- Development of the heart

Содержание
- 2. THE OBJECTIVES:
- 3. GENERAL PROVISIONS:
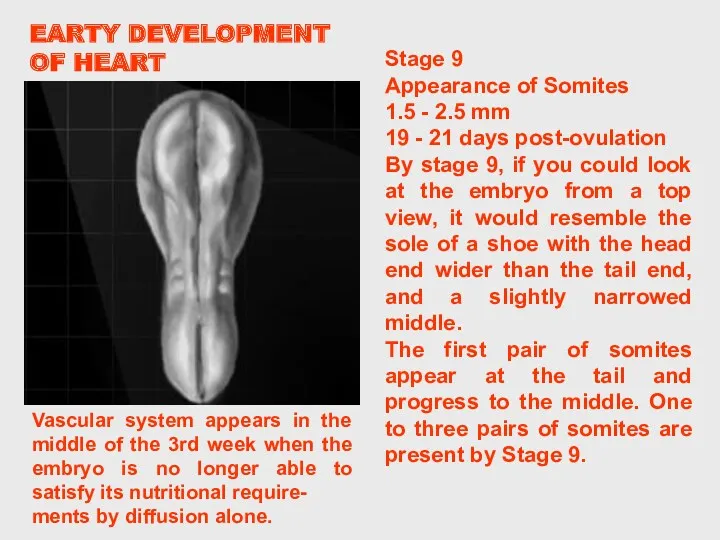
- 4. EARLY DEVELOPMENT OF THE EMBRYO Middle of the 3rd week – presomite stage, pan-cake appearance of
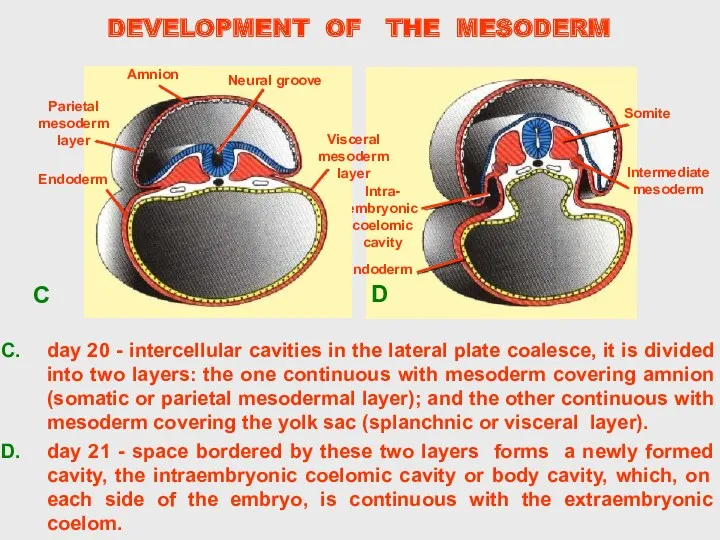
- 5. DEVELOPMENT OF THE MESODERM
- 6. DEVELOPMENT OF THE MESODERM
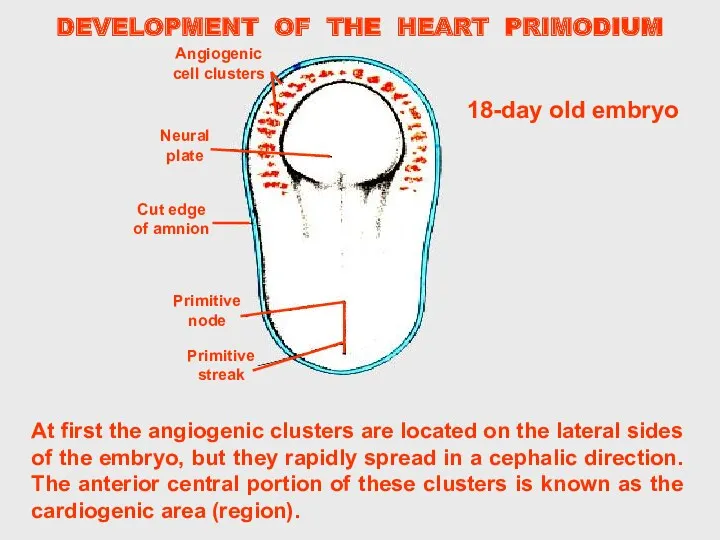
- 7. DEVELOPMENT OF THE HEART PRIMODIUM At first the angiogenic clusters are located on the lateral sides
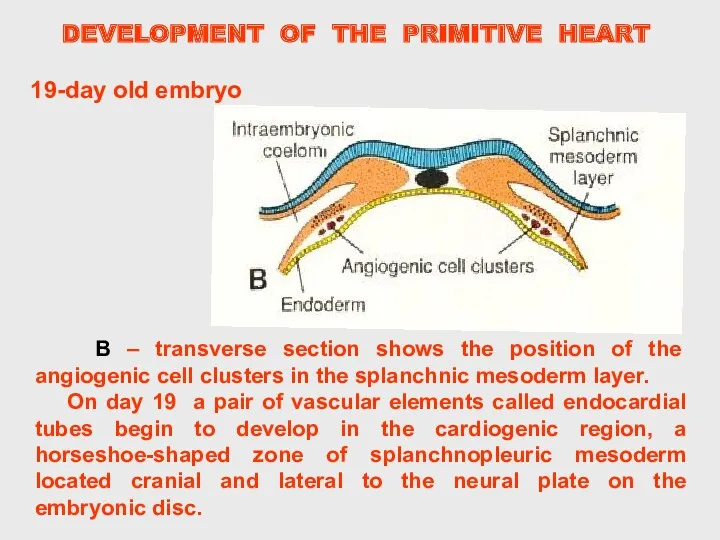
- 8. DEVELOPMENT OF THE PRIMITIVE HEART B – transverse section shows the position of the angiogenic cell
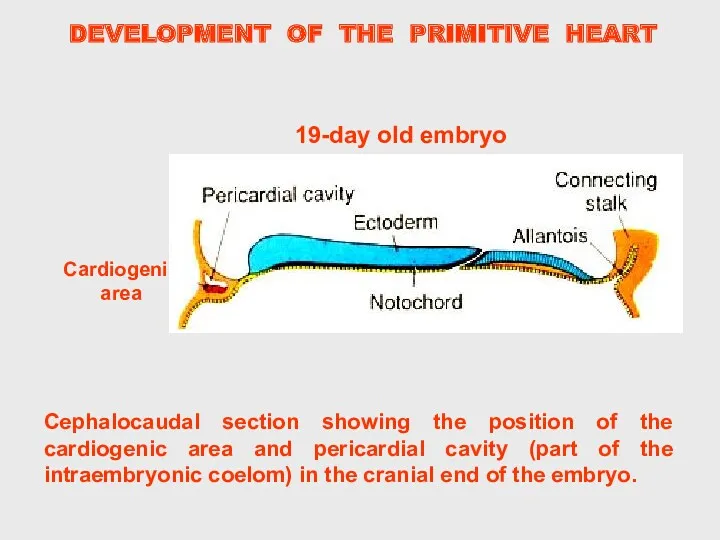
- 9. DEVELOPMENT OF THE PRIMITIVE HEART Cephalocaudal section showing the position of the cardiogenic area and pericardial
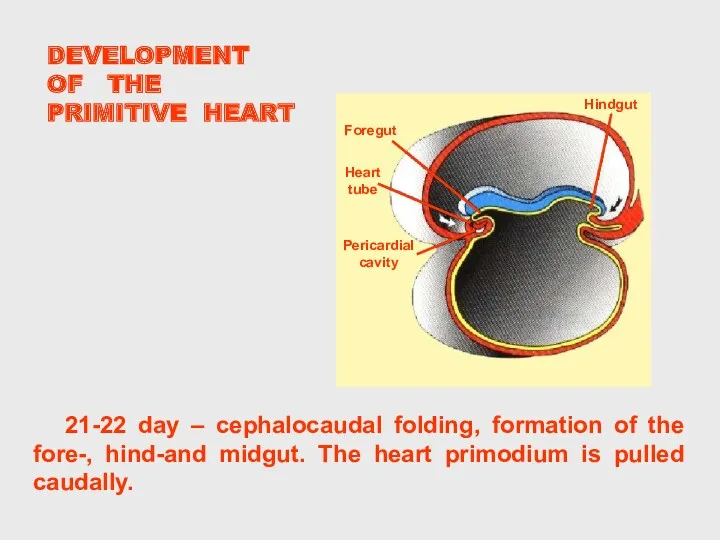
- 10. DEVELOPMENT OF THE PRIMITIVE HEART 21-22 day – cephalocaudal folding, formation of the fore-, hind-and midgut.
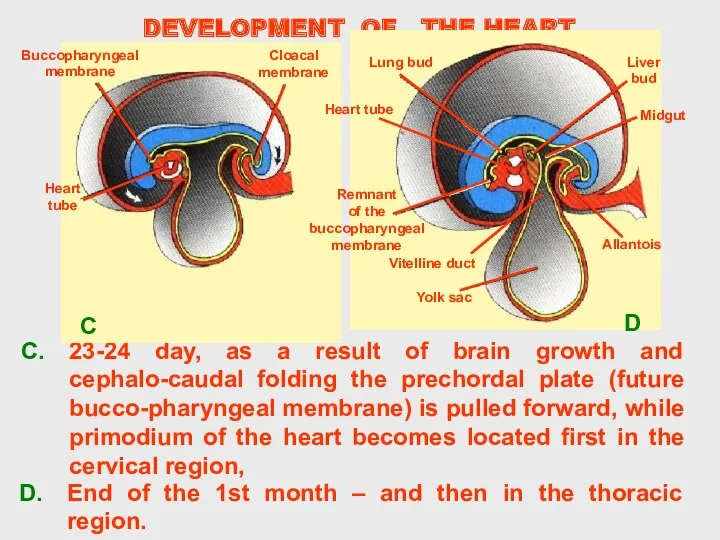
- 11. DEVELOPMENT OF THE HEART 23-24 day, as a result of brain growth and cephalo-caudal folding the
- 12. Cells of splanchnic mesodermal layer form the visceral layer of the serous membranes covering the abdominal
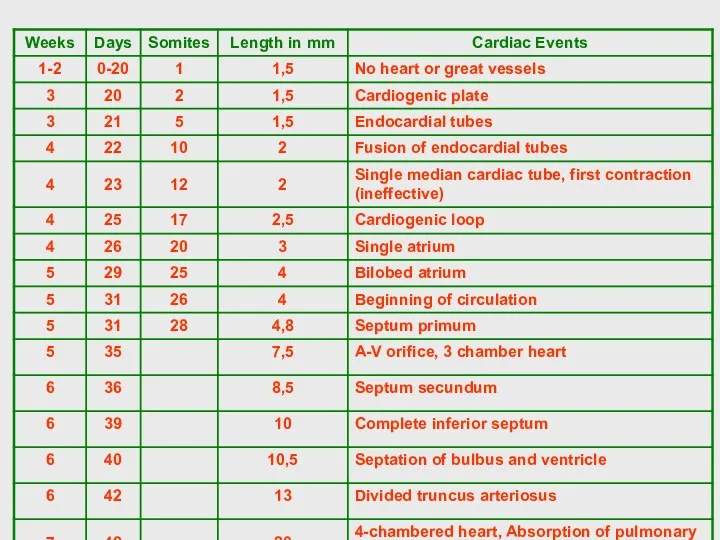
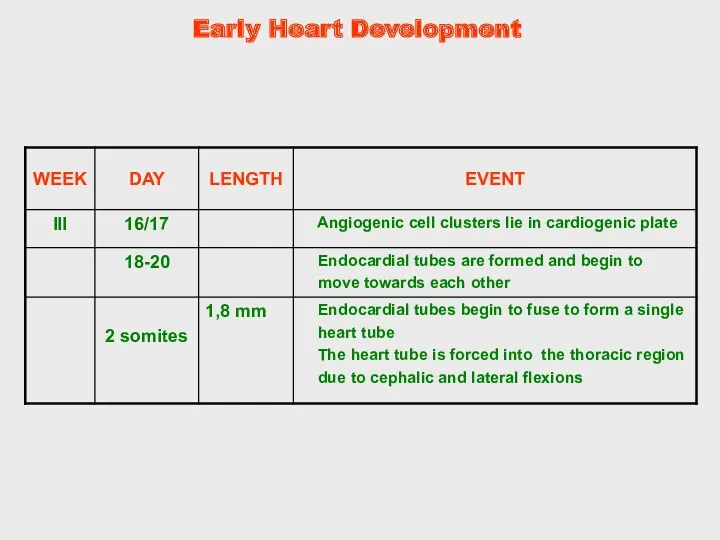
- 13. Stage 9 Appearance of Somites 1.5 - 2.5 mm 19 - 21 days post-ovulation By stage
- 15. The origins of the heart tube are clusters of angiogenic cells which are located in the
- 16. When the neural tube grows it pulls with it the prochordal plate (Oropharyngeal membrane) and the
- 17. Angiogenic cell clusters which lie in a horse-shoe shape configuration in the plate coalesce to form
- 18. These angiogenic cell clusters coalesce to form right and left endocardial tubes. Each tube is continuous
- 19. The lateral and cranial folding of the embryo forces the tubes into the thoracic cavity. As
- 20. As the single heart tube is being formed the mesoderm around it thickens to form the
- 21. At approximately day 21 the endocardial tubes are completely fused. The heart starts to beat at
- 23. The single tubular heart develops many constrictions outlining future structures. The cranial most area is the
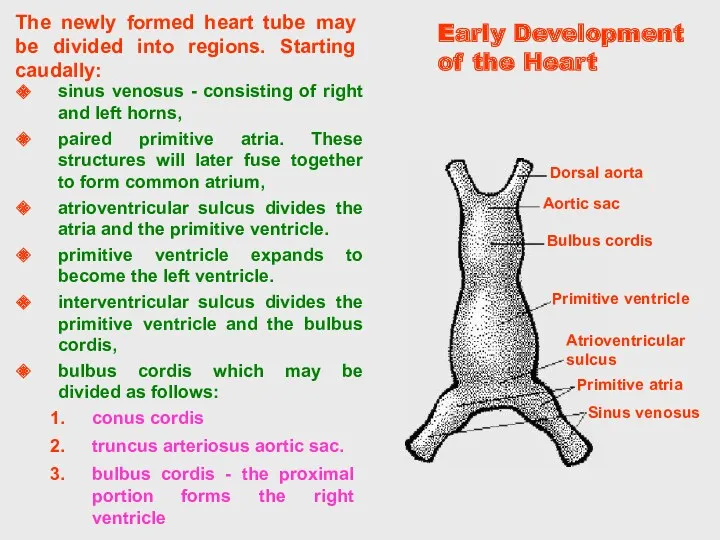
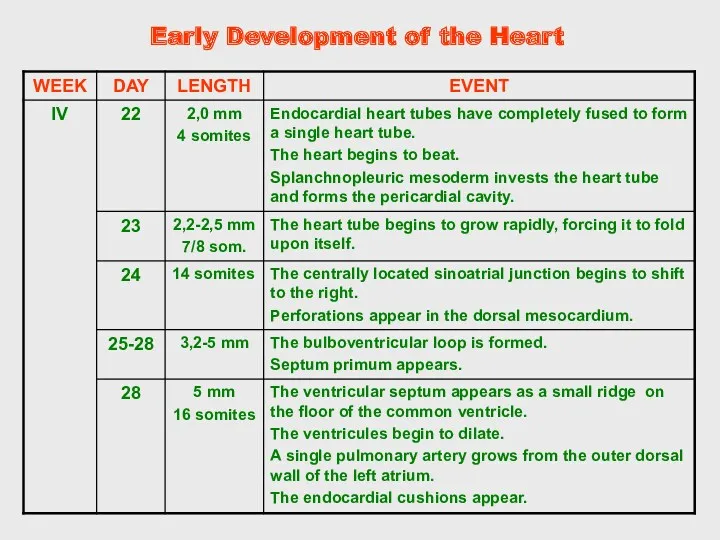
- 24. Early Development of the Heart The newly formed heart tube may be divided into regions. Starting
- 25. Early Heart Development
- 26. The original paired cardiac tubes fuse, with the "ventricular" primordia initially lying above the "atria". Growth
- 27. The bulboventricular portion of the heart grow faster than the pericardial sac and the rest of
- 28. The bulboventricular sulcus will become visible from the outside, and from the inside there will be
- 29. By the time the heart tube has formed the bulboventricular loop, the two primitive right and
- 30. The newly formed heart tube bulges into the pericardial cavity and is attached to the dorsal
- 31. The primitive heart tube can be subdivided into primordial heart chambers starting caudally at the inflow
- 32. Early Development of the Heart
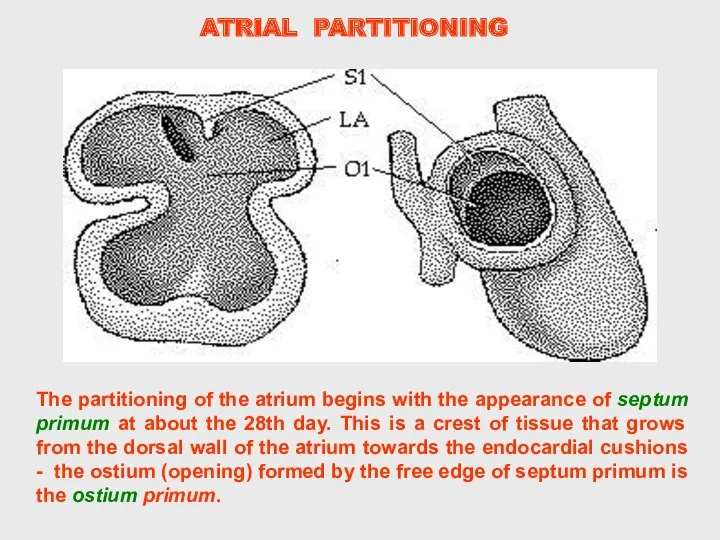
- 33. The partitioning of the atrium begins with the appearance of septum primum at about the 28th
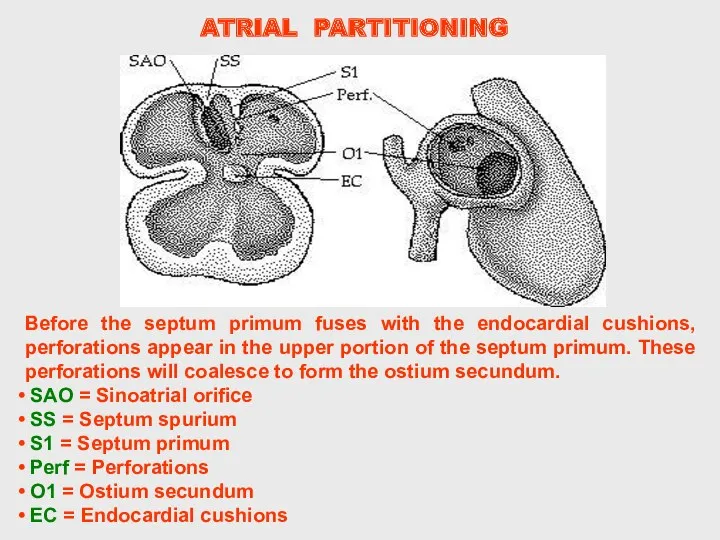
- 34. Before the septum primum fuses with the endocardial cushions, perforations appear in the upper portion of
- 35. Unlike the septum primum, septum secundum does not fuse with the endocardial cushions. Its free edge
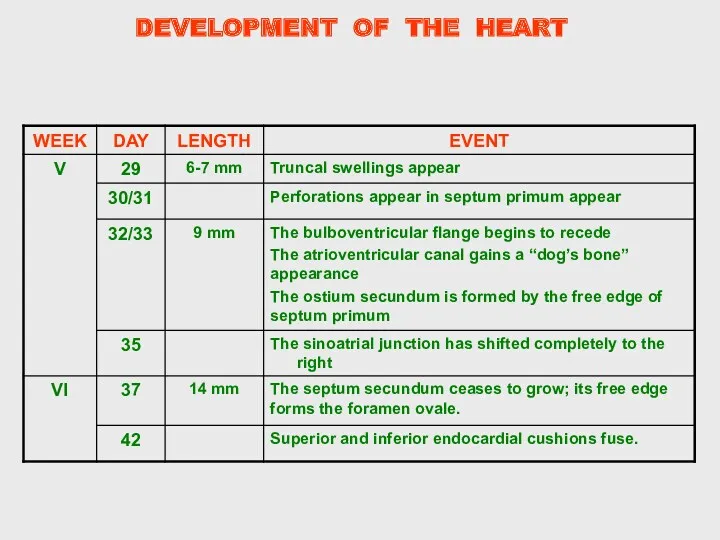
- 36. At the end of the 7th week the human heart has reached its final stage of
- 37. DEVELOPMENT OF THE HEART
- 38. Early Development of the Heart
- 39. Fate of the Sinus Venosus (Formation of the Right Atrium) Communication between the sinus venosus and
- 40. Conversely, the left vein counterparts are obliterated and the left sinus horn diminishes in size and
- 41. Internally, the sinoatrial orifice is flanked by two valves, the right and left venous valves. Superiorly
- 42. Further into development the right sinus horn is incorporated into the expanding right atium. As the
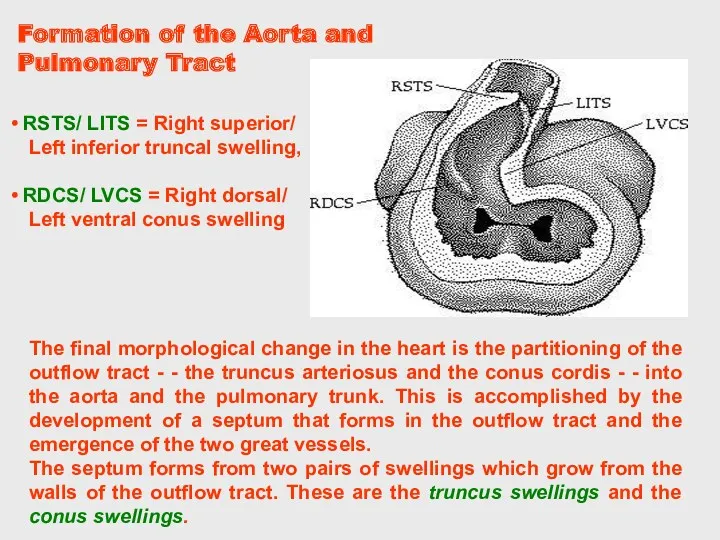
- 43. The final morphological change in the heart is the partitioning of the outflow tract - -
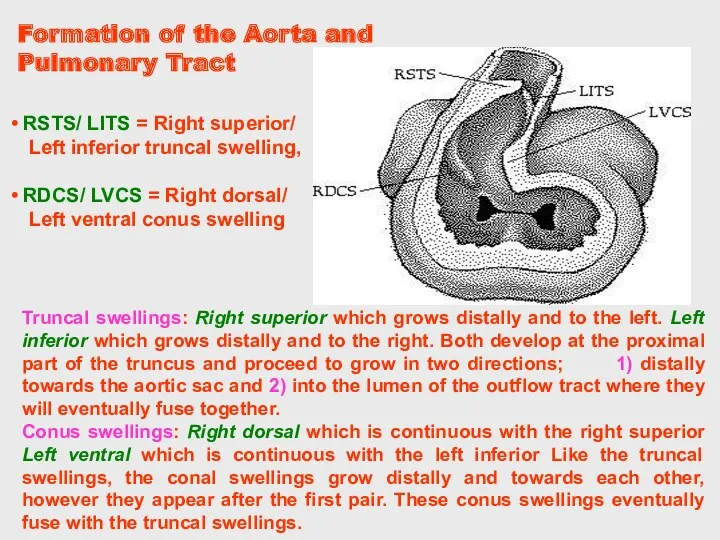
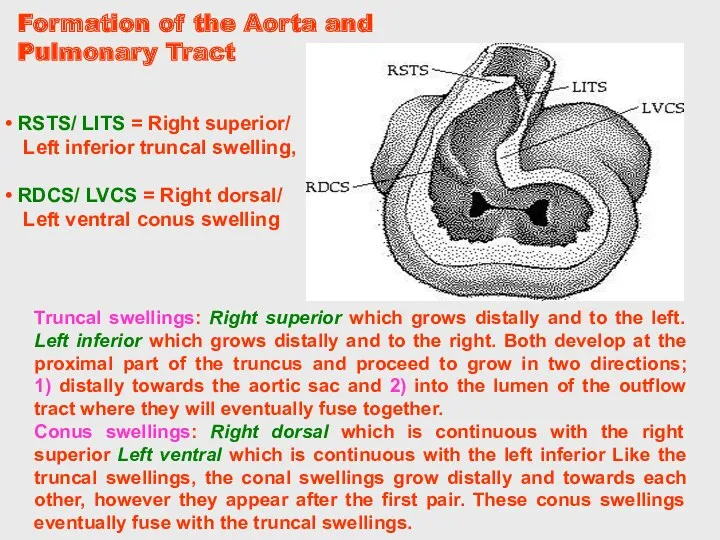
- 44. Truncal swellings: Right superior which grows distally and to the left. Left inferior which grows distally
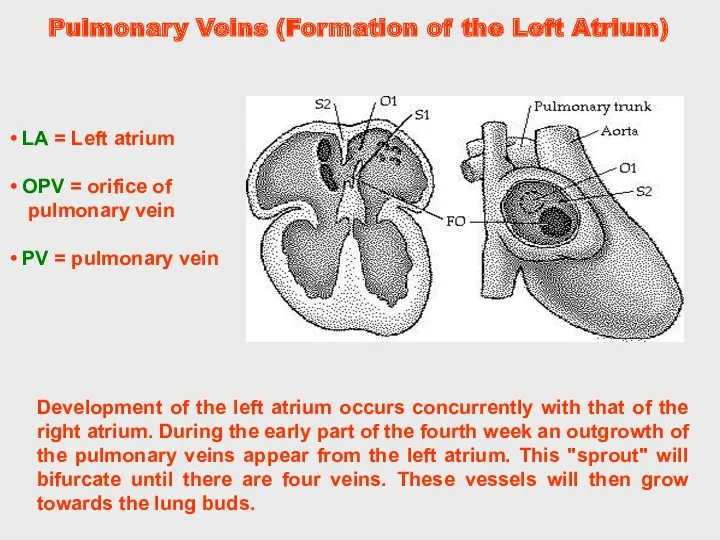
- 45. Pulmonary Veins (Formation of the Left Atrium) Development of the left atrium occurs concurrently with that
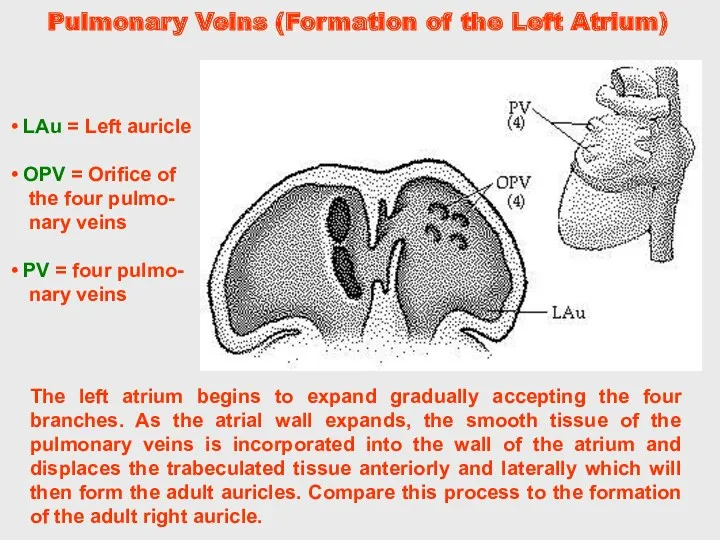
- 46. The left atrium begins to expand gradually accepting the four branches. As the atrial wall expands,
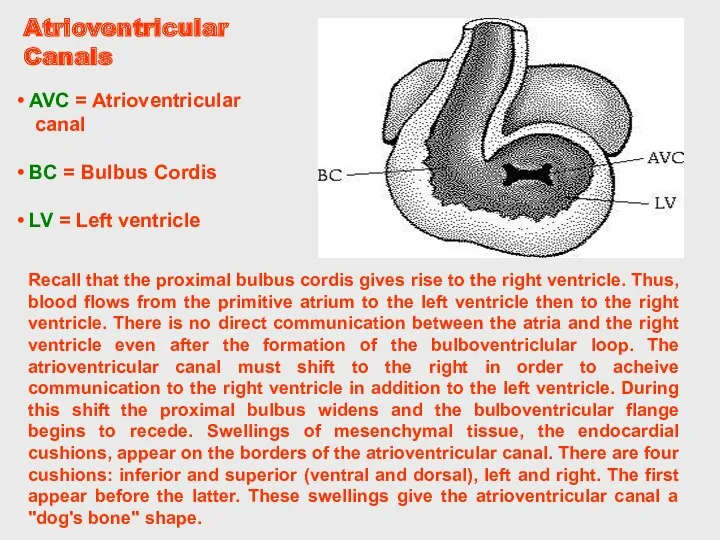
- 47. Recall that the proximal bulbus cordis gives rise to the right ventricle. Thus, blood flows from
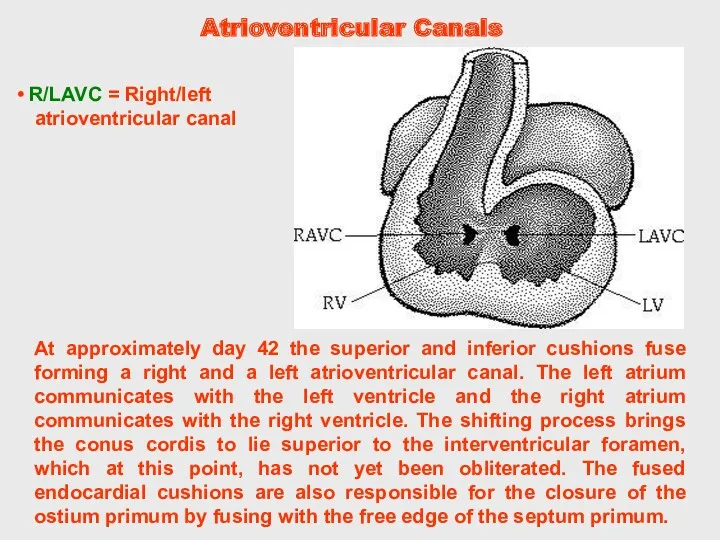
- 48. At approximately day 42 the superior and inferior cushions fuse forming a right and a left
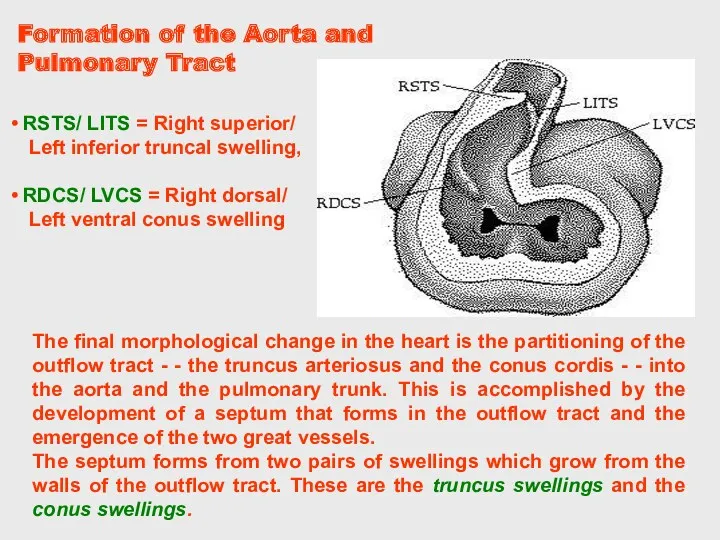
- 49. The final morphological change in the heart is the partitioning of the outflow tract - -
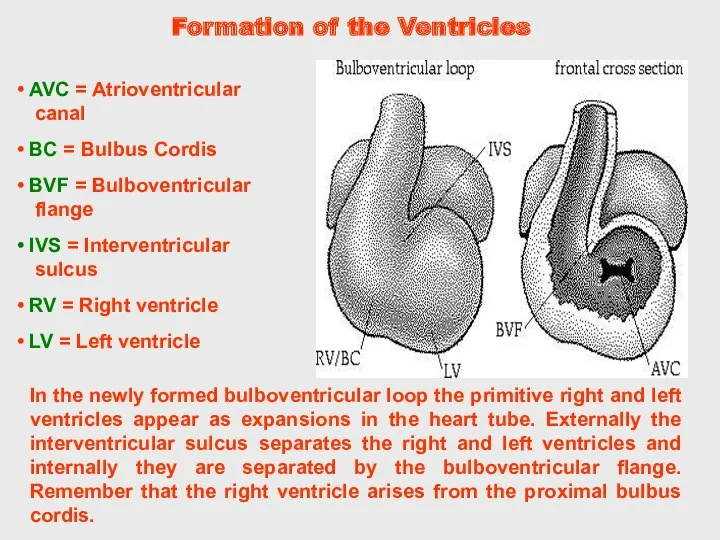
- 50. In the newly formed bulboventricular loop the primitive right and left ventricles appear as expansions in
- 51. During the shifting of the atrioventriclar canal the proximal bulbus cordis expands forming the right ventricle.
- 52. Secundum type involves septum primum or septum secundum. Atrial Septal Defect In a heart with an
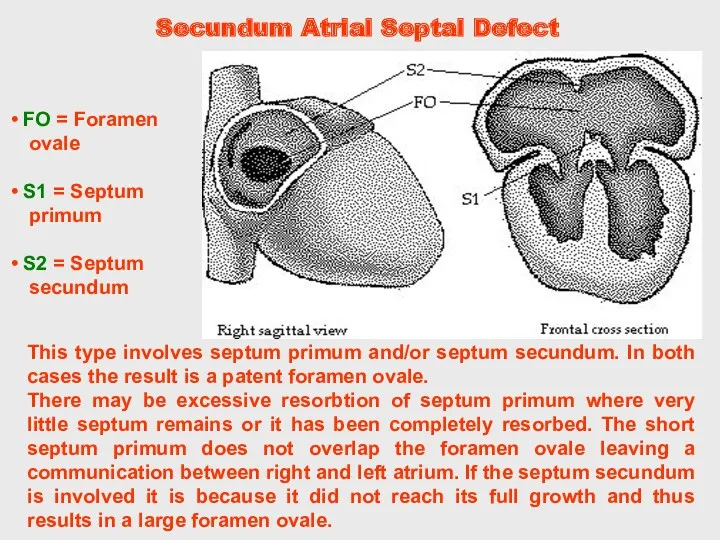
- 53. In this case, the ostium primum is patent because the septum primum does not fuse with
- 54. Truncal swellings: Right superior which grows distally and to the left. Left inferior which grows distally
- 55. Secundum Atrial Septal Defect This type involves septum primum and/or septum secundum. In both cases the
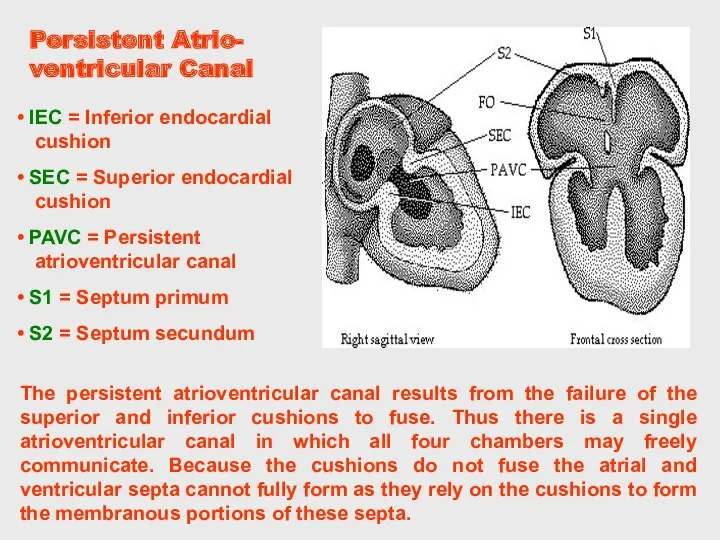
- 56. Persistent Atrio- ventricular Canal The persistent atrioventricular canal results from the failure of the superior and
- 57. In the case of a VSD there is a massive left to right shunting of blood
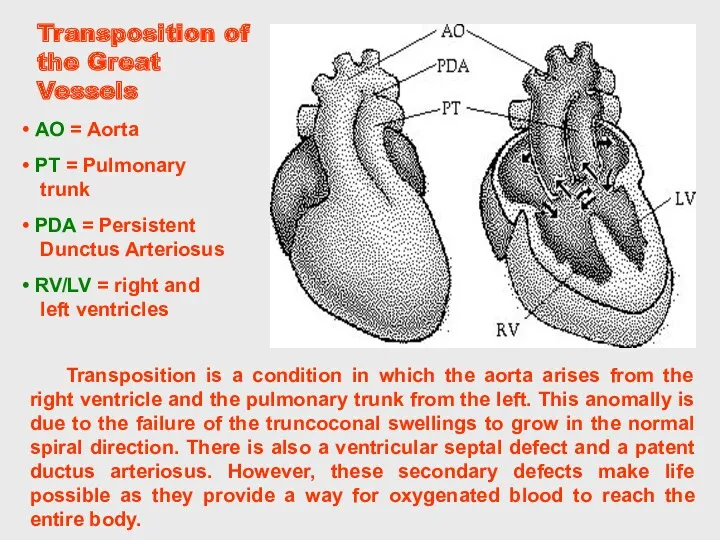
- 58. Transposition of the Great Vessels Transposition is a condition in which the aorta arises from the
- 59. Persistent Truncus Arteriosus A persistent truncus arteriosus results when the truncoconal swellings fail to grow. The
- 60. Tetralogy of Fallot right ventricular hypertrophy due to the shunting of blood from left to right.
- 61. Dextrocardia Dextrocardia is an anomaly in which the primitive heart tube folds to the left in
- 62. The embryo is shaped in a modified S curve. The embryo has a bulb-like tail and
- 63. MAIN STAGES OF THE ERALY HEART DEVELOPMENT
- 64. Heart chambers are filled with plasma and blood cells making the heart seem distended and prominent.
- 65. The embryo curves into a C shape. The arches that form the face and neck are
- 66. Septum primum fuses with septum intermedium in the heart. Stage 19, (approximately 47-48 post ovulatory days)
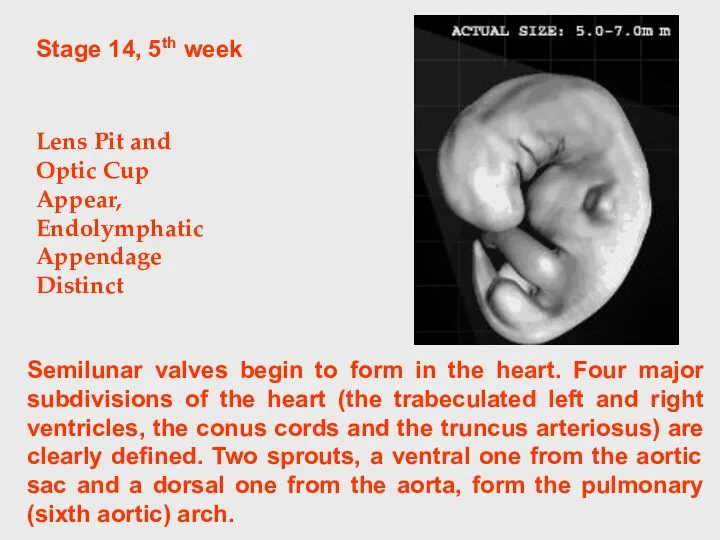
- 67. Stage 14, 5th week Lens Pit and Optic Cup Appear, Endolymphatic Appendage Distinct Semilunar valves begin
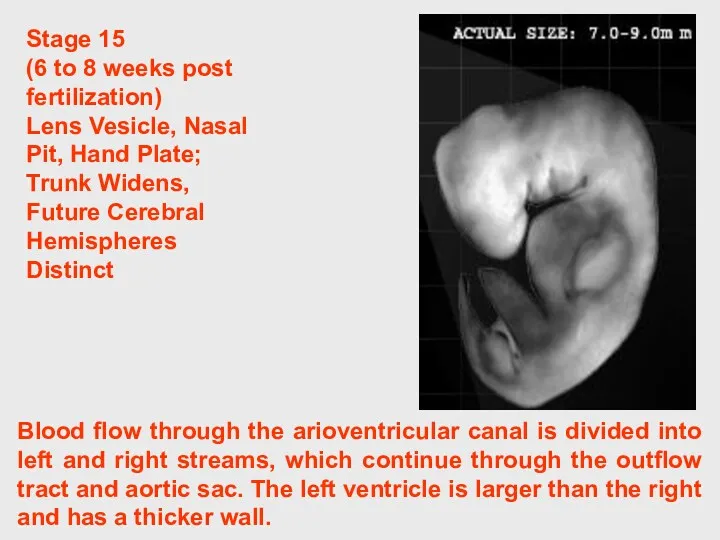
- 68. Blood flow through the arioventricular canal is divided into left and right streams, which continue through
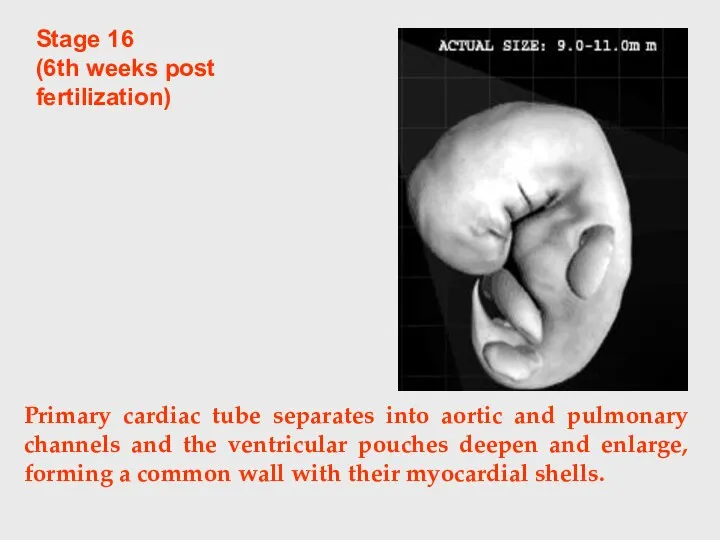
- 69. Stage 16 (6th weeks post fertilization) Primary cardiac tube separates into aortic and pulmonary channels and
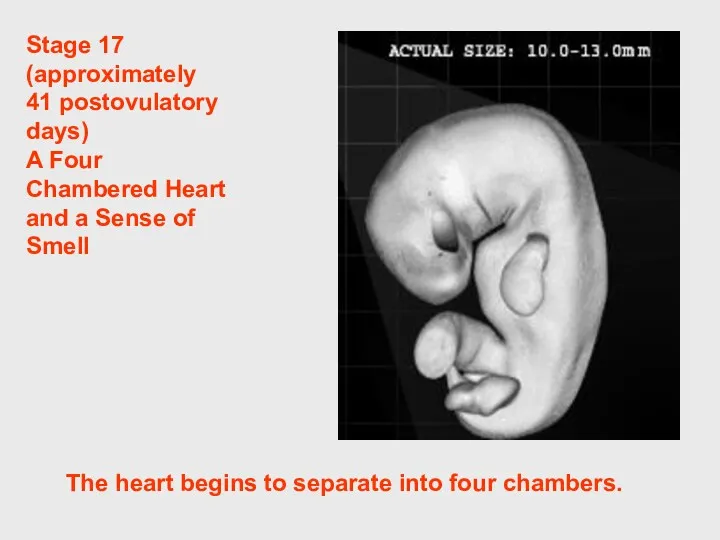
- 70. Stage 17 (approximately 41 postovulatory days) A Four Chambered Heart and a Sense of Smell The
- 71. Within the heart, the trunk of the pulmonary artery separates from the trunk of the aorta.
- 72. CONGENITAL MALFORMATIONS OF THE HEART AND GREAT VESSELS. They are common. The overall incidence is 0.7%
- 74. Скачать презентацию
THE OBJECTIVES:
THE OBJECTIVES:
GENERAL PROVISIONS:
GENERAL PROVISIONS:
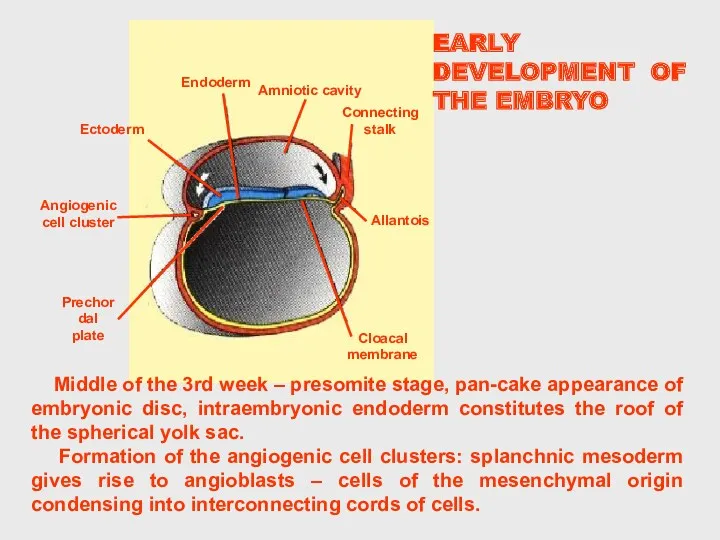
EARLY DEVELOPMENT OF THE EMBRYO
Middle of the 3rd week –
EARLY DEVELOPMENT OF THE EMBRYO
Middle of the 3rd week –
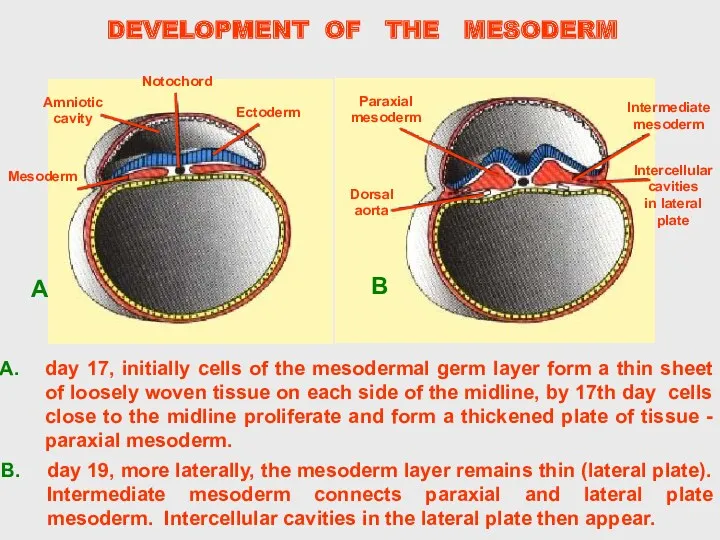
DEVELOPMENT OF THE MESODERM
DEVELOPMENT OF THE MESODERM
DEVELOPMENT OF THE MESODERM
DEVELOPMENT OF THE MESODERM
DEVELOPMENT OF THE HEART PRIMODIUM
At first the angiogenic clusters are located
DEVELOPMENT OF THE HEART PRIMODIUM
At first the angiogenic clusters are located
DEVELOPMENT OF THE PRIMITIVE HEART
B – transverse section shows the
DEVELOPMENT OF THE PRIMITIVE HEART
B – transverse section shows the
DEVELOPMENT OF THE PRIMITIVE HEART
Cephalocaudal section showing the position of the
DEVELOPMENT OF THE PRIMITIVE HEART
Cephalocaudal section showing the position of the
DEVELOPMENT
OF THE
PRIMITIVE HEART
21-22 day – cephalocaudal folding, formation
DEVELOPMENT
OF THE
PRIMITIVE HEART
21-22 day – cephalocaudal folding, formation
DEVELOPMENT OF THE HEART
23-24 day, as a result of brain growth
DEVELOPMENT OF THE HEART
23-24 day, as a result of brain growth
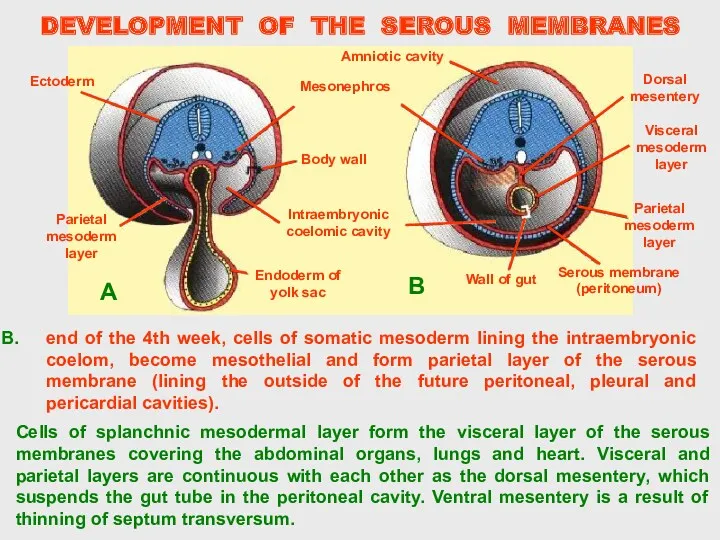
Cells of splanchnic mesodermal layer form the visceral layer of the
Cells of splanchnic mesodermal layer form the visceral layer of the
Stage 9
Appearance of Somites
1.5 - 2.5 mm
19 - 21
Stage 9
Appearance of Somites
1.5 - 2.5 mm
19 - 21
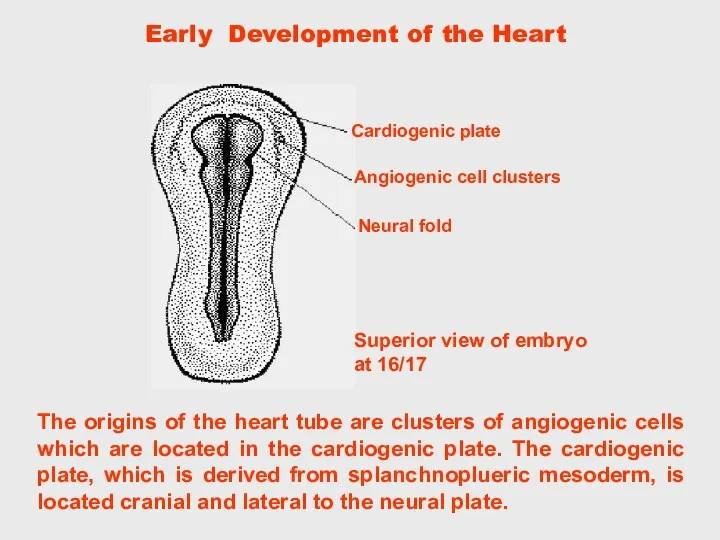
The origins of the heart tube are clusters of angiogenic cells
The origins of the heart tube are clusters of angiogenic cells
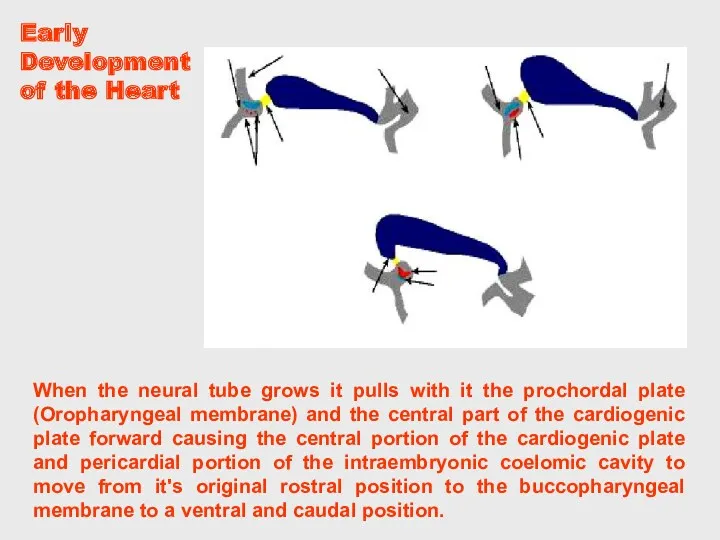
When the neural tube grows it pulls with it the prochordal
When the neural tube grows it pulls with it the prochordal
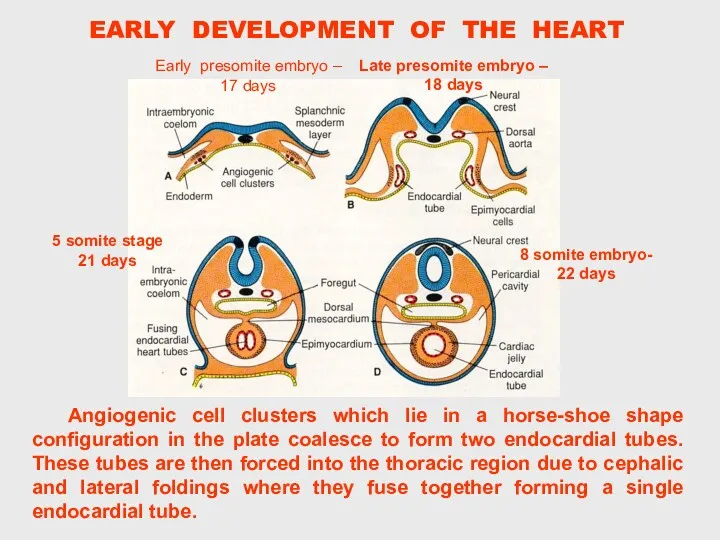
Angiogenic cell clusters which lie in a horse-shoe shape configuration in
Angiogenic cell clusters which lie in a horse-shoe shape configuration in
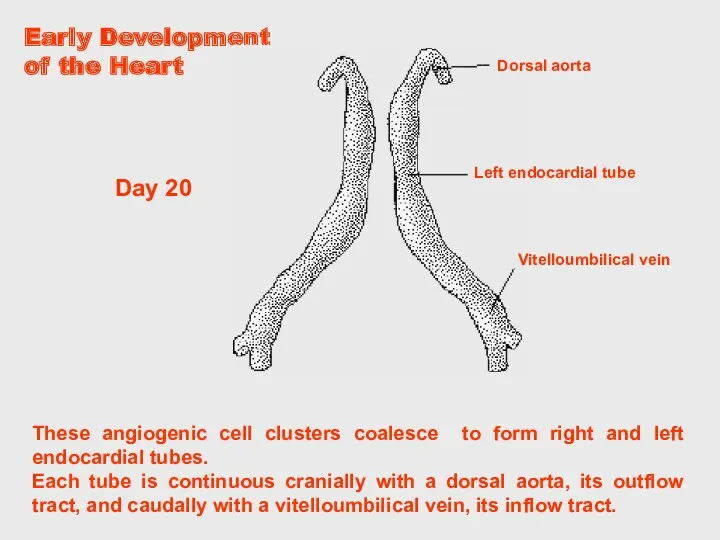
These angiogenic cell clusters coalesce to form right and left endocardial
These angiogenic cell clusters coalesce to form right and left endocardial
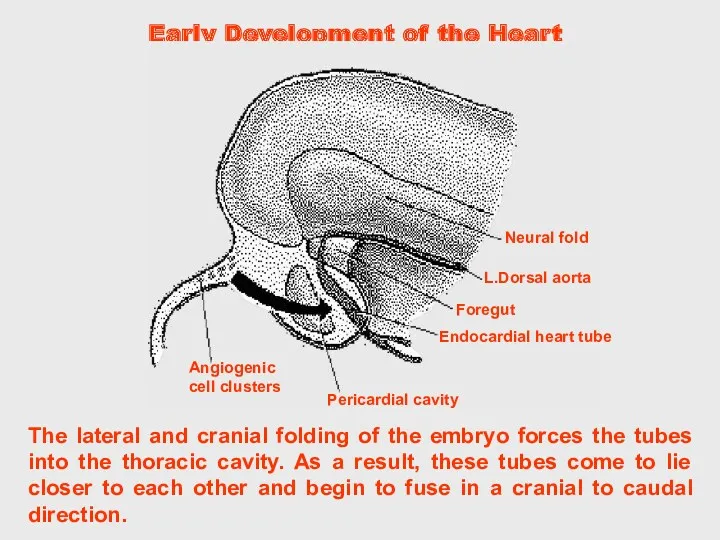
The lateral and cranial folding of the embryo forces the tubes
The lateral and cranial folding of the embryo forces the tubes
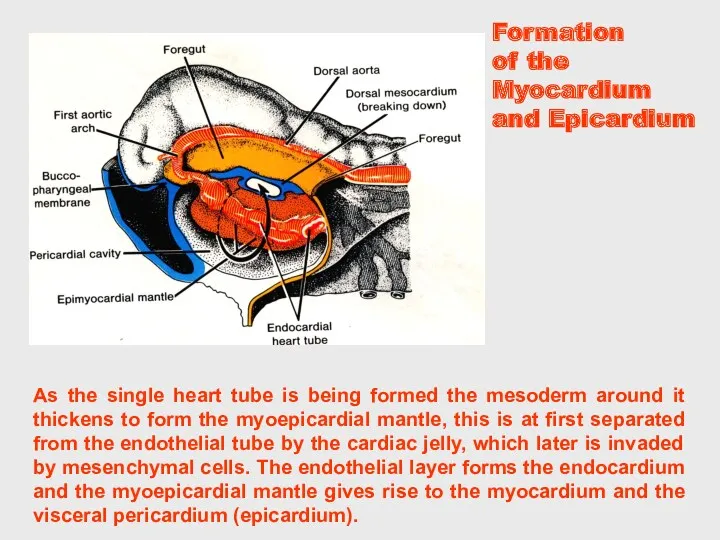
As the single heart tube is being formed the mesoderm around
As the single heart tube is being formed the mesoderm around
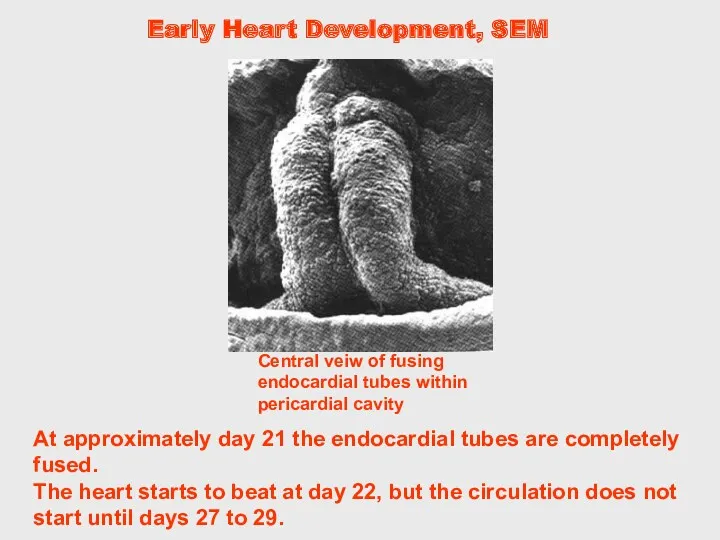
At approximately day 21 the endocardial tubes are completely fused.
The
At approximately day 21 the endocardial tubes are completely fused.
The

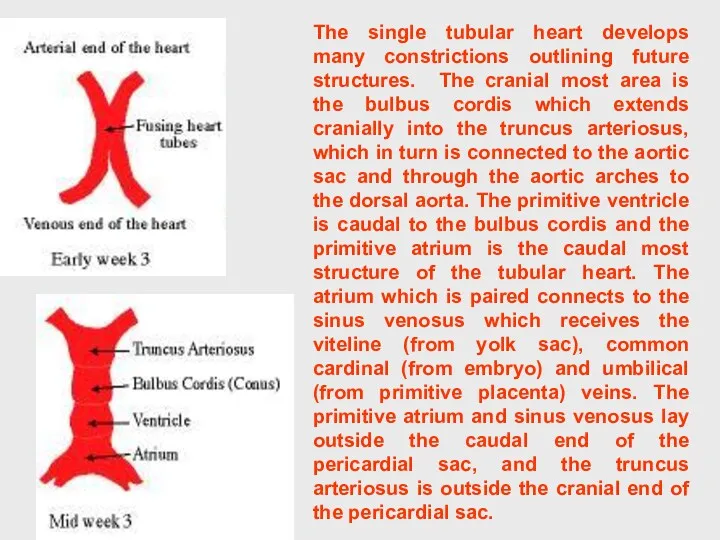
The single tubular heart develops many constrictions outlining future structures. The
The single tubular heart develops many constrictions outlining future structures. The
Early Development of the Heart
The newly formed heart tube may be
Early Development of the Heart
The newly formed heart tube may be
Early Heart Development
Early Heart Development
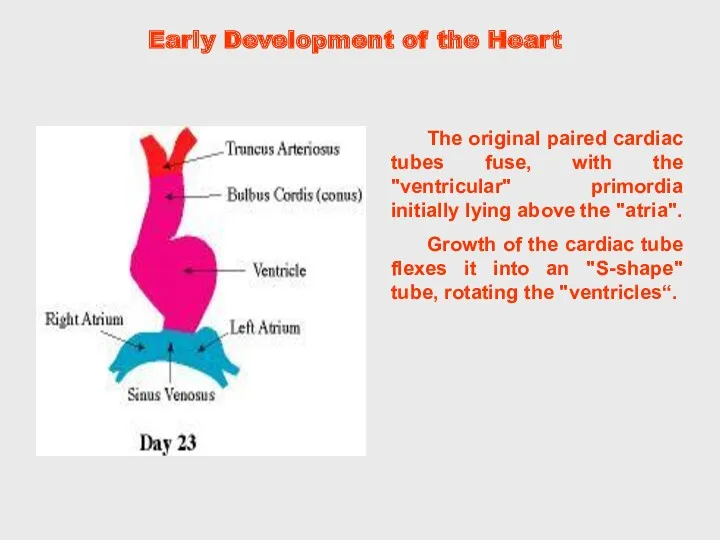
The original paired cardiac tubes fuse, with the "ventricular" primordia initially
The original paired cardiac tubes fuse, with the "ventricular" primordia initially
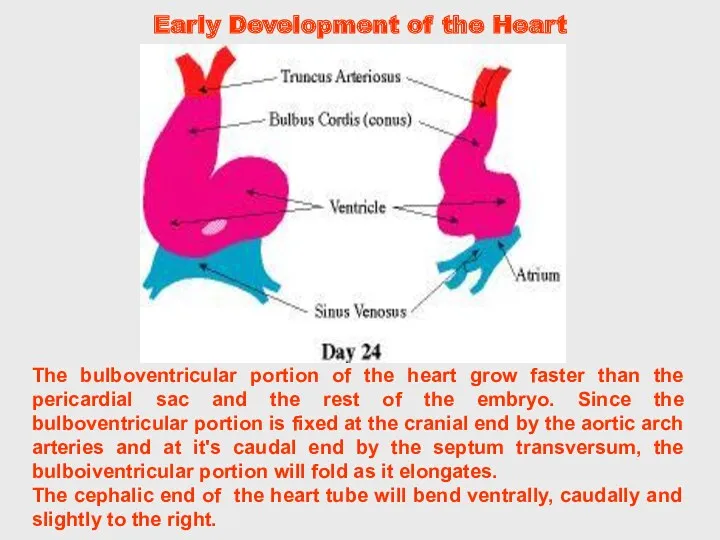
The bulboventricular portion of the heart grow faster than the pericardial
The bulboventricular portion of the heart grow faster than the pericardial
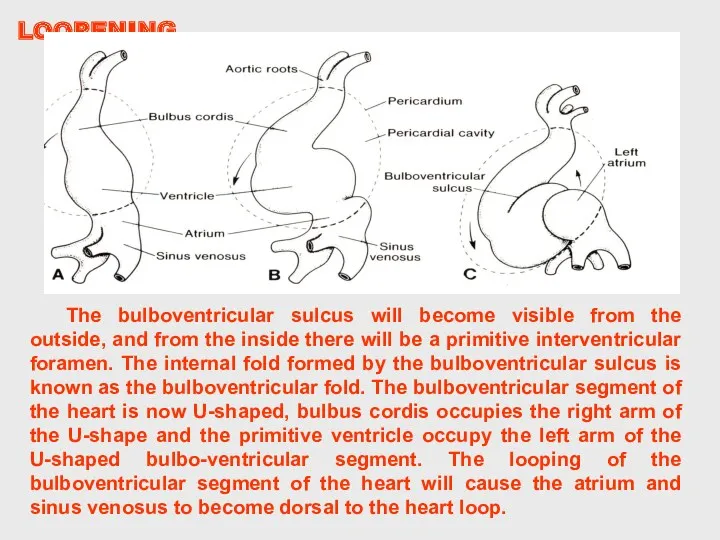
The bulboventricular sulcus will become visible from the outside, and from
The bulboventricular sulcus will become visible from the outside, and from
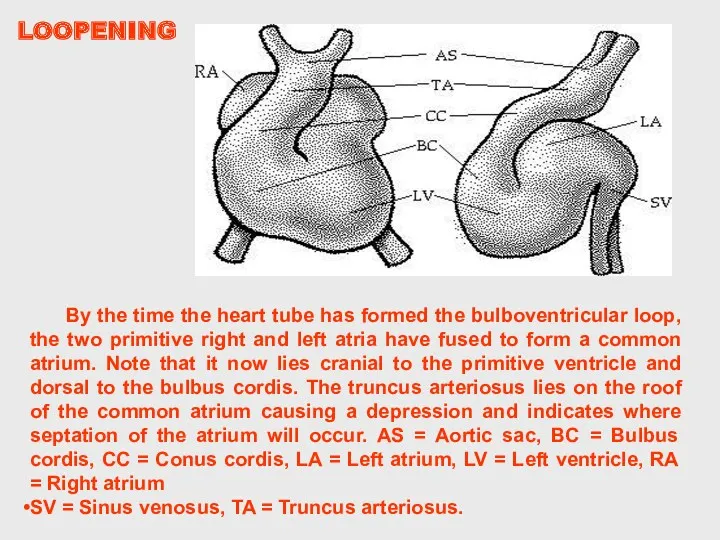
By the time the heart tube has formed the bulboventricular loop,
By the time the heart tube has formed the bulboventricular loop,
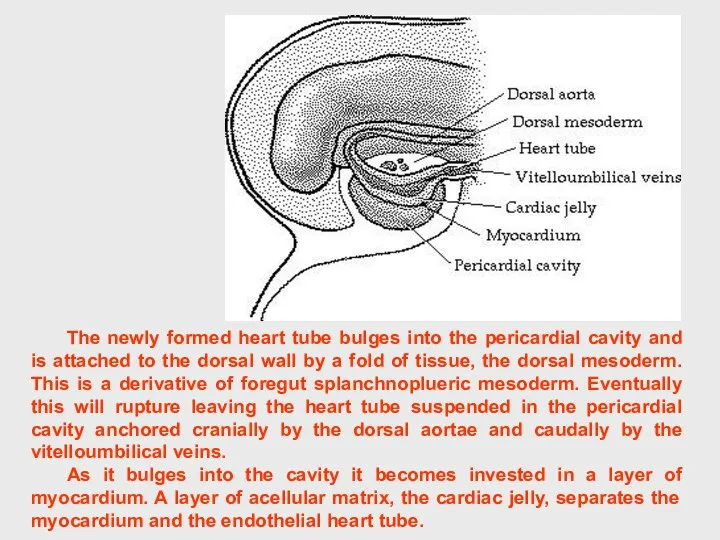
The newly formed heart tube bulges into the pericardial cavity and
The newly formed heart tube bulges into the pericardial cavity and
The primitive heart tube can be subdivided into primordial heart chambers
The primitive heart tube can be subdivided into primordial heart chambers
Early Development of the Heart
Early Development of the Heart
The partitioning of the atrium begins with the appearance of septum
The partitioning of the atrium begins with the appearance of septum
Before the septum primum fuses with the endocardial cushions, perforations appear
Before the septum primum fuses with the endocardial cushions, perforations appear
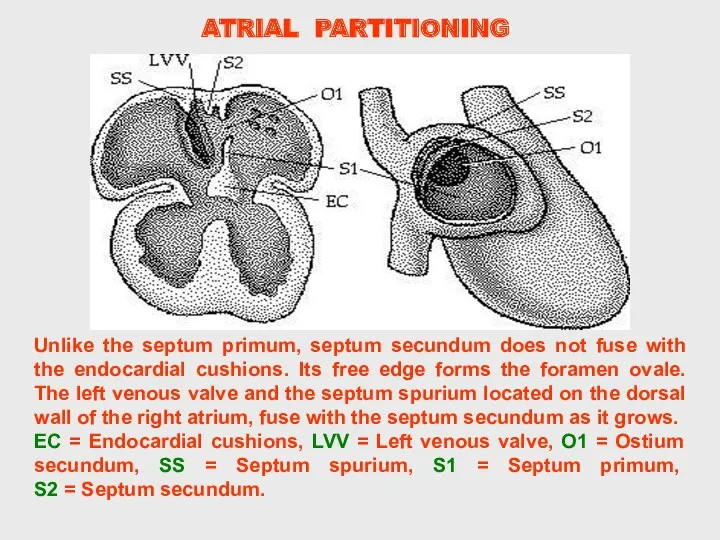
Unlike the septum primum, septum secundum does not fuse with the
Unlike the septum primum, septum secundum does not fuse with the
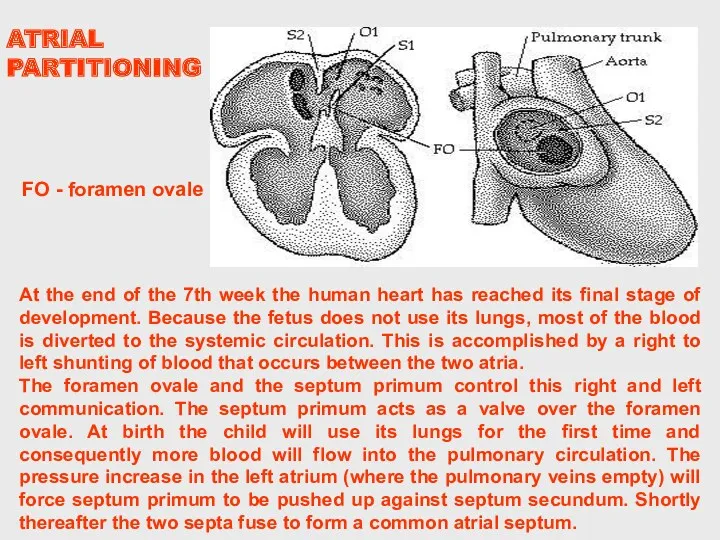
At the end of the 7th week the human heart has
At the end of the 7th week the human heart has
DEVELOPMENT OF THE HEART
DEVELOPMENT OF THE HEART
Early Development of the Heart
Early Development of the Heart
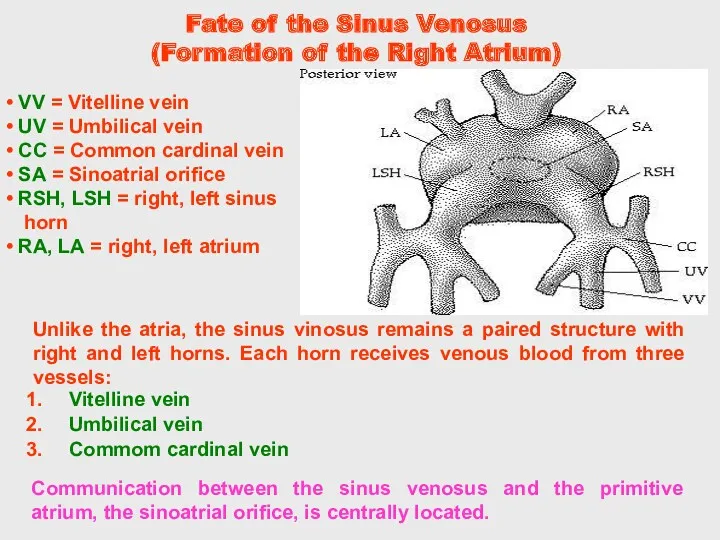
Fate of the Sinus Venosus (Formation of the Right Atrium)
Communication between
Fate of the Sinus Venosus (Formation of the Right Atrium)
Communication between
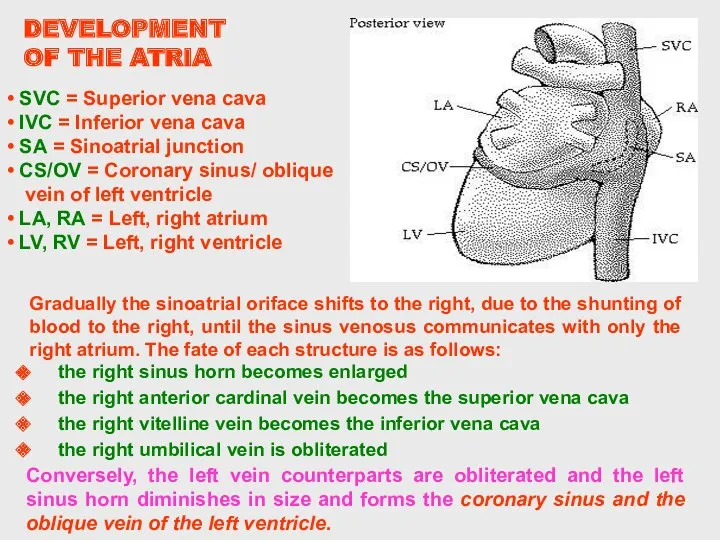
Conversely, the left vein counterparts are obliterated and the left sinus
Conversely, the left vein counterparts are obliterated and the left sinus
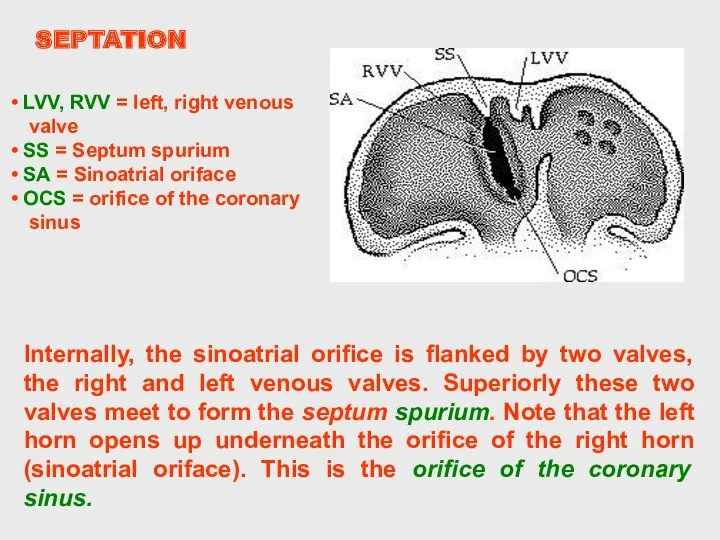
Internally, the sinoatrial orifice is flanked by two valves, the right
Internally, the sinoatrial orifice is flanked by two valves, the right
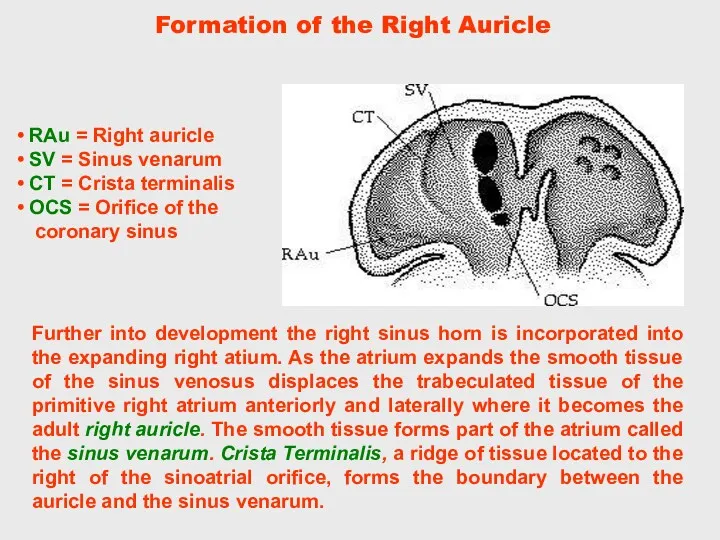
Further into development the right sinus horn is incorporated into the
Further into development the right sinus horn is incorporated into the
The final morphological change in the heart is the partitioning of
The final morphological change in the heart is the partitioning of
Truncal swellings: Right superior which grows distally and to the left.
Truncal swellings: Right superior which grows distally and to the left.
Pulmonary Veins (Formation of the Left Atrium)
Development of the left atrium
Pulmonary Veins (Formation of the Left Atrium)
Development of the left atrium
The left atrium begins to expand gradually accepting the four branches.
The left atrium begins to expand gradually accepting the four branches.
Recall that the proximal bulbus cordis gives rise to the right
Recall that the proximal bulbus cordis gives rise to the right
At approximately day 42 the superior and inferior cushions fuse forming
At approximately day 42 the superior and inferior cushions fuse forming
The final morphological change in the heart is the partitioning of
The final morphological change in the heart is the partitioning of
In the newly formed bulboventricular loop the primitive right and left
In the newly formed bulboventricular loop the primitive right and left
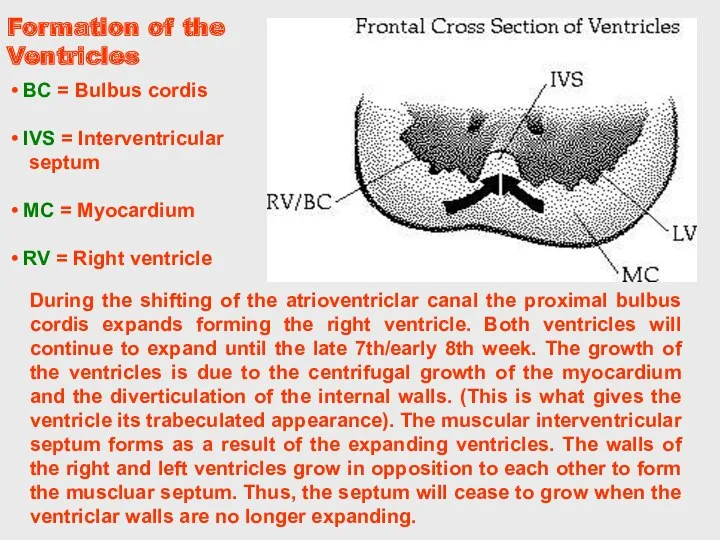
During the shifting of the atrioventriclar canal the proximal bulbus cordis
During the shifting of the atrioventriclar canal the proximal bulbus cordis
Secundum type involves septum primum or septum secundum.
Atrial Septal Defect
In a
Secundum type involves septum primum or septum secundum.
Atrial Septal Defect
In a
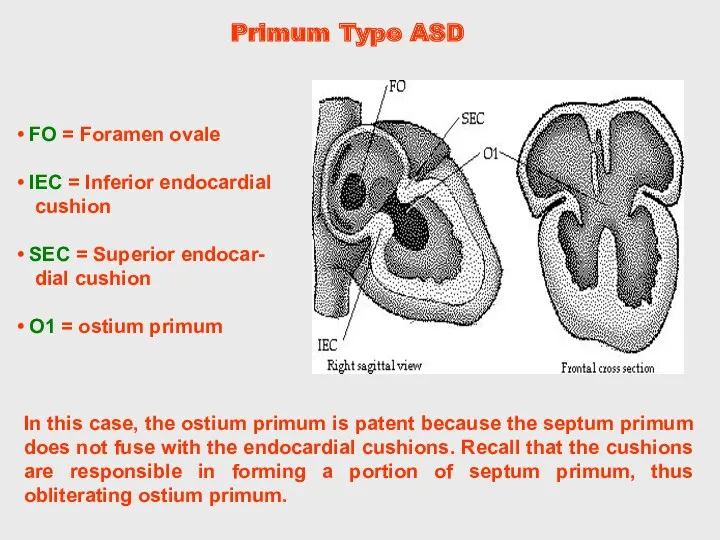
In this case, the ostium primum is patent because the septum
In this case, the ostium primum is patent because the septum
Truncal swellings: Right superior which grows distally and to the left.
Truncal swellings: Right superior which grows distally and to the left.
Secundum Atrial Septal Defect
This type involves septum primum and/or septum secundum.
Secundum Atrial Septal Defect
This type involves septum primum and/or septum secundum.
Persistent Atrio-
ventricular Canal
The persistent atrioventricular canal results from the failure of
Persistent Atrio-
ventricular Canal
The persistent atrioventricular canal results from the failure of
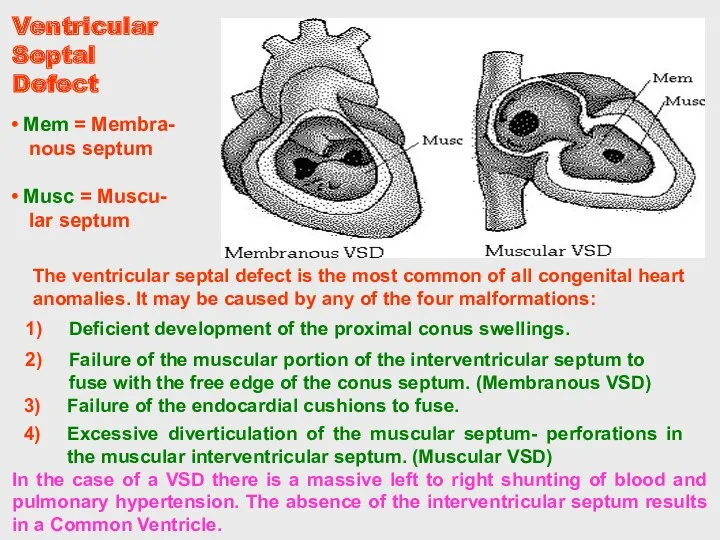
In the case of a VSD there is a massive left
In the case of a VSD there is a massive left
Transposition of the Great Vessels
Transposition is a condition in which the
Transposition of the Great Vessels
Transposition is a condition in which the
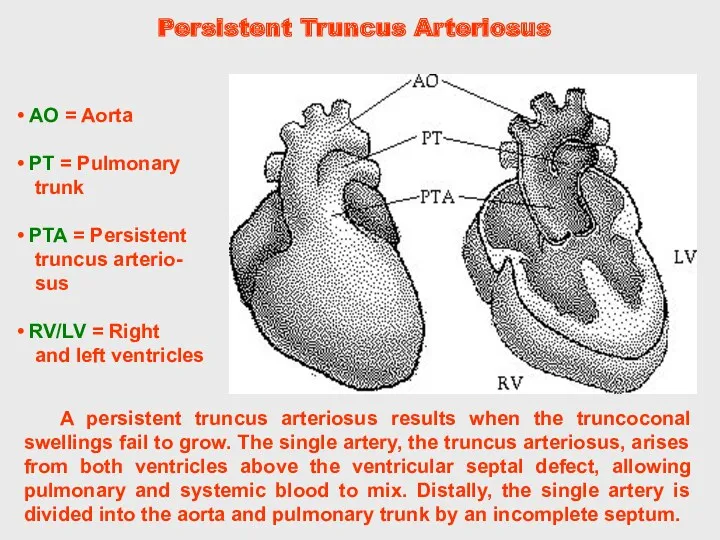
Persistent Truncus Arteriosus
A persistent truncus arteriosus results when the truncoconal swellings
Persistent Truncus Arteriosus
A persistent truncus arteriosus results when the truncoconal swellings
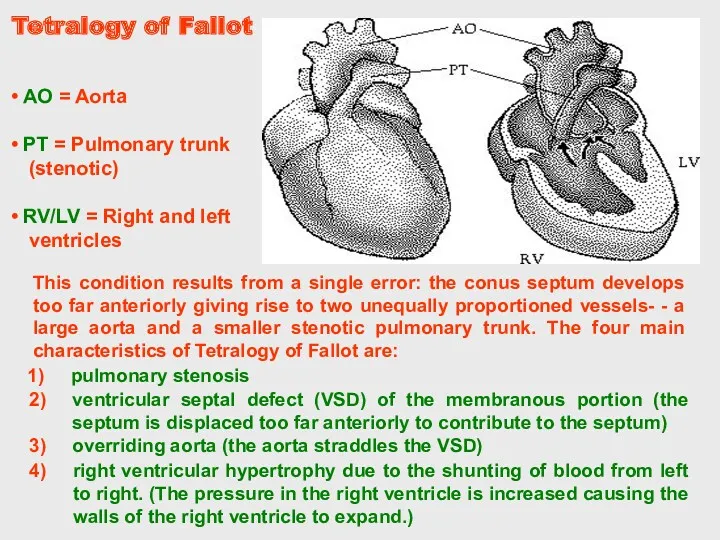
Tetralogy of Fallot
right ventricular hypertrophy due to the shunting of blood
Tetralogy of Fallot
right ventricular hypertrophy due to the shunting of blood
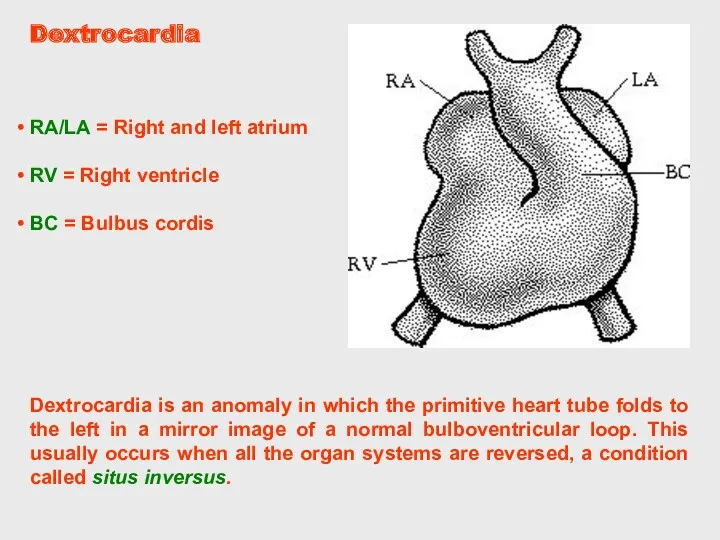
Dextrocardia
Dextrocardia is an anomaly in which the primitive heart tube folds
Dextrocardia
Dextrocardia is an anomaly in which the primitive heart tube folds
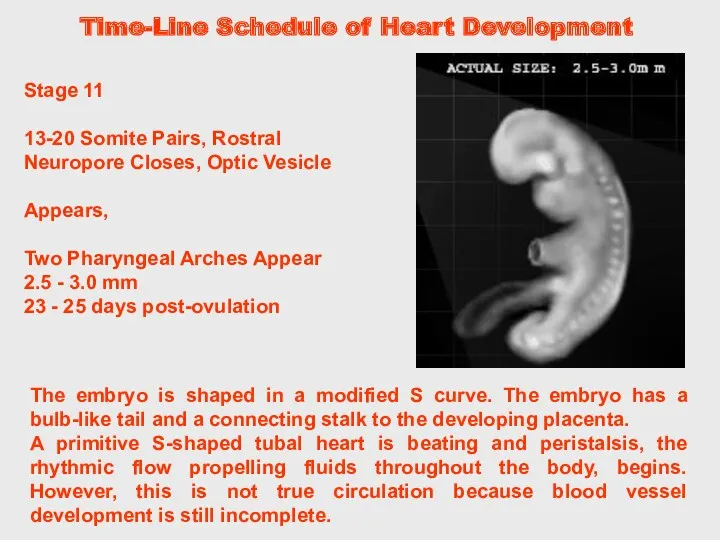
The embryo is shaped in a modified S curve. The embryo
The embryo is shaped in a modified S curve. The embryo
MAIN STAGES OF THE ERALY
HEART DEVELOPMENT
MAIN STAGES OF THE ERALY
HEART DEVELOPMENT
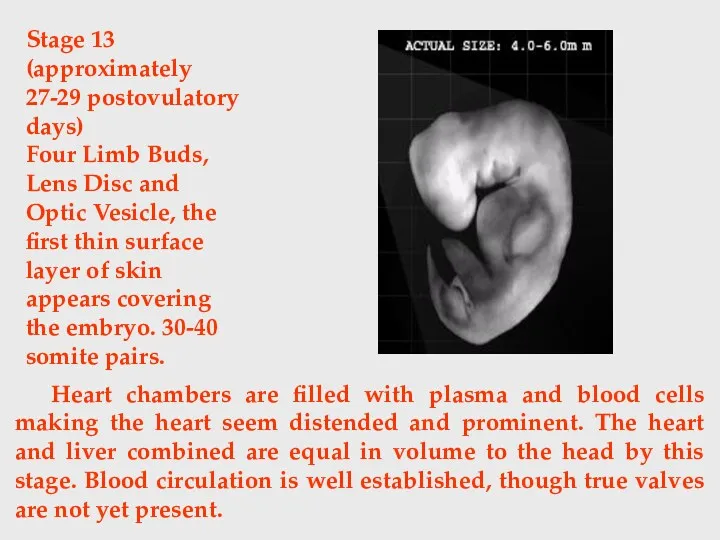
Heart chambers are filled with plasma and blood cells making the
Heart chambers are filled with plasma and blood cells making the
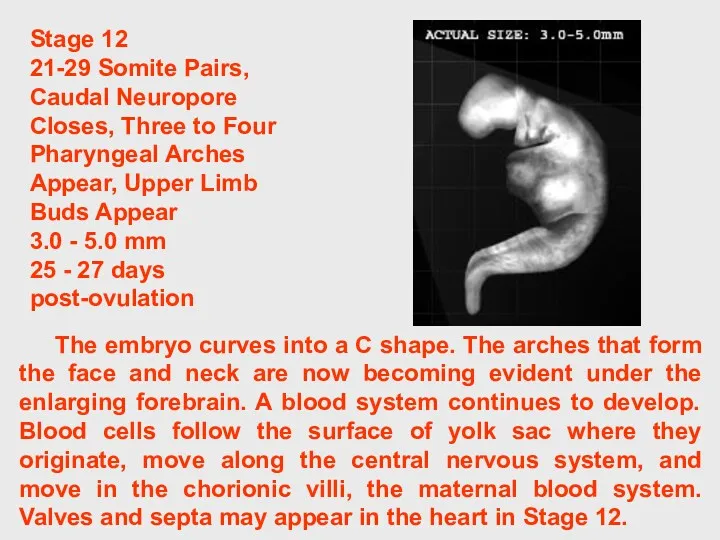
The embryo curves into a C shape. The arches that form
The embryo curves into a C shape. The arches that form
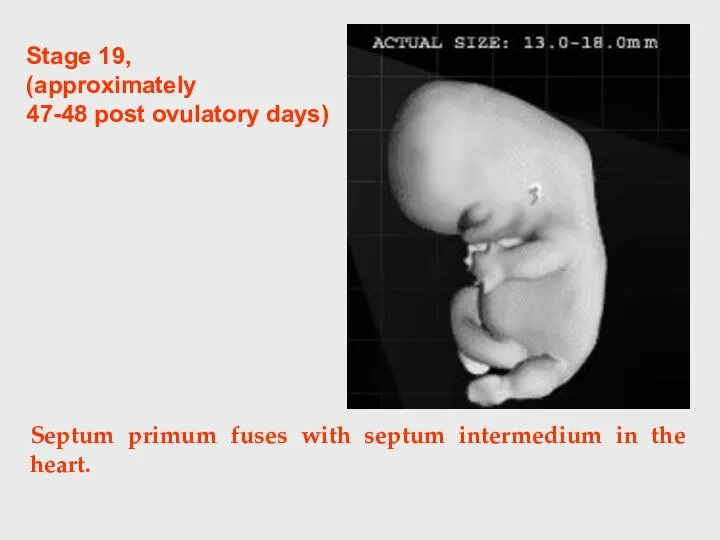
Septum primum fuses with septum intermedium in the heart.
Stage 19,
(approximately
Septum primum fuses with septum intermedium in the heart.
Stage 19,
(approximately
Stage 14, 5th week
Lens Pit and Optic Cup Appear, Endolymphatic Appendage
Stage 14, 5th week
Lens Pit and Optic Cup Appear, Endolymphatic Appendage
Blood flow through the arioventricular canal is divided into left and
Blood flow through the arioventricular canal is divided into left and
Stage 16
(6th weeks post fertilization)
Primary cardiac tube separates into
Stage 16
(6th weeks post fertilization)
Primary cardiac tube separates into
Stage 17
(approximately 41 postovulatory days)
A Four Chambered Heart and a
Stage 17
(approximately 41 postovulatory days)
A Four Chambered Heart and a
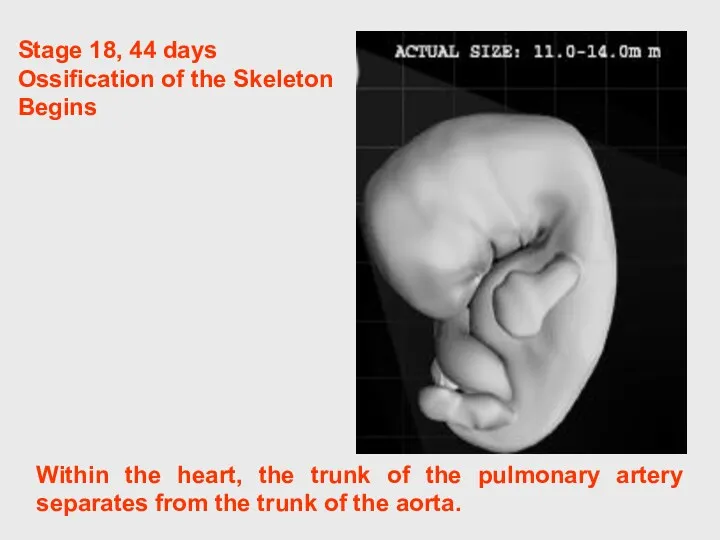
Within the heart, the trunk of the pulmonary artery separates from
Within the heart, the trunk of the pulmonary artery separates from
CONGENITAL MALFORMATIONS OF THE HEART AND GREAT VESSELS.
They are common.
The overall
CONGENITAL MALFORMATIONS OF THE HEART AND GREAT VESSELS.
They are common.
The overall
 Бинокулярное зрение
Бинокулярное зрение Казеозды пневмония
Казеозды пневмония Кардиогенный шок
Кардиогенный шок Болезни желчного пузыря и желчевыводящих путей. Желчно-каменная болезнь. Хронический панкреатит
Болезни желчного пузыря и желчевыводящих путей. Желчно-каменная болезнь. Хронический панкреатит Восточный массаж
Восточный массаж Лекция 8. Электрохимия
Лекция 8. Электрохимия Хроническая почечная недостаточность
Хроническая почечная недостаточность Аллергия. Виды аллергических реакций, их стадии, патогенез
Аллергия. Виды аллергических реакций, их стадии, патогенез Заболевания артерий и вен
Заболевания артерий и вен Тромбэмболия легочой артерии
Тромбэмболия легочой артерии Медициналық генетиканың зерттеу әдістері
Медициналық генетиканың зерттеу әдістері Анатомия органов мочеполового аппарата
Анатомия органов мочеполового аппарата Хейлиты. Глосситы
Хейлиты. Глосситы Пневмонии у беременных
Пневмонии у беременных Чистые руки – залог здоровья
Чистые руки – залог здоровья Третичный сифилис. Врожденный сифилис
Третичный сифилис. Врожденный сифилис Заболевания, сопровождающиеся синдромом сыпи
Заболевания, сопровождающиеся синдромом сыпи Остеоартроз. Клиника остеоартроза. Методы лечения
Остеоартроз. Клиника остеоартроза. Методы лечения Абдоминальный синдром при холепатиях, клиника, диагностика, дифференциальная диагностика, лечение
Абдоминальный синдром при холепатиях, клиника, диагностика, дифференциальная диагностика, лечение Опорно-двигательный аппарат
Опорно-двигательный аппарат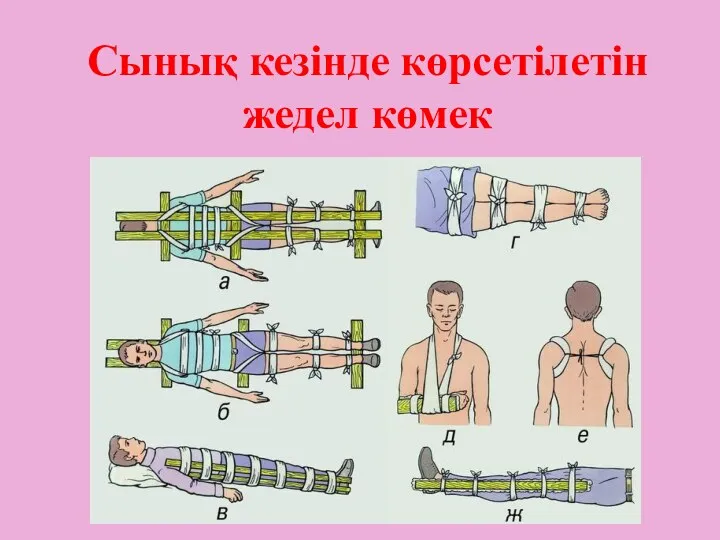 Сынық кезінде көрсетілетін жедел көмек
Сынық кезінде көрсетілетін жедел көмек Leptospira interrogans – возбудитель лептоспироза
Leptospira interrogans – возбудитель лептоспироза Заболевания плевры. Плевриты
Заболевания плевры. Плевриты Введение в нейрохирургию
Введение в нейрохирургию Заболевания прямой кишки: парапроктит, геморрой
Заболевания прямой кишки: парапроктит, геморрой Нарушение белкового обмена
Нарушение белкового обмена Медицинская генетика. (Лекция 1)
Медицинская генетика. (Лекция 1) Муковисцидоз. Патогенезі
Муковисцидоз. Патогенезі