- Heart Murmurs

Содержание
- 2. Outline I. Basic Pathophysiology II. Describing murmurs III. Systolic murmurs IV. Diastolic murmurs V. Continuous murmurs
- 3. Basic Pathophysiology Murmurs = Math Q = V*A Q = P/R NR = d*D*V/n Therefore: Inc.
- 4. Describing a heart murmur 1. Timing murmurs are longer than heart sounds HS can distinguished by
- 5. Describing a heart murmur con’t: 4. Radiation reflects the intensity of the murmur and the direction
- 6. Describing a heart murmur con’t: 6. Pitch high, medium, low 7. Quality blowing, harsh, rumbling, and
- 7. Systolic Murmurs Derived from increased turbulence associated with: 1. Increased flow across normal SL valve or
- 8. Early Systolic murmurs 1. Acute severe mitral regurgitation decrescendo murmur best heard at apical impulse Caused
- 9. Midsystolic (ejection) murmurs Are the most common kind of heart murmur Are usually crescendo-decrescendo They may
- 10. Aortic stenosis Loudest in aortic area; radiates along the carotid arteries Intensity varies directly with CO
- 11. Hypertrophic cardiomyopathy Loudest b/t left sternal edge and apex; Grade 2-3/6 Does NOT radiate into neck;
- 12. Pansystolic (Holosystolic) Murmurs Are pathologic Murmur begins immediately with S1 and continues up to S2 1.
- 13. Diastolic Murmurs Almost always indicate heart disease Two basic types: 1. Early decrescendo diastolic murmurs signify
- 14. Aortic Regurgitation Best heard in the 2nd ICS at the left sternal edge High pitched, decrescendo
- 15. Mitral Stenosis Two components: 1. Middiastolic - during rapid ventricular filling 2. Presystolic - during atrial
- 16. Continuous Murmurs Begin in systole, peak near s2, and continue into all or part of diastole.
- 17. Back to the Basics 1. When does it occur - systole or diastole 2. Where is
- 19. Скачать презентацию
Outline
I. Basic Pathophysiology
II. Describing murmurs
III. Systolic murmurs
IV. Diastolic murmurs
V. Continuous murmurs
VI.
Outline
I. Basic Pathophysiology
II. Describing murmurs
III. Systolic murmurs
IV. Diastolic murmurs
V. Continuous murmurs
VI.
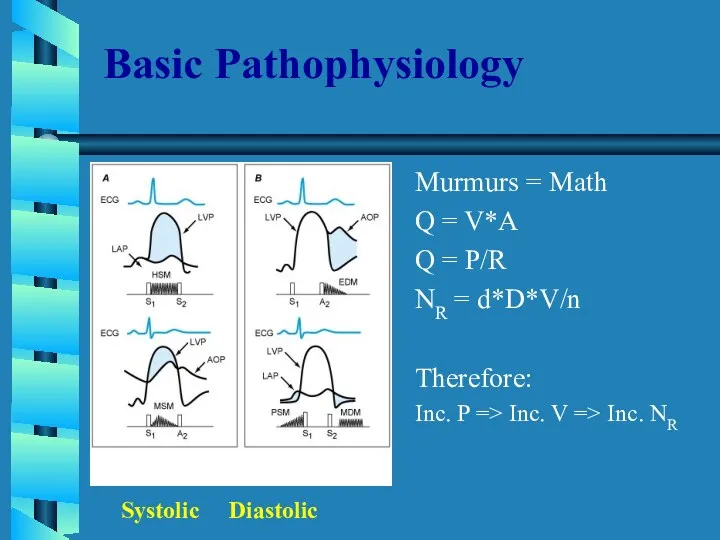
Basic Pathophysiology
Murmurs = Math
Q = V*A
Q = P/R
NR = d*D*V/n
Therefore:
Inc. P
Basic Pathophysiology
Murmurs = Math
Q = V*A
Q = P/R
NR = d*D*V/n
Therefore:
Inc. P
Describing a heart murmur
1. Timing
murmurs are longer than heart sounds
HS can
Describing a heart murmur
1. Timing
murmurs are longer than heart sounds
HS can
Describing a heart murmur con’t:
4. Radiation
reflects the intensity of the murmur
Describing a heart murmur con’t:
4. Radiation
reflects the intensity of the murmur
Describing a heart murmur con’t:
6. Pitch
high, medium, low
7. Quality
blowing, harsh, rumbling,
Describing a heart murmur con’t:
6. Pitch
high, medium, low
7. Quality
blowing, harsh, rumbling,
Systolic Murmurs
Derived from increased turbulence associated with:
1. Increased flow across normal
Systolic Murmurs
Derived from increased turbulence associated with:
1. Increased flow across normal
Early Systolic murmurs
1. Acute severe mitral regurgitation
decrescendo murmur
best heard at apical
Early Systolic murmurs
1. Acute severe mitral regurgitation
decrescendo murmur
best heard at apical
Midsystolic (ejection) murmurs
Are the most common kind of heart murmur
Are usually
Midsystolic (ejection) murmurs
Are the most common kind of heart murmur
Are usually
Aortic stenosis
Loudest in aortic area; radiates along the carotid arteries
Intensity varies
Aortic stenosis
Loudest in aortic area; radiates along the carotid arteries
Intensity varies
Hypertrophic cardiomyopathy
Loudest b/t left sternal edge and apex; Grade 2-3/6
Does NOT
Hypertrophic cardiomyopathy
Loudest b/t left sternal edge and apex; Grade 2-3/6
Does NOT
Pansystolic (Holosystolic) Murmurs
Are pathologic
Murmur begins immediately with S1 and continues up
Pansystolic (Holosystolic) Murmurs
Are pathologic
Murmur begins immediately with S1 and continues up
Diastolic Murmurs
Almost always indicate heart disease
Two basic types:
1. Early decrescendo diastolic
Diastolic Murmurs
Almost always indicate heart disease
Two basic types:
1. Early decrescendo diastolic
Aortic Regurgitation
Best heard in the 2nd ICS at the left sternal
Aortic Regurgitation
Best heard in the 2nd ICS at the left sternal
Mitral Stenosis
Two components:
1. Middiastolic - during rapid ventricular filling
2. Presystolic -
Mitral Stenosis
Two components:
1. Middiastolic - during rapid ventricular filling
2. Presystolic -
Continuous Murmurs
Begin in systole, peak near s2, and continue into all
Continuous Murmurs
Begin in systole, peak near s2, and continue into all
Back to the Basics
1. When does it occur - systole or
Back to the Basics
1. When does it occur - systole or
 История медицинского образования в России
История медицинского образования в России Балалардың ішкі ағзаларын пальпациялау
Балалардың ішкі ағзаларын пальпациялау Современный взгляд на проблему множественной миеломы
Современный взгляд на проблему множественной миеломы Dental clinics
Dental clinics Менингококковая инфекция
Менингококковая инфекция Современные методы нейродиагностики. МРТ для животных
Современные методы нейродиагностики. МРТ для животных Гендік инженерия және маркерлік гендер
Гендік инженерия және маркерлік гендер Скелетные мышцы. Общие закономерности строения и функций
Скелетные мышцы. Общие закономерности строения и функций Операции на сосудах, нервах и сухожилиях конечностей
Операции на сосудах, нервах и сухожилиях конечностей Руководство по надзору за ОВП: определение случая, эпидемиологическое расследование
Руководство по надзору за ОВП: определение случая, эпидемиологическое расследование Экстрапирамида жүйесінің тұқым қуалайтын аурулары
Экстрапирамида жүйесінің тұқым қуалайтын аурулары Нарушения памяти при локальных поражениях мозга
Нарушения памяти при локальных поражениях мозга Безопасная больничная среда. Дезинфекция
Безопасная больничная среда. Дезинфекция Рослини жовчогінної та сечогінної дії. Тема № 7
Рослини жовчогінної та сечогінної дії. Тема № 7 Көздің онкологиялық аурулары. Ретинобластома және тор қабықтың меланомасы
Көздің онкологиялық аурулары. Ретинобластома және тор қабықтың меланомасы Основы трансплантологии
Основы трансплантологии Постепенная потеря зрения
Постепенная потеря зрения Heart failure
Heart failure Возбудители туберкулеза, микобактериозов, лепры
Возбудители туберкулеза, микобактериозов, лепры Табиғи және техногенді радияциялық фон. Иондық сәулелену көзінің адам ағзасына әсерінің салдары
Табиғи және техногенді радияциялық фон. Иондық сәулелену көзінің адам ағзасына әсерінің салдары Фармакологія антибіотиків, противірусних та протигрибкових засобів
Фармакологія антибіотиків, противірусних та протигрибкових засобів Общие закономерности строения и функций
Общие закономерности строения и функций Поражающие факторы ядерного взрыва, их характеристика, влияние на организм человека
Поражающие факторы ядерного взрыва, их характеристика, влияние на организм человека Обзор клинического случая. Острый коронарный синдром
Обзор клинического случая. Острый коронарный синдром Sexually transmitted bacterial diseases
Sexually transmitted bacterial diseases Проблема часто болеющих детей. Организация диспансерного наблюдения и реабилитация часто болеющих детей
Проблема часто болеющих детей. Организация диспансерного наблюдения и реабилитация часто болеющих детей Нарушения водно-электролитного обмена
Нарушения водно-электролитного обмена Естің бұзылысы
Естің бұзылысы