- Development of CNS in embrio. Clinical evaluation of abnormalities

Содержание
- 2. Anatomo-physiological peculiarities of CNS in children and their clinical importance
- 3. The central nervous system appears at the beginning of the 3rd week as a slipper-shaped plate
- 4. Its lateral edges soon become elevated to form the neural folds. With further development, the neural
- 5. Neural tube defects account for the most congenital anomalies of the CNS and result from the
- 6. Neural tube defects (NTDs) spina bifida occulta meningocele myelomeningocele encephalocele anencephal
- 7. Neural tube defects (NTDs) can be diagnosed prenatally by ultrasound, and by determination of ά-fetoprotein (AFP)
- 8. Neural tube defects (NTDs) Meningocele (Meningoencephalocele) is herniation of meninges and brain(medulla) through a defect in
- 9. lumbar meningomyelocele in a 3-day-infant Neural tube defects (NTDs)
- 10. The sloping forehead and small head circumference are evident, although progressive ventricular enlargement often subsequently occurs
- 11. In embryo at its cephalic end of the neural tube the brain bladders are forming from
- 12. Hemispheres of the brain are developed from the first brain bladder. Errors of embryogenesis, connected with
- 13. Hydranencephaly Magnetic resonance imaging (MRI) shows the brain stem and spinal cord with some remnants of
- 14. CSF (cerebral spinal fluid) CSF flow results from the pressure gradient that exists between the ventricular
- 15. CSF Hydrocephalus resulting from CSF accumulation inside the brain is called internal hydrocephalus.
- 16. The cranial computerized tomogram (CT) of the infant`s brain with congenital virus-associated encephalopathy Cerebral atrophy with
- 17. CSF is absorbed primarily by the arachnoid villi through tight junctions of their endothelium by the
- 18. External hydrocephalus in the newborn with in utero infection of the brain (MRI)
- 19. Features of CNS in fetus and newborn The brain development is characterizing by gradual formation and
- 20. Features of CNS in fetus and newborn (continue) There is not clear differentiation of the brain’s
- 21. Features of CNS in fetus and newborn (continue) The blood-brain barrier (BBB) of the fetus and
- 22. Features of CNS in fetus and newborn Central and peripheral neurons form myelin coating gradually. Myelinization
- 23. Features of CNS in fetus and newborn The features of the brain vascular system of fetus
- 24. Neurological examination
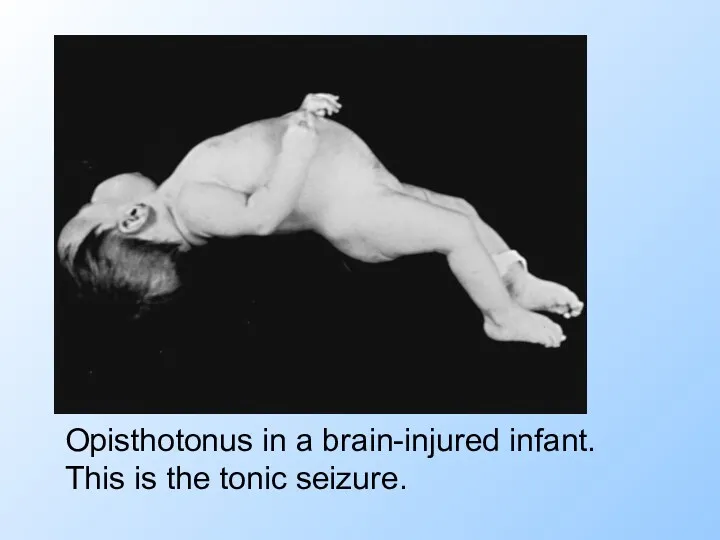
- 25. Neurologic evaluation of the child. Complaints&History. Seizures (convulsion) are involuntary, violent contraction of muscles. Seizures may
- 26. Opisthotonus in a brain-injured infant. This is the tonic seizure.
- 27. Objective neurological examination of the child should include 4 main diagnostic aspects: 1. Level of consciousness
- 28. A well child is conscious, alert and responsive Level of consciousness (LOC)
- 29. Level of consciousness (LOC) Lethargy or pathological sleepy (somnolence) is possible to determine as an unusual
- 30. Level of consciousness (LOC) This is a child with meningitis. The child is somnolent and can
- 31. Stages of coma Stupor: The stuporous patient arouses from sleep only after painful stimuli. Verbal responses
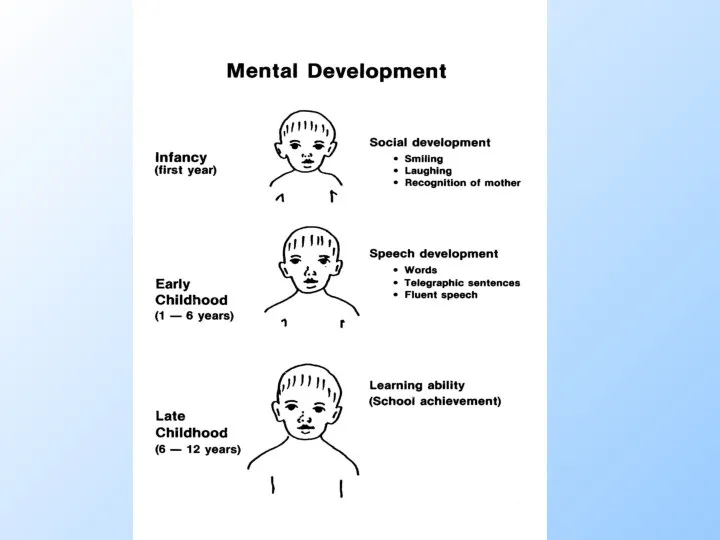
- 32. Mental development
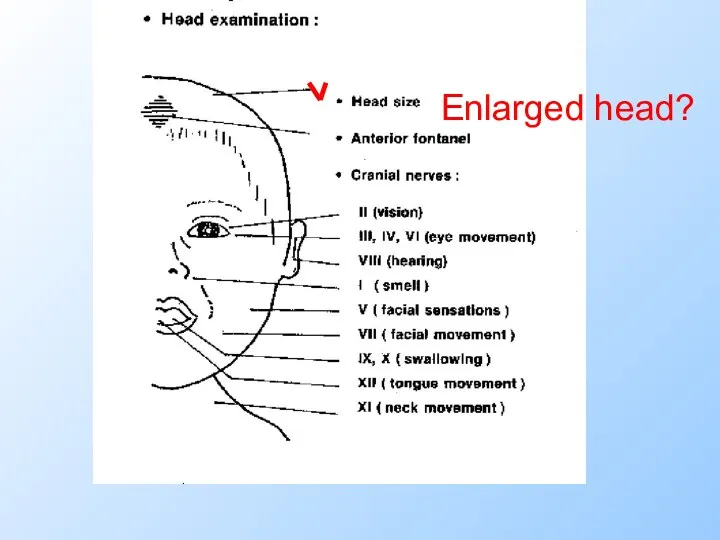
- 34. Head size
- 35. Enlarged head?
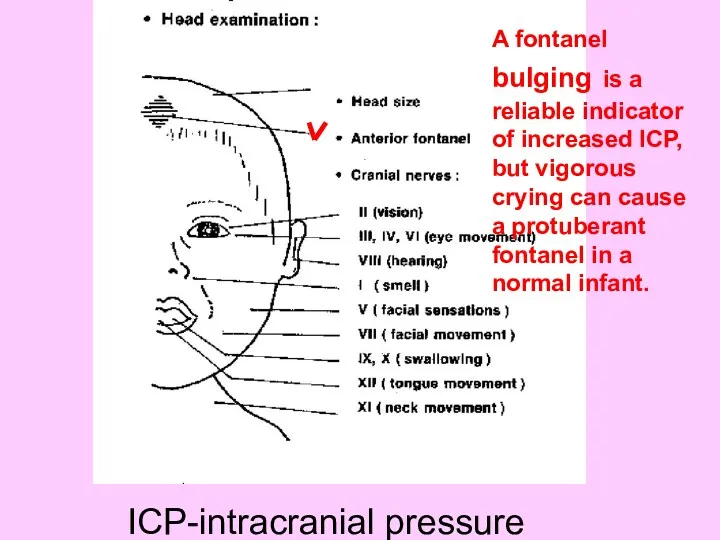
- 36. AF&PF
- 37. A fontanel bulging is a reliable indicator of increased ICP, but vigorous crying can cause a
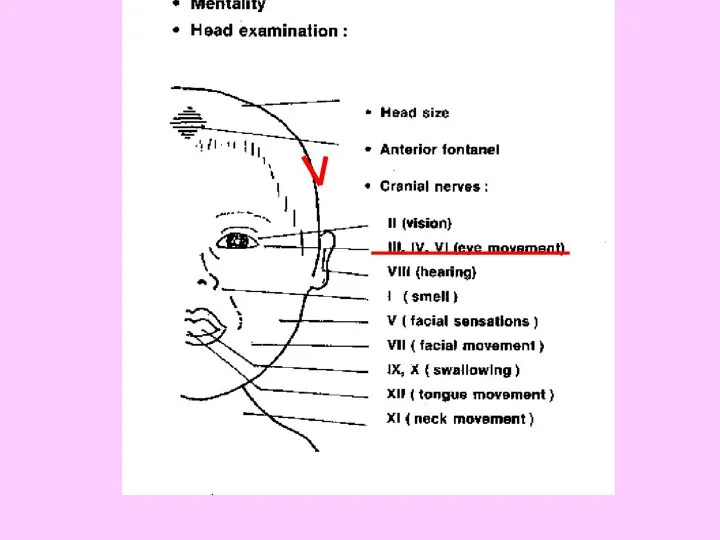
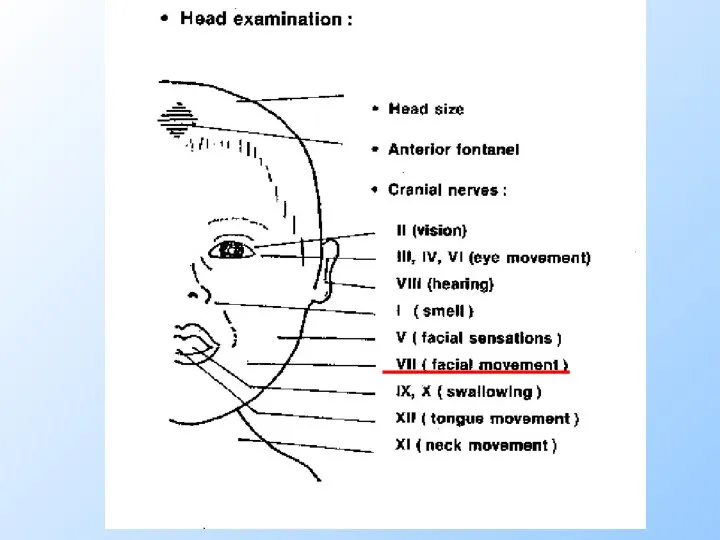
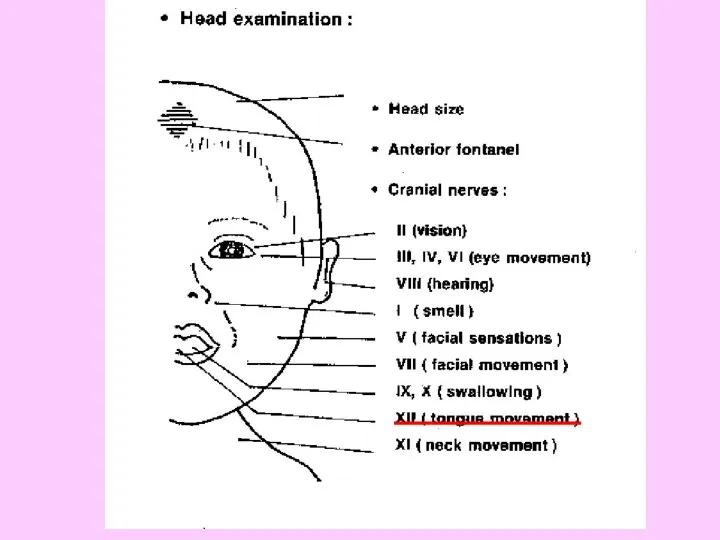
- 38. Cranial nerves
- 40. Oculomotor (3-rd) nerve paresis: ptosis (impossibility to lift an upper eyelid) and removal of an eyeball
- 42. Facial nerve palsy Facial nerve palsy
- 43. Facial nerve palsy. Notice the loss of the nasolabial fold and the mouth deviated to the
- 44. A newborn with right facial palsy
- 45. choking
- 47. Unilateral (right-side) hypoglossal (12th) nerve paresis. Tongue deviation.
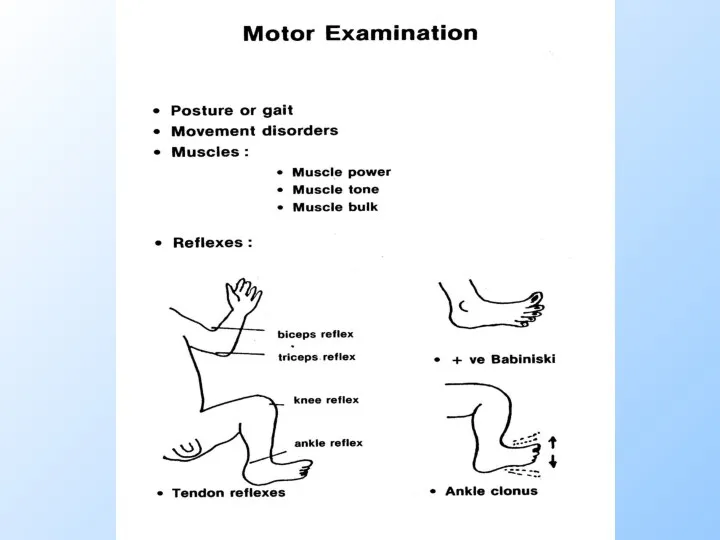
- 48. Motor examination
- 50. Abnormal gaits The spastic gait Circumduction gait Cerebellar ataxia waddling gait clumsy, tentative gait
- 51. Movement disorders Paralysis (palsy) – the absence of any voluntary movements Paresis is incomplete paralysis Ataxia
- 52. A newborn with brachial right sided paralysis (palsy). The arm hangs limp alongside the body and
- 53. Movement disorders Dystonia - slow twisting movements of limbs or trunk (alternation of a hypotonia with
- 54. Muscles Examination includes assessment of muscles’ development: wasting, pseudohypertrophy Tone: hypotonia, hypertonia Strength: increase, decrease
- 55. Posterior aspect of the legs of a father and his 6-year-old son with a rare autosomal
- 56. Hypotonia On ventral suspension, the baby assumes the position of a rag doll. When pulled up
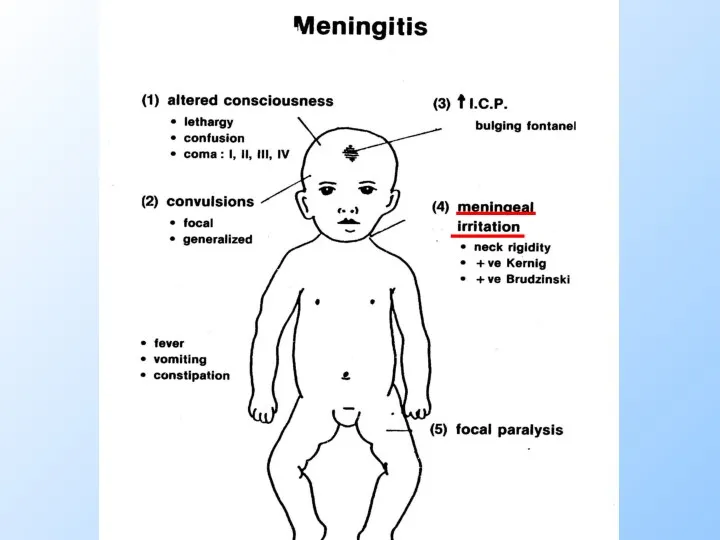
- 57. Main semiotics of CNS disorders. Meningitis.
- 59. Examination for neck rigidity in older child Meningeal irritation
- 60. Brudzinski’s sign Meningeal irritation
- 61. Kernig’s sign Meningeal irritation
- 62. LP The lumbar punction confirms the meningitis
- 63. Normal Values for Cerebrospinal Fluid (CSF)
- 64. CSF finding in bacterial meningitis ICP - increased White blood cell count, μL - 100 –
- 66. Скачать презентацию
Anatomo-physiological peculiarities
of CNS in children and their clinical
importance
Anatomo-physiological peculiarities
of CNS in children and their clinical
importance
The central nervous system appears at the beginning of the 3rd
The central nervous system appears at the beginning of the 3rd
Its lateral edges soon become elevated to form the neural folds.
Its lateral edges soon become elevated to form the neural folds.
Neural tube defects account for the most congenital anomalies of the
Neural tube defects account for the most congenital anomalies of the
Neural tube defects (NTDs)
spina bifida occulta
meningocele
myelomeningocele
encephalocele
anencephal
Neural tube defects (NTDs)
spina bifida occulta
meningocele
myelomeningocele
encephalocele
anencephal
Neural tube defects (NTDs)
can be diagnosed prenatally by ultrasound, and by
Neural tube defects (NTDs)
can be diagnosed prenatally by ultrasound, and by
Neural tube defects (NTDs)
Meningocele (Meningoencephalocele) is herniation of meninges and brain(medulla)
Neural tube defects (NTDs)
Meningocele (Meningoencephalocele) is herniation of meninges and brain(medulla)
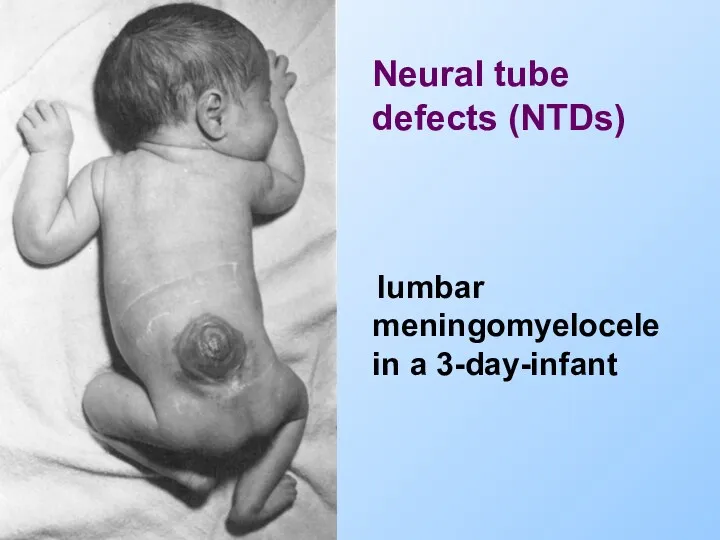
lumbar meningomyelocele in a 3-day-infant
Neural tube defects (NTDs)
lumbar meningomyelocele in a 3-day-infant
Neural tube defects (NTDs)
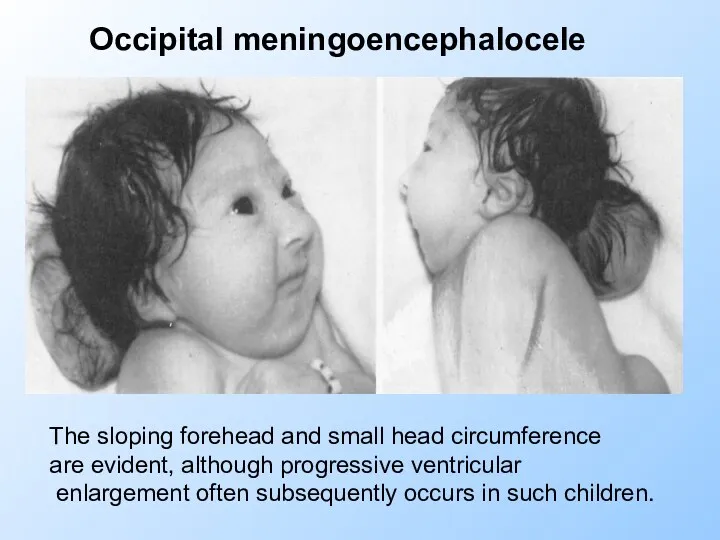
The sloping forehead and small head circumference
are evident, although progressive
The sloping forehead and small head circumference
are evident, although progressive
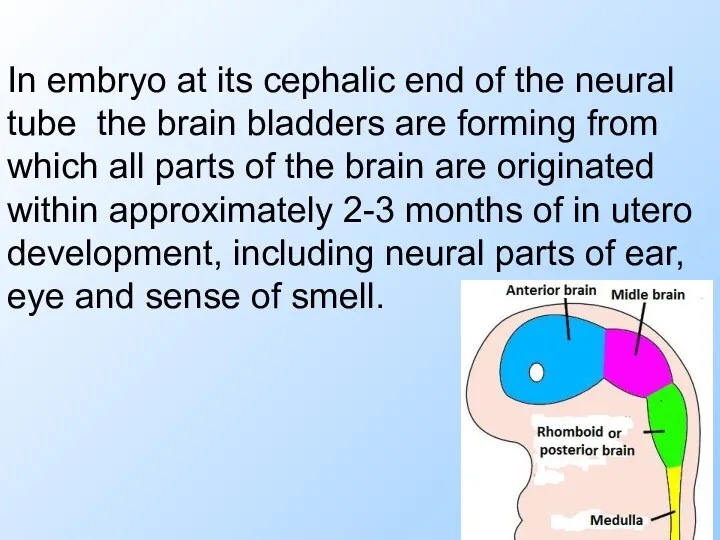
In embryo at its cephalic end of the neural tube the
In embryo at its cephalic end of the neural tube the
Hemispheres of the brain are developed from the first brain bladder.
Hemispheres of the brain are developed from the first brain bladder.
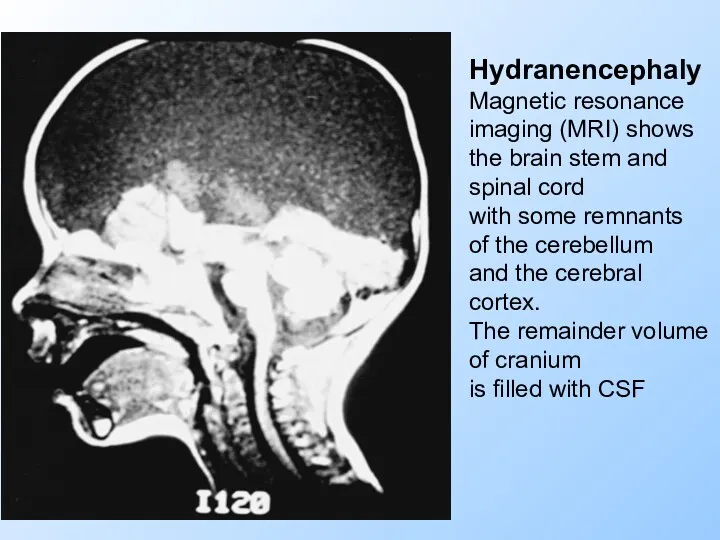
Hydranencephaly
Magnetic resonance
imaging (MRI) shows
the brain stem and
spinal cord
with some
Hydranencephaly
Magnetic resonance
imaging (MRI) shows
the brain stem and
spinal cord
with some
CSF (cerebral spinal fluid)
CSF flow results from the pressure gradient that
CSF (cerebral spinal fluid)
CSF flow results from the pressure gradient that
CSF
Hydrocephalus resulting from CSF accumulation inside the brain is called internal
CSF
Hydrocephalus resulting from CSF accumulation inside the brain is called internal
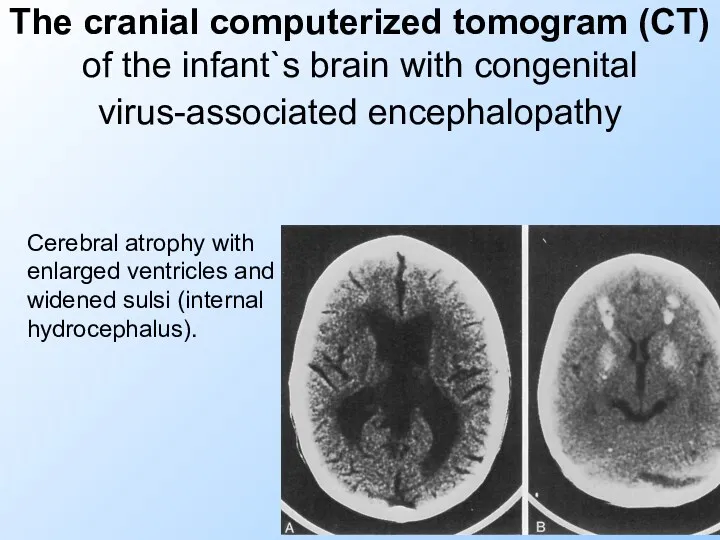
The cranial computerized tomogram (CT) of the infant`s brain with congenital
The cranial computerized tomogram (CT) of the infant`s brain with congenital
CSF is absorbed primarily by the arachnoid villi through tight junctions
CSF is absorbed primarily by the arachnoid villi through tight junctions
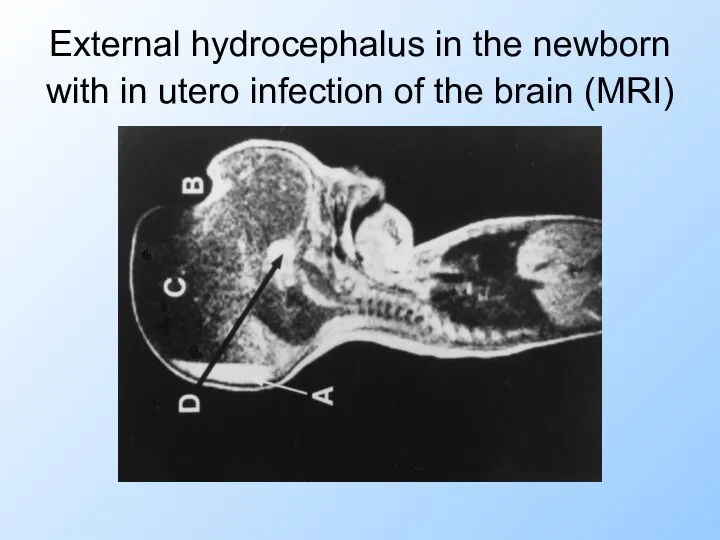
External hydrocephalus in the newborn with in utero infection of the
External hydrocephalus in the newborn with in utero infection of the
Features of CNS in fetus and newborn
The brain development is characterizing
Features of CNS in fetus and newborn
The brain development is characterizing
Features of CNS in fetus and newborn (continue)
There is not clear
Features of CNS in fetus and newborn (continue)
There is not clear
Features of CNS in fetus and newborn (continue)
The blood-brain barrier (BBB)
Features of CNS in fetus and newborn (continue)
The blood-brain barrier (BBB)
Features of CNS in fetus and newborn
Central and peripheral neurons form
Features of CNS in fetus and newborn
Central and peripheral neurons form
Features of CNS in fetus and newborn
The features of the brain
Features of CNS in fetus and newborn
The features of the brain
Neurological examination
Neurological examination
Neurologic evaluation of the child. Complaints&History.
Seizures (convulsion) are involuntary, violent
Neurologic evaluation of the child. Complaints&History.
Seizures (convulsion) are involuntary, violent
Opisthotonus in a brain-injured infant. This is the tonic seizure.
Opisthotonus in a brain-injured infant. This is the tonic seizure.
Objective neurological examination
of the child should include 4 main diagnostic aspects:
1.
Objective neurological examination
of the child should include 4 main diagnostic aspects:
1.
A well child is conscious, alert and responsive
Level of consciousness
A well child is conscious, alert and responsive
Level of consciousness
Level of consciousness (LOC)
Lethargy or pathological sleepy (somnolence) is possible to
Level of consciousness (LOC)
Lethargy or pathological sleepy (somnolence) is possible to
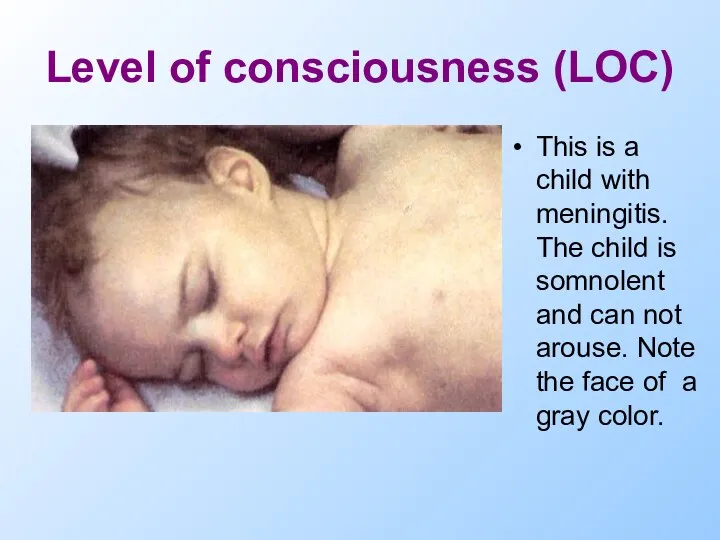
Level of consciousness (LOC)
This is a child with meningitis. The child
Level of consciousness (LOC)
This is a child with meningitis. The child
Stages of coma
Stupor: The stuporous patient arouses from sleep only after
Stages of coma
Stupor: The stuporous patient arouses from sleep only after

Mental development
Mental development
Head size
Head size
Enlarged head?
Enlarged head?

AF&PF
AF&PF
A fontanel bulging is a reliable indicator of increased ICP, but
A fontanel bulging is a reliable indicator of increased ICP, but
Cranial nerves
Cranial nerves
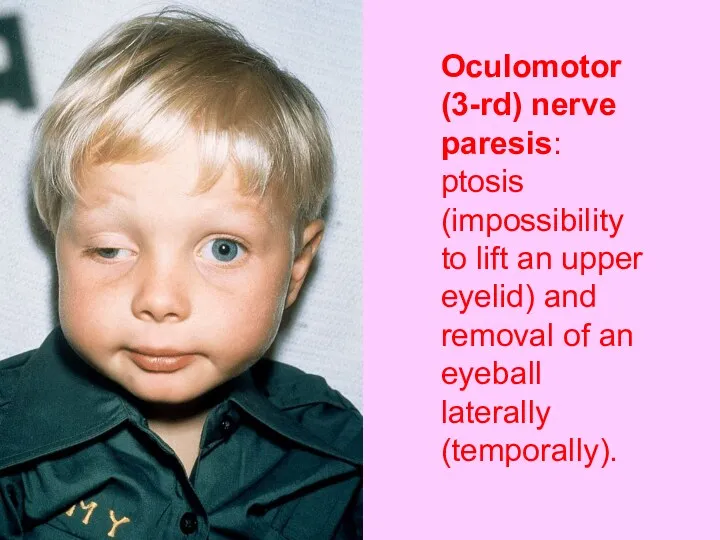
Oculomotor (3-rd) nerve paresis: ptosis (impossibility to lift an upper eyelid)
Oculomotor (3-rd) nerve paresis: ptosis (impossibility to lift an upper eyelid)
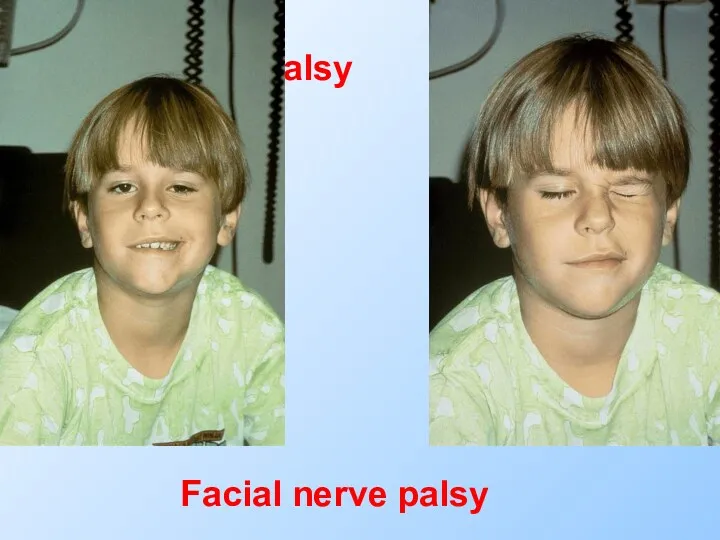
Facial nerve palsy
Facial nerve palsy
Facial nerve palsy
Facial nerve palsy
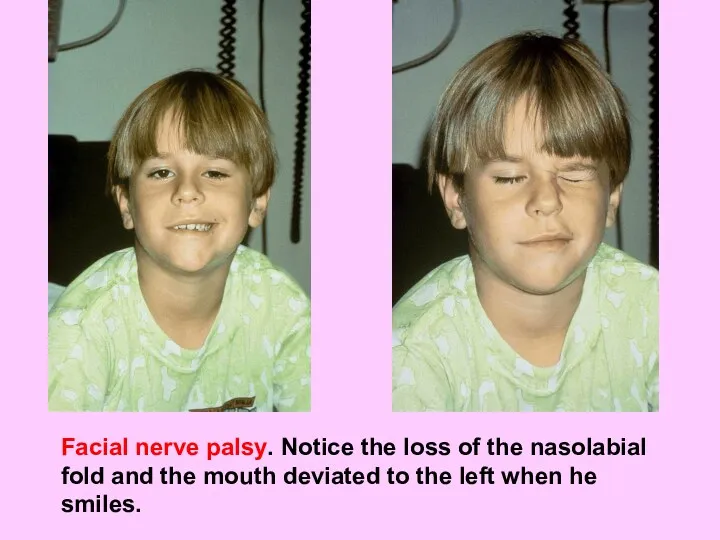
Facial nerve palsy. Notice the loss of the nasolabial fold and
Facial nerve palsy. Notice the loss of the nasolabial fold and
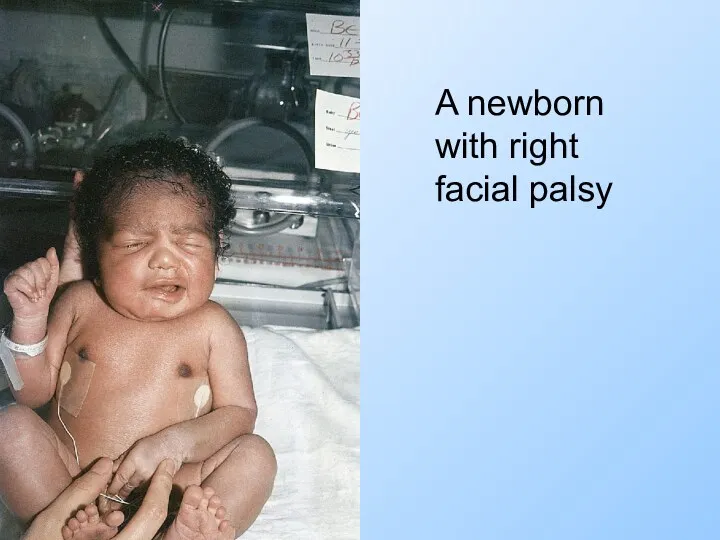
A newborn with right facial palsy
A newborn with right facial palsy
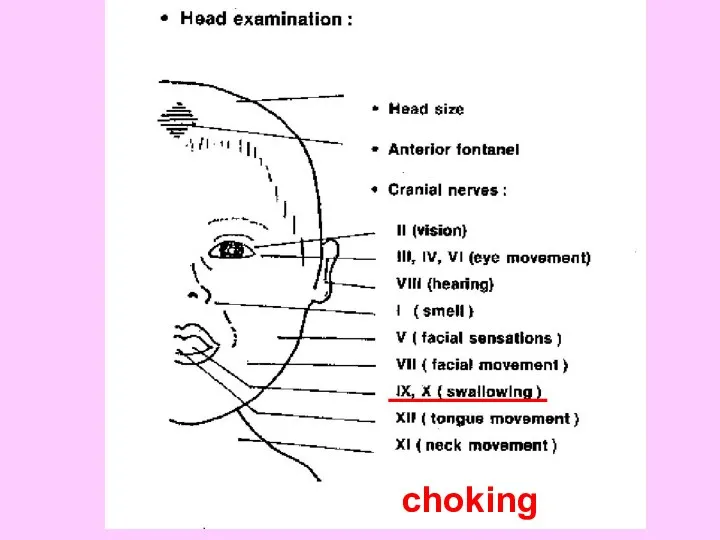
choking
choking
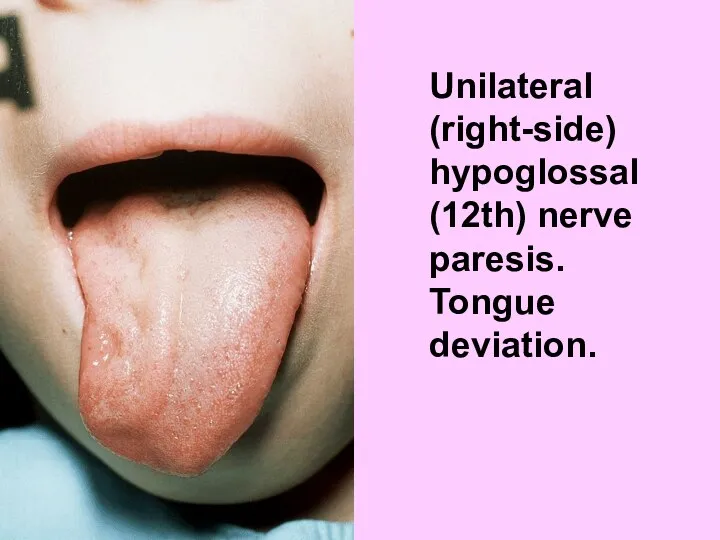
Unilateral (right-side) hypoglossal (12th) nerve paresis. Tongue deviation.
Unilateral (right-side) hypoglossal (12th) nerve paresis. Tongue deviation.
Motor examination
Motor examination
Abnormal gaits
The spastic gait
Circumduction gait
Cerebellar ataxia
waddling gait
Abnormal gaits
The spastic gait
Circumduction gait
Cerebellar ataxia
waddling gait
Movement disorders
Paralysis (palsy) – the absence of any voluntary movements
Movement disorders
Paralysis (palsy) – the absence of any voluntary movements
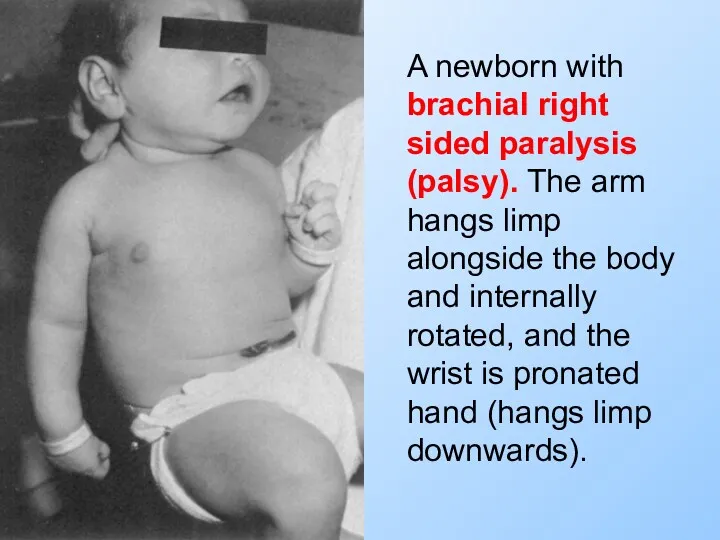
A newborn with brachial right sided paralysis (palsy). The arm hangs
A newborn with brachial right sided paralysis (palsy). The arm hangs
Movement disorders
Dystonia - slow twisting movements of limbs or trunk (alternation
Movement disorders
Dystonia - slow twisting movements of limbs or trunk (alternation
Muscles
Examination includes assessment of
muscles’ development: wasting, pseudohypertrophy
Tone: hypotonia, hypertonia
Muscles
Examination includes assessment of
muscles’ development: wasting, pseudohypertrophy
Tone: hypotonia, hypertonia
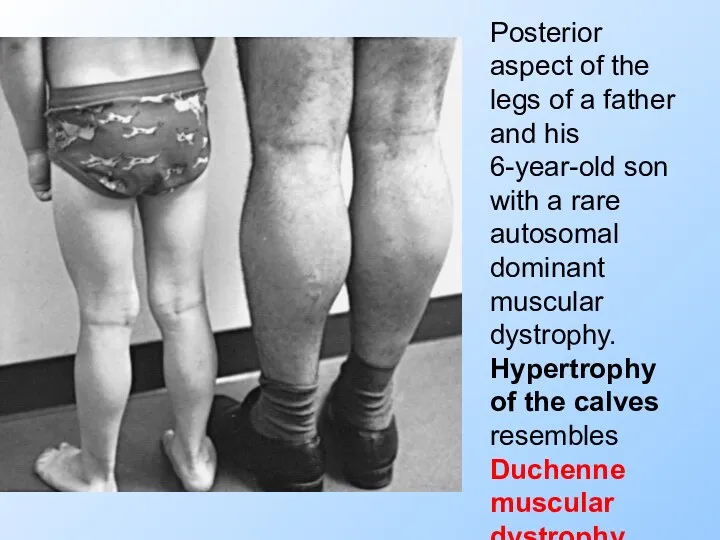
Posterior aspect of the legs of a father and his 6-year-old
Posterior aspect of the legs of a father and his 6-year-old
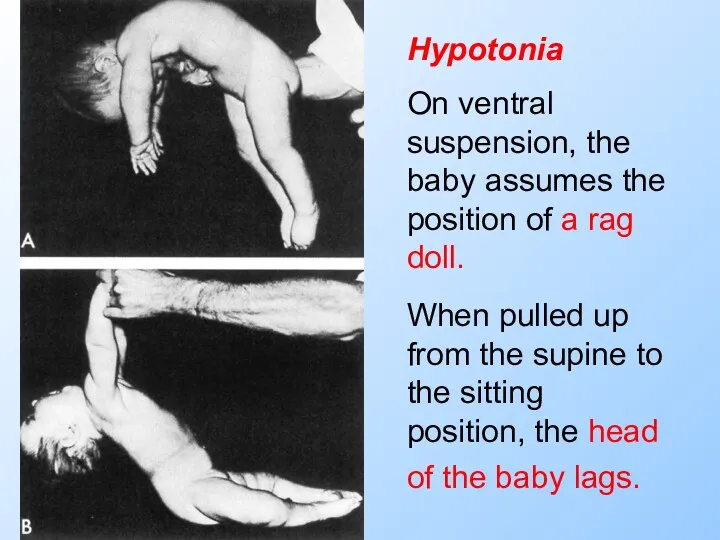
Hypotonia
On ventral suspension, the baby assumes the position of a rag
Hypotonia
On ventral suspension, the baby assumes the position of a rag

Main semiotics of CNS disorders. Meningitis.
Main semiotics of CNS disorders. Meningitis.
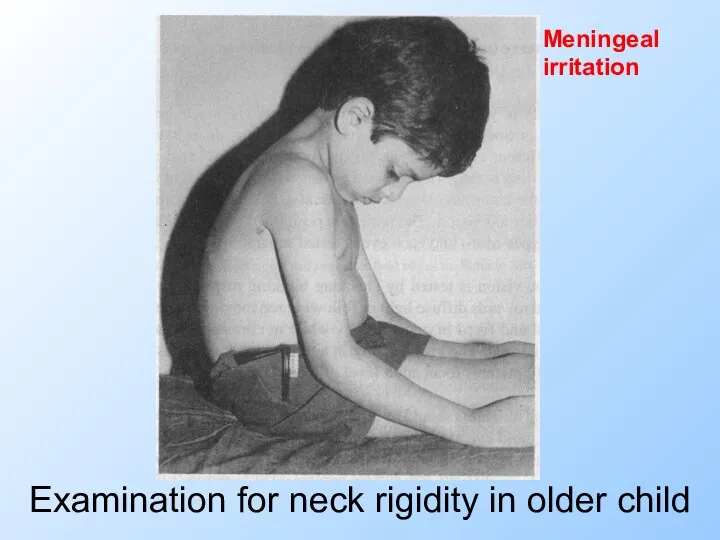
Examination for neck rigidity in older child
Meningeal irritation
Examination for neck rigidity in older child
Meningeal irritation

Brudzinski’s sign
Meningeal irritation
Brudzinski’s sign
Meningeal irritation
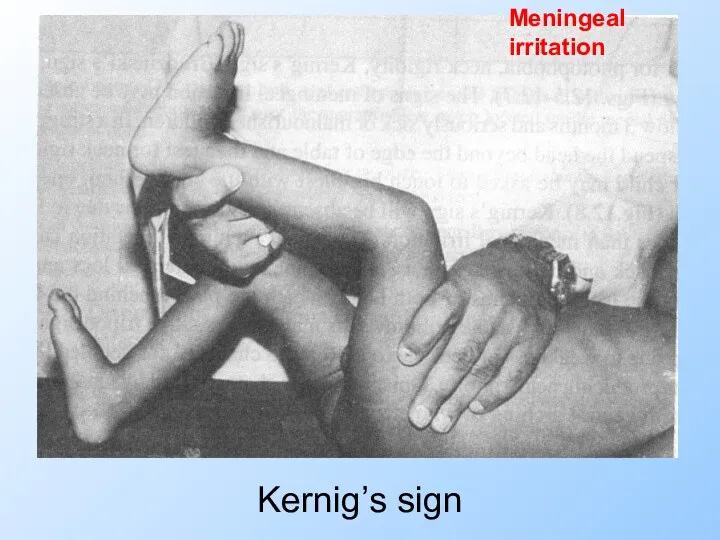
Kernig’s sign
Meningeal irritation
Kernig’s sign
Meningeal irritation
LP
The lumbar punction confirms the meningitis
LP
The lumbar punction confirms the meningitis
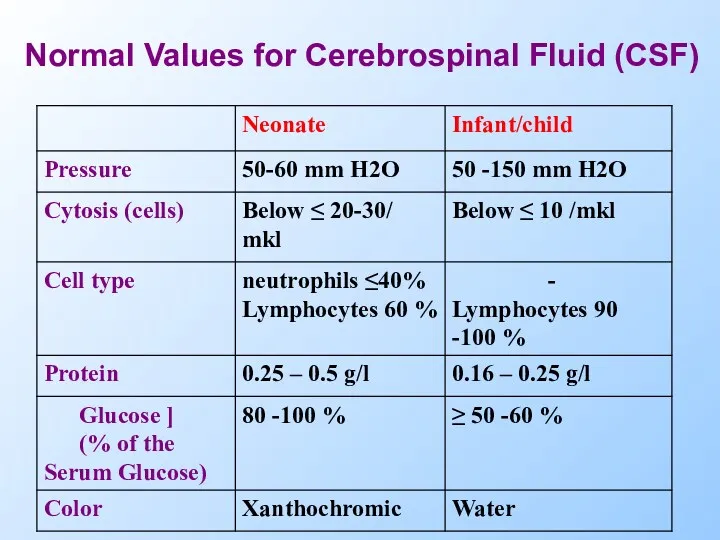
Normal Values for Cerebrospinal Fluid (CSF)
Normal Values for Cerebrospinal Fluid (CSF)
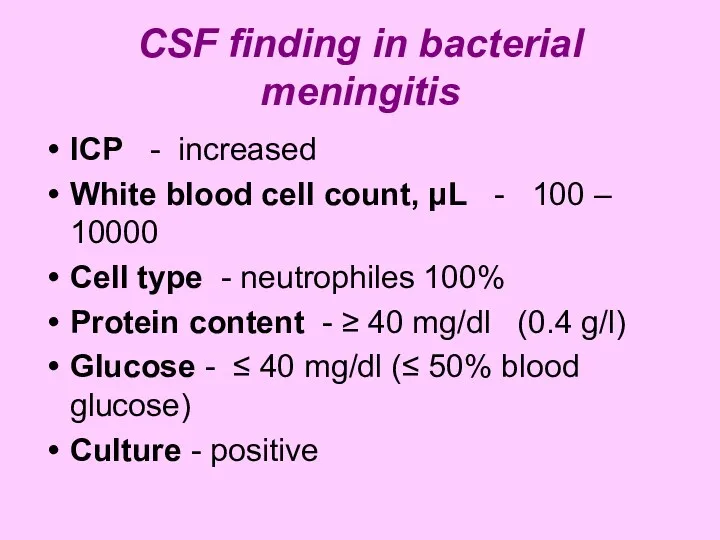
CSF finding in bacterial meningitis
ICP - increased
White blood cell count, μL
CSF finding in bacterial meningitis
ICP - increased
White blood cell count, μL
 Механизмы развития дыхательной недостаточности
Механизмы развития дыхательной недостаточности Қазақстандағы бүгінгі фармация
Қазақстандағы бүгінгі фармация Современный взгляд на кесарево сечение
Современный взгляд на кесарево сечение Ретинобластома. Определение понятия
Ретинобластома. Определение понятия Туберкулезный менингит
Туберкулезный менингит Українська медична термінологія
Українська медична термінологія Өкпенің ошақты туберкулезі
Өкпенің ошақты туберкулезі Физиология гемостаза
Физиология гемостаза Острый респираторный дистресс-синдром
Острый респираторный дистресс-синдром Производные фторхинолонов (ломефлоксацин, офлоксацин) и хиназолина (празозин). Требования к качеству, методы анализа
Производные фторхинолонов (ломефлоксацин, офлоксацин) и хиназолина (празозин). Требования к качеству, методы анализа Методы и режимы препарирования. Алгоритм выбора. Актуальные проблемы обезболивания а ортопедической стоматологии
Методы и режимы препарирования. Алгоритм выбора. Актуальные проблемы обезболивания а ортопедической стоматологии Красная волчанка
Красная волчанка Синдром желтухи у новорожденных и детей первого года жизни
Синдром желтухи у новорожденных и детей первого года жизни Наркология
Наркология Вирусные гепатиты на современном этапе
Вирусные гепатиты на современном этапе Сенильді психоздың дамуына әкелетін факторлар. Кәрі жастағы психикалық бұзылыстары бар науқастардың реабилитациясы
Сенильді психоздың дамуына әкелетін факторлар. Кәрі жастағы психикалық бұзылыстары бар науқастардың реабилитациясы Адам денесіндегі ұлпалар
Адам денесіндегі ұлпалар Астматикалық статус
Астматикалық статус Патогенна дія хімічних та біологічних факторів на організм. Роль спадковості в патології. (Лекція 4)
Патогенна дія хімічних та біологічних факторів на організм. Роль спадковості в патології. (Лекція 4) Болезнь Лайма
Болезнь Лайма Сахарный диабет, как социально-значимое заболевание
Сахарный диабет, как социально-значимое заболевание Risk for a health and ecological risk
Risk for a health and ecological risk Заготовка ЛРС. Общие правила сбора ЛРС
Заготовка ЛРС. Общие правила сбора ЛРС Великоустюгская центральная районная больница
Великоустюгская центральная районная больница Дәрігердің кәсіптік деформациясы
Дәрігердің кәсіптік деформациясы Роль медицинской сестры в подготовке пациента к плановой операции
Роль медицинской сестры в подготовке пациента к плановой операции Клиническая фармакология гипотензивных средств
Клиническая фармакология гипотензивных средств Геморрагиялық диатездер
Геморрагиялық диатездер