- Diseases of endocrine system

Содержание
- 2. Endocrine Pathology Cell signaling system Surface receptors cAMP and tyrosine kinase system Cytoplasmic receptors Penetrate cell
- 3. Endocrine Pathology Too much hormone activity Too little hormone activity Autoimmune destruction Inflammatory destruction Tumor or
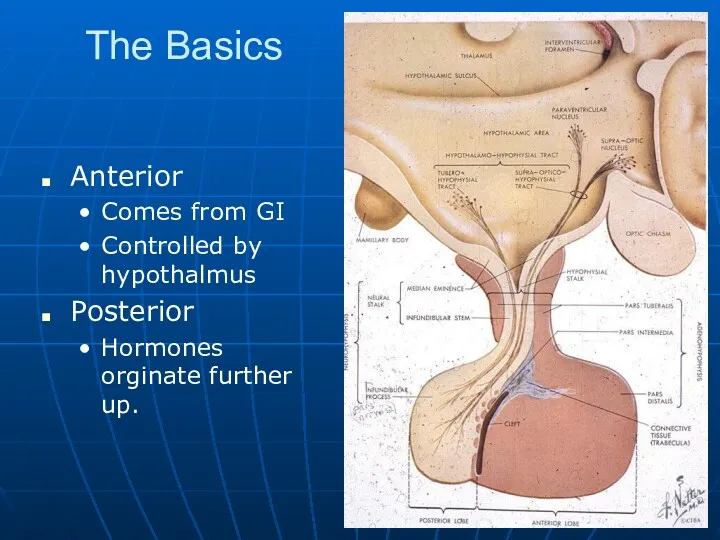
- 4. The Basics Anterior Comes from GI Controlled by hypothalmus Posterior Hormones orginate further up.
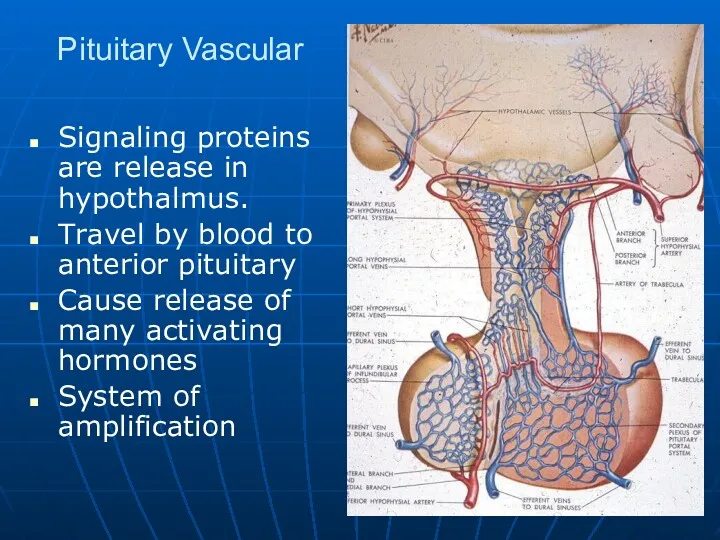
- 5. Pituitary Vascular Signaling proteins are release in hypothalmus. Travel by blood to anterior pituitary Cause release
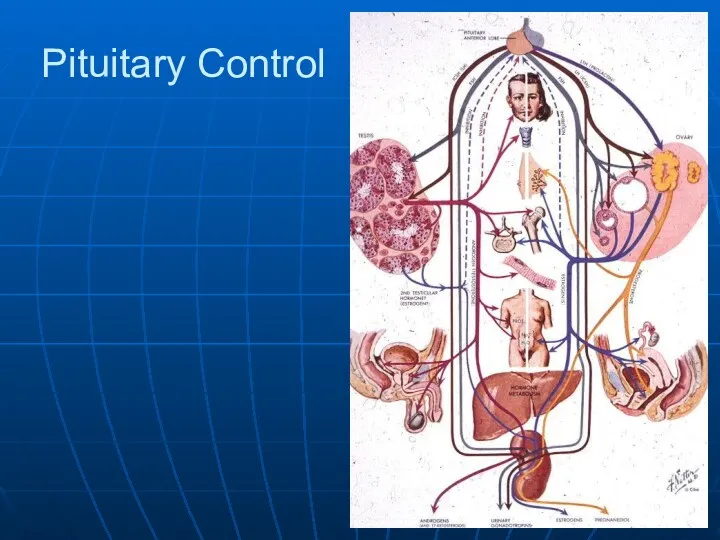
- 6. Pituitary Control
- 7. The normal gross appearance of the pituitary gland removed from the sella turcica is shown here.
- 8. The normal microscopic appearance of the pituitary gland is shown here. The adenohypophysis is at the
- 9. The normal microscopic appearance of the adenohypophysis is shown here. The adenohypophysis contains three major cell
- 10. This immunoperoxidase stain with antibody to prolactin identifies the specific acidophils in the anterior pituitary that
- 11. The neurohypophysis shown here resembles neural tissue, with glial cells, nerve fibers, nerve endings, and intra-axonal
- 12. Space Occupying Lesions Tumors Embryonic rests Squeeze gland out of existence. Generalized failure Visual field changes
- 13. Visual Fields Loss of temporal fields. Nasal retina Damage to decusating optic nerve fibers
- 14. Pituitary Adenomas Rare Make nothing or Prolactin ACTH, GH,TSH are very rare More often end up
- 15. The circumscribed mass lesion present here in the sella turcica is a pituitary adenoma. Though pituitary
- 16. This is a microadenoma of the anterior pituitary. Such microadenomas may appear in 1 to 5%
- 17. Here is a high power microscopic view of an adenohypophyseal adenoma. Endocrine neoplasms are composed of
- 18. The microscopic appearance of the pituitary adenoma is shown here. Note the monotonous appearance of these
- 19. Acromegaly Growth hormone excess after closing of epiphyses. Periosteal bone growth. Diabetes Prognathism
- 20. Hypopituitarism Destruction of gland. Ischemia ‘Benign’ adenoma destroying gland Craniopharyngioma Rathke’s pouch remenant Benign cyst, but
- 21. Ischemic Destruction Shehan’s syndrome Post delivery problem No lactation In time general failure of ‘downstream’ systems
- 22. The sella turcica at the base of the skull shown here contains a flattened pituitary at
- 23. These medium and high power microscopic views of the anterior pituitary demonstrate mononuclear inflammatory cell infiltrates
- 24. A craniopharyngioma is seen here at medium and high power. It is derived from remnants of
- 25. Posterior Pituitary Loss of ADH Diabetes insipidis Dose not make concentrated urine Large volumes of dilute
- 26. Control of Thyroid Hormone Hypothalmus Pituitary Thyroid Tissue level Establishes metabolic rate for the whole organism
- 27. This is the normal appearance of the thyroid gland on the anterior trachea of the neck.
- 28. Normal thyroid seen microscopically consists of follicles lined by a an epithelium and filled with colloid.
- 29. This normal thyroid follicle is lined by a cuboidal follicular epithelium with cells that can add
- 30. Hyperthyroidism Clinical findings Heat intolerance Tremor Tachycardia Hyperactive Increased body metabolism and temperature Ocular changes Main
- 31. Grave’s disease Grave’s disease is multi-organ systemic autoimmune disorder, manifested by the triad of basic features:
- 32. Hyperophthalmia Grave’s disease Antibody stimulates TSH receptors in extraocular muscles. Increased tissue in orbit causes eye
- 33. Nodular goiter Diffuse goiter
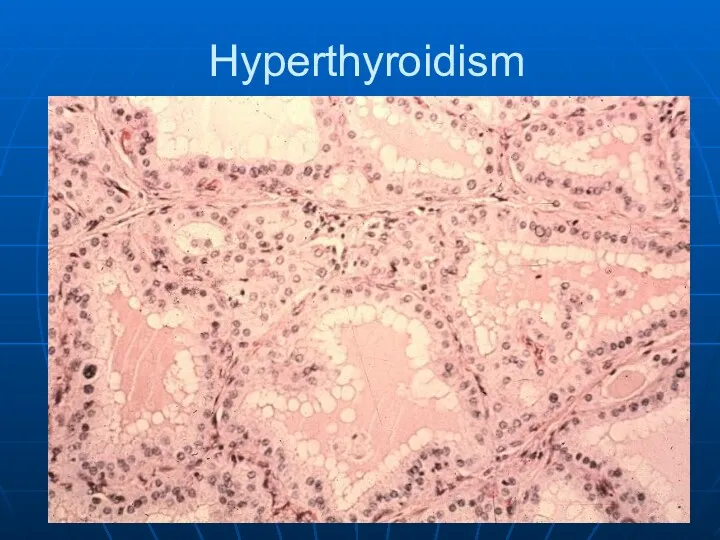
- 34. Hyperthyroidism
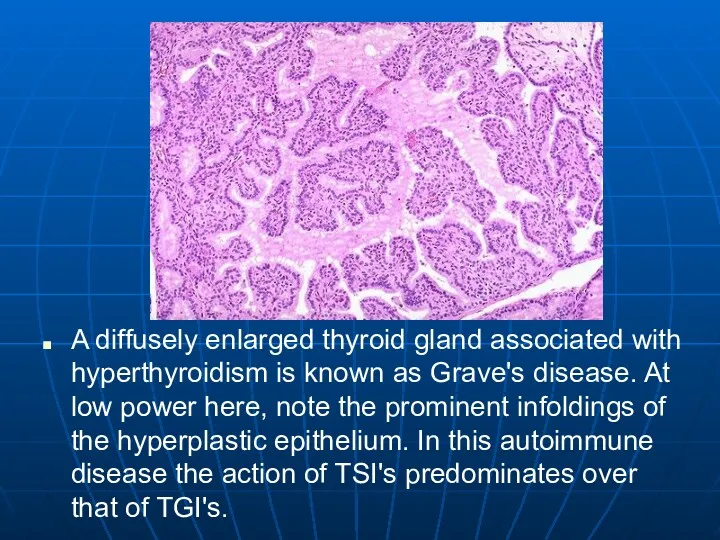
- 35. A diffusely enlarged thyroid gland associated with hyperthyroidism is known as Grave's disease. At low power
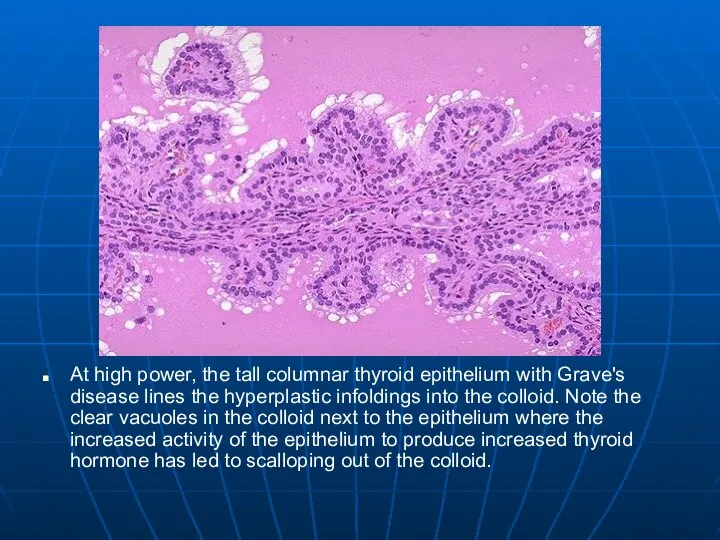
- 36. At high power, the tall columnar thyroid epithelium with Grave's disease lines the hyperplastic infoldings into
- 37. Tumors and Changes in Size
- 38. Goiter Nodular Uniform increase Scarring Cysts Generally euthyroid May cause airway compression
- 39. Hashimoto’s Thyroiditis Many antibodies T & B cells Active germinal centers Women 5:1 Scarring In time
- 40. Hashimoto’s Thryoiditis
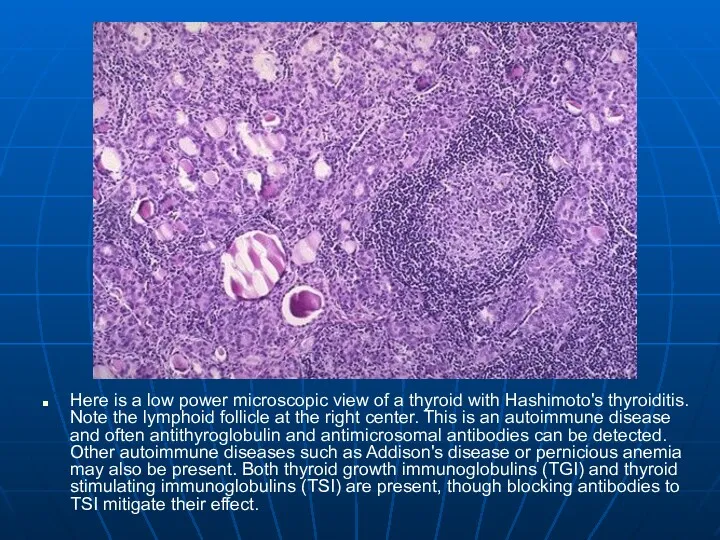
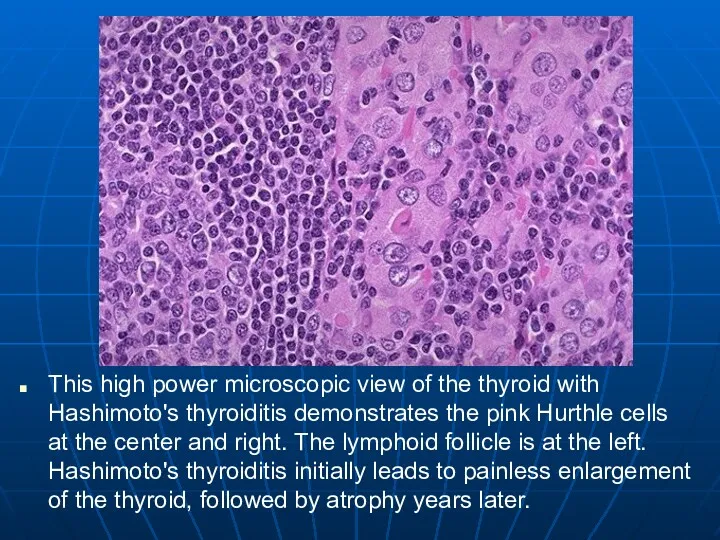
- 41. Here is a low power microscopic view of a thyroid with Hashimoto's thyroiditis. Note the lymphoid
- 42. This high power microscopic view of the thyroid with Hashimoto's thyroiditis demonstrates the pink Hurthle cells
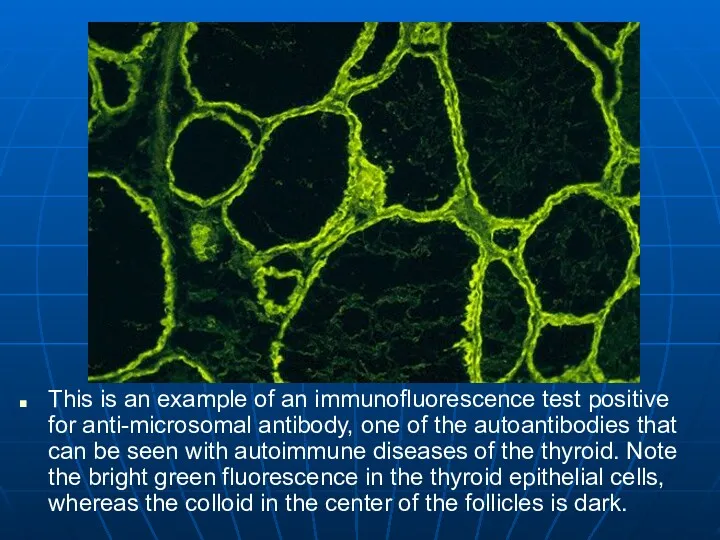
- 43. This is an example of an immunofluorescence test positive for anti-microsomal antibody, one of the autoantibodies
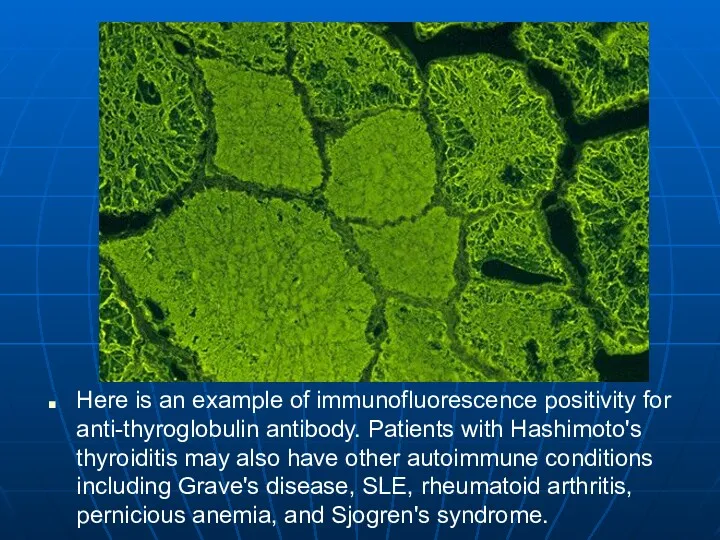
- 44. Here is an example of immunofluorescence positivity for anti-thyroglobulin antibody. Patients with Hashimoto's thyroiditis may also
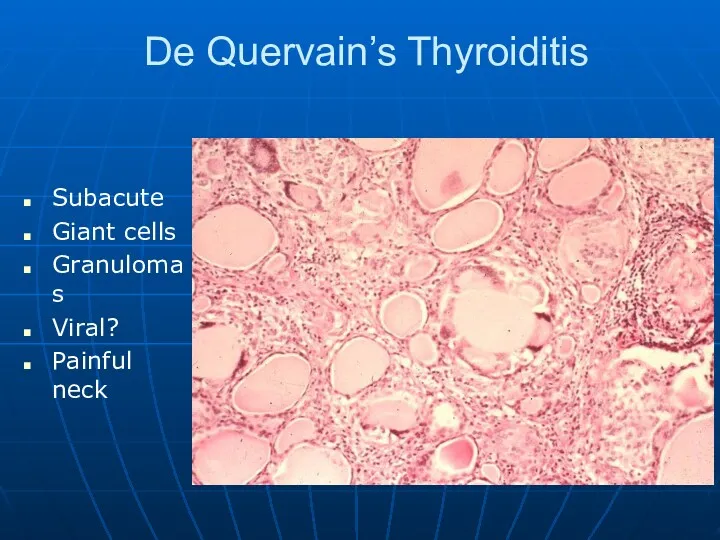
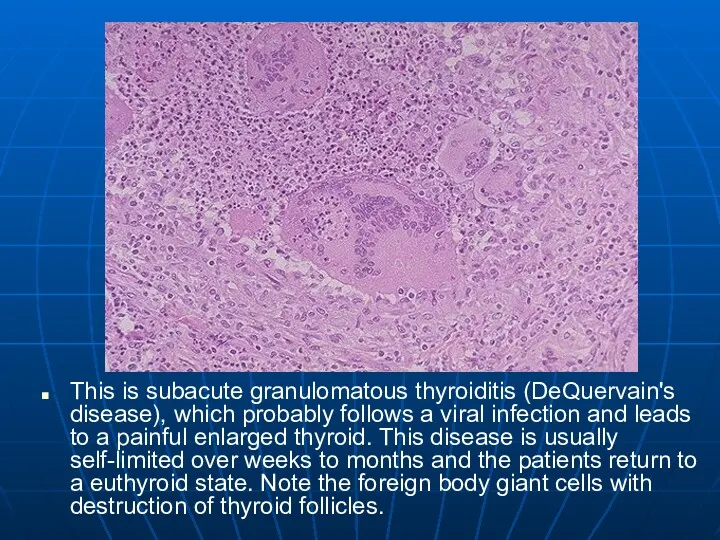
- 45. De Quervain’s Thyroiditis Subacute Giant cells Granulomas Viral? Painful neck
- 46. This is subacute granulomatous thyroiditis (DeQuervain's disease), which probably follows a viral infection and leads to
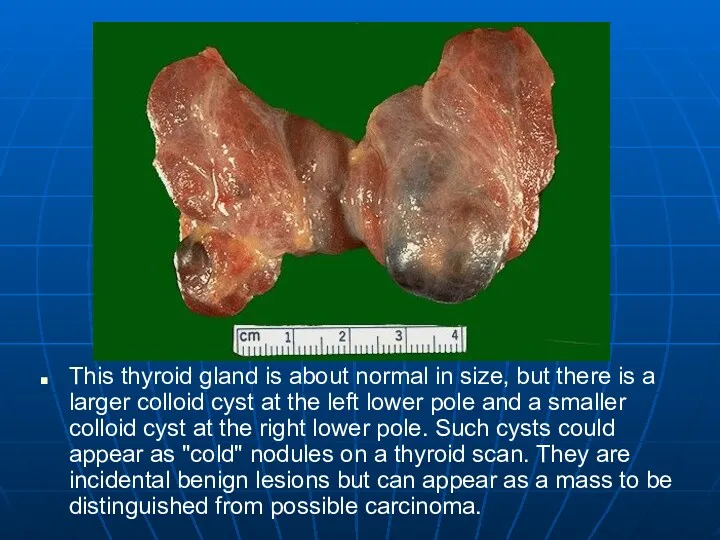
- 47. This thyroid gland is about normal in size, but there is a larger colloid cyst at
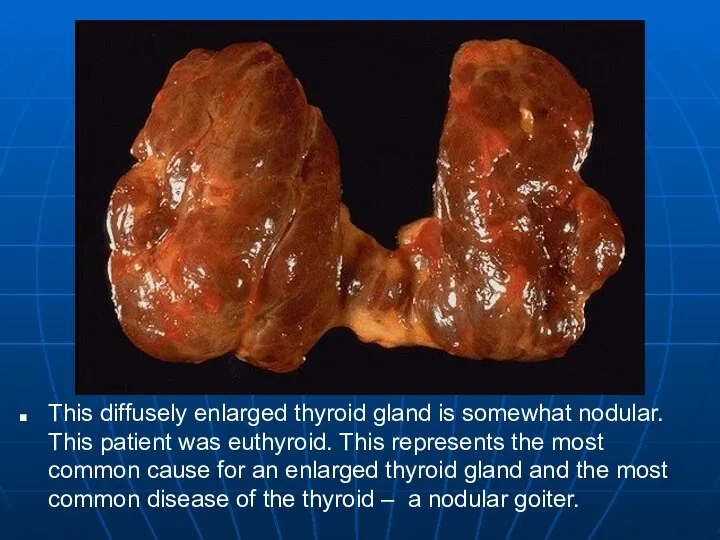
- 48. This diffusely enlarged thyroid gland is somewhat nodular. This patient was euthyroid. This represents the most
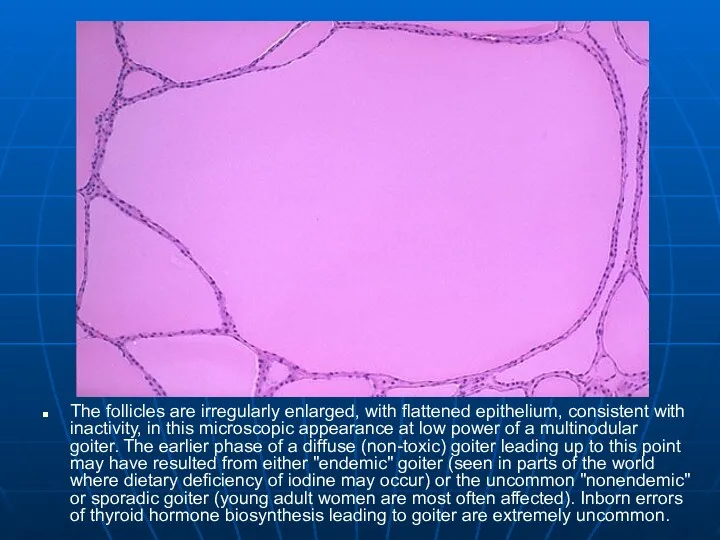
- 49. The follicles are irregularly enlarged, with flattened epithelium, consistent with inactivity, in this microscopic appearance at
- 50. Hypothyroidism Genetics Gland destruction Inflammatory Surgical removal Radiation treatment for hyperthyroidism Iodine deficiency Can’t make T4
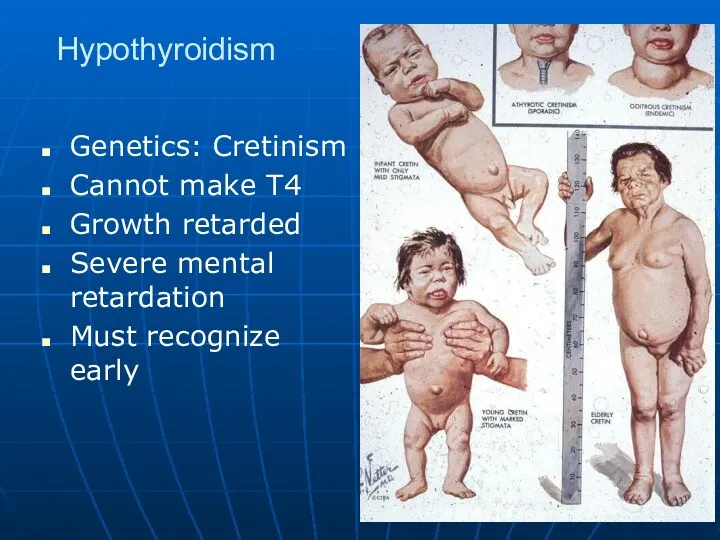
- 51. Hypothyroidism Genetics: Cretinism Cannot make T4 Growth retarded Severe mental retardation Must recognize early
- 52. Hypothyroidism Clinical Cold intolerance Bradycardia Heart failure High lipids Lethargic Photophobia Myxedema Skin and hair changes
- 53. This symmetrically small thyroid gland demonstrates atrophy. This patient was hypothyroid. This is the end result
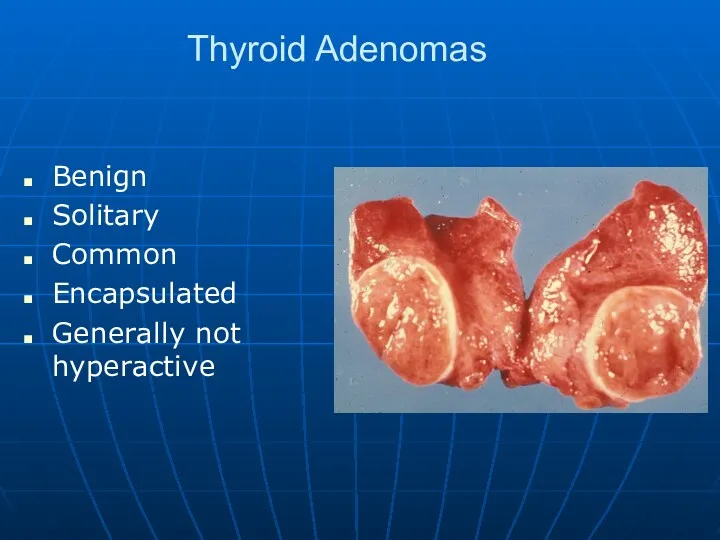
- 54. Thyroid Adenomas Benign Solitary Common Encapsulated Generally not hyperactive
- 55. Here is a surgical excision of a small mass from the thyroid gland that has been
- 56. Here is another follicular neoplasm (a follicular adenoma histologically) that is surrounded by a thin white
- 57. Normal thyroid follicles appear at the lower right. The follicular adenoma is at the center to
- 58. Malignancies of Thyroid Origin Arising from follicular cells Papillary Carcinoma Follicular Carcinoma Mixed pattern Interstitial cells
- 59. Papillary Carcinoma Papillary groups May have multiple sites Not actively producing T4 Readily treated Spread Nodes
- 60. Papillary Carcinoma
- 61. Sectioning through a lobe of excised thyroid gland reveals papillary carcinoma. This neoplasm can be multifocal,
- 62. Orphan Annie Nuclei Needle aspirates Open eyed nuclei indicative of papillary ca
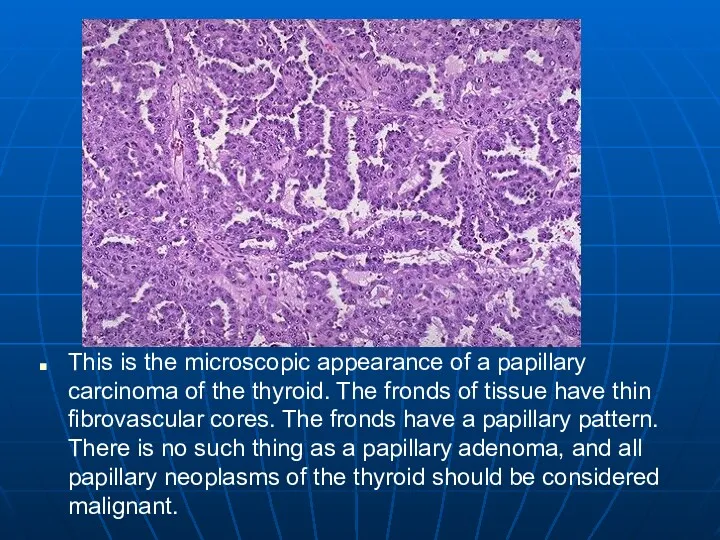
- 63. This is the microscopic appearance of a papillary carcinoma of the thyroid. The fronds of tissue
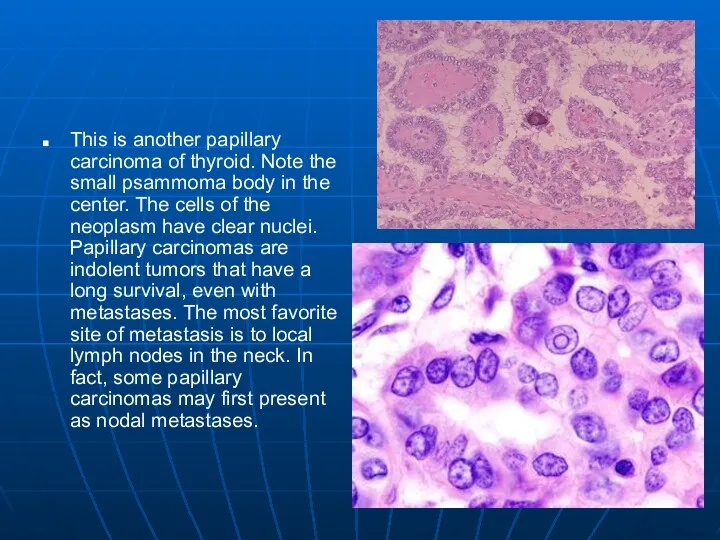
- 64. This is another papillary carcinoma of thyroid. Note the small psammoma body in the center. The
- 65. C Cell Carcinoma Interstitial cells Makes calcitonin Makes amyloid Beta pleated sheet protein Often part of
- 66. C Cell Carcinoma
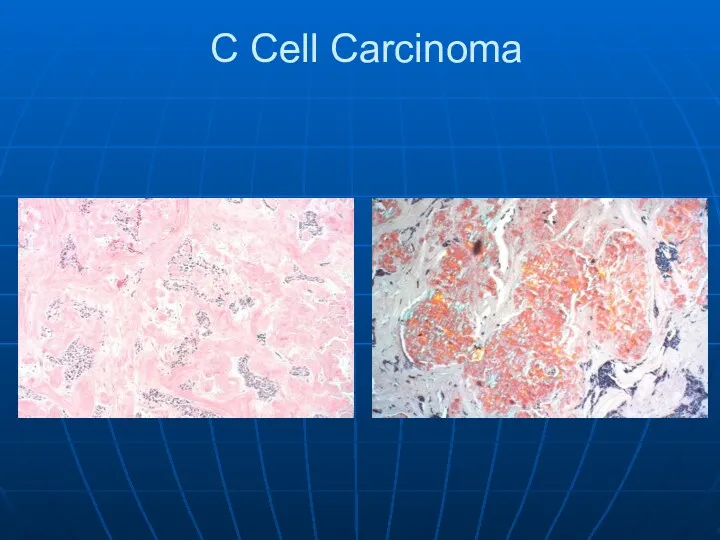
- 67. At the center and to the right is a medullary carcinoma of thyroid. At the far
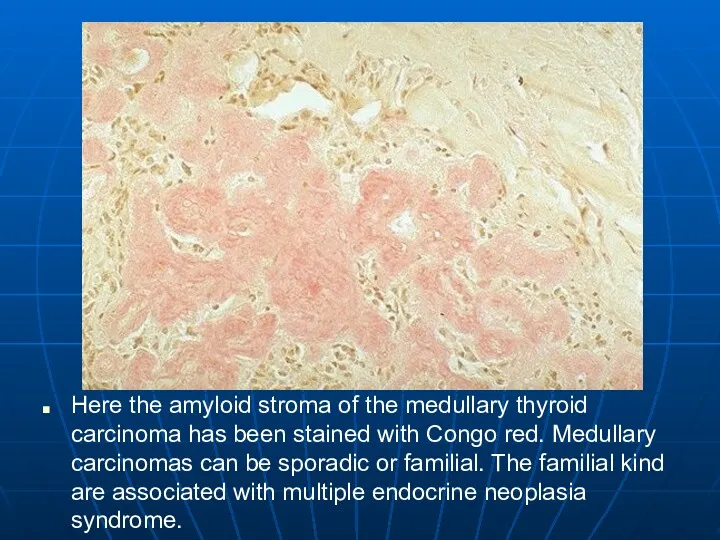
- 68. Here the amyloid stroma of the medullary thyroid carcinoma has been stained with Congo red. Medullary
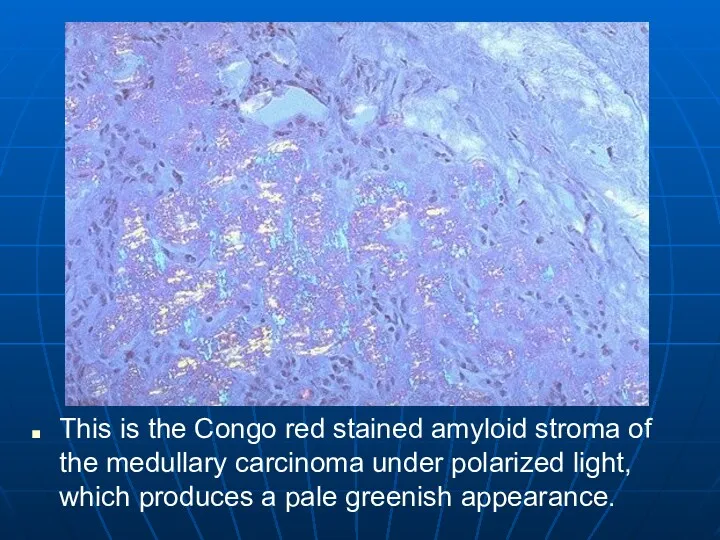
- 69. This is the Congo red stained amyloid stroma of the medullary carcinoma under polarized light, which
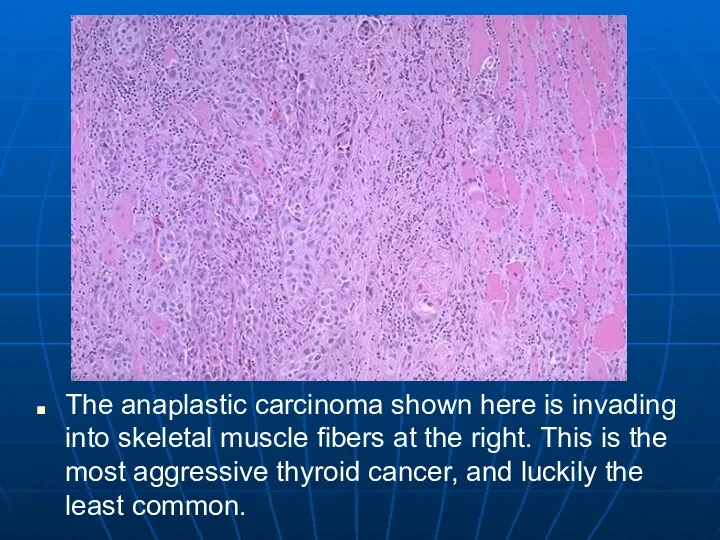
- 70. The anaplastic carcinoma shown here is invading into skeletal muscle fibers at the right. This is
- 71. There is no resemblance to normal thyroid tissue-hence the term "anaplastic" to characterize this thyroid carcinoma.
- 72. Parathyroid Come from the pharyngeal pouches Most of us have 4 Make PTH Mobilizes calcium Released
- 73. Parathyroid hyperplasia is shown here. Three and one-half glands have been removed (only half the gland
- 74. Here is a normal parathyroid gland. Variable numbers of steatocytes are mixed with the parathyroid tissue.
- 75. Hyperparathyroidism Primary Parathyroid adenoma 80% Hyperplasia 10-15% Parathyroid ca Hypercalcemia Stones, bones, abdominal groans and psychic
- 76. In parathyroid hyperplasia, there is little or no adipose tissue, but any or all cell types
- 77. Parathyroid Adenoma
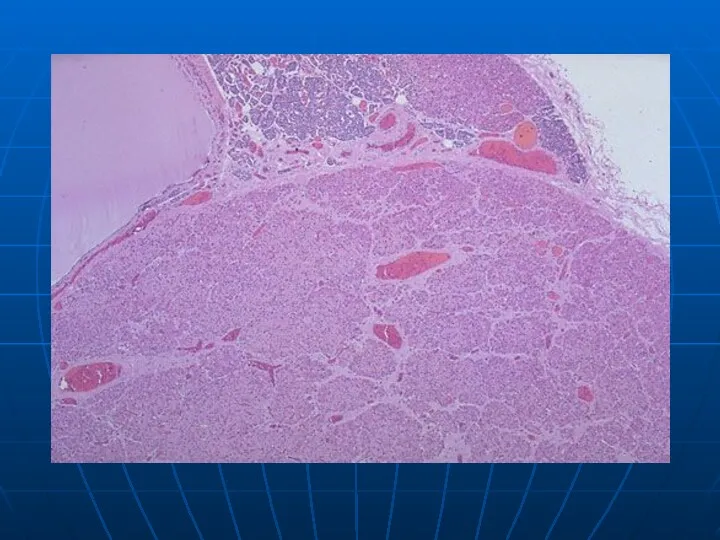
- 78. Here is a parathyroid adenoma, which is the most common cause for primary hyperparathyroidism. A rim
- 80. Secondary Hyperparathyroidism Renal failure almost always Phosphates build up in the blood. Cause calcium to drop.
- 81. This is the gross appearance of a parathyroid carcinoma. The serum calcium can be quite high.
- 82. This is a parathyroid carcinoma seen at medium power on the left and higher power on
- 83. Hypoparathyroidism Increased neuromuscular excitability May lead to tetany Irritability and possibly even psychosis Parkinson-like symptoms Cataracts
- 84. Adrenal Gland Really two glands in one. Cortex -> Salt Sugar Sex Medulla Epinephrine Norepinephrine
- 85. Here are normal adrenal glands. Each adult adrenal gland weighs from 4 to 6 grams.
- 86. The pair of adrenals in the center are normal. Those at the top come from a
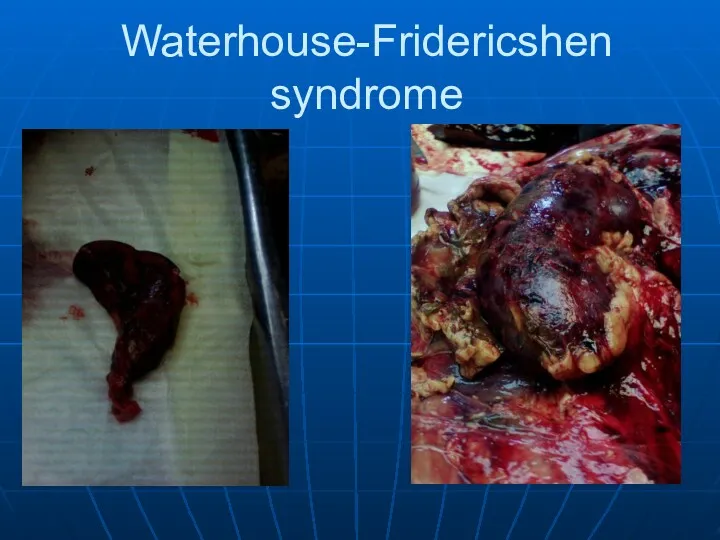
- 87. These adrenals are black-red from extensive hemorrhage in a patient with meningococcemia. This produces the Waterhouse-Friderichsen
- 88. Cushing’s Syndrome Effects of too much cortisol Moon face Central obesity Buffalo hump Osteoporosis Fractures Hypertension
- 89. Cushing’s Disease Altered feedback regulation at level of hypothalmus and pituitary It only takes a small
- 90. Cushing’s Disease
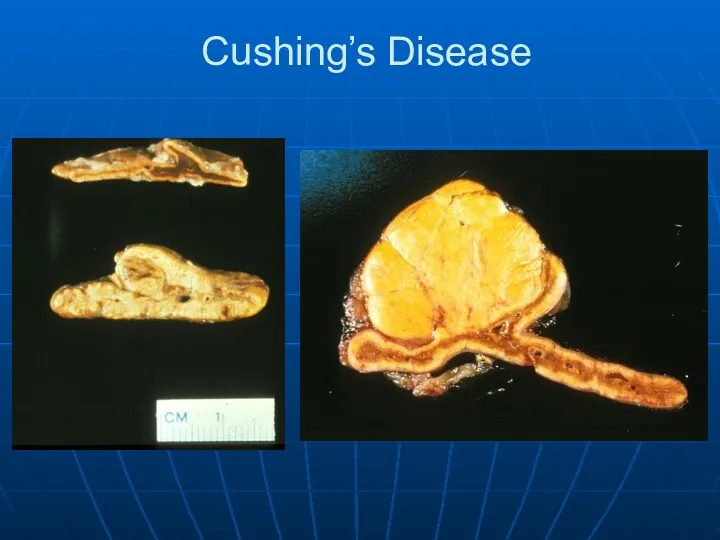
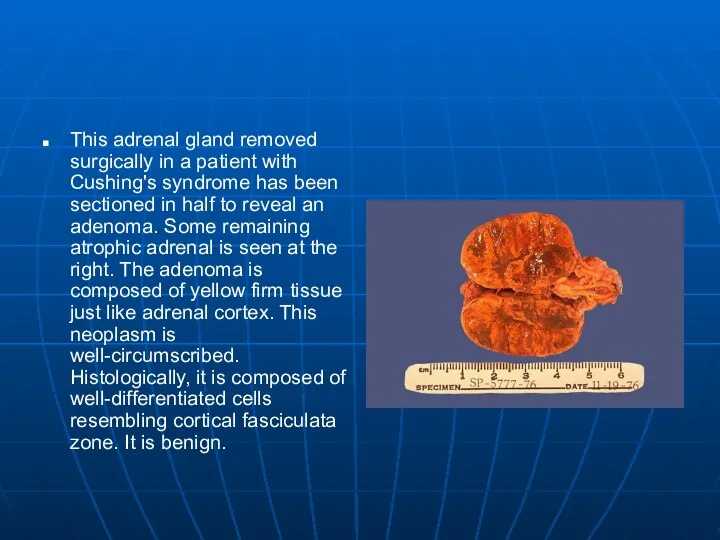
- 91. This adrenal gland removed surgically in a patient with Cushing's syndrome has been sectioned in half
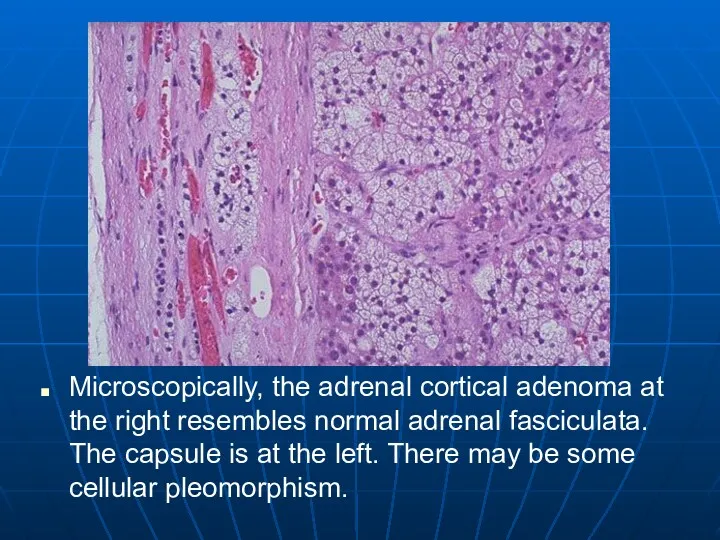
- 92. Microscopically, the adrenal cortical adenoma at the right resembles normal adrenal fasciculata. The capsule is at
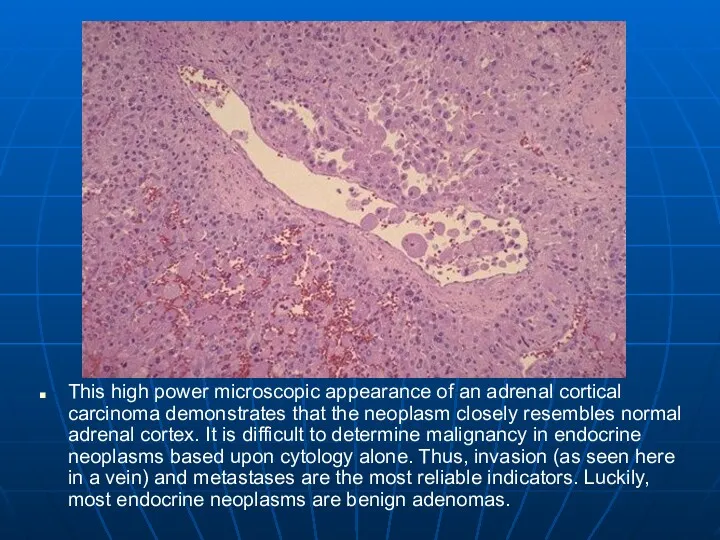
- 93. This high power microscopic appearance of an adrenal cortical carcinoma demonstrates that the neoplasm closely resembles
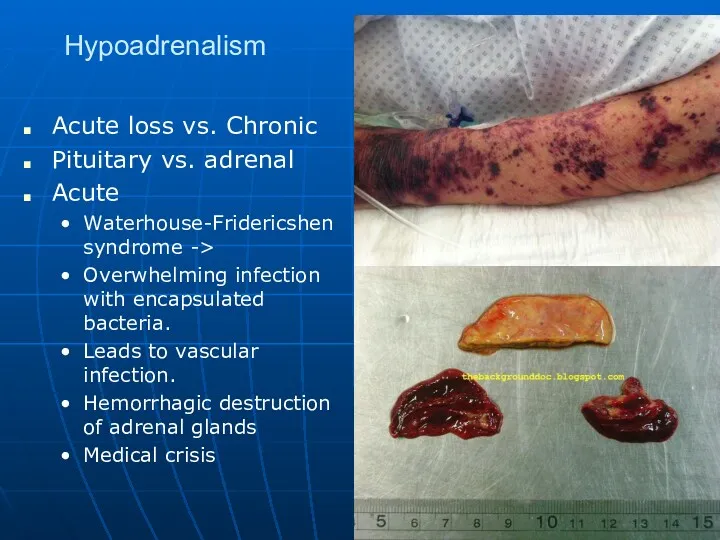
- 94. Hypoadrenalism Acute loss vs. Chronic Pituitary vs. adrenal Acute Waterhouse-Fridericshen syndrome -> Overwhelming infection with encapsulated
- 95. Waterhouse-Fridericshen syndrome
- 96. Waterhouse-Fridericshen syndrome
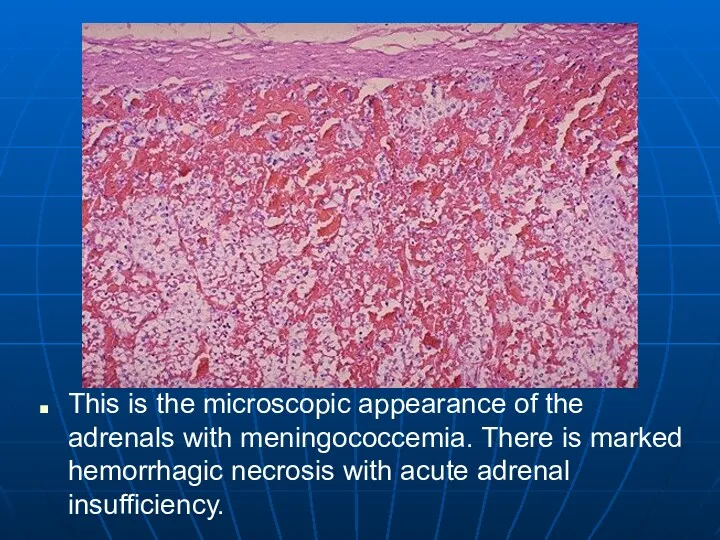
- 97. This is the microscopic appearance of the adrenals with meningococcemia. There is marked hemorrhagic necrosis with
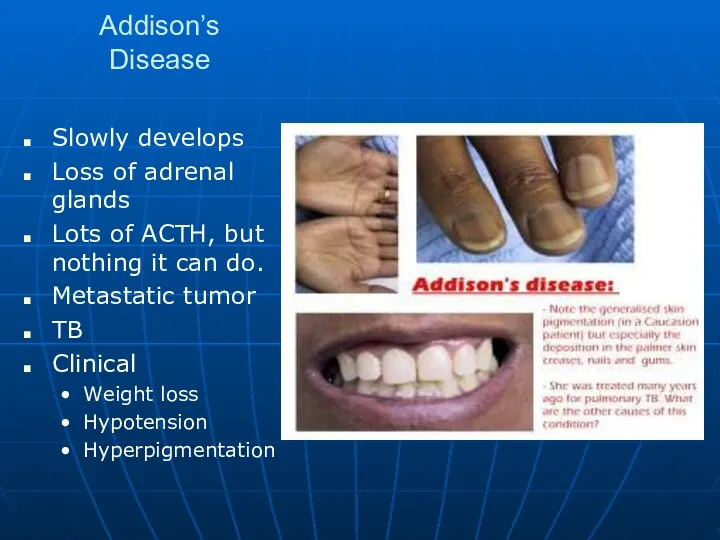
- 98. Addison’s Disease Slowly develops Loss of adrenal glands Lots of ACTH, but nothing it can do.
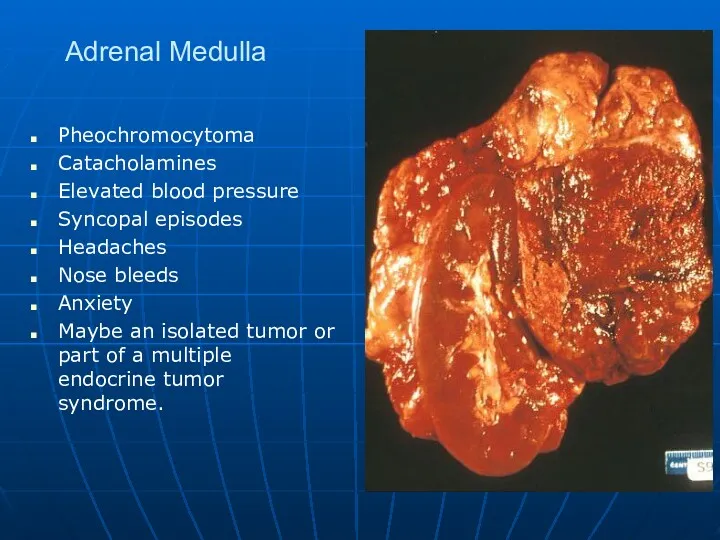
- 99. Adrenal Medulla Pheochromocytoma Catacholamines Elevated blood pressure Syncopal episodes Headaches Nose bleeds Anxiety Maybe an isolated
- 100. Pheochromocytoma
- 101. This large adrenal neoplasm has been sectioned in half. Note the grey-tan color of the tumor
- 102. There is some residual adrenal cortical tissue at the lower center right, with the darker cells
- 103. By electron microscopy, the neoplastic cells of the pheochromocytoma contain neurosecretory granules. It is these granules
- 104. Diabetes mellitus
- 105. Diabetes Mellitus General definition: Chronic disorder of glucose metabolism with hyperglycemia, triggered by conditions associated with
- 106. Diabetes Mellitus Secondary diabetes mellitus: Insulin deficiency due to islet damage from pancreatic disease such as
- 107. Diabetes Mellitus Definition
- 108. Diabetes Mellitus Definition
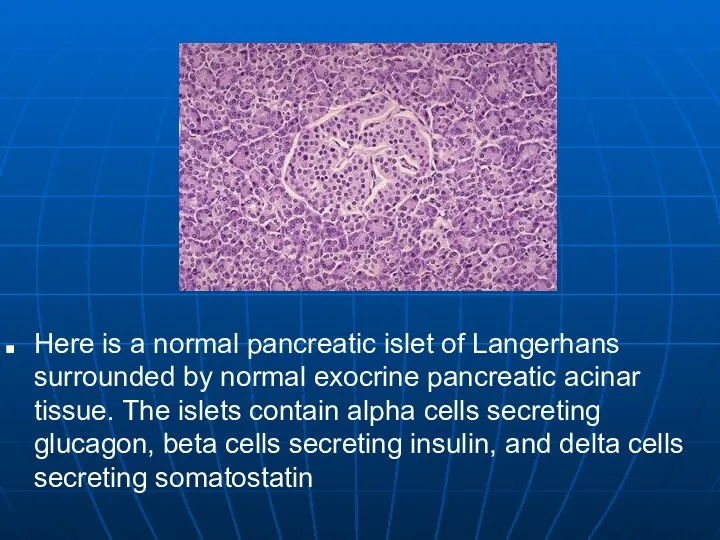
- 109. Here is a normal pancreatic islet of Langerhans surrounded by normal exocrine pancreatic acinar tissue. The
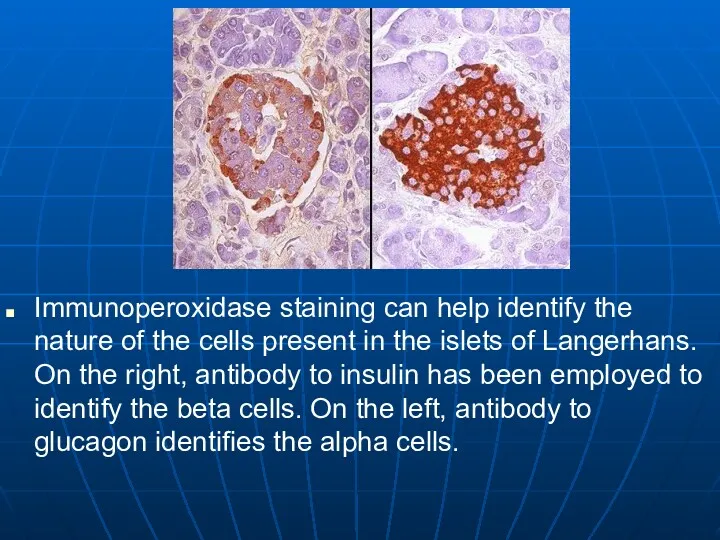
- 110. Immunoperoxidase staining can help identify the nature of the cells present in the islets of Langerhans.
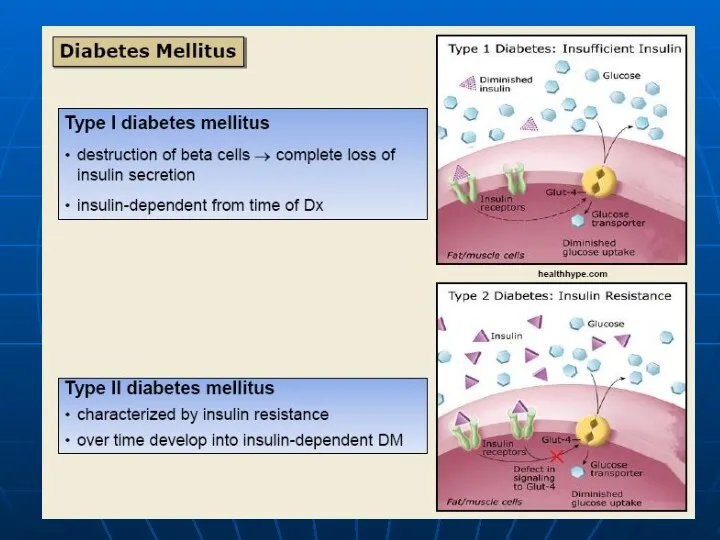
- 112. Type I Diabetes Mellitus Synonyms: juvenile-onset diabetes mellitus, insulin-dependent diabetes mellitus (IDDM). Autoimmune lymphocytic insulitis in
- 113. Type 1 Diabetes Mellitus Progressive destruction of pancreatic β cells Autoantibodies cause a reduction of 80%
- 114. This is an insulitis of an islet of Langerhans in a patient who will eventually develop
- 115. A Type I diabetes mellitus: loss of βcells (IH; insulin) x 200 B Type I diabetes
- 116. Diabetes Mellitus Type II Diabetes Mellitus Synonyms: adult-onset diabetes mellitus, non-insulindependent diabetes mellitus (NIDDM). Type IIa
- 117. Type 2 Diabetes Mellitus Accounts for 90% of patients with diabetes Usually occurs in people over
- 118. Pancreas continues to produce some endogenous insulin Insulin produced is either insufficient or poorly utilized by
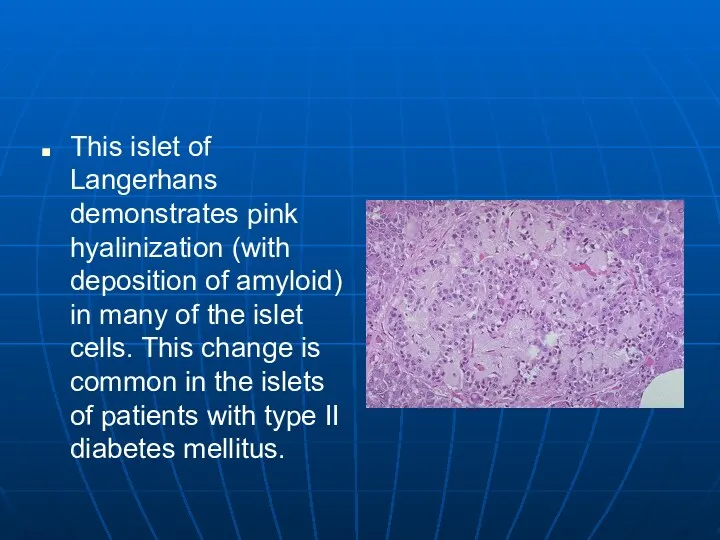
- 120. This islet of Langerhans demonstrates pink hyalinization (with deposition of amyloid) in many of the islet
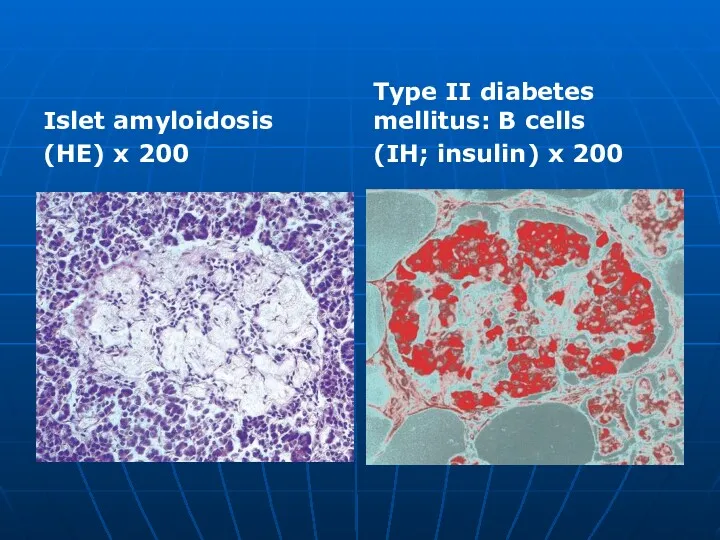
- 121. Islet amyloidosis (HE) x 200 Type II diabetes mellitus: В cells (IH; insulin) x 200
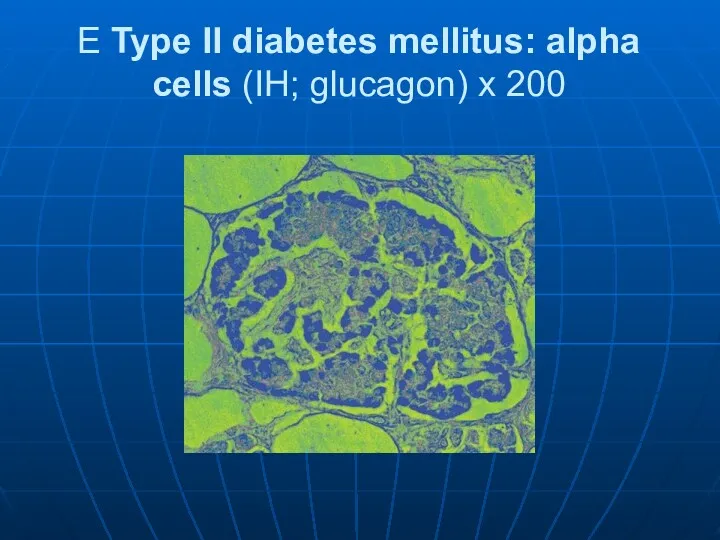
- 122. E Type II diabetes mellitus: alpha cells (IH; glucagon) x 200
- 123. Secondary Diabetes Results from another medical condition or due to the treatment of a medical condition
- 126. Diabetic macroangiopathy follows the pattern of atherosclerosis . Complications: – Coronary sclerosis can lead to myocardial
- 127. Diabetic gangrene
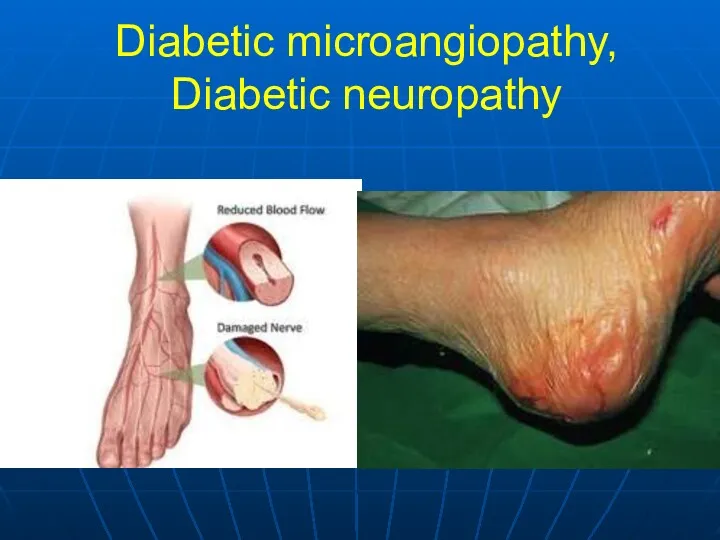
- 129. Diabetic microangiopathy: Chronic increased glucose concentration leads to glycosylation of proteins, altering the structure and permeability
- 130. Diabetic cataract: Osmotic vacuolar degeneration of the epithelium of the lens creates lens opacities. Diabetic liver:
- 131. Gestational Diabetes Develops during pregnancy Detected at 24 to 28 weeks of gestation ↑ Risk for
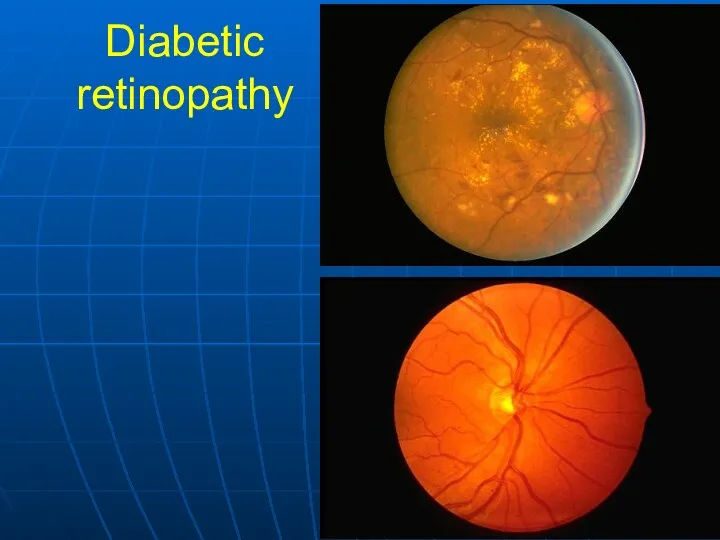
- 132. Diabetic retinopathy
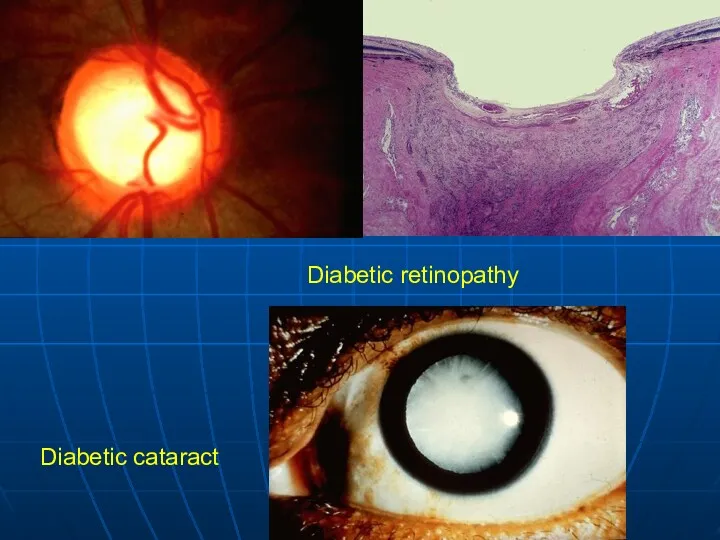
- 133. Diabetic retinopathy Diabetic cataract
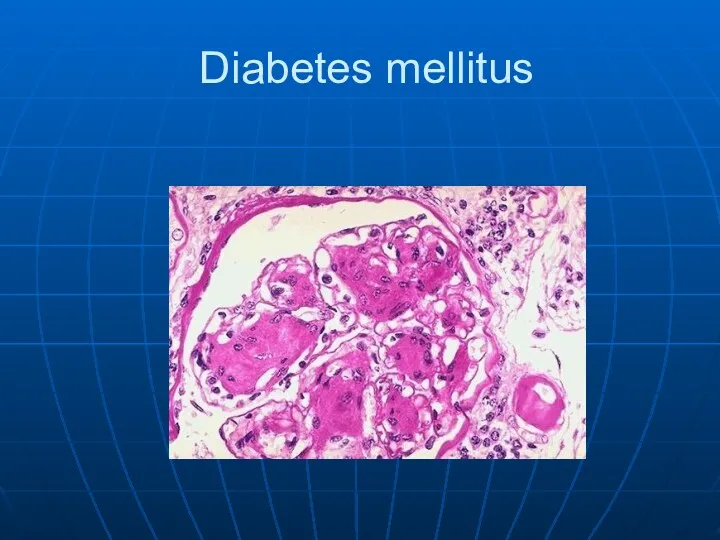
- 135. Diabetes mellitus
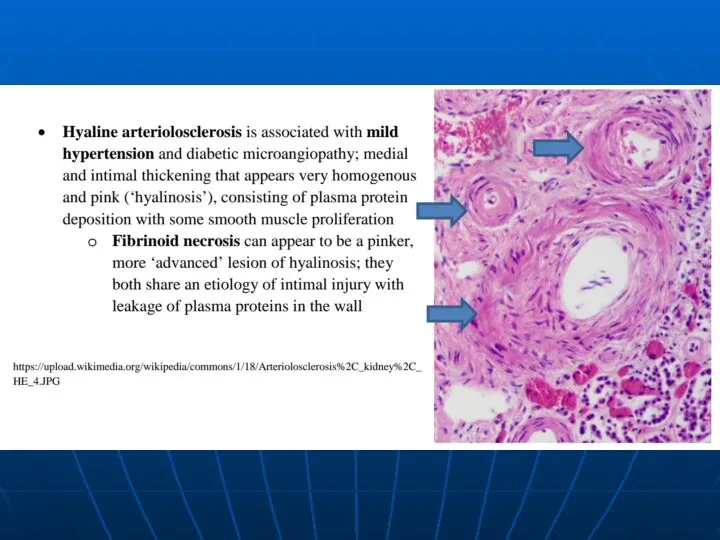
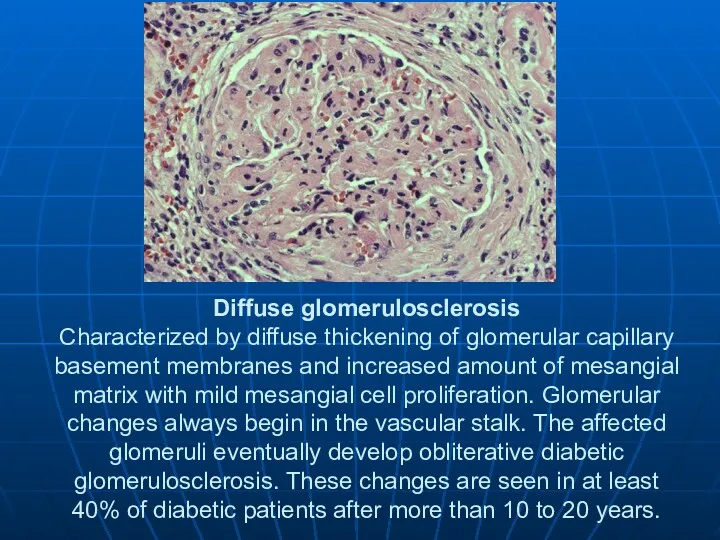
- 136. Diffuse glomerulosclerosis Characterized by diffuse thickening of glomerular capillary basement membranes and increased amount of mesangial
- 137. Diabetic microangiopathy, Diabetic neuropathy
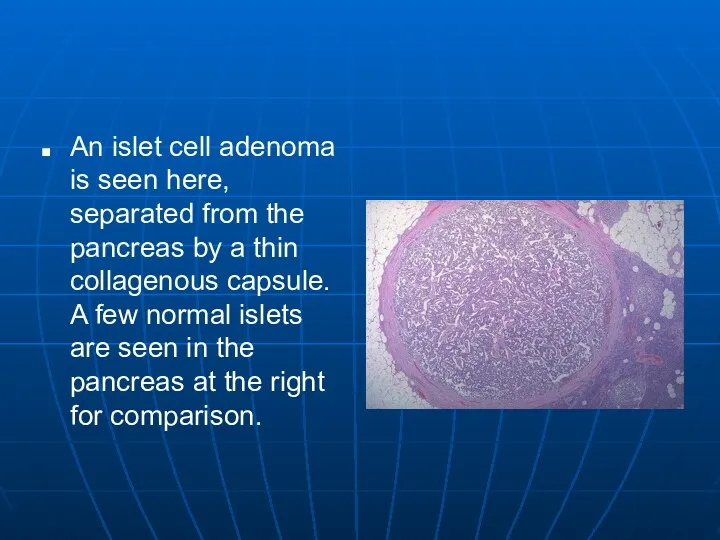
- 138. An islet cell adenoma is seen here, separated from the pancreas by a thin collagenous capsule.
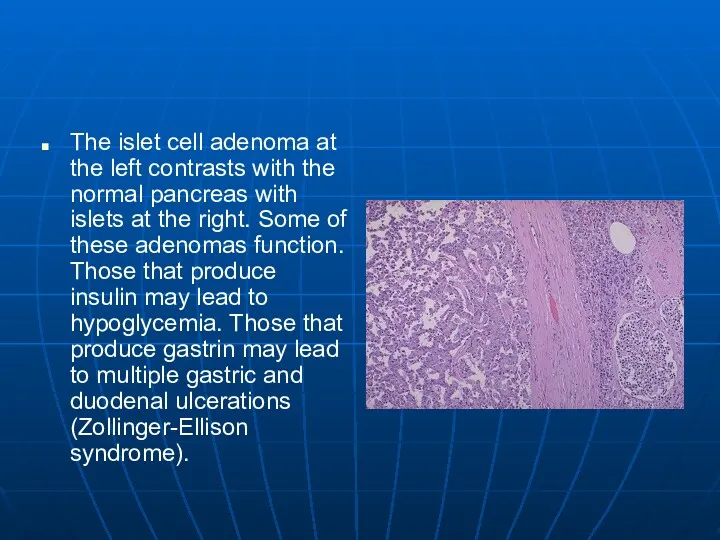
- 139. The islet cell adenoma at the left contrasts with the normal pancreas with islets at the
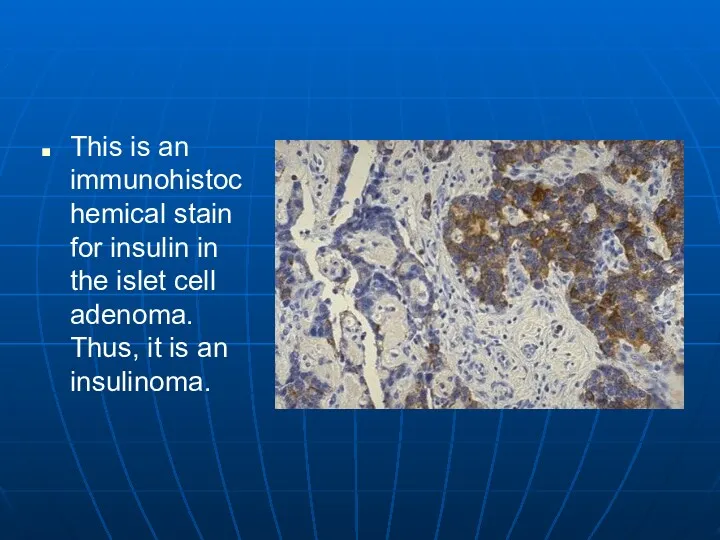
- 140. This is an immunohistochemical stain for insulin in the islet cell adenoma. Thus, it is an
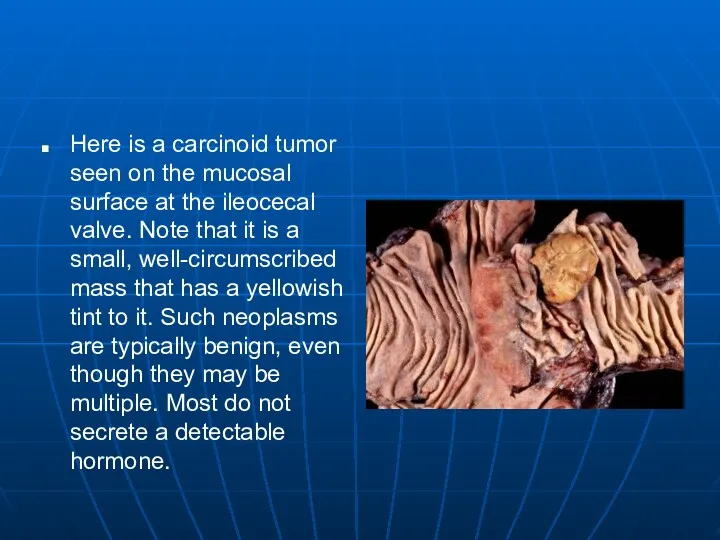
- 141. Here is a carcinoid tumor seen on the mucosal surface at the ileocecal valve. Note that
- 142. At low magnification, the small blue nests of tumor cells in this carcinoid tumor are grouped
- 143. At high magnification, the small nests of tumor cells in this carcinoid contain round cells with
- 144. This immunoperoxidase stain with antibody to ACTH demonstrates staining of the cells in this carcinoid tumor.
- 145. At higher power, the immunoperoxidase staining pattern with antibody to ACTH is shown in this carcinoid
- 147. Скачать презентацию
Endocrine Pathology
Cell signaling system
Surface receptors
cAMP and tyrosine kinase system
Cytoplasmic receptors
Penetrate cell
Endocrine Pathology
Cell signaling system
Surface receptors
cAMP and tyrosine kinase system
Cytoplasmic receptors
Penetrate cell
Endocrine Pathology
Too much hormone activity
Too little hormone activity
Autoimmune destruction
Inflammatory destruction
Tumor or
Endocrine Pathology
Too much hormone activity
Too little hormone activity
Autoimmune destruction
Inflammatory destruction
Tumor or
The Basics
Anterior
Comes from GI
Controlled by hypothalmus
Posterior
Hormones orginate further up.
The Basics
Anterior
Comes from GI
Controlled by hypothalmus
Posterior
Hormones orginate further up.
Pituitary Vascular
Signaling proteins are release in hypothalmus.
Travel by blood to anterior
Pituitary Vascular
Signaling proteins are release in hypothalmus.
Travel by blood to anterior
Pituitary Control
Pituitary Control
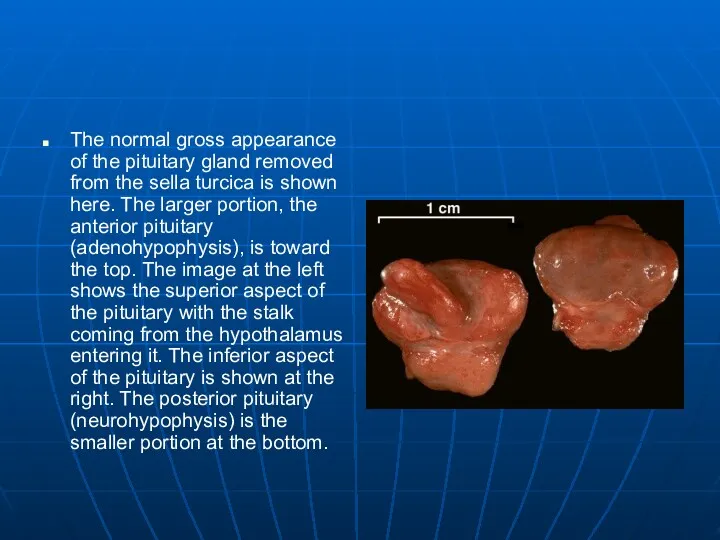
The normal gross appearance of the pituitary gland removed from the
The normal gross appearance of the pituitary gland removed from the
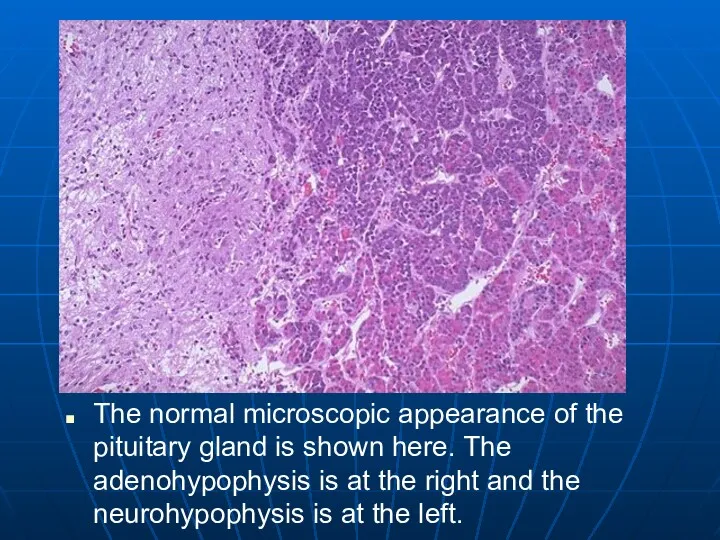
The normal microscopic appearance of the pituitary gland is shown here.
The normal microscopic appearance of the pituitary gland is shown here.
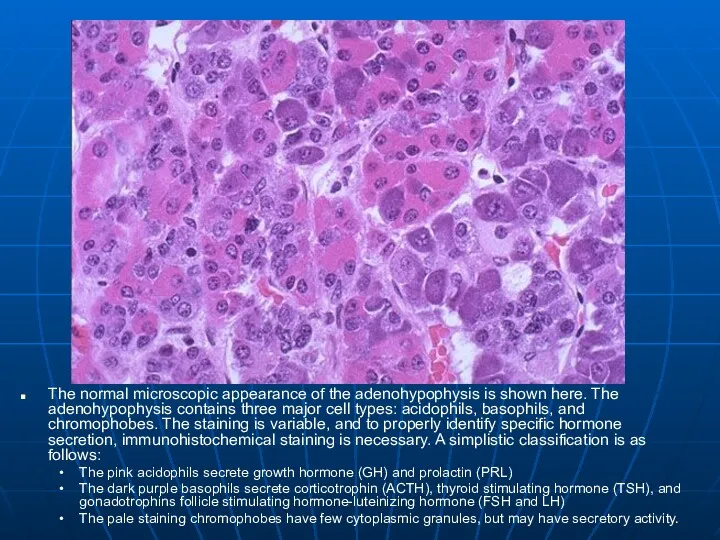
The normal microscopic appearance of the adenohypophysis is shown here. The
The normal microscopic appearance of the adenohypophysis is shown here. The
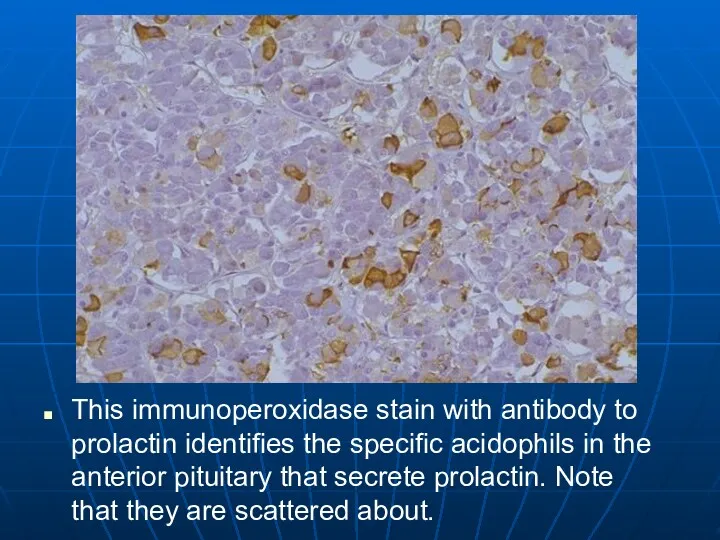
This immunoperoxidase stain with antibody to prolactin identifies the specific acidophils
This immunoperoxidase stain with antibody to prolactin identifies the specific acidophils
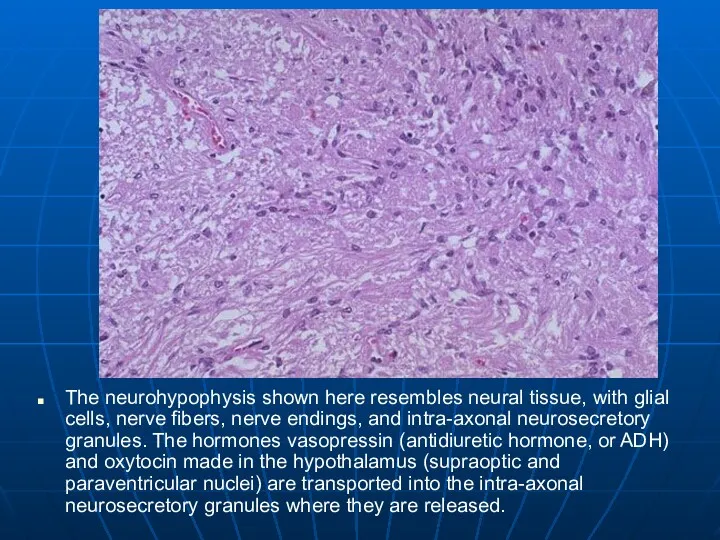
The neurohypophysis shown here resembles neural tissue, with glial cells, nerve
The neurohypophysis shown here resembles neural tissue, with glial cells, nerve
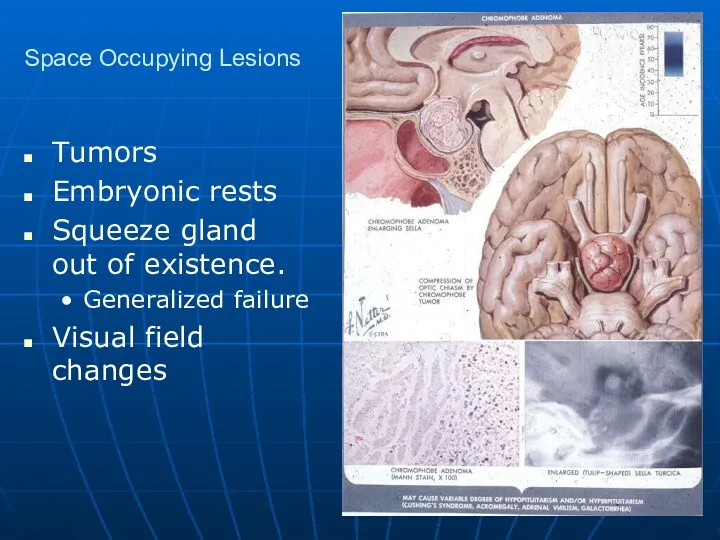
Space Occupying Lesions
Tumors
Embryonic rests
Squeeze gland out of existence.
Generalized failure
Visual field changes
Space Occupying Lesions
Tumors
Embryonic rests
Squeeze gland out of existence.
Generalized failure
Visual field changes
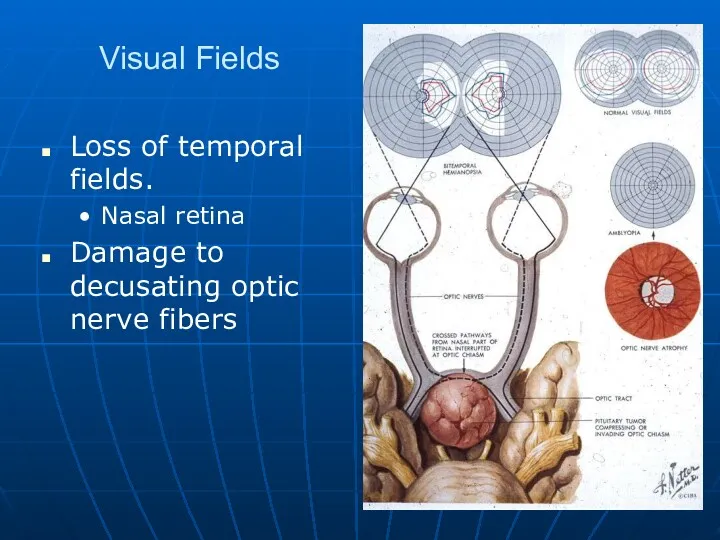
Visual Fields
Loss of temporal fields.
Nasal retina
Damage to decusating optic nerve fibers
Visual Fields
Loss of temporal fields.
Nasal retina
Damage to decusating optic nerve fibers
Pituitary Adenomas
Rare
Make nothing or
Prolactin
ACTH, GH,TSH are very rare
More often end up
Pituitary Adenomas
Rare
Make nothing or
Prolactin
ACTH, GH,TSH are very rare
More often end up
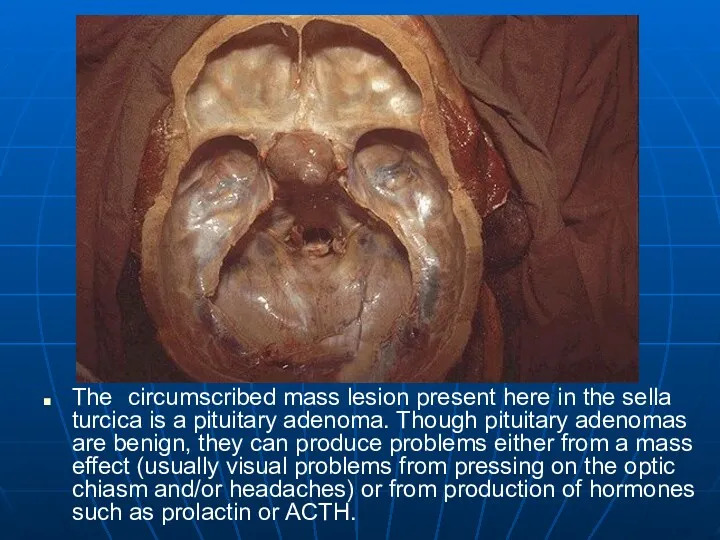
The circumscribed mass lesion present here in the sella turcica is
The circumscribed mass lesion present here in the sella turcica is
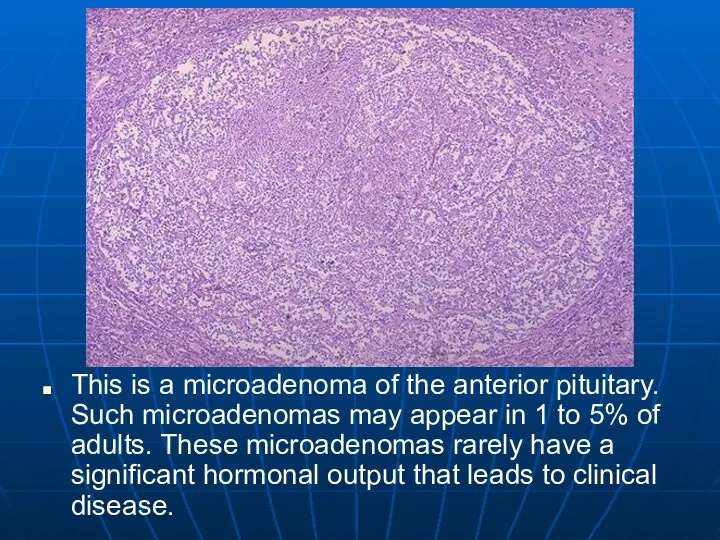
This is a microadenoma of the anterior pituitary. Such microadenomas may
This is a microadenoma of the anterior pituitary. Such microadenomas may
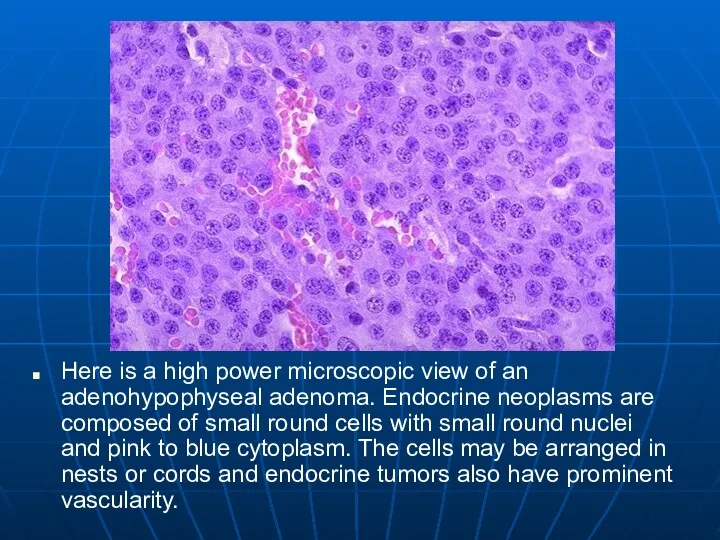
Here is a high power microscopic view of an adenohypophyseal adenoma.
Here is a high power microscopic view of an adenohypophyseal adenoma.
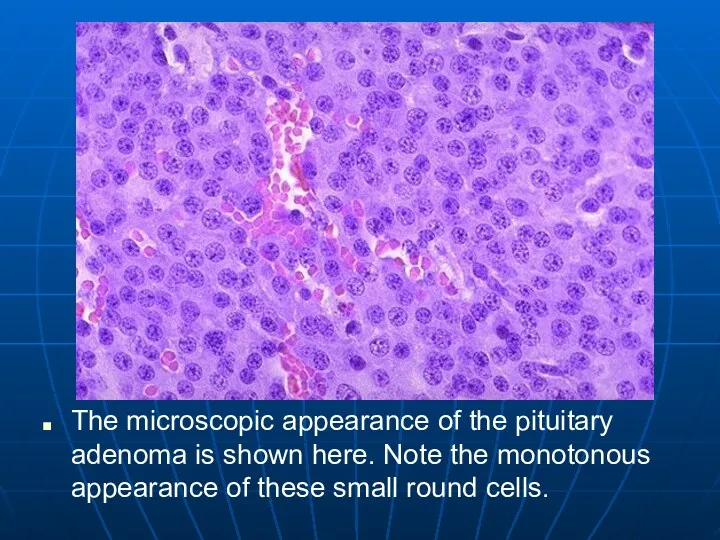
The microscopic appearance of the pituitary adenoma is shown here. Note
The microscopic appearance of the pituitary adenoma is shown here. Note
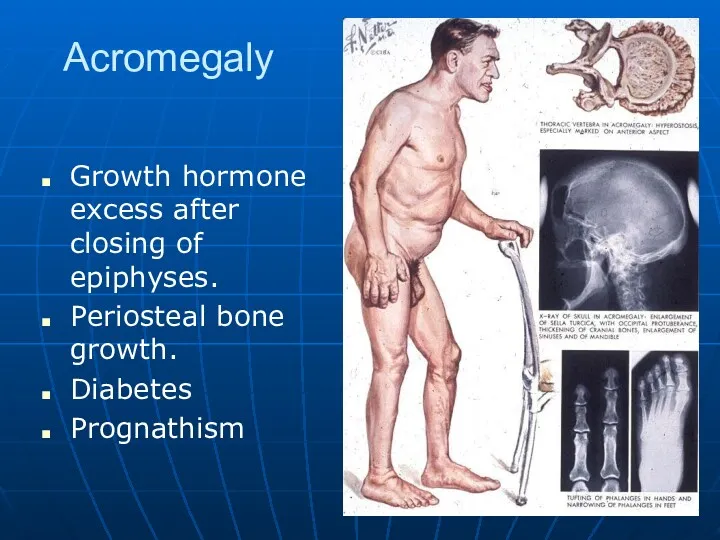
Acromegaly
Growth hormone excess after closing of epiphyses.
Periosteal bone growth.
Diabetes
Prognathism
Acromegaly
Growth hormone excess after closing of epiphyses.
Periosteal bone growth.
Diabetes
Prognathism
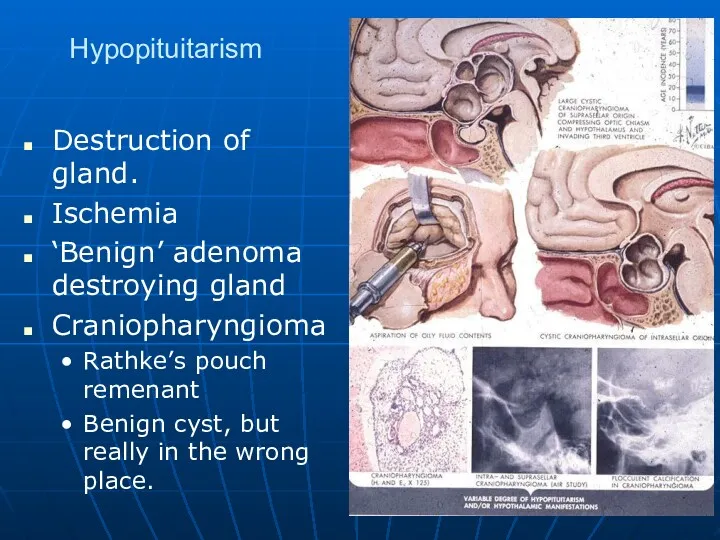
Hypopituitarism
Destruction of gland.
Ischemia
‘Benign’ adenoma destroying gland
Craniopharyngioma
Rathke’s pouch remenant
Benign cyst, but really
Hypopituitarism
Destruction of gland.
Ischemia
‘Benign’ adenoma destroying gland
Craniopharyngioma
Rathke’s pouch remenant
Benign cyst, but really
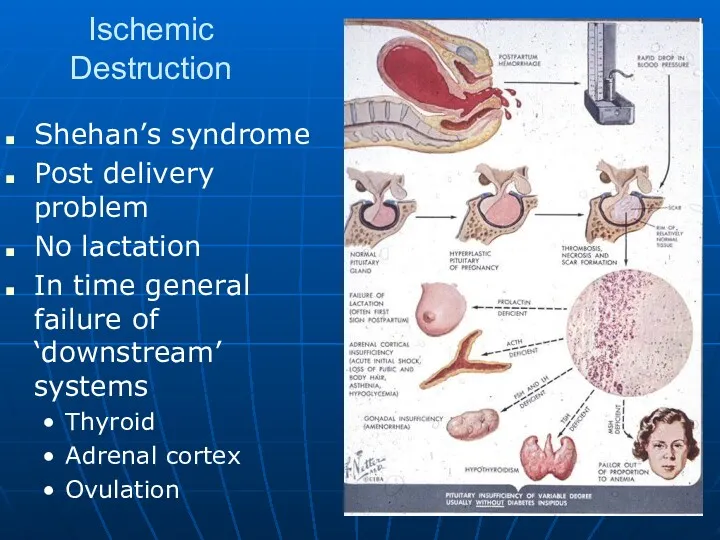
Ischemic Destruction
Shehan’s syndrome
Post delivery problem
No lactation
In time general failure of ‘downstream’
Ischemic Destruction
Shehan’s syndrome
Post delivery problem
No lactation
In time general failure of ‘downstream’
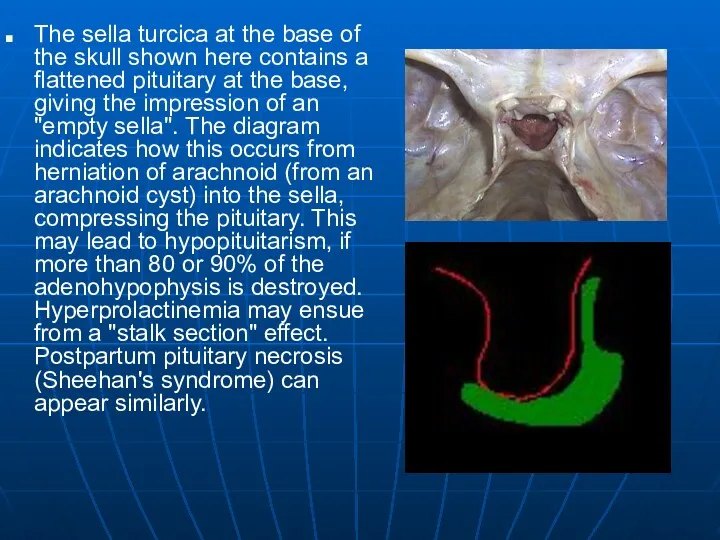
The sella turcica at the base of the skull shown here
The sella turcica at the base of the skull shown here
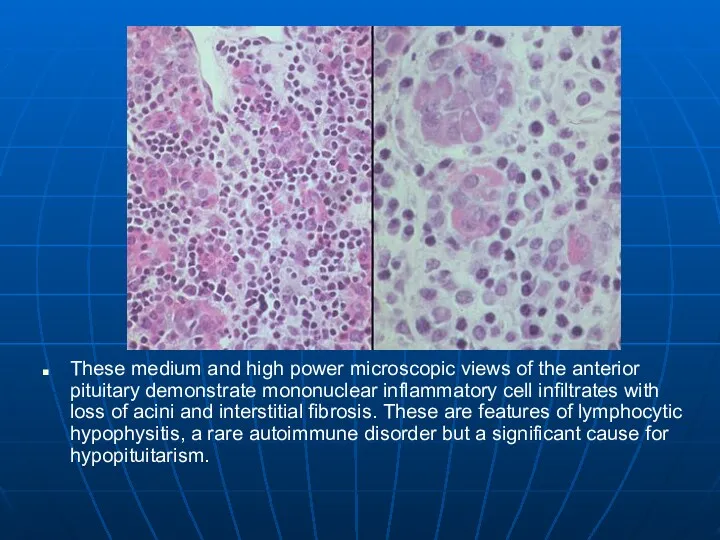
These medium and high power microscopic views of the anterior pituitary
These medium and high power microscopic views of the anterior pituitary
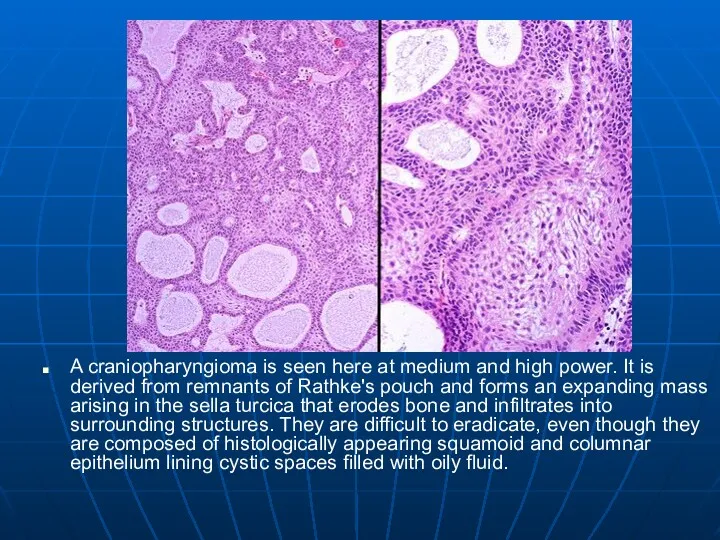
A craniopharyngioma is seen here at medium and high power. It
A craniopharyngioma is seen here at medium and high power. It
Posterior Pituitary
Loss of ADH
Diabetes insipidis
Dose not make concentrated urine
Large volumes of
Posterior Pituitary
Loss of ADH
Diabetes insipidis
Dose not make concentrated urine
Large volumes of
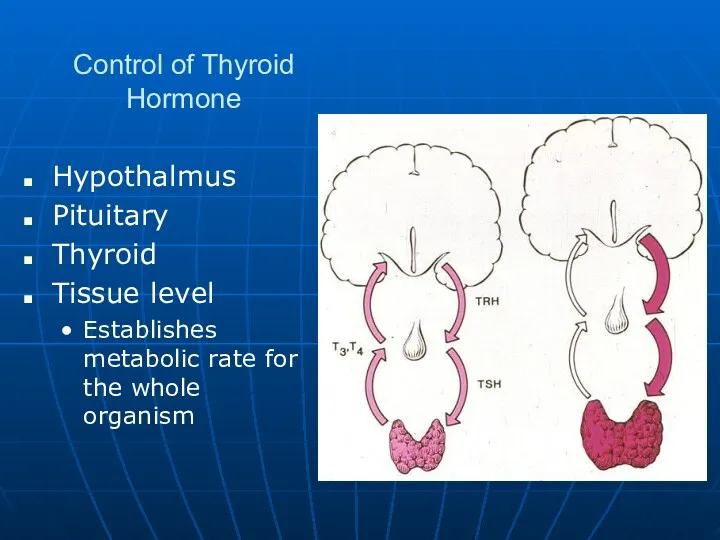
Control of Thyroid Hormone
Hypothalmus
Pituitary
Thyroid
Tissue level
Establishes metabolic rate for the whole organism
Control of Thyroid Hormone
Hypothalmus
Pituitary
Thyroid
Tissue level
Establishes metabolic rate for the whole organism
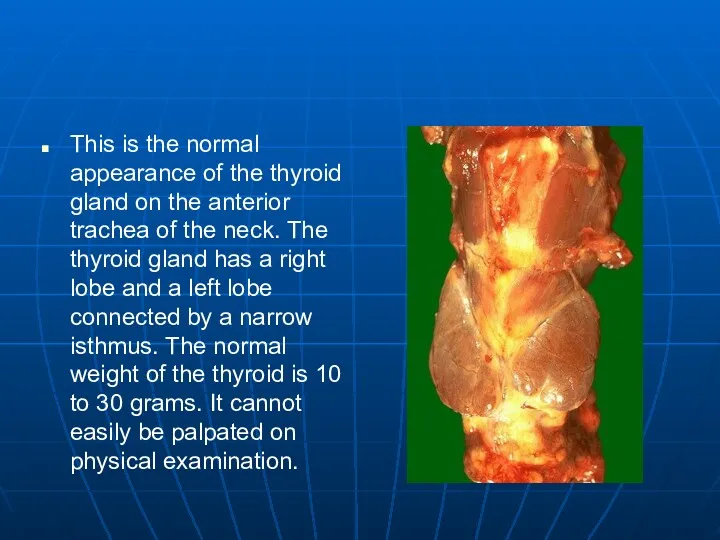
This is the normal appearance of the thyroid gland on the
This is the normal appearance of the thyroid gland on the
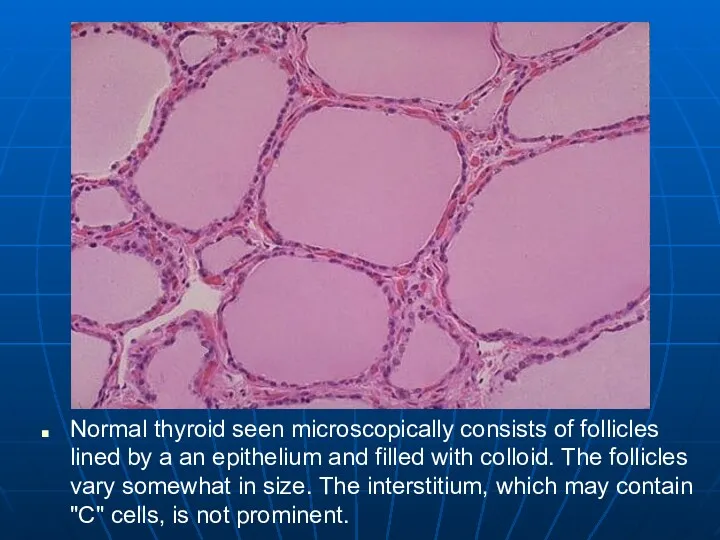
Normal thyroid seen microscopically consists of follicles lined by a an
Normal thyroid seen microscopically consists of follicles lined by a an
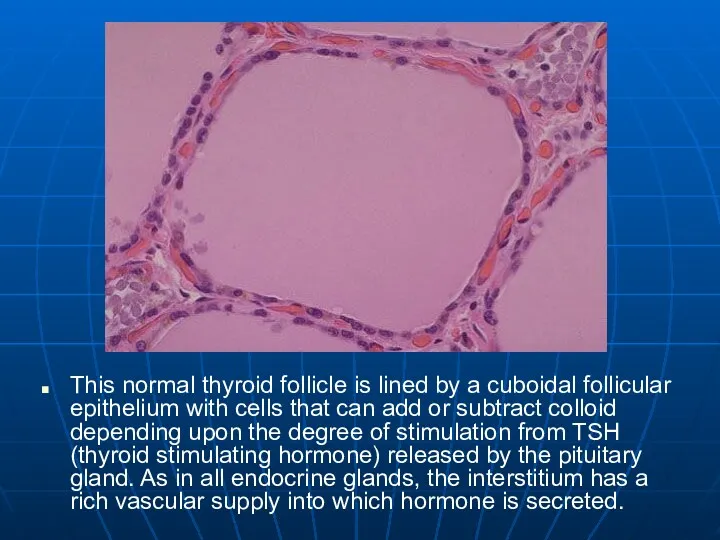
This normal thyroid follicle is lined by a cuboidal follicular epithelium
This normal thyroid follicle is lined by a cuboidal follicular epithelium
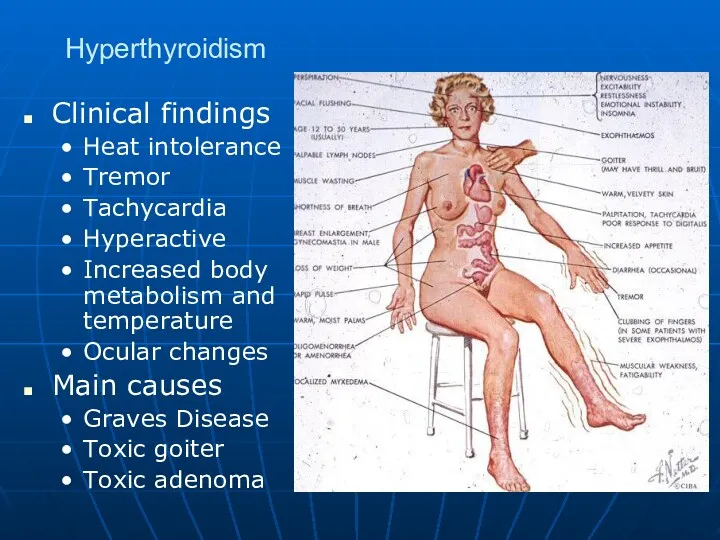
Hyperthyroidism
Clinical findings
Heat intolerance
Tremor
Tachycardia
Hyperactive
Increased body metabolism and temperature
Ocular changes
Main causes
Graves Disease
Toxic goiter
Toxic
Hyperthyroidism
Clinical findings
Heat intolerance
Tremor
Tachycardia
Hyperactive
Increased body metabolism and temperature
Ocular changes
Main causes
Graves Disease
Toxic goiter
Toxic
Grave’s disease
Grave’s disease is multi-organ systemic autoimmune disorder, manifested by the
Grave’s disease
Grave’s disease is multi-organ systemic autoimmune disorder, manifested by the
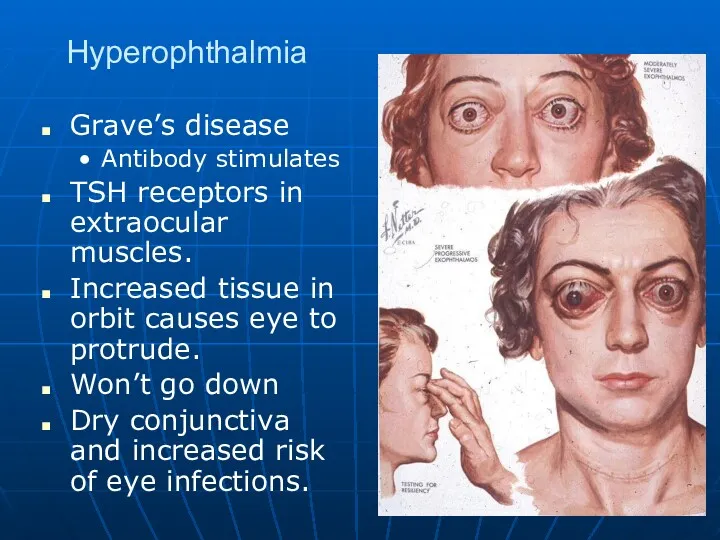
Hyperophthalmia
Grave’s disease
Antibody stimulates
TSH receptors in extraocular muscles.
Increased tissue in orbit causes
Hyperophthalmia
Grave’s disease
Antibody stimulates
TSH receptors in extraocular muscles.
Increased tissue in orbit causes
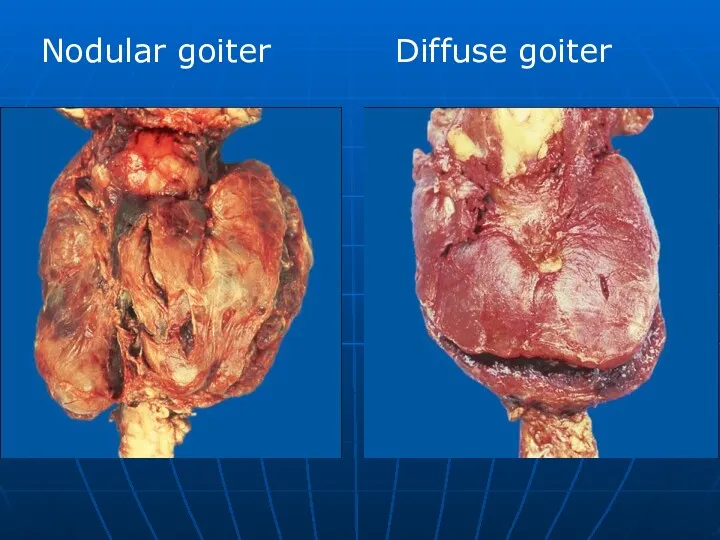
Nodular goiter
Diffuse goiter
Nodular goiter
Diffuse goiter
Hyperthyroidism
Hyperthyroidism
A diffusely enlarged thyroid gland associated with hyperthyroidism is known as
A diffusely enlarged thyroid gland associated with hyperthyroidism is known as
At high power, the tall columnar thyroid epithelium with Grave's disease
At high power, the tall columnar thyroid epithelium with Grave's disease
Tumors and Changes in Size
Tumors and Changes in Size
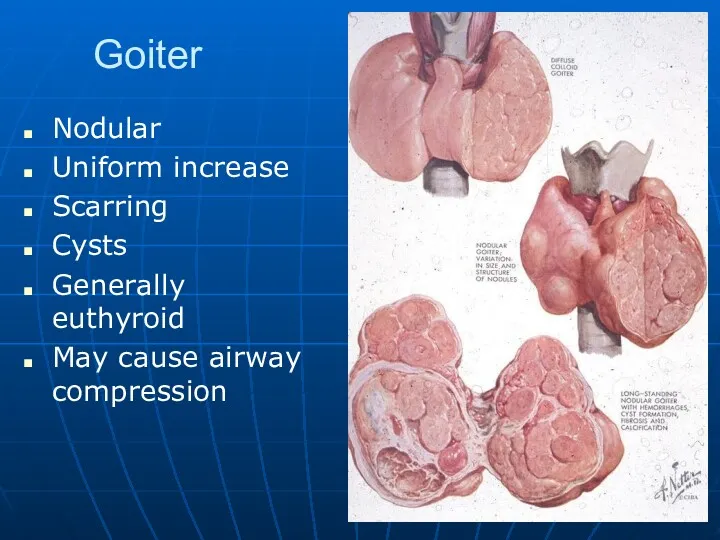
Goiter
Nodular
Uniform increase
Scarring
Cysts
Generally euthyroid
May cause airway compression
Goiter
Nodular
Uniform increase
Scarring
Cysts
Generally euthyroid
May cause airway compression
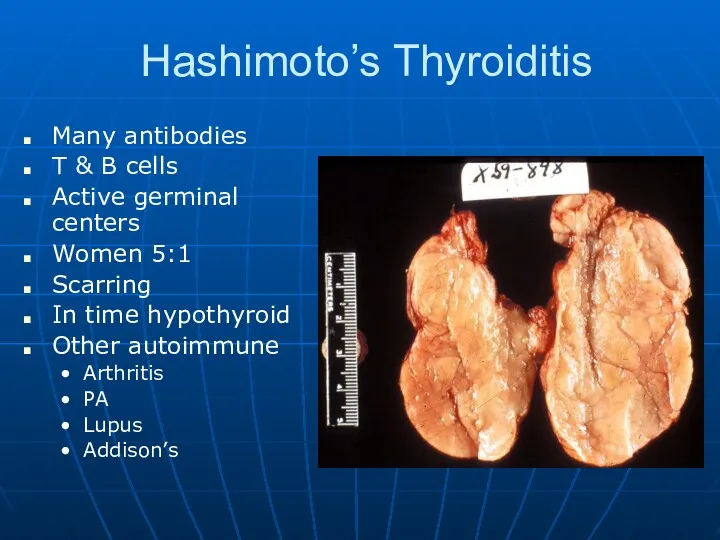
Hashimoto’s Thyroiditis
Many antibodies
T & B cells
Active germinal centers
Women 5:1
Scarring
In
Hashimoto’s Thyroiditis
Many antibodies
T & B cells
Active germinal centers
Women 5:1
Scarring
In
Hashimoto’s Thryoiditis
Hashimoto’s Thryoiditis
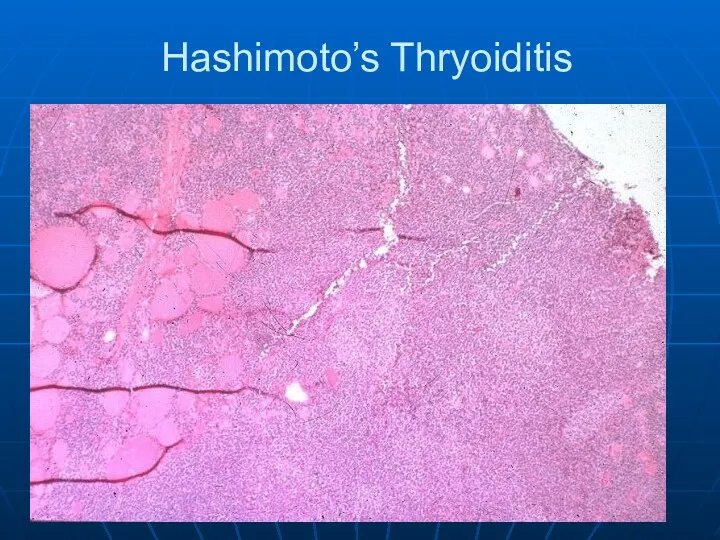
Here is a low power microscopic view of a thyroid with
Here is a low power microscopic view of a thyroid with
This high power microscopic view of the thyroid with Hashimoto's thyroiditis
This high power microscopic view of the thyroid with Hashimoto's thyroiditis
This is an example of an immunofluorescence test positive for anti-microsomal
This is an example of an immunofluorescence test positive for anti-microsomal
Here is an example of immunofluorescence positivity for anti-thyroglobulin antibody. Patients
Here is an example of immunofluorescence positivity for anti-thyroglobulin antibody. Patients
De Quervain’s Thyroiditis
Subacute
Giant cells
Granulomas
Viral?
Painful neck
De Quervain’s Thyroiditis
Subacute
Giant cells
Granulomas
Viral?
Painful neck
This is subacute granulomatous thyroiditis (DeQuervain's disease), which probably follows a
This is subacute granulomatous thyroiditis (DeQuervain's disease), which probably follows a
This thyroid gland is about normal in size, but there is
This thyroid gland is about normal in size, but there is
This diffusely enlarged thyroid gland is somewhat nodular. This patient was
This diffusely enlarged thyroid gland is somewhat nodular. This patient was
The follicles are irregularly enlarged, with flattened epithelium, consistent with inactivity,
The follicles are irregularly enlarged, with flattened epithelium, consistent with inactivity,
Hypothyroidism
Genetics
Gland destruction
Inflammatory
Surgical removal
Radiation treatment for hyperthyroidism
Iodine deficiency
Can’t make T4
Hypothalmic and/or pituitary
Hypothyroidism
Genetics
Gland destruction
Inflammatory
Surgical removal
Radiation treatment for hyperthyroidism
Iodine deficiency
Can’t make T4
Hypothalmic and/or pituitary
Hypothyroidism
Genetics: Cretinism
Cannot make T4
Growth retarded
Severe mental retardation
Must recognize early
Hypothyroidism
Genetics: Cretinism
Cannot make T4
Growth retarded
Severe mental retardation
Must recognize early
Hypothyroidism
Clinical
Cold intolerance
Bradycardia
Heart failure
High lipids
Lethargic
Photophobia
Myxedema
Skin and hair changes
Hypothyroidism
Clinical
Cold intolerance
Bradycardia
Heart failure
High lipids
Lethargic
Photophobia
Myxedema
Skin and hair changes
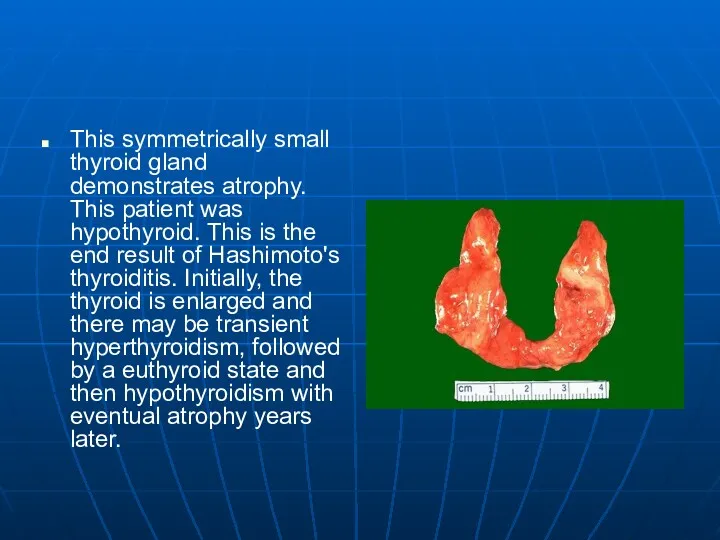
This symmetrically small thyroid gland demonstrates atrophy. This patient was hypothyroid.
This symmetrically small thyroid gland demonstrates atrophy. This patient was hypothyroid.
Thyroid Adenomas
Benign
Solitary
Common
Encapsulated
Generally not hyperactive
Thyroid Adenomas
Benign
Solitary
Common
Encapsulated
Generally not hyperactive
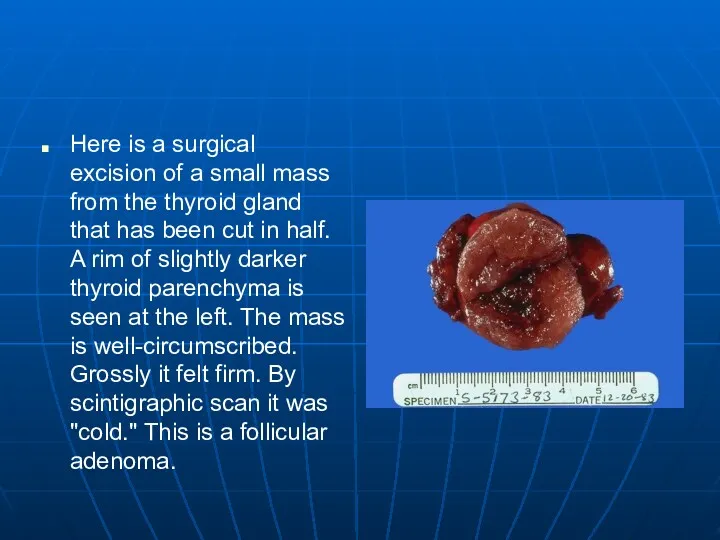
Here is a surgical excision of a small mass from the
Here is a surgical excision of a small mass from the
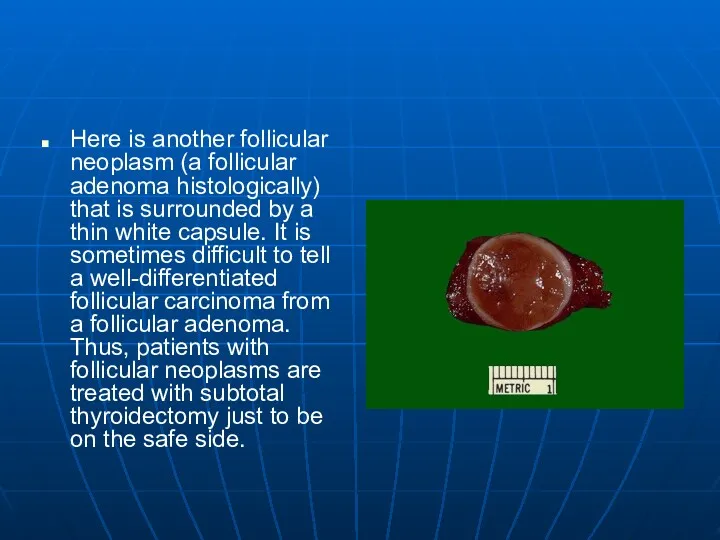
Here is another follicular neoplasm (a follicular adenoma histologically) that is
Here is another follicular neoplasm (a follicular adenoma histologically) that is
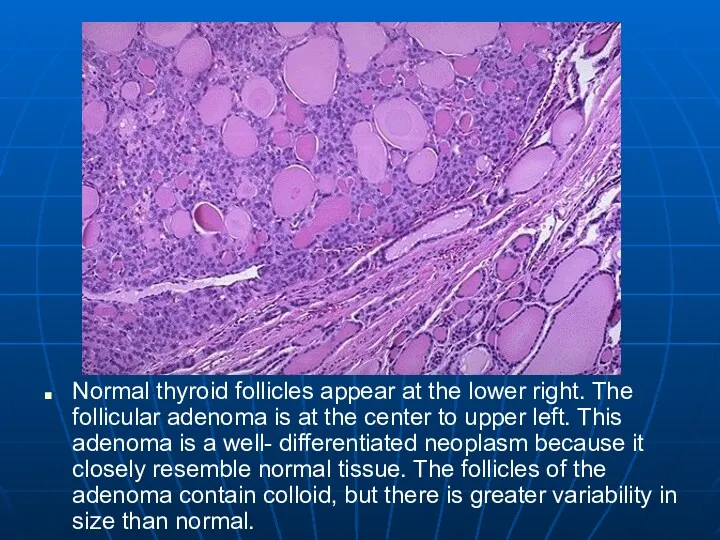
Normal thyroid follicles appear at the lower right. The follicular adenoma
Normal thyroid follicles appear at the lower right. The follicular adenoma
Malignancies of Thyroid Origin
Arising from follicular cells
Papillary Carcinoma
Follicular Carcinoma
Mixed pattern
Interstitial cells
Malignancies of Thyroid Origin
Arising from follicular cells
Papillary Carcinoma
Follicular Carcinoma
Mixed pattern
Interstitial cells
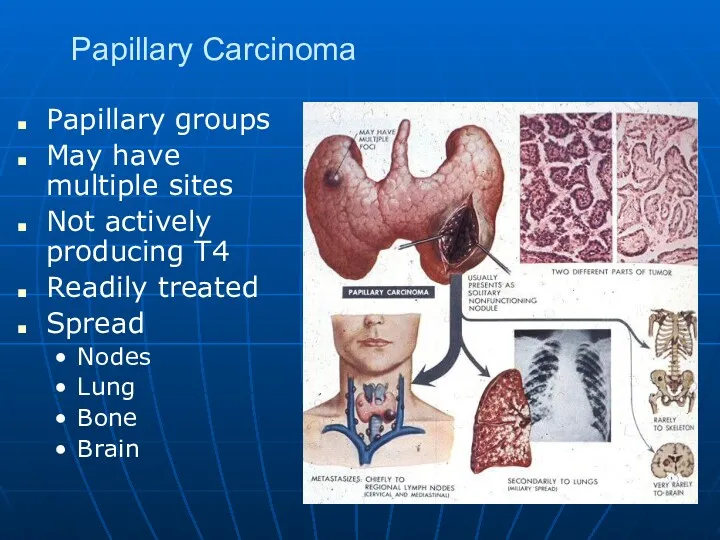
Papillary Carcinoma
Papillary groups
May have multiple sites
Not actively producing T4
Readily treated
Spread
Nodes
Lung
Bone
Brain
Papillary Carcinoma
Papillary groups
May have multiple sites
Not actively producing T4
Readily treated
Spread
Nodes
Lung
Bone
Brain
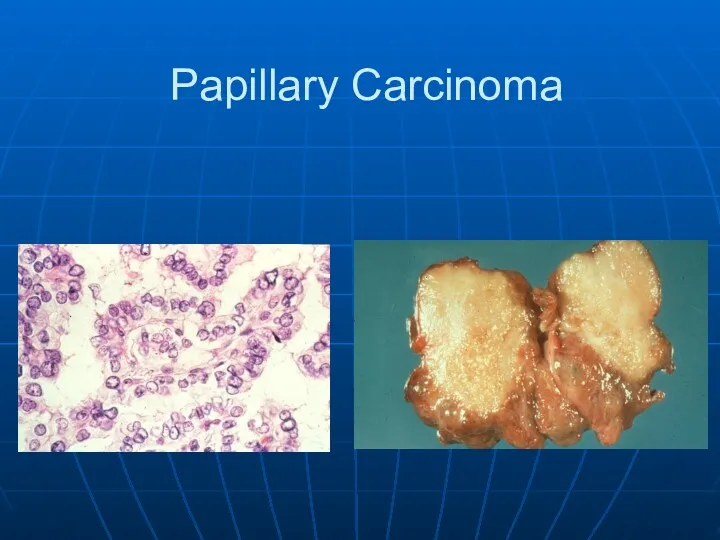
Papillary Carcinoma
Papillary Carcinoma
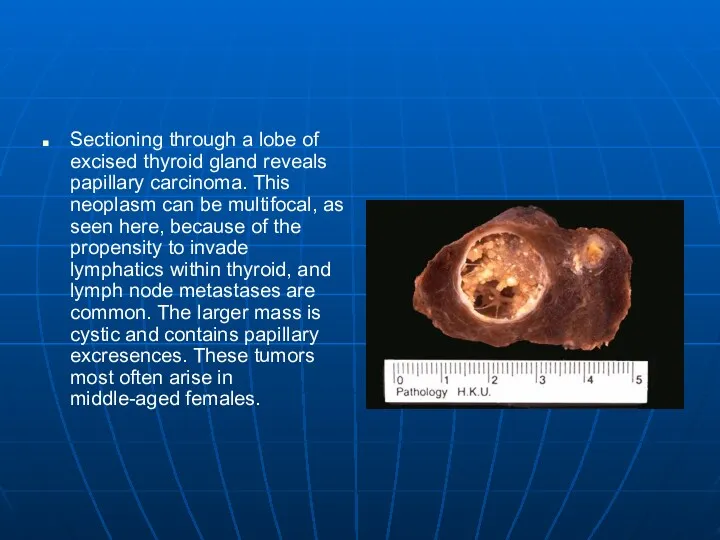
Sectioning through a lobe of excised thyroid gland reveals papillary carcinoma.
Sectioning through a lobe of excised thyroid gland reveals papillary carcinoma.
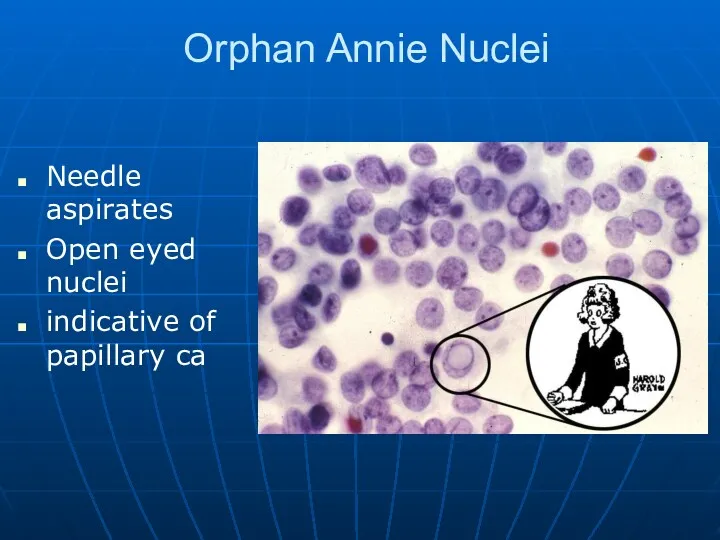
Orphan Annie Nuclei
Needle aspirates
Open eyed nuclei
indicative of papillary ca
Orphan Annie Nuclei
Needle aspirates
Open eyed nuclei
indicative of papillary ca
This is the microscopic appearance of a papillary carcinoma of the
This is the microscopic appearance of a papillary carcinoma of the
This is another papillary carcinoma of thyroid. Note the small psammoma
This is another papillary carcinoma of thyroid. Note the small psammoma
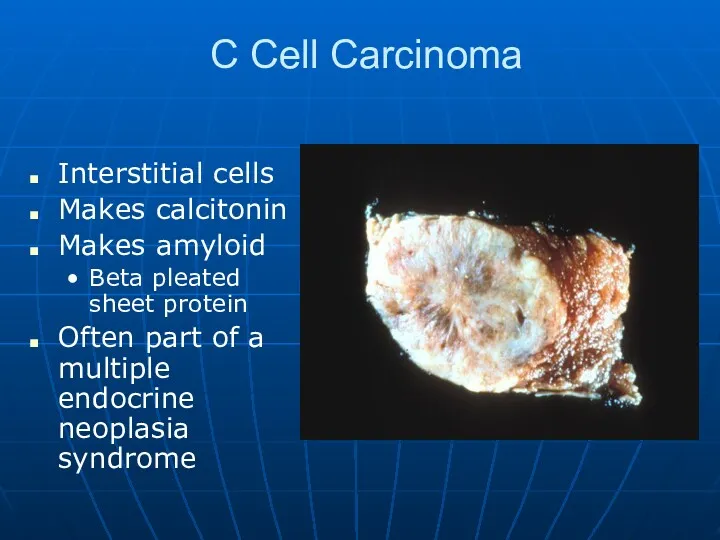
C Cell Carcinoma
Interstitial cells
Makes calcitonin
Makes amyloid
Beta pleated sheet protein
Often part of
C Cell Carcinoma
Interstitial cells
Makes calcitonin
Makes amyloid
Beta pleated sheet protein
Often part of
C Cell Carcinoma
C Cell Carcinoma

At the center and to the right is a medullary carcinoma
At the center and to the right is a medullary carcinoma
Here the amyloid stroma of the medullary thyroid carcinoma has been
Here the amyloid stroma of the medullary thyroid carcinoma has been
This is the Congo red stained amyloid stroma of the medullary
This is the Congo red stained amyloid stroma of the medullary
The anaplastic carcinoma shown here is invading into skeletal muscle fibers
The anaplastic carcinoma shown here is invading into skeletal muscle fibers
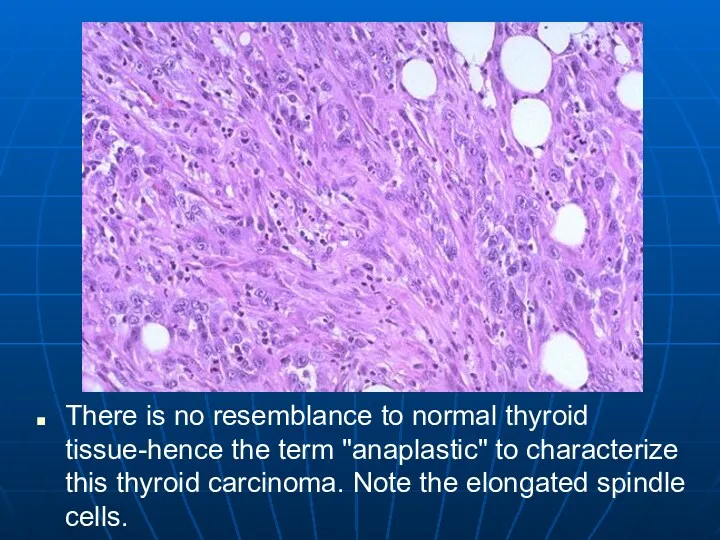
There is no resemblance to normal thyroid tissue-hence the term "anaplastic"
There is no resemblance to normal thyroid tissue-hence the term "anaplastic"
Parathyroid
Come from the pharyngeal pouches
Most of us have 4
Make PTH
Mobilizes calcium
Released
Parathyroid
Come from the pharyngeal pouches
Most of us have 4
Make PTH
Mobilizes calcium
Released
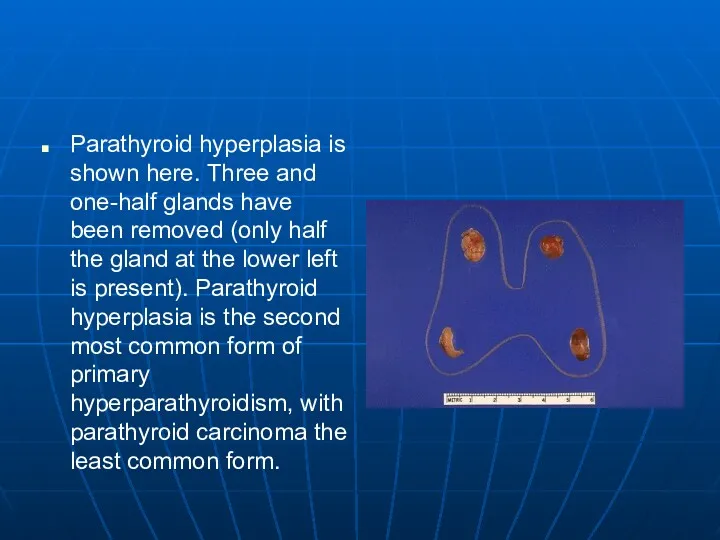
Parathyroid hyperplasia is shown here. Three and one-half glands have been
Parathyroid hyperplasia is shown here. Three and one-half glands have been
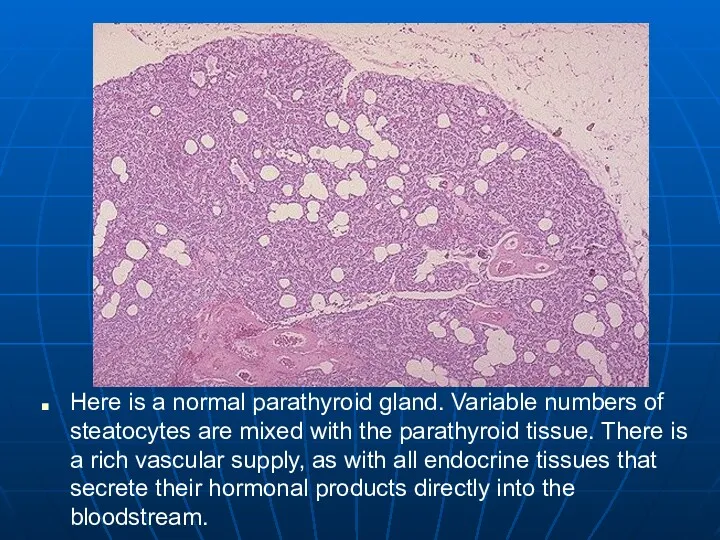
Here is a normal parathyroid gland. Variable numbers of steatocytes are
Here is a normal parathyroid gland. Variable numbers of steatocytes are
Hyperparathyroidism
Primary
Parathyroid adenoma 80%
Hyperplasia 10-15%
Parathyroid ca <5%
Hypercalcemia
Stones, bones, abdominal groans and psychic
Hyperparathyroidism
Primary
Parathyroid adenoma 80%
Hyperplasia 10-15%
Parathyroid ca <5%
Hypercalcemia
Stones, bones, abdominal groans and psychic
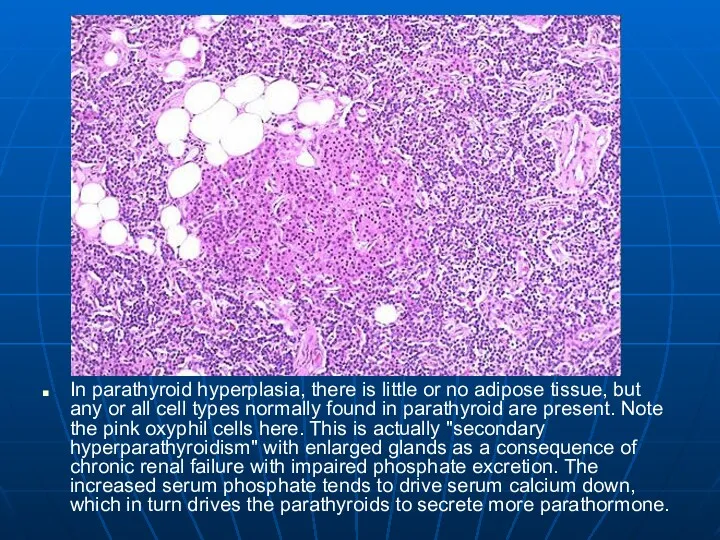
In parathyroid hyperplasia, there is little or no adipose tissue, but
In parathyroid hyperplasia, there is little or no adipose tissue, but
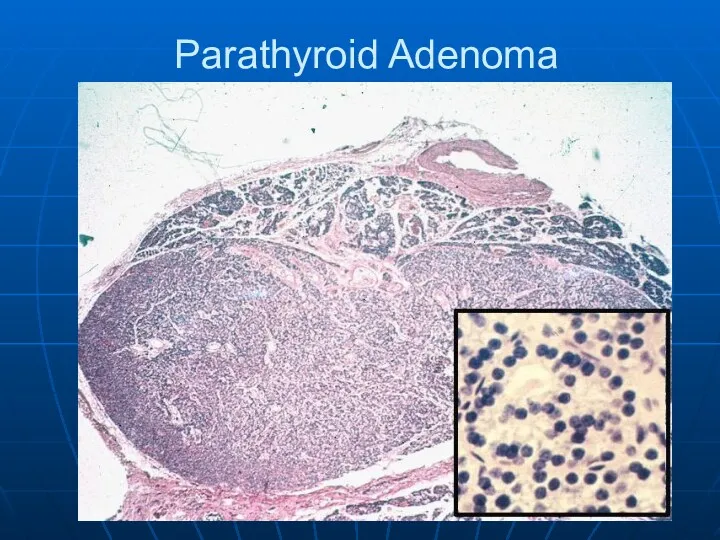
Parathyroid Adenoma
Parathyroid Adenoma
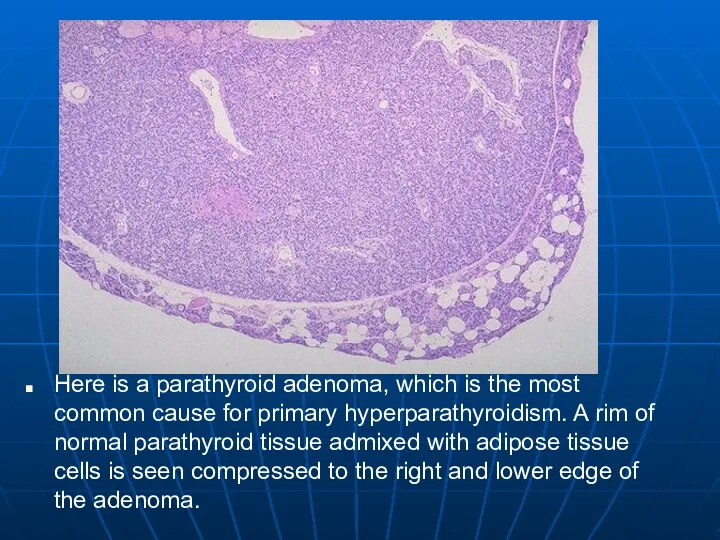
Here is a parathyroid adenoma, which is the most common cause
Here is a parathyroid adenoma, which is the most common cause
Secondary Hyperparathyroidism
Renal failure almost always
Phosphates build up in the blood.
Cause calcium
Secondary Hyperparathyroidism
Renal failure almost always
Phosphates build up in the blood.
Cause calcium
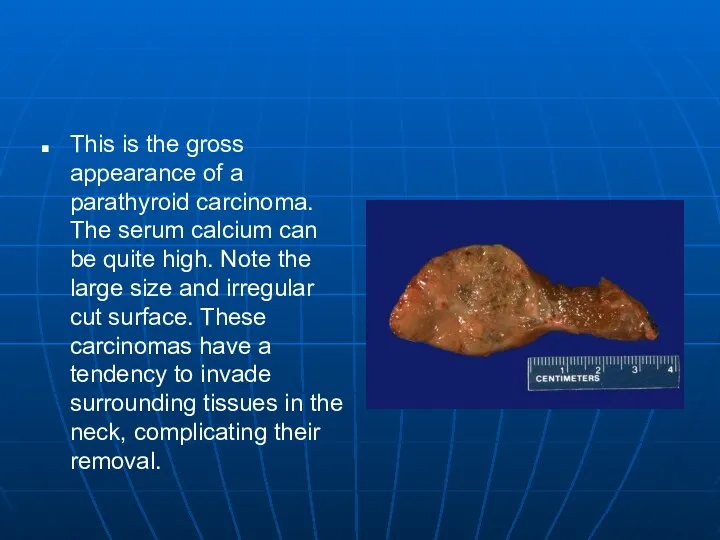
This is the gross appearance of a parathyroid carcinoma. The serum
This is the gross appearance of a parathyroid carcinoma. The serum
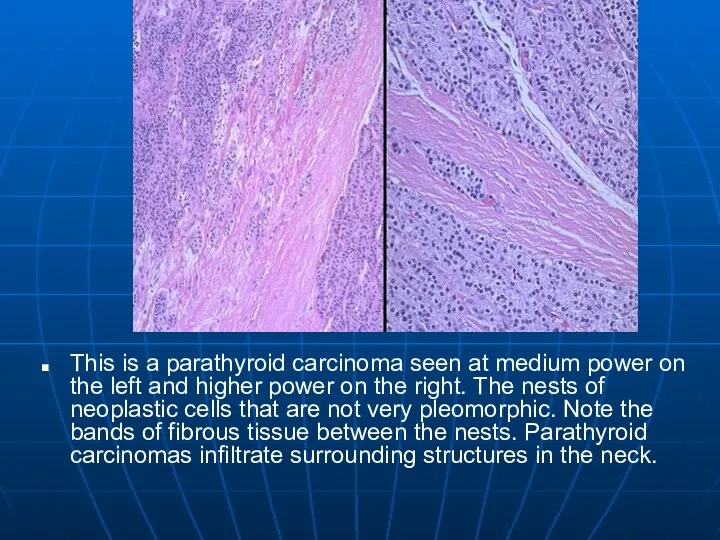
This is a parathyroid carcinoma seen at medium power on the
This is a parathyroid carcinoma seen at medium power on the
Hypoparathyroidism
Increased neuromuscular excitability
May lead to tetany
Irritability and possibly even psychosis
Parkinson-like symptoms
Cataracts
Causes
Autoimmune
Hypoparathyroidism
Increased neuromuscular excitability
May lead to tetany
Irritability and possibly even psychosis
Parkinson-like symptoms
Cataracts
Causes
Autoimmune
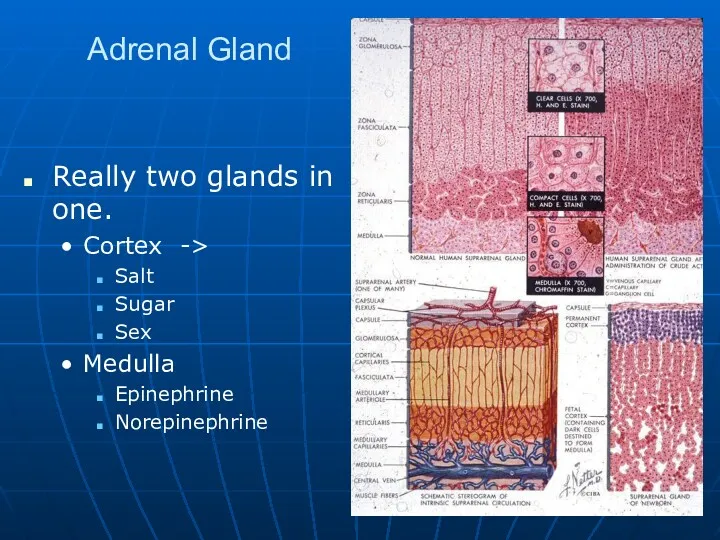
Adrenal Gland
Really two glands in one.
Cortex ->
Salt
Sugar
Sex
Medulla
Epinephrine
Norepinephrine
Adrenal Gland
Really two glands in one.
Cortex ->
Salt
Sugar
Sex
Medulla
Epinephrine
Norepinephrine
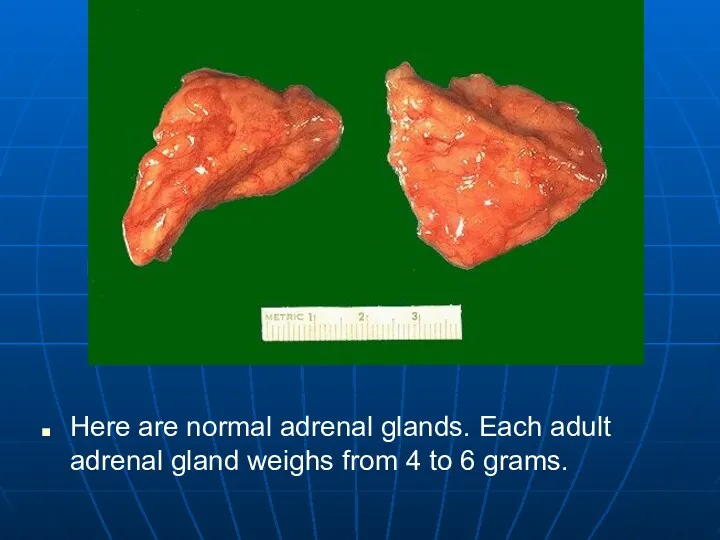
Here are normal adrenal glands. Each adult adrenal gland weighs from
Here are normal adrenal glands. Each adult adrenal gland weighs from
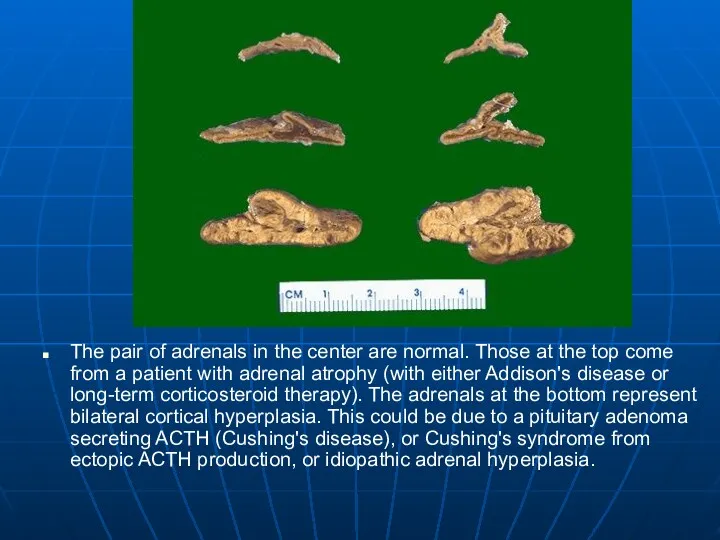
The pair of adrenals in the center are normal. Those at
The pair of adrenals in the center are normal. Those at
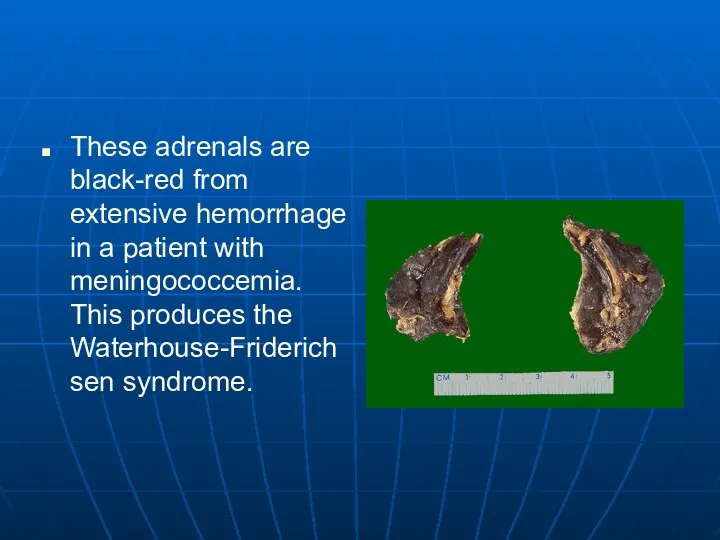
These adrenals are black-red from extensive hemorrhage in a patient with
These adrenals are black-red from extensive hemorrhage in a patient with
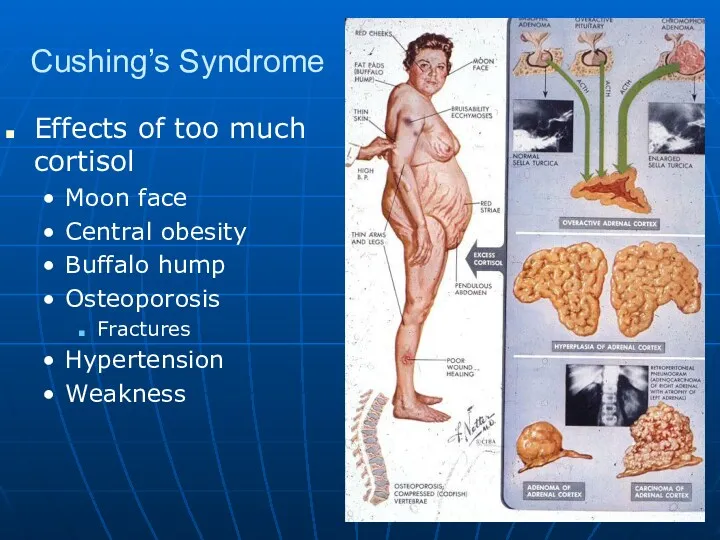
Cushing’s Syndrome
Effects of too much cortisol
Moon face
Central obesity
Buffalo hump
Osteoporosis
Fractures
Hypertension
Weakness
Cushing’s Syndrome
Effects of too much cortisol
Moon face
Central obesity
Buffalo hump
Osteoporosis
Fractures
Hypertension
Weakness
Cushing’s Disease
Altered feedback regulation at level of hypothalmus and pituitary
It only
Cushing’s Disease
Altered feedback regulation at level of hypothalmus and pituitary
It only
Cushing’s Disease
Cushing’s Disease
This adrenal gland removed surgically in a patient with Cushing's syndrome
This adrenal gland removed surgically in a patient with Cushing's syndrome
Microscopically, the adrenal cortical adenoma at the right resembles normal adrenal
Microscopically, the adrenal cortical adenoma at the right resembles normal adrenal
This high power microscopic appearance of an adrenal cortical carcinoma demonstrates
This high power microscopic appearance of an adrenal cortical carcinoma demonstrates
Hypoadrenalism
Acute loss vs. Chronic
Pituitary vs. adrenal
Acute
Waterhouse-Fridericshen syndrome ->
Overwhelming infection with encapsulated
Hypoadrenalism
Acute loss vs. Chronic
Pituitary vs. adrenal
Acute
Waterhouse-Fridericshen syndrome ->
Overwhelming infection with encapsulated

Waterhouse-Fridericshen syndrome
Waterhouse-Fridericshen syndrome
Waterhouse-Fridericshen syndrome
Waterhouse-Fridericshen syndrome
This is the microscopic appearance of the adrenals with meningococcemia. There
This is the microscopic appearance of the adrenals with meningococcemia. There
Addison’s Disease
Slowly develops
Loss of adrenal glands
Lots of ACTH, but nothing it
Addison’s Disease
Slowly develops
Loss of adrenal glands
Lots of ACTH, but nothing it
Adrenal Medulla
Pheochromocytoma
Catacholamines
Elevated blood pressure
Syncopal episodes
Headaches
Nose bleeds
Anxiety
Maybe an isolated tumor or part
Adrenal Medulla
Pheochromocytoma
Catacholamines
Elevated blood pressure
Syncopal episodes
Headaches
Nose bleeds
Anxiety
Maybe an isolated tumor or part
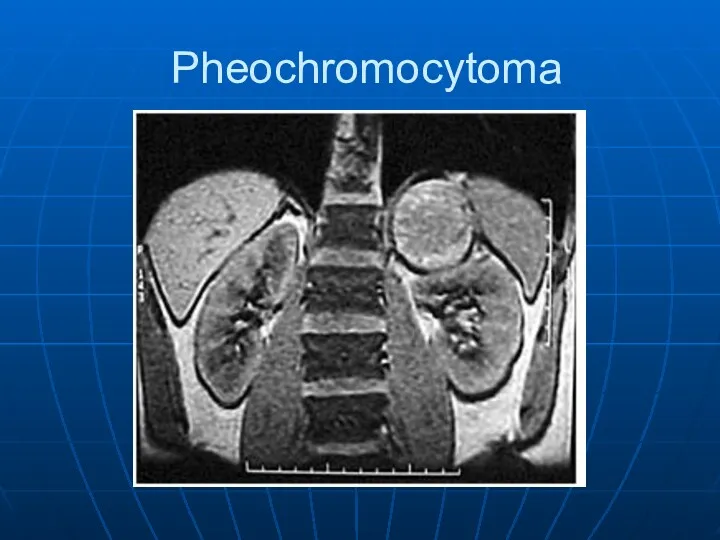
Pheochromocytoma
Pheochromocytoma
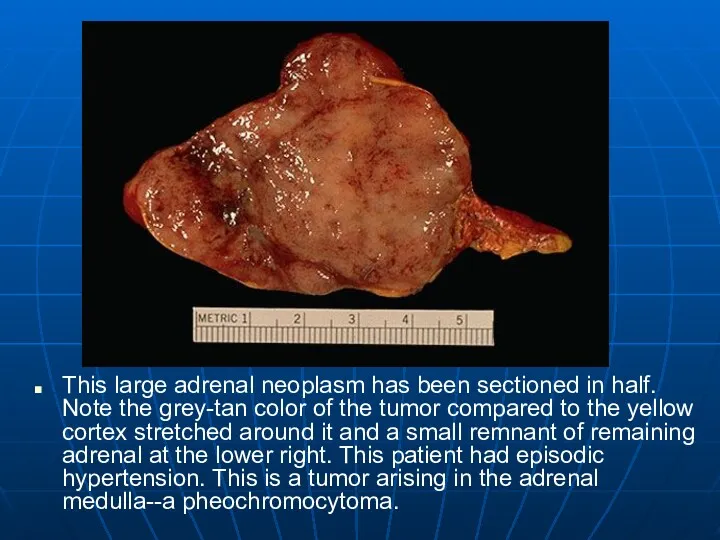
This large adrenal neoplasm has been sectioned in half. Note the
This large adrenal neoplasm has been sectioned in half. Note the
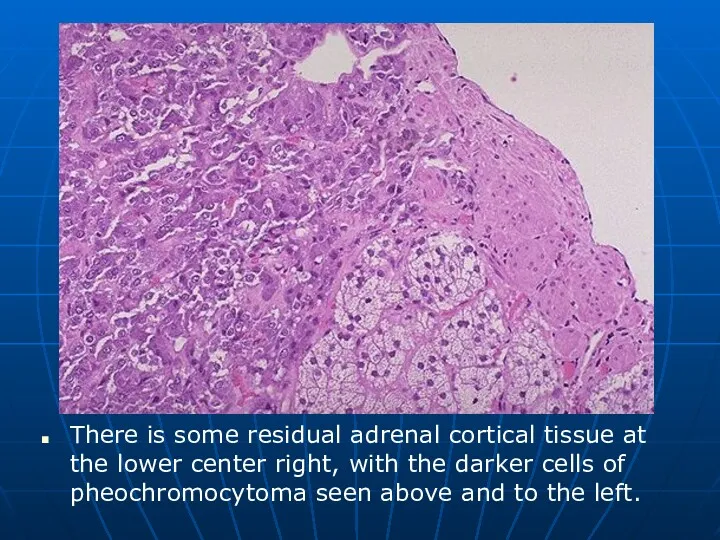
There is some residual adrenal cortical tissue at the lower center
There is some residual adrenal cortical tissue at the lower center
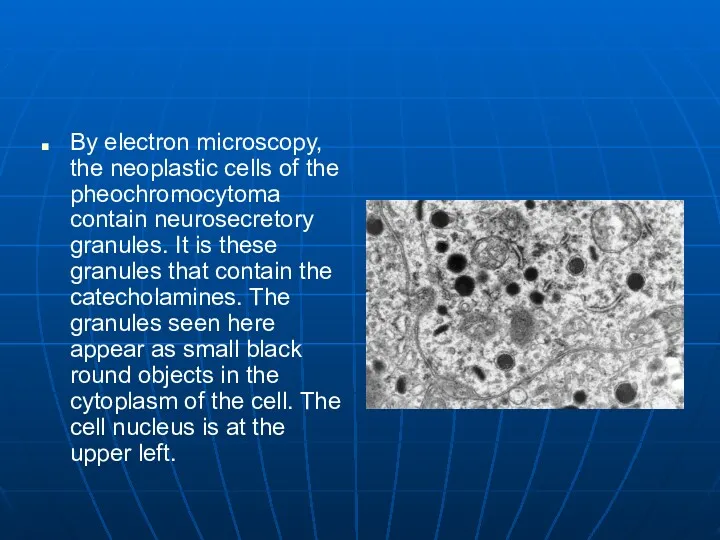
By electron microscopy, the neoplastic cells of the pheochromocytoma contain neurosecretory
By electron microscopy, the neoplastic cells of the pheochromocytoma contain neurosecretory
Diabetes mellitus
Diabetes mellitus
Diabetes Mellitus
General definition: Chronic disorder of glucose metabolism with hyperglycemia, triggered
Diabetes Mellitus
General definition: Chronic disorder of glucose metabolism with hyperglycemia, triggered
Diabetes Mellitus
Secondary diabetes mellitus: Insulin deficiency due to islet damage from
Diabetes Mellitus
Secondary diabetes mellitus: Insulin deficiency due to islet damage from
Diabetes Mellitus
Definition
Diabetes Mellitus
Definition
Diabetes Mellitus
Definition
Diabetes Mellitus
Definition
Here is a normal pancreatic islet of Langerhans surrounded by normal
Here is a normal pancreatic islet of Langerhans surrounded by normal
Immunoperoxidase staining can help identify the nature of the cells present
Immunoperoxidase staining can help identify the nature of the cells present
Type I Diabetes Mellitus
Synonyms: juvenile-onset diabetes mellitus, insulin-dependent diabetes mellitus (IDDM).
Autoimmune
Type I Diabetes Mellitus
Synonyms: juvenile-onset diabetes mellitus, insulin-dependent diabetes mellitus (IDDM).
Autoimmune
Type 1 Diabetes Mellitus
Progressive destruction of pancreatic β cells
Autoantibodies cause
Type 1 Diabetes Mellitus
Progressive destruction of pancreatic β cells
Autoantibodies cause
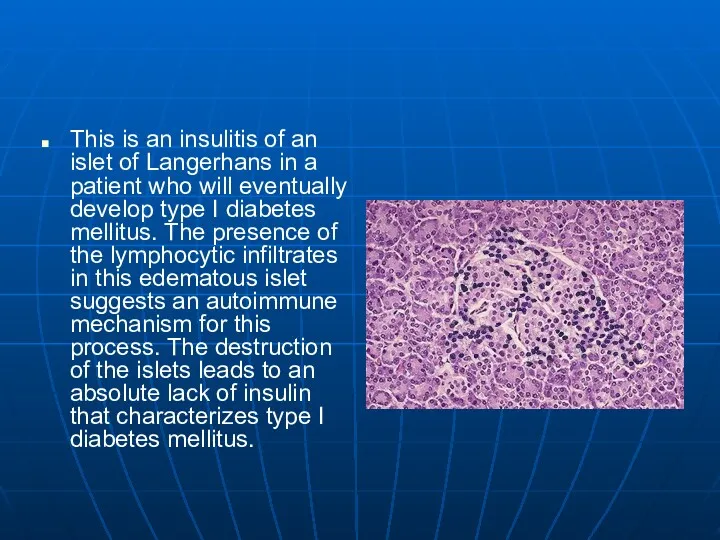
This is an insulitis of an islet of Langerhans in a
This is an insulitis of an islet of Langerhans in a
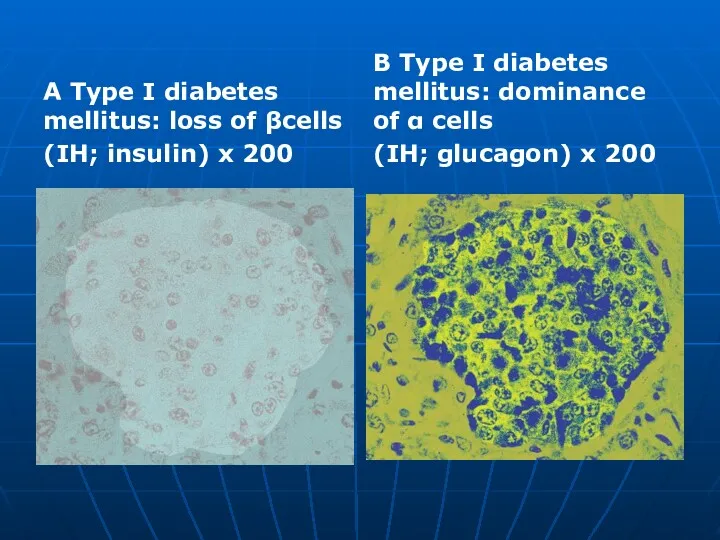
A Type I diabetes mellitus: loss of βcells
(IH; insulin) x 200
B
A Type I diabetes mellitus: loss of βcells
(IH; insulin) x 200
B
Diabetes Mellitus
Type II Diabetes Mellitus
Synonyms: adult-onset diabetes mellitus, non-insulindependent diabetes mellitus
Diabetes Mellitus
Type II Diabetes Mellitus
Synonyms: adult-onset diabetes mellitus, non-insulindependent diabetes mellitus
Type 2 Diabetes Mellitus
Accounts for 90% of patients with diabetes
Usually occurs
Type 2 Diabetes Mellitus
Accounts for 90% of patients with diabetes
Usually occurs
Pancreas continues to produce some endogenous insulin
Insulin produced is either insufficient
Pancreas continues to produce some endogenous insulin
Insulin produced is either insufficient
This islet of Langerhans demonstrates pink hyalinization (with deposition of amyloid)
This islet of Langerhans demonstrates pink hyalinization (with deposition of amyloid)
Islet amyloidosis
(HE) x 200
Type II diabetes mellitus: В cells
(IH; insulin) x
Islet amyloidosis
(HE) x 200
Type II diabetes mellitus: В cells
(IH; insulin) x
E Type II diabetes mellitus: alpha cells (IH; glucagon) x 200
E Type II diabetes mellitus: alpha cells (IH; glucagon) x 200
Secondary Diabetes
Results from another medical condition or due to the treatment
Secondary Diabetes
Results from another medical condition or due to the treatment
Diabetic macroangiopathy follows the pattern of atherosclerosis .
Complications:
– Coronary sclerosis can
Diabetic macroangiopathy follows the pattern of atherosclerosis .
Complications:
– Coronary sclerosis can

Diabetic gangrene
Diabetic gangrene

Diabetic microangiopathy: Chronic increased glucose concentration leads to glycosylation of proteins,
Diabetic microangiopathy: Chronic increased glucose concentration leads to glycosylation of proteins,
Diabetic cataract: Osmotic vacuolar degeneration of the epithelium of the lens
Diabetic cataract: Osmotic vacuolar degeneration of the epithelium of the lens
Gestational Diabetes
Develops during pregnancy
Detected at 24 to 28 weeks of
Gestational Diabetes
Develops during pregnancy
Detected at 24 to 28 weeks of
Diabetic retinopathy
Diabetic retinopathy
Diabetic retinopathy
Diabetic cataract
Diabetic retinopathy
Diabetic cataract
Diabetes mellitus
Diabetes mellitus
Diffuse glomerulosclerosis
Characterized by diffuse thickening of glomerular capillary basement membranes and
Diffuse glomerulosclerosis Characterized by diffuse thickening of glomerular capillary basement membranes and
Diabetic microangiopathy,
Diabetic neuropathy
Diabetic microangiopathy,
Diabetic neuropathy
An islet cell adenoma is seen here, separated from the pancreas
An islet cell adenoma is seen here, separated from the pancreas
The islet cell adenoma at the left contrasts with the normal
The islet cell adenoma at the left contrasts with the normal
This is an immunohistochemical stain for insulin in the islet cell
This is an immunohistochemical stain for insulin in the islet cell
Here is a carcinoid tumor seen on the mucosal surface at
Here is a carcinoid tumor seen on the mucosal surface at
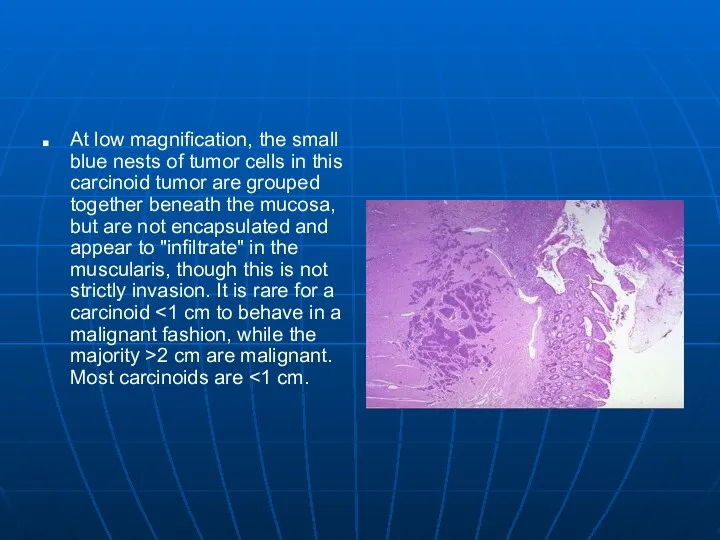
At low magnification, the small blue nests of tumor cells in
At low magnification, the small blue nests of tumor cells in
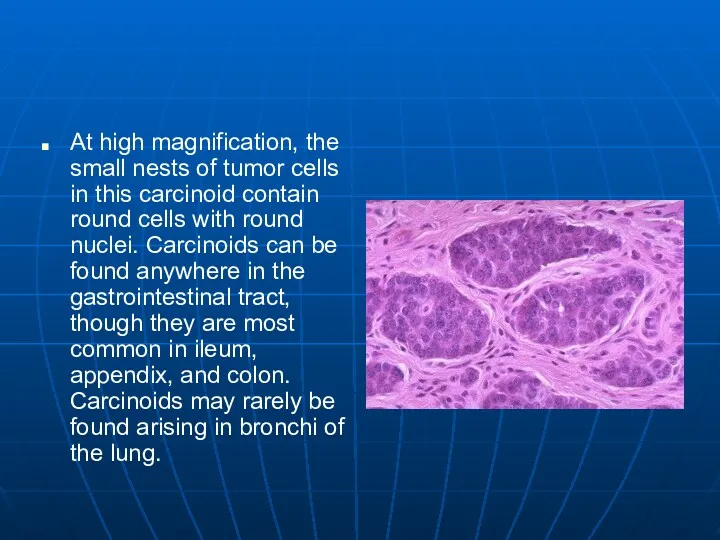
At high magnification, the small nests of tumor cells in this
At high magnification, the small nests of tumor cells in this
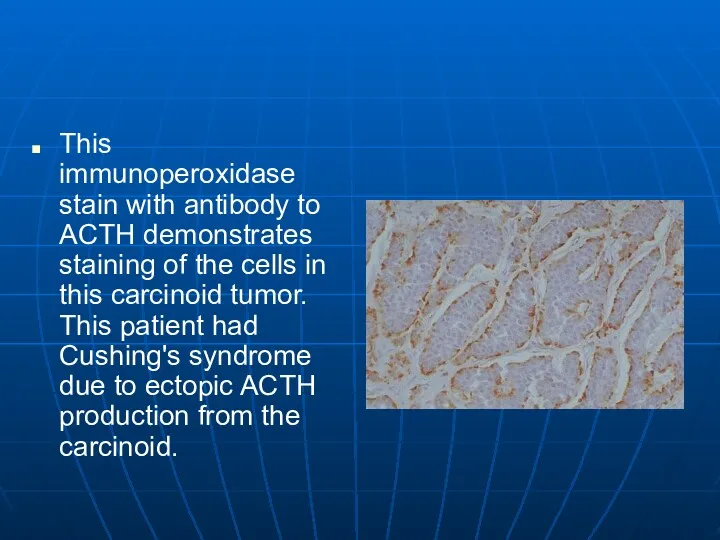
This immunoperoxidase stain with antibody to ACTH demonstrates staining of the
This immunoperoxidase stain with antibody to ACTH demonstrates staining of the
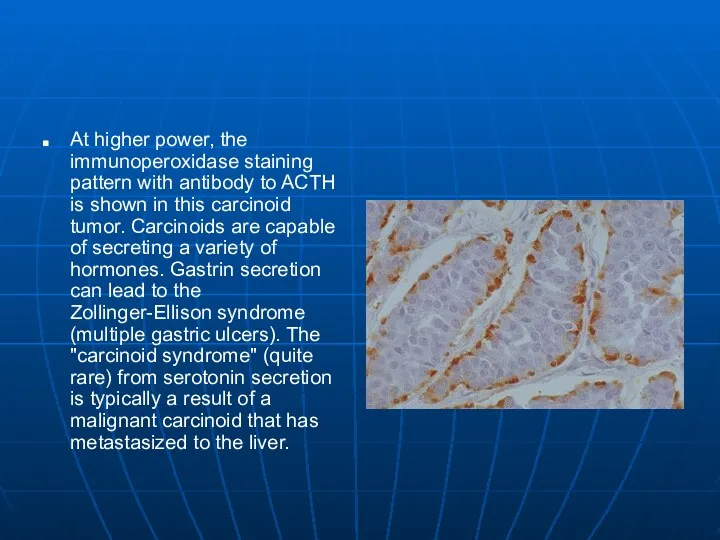
At higher power, the immunoperoxidase staining pattern with antibody to ACTH
At higher power, the immunoperoxidase staining pattern with antibody to ACTH
 СПИД и его профилактика
СПИД и его профилактика Актуальные проблемы комплексной реабилитации инвалидов на современном этапе
Актуальные проблемы комплексной реабилитации инвалидов на современном этапе Токсикозы беременных
Токсикозы беременных Клиническая фармакология антибактериальных лекарственных препаратов. Противовоспалительных препаратов
Клиническая фармакология антибактериальных лекарственных препаратов. Противовоспалительных препаратов Жатыр денесі обыры
Жатыр денесі обыры Мезентериальный тромбоз
Мезентериальный тромбоз Методы обследования в стоматологии
Методы обследования в стоматологии Дієтичне та лікувально-профілактичне харчування
Дієтичне та лікувально-профілактичне харчування Интенсивная терапия после абдоминальных операций
Интенсивная терапия после абдоминальных операций Нехимические зависимости (аддикции)
Нехимические зависимости (аддикции) Хранение и транспортирование товаров медицинского назначения на всех этапах товародвижения
Хранение и транспортирование товаров медицинского назначения на всех этапах товародвижения Синдромы функциональной несформированности, дефицитарности отделов головного мозга
Синдромы функциональной несформированности, дефицитарности отделов головного мозга Ми қан айналымы бұзылыстарының өтпелі түрлері
Ми қан айналымы бұзылыстарының өтпелі түрлері Аппендицит. Анатомия слепой кишки и червеобразного отростка
Аппендицит. Анатомия слепой кишки и червеобразного отростка Вакцина против полиомиелита
Вакцина против полиомиелита Средства физкультуры в регулировании работоспособности
Средства физкультуры в регулировании работоспособности Созылмалы гломерулонефрит
Созылмалы гломерулонефрит Парентеральное питание по технологии три в одном у критических больных
Парентеральное питание по технологии три в одном у критических больных Жедел көмек дәрігерінің тәжірибесіндегі бронхолитикалық ем
Жедел көмек дәрігерінің тәжірибесіндегі бронхолитикалық ем Трихофития
Трихофития Құзіреттілікке жеткізетін мақсат-міндеттері
Құзіреттілікке жеткізетін мақсат-міндеттері Внутренняя среда организма. Значение крови, её состав
Внутренняя среда организма. Значение крови, её состав Корнеальный синдром. Общие симптомы кератитов. Герпетические кератиты. Орбитальные и бульбарные боли. Иридоциклит
Корнеальный синдром. Общие симптомы кератитов. Герпетические кератиты. Орбитальные и бульбарные боли. Иридоциклит Малярия. Стадии развития малярийного плазмодия. (Лекция 12)
Малярия. Стадии развития малярийного плазмодия. (Лекция 12) Дифференциальная диагностика при распространенных заболеваниях в терапии
Дифференциальная диагностика при распространенных заболеваниях в терапии Педагогический совет Роль здорового питания в формировании здорового образа жизни дошкольников
Педагогический совет Роль здорового питания в формировании здорового образа жизни дошкольников Синдром слабости соединительной ткани
Синдром слабости соединительной ткани Пищевые токсикоинфекции
Пищевые токсикоинфекции