- Gastroenterology. Exam preparation

Содержание
- 3. Serum ascites albumin gradient 2.5 – 0.7 = 1.8 SAAG > 1.1 _________________ Ascitic protein =
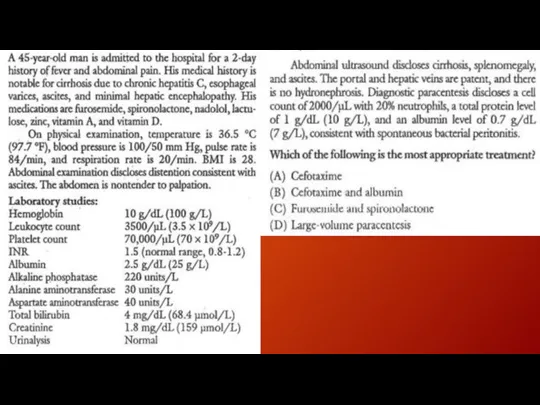
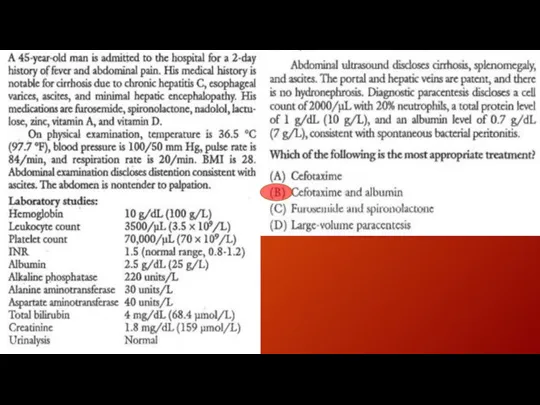
- 4. Spontaneous bacterial peritonitis common and severe complication of ascites characterized by spontaneous infection of the ascitic
- 5. Spontaneous bacterial peritonitis (cont.) Patients with ascites may present with fever, altered mental status, elevated white
- 6. Hepatorenal syndrome form of functional renal failure without renal pathology that occurs in about 10% of
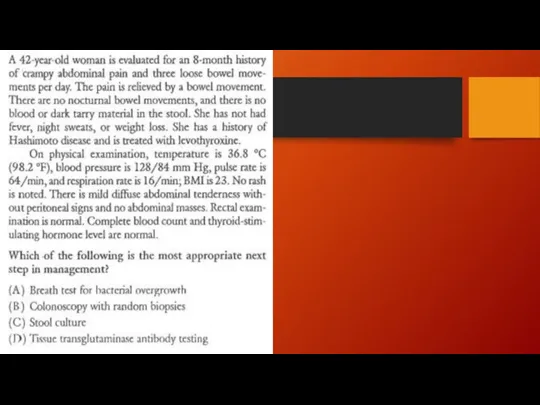
- 9. Irritable bowel syndrome
- 10. Diagnosis No specific laboratory or imaging test can be performed to diagnose irritable bowel syndrome. Diagnosis
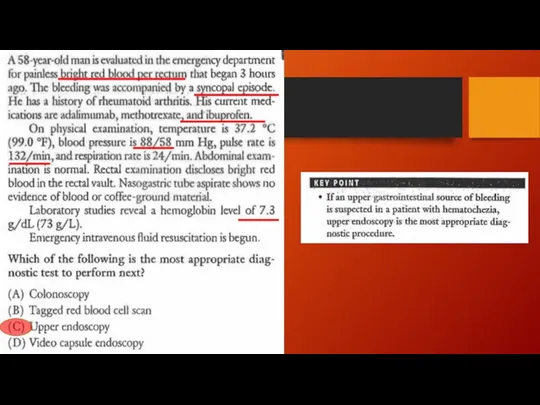
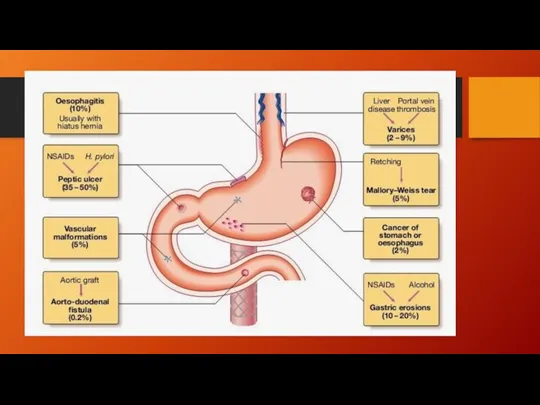
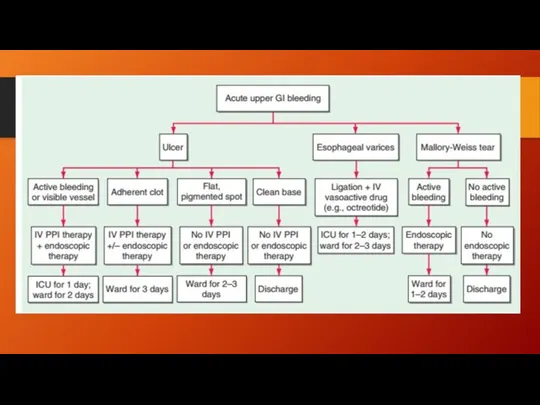
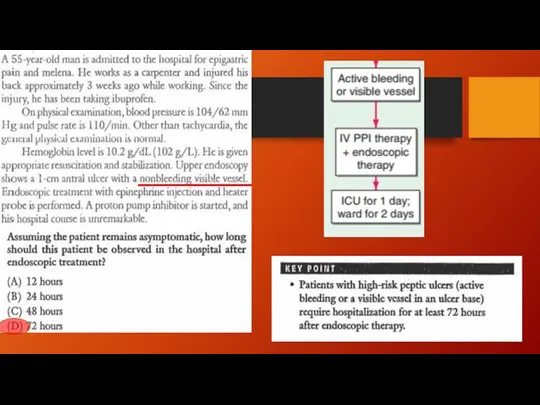
- 13. Melena – UGIB (as little as 150-200 ml of blood loss) Hematemesis – ongoing UGIB Hematochezia
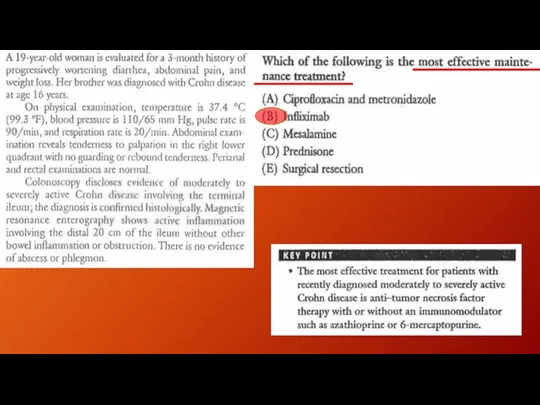
- 20. Endoscopic therapy
- 26. Dyspepsia in patient younger than 50 yo w/o alarm features Anemia Dysphagia Odynophagia Weight loss Vomiting
- 36. Скачать презентацию
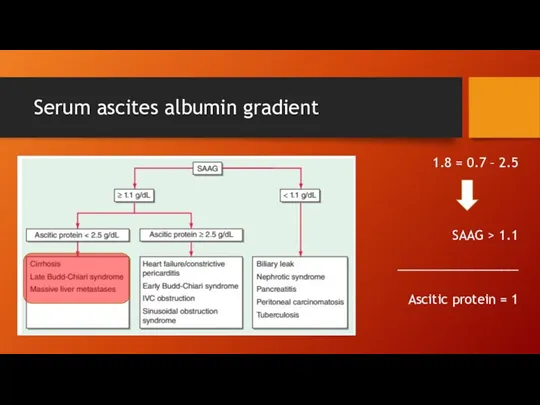
Serum ascites albumin gradient
2.5 – 0.7 = 1.8
SAAG > 1.1
_________________
Ascitic protein
Serum ascites albumin gradient
2.5 – 0.7 = 1.8
SAAG > 1.1
_________________
Ascitic protein
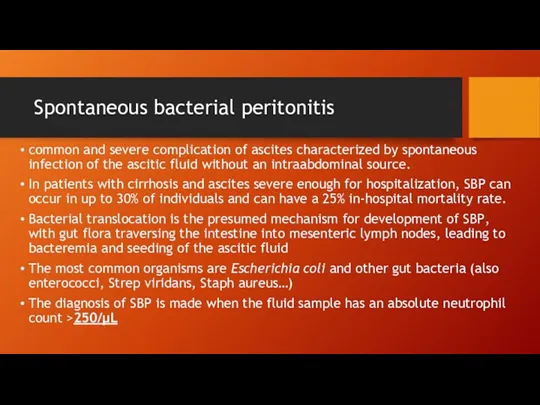
Spontaneous bacterial peritonitis
common and severe complication of ascites characterized by spontaneous
Spontaneous bacterial peritonitis
common and severe complication of ascites characterized by spontaneous
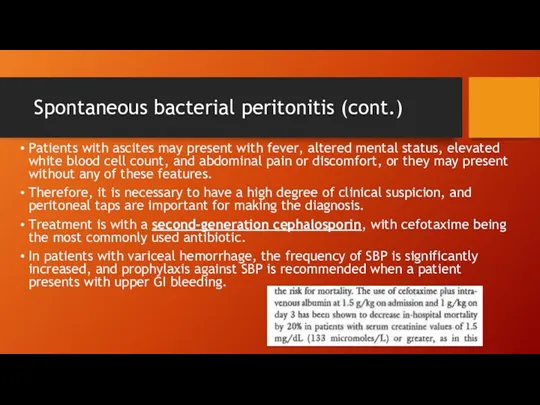
Spontaneous bacterial peritonitis (cont.)
Patients with ascites may present with fever, altered
Spontaneous bacterial peritonitis (cont.)
Patients with ascites may present with fever, altered
Hepatorenal syndrome
form of functional renal failure without renal pathology that occurs
Hepatorenal syndrome
form of functional renal failure without renal pathology that occurs
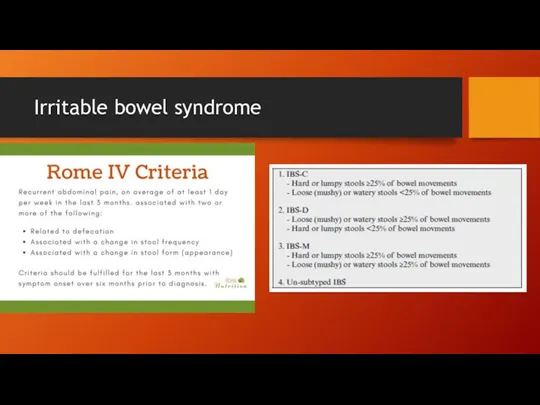
Irritable bowel syndrome
Irritable bowel syndrome
Diagnosis
No specific laboratory or imaging test can be performed to diagnose
Diagnosis
No specific laboratory or imaging test can be performed to diagnose
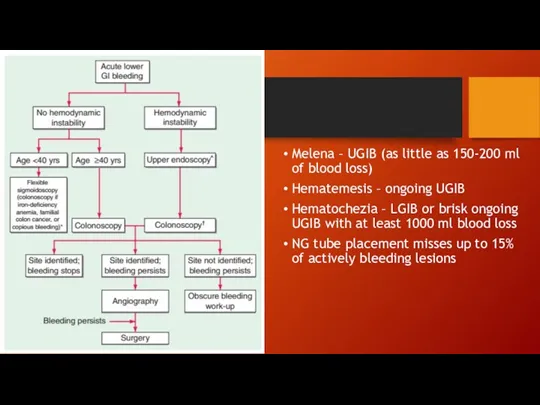
Melena – UGIB (as little as 150-200 ml of blood loss)
Hematemesis
Melena – UGIB (as little as 150-200 ml of blood loss)
Hematemesis
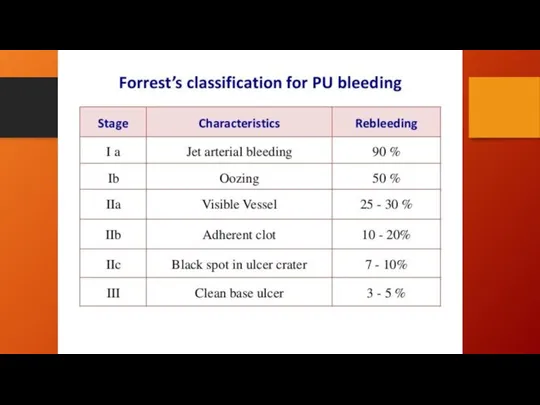

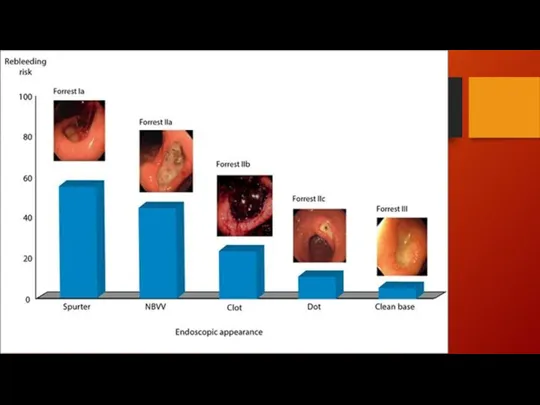
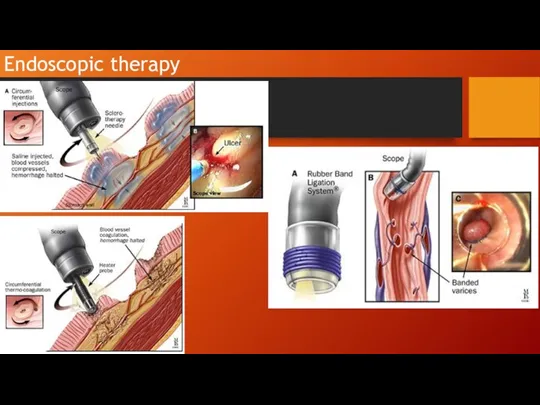
Endoscopic therapy
Endoscopic therapy

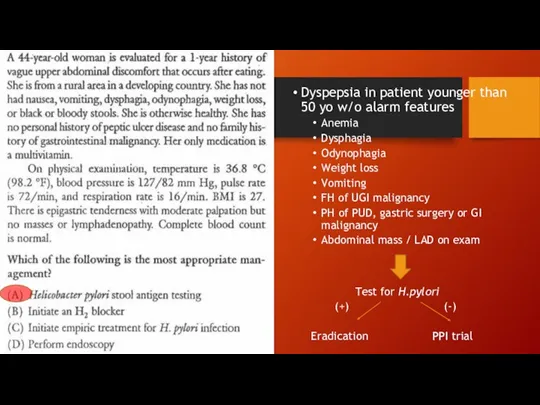
Dyspepsia in patient younger than 50 yo w/o alarm features
Anemia
Dysphagia
Odynophagia
Weight loss
Vomiting
FH
Dyspepsia in patient younger than 50 yo w/o alarm features
Anemia
Dysphagia
Odynophagia
Weight loss
Vomiting
FH
 Современные требования к назначению, оформлению рецептов, требований на ЛП и МИ и их отпуску из аптечных организаций
Современные требования к назначению, оформлению рецептов, требований на ЛП и МИ и их отпуску из аптечных организаций Специфическая (антидотная) фармакотерапия острых отравлений
Специфическая (антидотная) фармакотерапия острых отравлений Репродуктивное здоровье подростка
Репродуктивное здоровье подростка Воздействие наноматериалов на организм человека. Концепция токсикологических исследований
Воздействие наноматериалов на организм человека. Концепция токсикологических исследований Физиология половой дифференцировки и возрастные изменения функций половых желез
Физиология половой дифференцировки и возрастные изменения функций половых желез Медицинский отряд специального назначения
Медицинский отряд специального назначения Хирургические инфекции
Хирургические инфекции Будь здоров
Будь здоров Методы обследования больного - пальпация, перкуссия. Методы исследования и симптоматология заболеваний органов дыхания
Методы обследования больного - пальпация, перкуссия. Методы исследования и симптоматология заболеваний органов дыхания Биоэтика: возникновение, структура, принципы
Биоэтика: возникновение, структура, принципы Аса қауіпті аурулар
Аса қауіпті аурулар Аяқ қол хирургиялық аурулары,туа біткен ақаулары және жарақаттары
Аяқ қол хирургиялық аурулары,туа біткен ақаулары және жарақаттары Радионуклидная диагностика в кардиологии
Радионуклидная диагностика в кардиологии Психические расстройства вследствие органического поражения головного мозга
Психические расстройства вследствие органического поражения головного мозга Организация работы специализированных и линйных бригад скорой медицинской помощи
Организация работы специализированных и линйных бригад скорой медицинской помощи Гигиенические требования к условиям и режиму пребывания в детских и подростковых учреждениях
Гигиенические требования к условиям и режиму пребывания в детских и подростковых учреждениях Симптоматические гипертонии в амбулаторной практике
Симптоматические гипертонии в амбулаторной практике Новый коронавирус 2019- nCоV
Новый коронавирус 2019- nCоV Вскармливание детей грудного возраста
Вскармливание детей грудного возраста Врачебная этика Френсиса Бэкона
Врачебная этика Френсиса Бэкона Лікування хворих на цукровий діабет
Лікування хворих на цукровий діабет Организация и тактика медицинской службы (ОТМС)
Организация и тактика медицинской службы (ОТМС) Неотложная терапия анафилактических реакций
Неотложная терапия анафилактических реакций Правила парентерального введения лекарственных средств. Сестринское дело
Правила парентерального введения лекарственных средств. Сестринское дело Частная травматология. Повреждения тупыми предметами
Частная травматология. Повреждения тупыми предметами Инструкция для медицинского применения лекарств и вопросы безопасности
Инструкция для медицинского применения лекарств и вопросы безопасности Средства, действующие на эфферентную иннервацию
Средства, действующие на эфферентную иннервацию Опухоли почек
Опухоли почек