- Clinical anatomy of abdominal cavity

Содержание
- 2. liver in the upper right quadrant of the cavity. It is separated into right and left
- 3. borders: superior: inferior surface of diaphragm Inferior: mesocolon transversum Contents: hepatic bursa, pregastric bursa, omental bursa,
- 4. Borders: Superior: mesocolon transversum Inferior: inlet of the lesser pelvis contents: Right & left paracolic canals
- 5. After cutting through the abdominal wall, if you put your hand under the wall, you will
- 6. lig. falciforme lig. coronarium hepatis lig. triangulare lig. hepatogastricum lig. hepatoduodenale lig. hepatocolicum lig. hepatorenale lig.
- 7. duodenojejunal recess superior ileocaecal recess inferior ileocaecal recess retrocaecal recess intersigmoid recess Recesses - pouches formed
- 8. Plica gastropancreatica Plica ileocecalis Plica duodenalis superior Plica duodenalis inferior Plica umbilicalis mediana Plica umbilicalis medialis
- 9. RIGHT MESENTERIC SINUS borders: medial-root of the mesentry Lateral – ascending colon Superior – transverse colon
- 10. Right paracolic canal communicates with right hepatic bursa Borders: Medial – ascending colon Lateral – parietalperitoneum
- 11. HEPATIC BURSA Borders: Superior – diaphragm Inferior – transverse mesocolon Anterior – anterior abdominal wall Medial
- 12. Pregastric bursa Borders: Anterior – left lobe of the liver and anterior abdominal wall Posterior –
- 13. BORDERS: Superior – lobus caudatus hepatis Inferior – mesocolon transversum Anterior – stomach & lesser omentum
- 14. The branches to the stomach arise from the above: celiac (C) left gastric (LG) - supplies
- 15. The stomach drains either directly or indirectly into the portal vein as follows:short gastric veins (SG)
- 16. Nerve supply
- 18. Gastritis (acute or stress) Produces inflammation of the mucosa. Can be associated with erosions and bleeding.
- 19. Menetrier’s Disease (aka Hypertrophic Gastritis)
- 20. Gastric Polyps
- 21. Bezoars
- 22. The “Culprit” H. pylori Treatment: Triple therapy
- 23. Gastric ulcers
- 24. Gastric Ulcers
- 25. History of Peptic Ulcer Surgery Harberer 1882- first gastric resection for ulcer Billroth 1885- Billroth II
- 26. Laser Coagulation of Bleeding Ulcer
- 27. Coil Embolization of Bleeding Ulcer
- 28. Pyloroplasty for Bleeding Ulcer
- 29. Open Surgical Procedures Truncal vagotomy and pyloroplasty Truncal vagotomy and gastrojejunostomy Truncal vagotomy and antrectomy Highly
- 30. GASTROSTOMY Temporary gastrostomy Minimal gastrostomy Vitzel’s gastrostomy Stamm-Kader’s gastrostomy Permanent gastrostomy Toprover’s gastrostomy Beck Jian’s gastrostomy
- 32. Roux -en -Y Reconstruction
- 33. Antecolic and Retrocolic BII
- 34. Truncal Vagotomy Resect 1-2cm of each vagal trunk on distal esophagus. Reduces acid by 80%. Denervates
- 35. Antrectomy and Truncal Vagotomy with BI
- 36. Truncal Vagotomy and Antrectomy Entails distal gastrectomy of 50-60% of stomach. Removes parietal cell mass. Requires
- 37. Selective Vagotomy Total denervation of the stomach from diaphragmatic crus to pylorus. Procedure still needs drainage,
- 38. Highly Selective Vagotomy Spares nerves of Latarjet, but divides vagal branches to proximal 2/3 of stomach.
- 39. Types of Vagotomies
- 40. Gastric Adenocarcinoma
- 41. Duodenum 4 parts Metabolically active Produces many enzymes D2: site of pacemaker D2: posterolateral insertion of
- 42. Duodenum Brunner’s glands Blood supply: GDA- superior pancreaticoduodenal SMA- inferior pancreaticoduodenal
- 43. Blood Supply of the Duodenum superior pancreaticoduodenal anterior and posterior branches inferior pancreaticoduodenal anterior and posterior
- 44. Duodenal Ulcers
- 45. Obstruction
- 46. Small Bowel Obstruction History Prior surgery Hernias Signs and Symptoms Colicky abdominal pain Nausea and vomiting
- 47. Intestinum Crasum
- 48. Large Bowel Obstruction
- 49. colostomy
- 50. Anastamosis Stapled vs. Hand-Sewn Brundage et al. J trauma. 1999 Multicenter retrospective cohort design “anastamotic leaks
- 51. Anastamosis Burch et al. Ann of Surg. 1999. Prospective randomized trial of single-layer continuous vs. two
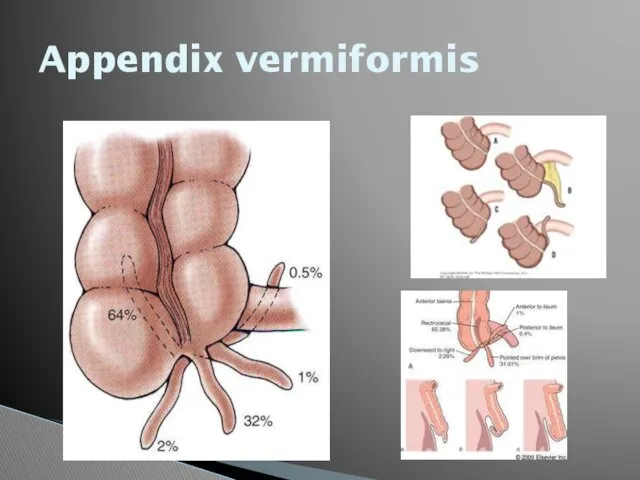
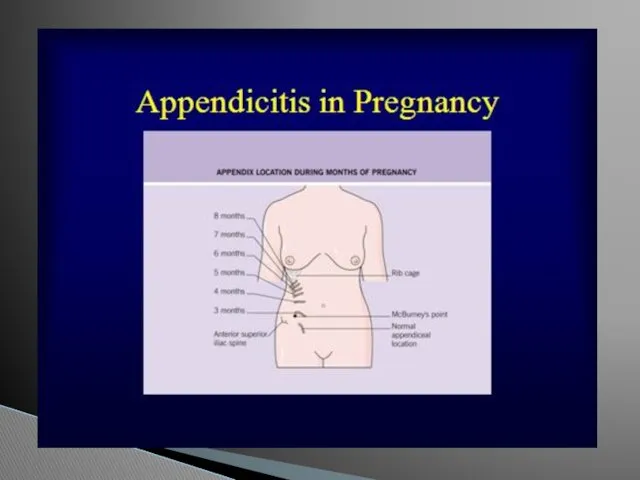
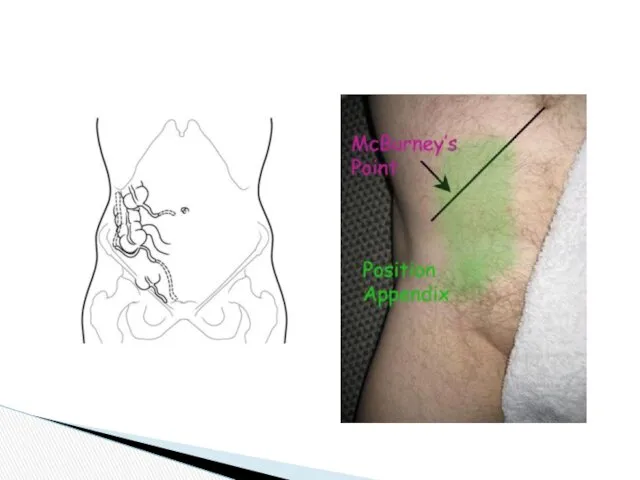
- 52. Appendix vermiformis
- 54. The caecum was at McBurney's point in 245 (80.9%) patients, pelvic in 45 (14.9%) and high
- 55. Topography of appendix vermiformis and ceacum
- 57. Ulcerative Colitis Disease Severity Mild colitis: 20% Moderate colitis: 71% Severe colitis: 9% Acute disease complications
- 58. Subtotal Colectomy
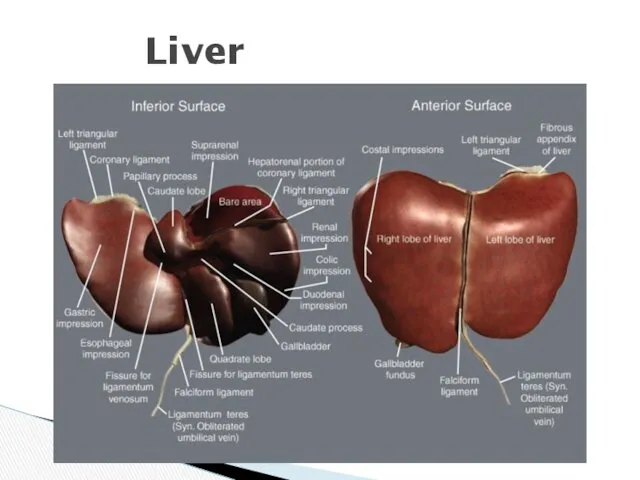
- 59. Liver
- 60. Liver
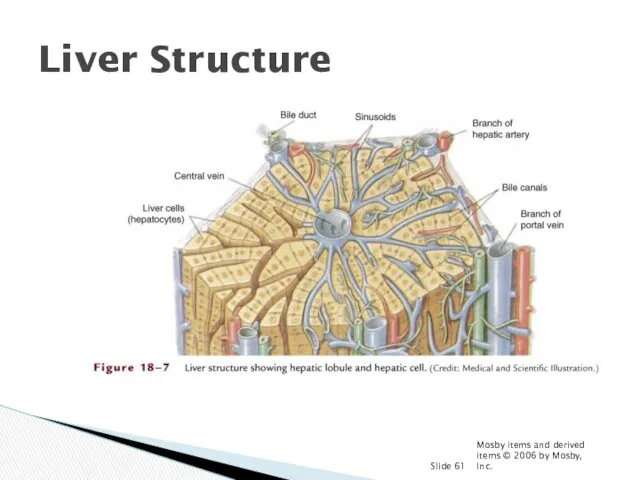
- 61. Mosby items and derived items © 2006 by Mosby, Inc. Slide Liver Structure
- 62. Porto-caval anastomoses
- 63. Caput Medusa
- 65. Varices on EGD
- 66. Varix Banding
- 67. Gall bladder
- 68. Arteries of the gall bladder
- 69. Innervation of gall bladder
- 70. Lymphatic drainage of the gallbladder
- 71. Harvest Time
- 72. CT Scan
- 73. Plain Films
- 74. Ultrasound
- 75. Laparoscopic Cholecystectomy
- 76. cancer
- 78. Скачать презентацию
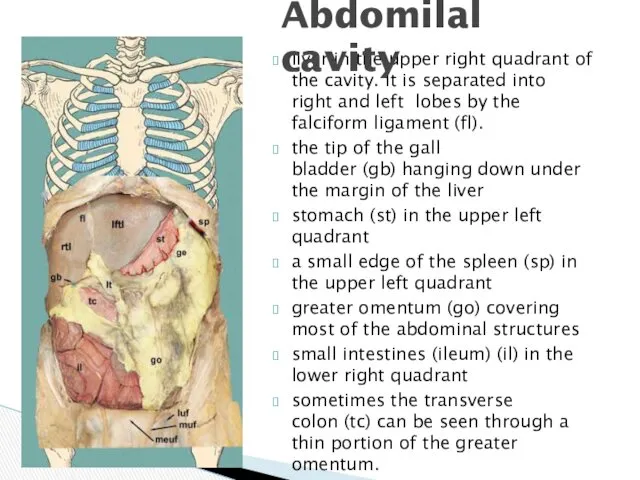
liver in the upper right quadrant of the cavity. It is
liver in the upper right quadrant of the cavity. It is
borders:
superior: inferior surface of diaphragm
Inferior: mesocolon transversum
Contents: hepatic bursa, pregastric bursa,
borders:
superior: inferior surface of diaphragm
Inferior: mesocolon transversum
Contents: hepatic bursa, pregastric bursa,
Borders:
Superior: mesocolon transversum
Inferior: inlet of the lesser pelvis
contents:
Right & left paracolic
Borders:
Superior: mesocolon transversum
Inferior: inlet of the lesser pelvis
contents:
Right & left paracolic
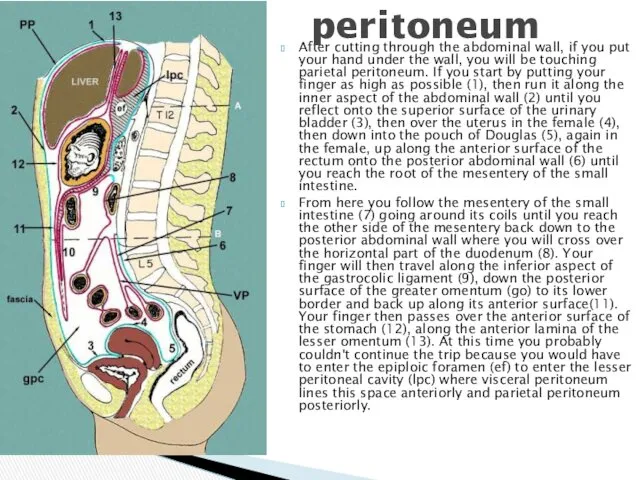
After cutting through the abdominal wall, if you put your hand
After cutting through the abdominal wall, if you put your hand

lig. falciforme
lig. coronarium hepatis
lig. triangulare
lig. hepatogastricum
lig. hepatoduodenale
lig. hepatocolicum
lig. hepatorenale
lig. gastrophrenicum
lig. gastrolienale
lig.
lig. falciforme
lig. coronarium hepatis
lig. triangulare
lig. hepatogastricum
lig. hepatoduodenale
lig. hepatocolicum
lig. hepatorenale
lig. gastrophrenicum
lig. gastrolienale
lig.
duodenojejunal recess
superior ileocaecal recess
inferior ileocaecal recess
retrocaecal recess
intersigmoid recess
Recesses - pouches formed
duodenojejunal recess
superior ileocaecal recess
inferior ileocaecal recess
retrocaecal recess
intersigmoid recess
Recesses - pouches formed
Plica gastropancreatica
Plica ileocecalis
Plica duodenalis superior
Plica duodenalis inferior
Plica umbilicalis mediana
Plica umbilicalis medialis
Plica
Plica gastropancreatica
Plica ileocecalis
Plica duodenalis superior
Plica duodenalis inferior
Plica umbilicalis mediana
Plica umbilicalis medialis
Plica
RIGHT MESENTERIC SINUS
borders:
medial-root of the mesentry
Lateral – ascending colon
Superior –
RIGHT MESENTERIC SINUS
borders:
medial-root of the mesentry
Lateral – ascending colon
Superior –
Right paracolic canal communicates with right hepatic bursa
Borders:
Medial – ascending colon
Lateral
Right paracolic canal communicates with right hepatic bursa
Borders:
Medial – ascending colon
Lateral
HEPATIC BURSA
Borders:
Superior – diaphragm
Inferior – transverse mesocolon
Anterior – anterior abdominal wall
Medial
HEPATIC BURSA
Borders:
Superior – diaphragm
Inferior – transverse mesocolon
Anterior – anterior abdominal wall
Medial
Pregastric bursa
Borders:
Anterior – left lobe of the liver and anterior abdominal
Pregastric bursa
Borders:
Anterior – left lobe of the liver and anterior abdominal
BORDERS:
Superior – lobus caudatus hepatis
Inferior – mesocolon transversum
Anterior – stomach &
BORDERS:
Superior – lobus caudatus hepatis
Inferior – mesocolon transversum
Anterior – stomach &
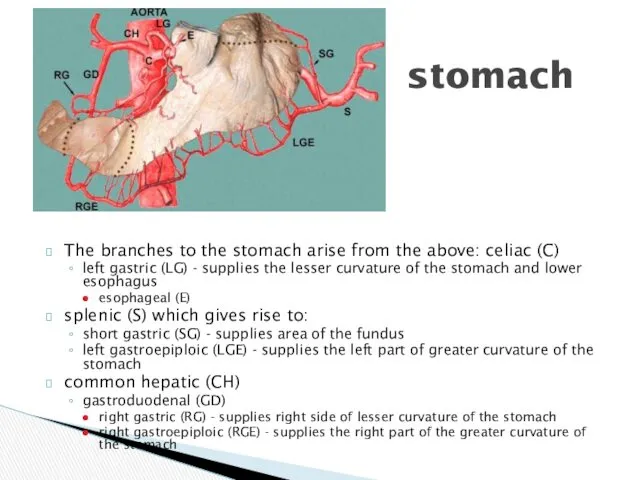
The branches to the stomach arise from the above: celiac (C)
left gastric (LG) -
The branches to the stomach arise from the above: celiac (C)
left gastric (LG) -
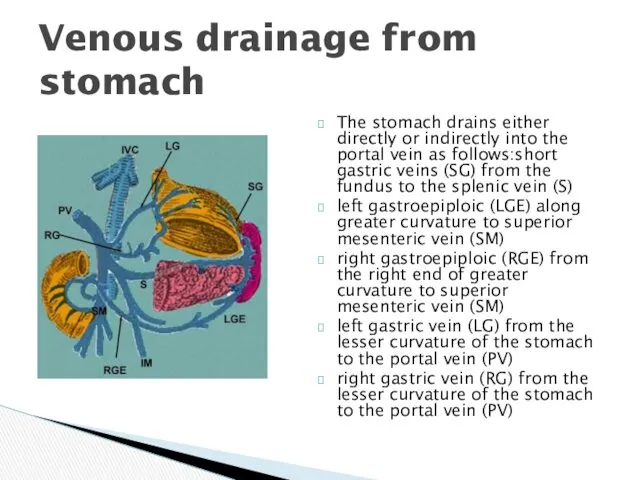
The stomach drains either directly or indirectly into the portal vein
The stomach drains either directly or indirectly into the portal vein
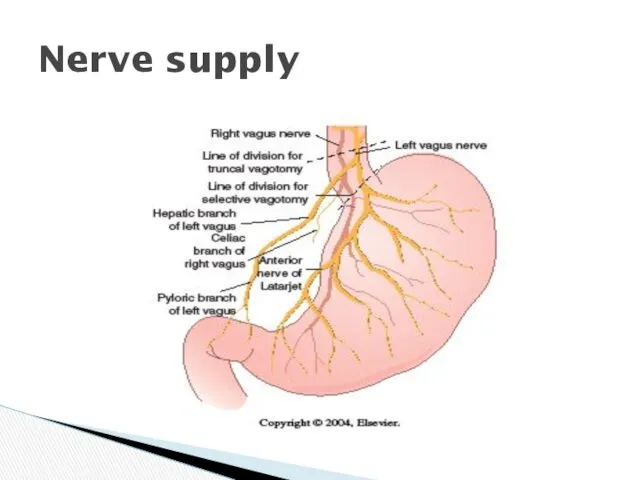
Nerve supply
Nerve supply
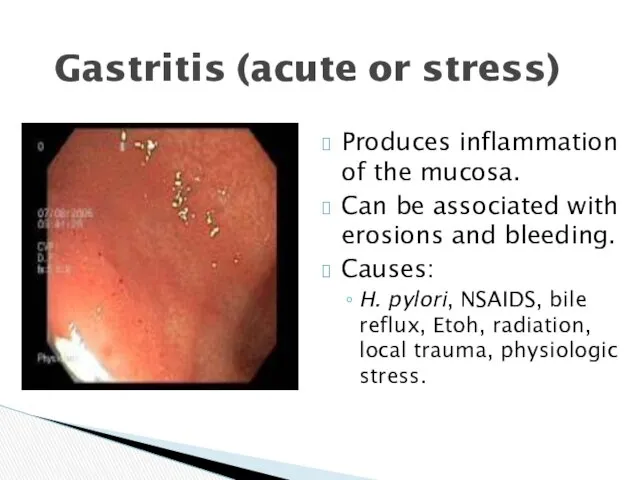
Gastritis (acute or stress)
Produces inflammation of the mucosa.
Can be associated with
Gastritis (acute or stress)
Produces inflammation of the mucosa.
Can be associated with
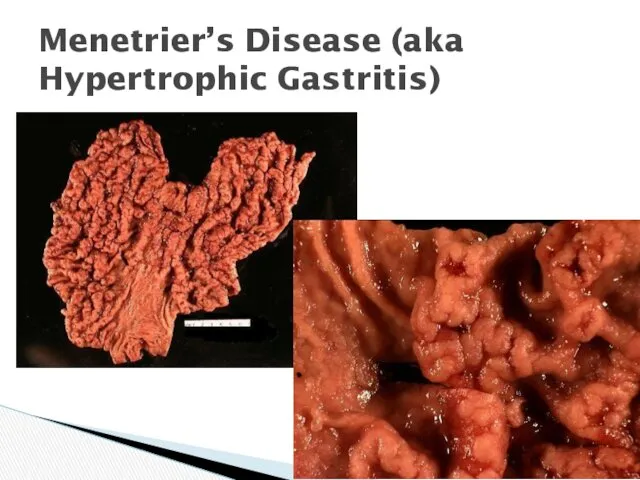
Menetrier’s Disease (aka Hypertrophic Gastritis)
Menetrier’s Disease (aka Hypertrophic Gastritis)
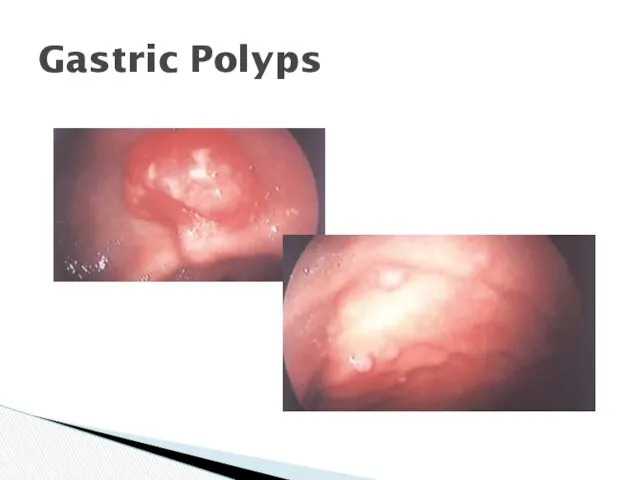
Gastric Polyps
Gastric Polyps
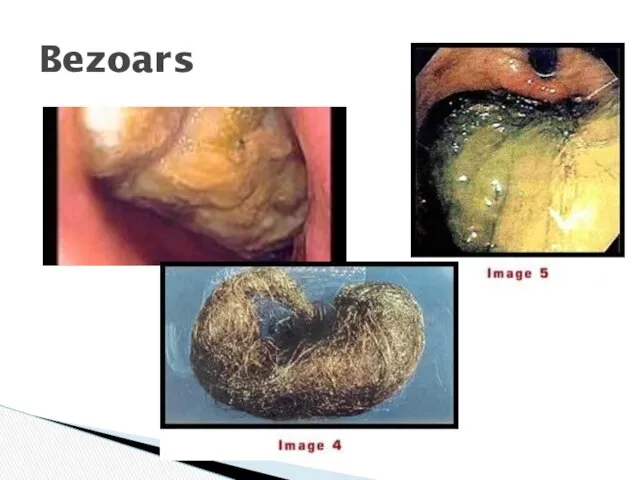
Bezoars
Bezoars
The “Culprit”
H. pylori
Treatment:
Triple therapy
The “Culprit”
H. pylori
Treatment:
Triple therapy
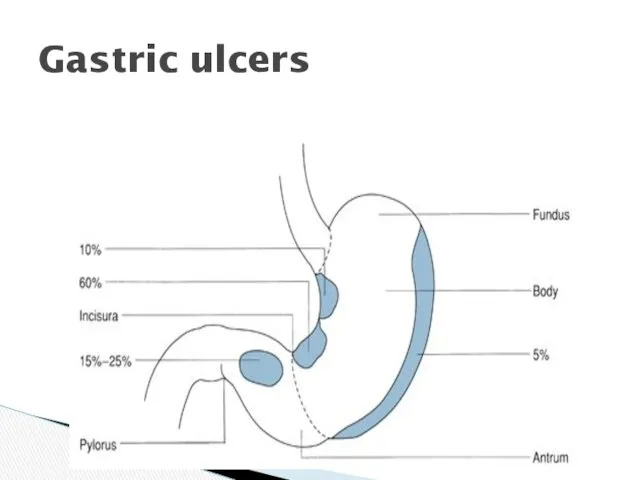
Gastric ulcers
Gastric ulcers

Gastric Ulcers
Gastric Ulcers
History of Peptic Ulcer Surgery
Harberer 1882- first gastric resection for ulcer
Billroth
History of Peptic Ulcer Surgery
Harberer 1882- first gastric resection for ulcer
Billroth
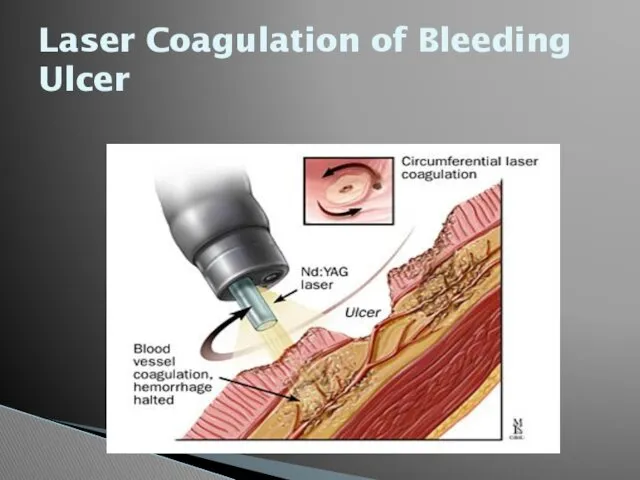
Laser Coagulation of Bleeding Ulcer
Laser Coagulation of Bleeding Ulcer
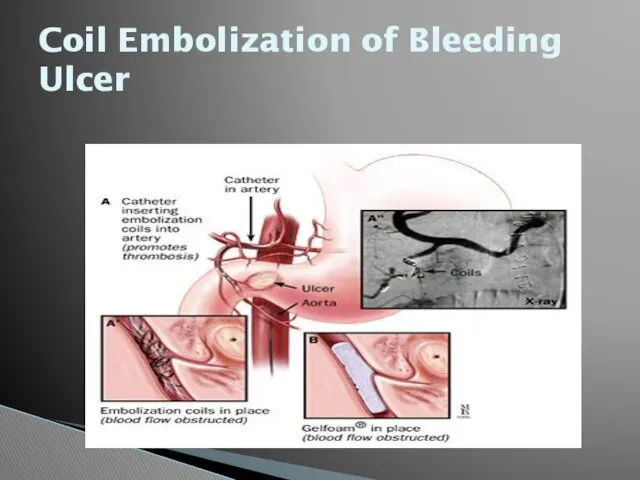
Coil Embolization of Bleeding Ulcer
Coil Embolization of Bleeding Ulcer
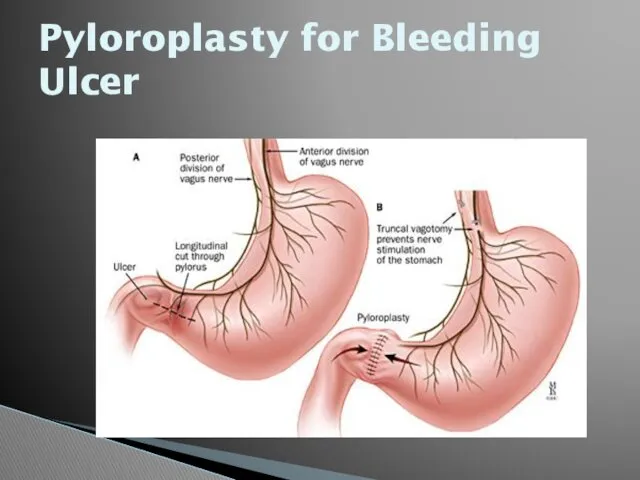
Pyloroplasty for Bleeding Ulcer
Pyloroplasty for Bleeding Ulcer
Open Surgical Procedures
Truncal vagotomy and pyloroplasty
Truncal vagotomy and gastrojejunostomy
Truncal vagotomy and
Open Surgical Procedures
Truncal vagotomy and pyloroplasty
Truncal vagotomy and gastrojejunostomy
Truncal vagotomy and
GASTROSTOMY
Temporary gastrostomy
Minimal gastrostomy
Vitzel’s gastrostomy
Stamm-Kader’s gastrostomy
Permanent gastrostomy
Toprover’s gastrostomy
Beck Jian’s gastrostomy
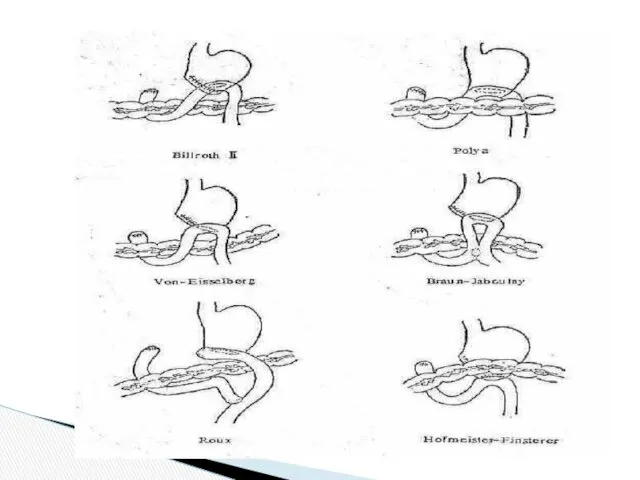
PARTIAL RESECTION OF
GASTROSTOMY
Temporary gastrostomy
Minimal gastrostomy
Vitzel’s gastrostomy
Stamm-Kader’s gastrostomy
Permanent gastrostomy
Toprover’s gastrostomy
Beck Jian’s gastrostomy
PARTIAL RESECTION OF
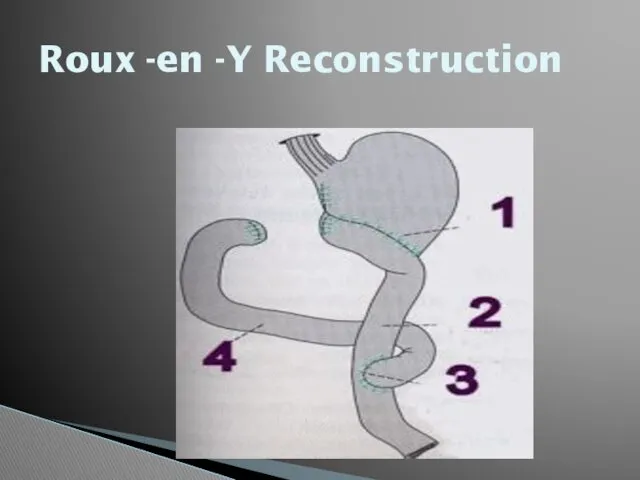
Roux -en -Y Reconstruction
Roux -en -Y Reconstruction
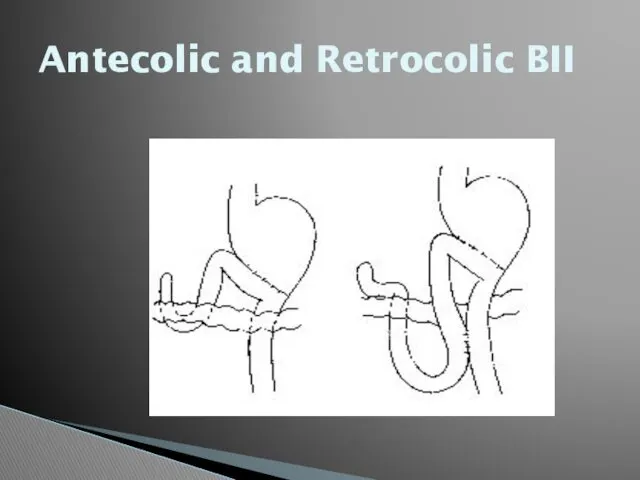
Antecolic and Retrocolic BII
Antecolic and Retrocolic BII
Truncal Vagotomy
Resect 1-2cm of each vagal trunk on distal esophagus.
Reduces acid
Truncal Vagotomy
Resect 1-2cm of each vagal trunk on distal esophagus.
Reduces acid
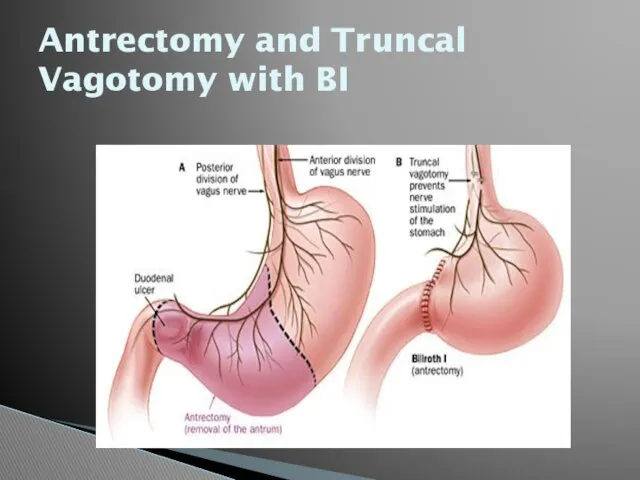
Antrectomy and Truncal Vagotomy with BI
Antrectomy and Truncal Vagotomy with BI
Truncal Vagotomy and Antrectomy
Entails distal gastrectomy of 50-60% of stomach.
Removes parietal
Truncal Vagotomy and Antrectomy
Entails distal gastrectomy of 50-60% of stomach.
Removes parietal
Selective Vagotomy
Total denervation of the stomach from diaphragmatic crus to pylorus.
Procedure
Selective Vagotomy
Total denervation of the stomach from diaphragmatic crus to pylorus.
Procedure
Highly Selective Vagotomy
Spares nerves of Latarjet, but divides vagal branches to
Highly Selective Vagotomy
Spares nerves of Latarjet, but divides vagal branches to
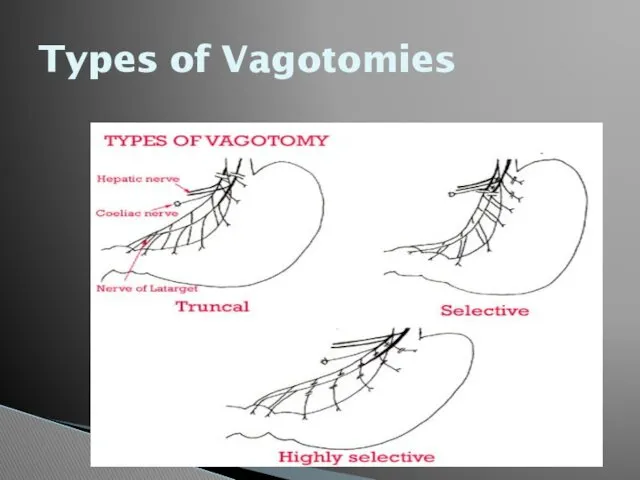
Types of Vagotomies
Types of Vagotomies
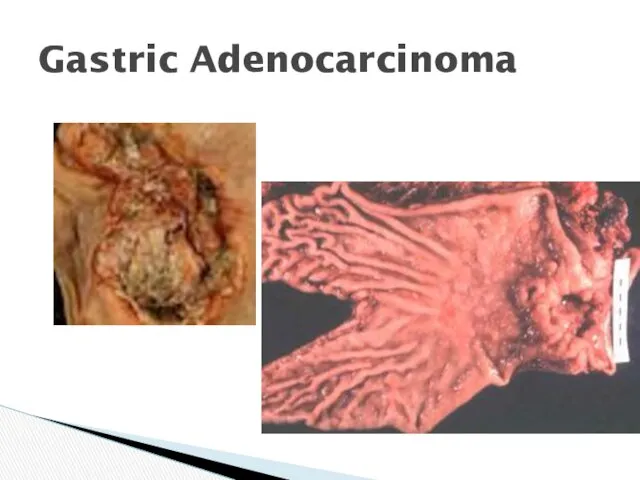
Gastric Adenocarcinoma
Gastric Adenocarcinoma
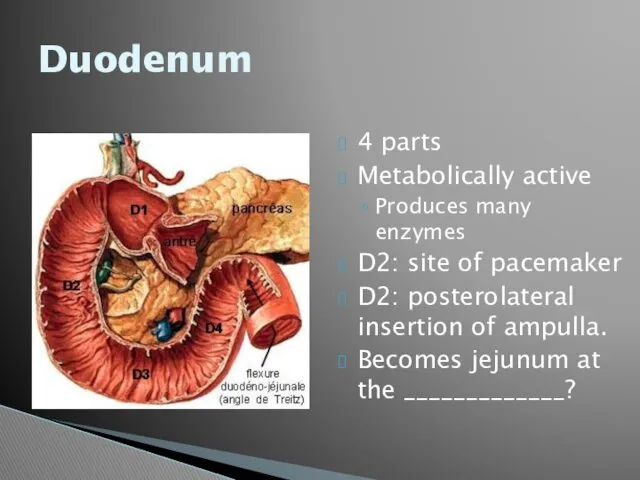
Duodenum
4 parts
Metabolically active
Produces many enzymes
D2: site of pacemaker
D2: posterolateral insertion of
Duodenum
4 parts
Metabolically active
Produces many enzymes
D2: site of pacemaker
D2: posterolateral insertion of
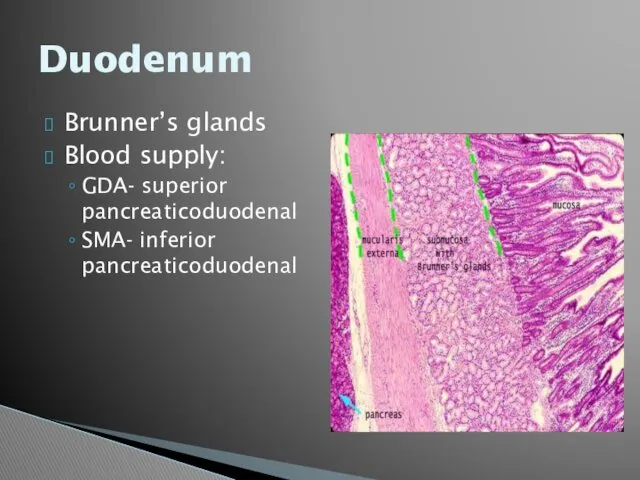
Duodenum
Brunner’s glands
Blood supply:
GDA- superior pancreaticoduodenal
SMA- inferior pancreaticoduodenal
Duodenum
Brunner’s glands
Blood supply:
GDA- superior pancreaticoduodenal
SMA- inferior pancreaticoduodenal
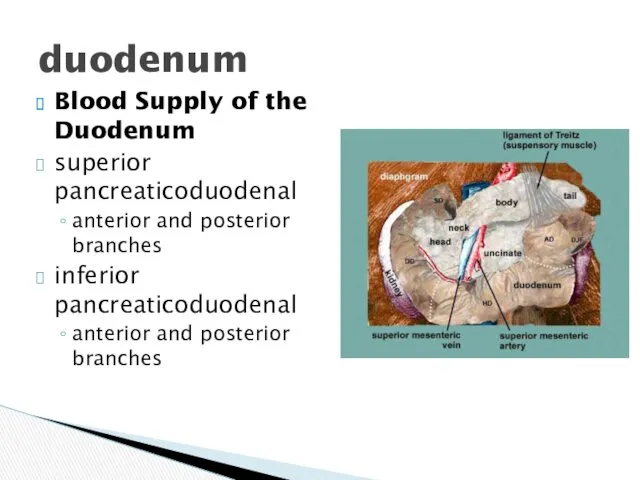
Blood Supply of the Duodenum
superior pancreaticoduodenal
anterior and posterior branches
inferior pancreaticoduodenal
anterior and
Blood Supply of the Duodenum
superior pancreaticoduodenal
anterior and posterior branches
inferior pancreaticoduodenal
anterior and
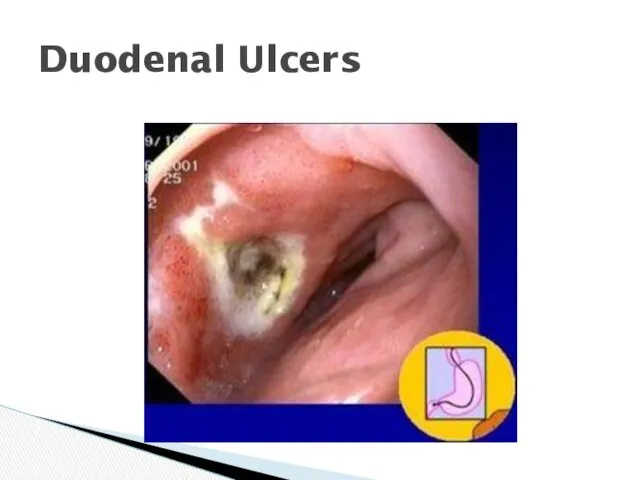
Duodenal Ulcers
Duodenal Ulcers
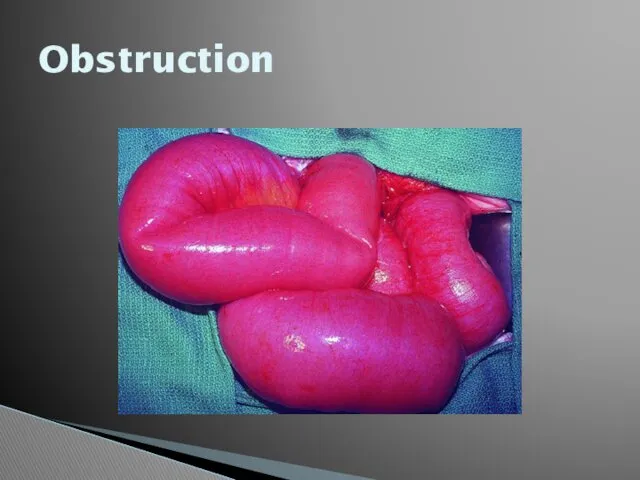
Obstruction
Obstruction
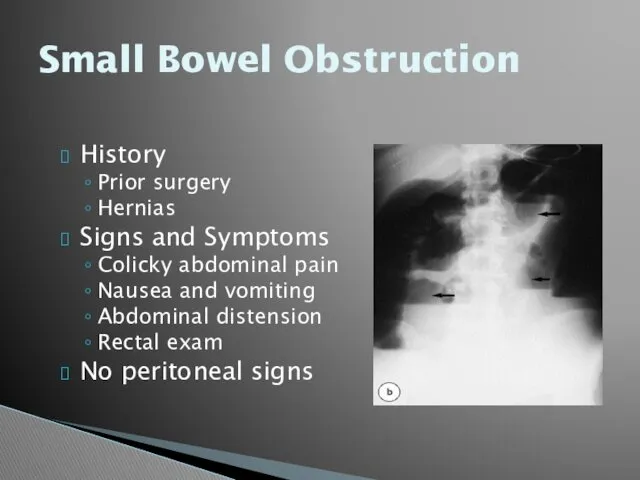
Small Bowel Obstruction
History
Prior surgery
Hernias
Signs and Symptoms
Colicky abdominal pain
Nausea and vomiting
Abdominal distension
Rectal
Small Bowel Obstruction
History
Prior surgery
Hernias
Signs and Symptoms
Colicky abdominal pain
Nausea and vomiting
Abdominal distension
Rectal
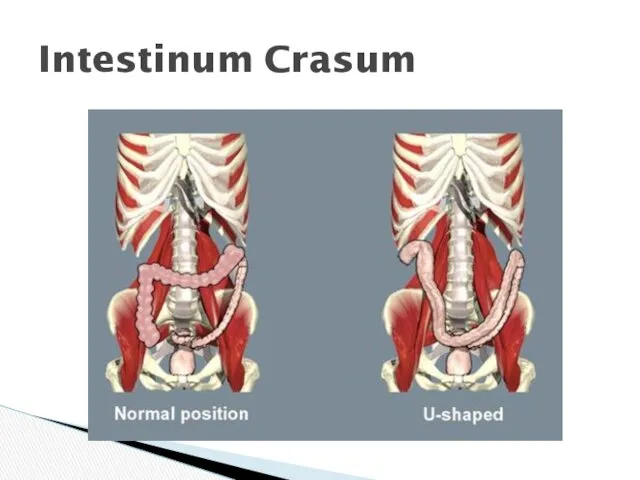
Intestinum Crasum
Intestinum Crasum
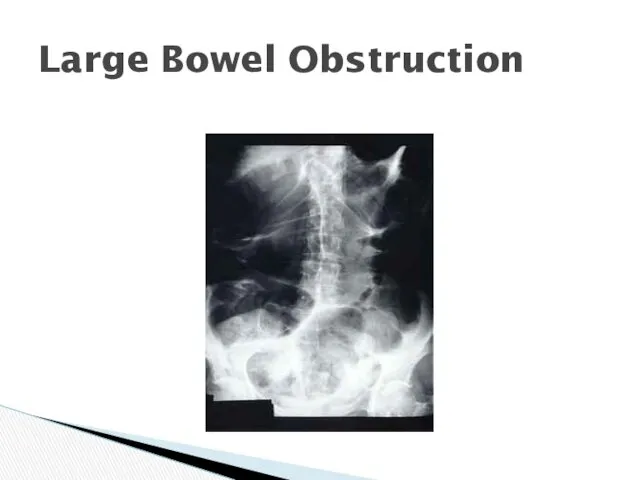
Large Bowel Obstruction
Large Bowel Obstruction
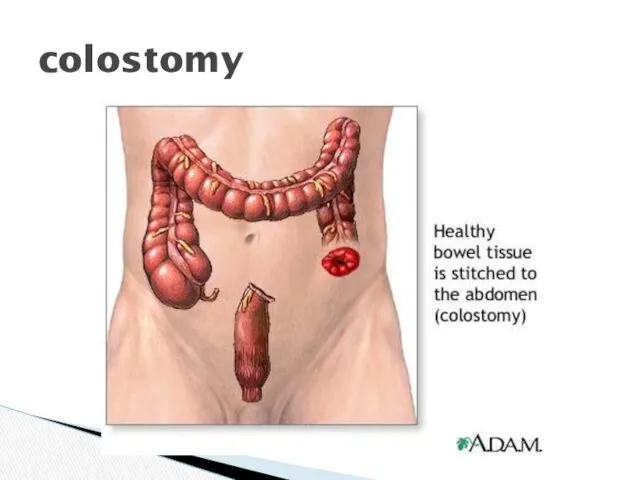
colostomy
colostomy
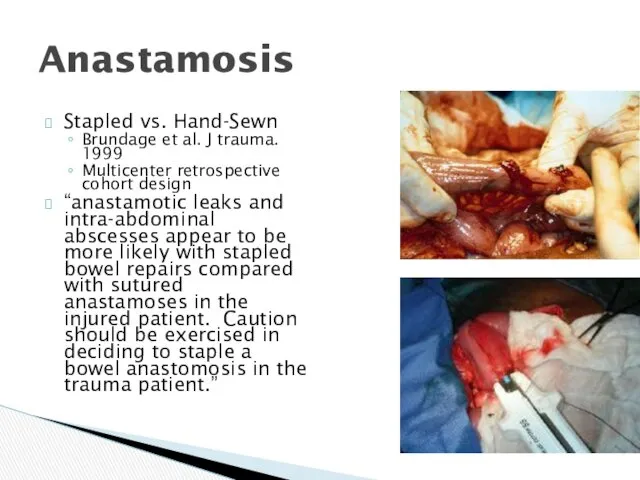
Anastamosis
Stapled vs. Hand-Sewn
Brundage et al. J trauma. 1999
Multicenter retrospective cohort design
“anastamotic
Anastamosis
Stapled vs. Hand-Sewn
Brundage et al. J trauma. 1999
Multicenter retrospective cohort design
“anastamotic
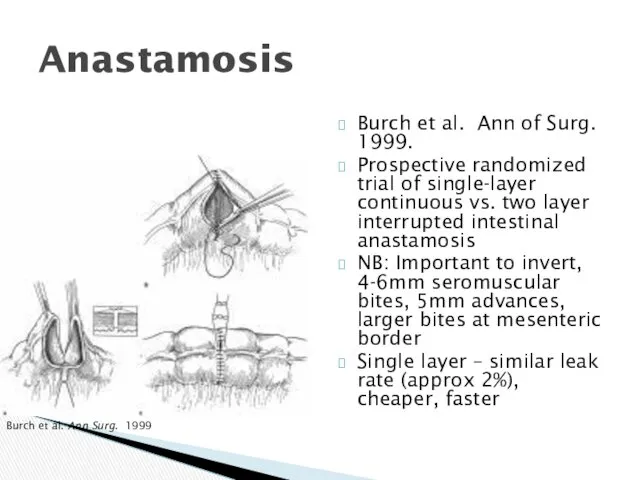
Anastamosis
Burch et al. Ann of Surg. 1999.
Prospective randomized trial of single-layer
Anastamosis
Burch et al. Ann of Surg. 1999.
Prospective randomized trial of single-layer
Appendix vermiformis
Appendix vermiformis
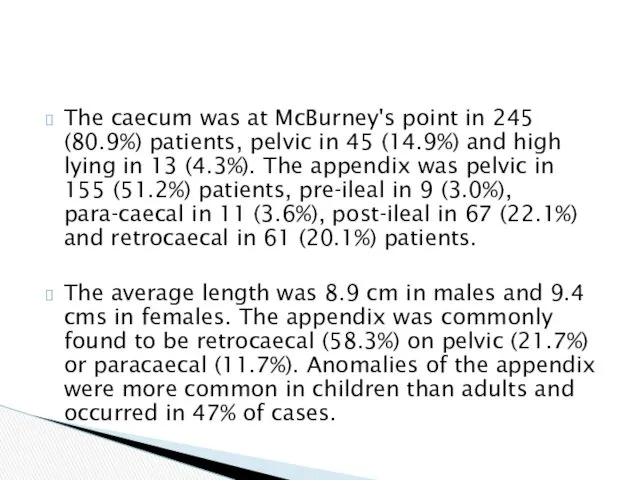
The caecum was at McBurney's point in 245 (80.9%) patients, pelvic
The caecum was at McBurney's point in 245 (80.9%) patients, pelvic
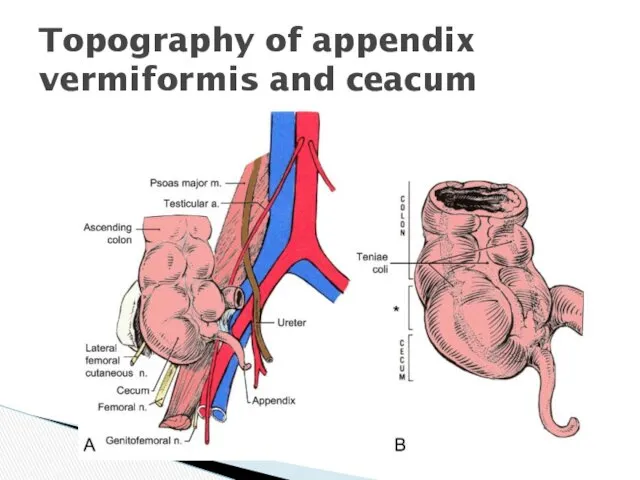
Topography of appendix vermiformis and ceacum
Topography of appendix vermiformis and ceacum
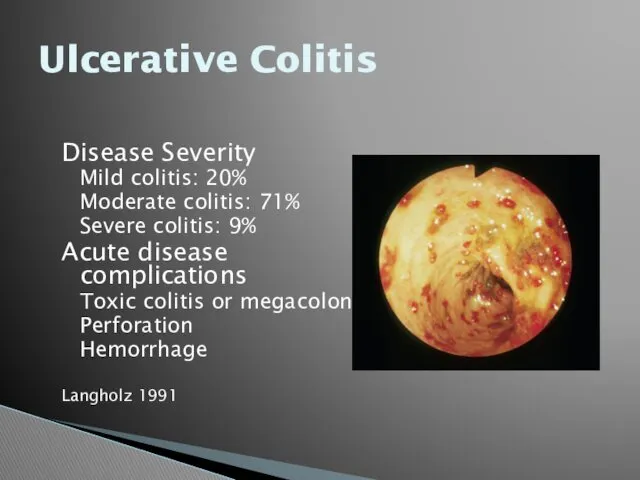
Ulcerative Colitis
Disease Severity
Mild colitis: 20%
Moderate colitis: 71%
Severe colitis: 9%
Acute disease complications
Toxic
Ulcerative Colitis
Disease Severity
Mild colitis: 20%
Moderate colitis: 71%
Severe colitis: 9%
Acute disease complications
Toxic
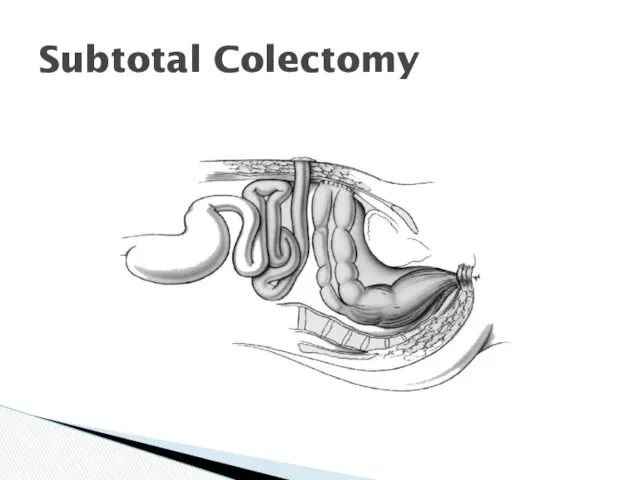
Subtotal Colectomy
Subtotal Colectomy
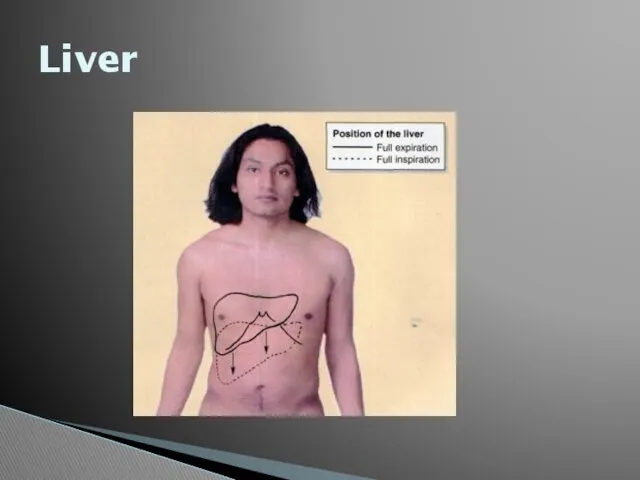
Liver
Liver
Liver
Liver
Mosby items and derived items © 2006 by Mosby, Inc.
Slide
Mosby items and derived items © 2006 by Mosby, Inc.
Slide
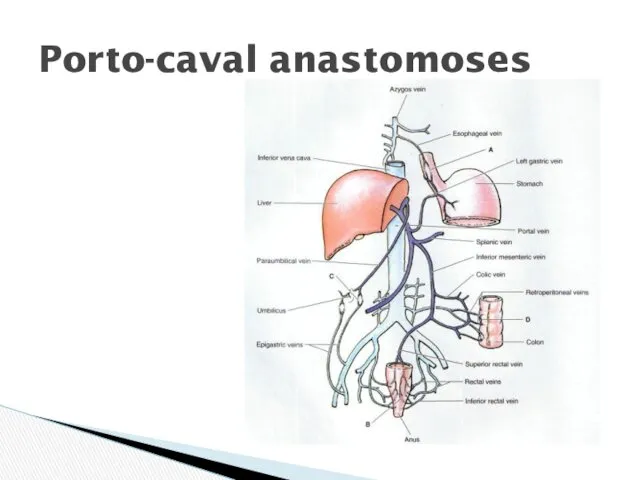
Porto-caval anastomoses
Porto-caval anastomoses
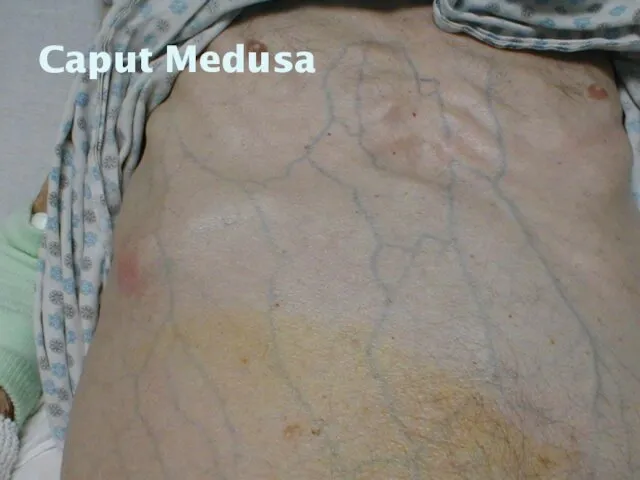
Caput Medusa
Caput Medusa

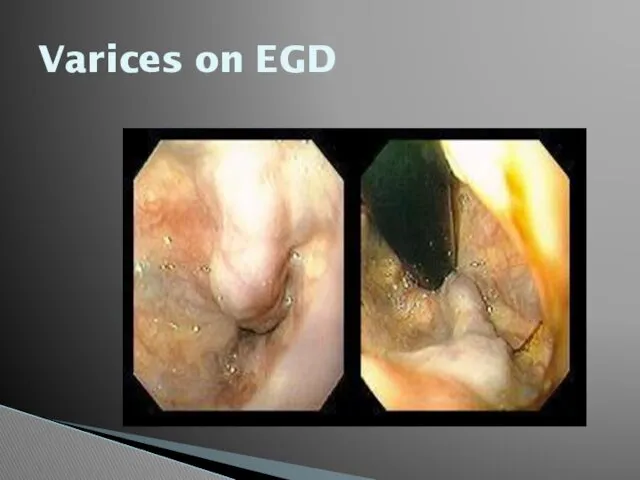
Varices on EGD
Varices on EGD
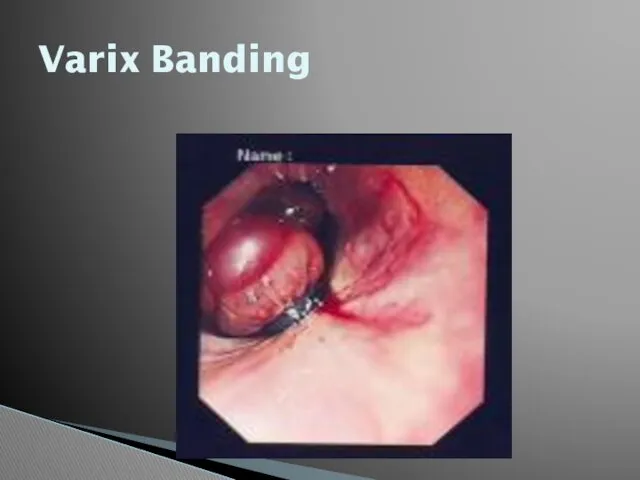
Varix Banding
Varix Banding
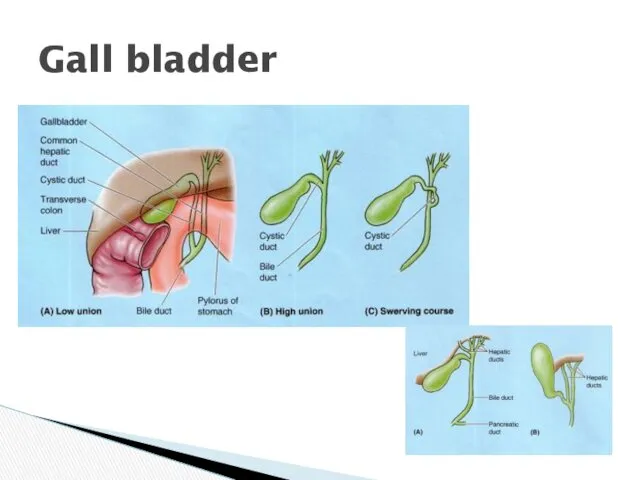
Gall bladder
Gall bladder
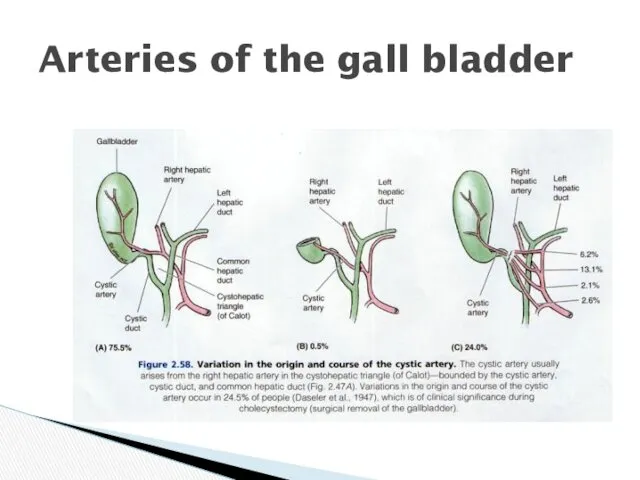
Arteries of the gall bladder
Arteries of the gall bladder
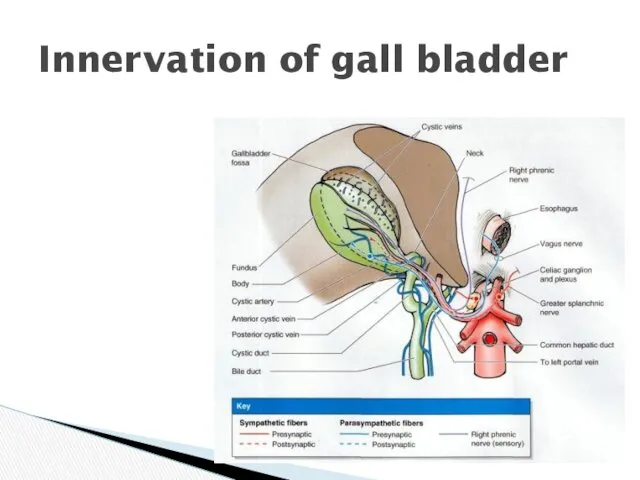
Innervation of gall bladder
Innervation of gall bladder
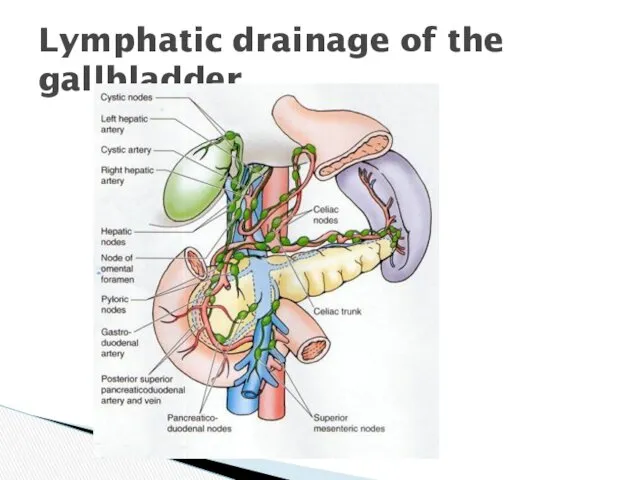
Lymphatic drainage of the gallbladder
Lymphatic drainage of the gallbladder

Harvest Time
Harvest Time
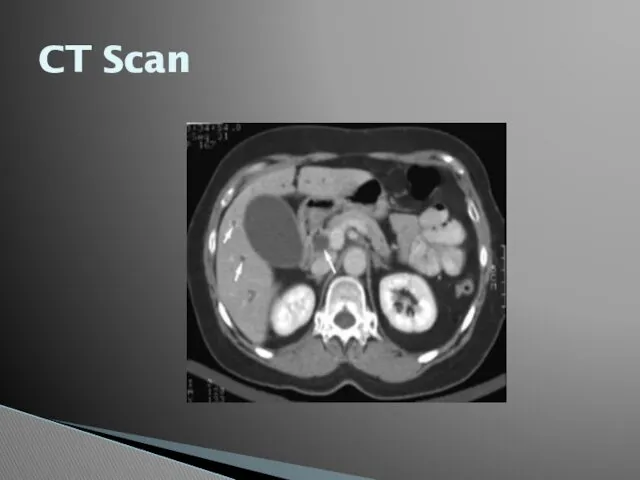
CT Scan
CT Scan

Plain Films
Plain Films

Ultrasound
Ultrasound
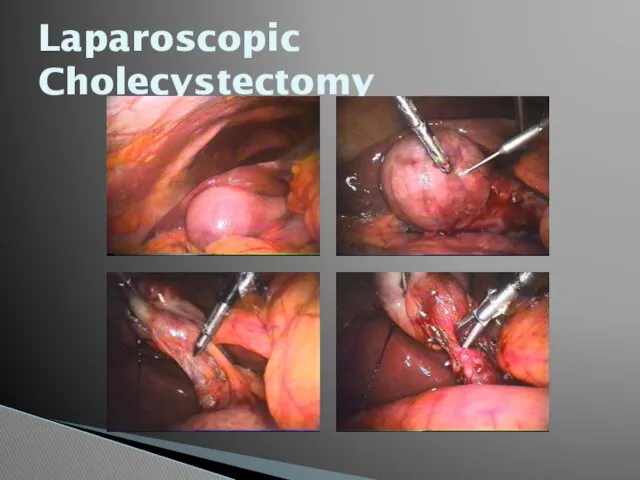
Laparoscopic Cholecystectomy
Laparoscopic Cholecystectomy
cancer
cancer
 Туберкулез животных
Туберкулез животных Гепато-лентикулярная дегенерация (гепато-церебральная дистрофия, болезнь Вильсона-Коновалова)
Гепато-лентикулярная дегенерация (гепато-церебральная дистрофия, болезнь Вильсона-Коновалова) Группы крови.. Иммунитет
Группы крови.. Иммунитет Ультразвуковая диапевтика в урологии
Ультразвуковая диапевтика в урологии Равновесные процессы в контроле качества фармацевтической субстанции Silver Nitrate
Равновесные процессы в контроле качества фармацевтической субстанции Silver Nitrate Дивертикулярная болезнь ободочной кишки у пожилых
Дивертикулярная болезнь ободочной кишки у пожилых Презентация ООИБ-ПНД
Презентация ООИБ-ПНД Болезни склеры. Клиника, диагностика, лечение
Болезни склеры. Клиника, диагностика, лечение Basic first aid
Basic first aid Профилактика заболеваний, передающихся половым путем
Профилактика заболеваний, передающихся половым путем Вплив тютюнопаління, алкоголю, наркотиків і токсинів на нервову систему та поведінку людини
Вплив тютюнопаління, алкоголю, наркотиків і токсинів на нервову систему та поведінку людини Женская и мужская стерилизация
Женская и мужская стерилизация Анафилактический шок
Анафилактический шок Неотложная помощь при гипертоническом кризе, обмороке, коллапсе, шоке у детей
Неотложная помощь при гипертоническом кризе, обмороке, коллапсе, шоке у детей Бауыр эхинококкозы
Бауыр эхинококкозы Применение лекарственных средств, используемых в иммунологии у беременных, в период лактации
Применение лекарственных средств, используемых в иммунологии у беременных, в период лактации Қартаюдың биологиялық,медициналық аспектілері. Қартаю теориялары
Қартаюдың биологиялық,медициналық аспектілері. Қартаю теориялары Паразитарные заболевания печени
Паразитарные заболевания печени Организация питания в ДОУ
Организация питания в ДОУ Строение и развитие периферических органов эндокринной системы
Строение и развитие периферических органов эндокринной системы Изготовление лекарственной формы по прописи, используя теоретические знания в соответствии с требованиями нд
Изготовление лекарственной формы по прописи, используя теоретические знания в соответствии с требованиями нд Ревматоидный артрит
Ревматоидный артрит Тіс анатомиясы
Тіс анатомиясы Особенности косметических средств и процедуры салонного ухода за жирной кожей
Особенности косметических средств и процедуры салонного ухода за жирной кожей Воспаление. Этиология воспаления
Воспаление. Этиология воспаления Ишемическая болезнь сердца. Клинические, лабораторные и инструментальные особенности
Ишемическая болезнь сердца. Клинические, лабораторные и инструментальные особенности Рентгеноанатомия опорно-двигательного аппарата
Рентгеноанатомия опорно-двигательного аппарата Нервная регуляция
Нервная регуляция