- Hypocortisolism Addison's disease

Содержание
- 2. Hypocortisolism Addison's disease John F. Kennedy (1917--1963)
- 3. Addison's disease Chronic adrenal insufficiency, hypocorticism a rare endocrine disorder that caused by insufficient cortisol and
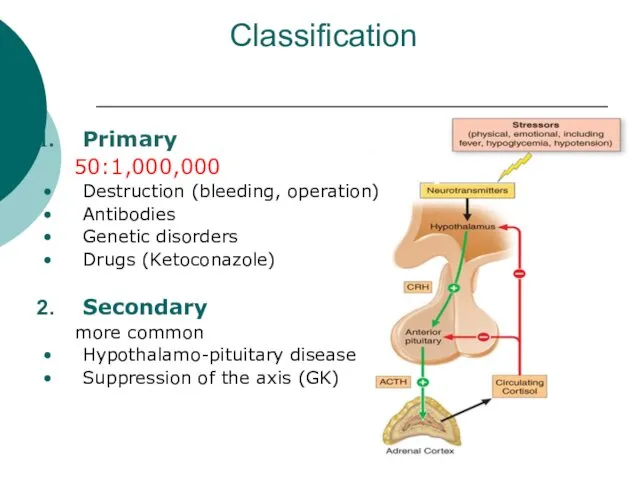
- 4. Classification Primary 50:1,000,000 Destruction (bleeding, operation) Antibodies Genetic disorders Drugs (Ketoconazole) Secondary more common Hypothalamo-pituitary disease
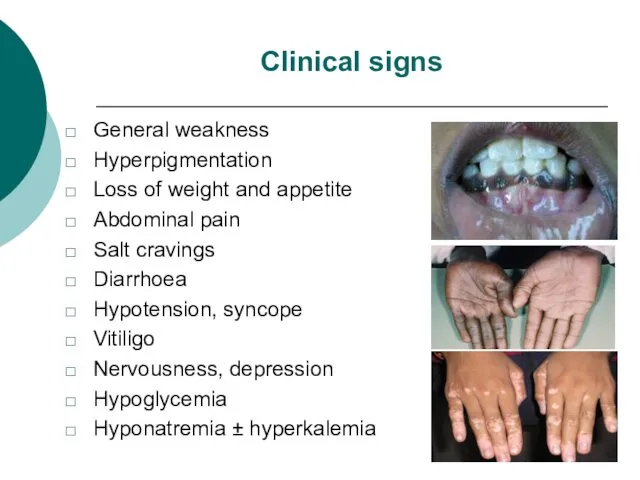
- 5. Clinical signs General weakness Hyperpigmentation Loss of weight and appetite Abdominal pain Salt cravings Diarrhoea Hypotension,
- 6. Diagnosis more than 17-20 mkg/dl 500-550 nmol/L High clinical suspicious Test SYNACTHEN IV COSYNTHROPINE 250 MKG
- 7. Chronic treatment Primary adrenal insuf.: Hydrocortisone 20-25 mg/d or Prednisone 7.5 mg/d. Secondary adrenal insuf.: Hydrocortisone
- 8. מקרה קליני 1 אישה בת 44 , נשואה+2 בריאה פרט לחסר B12 וברזל, מטופלת לפני 6
- 9. מקרה קליני 1 (המשך) באשפוז יציבה המודינאמית ונשימתית ל"ד 120\75, דופק סביב 80 ללא ממצאים פיזיקאליים
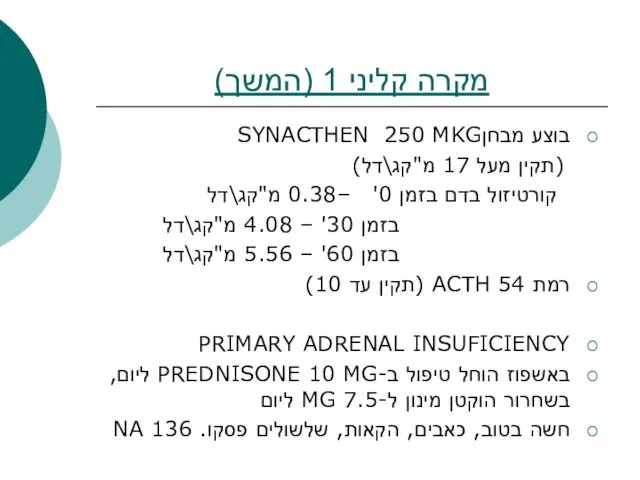
- 10. מקרה קליני 1 (המשך) בוצע מבחןSYNACTHEN 250 MKG (תקין מעל 17 מ"קג\דל) קורטיזול בדם בזמן 0'
- 12. Скачать презентацию
Hypocortisolism
Addison's disease
John F. Kennedy (1917--1963)
Hypocortisolism
Addison's disease
John F. Kennedy (1917--1963)
Addison's disease
Chronic adrenal insufficiency, hypocorticism
a rare endocrine disorder
that
Addison's disease
Chronic adrenal insufficiency, hypocorticism
a rare endocrine disorder
that
Classification
Primary
50:1,000,000
Destruction (bleeding, operation)
Antibodies
Genetic disorders
Drugs (Ketoconazole)
Secondary
more common
Hypothalamo-pituitary disease
Suppression of
Classification
Primary
50:1,000,000
Destruction (bleeding, operation)
Antibodies
Genetic disorders
Drugs (Ketoconazole)
Secondary
more common
Hypothalamo-pituitary disease
Suppression of
Clinical signs
General weakness
Hyperpigmentation
Loss of weight and appetite
Abdominal pain
Salt cravings
Diarrhoea
Hypotension, syncope
Vitiligo
Nervousness, depression
Hypoglycemia
Hyponatremia
Clinical signs
General weakness
Hyperpigmentation
Loss of weight and appetite
Abdominal pain
Salt cravings
Diarrhoea
Hypotension, syncope
Vitiligo
Nervousness, depression
Hypoglycemia
Hyponatremia
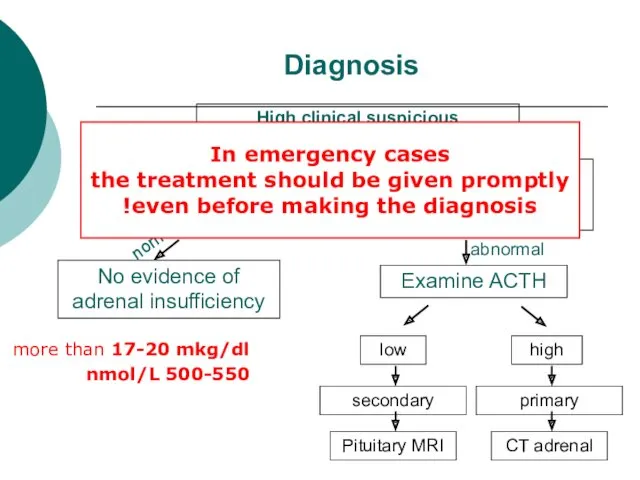
Diagnosis
more than 17-20 mkg/dl
500-550 nmol/L
High clinical suspicious
Test SYNACTHEN
IV COSYNTHROPINE 250 MKG
Blood
Diagnosis
more than 17-20 mkg/dl
500-550 nmol/L
High clinical suspicious
Test SYNACTHEN
IV COSYNTHROPINE 250 MKG
Blood
Chronic treatment
Primary adrenal insuf.: Hydrocortisone 20-25 mg/d or Prednisone 7.5
Chronic treatment
Primary adrenal insuf.: Hydrocortisone 20-25 mg/d or Prednisone 7.5
מקרה קליני 1
אישה בת 44 , נשואה+2
בריאה פרט לחסר B12 וברזל,
מקרה קליני 1
אישה בת 44 , נשואה+2
בריאה פרט לחסר B12 וברזל,
מקרה קליני 1 (המשך)
באשפוז יציבה המודינאמית ונשימתית
ל"ד 120\75, דופק סביב 80
ללא
מקרה קליני 1 (המשך)
באשפוז יציבה המודינאמית ונשימתית
ל"ד 120\75, דופק סביב 80
ללא
מקרה קליני 1 (המשך)
בוצע מבחןSYNACTHEN 250 MKG
(תקין מעל 17 מ"קג\דל)
מקרה קליני 1 (המשך)
בוצע מבחןSYNACTHEN 250 MKG
(תקין מעל 17 מ"קג\דל)
 Бронхиальная астма у детей
Бронхиальная астма у детей Противовоспалительные лекарственные средства (ПВЛС)
Противовоспалительные лекарственные средства (ПВЛС) Мүгедектік
Мүгедектік Түбір өзектерді көлікті өңдеу әдістері
Түбір өзектерді көлікті өңдеу әдістері Малярия, токсоплазма, лямблии
Малярия, токсоплазма, лямблии Сүйек сыну. Буын шығу соғып алу. Сіңір созылу
Сүйек сыну. Буын шығу соғып алу. Сіңір созылу Бронхиальная астма
Бронхиальная астма Сифилитический увеит
Сифилитический увеит Қыз баланың, бойжеткеннің және әйелдің жеке бас гигиенасы
Қыз баланың, бойжеткеннің және әйелдің жеке бас гигиенасы Тамыр ішіндегі шашыранды қан ұю (ТШҚҰ) синдромы
Тамыр ішіндегі шашыранды қан ұю (ТШҚҰ) синдромы Кожно – кинестетический анализатор. Сенсорные кожно-кинестетические расстройства. Исследование тактильного гнозиса
Кожно – кинестетический анализатор. Сенсорные кожно-кинестетические расстройства. Исследование тактильного гнозиса Помощь при отравлениях
Помощь при отравлениях Группы крови. Гемостаз
Группы крови. Гемостаз Эпидемиологическая характеристика инфекционных заболеваний с аэрозольным механизмом передачи инфекции
Эпидемиологическая характеристика инфекционных заболеваний с аэрозольным механизмом передачи инфекции Ожоги лица. Клиника, диагностика, лечение
Ожоги лица. Клиника, диагностика, лечение Визначення туберкульозу як наукової і практичної проблеми. Історія фтизіатрії. Епідеміологія туберкульозу
Визначення туберкульозу як наукової і практичної проблеми. Історія фтизіатрії. Епідеміологія туберкульозу Glomerulonefrit, endokardit, kolit
Glomerulonefrit, endokardit, kolit Болезнь Вильсона-Коновалова. Дифференциальный диагноз с хроническими гепатитами
Болезнь Вильсона-Коновалова. Дифференциальный диагноз с хроническими гепатитами Сердце в традиционной китайской медицине
Сердце в традиционной китайской медицине Эндовидеохирургия. Выполняемые операции
Эндовидеохирургия. Выполняемые операции СРС на тему: Холодовая цепь
СРС на тему: Холодовая цепь Терминальные состояние: стадии, клиника, диагностика, критерии оценки тяжести состояния больного
Терминальные состояние: стадии, клиника, диагностика, критерии оценки тяжести состояния больного Бронхоэктатическая болезнь
Бронхоэктатическая болезнь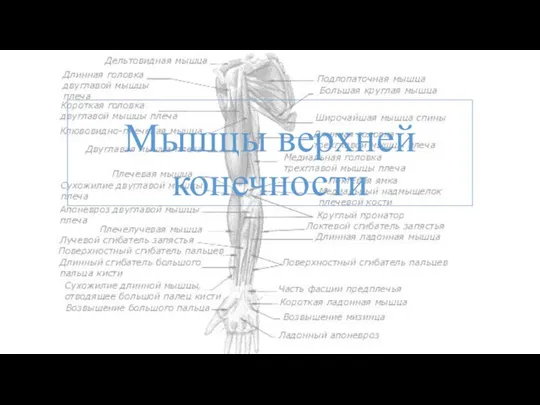 Мышцы верхней конечности
Мышцы верхней конечности Общие тенденции развития медицинской реабилитации в Краснодарском крае
Общие тенденции развития медицинской реабилитации в Краснодарском крае Лікарські рослини, їх значення. Ароматерапія
Лікарські рослини, їх значення. Ароматерапія Предменструальный, климактерический синдром, посткастрационный синдром
Предменструальный, климактерический синдром, посткастрационный синдром Харчові отруєння
Харчові отруєння