- Heart diseases. Arrhythmia

Содержание
- 2. Myocarditis Inflammation of the heart muscle Classification specific and non-specific (specific –when inflammation is granulomatous). acute,
- 3. Infectious causes Viral – coxsackie B virus, Epstein-Barr virus, cytomegalovirus, influenza A and B, herpes. Bacterial
- 4. Non-infectious causes Cardiotoxins – catecholamines, cocaine, alcohol, carbon monoxide, arsenic, heavy metals (copper, lead, iron). Hypersensitivity
- 5. Clinical manifestation excessive fatigue, chest pains, unexplained sinus tachycardia, congestive heart failure low voltage QRS complexes,
- 6. Cardiac failure A state in which impaired cardiac function is unable to maintain an adequate circulation
- 7. Cardiac failure classification Myocardial – due to direct affection of myocardium Overload – due to heart
- 8. Heart overload Increased pressure load (afterload) is observed at systemic and pulmonary arterial hypertension, valvular stenosis
- 9. Cardiac failure classifications Acute cardiac failure - sudden reduction in CO resulting in systemic hypotension acute
- 10. Left ventricle failure pulmonary congestion and lungs oedema High pulmonary venous pressure leads to extravasation of
- 11. Right ventricle failure increased systemic venous pressure. edema (feet, ankles, abdominal viscera, especially liver). impaired liver
- 12. Cardiac failure classification primary heart failure (cardiogenic form) - IHD, AMI, myocarditis secondary heart failure (non-cardiogenic
- 13. Cardiac failure symptoms Shortness of breath ("dyspnea") - due to excess fluid in the lungs. Fatigue
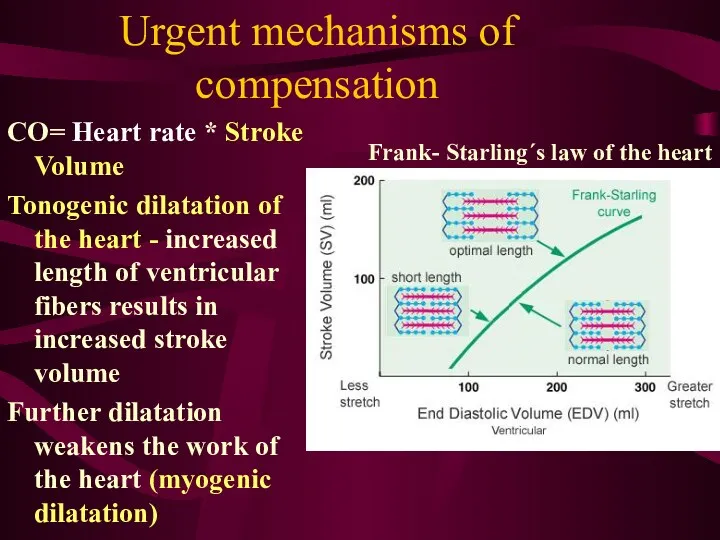
- 14. Urgent mechanisms of compensation CO= Heart rate * Stroke Volume Tonogenic dilatation of the heart -
- 15. Urgent mechanisms of compensation Increased sympathetic tone - the constriction of blood vessels and tachycardia Constriction
- 16. Long-term mechanism of compensation Myocardial hypertrophy Physiological hypertrophy - high stroke volume - develops in high
- 17. Reasons of pathological hyperthrophy Heart diseases: Myocardial disorders, pericarditis, valvular disorders, congenital heart disease. Vascular disorders:
- 18. Ischemic heart disease IHD or coronary artery disease - imbalance between the myocardial supply and its
- 19. Etiology of IHD The reasons of low oxygen supply: Atherosclerosis, Spasm of arteries, Thrombus and Embolism,
- 20. Angina pectoris Angina pectoris is chest pain due to ischemia of the heart muscle. Greek ankhon
- 21. Angina pectoris Hypoxia Acidosis Ischemia Myocardial cells injury
- 22. Angina pectoris Triggers of angina: physical exertion emotional stress heavy meals extreme cold and heat, excessive
- 23. Myocardial infarction Death or necrosis of myocardial cells Etiology increased myocardial metabolic demand physical exertion, severe
- 24. Myocardial infarction The severity of MI is dependent on: level of the occlusion in the coronary
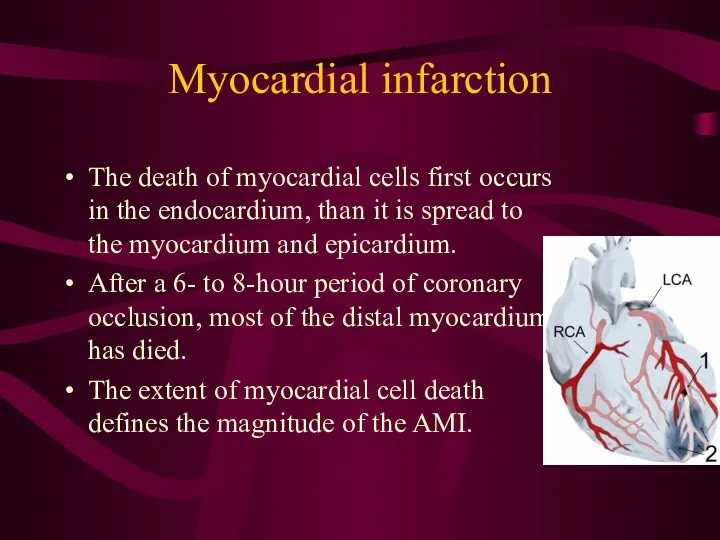
- 25. Myocardial infarction The death of myocardial cells first occurs in the endocardium, than it is spread
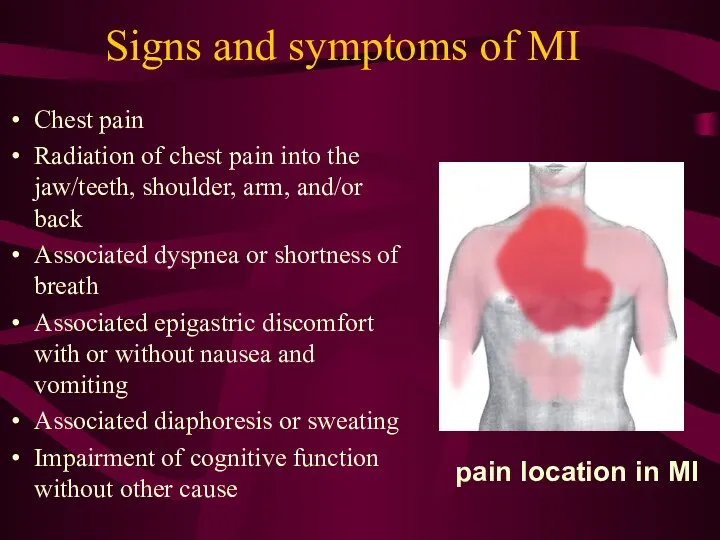
- 26. Signs and symptoms of MI Chest pain Radiation of chest pain into the jaw/teeth, shoulder, arm,
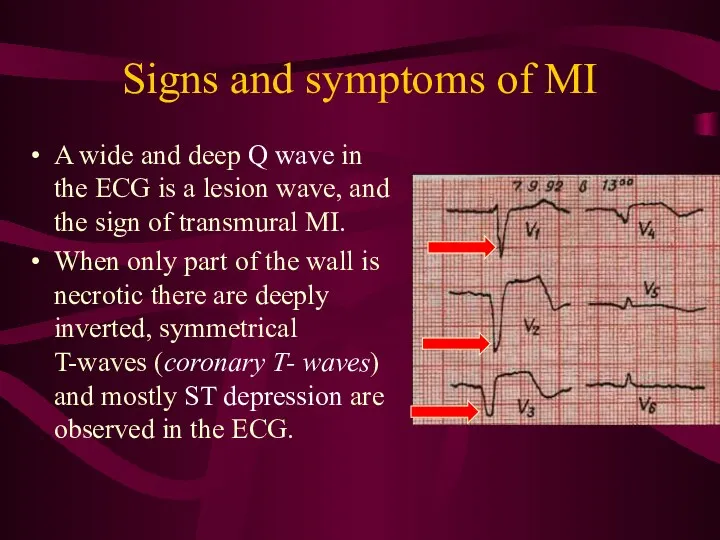
- 27. Signs and symptoms of MI A wide and deep Q wave in the ECG is a
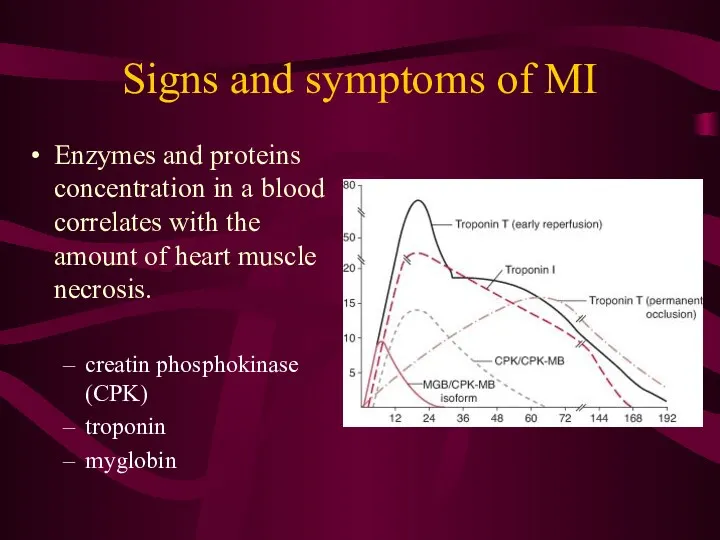
- 28. Signs and symptoms of MI Enzymes and proteins concentration in a blood correlates with the amount
- 29. Reperfusion of MI circulation brings neutrophils to re-perfused tissues that release toxic oxygen radicals and cytokines
- 30. Cardiogenic shock Cardiogenic shock is a severe reduction of cardiac output The pulmonary capillary wedge pressure
- 31. Cardiogenic shock symptoms Anxiety, restlessness, altered mental state Hypotension A rapid, weak, thready pulse Cool, clammy,
- 32. Arrhythmia classification
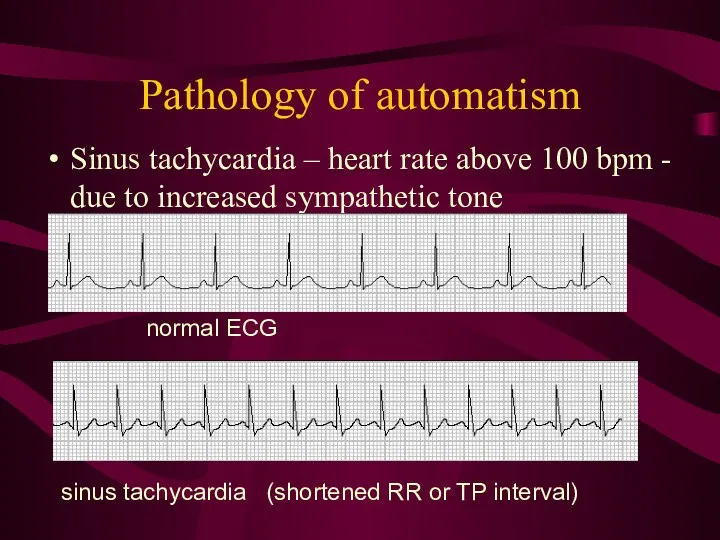
- 33. Pathology of automatism Sinus tachycardia – heart rate above 100 bpm - due to increased sympathetic
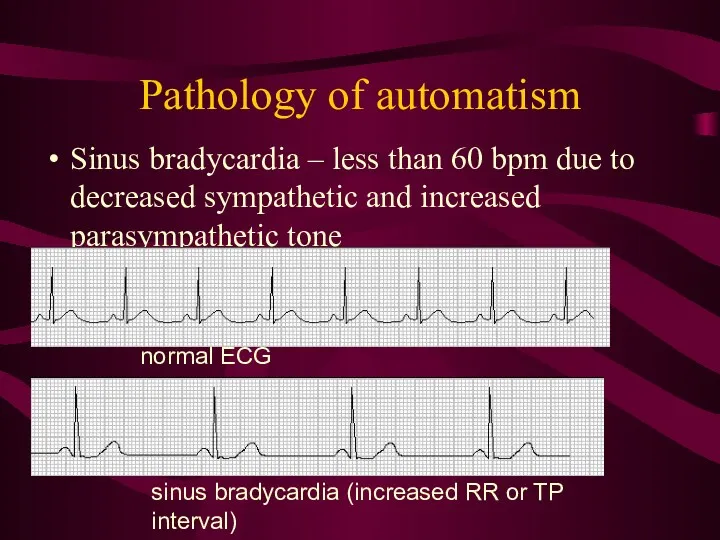
- 34. Pathology of automatism Sinus bradycardia – less than 60 bpm due to decreased sympathetic and increased
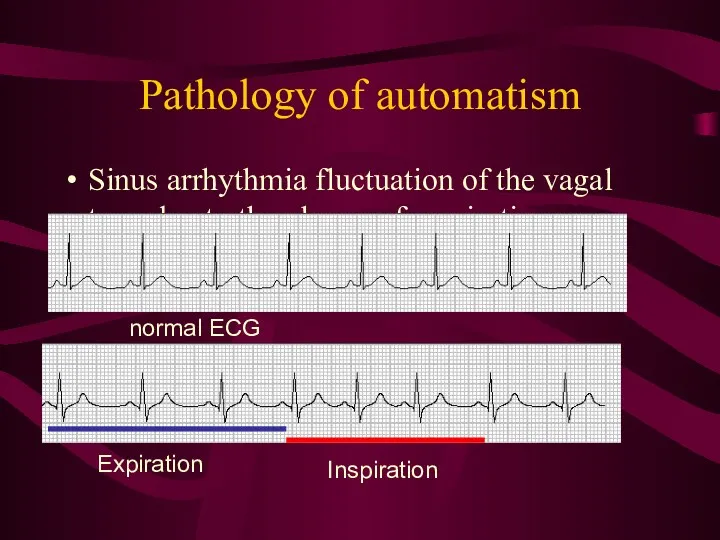
- 35. Pathology of automatism Sinus arrhythmia fluctuation of the vagal tone due to the phases of respiration
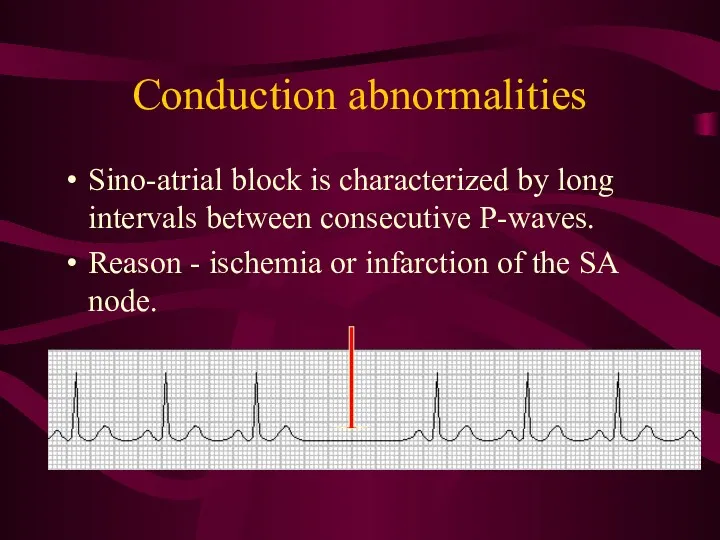
- 36. Conduction abnormalities Sino-atrial block is characterized by long intervals between consecutive P-waves. Reason - ischemia or
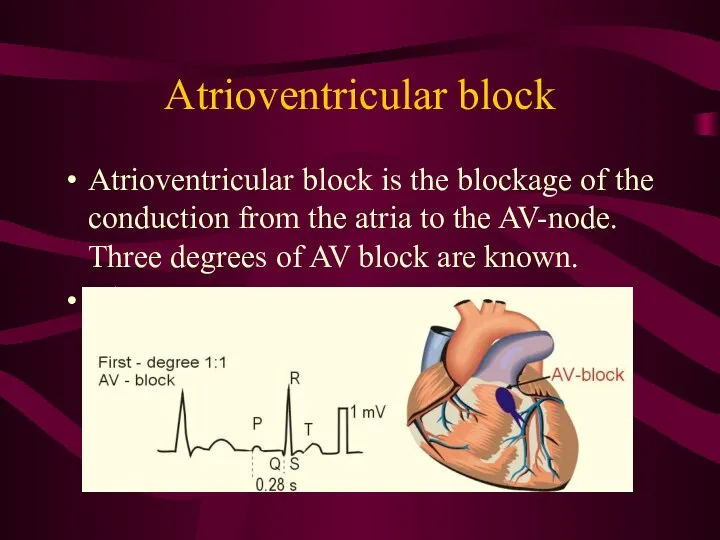
- 37. Atrioventricular block Atrioventricular block is the blockage of the conduction from the atria to the AV-node.
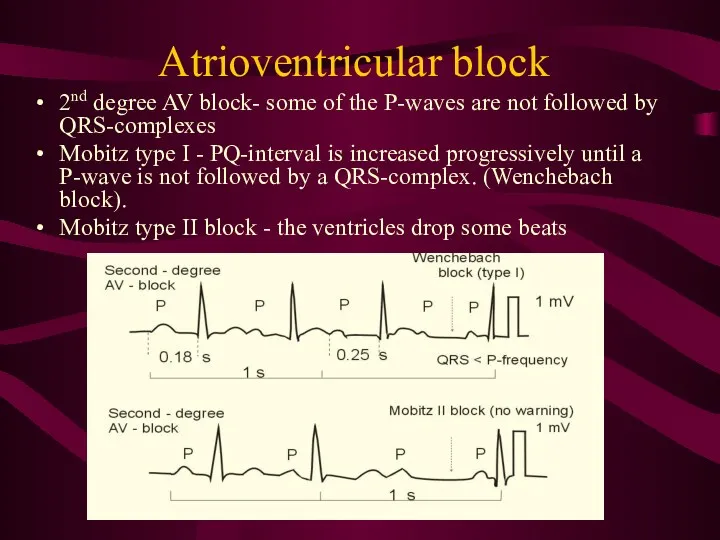
- 38. Atrioventricular block 2nd degree AV block- some of the P-waves are not followed by QRS-complexes Mobitz
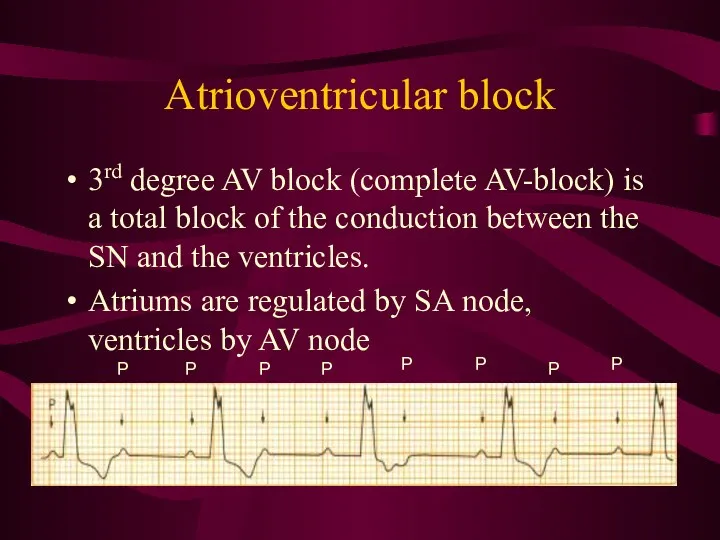
- 39. Atrioventricular block 3rd degree AV block (complete AV-block) is a total block of the conduction between
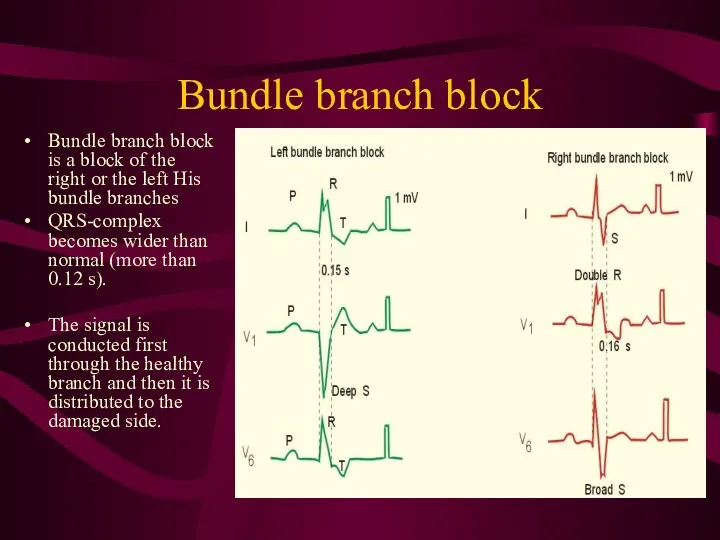
- 40. Bundle branch block Bundle branch block is a block of the right or the left His
- 41. Pathology of excitability Pathology of excitability is usually manifested with ectopic beats (outside the sinus node).
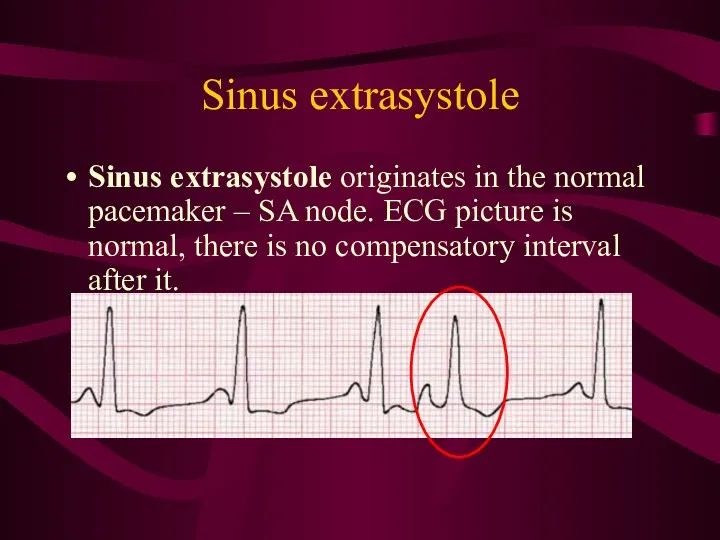
- 42. Sinus extrasystole Sinus extrasystole originates in the normal pacemaker – SA node. ECG picture is normal,
- 43. Atrial ectopic beat Atrial ectopic beats have abnormal P-waves and are usually followed by normal QRS-complexes.
- 44. Premature junctional contractions Ectopic beat originate in the atrio-ventricular node. P-wave is negative Compensatory interval a
- 45. Ventricular ectopic beat wide QRS-complex (above 0.12 s), long compensatory interval (2RR)
- 46. Paroxysmal ectopic tachycardia Paroxysmal atrial tachycardia is elicited in the atrial tissue outside the SA node
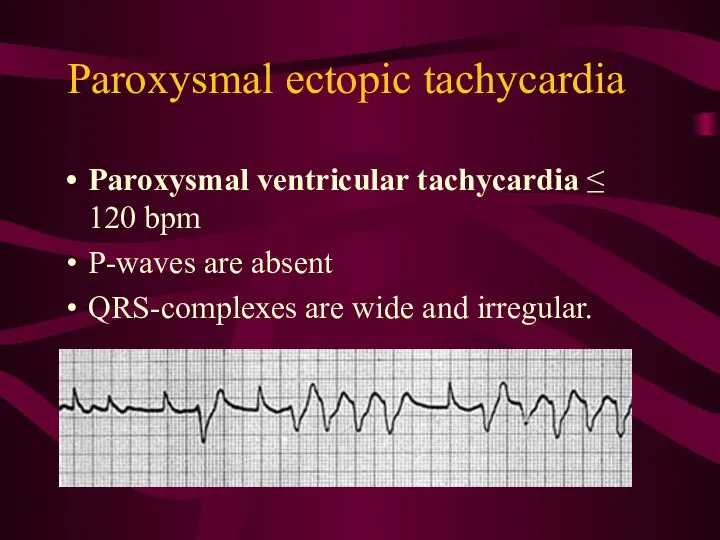
- 47. Paroxysmal ectopic tachycardia Paroxysmal ventricular tachycardia ≤ 120 bpm P-waves are absent QRS-complexes are wide and
- 48. Disorders of hemodynamic in the pathology of excitability Single extrasystole clinically manifests in the feeling of
- 49. Atrial fibrillation and flutter Atrial fibrillation - more than 400 P-waves per min , QRS-frequency of
- 50. Reasons of atrial fibrillation Re-entry phenomenon - cardiac impulse travel around in cardiac muscle without stopping
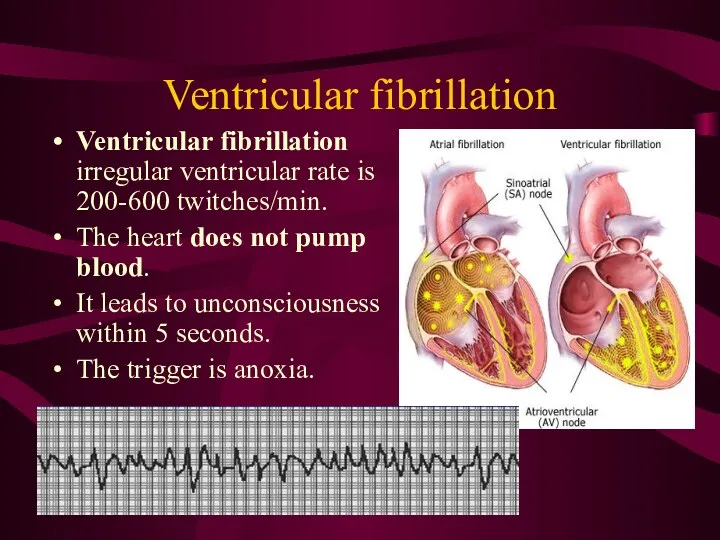
- 51. Ventricular fibrillation Ventricular fibrillation irregular ventricular rate is 200-600 twitches/min. The heart does not pump blood.
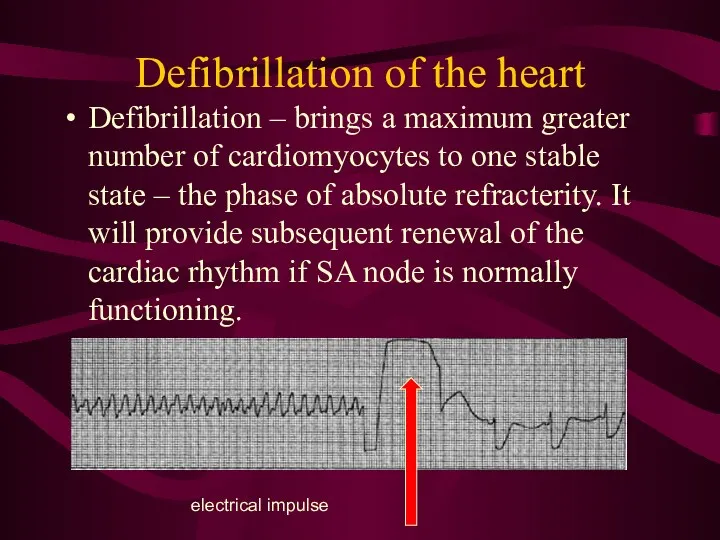
- 52. Defibrillation of the heart Defibrillation – brings a maximum greater number of cardiomyocytes to one stable
- 54. Скачать презентацию
Myocarditis
Inflammation of the heart muscle
Classification
specific and non-specific (specific –when inflammation
Myocarditis
Inflammation of the heart muscle
Classification
specific and non-specific (specific –when inflammation
Infectious causes
Viral – coxsackie B virus, Epstein-Barr virus, cytomegalovirus, influenza
Infectious causes
Viral – coxsackie B virus, Epstein-Barr virus, cytomegalovirus, influenza
Non-infectious causes
Cardiotoxins – catecholamines, cocaine, alcohol, carbon monoxide, arsenic, heavy metals
Non-infectious causes
Cardiotoxins – catecholamines, cocaine, alcohol, carbon monoxide, arsenic, heavy metals
Clinical manifestation
excessive fatigue,
chest pains,
unexplained sinus tachycardia,
congestive heart failure
low
Clinical manifestation
excessive fatigue,
chest pains,
unexplained sinus tachycardia,
congestive heart failure
low
Cardiac failure
A state in which impaired cardiac function is unable
Cardiac failure
A state in which impaired cardiac function is unable
Cardiac failure classification
Myocardial – due to direct affection of myocardium
Overload –
Cardiac failure classification
Myocardial – due to direct affection of myocardium
Overload –
Heart overload
Increased pressure load (afterload) is observed at systemic and pulmonary
Heart overload
Increased pressure load (afterload) is observed at systemic and pulmonary
Cardiac failure classifications
Acute cardiac failure - sudden reduction in CO resulting
Cardiac failure classifications
Acute cardiac failure - sudden reduction in CO resulting
Left ventricle failure
pulmonary congestion and lungs oedema
High pulmonary venous pressure
Left ventricle failure
pulmonary congestion and lungs oedema
High pulmonary venous pressure
Right ventricle failure
increased systemic venous pressure.
edema (feet, ankles, abdominal viscera, especially
Right ventricle failure
increased systemic venous pressure.
edema (feet, ankles, abdominal viscera, especially
Cardiac failure classification
primary heart failure (cardiogenic form) - IHD, AMI, myocarditis
Cardiac failure classification
primary heart failure (cardiogenic form) - IHD, AMI, myocarditis
Cardiac failure symptoms
Shortness of breath ("dyspnea") - due to excess fluid
Cardiac failure symptoms
Shortness of breath ("dyspnea") - due to excess fluid
Urgent mechanisms of compensation
CO= Heart rate * Stroke Volume
Tonogenic dilatation of
Urgent mechanisms of compensation
CO= Heart rate * Stroke Volume
Tonogenic dilatation of

Urgent mechanisms of compensation
Increased sympathetic tone - the constriction of blood
Urgent mechanisms of compensation
Increased sympathetic tone - the constriction of blood
Long-term mechanism of compensation
Myocardial hypertrophy
Physiological hypertrophy - high stroke volume
Long-term mechanism of compensation
Myocardial hypertrophy
Physiological hypertrophy - high stroke volume
Reasons of pathological hyperthrophy
Heart diseases: Myocardial disorders, pericarditis, valvular disorders, congenital
Reasons of pathological hyperthrophy
Heart diseases: Myocardial disorders, pericarditis, valvular disorders, congenital
Ischemic heart disease
IHD or coronary artery disease - imbalance between
Ischemic heart disease
IHD or coronary artery disease - imbalance between
Etiology of IHD
The reasons of low oxygen supply:
Atherosclerosis,
Spasm of
Etiology of IHD
The reasons of low oxygen supply:
Atherosclerosis,
Spasm of
Angina pectoris
Angina pectoris is chest pain due to ischemia of the
Angina pectoris
Angina pectoris is chest pain due to ischemia of the
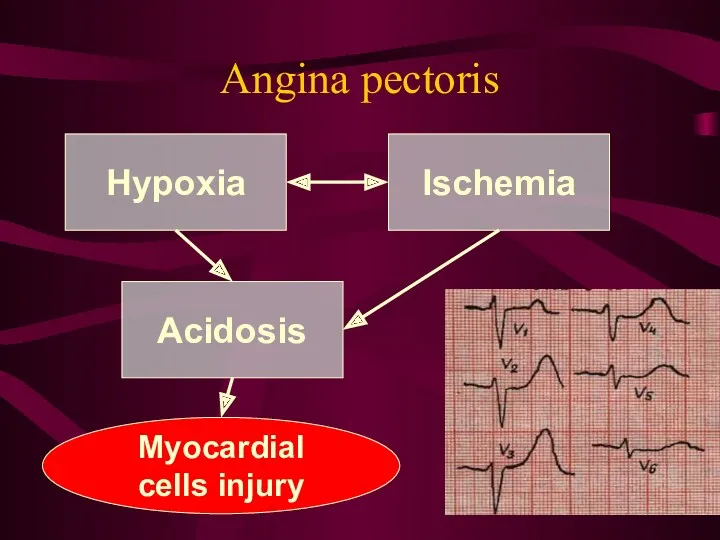
Angina pectoris
Hypoxia
Acidosis
Ischemia
Myocardial
cells injury
Angina pectoris
Hypoxia
Acidosis
Ischemia
Myocardial
cells injury
Angina pectoris
Triggers of angina:
physical exertion
emotional stress
heavy meals
extreme cold
Angina pectoris
Triggers of angina:
physical exertion
emotional stress
heavy meals
extreme cold
Myocardial infarction
Death or necrosis of myocardial cells
Etiology
increased myocardial metabolic
Myocardial infarction
Death or necrosis of myocardial cells
Etiology
increased myocardial metabolic
Myocardial infarction
The severity of MI is dependent on:
level of the occlusion
Myocardial infarction
The severity of MI is dependent on:
level of the occlusion
Myocardial infarction
The death of myocardial cells first occurs in the endocardium,
Myocardial infarction
The death of myocardial cells first occurs in the endocardium,
Signs and symptoms of MI
Chest pain
Radiation of chest pain into the
Signs and symptoms of MI
Chest pain
Radiation of chest pain into the
Signs and symptoms of MI
A wide and deep Q wave in
Signs and symptoms of MI
A wide and deep Q wave in
Signs and symptoms of MI
Enzymes and proteins concentration in a blood
Signs and symptoms of MI
Enzymes and proteins concentration in a blood
Reperfusion of MI
circulation brings neutrophils to re-perfused tissues that release
Reperfusion of MI
circulation brings neutrophils to re-perfused tissues that release
Cardiogenic shock
Cardiogenic shock is a severe reduction of cardiac output
Cardiogenic shock
Cardiogenic shock is a severe reduction of cardiac output
Cardiogenic shock symptoms
Anxiety, restlessness, altered mental state
Hypotension
A rapid, weak, thready pulse
Cardiogenic shock symptoms
Anxiety, restlessness, altered mental state
Hypotension
A rapid, weak, thready pulse
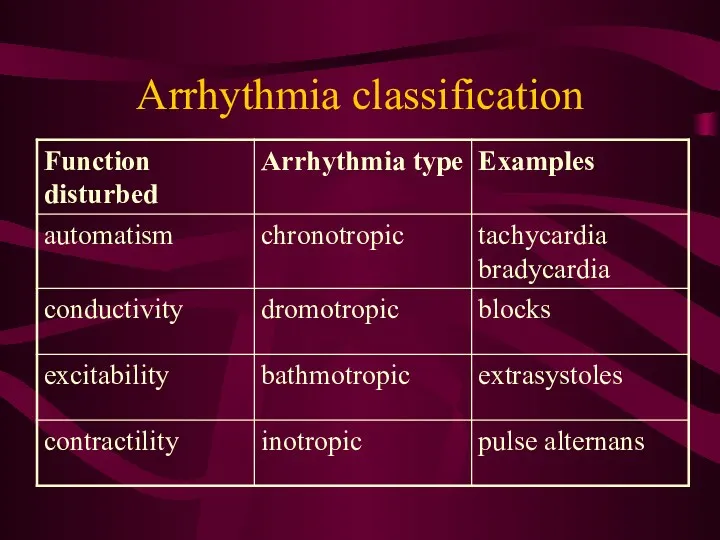
Arrhythmia classification
Arrhythmia classification
Pathology of automatism
Sinus tachycardia – heart rate above 100 bpm
Pathology of automatism
Sinus tachycardia – heart rate above 100 bpm
Pathology of automatism
Sinus bradycardia – less than 60 bpm due
Pathology of automatism
Sinus bradycardia – less than 60 bpm due
Pathology of automatism
Sinus arrhythmia fluctuation of the vagal tone due to
Pathology of automatism
Sinus arrhythmia fluctuation of the vagal tone due to
Conduction abnormalities
Sino-atrial block is characterized by long intervals between consecutive
Conduction abnormalities
Sino-atrial block is characterized by long intervals between consecutive
Atrioventricular block
Atrioventricular block is the blockage of the conduction from the
Atrioventricular block
Atrioventricular block is the blockage of the conduction from the
Atrioventricular block
2nd degree AV block- some of the P-waves are not
Atrioventricular block
2nd degree AV block- some of the P-waves are not
Atrioventricular block
3rd degree AV block (complete AV-block) is a total block
Atrioventricular block
3rd degree AV block (complete AV-block) is a total block
Bundle branch block
Bundle branch block is a block of the
Bundle branch block
Bundle branch block is a block of the
Pathology of excitability
Pathology of excitability is usually manifested with ectopic
Pathology of excitability
Pathology of excitability is usually manifested with ectopic
Sinus extrasystole
Sinus extrasystole originates in the normal pacemaker – SA
Sinus extrasystole
Sinus extrasystole originates in the normal pacemaker – SA
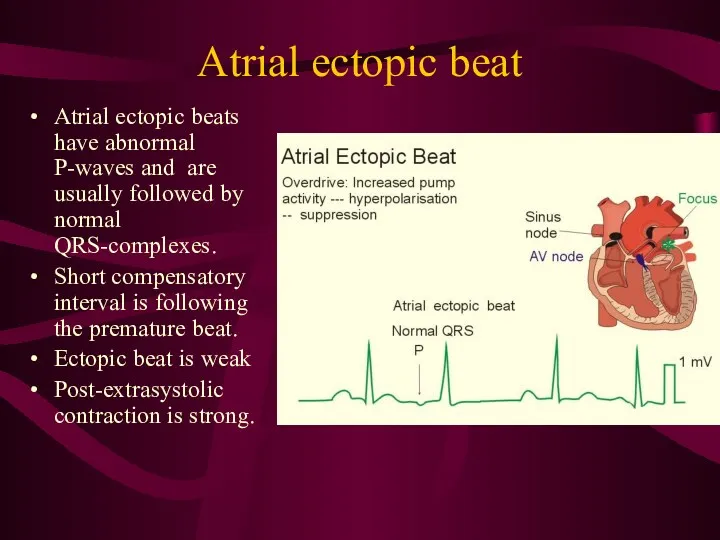
Atrial ectopic beat
Atrial ectopic beats have abnormal P-waves and are
Atrial ectopic beat
Atrial ectopic beats have abnormal P-waves and are
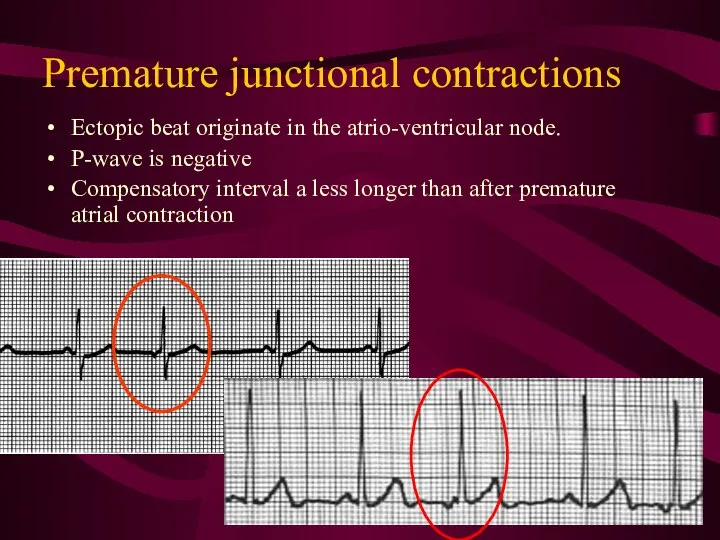
Premature junctional contractions
Ectopic beat originate in the atrio-ventricular node.
P-wave is
Premature junctional contractions
Ectopic beat originate in the atrio-ventricular node.
P-wave is
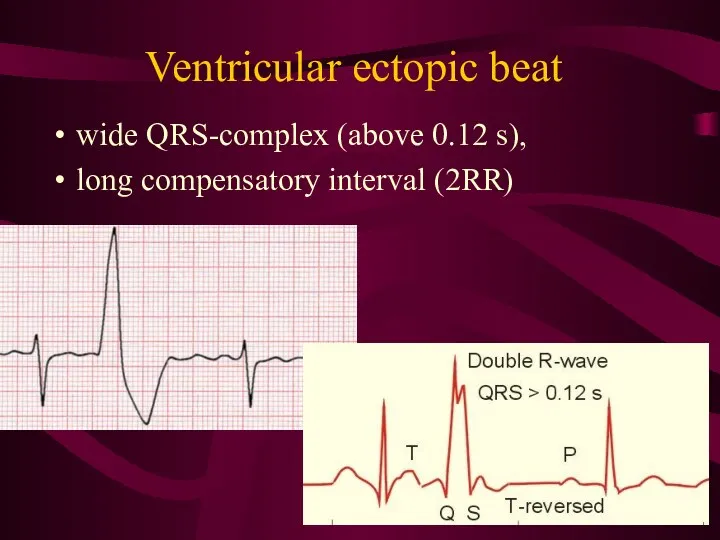
Ventricular ectopic beat
wide QRS-complex (above 0.12 s),
long compensatory interval
Ventricular ectopic beat
wide QRS-complex (above 0.12 s),
long compensatory interval
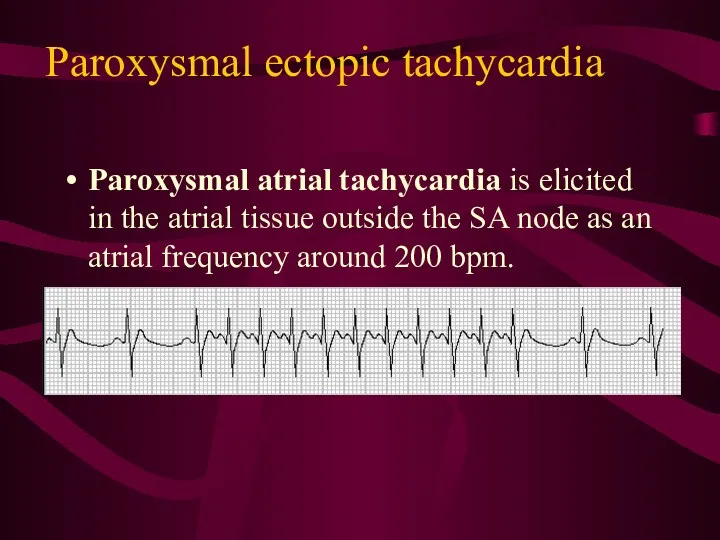
Paroxysmal ectopic tachycardia
Paroxysmal atrial tachycardia is elicited in the atrial
Paroxysmal ectopic tachycardia
Paroxysmal atrial tachycardia is elicited in the atrial
Paroxysmal ectopic tachycardia
Paroxysmal ventricular tachycardia ≤ 120 bpm
P-waves are absent
QRS-complexes are
Paroxysmal ectopic tachycardia
Paroxysmal ventricular tachycardia ≤ 120 bpm
P-waves are absent
QRS-complexes are
Disorders of hemodynamic in the pathology of excitability
Single extrasystole clinically manifests
Disorders of hemodynamic in the pathology of excitability
Single extrasystole clinically manifests
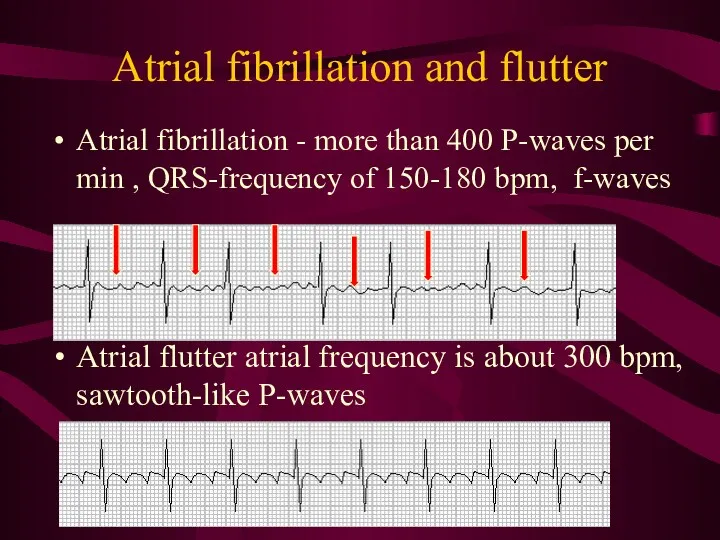
Atrial fibrillation and flutter
Atrial fibrillation - more than 400 P-waves per
Atrial fibrillation and flutter
Atrial fibrillation - more than 400 P-waves per
Reasons of atrial fibrillation
Re-entry phenomenon - cardiac impulse travel around in
Reasons of atrial fibrillation
Re-entry phenomenon - cardiac impulse travel around in
Ventricular fibrillation
Ventricular fibrillation irregular ventricular rate is 200-600 twitches/min.
The heart
Ventricular fibrillation
Ventricular fibrillation irregular ventricular rate is 200-600 twitches/min.
The heart
Defibrillation of the heart
Defibrillation – brings a maximum greater number of
Defibrillation of the heart
Defibrillation – brings a maximum greater number of
 Лейкокория у детей
Лейкокория у детей Методика исследования периферических и внутригрудных лимфатических узлов
Методика исследования периферических и внутригрудных лимфатических узлов Инфекционные болезни - чума
Инфекционные болезни - чума Наложение шин на руку
Наложение шин на руку Сердечно-легочная реанимация
Сердечно-легочная реанимация Жүктілікпен байланысты гипертензиясы Ерте токсикоздар
Жүктілікпен байланысты гипертензиясы Ерте токсикоздар Воздействие на поведение водителя психотропных, наркотических веществ, алкоголя и медицинских препаратов
Воздействие на поведение водителя психотропных, наркотических веществ, алкоголя и медицинских препаратов Косметические средства ухода за кожей детей при аномалиях конституции
Косметические средства ухода за кожей детей при аномалиях конституции Diet and teen health
Diet and teen health Зрительный нерв. Заболевания зрительного нерва
Зрительный нерв. Заболевания зрительного нерва Реанимационная помощь
Реанимационная помощь Дәрілік заттардың әсерінің ағза қасиеттеріне тәуелділігі. Фармакологиялық әсердің дәрілік заттардың қасиеттері мен қолдану
Дәрілік заттардың әсерінің ағза қасиеттеріне тәуелділігі. Фармакологиялық әсердің дәрілік заттардың қасиеттері мен қолдану Antimicrobial drugs
Antimicrobial drugs Снотворные и противосудорожные средства. Противопаркинсонические средства
Снотворные и противосудорожные средства. Противопаркинсонические средства Предмет и задачи медицинской микробиологии. История микробиологии. Медицинская микробиология XXI века
Предмет и задачи медицинской микробиологии. История микробиологии. Медицинская микробиология XXI века Ошибки диагностики и лечения при сочетанной травме
Ошибки диагностики и лечения при сочетанной травме Профилактика стоматологических заболеваний в раннем детском возрасте
Профилактика стоматологических заболеваний в раннем детском возрасте Вскармливание детей грудного возраста. Раздел 1.Лекция 6
Вскармливание детей грудного возраста. Раздел 1.Лекция 6 Современные направления пластической хирургии в акушерстве и гинекологии
Современные направления пластической хирургии в акушерстве и гинекологии Местные анестетики
Местные анестетики Всероссийский день трезвости
Всероссийский день трезвости ВКР: Анализ работы медсестры процедурного кабинета хирургического отделения стационара
ВКР: Анализ работы медсестры процедурного кабинета хирургического отделения стационара Врожденные аномалии грудной клетки
Врожденные аномалии грудной клетки Вреден ли фаст-фуд для нашего здоровья
Вреден ли фаст-фуд для нашего здоровья Здоровый образ жизни и профилактика основных неинфекционных заболеваний
Здоровый образ жизни и профилактика основных неинфекционных заболеваний Қазіргі заманғы денсаулық сақтау, әлемдік тенденция, дамыған елдер
Қазіргі заманғы денсаулық сақтау, әлемдік тенденция, дамыған елдер Иммуногенез бұзылуының морфологиясы. Тимустың, шеткері лимфалық тіндердің иммунгенез бұзылғандағы өзгерістері
Иммуногенез бұзылуының морфологиясы. Тимустың, шеткері лимфалық тіндердің иммунгенез бұзылғандағы өзгерістері Жүкті студенттердің медико-әлеуметтік аспектілері
Жүкті студенттердің медико-әлеуметтік аспектілері