- Colonic Polyps

Содержание
- 2. Colon Polyps The term polyp of the colon refers to a protuberance into the lumen from
- 3. Non-neoplastic polyps Hyperplastic Mucosal Inflammatory Submucosal Adenomatous Serrated –mixed hyperplastic and adenomatous Hamartomous
- 4. Hyperplastic polyps Located in the rectosigmoid Rarely develop into colorectal cancers
- 5. Hyperplastic polyposis syndrome (HPS) refers to a condition characterized by multiple, large and/or proximal hyperplastic polyps
- 6. WHO criteria for HPS At least five hyperplastic polyps proximal to the sigmoid colon, of which
- 7. Mucosal polyps Mucosal polyps are small (usually
- 8. Inflammatory pseudo-polyps Inflammatory pseudopolyps are irregularly shaped islands of residual intact colonic mucosa that are the
- 9. Submucosal polyps Lymphoid aggregates, Lipomas, Leiomyomas, Pneumatosis cystoid intestinalis, Hemangiomas, Fibromas, Carcinoids, Metastatic lesions
- 10. Endoscopic Ultrasound Useful in defining the site of origin and for biopsy of sub-mucosal lesions if
- 11. Hamartomatous polyps Juvenile polyps Peutz-Jeghers polyps
- 12. Juvenile Polyps Juvenile polyps are hamartomatous lesions that consist of a lamina propria and dilated cystic
- 13. Familial Juvenile Polyposis FJP is associated with an increased risk for the development of colorectal cancer,
- 14. Peutz-Jeghers polyps The Peutz-Jeghers polyp is a hamartomatous lesion of glandular epithelium supported by smooth muscle
- 15. Peutz-Jeghers polyps Patients with PJS are at increased risk of both gastrointestinal (gastric, small bowel, colon,
- 16. ADENOMATOUS POLYPS About two-thirds of all colonic polyps are adenomas. Adenomas are by definition dysplastic and
- 17. ADENOMATOUS POLYPS The time for development of adenomas to cancer is about seven years. Approximately 30
- 18. Prevalence of adenomatous colonic polyps increases with age
- 19. Synchronous lesion An adenoma that is diagnosed at the same time as an index colorectal neoplasm
- 20. Metachronous lesion One that is diagnosed at least six months later is considered metachronous lesion
- 21. Pathologic classification The histologic features and size of colonic adenomas are the major determinants of their
- 22. Tubular adenomas Tubular adenomas account for more than 80 percent of colonic adenomas. They are characterized
- 23. Colonic adenoma
- 24. Villous adenomas Villous adenomas account for 5 to 15 percent of adenomas. They are characterized by
- 25. Tubulovillous adenomas Tubulovillous adenomas account for 5 to 15 percent of adenomas. Have 26 to 75
- 26. Polyp base Sessile - base is attached to the colon wall, Pedunculated if a mucosal stalk
- 27. Dysplasia All adenomas are dysplastic. A new system that recognizes two grades of dysplasia - HIGH
- 28. Invasive malignancy Invasive malignancy is defined by a breach of the muscularis mucosa by neoplastic cells.
- 29. Clinical presentation and natural history of Adenomas Adenomas are generally asymptomatic and are most often detected
- 30. ADVANCED ADENOMA Villous histology, Increasing polyp size, High-grade dysplasia
- 31. Polyp size & advanced features The proportion of adenomas showing advanced histologic features (high-grade dysplasia or
- 32. Age & advanced features Older age is also associated with high-grade dysplasia within an adenoma, independent
- 33. Advanced pathologic risk factors Adenomatous polyps >1 cm in diameter Adenomatous polyps with high-grade dysplasia Adenomatous
- 34. Detection and colonoscopic removal of polyps Colonoscopy is considered the optimal examination for the detection of
- 35. Detection and colonoscopic removal of polyps The colonoscopic miss rate determined by two same day endoscopic
- 36. Prevention Guidelines proposed by American College of Gastroenterology (ACG): A diet that is low in fat
- 37. Surveillance Patients with small rectal hyperplastic polyps should be considered to have normal colonoscopies, and therefore
- 38. Surveillance Patients with only 1 or 2 small ( tubular adenomas only low-grade dysplasia should have
- 39. Surveillance Patients with multiple (3-10) adenomas, adenoma > 1 cm, adenoma with villous features, high-grade dysplasia
- 40. Surveillance Patients who have more than 10 adenomas at 1 examination should be examined at a
- 41. Surveillance Patients with sessile adenomas that are removed piecemeal should be considered for follow-up evaluation at
- 42. Hereditary nonpolyposis colorectal cancer Colonoscopy every one to two years beginning at age 20 to 25,
- 43. Familial Adenomatous Polyposis Colonoscopy every 12 months starting at around age 10 to 12 and continuing
- 45. Скачать презентацию
Colon Polyps
The term polyp of the colon refers to a protuberance
Colon Polyps
The term polyp of the colon refers to a protuberance
Non-neoplastic polyps
Hyperplastic
Mucosal
Inflammatory
Submucosal
Adenomatous
Serrated –mixed hyperplastic and adenomatous
Hamartomous
Non-neoplastic polyps
Hyperplastic
Mucosal
Inflammatory
Submucosal
Adenomatous
Serrated –mixed hyperplastic and adenomatous
Hamartomous
Hyperplastic polyps
Located in the rectosigmoid
< 5 mm in size
Rarely
Hyperplastic polyps
Located in the rectosigmoid
< 5 mm in size
Rarely
Hyperplastic polyposis syndrome
(HPS) refers to a condition characterized by multiple, large
Hyperplastic polyposis syndrome
(HPS) refers to a condition characterized by multiple, large
WHO criteria for HPS
At least five hyperplastic polyps proximal to the
WHO criteria for HPS
At least five hyperplastic polyps proximal to the
Mucosal polyps
Mucosal polyps are small (usually <5 mm) excrescences of tissue
Mucosal polyps
Mucosal polyps are small (usually <5 mm) excrescences of tissue
Inflammatory pseudo-polyps
Inflammatory pseudopolyps are irregularly shaped islands of residual intact colonic
Inflammatory pseudo-polyps
Inflammatory pseudopolyps are irregularly shaped islands of residual intact colonic
Submucosal polyps
Lymphoid aggregates,
Lipomas,
Leiomyomas,
Pneumatosis cystoid intestinalis,
Hemangiomas,
Fibromas,
Carcinoids,
Submucosal polyps
Lymphoid aggregates,
Lipomas,
Leiomyomas,
Pneumatosis cystoid intestinalis,
Hemangiomas,
Fibromas,
Carcinoids,
Endoscopic Ultrasound
Useful in defining the site of origin and for biopsy
Endoscopic Ultrasound
Useful in defining the site of origin and for biopsy
Hamartomatous polyps
Juvenile polyps
Peutz-Jeghers polyps
Hamartomatous polyps
Juvenile polyps
Peutz-Jeghers polyps
Juvenile Polyps
Juvenile polyps are hamartomatous lesions that consist of a lamina
Juvenile Polyps
Juvenile polyps are hamartomatous lesions that consist of a lamina
Familial Juvenile Polyposis
FJP is associated with an increased risk for the
Familial Juvenile Polyposis
FJP is associated with an increased risk for the
Peutz-Jeghers polyps
The Peutz-Jeghers polyp is a hamartomatous lesion of glandular epithelium
Peutz-Jeghers polyps
The Peutz-Jeghers polyp is a hamartomatous lesion of glandular epithelium
Peutz-Jeghers polyps
Patients with PJS are at increased risk of both gastrointestinal
Peutz-Jeghers polyps
Patients with PJS are at increased risk of both gastrointestinal
ADENOMATOUS POLYPS
About two-thirds of all colonic polyps are adenomas.
Adenomas
ADENOMATOUS POLYPS
About two-thirds of all colonic polyps are adenomas.
Adenomas
ADENOMATOUS POLYPS
The time for development of adenomas to cancer is about
ADENOMATOUS POLYPS
The time for development of adenomas to cancer is about
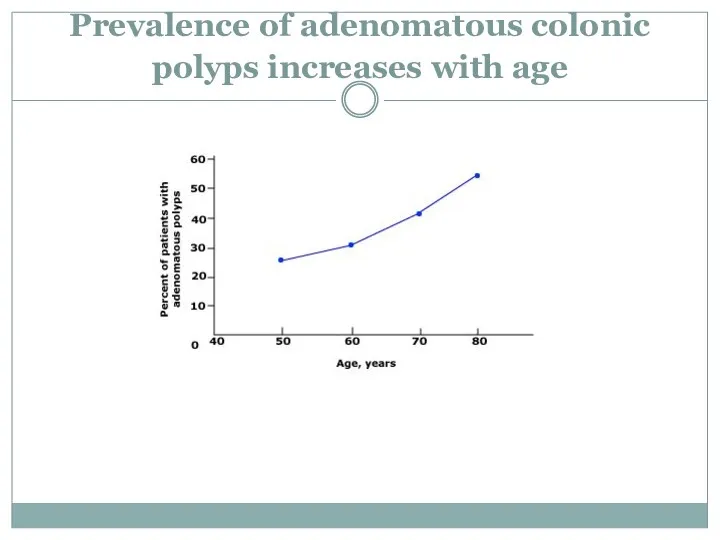
Prevalence of adenomatous colonic polyps increases with age
Prevalence of adenomatous colonic polyps increases with age
Synchronous lesion
An adenoma that is diagnosed at the same time as
Synchronous lesion
An adenoma that is diagnosed at the same time as
Metachronous lesion
One that is diagnosed at least six months later is
Metachronous lesion
One that is diagnosed at least six months later is
Pathologic classification
The histologic features and size of colonic adenomas are
Pathologic classification
The histologic features and size of colonic adenomas are
Tubular adenomas
Tubular adenomas account for more than 80 percent of colonic
Tubular adenomas
Tubular adenomas account for more than 80 percent of colonic
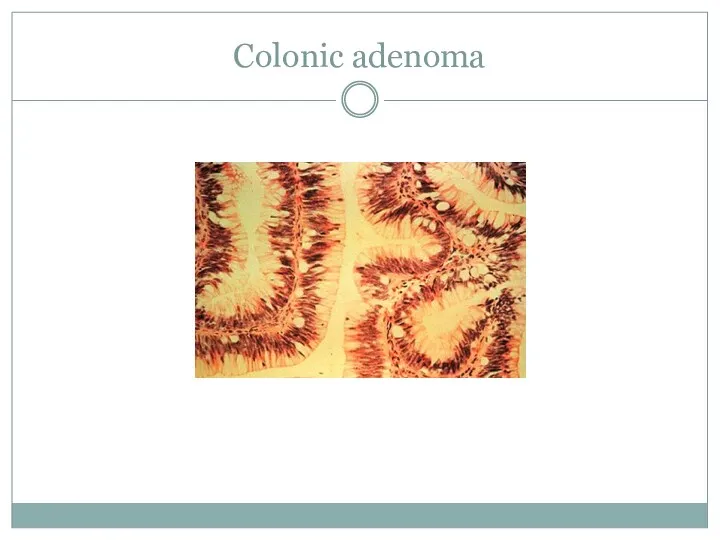
Colonic adenoma
Colonic adenoma
Villous adenomas
Villous adenomas account for 5 to 15 percent of adenomas.
Villous adenomas
Villous adenomas account for 5 to 15 percent of adenomas.
Tubulovillous adenomas
Tubulovillous adenomas account for 5 to 15 percent of adenomas.
Tubulovillous adenomas
Tubulovillous adenomas account for 5 to 15 percent of adenomas.
Polyp base
Sessile - base is attached to the colon wall,
Pedunculated
Polyp base
Sessile - base is attached to the colon wall,
Pedunculated
Dysplasia
All adenomas are dysplastic.
A new system that recognizes two grades
Dysplasia
All adenomas are dysplastic.
A new system that recognizes two grades
Invasive malignancy
Invasive malignancy is defined by a breach of the muscularis
Invasive malignancy
Invasive malignancy is defined by a breach of the muscularis
Clinical presentation and
natural history of Adenomas
Adenomas are generally asymptomatic and
Clinical presentation and
natural history of Adenomas
Adenomas are generally asymptomatic and
ADVANCED ADENOMA
Villous histology,
Increasing polyp size,
High-grade dysplasia
ADVANCED ADENOMA
Villous histology,
Increasing polyp size,
High-grade dysplasia
Polyp size & advanced features
The proportion of adenomas showing advanced histologic
Polyp size & advanced features
The proportion of adenomas showing advanced histologic
Age & advanced features
Older age is also associated with high-grade dysplasia
Age & advanced features
Older age is also associated with high-grade dysplasia
Advanced pathologic risk factors
Adenomatous polyps >1 cm in diameter
Adenomatous polyps
Advanced pathologic risk factors
Adenomatous polyps >1 cm in diameter
Adenomatous polyps
Detection and colonoscopic removal of polyps
Colonoscopy is considered the optimal examination
Detection and colonoscopic removal of polyps
Colonoscopy is considered the optimal examination
Detection and colonoscopic removal of polyps
The colonoscopic miss rate determined by
Detection and colonoscopic removal of polyps
The colonoscopic miss rate determined by
Prevention
Guidelines proposed by American College of Gastroenterology (ACG):
A diet that is
Prevention
Guidelines proposed by American College of Gastroenterology (ACG):
A diet that is
Surveillance
Patients with small rectal hyperplastic polyps should be considered to have
Surveillance
Patients with small rectal hyperplastic polyps should be considered to have
Surveillance
Patients with
only 1 or 2
small (<1 cm)
tubular adenomas
Surveillance
Patients with
only 1 or 2
small (<1 cm)
tubular adenomas
Surveillance
Patients with
multiple (3-10) adenomas,
adenoma > 1 cm,
adenoma with
Surveillance
Patients with
multiple (3-10) adenomas,
adenoma > 1 cm,
adenoma with
Surveillance
Patients who have
more than 10 adenomas at 1 examination
should
Surveillance
Patients who have
more than 10 adenomas at 1 examination
should
Surveillance
Patients with
sessile adenomas
that are removed piecemeal
should be considered
Surveillance
Patients with
sessile adenomas
that are removed piecemeal
should be considered
Hereditary nonpolyposis colorectal cancer
Colonoscopy every one to two years beginning at
Hereditary nonpolyposis colorectal cancer
Colonoscopy every one to two years beginning at
Familial Adenomatous Polyposis
Colonoscopy every 12 months starting at around age 10
Familial Adenomatous Polyposis
Colonoscopy every 12 months starting at around age 10
 Обстеження пацієнтів в клініці ортопедичної стоматології
Обстеження пацієнтів в клініці ортопедичної стоматології Рентгеноанатомия ЖКТ
Рентгеноанатомия ЖКТ Анализ регионального опыта внедрения независимой оценки качества оказания услуг медицинскими организациями
Анализ регионального опыта внедрения независимой оценки качества оказания услуг медицинскими организациями Технические методы диагностических исследований и лечебных воздействий
Технические методы диагностических исследований и лечебных воздействий Патология вилочковой железы
Патология вилочковой железы Ұрықтану. Жүктілер физиологиясы. Жүктілік диагностикасы. Акушериядағы зерттеу әдістері
Ұрықтану. Жүктілер физиологиясы. Жүктілік диагностикасы. Акушериядағы зерттеу әдістері Микробиология холеры
Микробиология холеры Трансмиссивная (кровяная) инфекция
Трансмиссивная (кровяная) инфекция Қазіргі балалар хирургиясындағы науқастарға болжам мен реабилитация
Қазіргі балалар хирургиясындағы науқастарға болжам мен реабилитация Ревматоидтык артрит
Ревматоидтык артрит Автоматизация рабочего места администратора отделения травматологии
Автоматизация рабочего места администратора отделения травматологии Атеросклероз. Ишемическая болезнь сердца
Атеросклероз. Ишемическая болезнь сердца Қазақстандағы денсаулық сақтау ұйымы және бағдарламалары
Қазақстандағы денсаулық сақтау ұйымы және бағдарламалары Кома жағдайлардың ажырату диагностикасы
Кома жағдайлардың ажырату диагностикасы Жедел бүйрек жеткіліксіздігі
Жедел бүйрек жеткіліксіздігі Дисфункциональные маточные кровотечения
Дисфункциональные маточные кровотечения Шок (сілейме) дегеніміз
Шок (сілейме) дегеніміз Медико-этические и социально-правовые аспекты современной трансплантологии
Медико-этические и социально-правовые аспекты современной трансплантологии Безопасность медицинского труда. (Тема 1.12)
Безопасность медицинского труда. (Тема 1.12) Неврит и невралгия лицевого нерва
Неврит и невралгия лицевого нерва Рак шейки матки
Рак шейки матки Оказание помощи детям при коклюше, ветряной оспе, эпидемическом паротите
Оказание помощи детям при коклюше, ветряной оспе, эпидемическом паротите Методы лучевого исследования печени и желчевыделительной системы. (Лекция 35)
Методы лучевого исследования печени и желчевыделительной системы. (Лекция 35) Диссеминированный туберкулез легких
Диссеминированный туберкулез легких Аллергия
Аллергия Этиология, определение понятия. Причины, условия и факторы болезни. Определение понятий. Виды
Этиология, определение понятия. Причины, условия и факторы болезни. Определение понятий. Виды Изменения в законодательстве в сфере медико-социальной экспертизы
Изменения в законодательстве в сфере медико-социальной экспертизы Острый аппендицит. История учения об аппендиците. Анатомо-физиологические особенности
Острый аппендицит. История учения об аппендиците. Анатомо-физиологические особенности