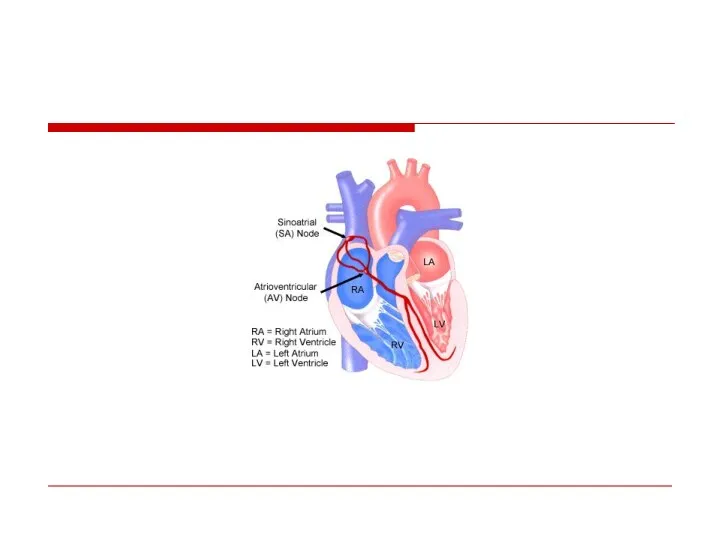
- Cardiac arrhythmias

Содержание
- 9. Normal Sinus rhythm
- 10. Classification Tachyarrhythmia: - Supraventricular - Ventricular Bradiarrhythmia
- 11. APB or PAC
- 12. Atrial Fibrillation The most common arrhythmia in clinical practice Frequency increases with age
- 13. Irregularly irregular rhythm No P waves F waves
- 14. Mechanism
- 15. Most common causes Valvular heart disease: (MS,MR) LV hypertrophy (HTN, other cause) Cardiomyopathy Thyrotoxicosis Alcohol (“holiday
- 16. Rapid AF
- 17. Consequences of Atrial Fibrillation Hemodynamic loss of synchronous atrial mechanical activity irregularity of ventricular response inappropriately
- 18. Classification
- 19. Treatment options 1. Rhythm control – restoration and maintenance of sinus rhythm 2. Rate control Prevention
- 20. Williams Classification of Antyarrhythmic Drugs Class I- blocking the fast Na channels: IA – Reduce V
- 21. IB : Do not reduce V max and shorten action potential duration Lidocaine Phenytoin Mexiletine IC:
- 22. Class II – beta blockers Class III – K channel blockers - Amiodaron - Sotalol -
- 23. Cardioversion Pharmacological Propafenon Amiodaron Flecainide
- 24. Cardioversion Electric In acute setting (hemodynamically unstable pt) In Chronic Setting Elective cardioversion
- 25. Predictors of successful cardioverson Short AF duration Young age Normal atrial size No organic heart pathology
- 26. Maintenance of sinus rhythm Propafenon Amiodaron Dronedaron Sotalol Flecainide
- 29. Rate Control Acute setting – IV - Esmolol - Metoprolol - Verapamil - Dilthiazem - Digoxin
- 31. – Severe symptoms due to AF – Patients with CHF – Younger patients – Patients with
- 32. Rate Control as First-Line Choice Consider rate control as first-line therapy if: – Patient is relatively
- 33. Left Atrial Appendage
- 34. Anticoagulation
- 35. CHADS2 score
- 37. Novel Oral Anticoagulants Dabigatran (Pradaxa)- direct oral thrombin inhibitor Rivaroxaban (Xarelto)– direct oral factor Xa inhibitor
- 38. Invasive AF treatment
- 39. RF ablation
- 40. Invasive AF management Rate control “Ablate and pace” – A-v nodal ablation & Permanent pacemaker
- 41. Pulmonary Venous Isolation For recurrent paroxysmal AF
- 42. Cox-Maze Procedure Left Atrial Isolation (1980) Corridor Procedure (1985) Maze Procedure (1987) Pathway from the SA
- 43. Maze
- 44. LA appendage closure
- 45. Atrial flutter
- 48. Management Electric Cardioversion Slowing Ventricular rate - Beta Blockers - Ca Channel blocker - Digoxin Propafenon
- 49. Prevention Isthmus ablation
- 50. Preexitation – WPW syndrome (accessory pathway(
- 51. AVRT Short PR ( Wide QRS with delta wave ST-T Changes
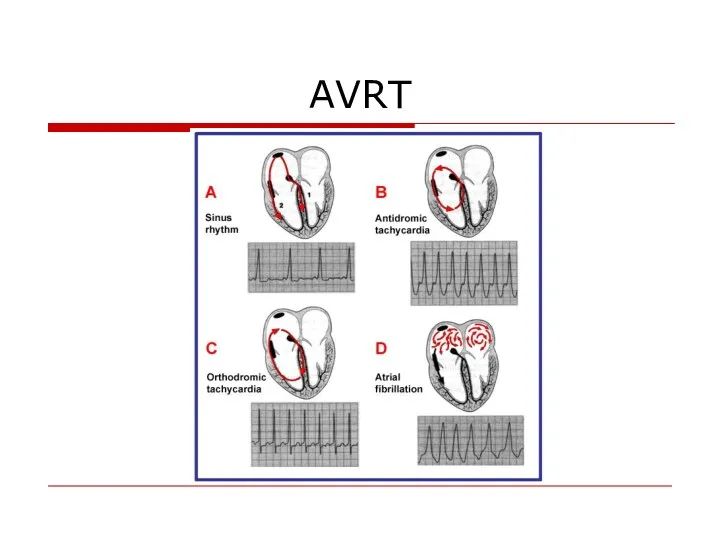
- 53. AVRT
- 54. AVRT
- 55. Treatment Acute treatment: Wide complex – Procainamide DC Shock Narrow complex – Verapamil, Beta Blockers Preventive
- 56. AF with WPW – high risk of VF
- 57. Double A-V nodal physiology
- 59. AVNRT
- 60. Management of narrow complex SVT If unstable – DC shock If Stable : 1. Vagal maneuvers
- 61. Preventive treatment Drugs EPS
- 62. Ventricular Arrhythmias
- 63. Ventricular premature beats Ventricular premature complexes premature occurrence of a QRS complex that is abnormal in
- 64. Compensatory pause
- 65. Bigeminy
- 66. Trigeminy
- 67. VPB’s
- 68. Unifocal & Multifocal
- 69. Couplet & Triplet
- 70. Causes LV false tendons, infection in ischemic or inflamed myocardium, hypoxia, Anesthesiaor surgery. Medications electrolyte imbalance,
- 71. Complex Ventricular Arrhythmia Nonsustained ventricular tachycardia (VT) ♥ Monomorphic ♥ Polymorphic Sustained VT ♥ Monomorphic ♥
- 72. Definition: Ventricular tachycardia consist of at least three consecutive QRS complexes originating from the ventricles and
- 73. VT -monomorphic
- 74. Sustained Polymorphic VT
- 75. VF
- 76. VF with Defibrillation (12-lead ECG)
- 77. Causes Chronic coronary heart disease Heart failure Congenital heart disease Neurological disorders Structurally normal hearts Sudden
- 78. Ventricular fibrillation - 62.4% Bradyarrhythmias (including advanced AV block and asystole) - 16.5% Torsades de pointes
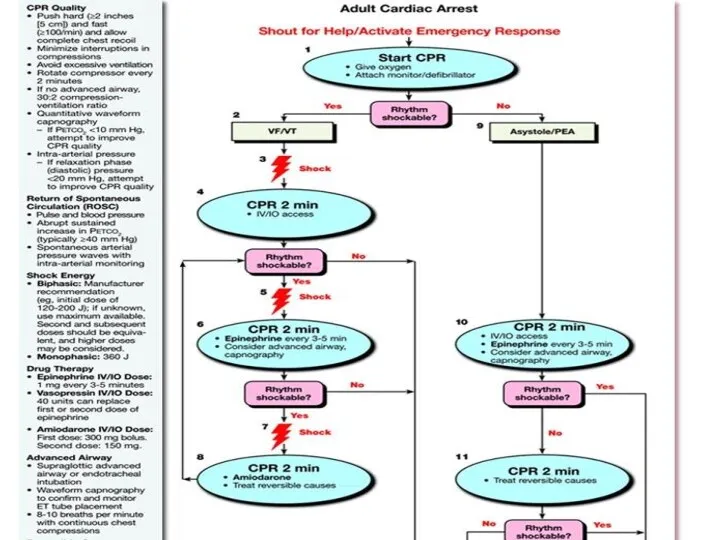
- 79. VA management Acute Chronic (secondary prevention)
- 80. Sustained VT Hemodynamically stable: - Amiodaron - Lidocain - Procainamide If pfarmacotherapy ineffective – DC shock
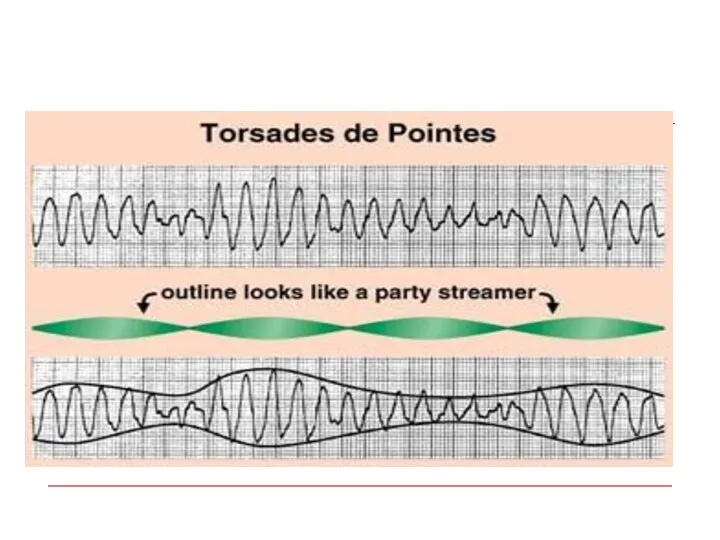
- 81. Polymorphic VT Polymorphic VT with long QT – Torsades de pointes Treatment – Mg , Pacing
- 83. Chronic Management (secondary prevention) Evaluation - Rest ECG - Exersise test - Ambulatory ECG - Imaging
- 84. Treatment of the underlying disease Revascularisation Valve surgery CHD repair
- 85. ♥ Electrolytes: Mg & K ♥ ACE inhibitors, ♥ Antithrombotic and antiplatelet agents ♥ Statins Non-antiarrhythmic
- 86. Antiarrhytmic drugs Antiarrhythmic drugs (except for BB) should not be used as primary preventive therapy of
- 87. Invasive treatment AICD EPS with ablation Surgical ablation
- 88. AICD for primary prevention of SCD 1.Post MI - LVEF - LVEF 30-35%, NYHA II-III -LVEF
- 89. Long QT syndrome Congenital (family) Acquired: Electrolyte anomalies – K, Mg Drug induced -Antiarrhytmics - Tricyclic
- 91. Long QT syndrome treatment Acute 1.Remove the precipitating factor 2. Mg IV 3. Pacing 4. Isoproterenol
- 92. Long QT syndrome treatment Chronic – for congenital long QT 1.Beta blockers 2. AICD
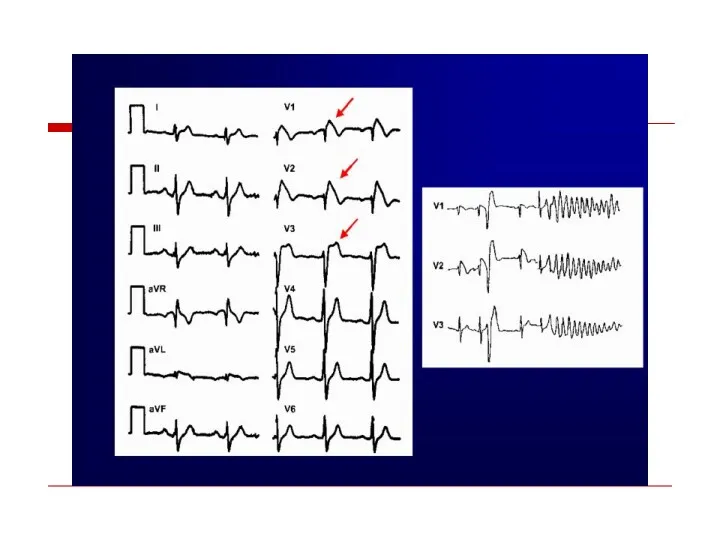
- 94. Brugada syndrome
- 97. CLBBB
- 98. CRBBB
- 100. “Wide Complex Tachycardia” VT SVT with Preexistent BBB Rate dependent BBB Preexitation
- 102. Wide QRS Irregular Tachycardia: Atrial Fibrillation with antidromic conduction in patient with accessory pathway – Not
- 103. AV Dissociation QRS > 0.14 QRS Axis between – 90 & - 180 degrees Positive QRS
- 104. A three-lead rhythm strip from a 62-year-old man who presented with acute shortness of breath 2
- 105. Sustained monomorphic ventricular tachycardia with atrioventricular (AV) dissociation. Note the independence of the atrial (sinus) rate
- 106. ?
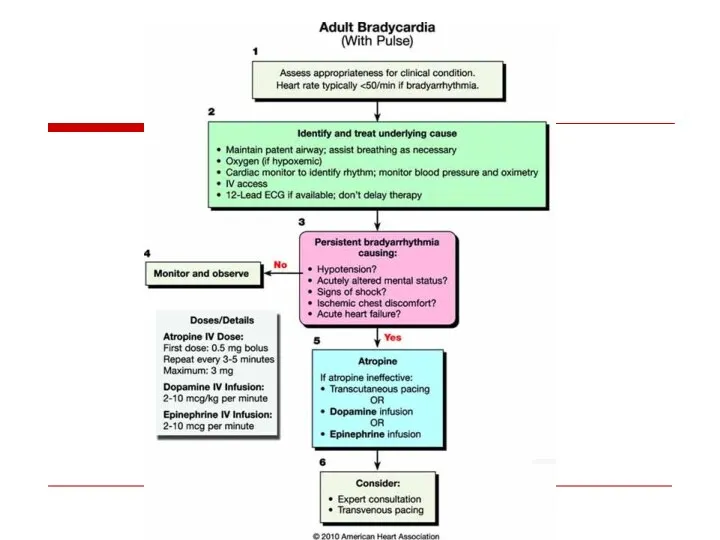
- 108. Atrioventricular Conduction Disturbances and Bradyarrhythmias
- 109. Sites of Disturbances in Impulse Formation or Conduction Leading to Bradyarrhythmias SA Node AV Node His-Purkinje
- 110. Pacemaker Hierarchy (Dominant vs Subsidiary/Escape Pacemakers) SA Node (+Atria) AV Junction (=AVN/His Bundle) Ventricles (= Distal
- 111. AV Block
- 112. AV Block - Definitions First Degree: Prolonged conduction time Second Degree: Intermittent non-conduction Third Degree: Persistent
- 113. First Degree AV Block (PR > .20 sec [1 big box]) II P P P .36
- 115. Second Degree AV Block - Type I (Wenkebach or Mobitz I Block) P P P P
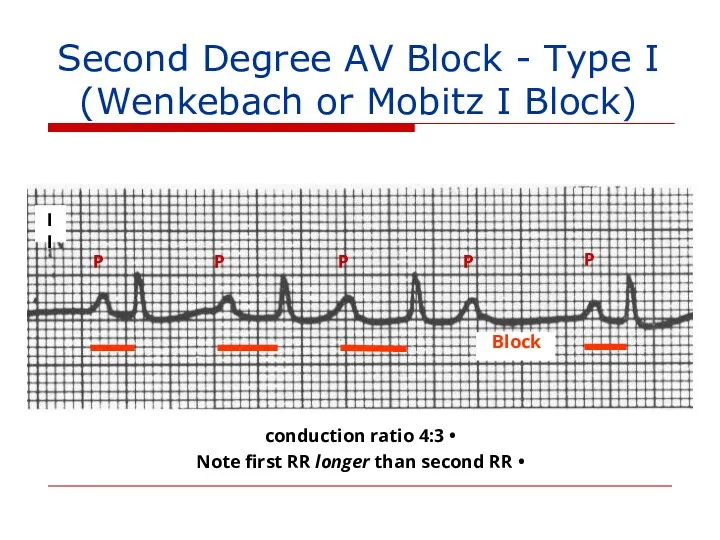
- 116. II Block P P P P P 4:3 conduction ratio Note first RR longer than second
- 117. II
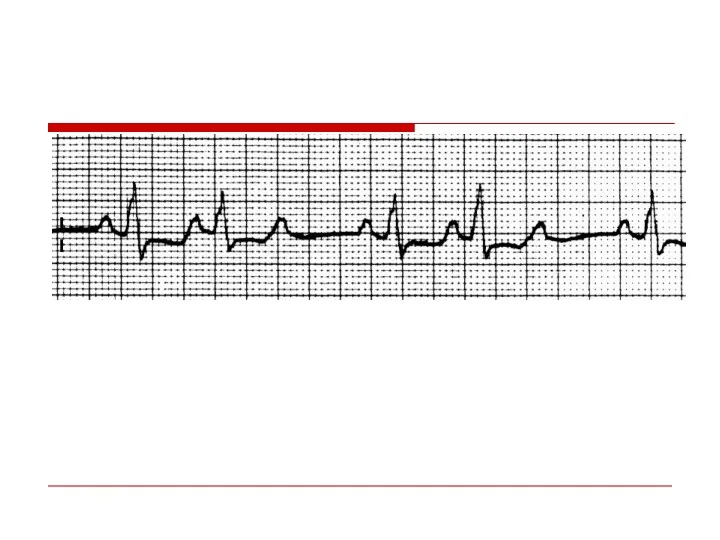
- 118. II P P P P P P Second Degree AV Block - Type II (Mobitz II)
- 119. Second Degree AV Block - Type II P P P P P 4:3 conduction ratio Block
- 120. II P P P P P P 2:1 Second Degree AV Block - Type I or
- 121. EKG/Clinical Clues* to site of 2:1 Second Degree AV block QRS narrow Improves with exercise (catecholamine-facilitated
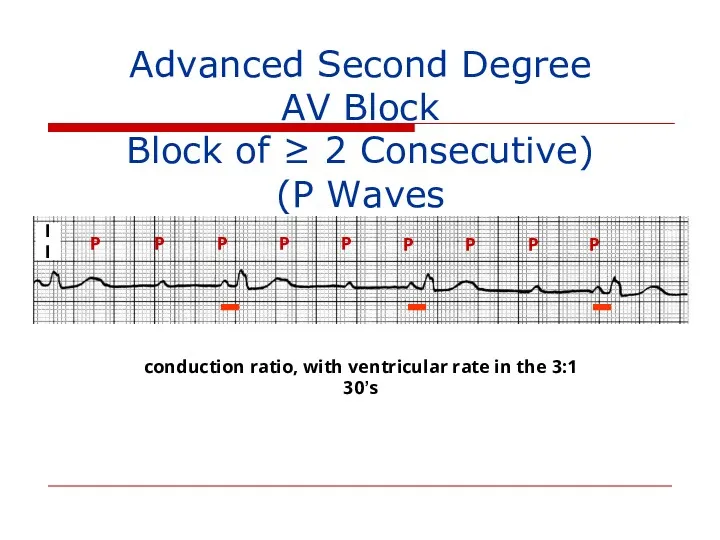
- 122. II P P P P P P P P P 3:1 conduction ratio, with ventricular rate
- 123. Site of AV Block vs. Escape Rhythm AV Node: Junctional or ventricular His-Purkinje System: Ventricular
- 125. Third Degree AV Block (Complete Heart Block) P P P P P P P waves at
- 126. Unreliability of Ventricular Escape Rhythm in Third Degree AV Block P P (P) P P P
- 129. Causes of NON-Physiologic AV Block Ischemic heart disease, cardiomyopathy and degenerative changes Drugs that depress AV
- 130. Sinus Bradyarrhythmias
- 131. Sinus Bradycardia II P wave upright in leads I and II, just as in normal sinus
- 132. Causes of Sinus Bradycardia Increased vagal tone Drugs: beta blockers, calcium channel blockers, amiodarone, digoxin (indirect
- 133. Sequence of P Wave Generation Sinus Node SA Junction Atrium (P wave) Non-visible process on the
- 134. Inspiration Expiration SA nodal acceleration SA nodal deceleration Sinus Arrhythmia
- 135. Sinoatrial (SA) Exit Block - Definitions First Degree: Prolonged SA conduction time (non-detectable on EKG; no
- 136. Second Degree SA Exit Block - Type I (Wenkebach) P P P P 4:3 pattern Missing
- 137. Second Degree SA Exit Block - Type II PP: P P P P P One P
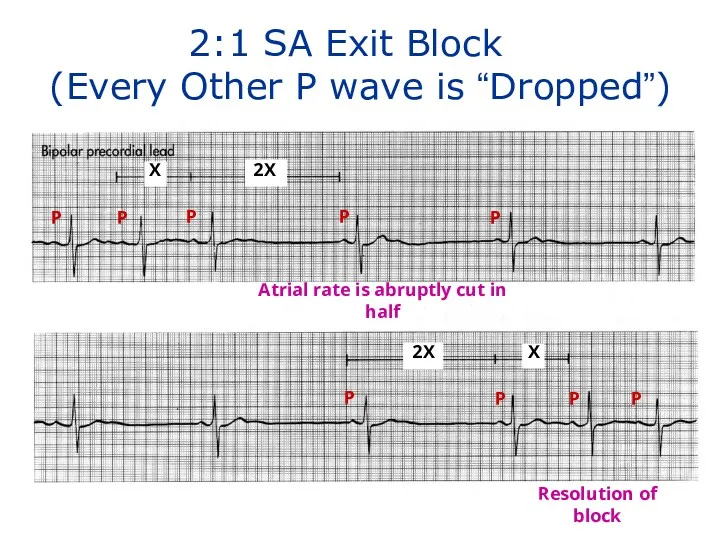
- 138. X 2X 2X X P P P P P P P P 2:1 SA Exit Block
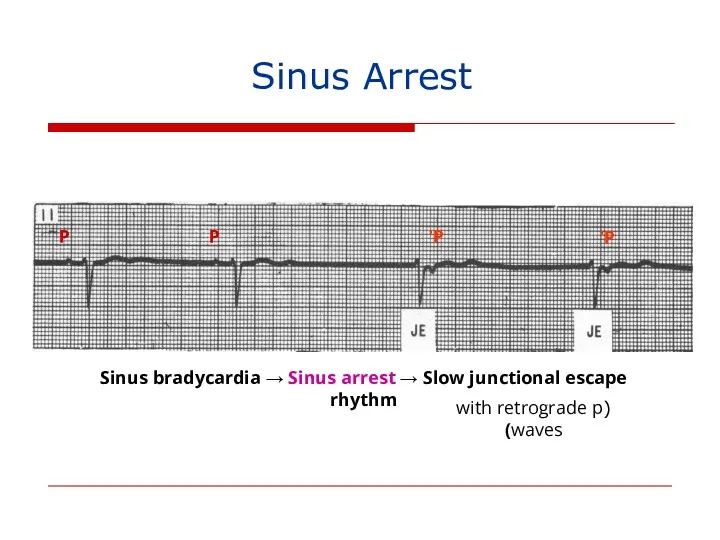
- 139. P P P’ P’ Sinus bradycardia → Sinus arrest → Slow junctional escape rhythm (with retrograde
- 140. Tachycardia-Bradycardia (Form of “Sick Sinus”) Syndrome Atrial Flutter Sinus arrest Junctional escape (tardy) Atrial Flutter terminates
- 141. Sinus Arrest → Asystole Sinus rhythm Sinus brady. → Sinus arrest → V. escape rhythm Failure
- 142. Causes of SA Exit Block and Sinus Pauses/Arrest Increased vagal tone (very intense for sinus arrest)
- 143. Sick Sinus Syndrome (1) persistent spontaneous sinus bradycardia not caused by drugs and inappropriate for the
- 146. Скачать презентацию
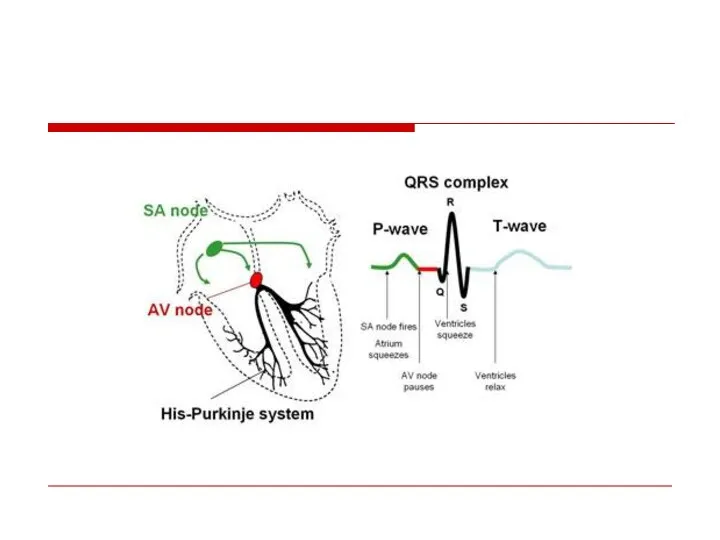
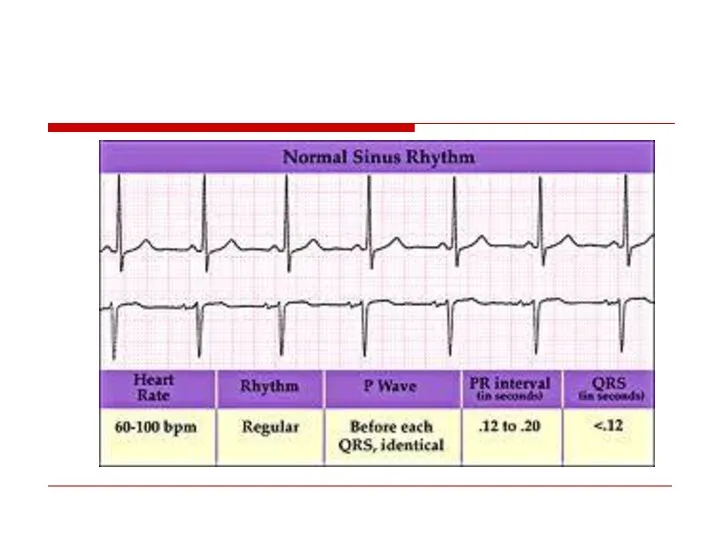
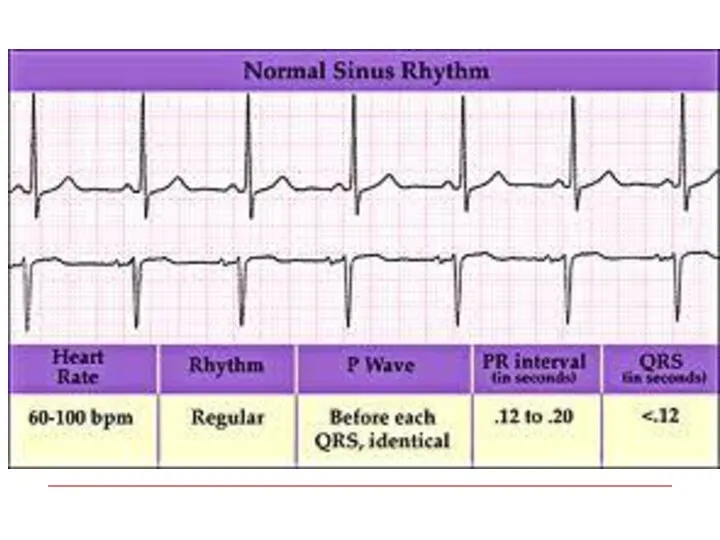
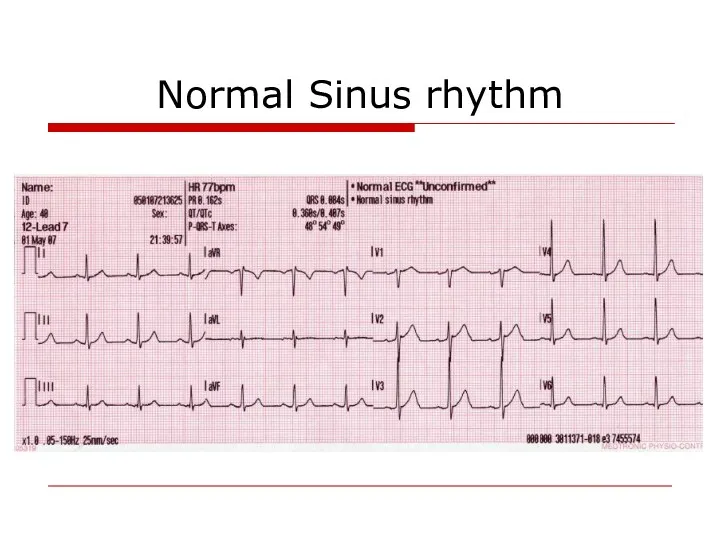
Normal Sinus rhythm
Normal Sinus rhythm
Classification
Tachyarrhythmia:
- Supraventricular
- Ventricular
Bradiarrhythmia
Classification
Tachyarrhythmia:
- Supraventricular
- Ventricular
Bradiarrhythmia
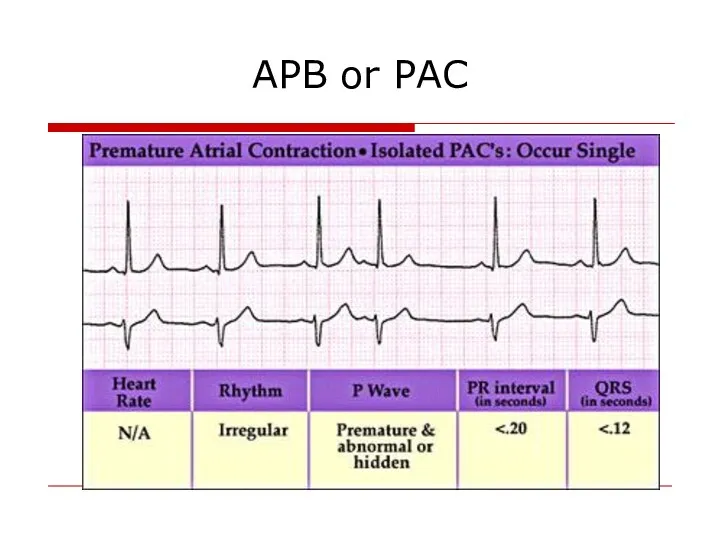
APB or PAC
APB or PAC
Atrial Fibrillation
The most common arrhythmia in clinical practice
Frequency increases with age
Atrial Fibrillation
The most common arrhythmia in clinical practice
Frequency increases with age
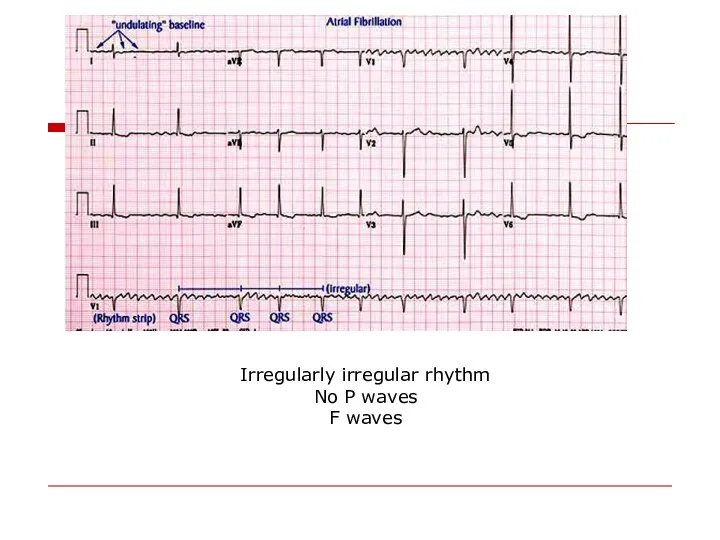
Irregularly irregular rhythm
No P waves
F waves
Irregularly irregular rhythm
No P waves
F waves
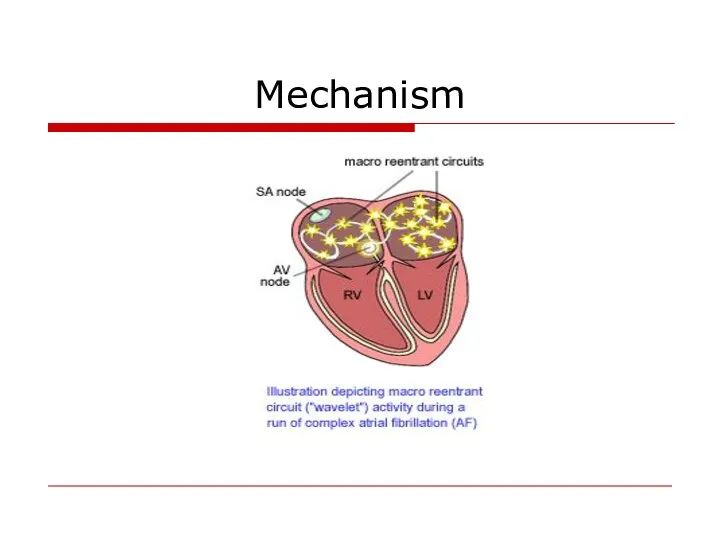
Mechanism
Mechanism
Most common causes
Valvular heart disease: (MS,MR)
LV hypertrophy (HTN, other cause)
Cardiomyopathy
Thyrotoxicosis
Alcohol (“holiday
Most common causes
Valvular heart disease: (MS,MR)
LV hypertrophy (HTN, other cause)
Cardiomyopathy
Thyrotoxicosis
Alcohol (“holiday
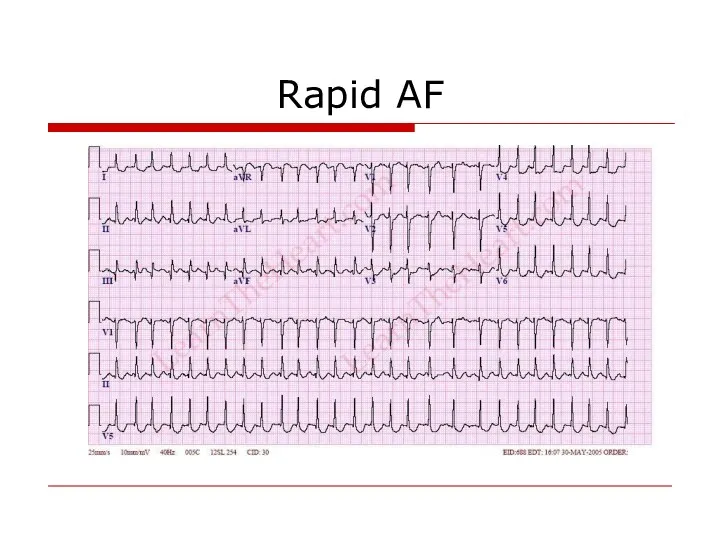
Rapid AF
Rapid AF
Consequences of Atrial Fibrillation
Hemodynamic
loss of synchronous atrial mechanical activity
irregularity of ventricular
Consequences of Atrial Fibrillation
Hemodynamic
loss of synchronous atrial mechanical activity
irregularity of ventricular
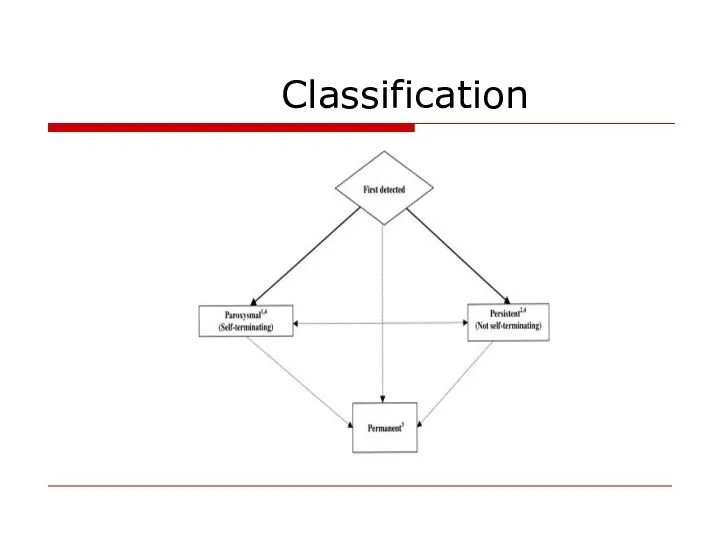
Classification
Classification
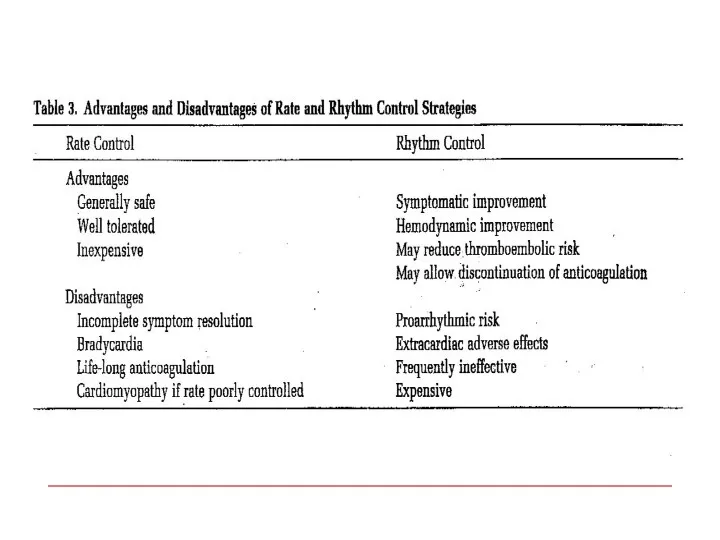
Treatment options
1. Rhythm control – restoration and maintenance of sinus rhythm
2.
Treatment options
1. Rhythm control – restoration and maintenance of sinus rhythm
2.
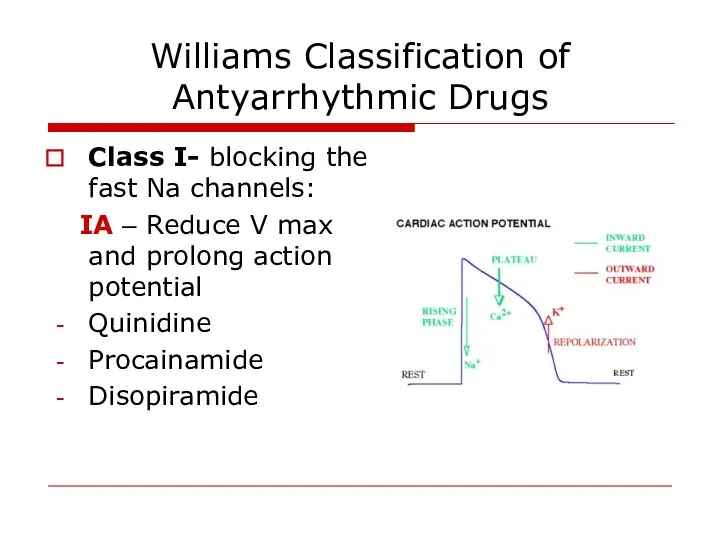
Williams Classification of Antyarrhythmic Drugs
Class I- blocking the fast Na channels:
Williams Classification of Antyarrhythmic Drugs
Class I- blocking the fast Na channels:
IB : Do not reduce V max and shorten action
IB : Do not reduce V max and shorten action
Class II – beta blockers
Class III – K channel blockers
-
Class II – beta blockers
Class III – K channel blockers
-
Cardioversion
Pharmacological
Propafenon
Amiodaron
Flecainide
Cardioversion
Pharmacological
Propafenon
Amiodaron
Flecainide
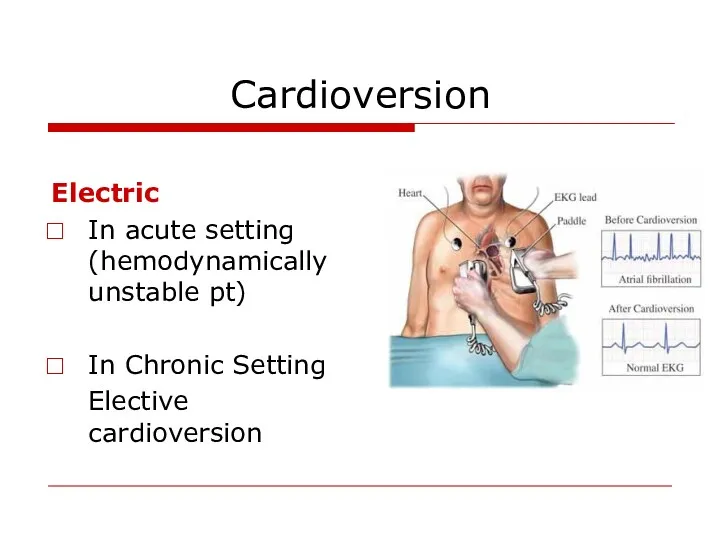
Cardioversion
Electric
In acute setting (hemodynamically unstable pt)
In Chronic Setting
Elective cardioversion
Cardioversion
Electric
In acute setting (hemodynamically unstable pt)
In Chronic Setting
Elective cardioversion
Predictors of successful cardioverson
Short AF duration
Young age
Normal atrial size
No organic heart
Predictors of successful cardioverson
Short AF duration
Young age
Normal atrial size
No organic heart
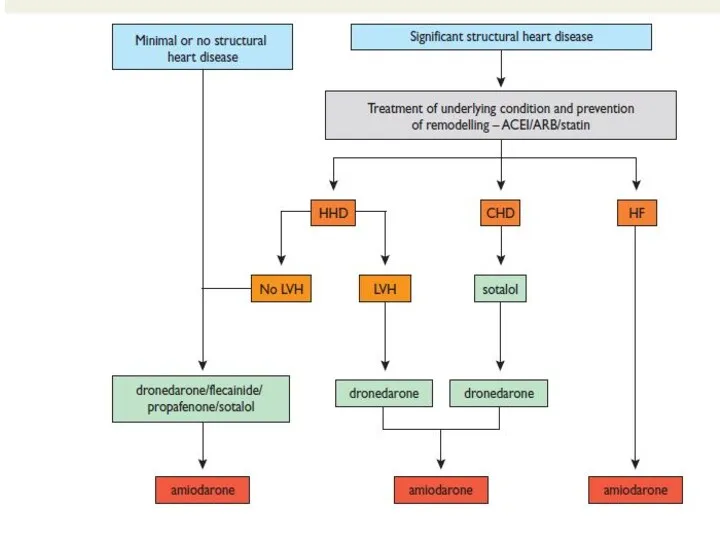
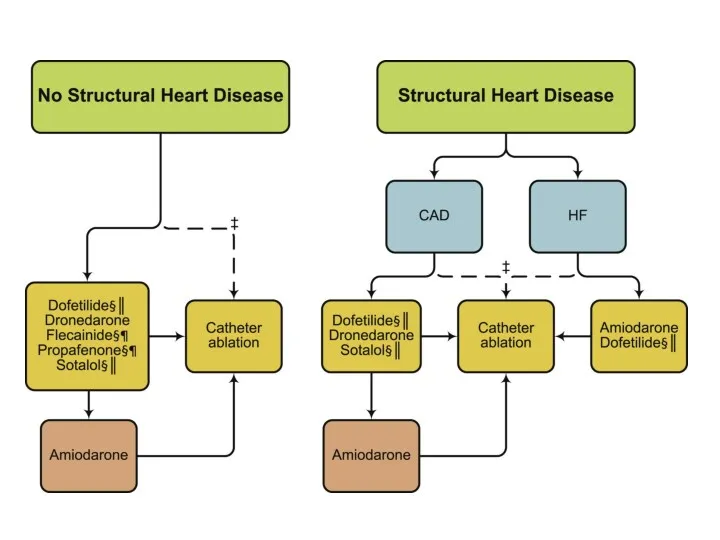
Maintenance of sinus rhythm
Propafenon
Amiodaron
Dronedaron
Sotalol
Flecainide
Maintenance of sinus rhythm
Propafenon
Amiodaron
Dronedaron
Sotalol
Flecainide
Rate Control
Acute setting – IV
- Esmolol
- Metoprolol
- Verapamil
Rate Control
Acute setting – IV
- Esmolol
- Metoprolol
- Verapamil
– Severe symptoms due to AF
– Patients with CHF
– Younger patients
–
– Severe symptoms due to AF
– Patients with CHF
– Younger patients
–
Rate Control as First-Line Choice
Consider rate control as first-line therapy if:
–
Rate Control as First-Line Choice
Consider rate control as first-line therapy if:
–
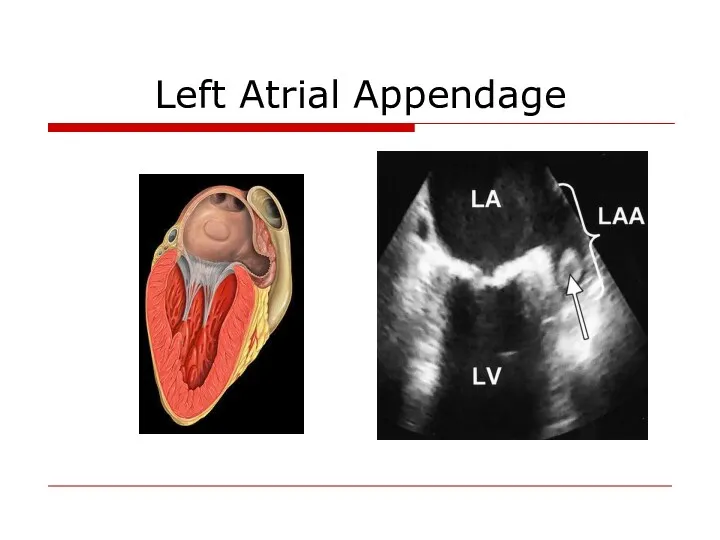
Left Atrial Appendage
Left Atrial Appendage
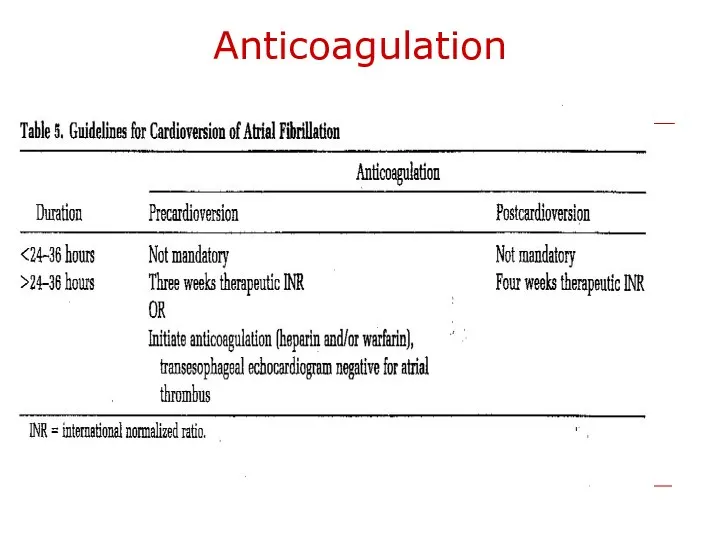
Anticoagulation
Anticoagulation
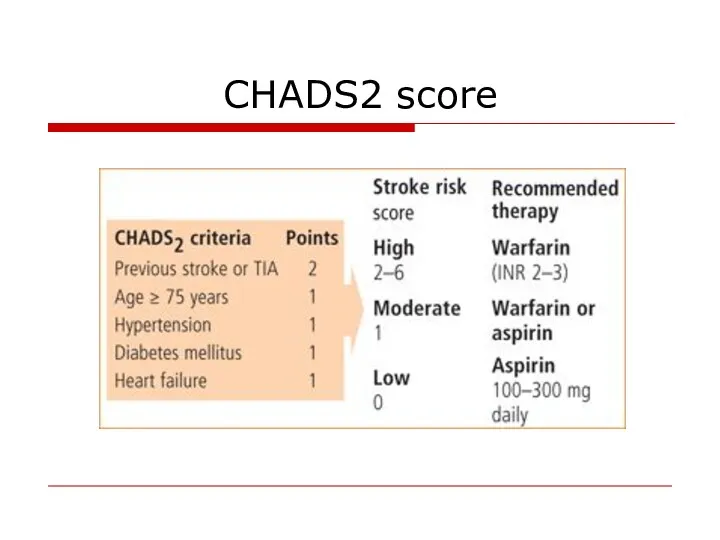
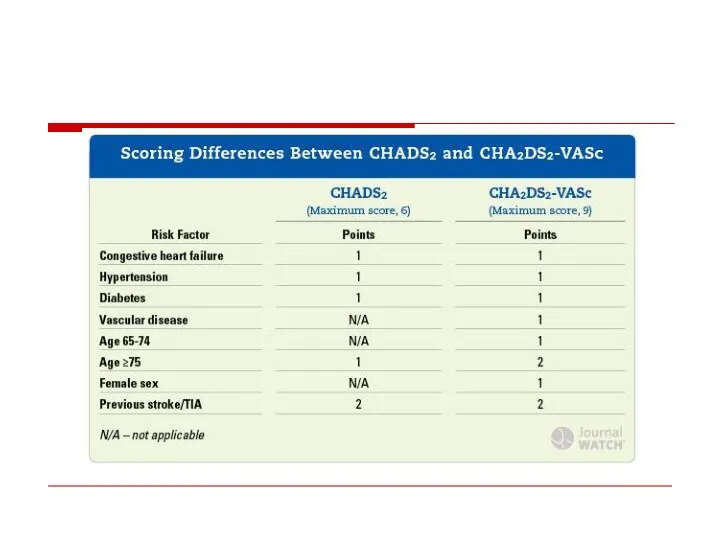
CHADS2 score
CHADS2 score
Novel Oral Anticoagulants
Dabigatran (Pradaxa)- direct oral thrombin inhibitor
Rivaroxaban (Xarelto)– direct oral
Novel Oral Anticoagulants
Dabigatran (Pradaxa)- direct oral thrombin inhibitor
Rivaroxaban (Xarelto)– direct oral
Invasive AF treatment
Invasive AF treatment
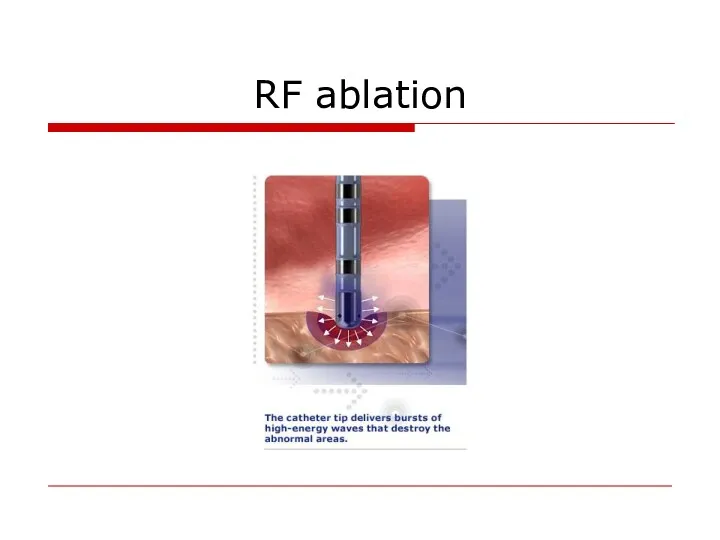
RF ablation
RF ablation
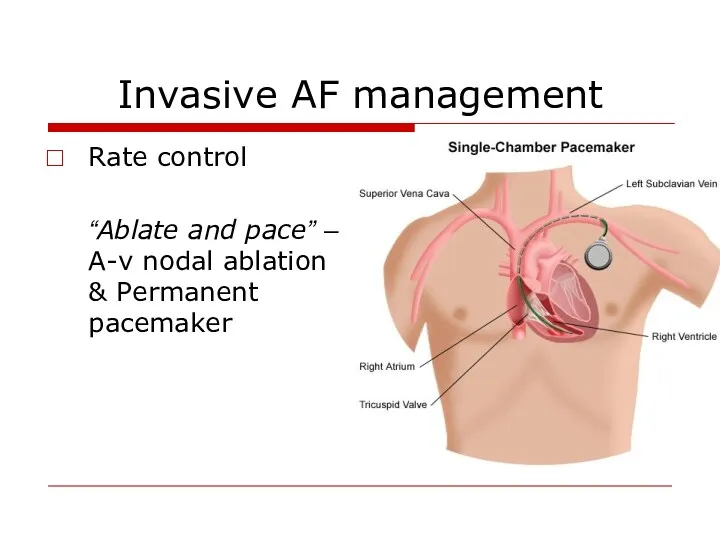
Invasive AF management
Rate control
“Ablate and pace” – A-v nodal
Invasive AF management
Rate control
“Ablate and pace” – A-v nodal
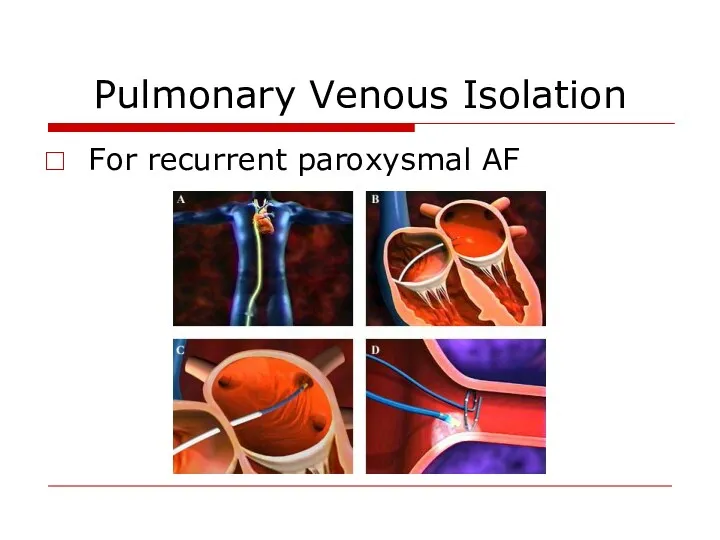
Pulmonary Venous Isolation
For recurrent paroxysmal AF
Pulmonary Venous Isolation
For recurrent paroxysmal AF
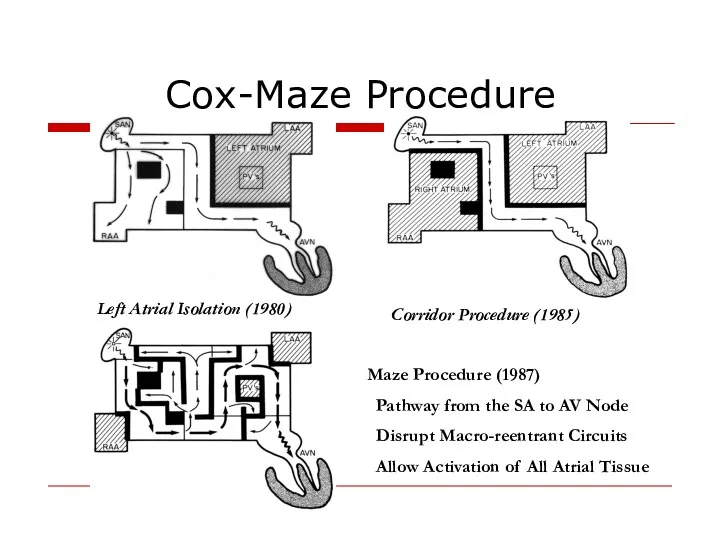
Cox-Maze Procedure
Left Atrial Isolation (1980)
Corridor Procedure (1985)
Maze Procedure (1987)
Pathway from
Cox-Maze Procedure
Left Atrial Isolation (1980)
Corridor Procedure (1985)
Maze Procedure (1987)
Pathway from
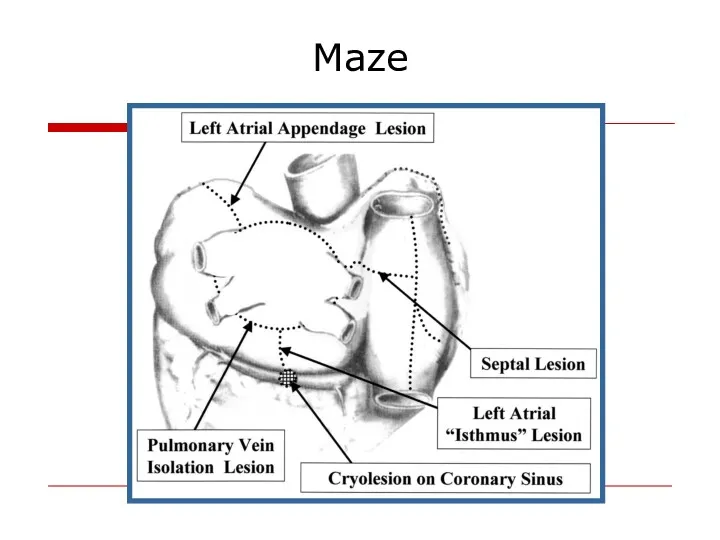
Maze
Maze
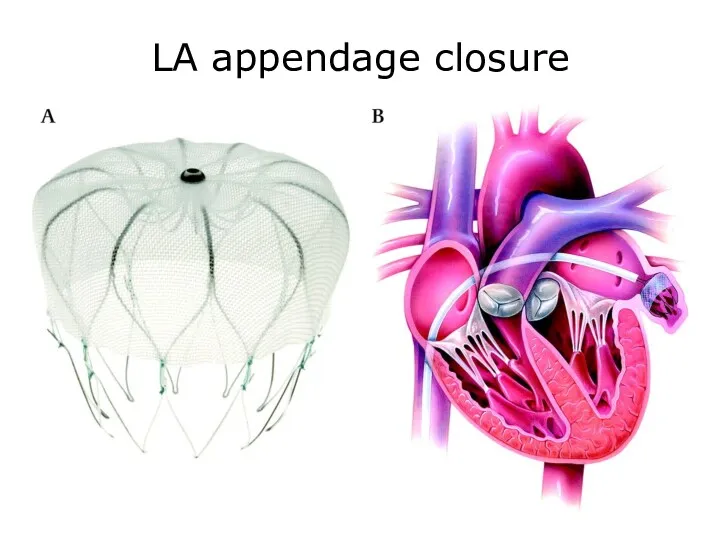
LA appendage closure
LA appendage closure
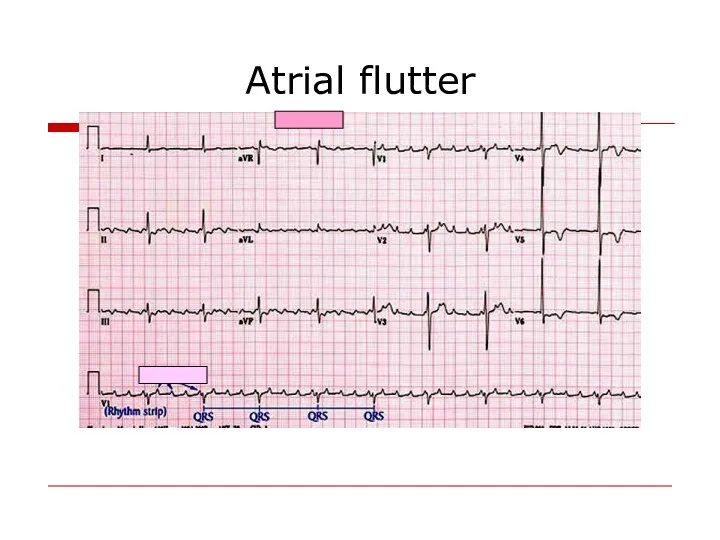
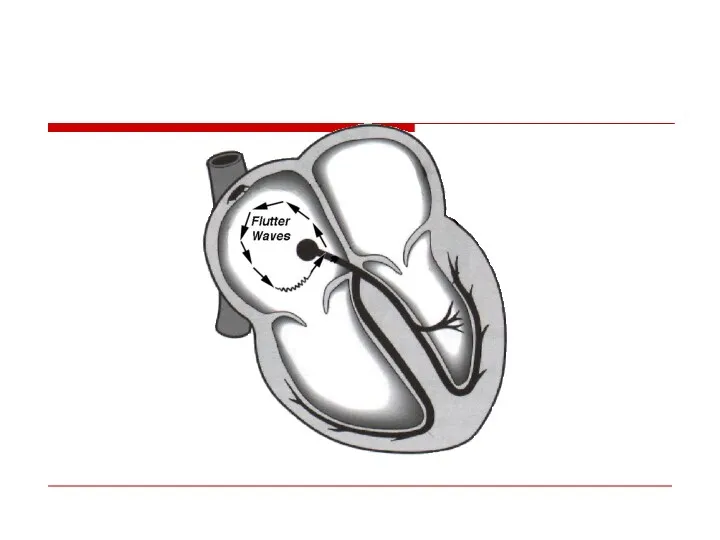
Atrial flutter
Atrial flutter
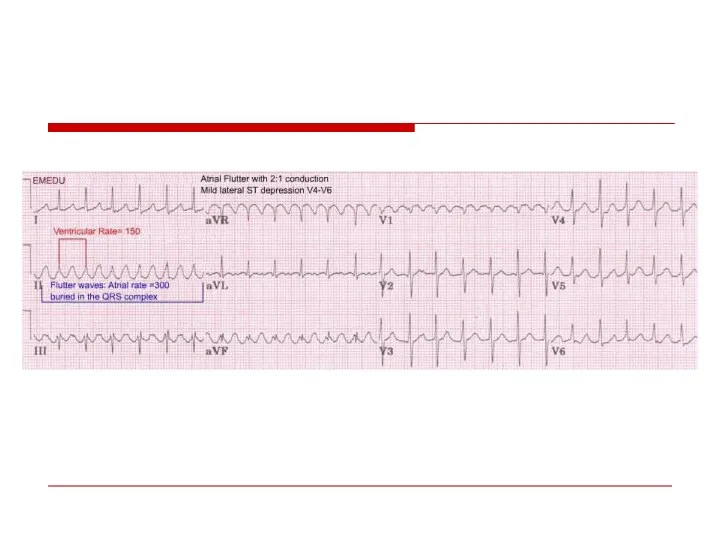
Management
Electric Cardioversion
Slowing Ventricular rate
- Beta Blockers
- Ca Channel blocker
Management
Electric Cardioversion
Slowing Ventricular rate
- Beta Blockers
- Ca Channel blocker
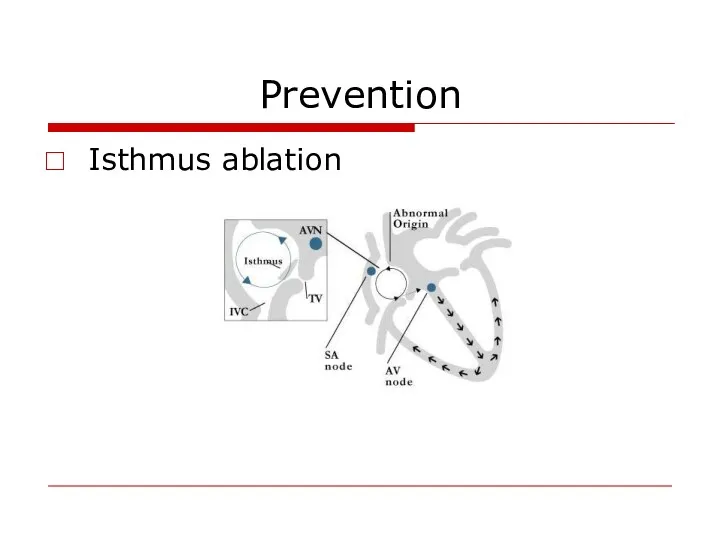
Prevention
Isthmus ablation
Prevention
Isthmus ablation
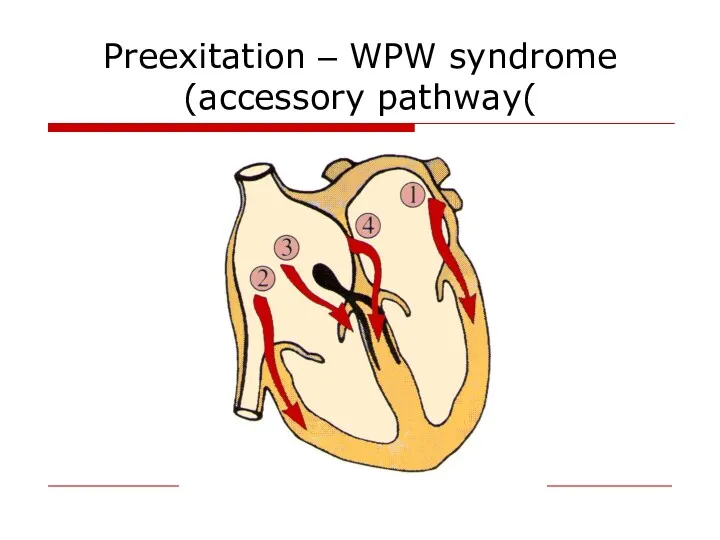
Preexitation – WPW syndrome
(accessory pathway(
Preexitation – WPW syndrome
(accessory pathway(
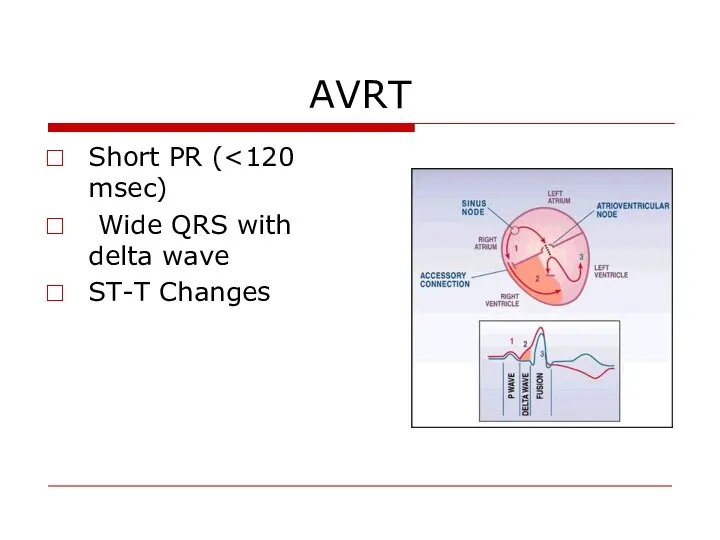
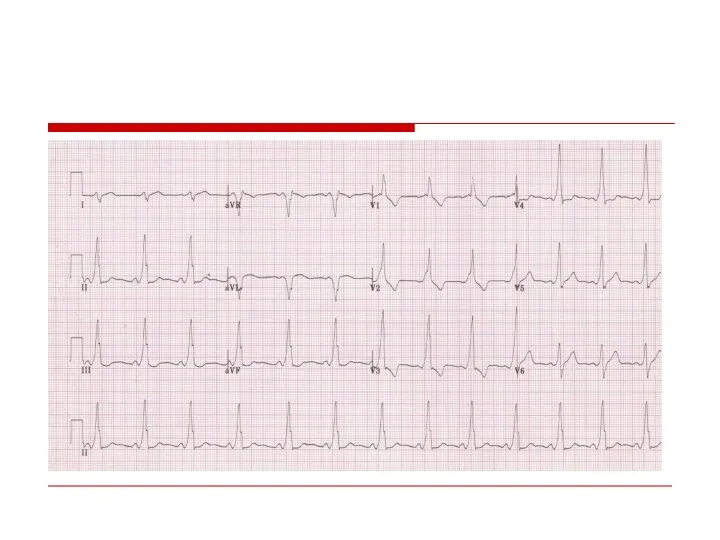
AVRT
Short PR (<120 msec)
Wide QRS with delta wave
ST-T Changes
AVRT
Short PR (<120 msec)
Wide QRS with delta wave
ST-T Changes
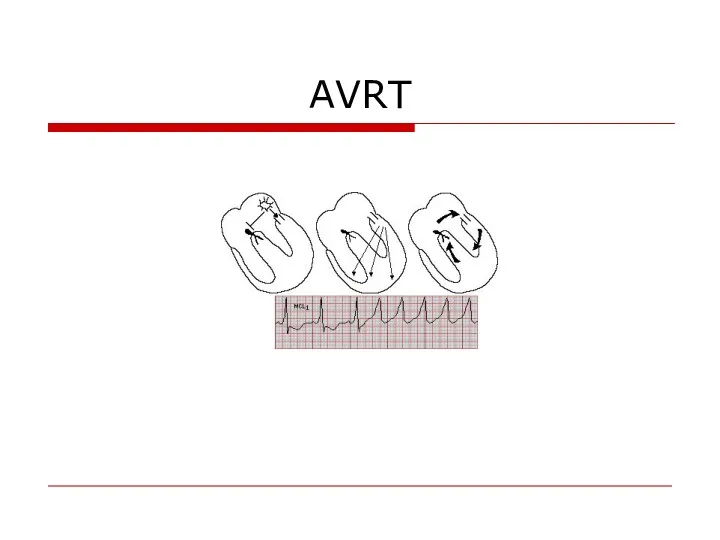
AVRT
AVRT
AVRT
AVRT
Treatment
Acute treatment:
Wide complex – Procainamide
DC Shock
Narrow complex –
Treatment
Acute treatment:
Wide complex – Procainamide
DC Shock
Narrow complex –
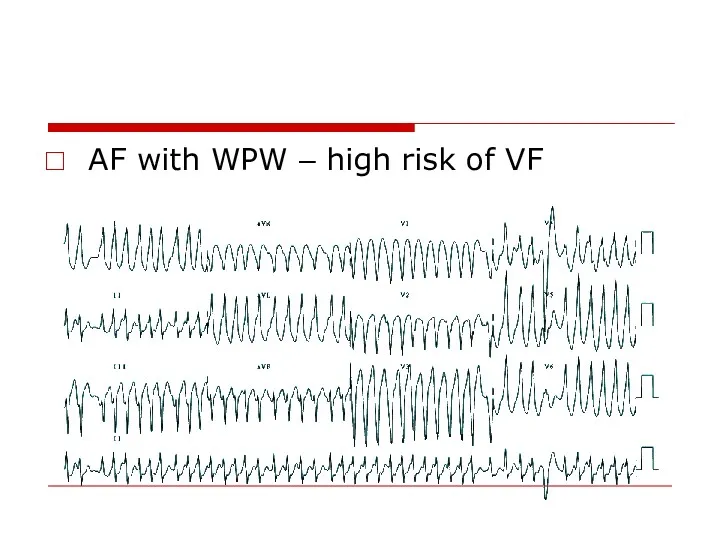
AF with WPW – high risk of VF
AF with WPW – high risk of VF
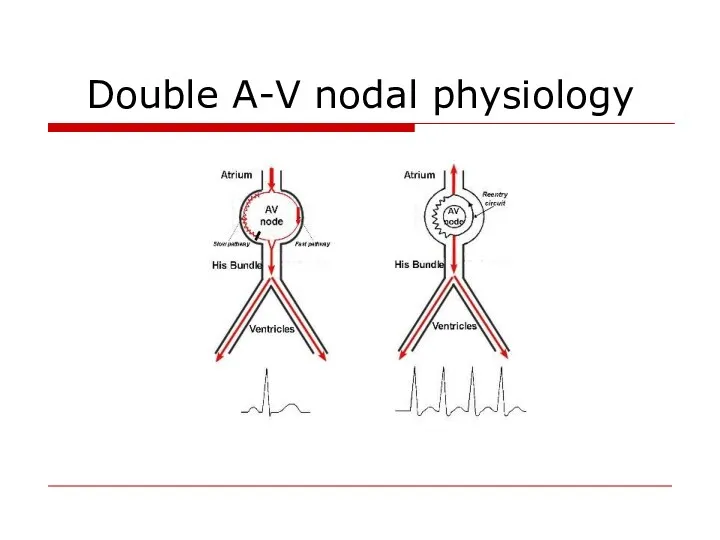
Double A-V nodal physiology
Double A-V nodal physiology
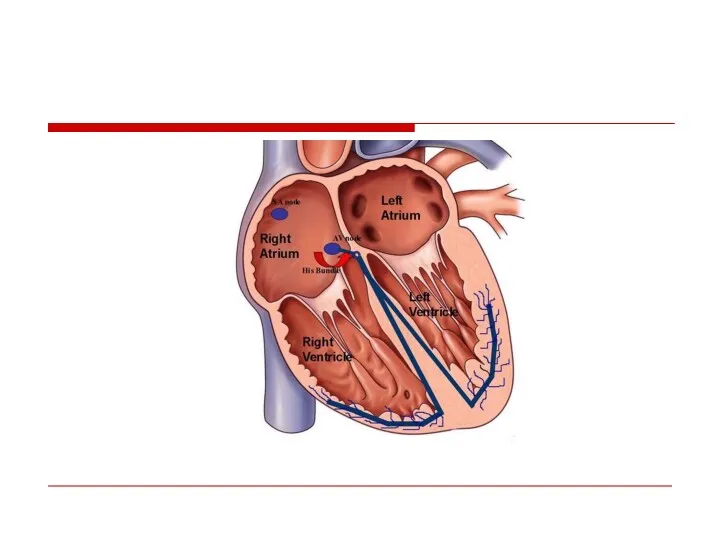
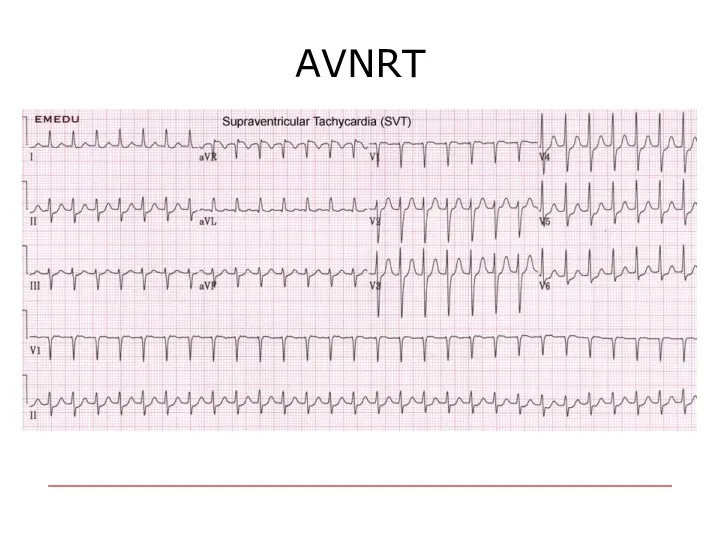
AVNRT
AVNRT
Management of narrow complex SVT
If unstable – DC shock
If Stable :
Management of narrow complex SVT
If unstable – DC shock
If Stable :
Preventive treatment
Drugs
EPS
Preventive treatment
Drugs
EPS
Ventricular Arrhythmias
Ventricular Arrhythmias
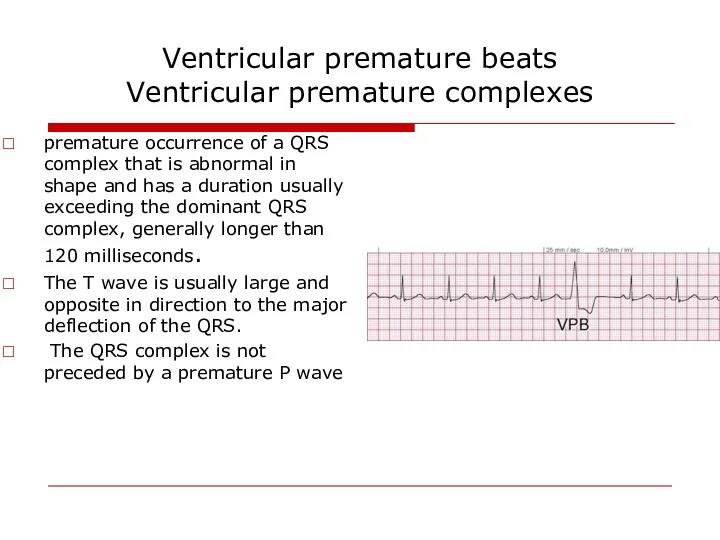
Ventricular premature beats
Ventricular premature complexes
premature occurrence of a QRS complex
Ventricular premature beats
Ventricular premature complexes
premature occurrence of a QRS complex
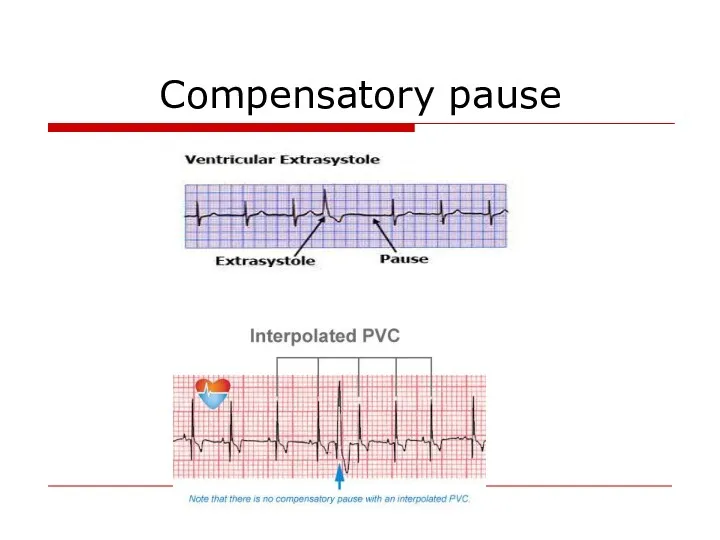
Compensatory pause
Compensatory pause
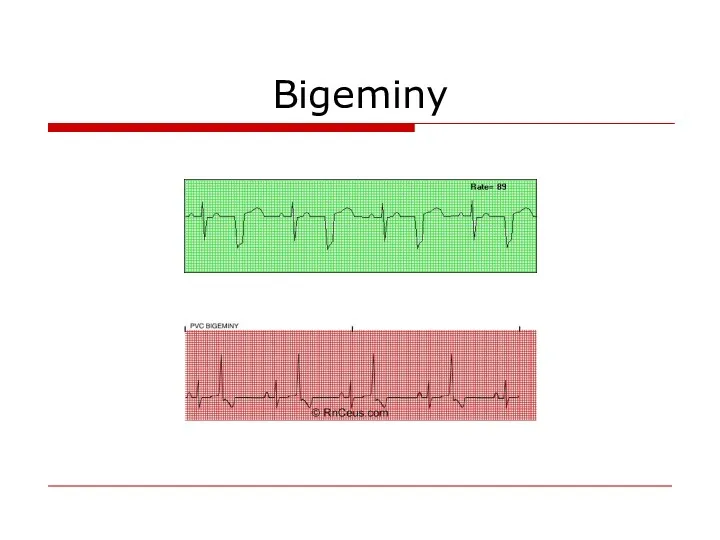
Bigeminy
Bigeminy
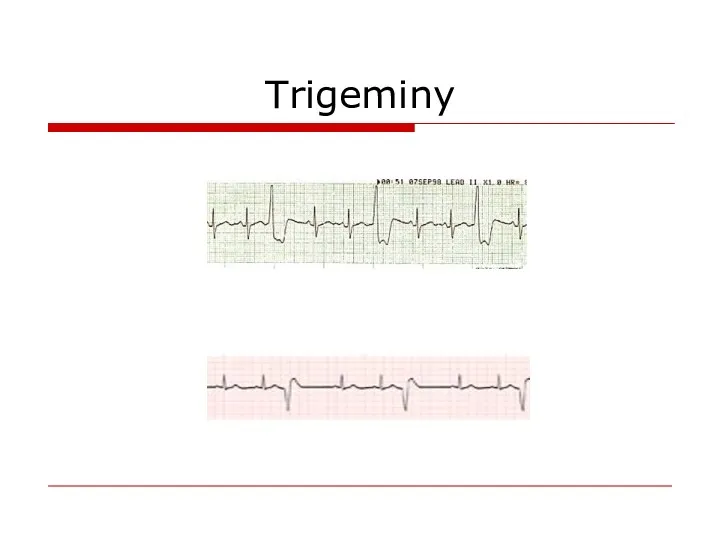
Trigeminy
Trigeminy
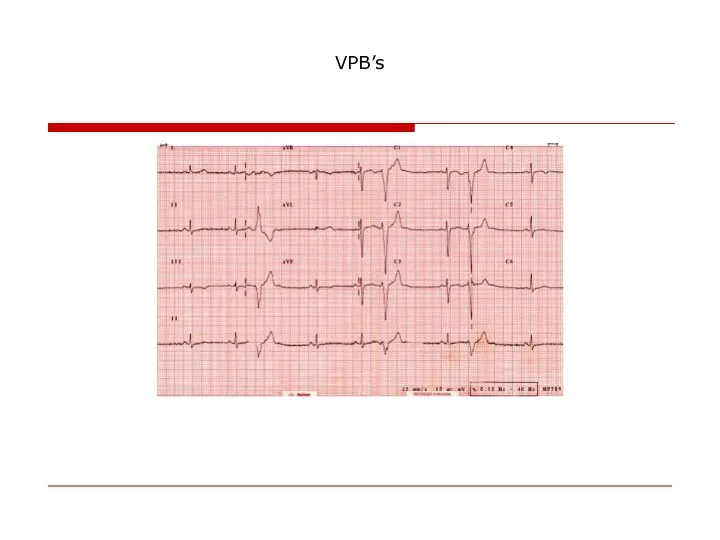
VPB’s
VPB’s
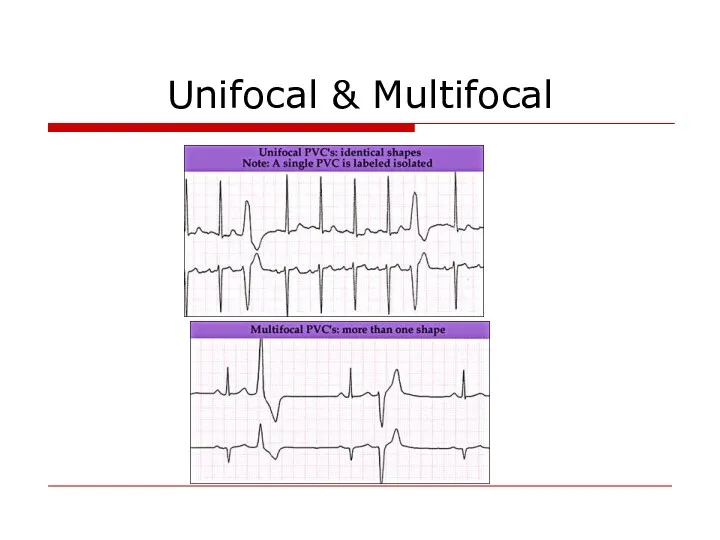
Unifocal & Multifocal
Unifocal & Multifocal
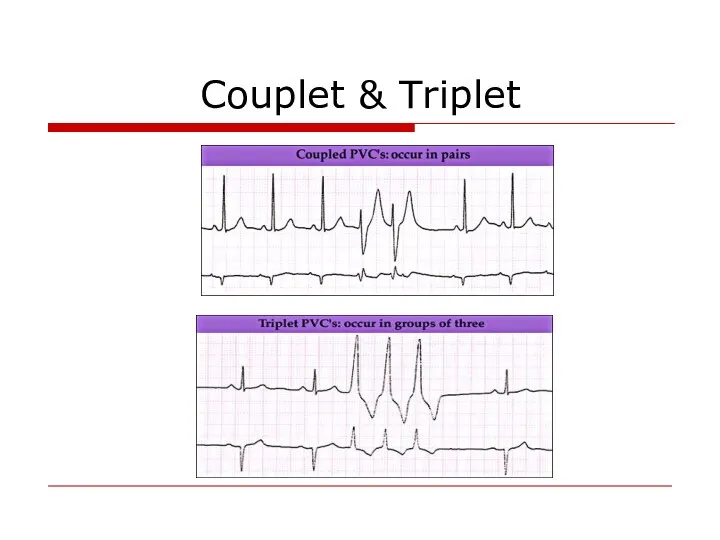
Couplet & Triplet
Couplet & Triplet
Causes
LV false tendons,
infection
in ischemic or inflamed myocardium,
hypoxia,
Anesthesiaor
Causes
LV false tendons,
infection
in ischemic or inflamed myocardium,
hypoxia,
Anesthesiaor
Complex Ventricular Arrhythmia
Nonsustained ventricular tachycardia (VT)
♥ Monomorphic
♥ Polymorphic
Sustained VT
♥ Monomorphic
♥ Polymorphic
Torsades
Complex Ventricular Arrhythmia
Nonsustained ventricular tachycardia (VT)
♥ Monomorphic
♥ Polymorphic
Sustained VT
♥ Monomorphic
♥ Polymorphic
Torsades
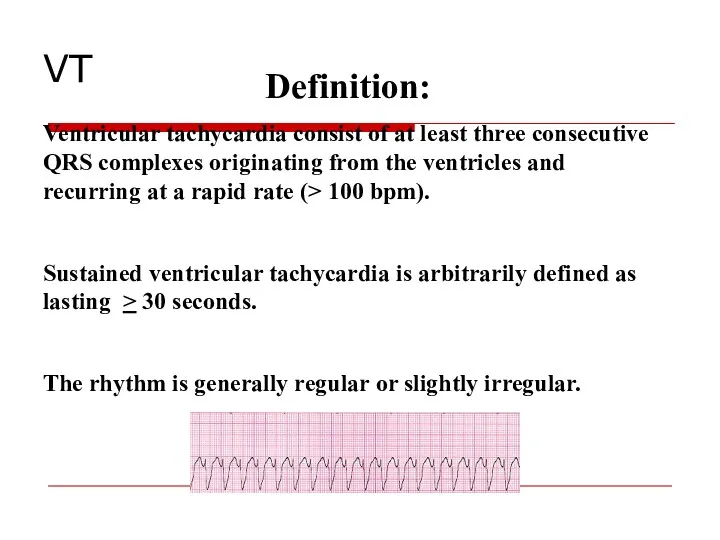
Definition:
Ventricular tachycardia consist of at least three consecutive QRS complexes originating
Definition:
Ventricular tachycardia consist of at least three consecutive QRS complexes originating
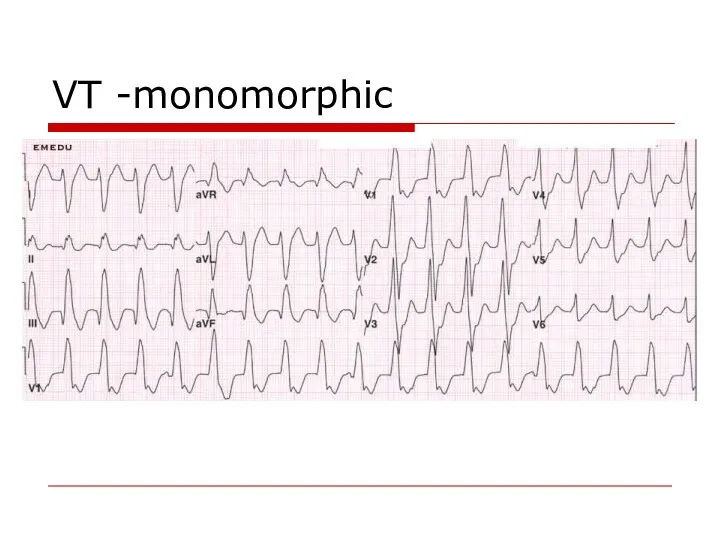
VT -monomorphic
VT -monomorphic
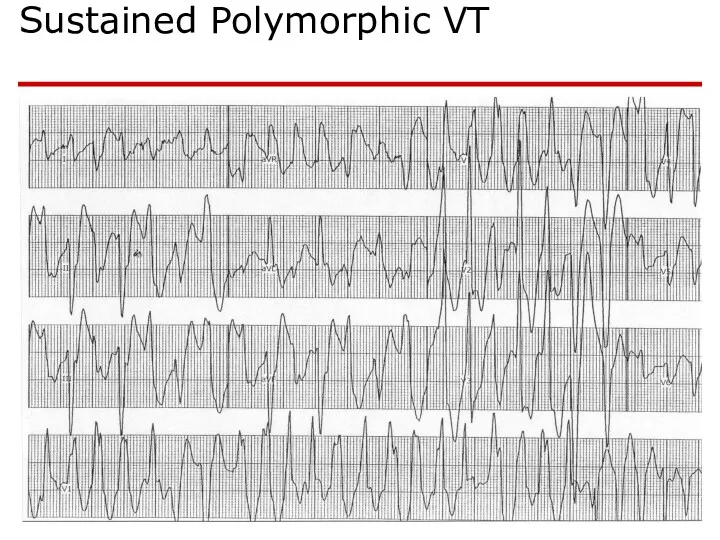
Sustained Polymorphic VT
Sustained Polymorphic VT
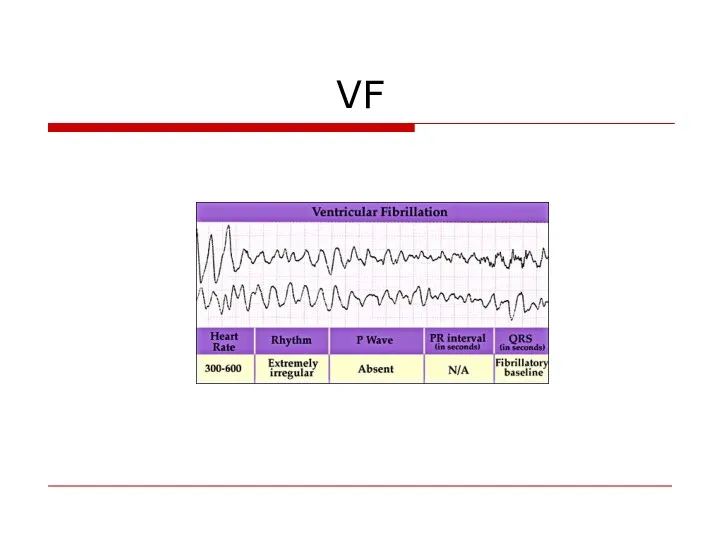
VF
VF
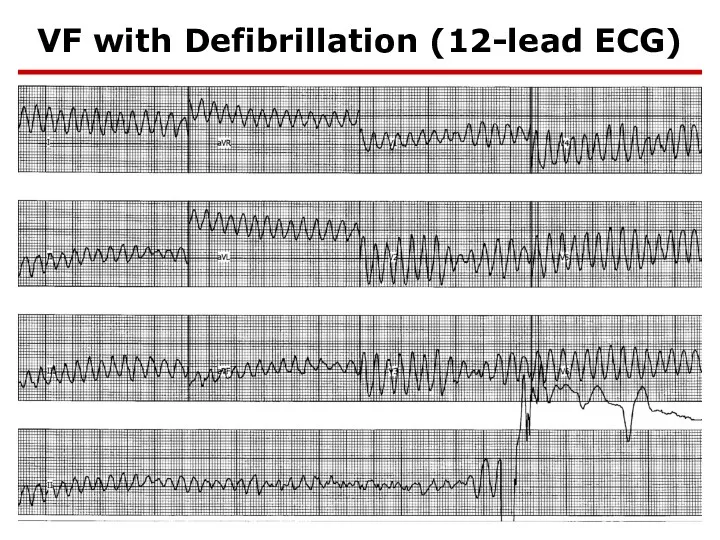
VF with Defibrillation (12-lead ECG)
VF with Defibrillation (12-lead ECG)
Causes
Chronic coronary heart disease
Heart failure
Congenital heart disease
Neurological disorders
Structurally normal hearts
Sudden infant
Causes
Chronic coronary heart disease
Heart failure
Congenital heart disease
Neurological disorders
Structurally normal hearts
Sudden infant
Ventricular fibrillation - 62.4%
Bradyarrhythmias (including advanced AV block and asystole) -
Ventricular fibrillation - 62.4%
Bradyarrhythmias (including advanced AV block and asystole) -
VA management
Acute
Chronic (secondary prevention)
VA management
Acute
Chronic (secondary prevention)
Sustained VT
Hemodynamically stable:
- Amiodaron
- Lidocain
- Procainamide
If pfarmacotherapy ineffective
Sustained VT
Hemodynamically stable:
- Amiodaron
- Lidocain
- Procainamide
If pfarmacotherapy ineffective
Polymorphic VT
Polymorphic VT with long QT – Torsades de pointes
Treatment
Polymorphic VT
Polymorphic VT with long QT – Torsades de pointes
Treatment
Chronic Management (secondary prevention)
Evaluation
- Rest ECG
- Exersise test
-
Chronic Management (secondary prevention)
Evaluation
- Rest ECG
- Exersise test
-
Treatment of the underlying disease
Revascularisation
Valve surgery
CHD repair
Treatment of the underlying disease
Revascularisation
Valve surgery
CHD repair
♥ Electrolytes: Mg & K
♥ ACE inhibitors,
♥ Antithrombotic and antiplatelet
♥ ACE inhibitors,
♥ Antithrombotic and antiplatelet
Antiarrhytmic drugs
Antiarrhythmic drugs (except for BB) should not be used as
Antiarrhytmic drugs
Antiarrhythmic drugs (except for BB) should not be used as
Invasive treatment
AICD
EPS with ablation
Surgical ablation
Invasive treatment
AICD
EPS with ablation
Surgical ablation
AICD for primary prevention of SCD
1.Post MI
- LVEF < 30%
AICD for primary prevention of SCD
1.Post MI
- LVEF < 30%
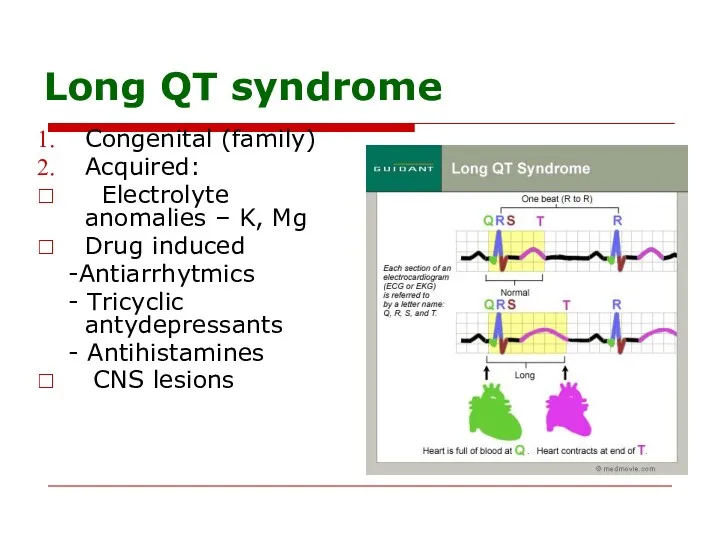
Long QT syndrome
Congenital (family)
Acquired:
Electrolyte anomalies – K, Mg
Drug induced
-Antiarrhytmics
Long QT syndrome
Congenital (family)
Acquired:
Electrolyte anomalies – K, Mg
Drug induced
-Antiarrhytmics
Long QT syndrome treatment
Acute
1.Remove the precipitating factor
2. Mg IV
3. Pacing
4.
Long QT syndrome treatment
Acute
1.Remove the precipitating factor
2. Mg IV
3. Pacing
4.
Long QT syndrome treatment
Chronic – for congenital long QT
1.Beta
Long QT syndrome treatment
Chronic – for congenital long QT
1.Beta
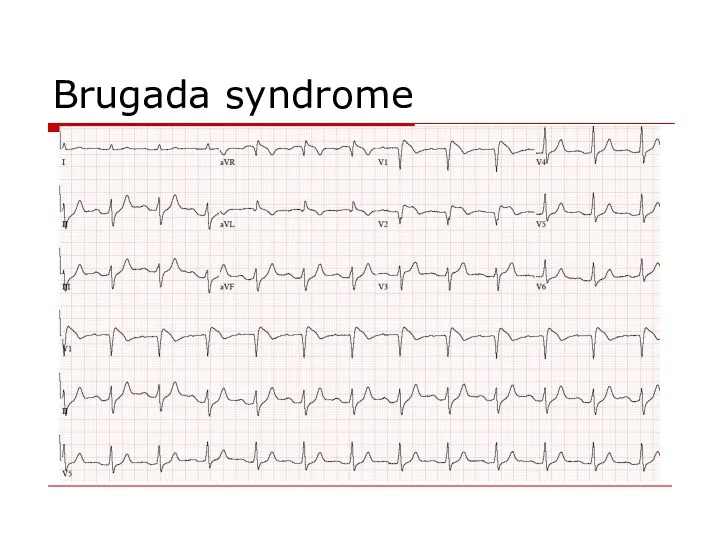
Brugada syndrome
Brugada syndrome
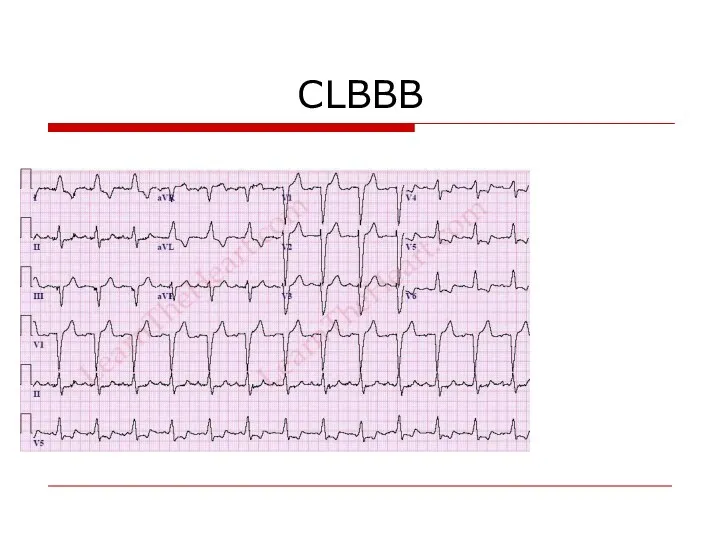
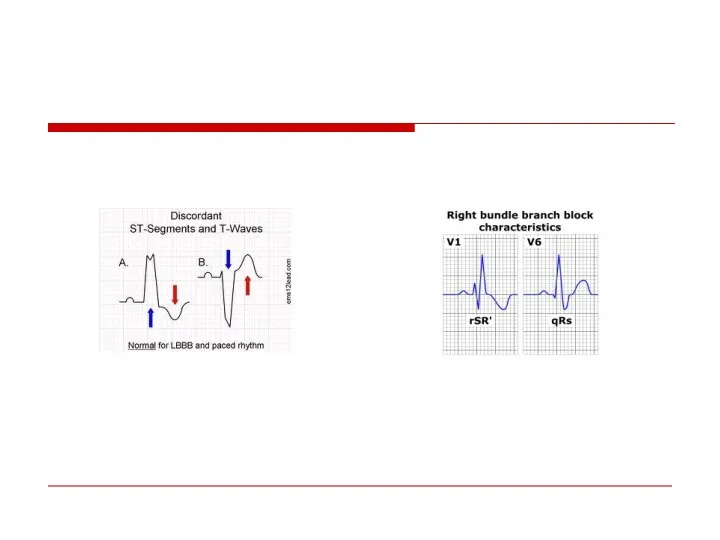
CLBBB
CLBBB
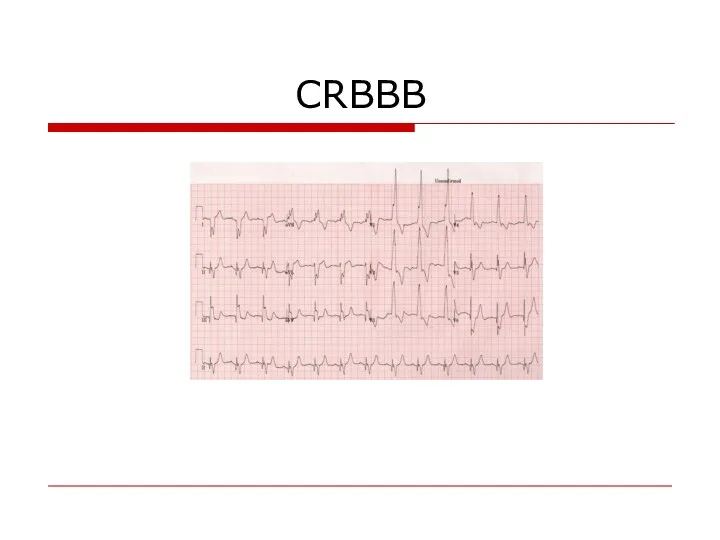
CRBBB
CRBBB
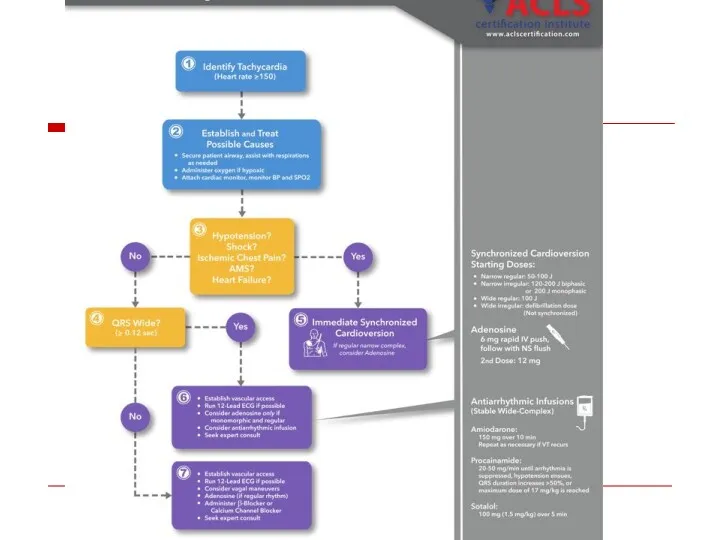
“Wide Complex Tachycardia”
VT
SVT with
Preexistent BBB
Rate dependent BBB
Preexitation
“Wide Complex Tachycardia”
VT
SVT with
Preexistent BBB
Rate dependent BBB
Preexitation
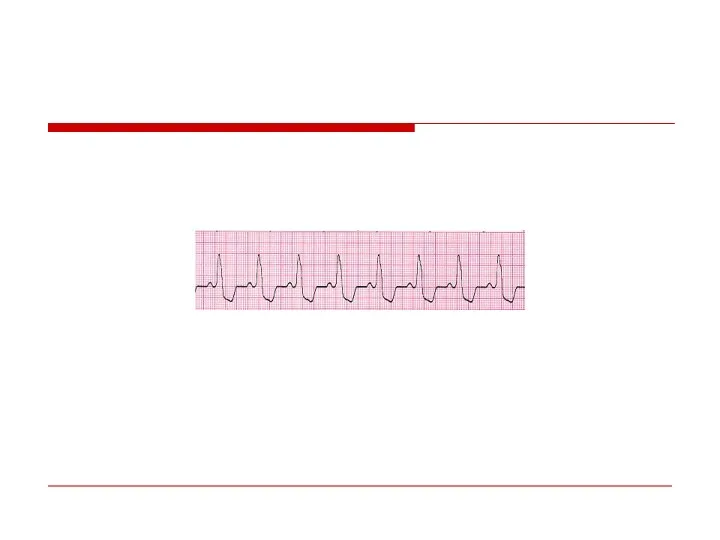
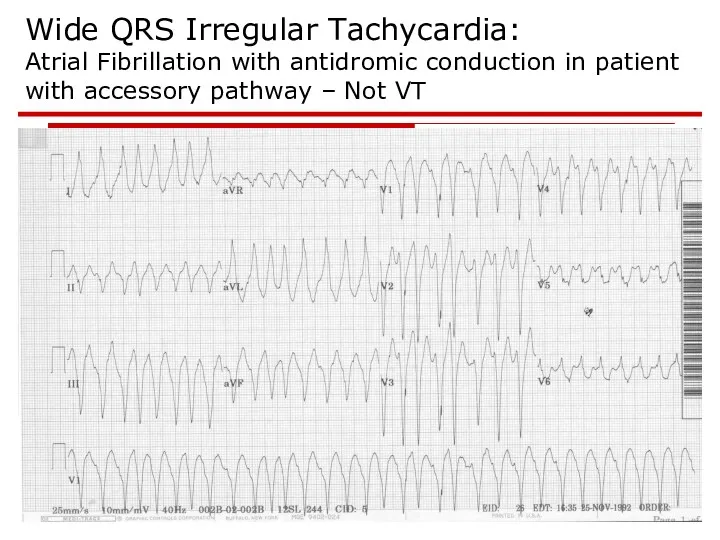
Wide QRS Irregular Tachycardia:
Atrial Fibrillation with antidromic conduction in patient with
Wide QRS Irregular Tachycardia: Atrial Fibrillation with antidromic conduction in patient with
AV Dissociation
QRS > 0.14
QRS Axis between – 90 & - 180
AV Dissociation
QRS > 0.14
QRS Axis between – 90 & - 180
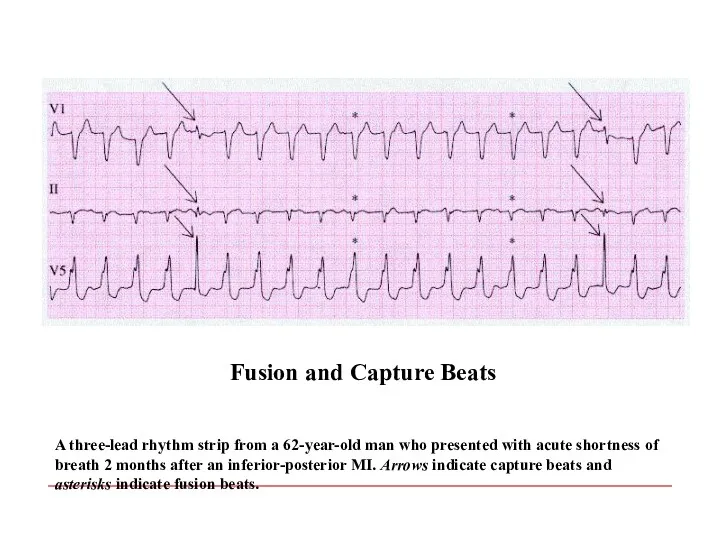
A three-lead rhythm strip from a 62-year-old man who presented with
A three-lead rhythm strip from a 62-year-old man who presented with
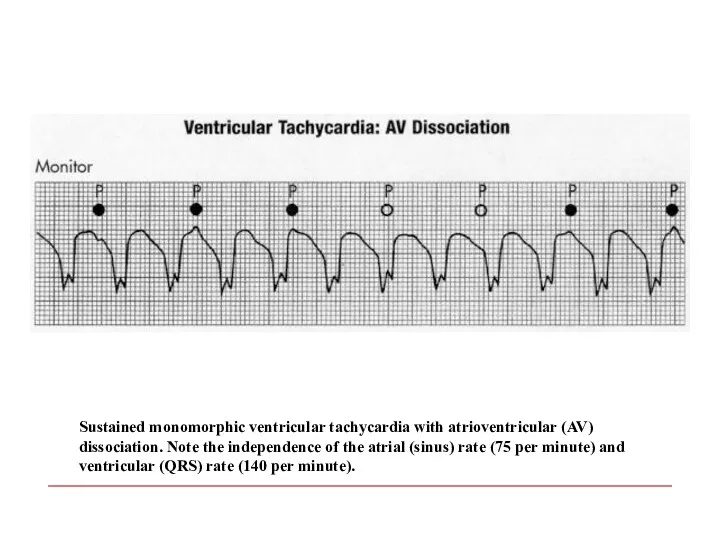
Sustained monomorphic ventricular tachycardia with atrioventricular (AV) dissociation. Note the independence
Sustained monomorphic ventricular tachycardia with atrioventricular (AV) dissociation. Note the independence
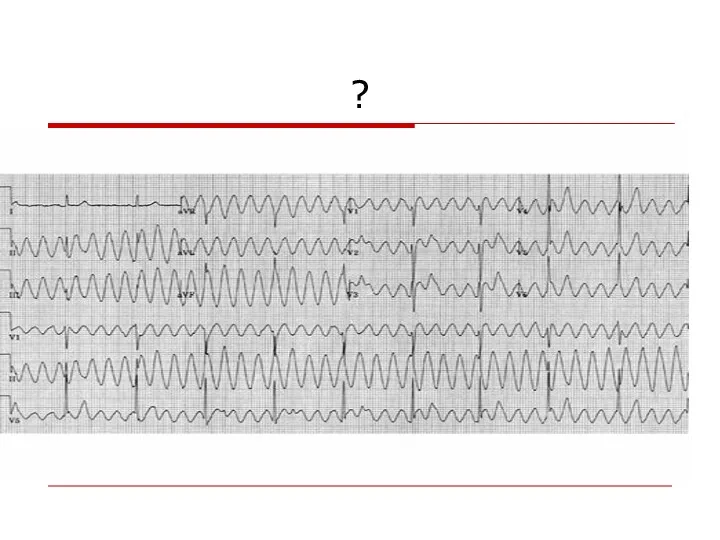
?
?
Atrioventricular Conduction Disturbances and Bradyarrhythmias
Atrioventricular Conduction Disturbances and Bradyarrhythmias
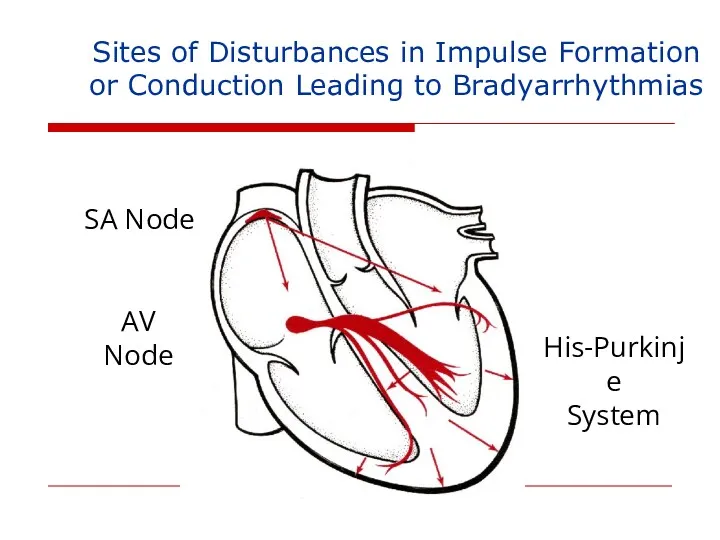
Sites of Disturbances in Impulse Formation
or Conduction Leading to Bradyarrhythmias
SA
Sites of Disturbances in Impulse Formation
or Conduction Leading to Bradyarrhythmias
SA
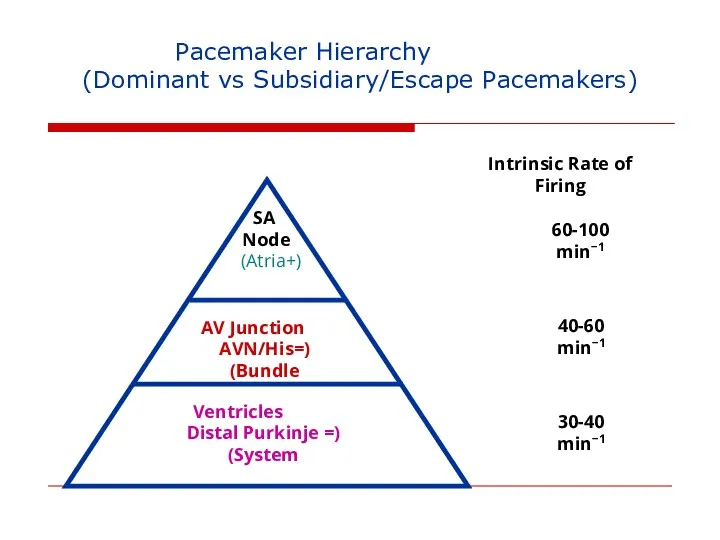
Pacemaker Hierarchy
(Dominant vs Subsidiary/Escape Pacemakers)
SA
Node
(+Atria)
AV
Pacemaker Hierarchy
(Dominant vs Subsidiary/Escape Pacemakers)
SA
Node
(+Atria)
AV
AV Block
AV Block
AV Block - Definitions
First Degree: Prolonged conduction time
Second Degree: Intermittent non-conduction
Third
AV Block - Definitions
First Degree: Prolonged conduction time
Second Degree: Intermittent non-conduction
Third
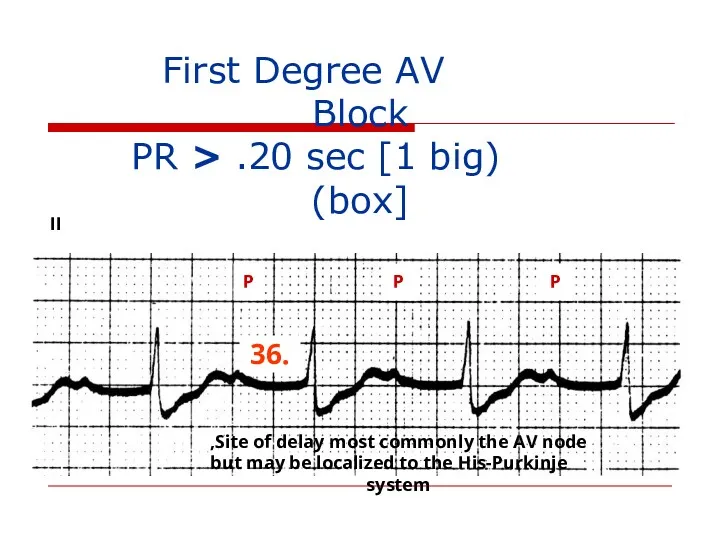
First Degree AV Block
(PR > .20 sec [1 big
First Degree AV Block
(PR > .20 sec [1 big
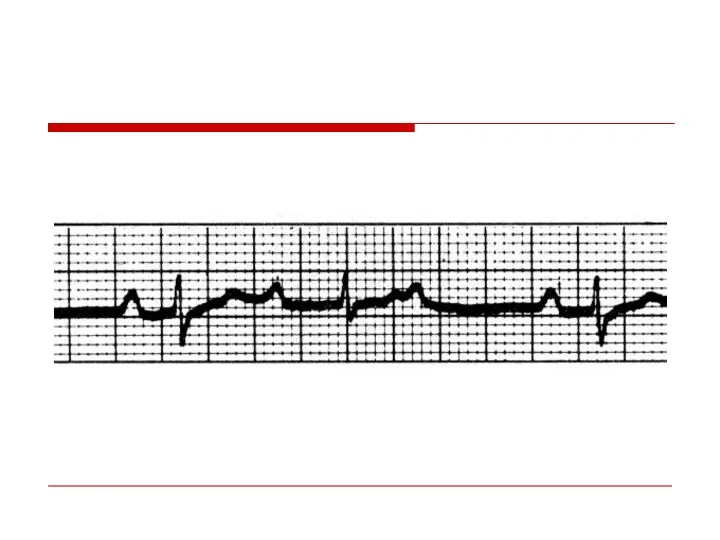
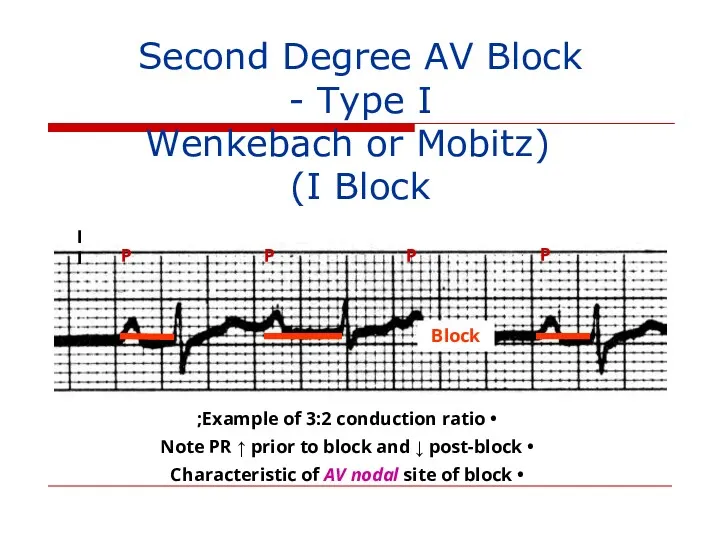
Second Degree AV Block - Type I
(Wenkebach or Mobitz I
Second Degree AV Block - Type I
(Wenkebach or Mobitz I
II
Block
P
P
P
P
P
4:3 conduction ratio
Note first RR longer than second RR
Second
II
Block
P
P
P
P
P
4:3 conduction ratio
Note first RR longer than second RR
Second
II
II
II
P
P
P
P
P
P
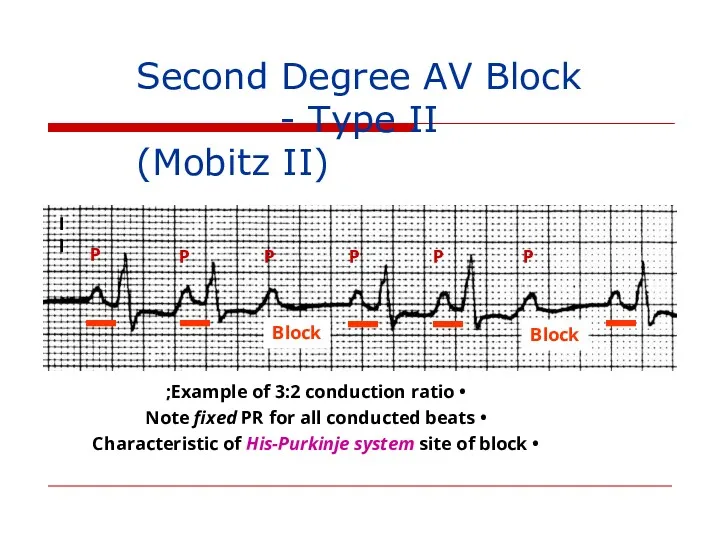
Second Degree AV Block - Type II
(Mobitz II)
Example of
II
P
P
P
P
P
P
Second Degree AV Block - Type II
(Mobitz II)
Example of
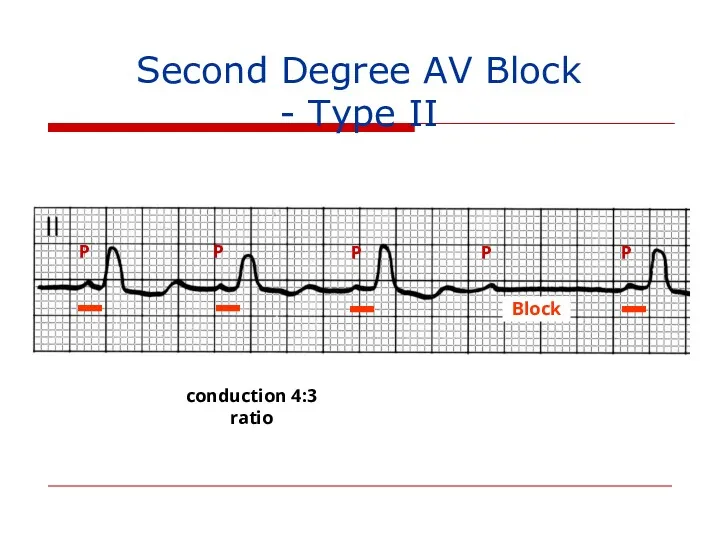
Second Degree AV Block - Type II
P
P
P
P
P
4:3 conduction ratio
Block
Second Degree AV Block - Type II
P
P
P
P
P
4:3 conduction ratio
Block
II
P
P
P
P
P
P
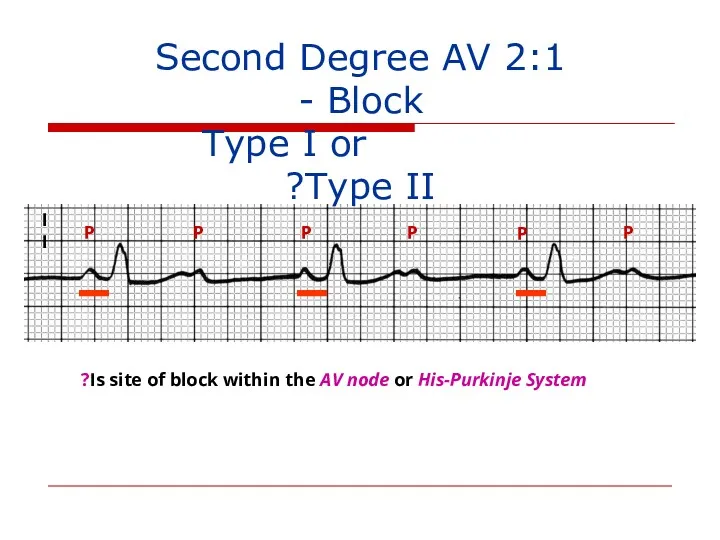
2:1 Second Degree AV Block -
Type I or Type
II
P
P
P
P
P
P
2:1 Second Degree AV Block -
Type I or Type
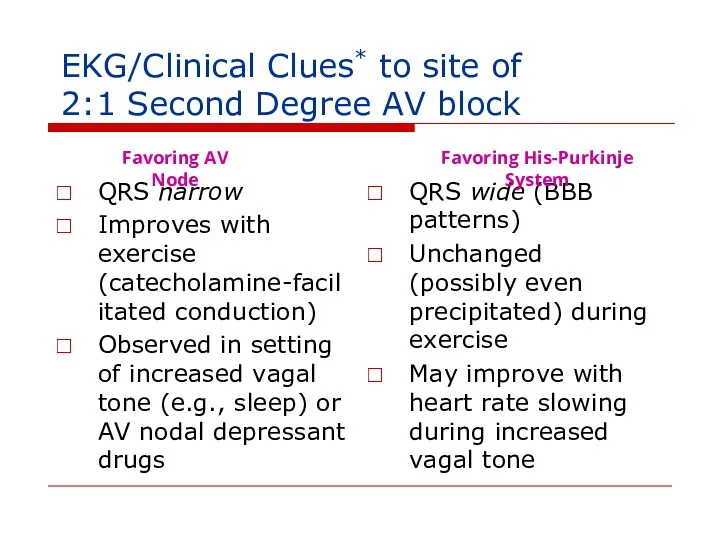
EKG/Clinical Clues* to site of
2:1 Second Degree AV block
QRS narrow
Improves with
EKG/Clinical Clues* to site of
2:1 Second Degree AV block
QRS narrow
Improves with
II
P
P
P
P
P
P
P
P
P
3:1 conduction ratio, with ventricular rate in the 30’s
Advanced Second Degree
II
P
P
P
P
P
P
P
P
P
3:1 conduction ratio, with ventricular rate in the 30’s
Advanced Second Degree
Site of AV Block vs. Escape Rhythm
AV Node: Junctional or ventricular
His-Purkinje
Site of AV Block vs. Escape Rhythm
AV Node: Junctional or ventricular
His-Purkinje
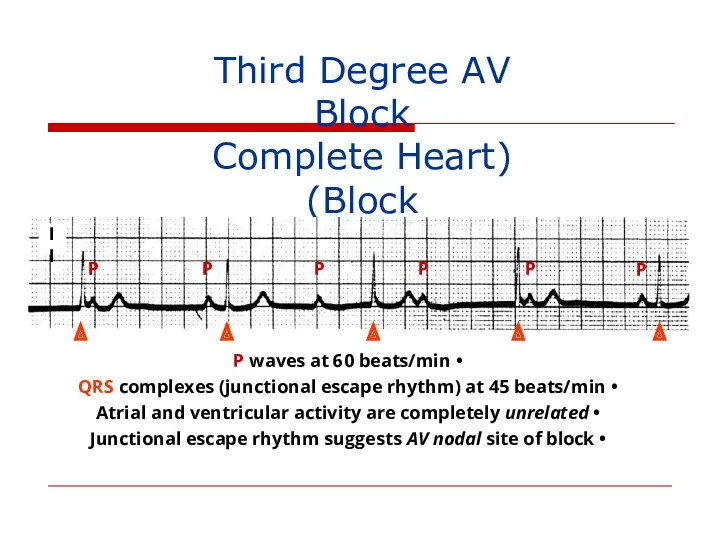
Third Degree AV Block
(Complete Heart Block)
P
P
P
P
P
P
P waves at 60 beats/min
Third Degree AV Block
(Complete Heart Block)
P
P
P
P
P
P
P waves at 60 beats/min
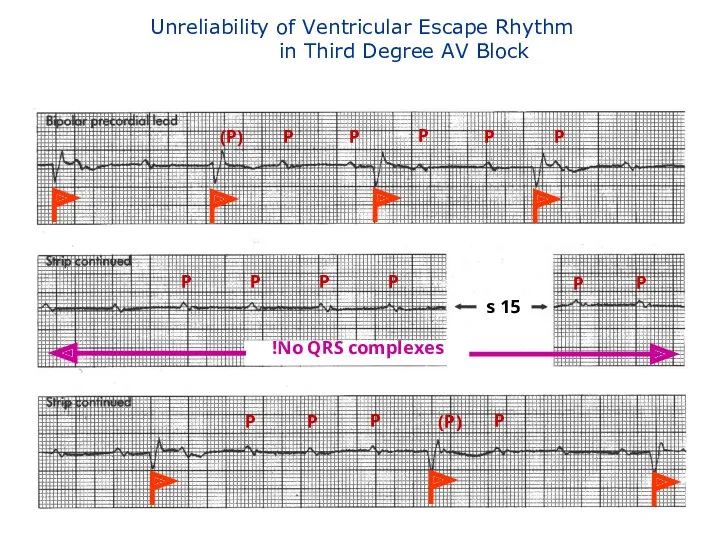
Unreliability of Ventricular Escape Rhythm
in Third Degree AV Block
P
P
(P)
P
P
P
P
P
P
P
P
P
No QRS
Unreliability of Ventricular Escape Rhythm
in Third Degree AV Block
P
P
(P)
P
P
P
P
P
P
P
P
P
No QRS


Causes of NON-Physiologic AV Block
Ischemic heart disease, cardiomyopathy and degenerative changes
Drugs
Causes of NON-Physiologic AV Block
Ischemic heart disease, cardiomyopathy and degenerative changes
Drugs
Sinus Bradyarrhythmias
Sinus Bradyarrhythmias
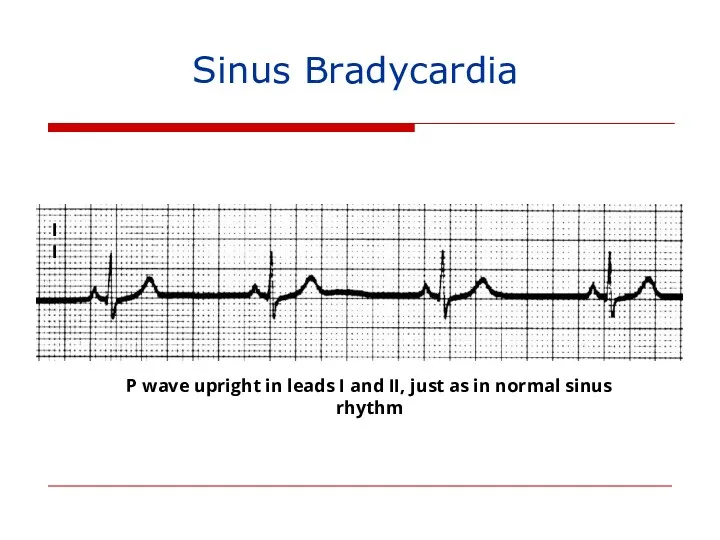
Sinus Bradycardia
II
P wave upright in leads I and II, just as
Sinus Bradycardia
II
P wave upright in leads I and II, just as
Causes of Sinus Bradycardia
Increased vagal tone
Drugs: beta blockers, calcium channel blockers,
Causes of Sinus Bradycardia
Increased vagal tone
Drugs: beta blockers, calcium channel blockers,
Sequence of P Wave Generation
Sinus
Node
SA
Junction
Atrium
(P wave)
Non-visible process on the
Sequence of P Wave Generation
Sinus
Node
SA
Junction
Atrium
(P wave)
Non-visible process on the
Inspiration
Expiration
SA nodal acceleration
SA nodal deceleration
Sinus Arrhythmia
Inspiration
Expiration
SA nodal acceleration
SA nodal deceleration
Sinus Arrhythmia
Sinoatrial (SA) Exit Block - Definitions
First Degree: Prolonged SA conduction time
Sinoatrial (SA) Exit Block - Definitions
First Degree: Prolonged SA conduction time
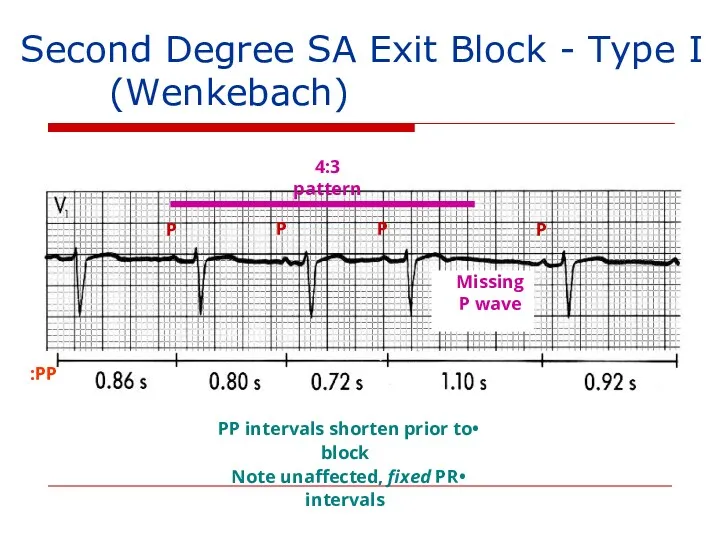
Second Degree SA Exit Block - Type I
(Wenkebach)
P
P
P
P
4:3 pattern
Missing
P
Second Degree SA Exit Block - Type I
(Wenkebach)
P
P
P
P
4:3 pattern
Missing
P
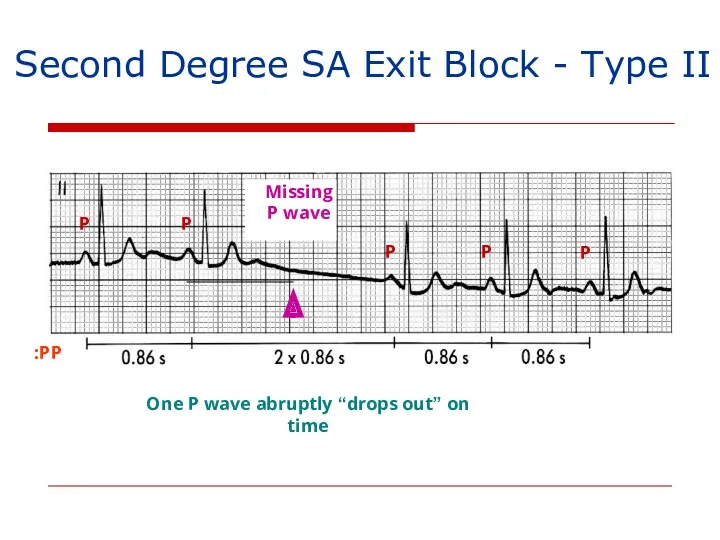
Second Degree SA Exit Block - Type II
PP:
P
P
P
P
P
One P wave abruptly
Second Degree SA Exit Block - Type II
PP:
P
P
P
P
P
One P wave abruptly
X
2X
2X
X
P
P
P
P
P
P
P
P
2:1 SA Exit Block
(Every Other P wave is “Dropped”)
Atrial rate
X
2X
2X
X
P
P
P
P
P
P
P
P
2:1 SA Exit Block
(Every Other P wave is “Dropped”)
Atrial rate
P
P
P’
P’
Sinus bradycardia → Sinus arrest → Slow junctional escape rhythm
(with retrograde
P
P
P’
P’
Sinus bradycardia → Sinus arrest → Slow junctional escape rhythm
(with retrograde
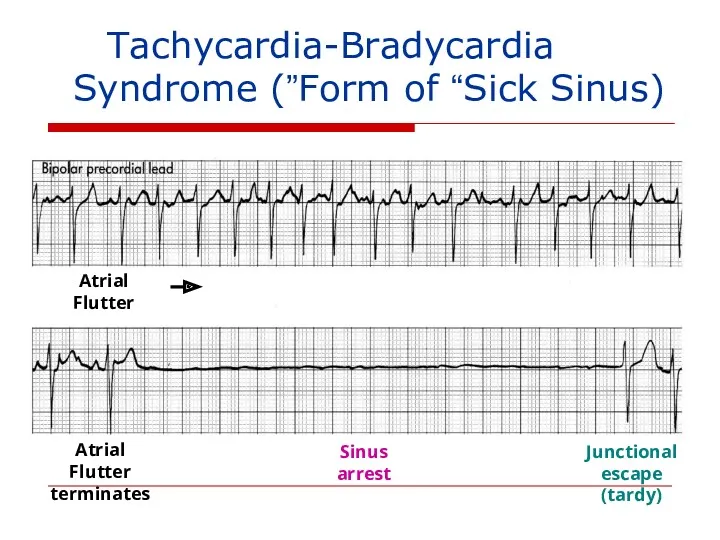
Tachycardia-Bradycardia
(Form of “Sick Sinus”) Syndrome
Atrial Flutter
Sinus arrest
Junctional
escape
Tachycardia-Bradycardia
(Form of “Sick Sinus”) Syndrome
Atrial Flutter
Sinus arrest
Junctional
escape
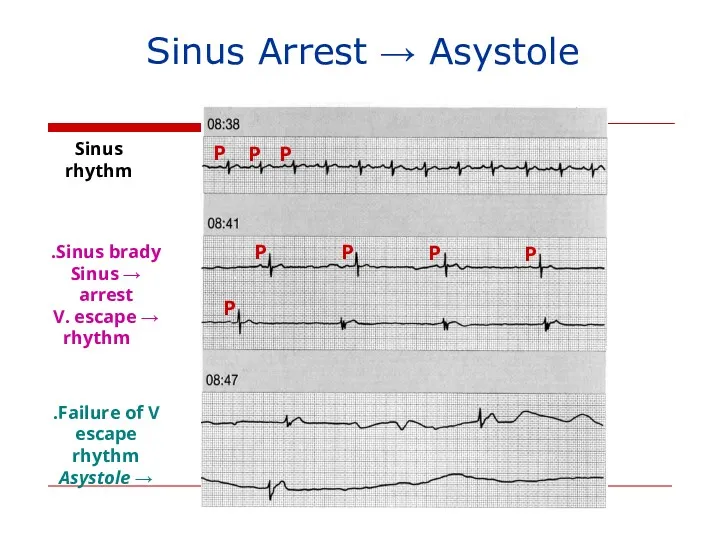
Sinus Arrest → Asystole
Sinus rhythm
Sinus brady.
→ Sinus arrest
→ V. escape
rhythm
Failure
Sinus Arrest → Asystole
Sinus rhythm
Sinus brady.
→ Sinus arrest
→ V. escape
rhythm
Failure
Causes of SA Exit Block and Sinus Pauses/Arrest
Increased vagal tone
Causes of SA Exit Block and Sinus Pauses/Arrest
Increased vagal tone
Sick Sinus Syndrome
(1) persistent spontaneous sinus bradycardia not caused by drugs
Sick Sinus Syndrome
(1) persistent spontaneous sinus bradycardia not caused by drugs
 В-лимфоциты – основные эффекторы гуморального иммунного ответа. Лекция 5
В-лимфоциты – основные эффекторы гуморального иммунного ответа. Лекция 5 Лицо ассимметрично
Лицо ассимметрично Первичный билиарный цирроз. Диагностика и лечение
Первичный билиарный цирроз. Диагностика и лечение Физиотерапия. Механизмы формирования реакций организма на физические факторы. Принципы лечебного применения физических факторов
Физиотерапия. Механизмы формирования реакций организма на физические факторы. Принципы лечебного применения физических факторов Мейірбикелік күтім
Мейірбикелік күтім Посттранскрипционды гендер экспрессияның регуляциясы
Посттранскрипционды гендер экспрессияның регуляциясы Экстремальные жизненные ситуации. Первая помощь
Экстремальные жизненные ситуации. Первая помощь Особенности сестринского ухода за пациентами и реабилитация при повреждении костей таза
Особенности сестринского ухода за пациентами и реабилитация при повреждении костей таза Геморрагические диатезы
Геморрагические диатезы Гидроцефалия. Диагностика МРТ
Гидроцефалия. Диагностика МРТ Традиционные методы лечения
Традиционные методы лечения Адгезивы. Химическая структура и свойства современных адгезивных систем
Адгезивы. Химическая структура и свойства современных адгезивных систем Правила проведения доклинического исследования лекарственного средства для ветеринарного применения, клинического исследования
Правила проведения доклинического исследования лекарственного средства для ветеринарного применения, клинического исследования Анемиялық синдром (анемиямен көрінетін аурулардың дифференциалы диагностикасы)
Анемиялық синдром (анемиямен көрінетін аурулардың дифференциалы диагностикасы) Пропедевтика внутренних болезней. Цели и задачи. Методы исследования. Исследование сердечно-сосудистой системы
Пропедевтика внутренних болезней. Цели и задачи. Методы исследования. Исследование сердечно-сосудистой системы Правовые и этнические основы оказания первой помощи
Правовые и этнические основы оказания первой помощи Рентгенологические методы исследования
Рентгенологические методы исследования Онкология сегодня
Онкология сегодня Показатели состояния общественного здоровья
Показатели состояния общественного здоровья The subject and tasks of biochemistry. The importance of biochemical research in medicine
The subject and tasks of biochemistry. The importance of biochemical research in medicine Емшекпен емізу
Емшекпен емізу Медицина и робототехника
Медицина и робототехника Рвотные и противорвотные средства
Рвотные и противорвотные средства Акушерская тактика при COVID-19
Акушерская тактика при COVID-19 Остеохондроз и методы его лечения
Остеохондроз и методы его лечения Виды повязок
Виды повязок Картина крови при различных видах анемий
Картина крови при различных видах анемий Аллергические состояния, проявления в полости рта. Клиника, диагностика, лечение
Аллергические состояния, проявления в полости рта. Клиника, диагностика, лечение