- Chronic obstructive pulmonary disease

Содержание
- 2. Chronic Obstructive Pulmonary diseases (COPD) – are a group of conditions that characterized by increased resistance
- 3. CHRONIC BRONCHITIS (CB) It is present in any patient who has persistent cough with sputum production
- 4. Histological features of the airways: Chronic irritation by inhaled substances lead to: replacement of the ciliated
- 5. Outcomes and complications: - Atypical metaplasia and dysplasia of the respiratory epithelium, providing a possible soil
- 6. BRONCHIECTASIS (BE) BE is defined as abnormal and irreversible dilatation of the bronchi and bronchioles developing
- 7. Etiopathogenesis of BE: 1. Endobronchial obstruction by tumor, foreign bodies, and compression by enlarged hilar lymph
- 8. Etiopathogenesis of BE: BE usually affects distal bronchi and bronchioles beyond the segmental bonchi. The lungs
- 9. Classification of BE: Cylindrical: long, tube-like enlargements in 1 to 4 type of bronchus. Fusiform: having
- 10. The histologic findings of BE: An intense acute and chronic inflammatory exudation within the walls of
- 11. Outcomes and complications: 1. Obstructive ventilatory insufficiency can lead to marked dyspnea and cyanosis. 2. Pulmonary
- 12. EMPHYSEMA It is a condition of the lung characterized by abnormal permanent enlargement of the airspace
- 13. Pathogenesis of emphysema Disease is accompanied with destruction of elastic and collagen fibers of lungs due
- 14. Classification of emphysema: The following forms are differentiated according to the affected section of the pulmonary
- 15. Centriacinar (cenrolobular) emphysema The distinctive feature of this type is the pattern of involvement of the
- 16. Panacinar emphysema Panacinar emphysema occurs with loss of all portions of the acinus from the respiratory
- 17. Bullous emphysema The chest cavity is opened at autopsy to reveal numerous large bullae apparent on
- 18. Microscopic examination The abnormal fenestrations in the walls of the alveoli. The complete destruction of septal
- 19. Special forms of emphysema according to cause: 1. Compensatory E. This term is sometimes used to
- 20. Asthma is a disease of airways that is characterized by increased responsiveness of the tracheobronchial tree
- 21. BRONCHIAL ASTHMA (BA): A severe and unremitting type of the disease termed status asthmaticus may prove
- 22. PATHOGENESIS of BA: Chronic airway inflammation involving many cell types and inflammatory mediators accompanies the bronchial
- 23. MORPHOLOGY of BA: Grossly, the lungs are overdistended because of overinflation, and there may be small
- 24. Histologic findings of BA 1. Thickening of the basement membrane of the bronchial epithelium; 2. Edema
- 25. The classic asthmatic attack lasts up to several hours and is followed by prolonged coughing; the
- 26. IDIOPATHIC PULMONARY FIBROSIS Diffuse interstitial fibrosis occurs as a result of different pulmonary diseases such as
- 27. PATHOGENESIS The pathogenesis of idiopathic pulmonary fibrosis is unknown and the condition is diagnosed by excluding
- 28. MORPHOLOGY: Pathological changes are bilateral and widespread. · Macroscopically the lungs are dense, reduced volume. ·
- 29. HYPERSENSITIVITY PNEUMONITIS Hypersensitivity pneumonitis occur when there is an inhaled organic dust that produces a localized
- 31. Скачать презентацию
Chronic Obstructive Pulmonary diseases (COPD) – are a group of conditions
Chronic Obstructive Pulmonary diseases (COPD) – are a group of conditions
CHRONIC BRONCHITIS (CB)
It is present in any patient who has persistent
CHRONIC BRONCHITIS (CB)
It is present in any patient who has persistent
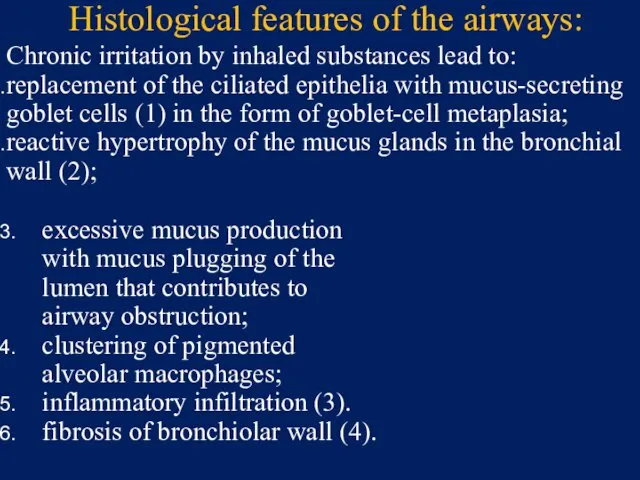
Histological features of the airways:
Chronic irritation by inhaled substances lead to:
replacement
Histological features of the airways:
Chronic irritation by inhaled substances lead to:
replacement
Outcomes and complications:
- Atypical metaplasia and dysplasia of the respiratory epithelium,
Outcomes and complications:
- Atypical metaplasia and dysplasia of the respiratory epithelium,
BRONCHIECTASIS (BE)
BE is defined as abnormal and irreversible dilatation of the
BRONCHIECTASIS (BE)
BE is defined as abnormal and irreversible dilatation of the
Etiopathogenesis of BE:
1. Endobronchial obstruction by tumor, foreign bodies, and compression
Etiopathogenesis of BE:
1. Endobronchial obstruction by tumor, foreign bodies, and compression
Etiopathogenesis of BE:
BE usually affects distal bronchi and bronchioles beyond the
Etiopathogenesis of BE:
BE usually affects distal bronchi and bronchioles beyond the
Classification of BE:
Cylindrical: long, tube-like enlargements in 1 to 4 type
Classification of BE:
Cylindrical: long, tube-like enlargements in 1 to 4 type
The histologic findings of BE:
An intense acute and chronic inflammatory exudation
The histologic findings of BE:
An intense acute and chronic inflammatory exudation
Outcomes and complications:
1. Obstructive ventilatory insufficiency can lead to marked dyspnea
Outcomes and complications:
1. Obstructive ventilatory insufficiency can lead to marked dyspnea
EMPHYSEMA
It is a condition of the lung characterized by abnormal permanent
EMPHYSEMA
It is a condition of the lung characterized by abnormal permanent
Pathogenesis of emphysema
Disease is accompanied with destruction of elastic and collagen
Pathogenesis of emphysema
Disease is accompanied with destruction of elastic and collagen
Classification of emphysema:
The following forms are differentiated according to the affected
Classification of emphysema:
The following forms are differentiated according to the affected
Centriacinar (cenrolobular) emphysema
The distinctive feature of this type is the
Centriacinar (cenrolobular) emphysema
The distinctive feature of this type is the
Panacinar emphysema
Panacinar emphysema occurs with loss of all portions of the
Panacinar emphysema
Panacinar emphysema occurs with loss of all portions of the
Bullous emphysema
The chest cavity is opened at autopsy to reveal
Bullous emphysema
The chest cavity is opened at autopsy to reveal
Microscopic examination
The abnormal fenestrations in the walls of the alveoli.
The complete
Microscopic examination
The abnormal fenestrations in the walls of the alveoli.
The complete
Special forms of emphysema according to cause:
1. Compensatory E. This term
Special forms of emphysema according to cause:
1. Compensatory E. This term
Asthma is a disease of airways that is characterized by increased
Asthma is a disease of airways that is characterized by increased
BRONCHIAL ASTHMA (BA):
A severe and unremitting type of the disease
BRONCHIAL ASTHMA (BA):
A severe and unremitting type of the disease
PATHOGENESIS of BA:
Chronic airway inflammation involving many cell types and inflammatory
PATHOGENESIS of BA:
Chronic airway inflammation involving many cell types and inflammatory
MORPHOLOGY of BA:
Grossly, the lungs are overdistended because of overinflation, and
MORPHOLOGY of BA:
Grossly, the lungs are overdistended because of overinflation, and
Histologic findings of BA
1. Thickening of the basement membrane of the
Histologic findings of BA
1. Thickening of the basement membrane of the
The classic asthmatic attack lasts up to several hours and is
The classic asthmatic attack lasts up to several hours and is
IDIOPATHIC PULMONARY FIBROSIS
Diffuse interstitial fibrosis occurs as a result of different
IDIOPATHIC PULMONARY FIBROSIS
Diffuse interstitial fibrosis occurs as a result of different
PATHOGENESIS
The pathogenesis of idiopathic pulmonary fibrosis is unknown and the
PATHOGENESIS
The pathogenesis of idiopathic pulmonary fibrosis is unknown and the
MORPHOLOGY:
Pathological changes are bilateral and widespread.
· Macroscopically the lungs are dense,
MORPHOLOGY:
Pathological changes are bilateral and widespread. · Macroscopically the lungs are dense,
HYPERSENSITIVITY PNEUMONITIS
Hypersensitivity pneumonitis occur when there is an inhaled organic
HYPERSENSITIVITY PNEUMONITIS
Hypersensitivity pneumonitis occur when there is an inhaled organic
 Ерте жастағы қауіп тобындағы балаларды ПМСП жағдайында бақылаудың дифференцирленген бақылау тактикасы
Ерте жастағы қауіп тобындағы балаларды ПМСП жағдайында бақылаудың дифференцирленген бақылау тактикасы Биотикалық факторға төзімді өсімдіктерді гендік инженерия арқылы кұрастыру
Биотикалық факторға төзімді өсімдіктерді гендік инженерия арқылы кұрастыру Желудочно-кишечные кровотечения
Желудочно-кишечные кровотечения Центральная регуляция позы и равновесия тела и организация целенаправленных движений
Центральная регуляция позы и равновесия тела и организация целенаправленных движений Правильное питание – залог здоровья
Правильное питание – залог здоровья Иммунитет при инфекционных заболеваниях
Иммунитет при инфекционных заболеваниях Оперативті хирургиялық техниканың қазіргі кездегі құрал сайман негіздері
Оперативті хирургиялық техниканың қазіргі кездегі құрал сайман негіздері Основные аспекты содержания и методики АФК. Адаптивная физическая культура
Основные аспекты содержания и методики АФК. Адаптивная физическая культура Лекарственные растения в нашей жизни
Лекарственные растения в нашей жизни Аневризма брюшного отдела аорты
Аневризма брюшного отдела аорты Ирригоскопия - жуан ішек препараттының ішіне ретроградты енгізумен ішектің рентгенологиялық зерттеу
Ирригоскопия - жуан ішек препараттының ішіне ретроградты енгізумен ішектің рентгенологиялық зерттеу Возрастные аспекты развития физиологического вида прикуса
Возрастные аспекты развития физиологического вида прикуса Схема истории болезни
Схема истории болезни Воспаление. Общие вопросы
Воспаление. Общие вопросы Сочетание ХОБЛ и ИБС: случайность или закономерность
Сочетание ХОБЛ и ИБС: случайность или закономерность Дивертикулез толстой кишки
Дивертикулез толстой кишки Предоперационная подготовка гинекологических больных
Предоперационная подготовка гинекологических больных Плеврит
Плеврит Производственная санитария, её задачи. Уход за производственным помещением
Производственная санитария, её задачи. Уход за производственным помещением Серцево-легенева реанімація
Серцево-легенева реанімація Гипертонические кризы
Гипертонические кризы УЗИ желудочно-кишечного тракта
УЗИ желудочно-кишечного тракта Тәуліктік PH-метрия
Тәуліктік PH-метрия Гипертонические кризы, классификация, патогенез, неотложная помощь
Гипертонические кризы, классификация, патогенез, неотложная помощь Терминальные состояния
Терминальные состояния Фармакологія антибіотиків, противірусних та протигрибкових засобів
Фармакологія антибіотиків, противірусних та протигрибкових засобів Профессиональные вредности в работе врача-стоматолога и профилактика последствий их воздействия
Профессиональные вредности в работе врача-стоматолога и профилактика последствий их воздействия Аспирин и его влияние на организм человека
Аспирин и его влияние на организм человека