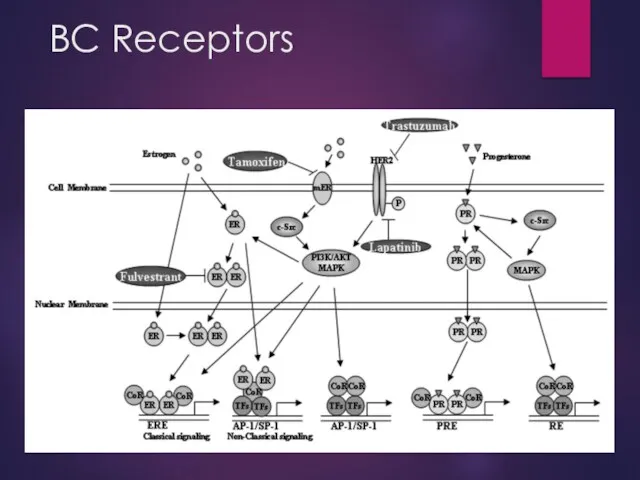
BC Receptors
BC Receptors
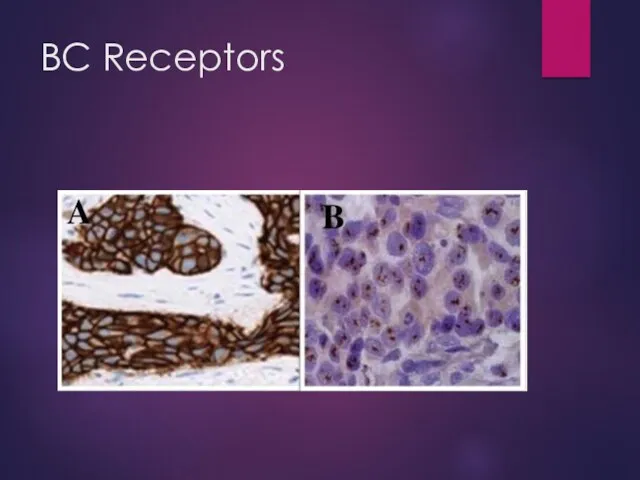
BC Receptors
BC Receptors
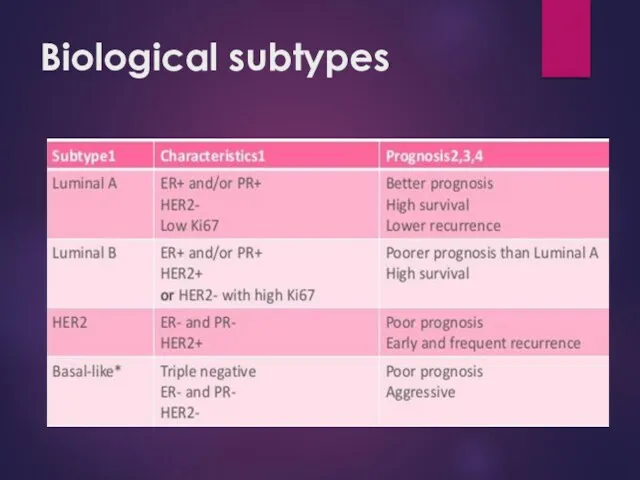
Biological subtypes
Biological subtypes
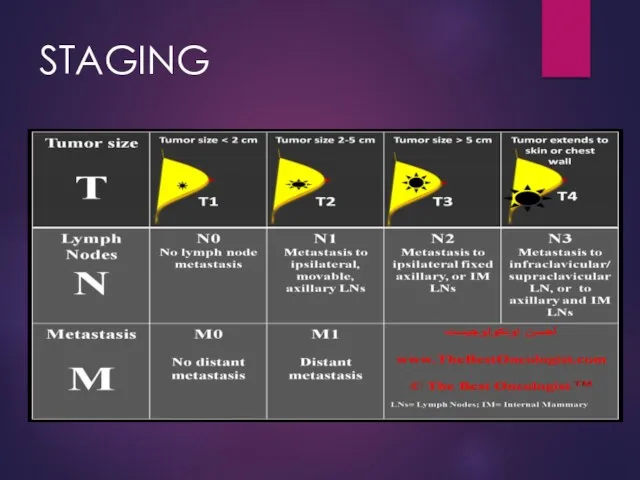
STAGING
STAGING
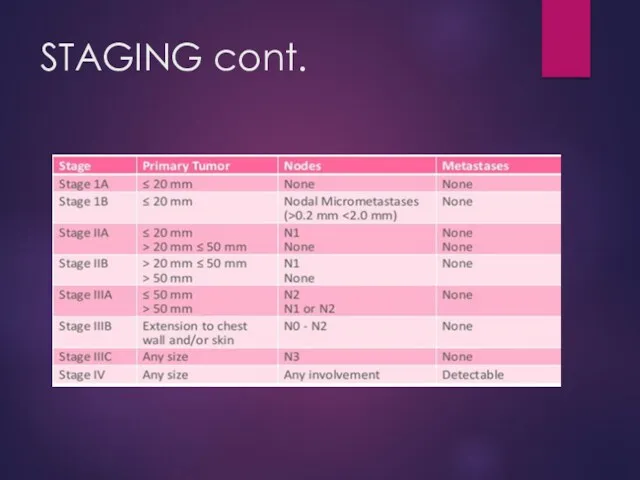
STAGING cont.
STAGING cont.
DS
Mammography
US
MRI
CT (chest/abdomen)
Bone scan or PET CT
CT/MRI head
Tumor markers
DS
Mammography
US
MRI
CT (chest/abdomen)
Bone scan or PET CT
CT/MRI head
Tumor markers
Systemic therapy:
Hormonal therapy
Chemotherapy
Targeted therapies
Local therapy:
Surgery
Radiation therapy
Treatment of breast cancer
Systemic therapy:
Hormonal therapy
Chemotherapy
Targeted therapies
Local therapy:
Surgery
Radiation therapy
Treatment of breast cancer
Surgery
In the patient with clinical stage I, II, and T3N1 disease,
Surgery
In the patient with clinical stage I, II, and T3N1 disease,
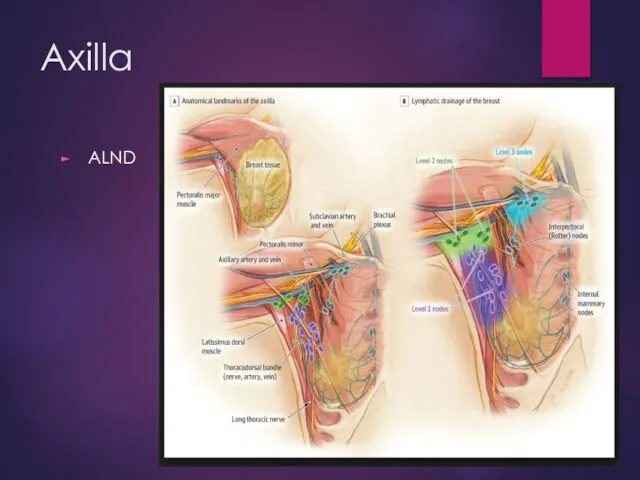
Axilla
ALND
Axilla
ALND

Axilla
SLNB (less lymphedema)
- Majority of stage I-II BC pts
-
Axilla
SLNB (less lymphedema)
- Majority of stage I-II BC pts
-

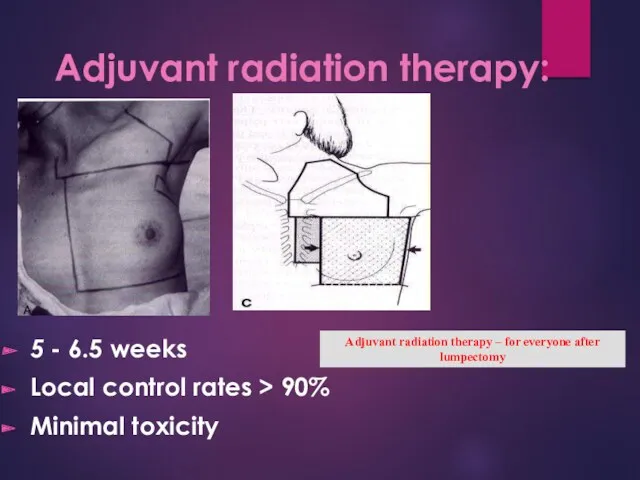
Adjuvant radiation therapy:
5 - 6.5 weeks
Local control rates > 90%
Minimal toxicity
Adjuvant
Adjuvant radiation therapy:
5 - 6.5 weeks
Local control rates > 90%
Minimal toxicity
Adjuvant

Breast cancer treatment
Radiotherapy
Breast cancer treatment
Radiotherapy
Postmastectomy RT
All women with > 3 positive nodes.
a tumor larger than
Postmastectomy RT
All women with > 3 positive nodes.
a tumor larger than
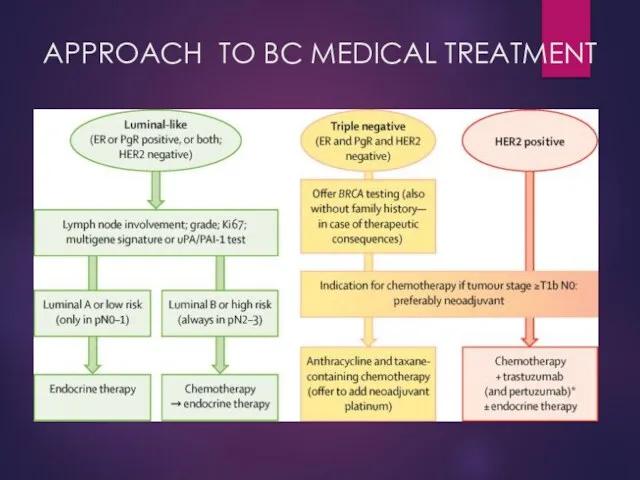
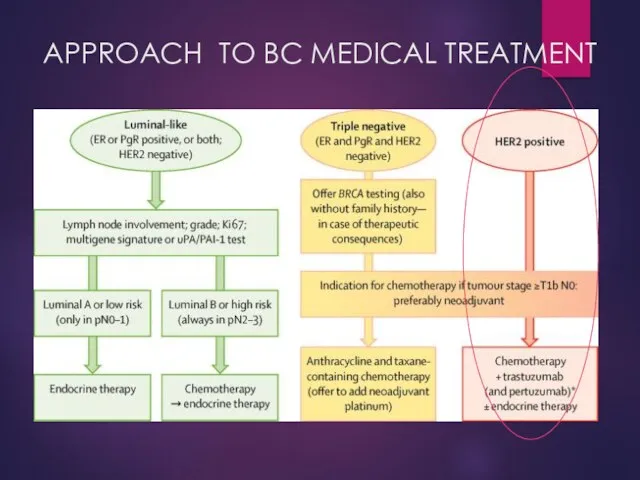
APPROACH TO BC MEDICAL TREATMENT
APPROACH TO BC MEDICAL TREATMENT
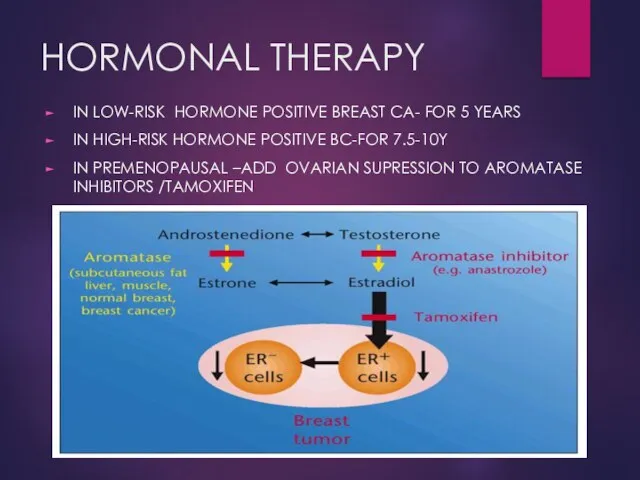
HORMONAL THERAPY
IN LOW-RISK HORMONE POSITIVE BREAST CA- FOR 5 YEARS
IN HIGH-RISK
HORMONAL THERAPY
IN LOW-RISK HORMONE POSITIVE BREAST CA- FOR 5 YEARS
IN HIGH-RISK
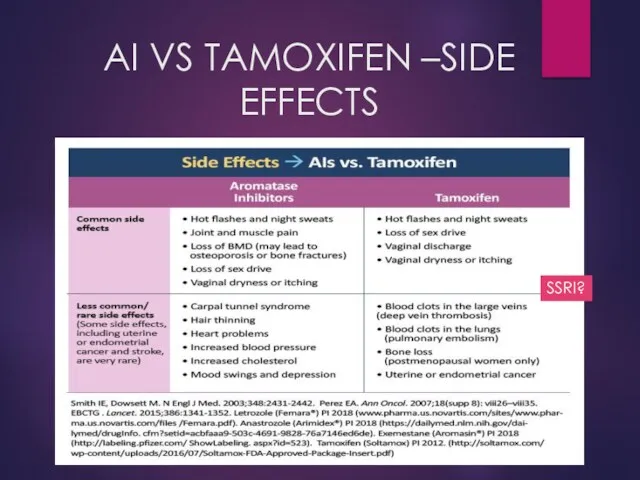
AI VS TAMOXIFEN –SIDE EFFECTS
SSRI?
AI VS TAMOXIFEN –SIDE EFFECTS
SSRI?
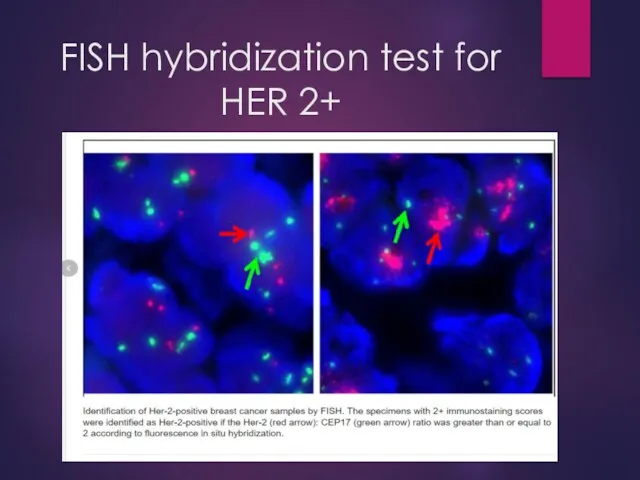
FISH hybridization test for HER 2+
FISH hybridization test for HER 2+
APPROACH TO BC MEDICAL TREATMENT
APPROACH TO BC MEDICAL TREATMENT
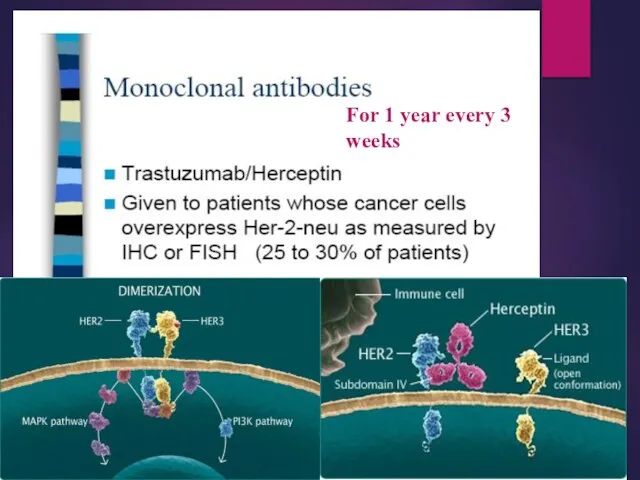
For 1 year every 3 weeks
For 1 year every 3 weeks
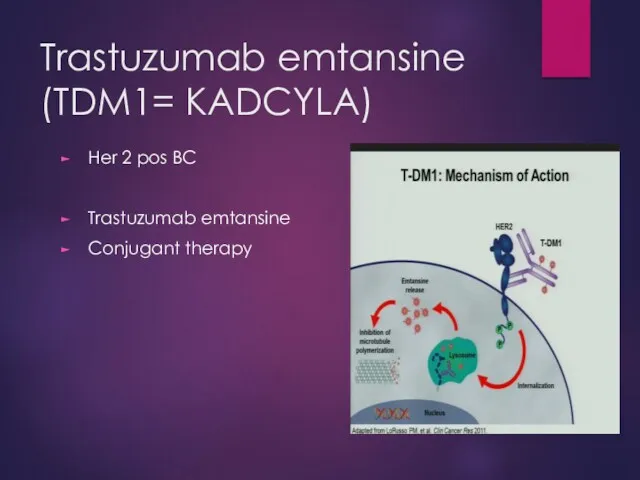
Trastuzumab emtansine
(TDM1= KADCYLA)
Her 2 pos BC
Trastuzumab emtansine
Conjugant therapy
Trastuzumab emtansine
(TDM1= KADCYLA)
Her 2 pos BC
Trastuzumab emtansine
Conjugant therapy
Neoadjuvant chemotherapy
Indications
T4
cN pos
Inflamatory BC
Rationale
Tumor shrinkage
Opportunity for BCS
Early treating of micrometastasis
Aggressive biological
Neoadjuvant chemotherapy
Indications
T4
cN pos
Inflamatory BC
Rationale
Tumor shrinkage
Opportunity for BCS
Early treating of micrometastasis
Aggressive biological
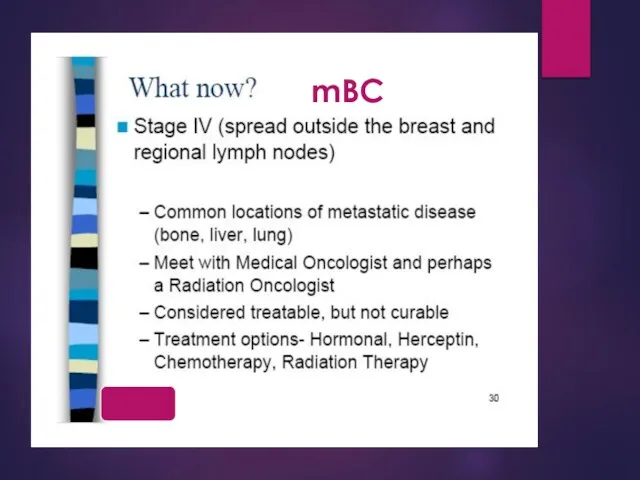
mBC
mBC
THERAPEUTIC ENDPOINTS
OVERALL SURVIVAL
QUALITY OF LIFE
RESPONSE RATE
TIME TO PROGRESSION
TIME TO TREATMENT
THERAPEUTIC ENDPOINTS
OVERALL SURVIVAL
QUALITY OF LIFE
RESPONSE RATE
TIME TO PROGRESSION
TIME TO TREATMENT
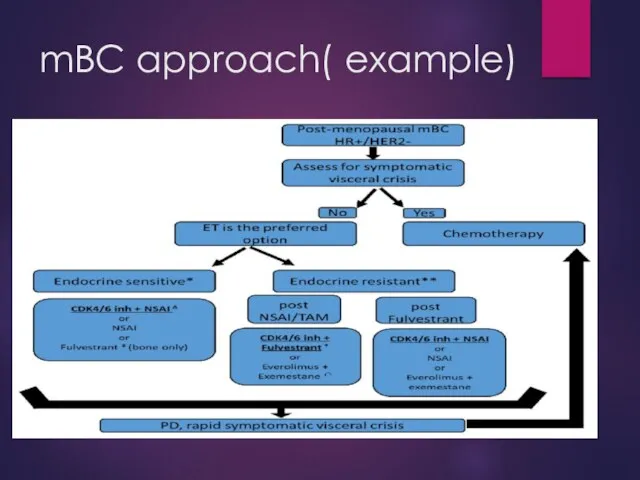
mBC approach( example)
mBC approach( example)
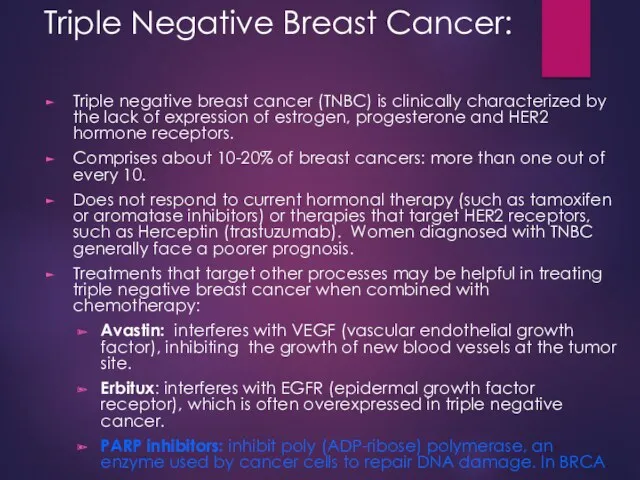
Triple Negative Breast Cancer:
Triple negative breast cancer (TNBC) is clinically characterized
Triple Negative Breast Cancer:
Triple negative breast cancer (TNBC) is clinically characterized
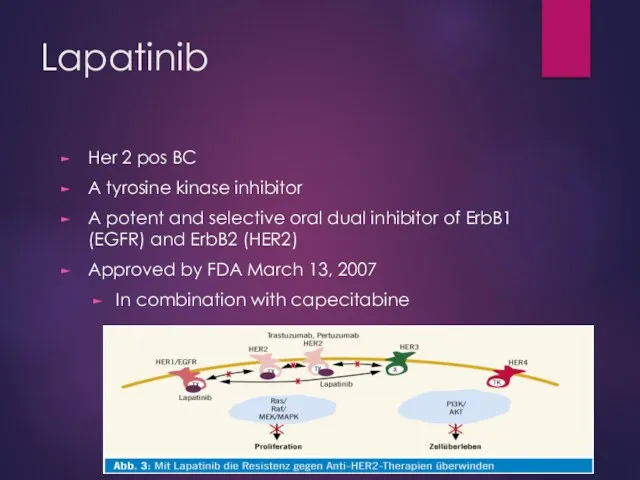
Lapatinib
Her 2 pos BC
A tyrosine kinase inhibitor
A potent and selective
Lapatinib
Her 2 pos BC
A tyrosine kinase inhibitor
A potent and selective
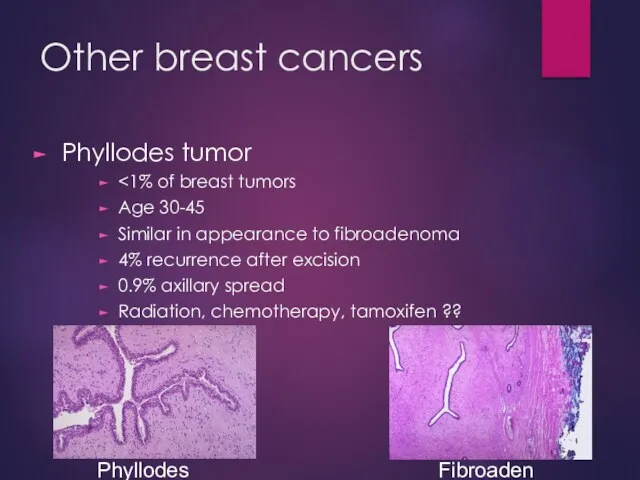
Other breast cancers
Phyllodes tumor
<1% of breast tumors
Age 30-45
Similar in appearance to
Other breast cancers
Phyllodes tumor
<1% of breast tumors
Age 30-45
Similar in appearance to
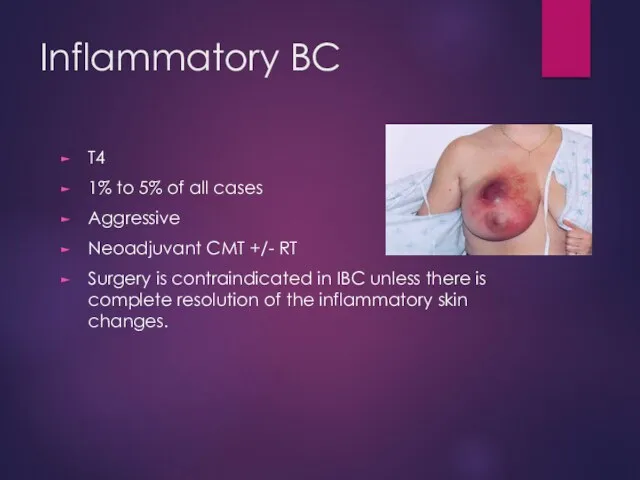
Inflammatory BC
T4
1% to 5% of all cases
Aggressive
Neoadjuvant CMT +/- RT
Surgery is
Inflammatory BC
T4
1% to 5% of all cases
Aggressive
Neoadjuvant CMT +/- RT
Surgery is
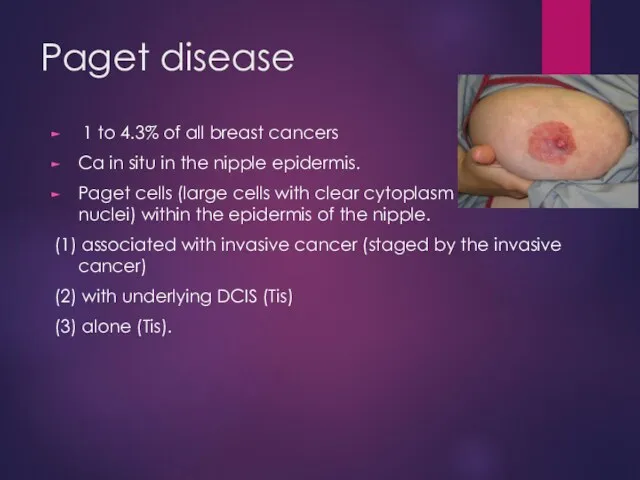
Paget disease
1 to 4.3% of all breast cancers
Ca in situ in
Paget disease
1 to 4.3% of all breast cancers
Ca in situ in
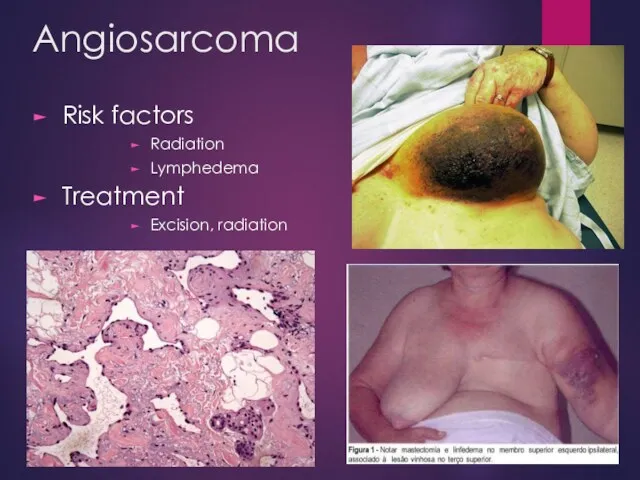
Angiosarcoma
Risk factors
Radiation
Lymphedema
Treatment
Excision, radiation
Angiosarcoma
Risk factors
Radiation
Lymphedema
Treatment
Excision, radiation
Male breast cancer
90% are invasive at time of diagnosis
80% ER+, 75%
Male breast cancer
90% are invasive at time of diagnosis
80% ER+, 75%
CASE 1
03.2021 Diagnosis
INCIDENTAL IMAGING TEST
CT CHEST
AGE-76 Y.O.
CASE 1
03.2021 Diagnosis
INCIDENTAL IMAGING TEST
CT CHEST
AGE-76 Y.O.
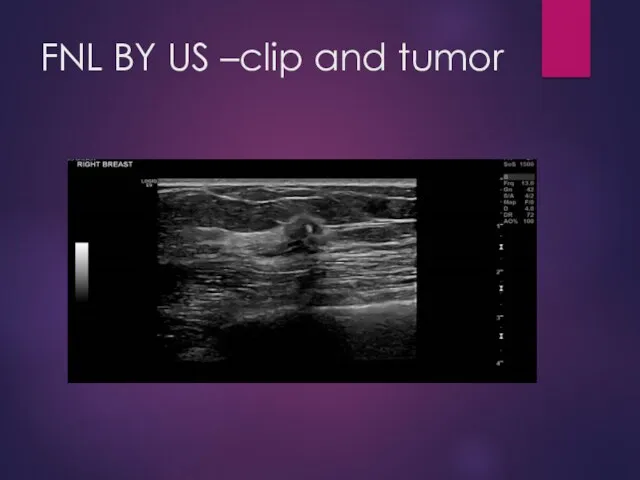
FNL BY US –clip and tumor
FNL BY US –clip and tumor
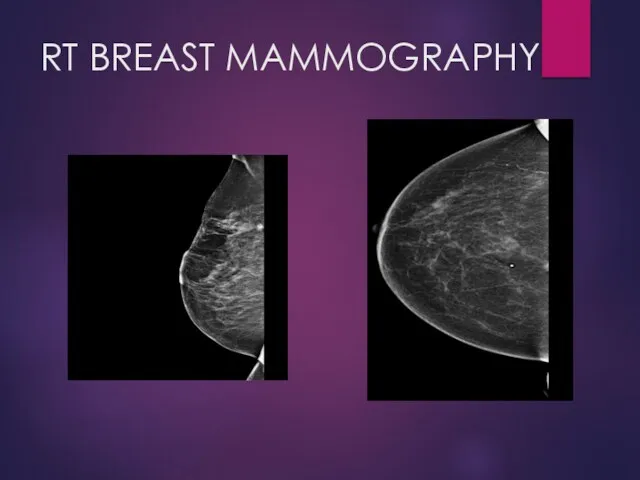
RT BREAST MAMMOGRAPHY
RT BREAST MAMMOGRAPHY
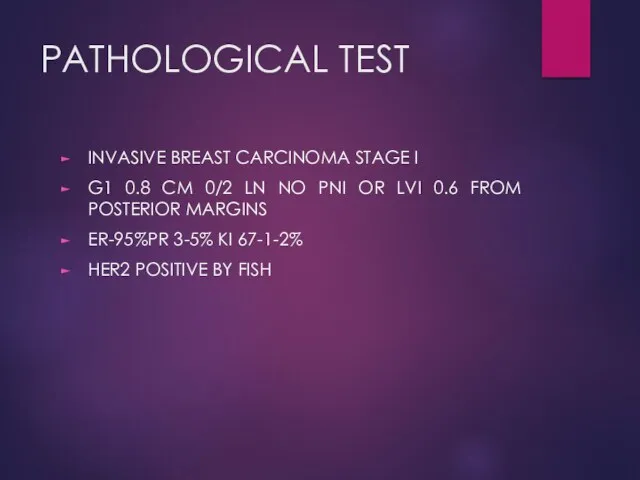
PATHOLOGICAL TEST
INVASIVE BREAST CARCINOMA STAGE I
G1 0.8 CM 0/2 LN
PATHOLOGICAL TEST
INVASIVE BREAST CARCINOMA STAGE I
G1 0.8 CM 0/2 LN
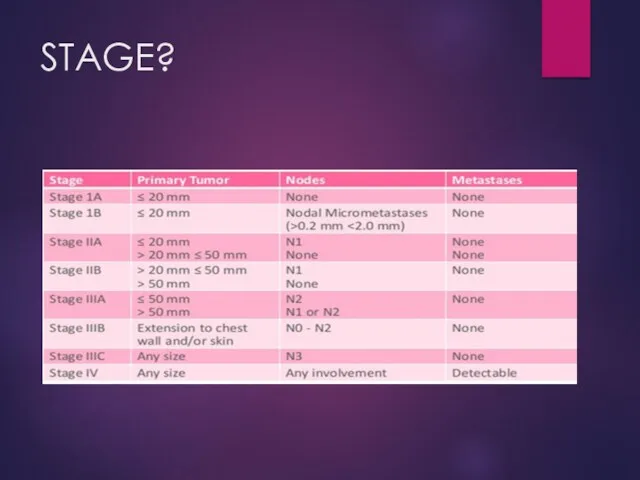
STAGE?
STAGE?
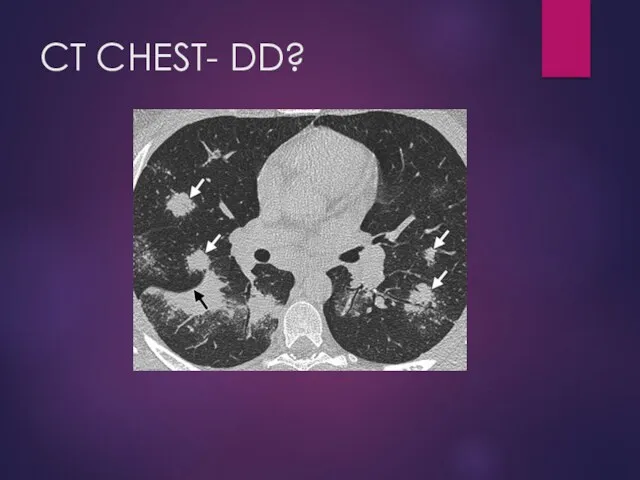
CT CHEST- DD?
CT CHEST- DD?
CASE 2
AGE -48
SELF EXAMINATION- BREAST TUMOR
CASE 2
AGE -48
SELF EXAMINATION- BREAST TUMOR
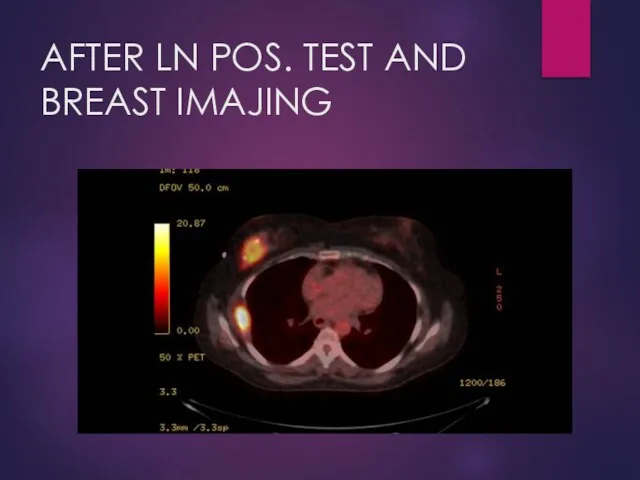
AFTER LN POS. TEST AND BREAST IMAJING
AFTER LN POS. TEST AND BREAST IMAJING
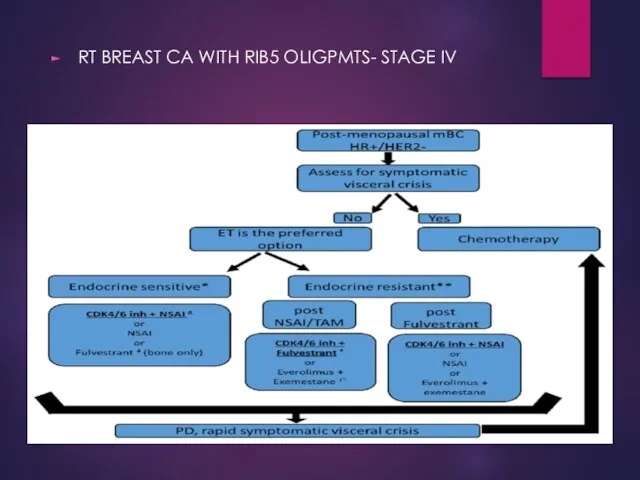
RT BREAST CA WITH RIB5 OLIGPMTS- STAGE IV
RT BREAST CA WITH RIB5 OLIGPMTS- STAGE IV
 Международный день недоношенных детей
Международный день недоношенных детей Дифференциальный диагноз состояний, сопровождающихся астмоидным дыханием, лечение и поодерживающий уход
Дифференциальный диагноз состояний, сопровождающихся астмоидным дыханием, лечение и поодерживающий уход Генетика человека
Генетика человека Дыхательная гимнастика по методике Б.С. Толкачева. презентация
Дыхательная гимнастика по методике Б.С. Толкачева. презентация Пневмонии у детей
Пневмонии у детей Анатомия глазного яблока
Анатомия глазного яблока Оказание медицинской помощи по профилю акушерство и гинекология
Оказание медицинской помощи по профилю акушерство и гинекология Особенности детей ОВЗ с умственной отсталостью. Обучение и воспитание
Особенности детей ОВЗ с умственной отсталостью. Обучение и воспитание Уақытша және тұрақты тістердегі жегінің этиологиясы және патогенез, клиникасы, диагностика және емдеу принципі
Уақытша және тұрақты тістердегі жегінің этиологиясы және патогенез, клиникасы, диагностика және емдеу принципі Здоровый образ жизни
Здоровый образ жизни Курация больного с оформлением учебной истории болезни. История болезни, как научно-медицинский и юридический документ
Курация больного с оформлением учебной истории болезни. История болезни, как научно-медицинский и юридический документ Болезни слюнных желез
Болезни слюнных желез Балалардағы безгек
Балалардағы безгек Правила измерения артериального давления
Правила измерения артериального давления ЭКГ-диагностика ишемической болезни сердца - стенокардии и инфаркта миокарда
ЭКГ-диагностика ишемической болезни сердца - стенокардии и инфаркта миокарда Отравляющие и АОХВ общеядовитого действия. Клиника, диагностика, лечение
Отравляющие и АОХВ общеядовитого действия. Клиника, диагностика, лечение ҚР және аймақтардағы ісік ауруларының құрылымы мен деңгейін салыстырмалы талдау
ҚР және аймақтардағы ісік ауруларының құрылымы мен деңгейін салыстырмалы талдау Nanotechnology and their application in medicine
Nanotechnology and their application in medicine Гигиена лечебно-профилактических учреждений
Гигиена лечебно-профилактических учреждений Неврозы, страхи и энурез детского возраста
Неврозы, страхи и энурез детского возраста Контрастные вещества, применяемые в лучевой диагностике
Контрастные вещества, применяемые в лучевой диагностике Фармакокоррекция заболеваний органов пищеварения
Фармакокоррекция заболеваний органов пищеварения Неотложная терапия в: ревматологии, кардиологии, гастроэнтерологии
Неотложная терапия в: ревматологии, кардиологии, гастроэнтерологии Методы анализа лекарственных средств
Методы анализа лекарственных средств Физиология послеродового периода
Физиология послеродового периода Аутизм
Аутизм Фантомный курс. Строение женского таза
Фантомный курс. Строение женского таза Парентеральный гепатит
Парентеральный гепатит