- Inflammatory Bowel Diseases

Содержание
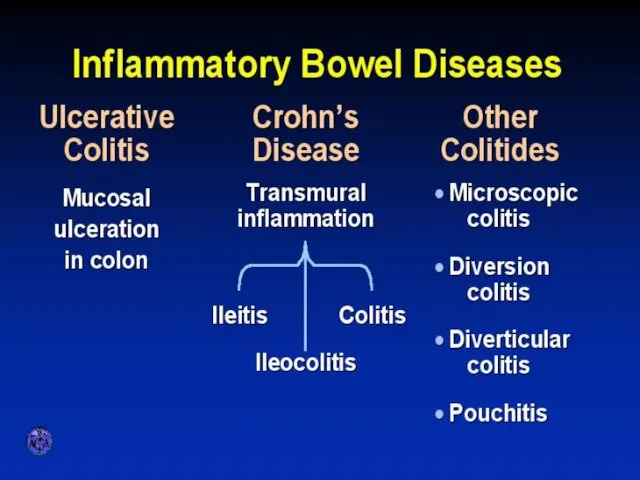
- 2. INFLAMMATORY BOWEL DISEASES
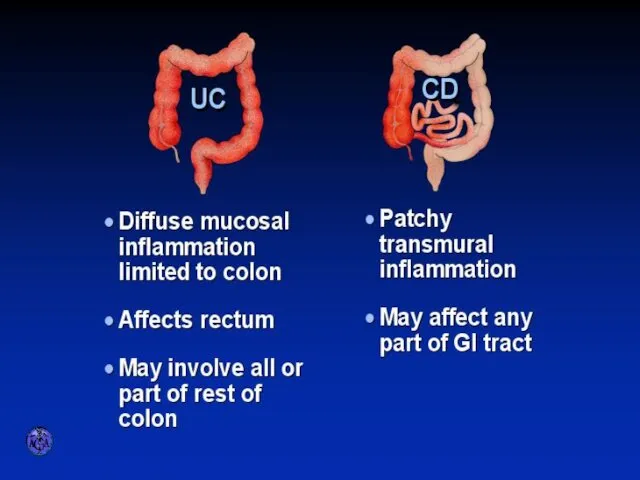
- 3. ULCERATIVE COLITIS AND CROHN’S DISEASE
- 5. Etiology and Pathogenesis Genetically predisposed individuals Chronic activation of the mucosal immune system may represent an
- 6. Genetic Considerations CARD15 senses bacterial muramyl dipeptide and regulates intracellular signaling expressed by intestinal epithelial cells,
- 7. VARIETIES OF COLITIS
- 8. DIFFERENTIAL DIAGNOSIS OF INFECTIOUS AND ULCERATIVE COLITIS
- 9. DIFFERENTIAL DIAGNOSIS OF IBD AND IBS
- 10. CHARACTERISTIC FEATURES OF ULCERATIVE COLITIS
- 11. Pathology Ulcerative Colitis: Macroscopic Features mucosal disease that usually involves the rectum and extends proximally to
- 12. UC Physical findings Abdomen: tenderness and distension, but can be normal Extra colonic: arthritis, skin changes
- 13. UC Laboratory findings No specific findings ESR ↑, CRP ↑, anemia (chronic disease, Fe↓), WBC ↑
- 14. UC Clinical Features Relapsing disease (~ 80% 1yr) Symptoms usually parallel disease extent (More disease→more systemic
- 15. UC- Complications Bleeding Perforation Toxicity Cancer
- 17. Crohn’s disease (CD) Transmural disease, symptoms depend on site of involvement and complications Abdominal pain, diarrhea
- 18. ANATOMIC DISTRIBUTION Terminal ileum is involved in 75%
- 19. CD Small bowel Abdominal pain (mainly RLQ), may be constant and dull, may be colicky (obstruction)
- 20. CD Colon Colon: diarrhea, less rectal bleeding (less colon & rectum involved), characteristic rectal sparing. Perianal
- 21. CD Perianal Disease Fissures Fistulas Perirectal abscess
- 22. CD Pathology Macroscopic Features terminal ileum is involved in 75% the rectum is often spared in
- 23. VIENNA CLASSIFICATION
- 24. CLINICAL PATTERNS
- 25. FISTULIZATION
- 26. CONFINED PERFORATION
- 27. Natural history of CD accumulation of disease complications 2065 pts Follow up 1974-2000 Kaplan-Meier estimates of
- 28. APPROACH TO DIFFERENTIAL DIAGNOSIS OF ULCERATIVE VERSUS CROHN’S COLITITS
- 29. Extraintestinal Manifestations Arthritis - Peripheral -dependent on disease activity - Axial-independent of disease activity Ocular -
- 30. Extra-intestinal manifestations, co-morbidities and complications of CD Uveitis1 Pyoderma gangrenosum2,3 Psoriasis4 Spondyloarthropathy5
- 31. Extraintestinal Manifestations Rheumatologic Peripheral arthritis- 15–20% of IBD patients more common in CD worsens with exacerbations
- 32. Extraintestinal Manifestations Rheumatologic Sacroilitis Symmetric equally in UC and CD often asymptomatic does not correlate with
- 33. Extraintestinal manifestations - Skin Pyoderma gangrenosum- more in UC patients may occur years before the onset
- 35. Extraintestinal Manifestations - Skin - Erythema nodosum (15% of CD patients and 10% of UC patients)
- 36. Erythema nodosum
- 37. Extraintestinal Manifestations Ocular: The most common are conjunctivitis, anterior uveitis/iritis, and episcleritis Uveitis is associated with
- 38. Extraintestinal Manifestations Urologic calculi, ureteral obstruction, and fistulas nephrolithiasis (10–20%) occurs in patients with CD hyperoxaluria
- 39. Extraintestinal Manifestations Thromboembolic Disorders increased risk of both venous and arterial thrombosis Other Disorders cardiopulmonary manifestations:
- 40. Diagnosis History - How long? - How bad: no. of stools? Blood? Signs of rectal involvement
- 41. Diagnosis Laboratory tests- non specific and reflect disease severity & involvement Anemia- normocytic normochromic (chronic disease),
- 42. Diagnosis Stool: Steatorrhea (mild), WBC in stool, Increased calprotectin Disturbed Liver function tests (Alk. P- PSC,
- 43. Diagnosis Determine anatomic involvement Determine nature of involvement (UC Vs CD Vs others)
- 44. Diagnosis Endoscopic examinations: Rectosigmoidoscopy- rectum? Mucosal morphology? (ulcer type, skip areas) Colonoscopy- Same + disease extent
- 45. ENDOSCOPIC SPECTRUM OF SEVERITY
- 46. Tissue inflammatory infiltration by lymphocytes, plasma cells, and neutrophils with large lymphoid aggregates Cryptitis and crypt
- 47. ENDOSCOPIC APPEARANCES CD aphthae stellate ulcer longitudinal ulcer Macroulcerations and pseudoplyps
- 48. Diagnosis Radiology Barium enema: fistula, sinus tract, stricturing (not used today) Small bowel follow through- small
- 49. TRANSVERSE COLON STRICTURE
- 50. SPECTRUM OF ILEITIS marked edema and nodularity in addition to ulceration narrowing and spasm deeper ulceration+
- 51. Diagnosis CT – replaced SBFT, allows for detection of extramural complications ( abscess, fistula, retroperitoneal disease)
- 52. CT can asses inflammation, bowel wall thikening, fat, strictures and fistula Abdominal CT in IBD Diagnosis
- 53. DISTINGUISHING FEATURES OF CROHN’S DISEASE
- 54. GOALS OF THERAPY
- 55. CONVENTIONAL DRUG THERAPIES Biologics Anti- TNF Anti-cytokine Anti Migration
- 56. SULFASALAZINE
- 57. AMINOSALICYLATES
- 58. AMINOSALICYLATE DISTRIBUTION
- 59. STEROID PREPARATIONS Systemic / Topical
- 61. Immuno-suppressors in IBD Azathioprine, 6-Mercaptopurine Methotrexate Cyclosporin Tacrolimus
- 63. Side effects thiopurines (cont.) Small increased risk of developing lymphoma Increased risk of non- melanoma skin
- 64. TOXICITY OF CYCLOSPORINE
- 65. Chronic Inflammation: Imbalance Between Mediators
- 66. Migration of Cells into Tissues E, P Selectins Mucosa ACTIVATION ARREST ROLLING TRANSMIGRATION
- 67. Biologicals Anti TNF agents: - Infliximab (Remicade), Adalimumab (Humera), Golimumab (Simponi) Anti migration: - Natalizumab -
- 68. Chimerized and Humanized Antibodies
- 69. Infliximab Mechanism of Action
- 70. Integrin Structure β 1,7 α 4 Plasma membrane
- 71. ADVERSE EFFECTS OF INFLIXIMAB
- 72. Biologicals: Pre-therapy preparations TB exposure: Skin test/quatiferon + Rx HBV, HIV, Varicella exposure Immunize: Pneumovax, Influenza
- 73. Diagnosis
- 74. UC Active Disease Highly Active Mild-Moderate Remission Extent of Disease
- 75. Main clinical points to address Factors that affect treatment choice: - Disease distribution (proctitis, left sided,
- 76. Patient assessment Exclusion of infectious agents: STD in proctitis Bacterial (including C. Diff) and parasitic infections
- 77. Outpatient assessment of the severity of active UC: T&W- Important not to miss severe progressive disease
- 78. UC - Mild to moderate activity 5-ASA/SZP: Both induction of remission and maintenance Dose – dependent
- 79. UC - Left sided & Pan colitis Mild to moderate activity If steroid dependent: Azathioprine/ 6-MP
- 80. Severe UC Prevalence ~ 20% for first and recurrent attacks Severe active UC with systemic toxicity
- 81. Severe UC Correct: Hypokalemia, hypomagnesemia (toxic dilatation ↑) Hemoglobin Nutritional support (complications enteral Vs parenteral 9%
- 83. Active UC Mild Steroids, AZA, 6-MP, Infliximab IV steroids, cyclosporine Infliximab Surgery Remission 5-ASA, AZA, 6-MP,
- 84. CD
- 85. CD- Colon Mild -Moderate SZP-/5-ASA for colonic disease only Side effects: paradoxical diarrhea, nausea, vomiting, headache,
- 86. CD-Small Bowel Steroids: Generally try to avoid due to side effects Controlled trials show definite efficacy
- 87. CD – Moderate Activity Immunosuppressive agents Azathioprine, 6 MP Steroid dependent or resistant disease Steroid sparing
- 88. CD-Moderate Disease Methotrexate IM - 40% efficiency for 16 wks Reduced Steroid use Max efficiency -
- 89. INFLIXIMAB IN ACTIVE CROHN’S DISEASE Anti TNF therapy in Crohn’s disease
- 90. Biologicals No difference between Infliximab and Adalimumab for efficacy Different modes of administration Loading, scheduled therapy
- 91. CD- Severe Disease Hospitalization IV steroids If abscess, fistula- drain, consider TPN Anti TNF Abs
- 92. CD- Effect of Disease Type Perianal & fistula: Antibiotics Azathioprine/6 MP Infliximab Surgery Treatment sequence: Image,
- 93. CD- Effect of Disease Type Fibrostenotic disease - Need to differentiate inflammation/scare If scare: surgery Medical
- 94. CD- Maintenance of Remission Not Steroids ! 5-ASA: low efficiency (1:13), SE ↓ May benefit post
- 95. CD- Maintenance of Remission Immunomodulatory drugs Azathioprine/6MP: efficient regardless of therapy mode MTX: Good for pts
- 96. Active CD Colon: 5ASA/SZP SB: Budesonide Steroids Prednisone/Budesonide Immunomodulatory agents AZA/6MP MTX Infliximab Surgery when indicated
- 97. CD in Remission Medical Immunomodulation AZA/6MP/MTX Infliximab
- 98. The evolution of therapy: Should we invert the pyramid? Which patients should be treated with anti-TNF?
- 99. Future evolution Should we aim for mucosal healing? Should we perform early surgery? Risk / benefit
- 100. Case Study 30-year-old woman was admitted with a 4-week history of increasing bloody diarrhea and abdominal
- 101. Case Study The rectal biopsy : many crypt abscesses were present. The lamina propria contained a
- 102. י.ע. 9/2011 בת 54, מזה כחודש וחצי סובלת משלשולים רבים, יציאות דמיות וריריות לסירוגין, ירידה במשקל
- 103. אושפזה בפנימית להמשך בירור וטיפול. בקבלתה הוחל טיפול בסטרואידים ורפסל.במהלך אשפוזה שיפור ניכר בתלונות. לאחר 3
- 104. באשפוז הקודם הותחל גם טיפול גם ב6-MP. שוחחתי ארוכות עם החולה ובעלה אודות הסיכונים שבטיפול זה
- 105. י.ע. 18/10/2011 הגיעה לביקורת, טופלה עד כה בפרדניזון עם ירידה הדרגתית וסיימה לפני שבועיים. בנוסף הותחל
- 106. י.ע. 26/12/2011 שני אשפוזים בפנימית: פעם אחת בשל החמרה שטופלה בסטרואידים, פעם שניה בשל מחלת ריאות
- 107. י.ע. 23/7/2012 מזה 4 ימים עלייה בתדירות היציאות, 6-7 ליום, חלקן עם דם. כאבי בטן מטרימים.
- 109. Скачать презентацию
INFLAMMATORY BOWEL DISEASES
INFLAMMATORY BOWEL DISEASES
ULCERATIVE COLITIS AND CROHN’S DISEASE
ULCERATIVE COLITIS AND CROHN’S DISEASE
Etiology and Pathogenesis
Genetically predisposed individuals
Chronic activation of the mucosal immune system
Etiology and Pathogenesis
Genetically predisposed individuals
Chronic activation of the mucosal immune system
Genetic Considerations
CARD15
senses bacterial muramyl dipeptide and regulates intracellular signaling
expressed by
Genetic Considerations
CARD15
senses bacterial muramyl dipeptide and regulates intracellular signaling
expressed by
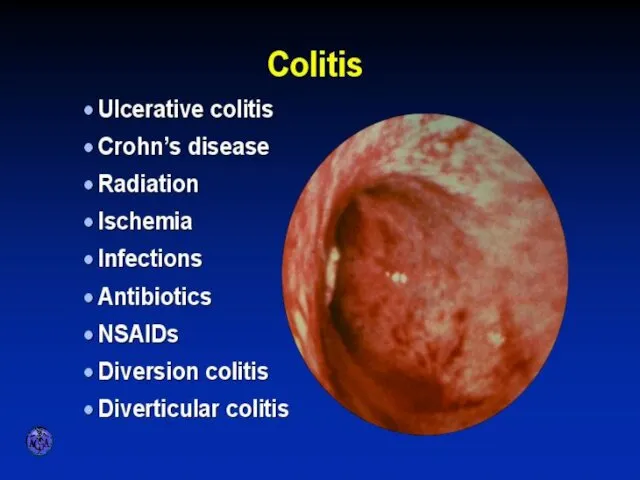
VARIETIES OF COLITIS
VARIETIES OF COLITIS
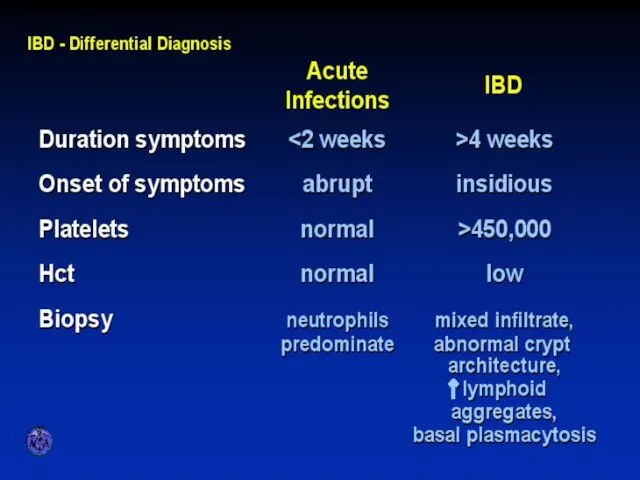
DIFFERENTIAL DIAGNOSIS OF INFECTIOUS AND ULCERATIVE COLITIS
DIFFERENTIAL DIAGNOSIS OF INFECTIOUS AND ULCERATIVE COLITIS
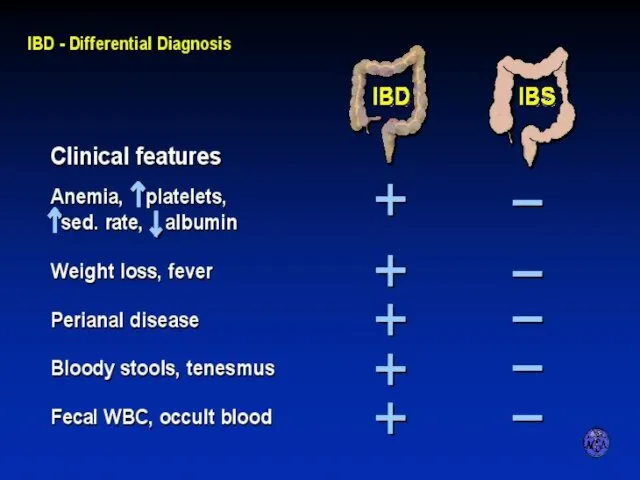
DIFFERENTIAL DIAGNOSIS OF IBD AND IBS
DIFFERENTIAL DIAGNOSIS OF IBD AND IBS
CHARACTERISTIC FEATURES OF ULCERATIVE COLITIS
CHARACTERISTIC FEATURES OF ULCERATIVE COLITIS
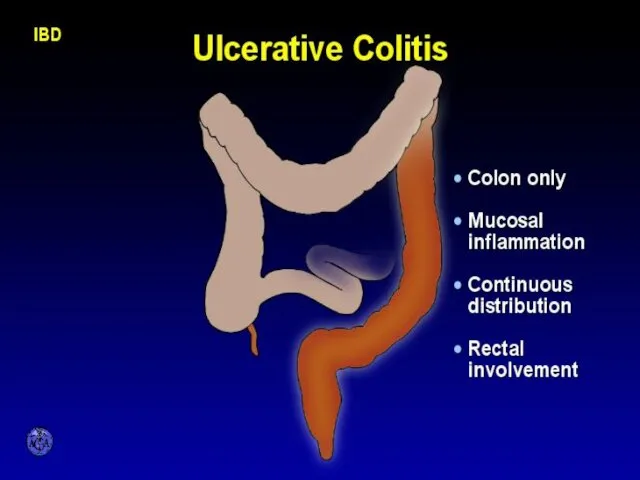
Pathology
Ulcerative Colitis: Macroscopic Features
mucosal disease that usually involves the rectum and
Pathology
Ulcerative Colitis: Macroscopic Features
mucosal disease that usually involves the rectum and
UC Physical findings
Abdomen: tenderness and distension, but can be normal
Extra
UC Physical findings
Abdomen: tenderness and distension, but can be normal
Extra
UC Laboratory findings
No specific findings
ESR ↑, CRP ↑, anemia (chronic disease,
UC Laboratory findings
No specific findings
ESR ↑, CRP ↑, anemia (chronic disease,
UC Clinical Features
Relapsing disease (~ 80% 1yr)
Symptoms usually parallel disease extent
(More
UC Clinical Features
Relapsing disease (~ 80% 1yr)
Symptoms usually parallel disease extent
(More
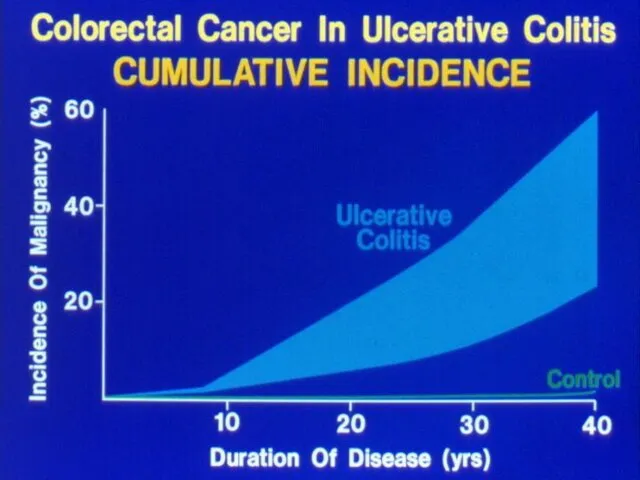
UC- Complications
Bleeding
Perforation
Toxicity
Cancer
UC- Complications
Bleeding
Perforation
Toxicity
Cancer
Crohn’s disease (CD)
Transmural disease, symptoms depend on site of involvement and
Crohn’s disease (CD)
Transmural disease, symptoms depend on site of involvement and
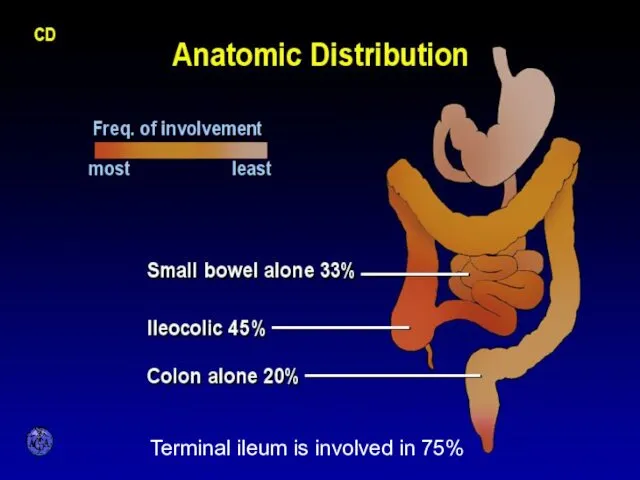
ANATOMIC DISTRIBUTION
Terminal ileum is involved in 75%
ANATOMIC DISTRIBUTION
Terminal ileum is involved in 75%
CD Small bowel
Abdominal pain (mainly RLQ), may be constant and dull,
CD Small bowel
Abdominal pain (mainly RLQ), may be constant and dull,
CD Colon
Colon: diarrhea, less rectal bleeding (less colon & rectum involved),
CD Colon
Colon: diarrhea, less rectal bleeding (less colon & rectum involved),
CD Perianal Disease
Fissures
Fistulas
Perirectal abscess
CD Perianal Disease
Fissures
Fistulas
Perirectal abscess
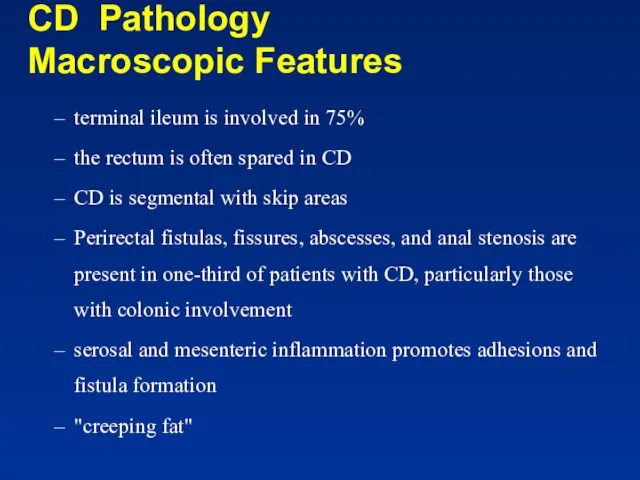
CD Pathology
Macroscopic Features
terminal ileum is involved in 75%
the
CD Pathology
Macroscopic Features
terminal ileum is involved in 75%
the
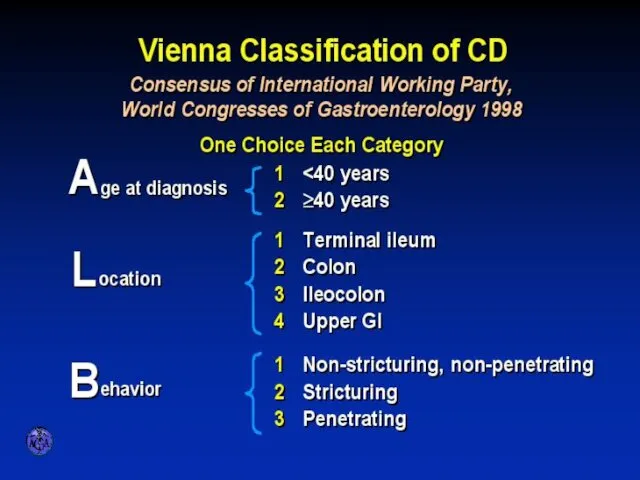
VIENNA CLASSIFICATION
VIENNA CLASSIFICATION
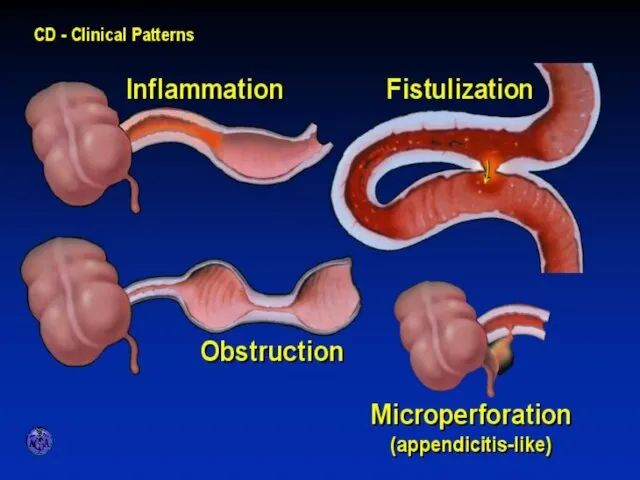
CLINICAL PATTERNS
CLINICAL PATTERNS
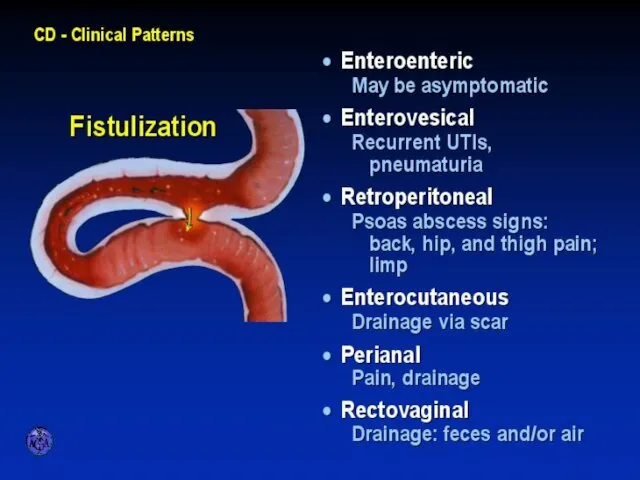
FISTULIZATION
FISTULIZATION
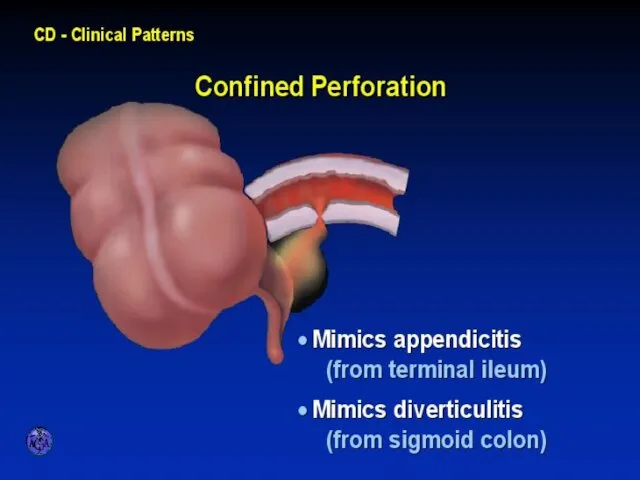
CONFINED PERFORATION
CONFINED PERFORATION
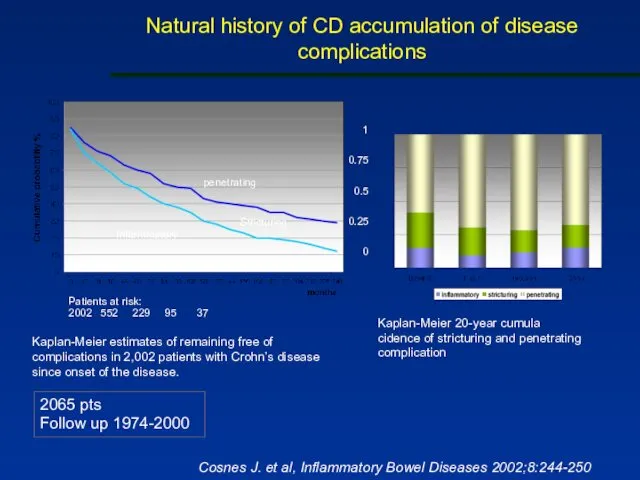
Natural history of CD accumulation of disease complications
2065 pts
Follow
Natural history of CD accumulation of disease complications
2065 pts Follow
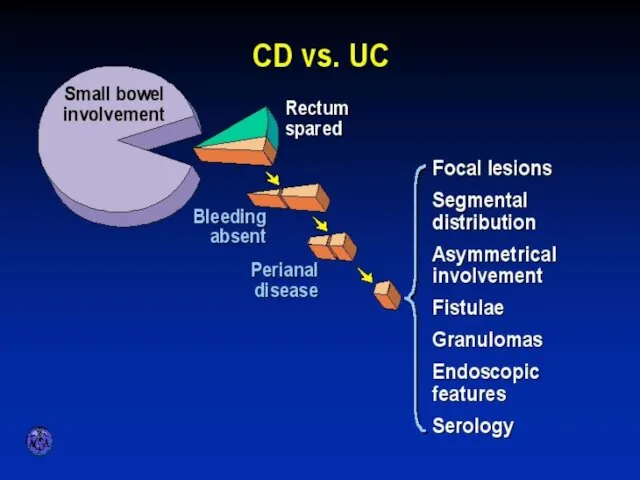
APPROACH TO DIFFERENTIAL DIAGNOSIS OF ULCERATIVE VERSUS CROHN’S COLITITS
APPROACH TO DIFFERENTIAL DIAGNOSIS OF ULCERATIVE VERSUS CROHN’S COLITITS
Extraintestinal Manifestations
Arthritis
- Peripheral -dependent on disease activity
- Axial-independent of disease activity
Ocular
-
Extraintestinal Manifestations
Arthritis
- Peripheral -dependent on disease activity
- Axial-independent of disease activity
Ocular
-
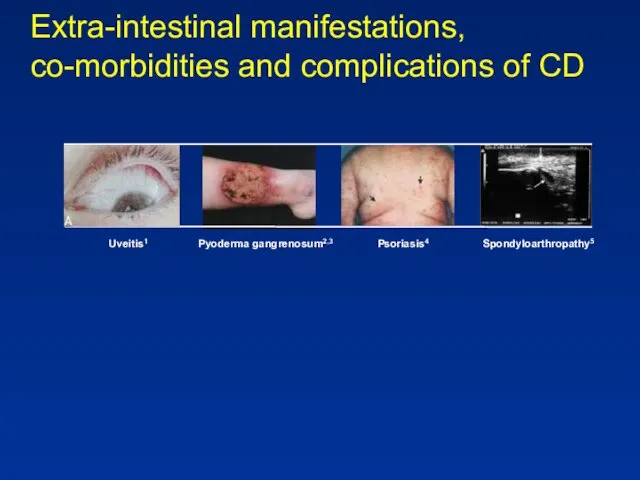
Extra-intestinal manifestations, co-morbidities and complications of CD
Uveitis1
Pyoderma gangrenosum2,3
Psoriasis4
Spondyloarthropathy5
Extra-intestinal manifestations, co-morbidities and complications of CD
Uveitis1
Pyoderma gangrenosum2,3
Psoriasis4
Spondyloarthropathy5
Extraintestinal Manifestations Rheumatologic
Peripheral arthritis- 15–20% of IBD patients
more common in
Extraintestinal Manifestations Rheumatologic
Peripheral arthritis- 15–20% of IBD patients
more common in
Extraintestinal Manifestations Rheumatologic
Sacroilitis
Symmetric
equally in UC and CD
often asymptomatic
does not correlate with
Extraintestinal Manifestations Rheumatologic
Sacroilitis
Symmetric
equally in UC and CD
often asymptomatic
does not correlate with
Extraintestinal manifestations - Skin
Pyoderma gangrenosum- more in UC patients
may occur
Extraintestinal manifestations - Skin
Pyoderma gangrenosum- more in UC patients
may occur

Extraintestinal Manifestations - Skin
- Erythema nodosum (15% of CD patients
Extraintestinal Manifestations - Skin
- Erythema nodosum (15% of CD patients

Erythema nodosum
Erythema nodosum
Extraintestinal Manifestations
Ocular:
The most common are conjunctivitis, anterior uveitis/iritis, and episcleritis
Uveitis
Extraintestinal Manifestations
Ocular:
The most common are conjunctivitis, anterior uveitis/iritis, and episcleritis
Uveitis
Extraintestinal Manifestations
Urologic
calculi, ureteral obstruction, and fistulas
nephrolithiasis (10–20%) occurs in patients
Extraintestinal Manifestations
Urologic
calculi, ureteral obstruction, and fistulas
nephrolithiasis (10–20%) occurs in patients
Extraintestinal Manifestations
Thromboembolic Disorders
increased risk of both venous and arterial thrombosis
Extraintestinal Manifestations
Thromboembolic Disorders
increased risk of both venous and arterial thrombosis
Diagnosis
History
- How long?
- How bad: no. of stools? Blood?
Signs
Diagnosis
History
- How long?
- How bad: no. of stools? Blood?
Signs
Diagnosis
Laboratory tests- non specific and reflect disease severity & involvement
Anemia-
Diagnosis
Laboratory tests- non specific and reflect disease severity & involvement
Anemia-
Diagnosis
Stool: Steatorrhea (mild), WBC in stool, Increased calprotectin
Disturbed Liver function tests
Diagnosis
Stool: Steatorrhea (mild), WBC in stool, Increased calprotectin
Disturbed Liver function tests
Diagnosis
Determine anatomic involvement
Determine nature of involvement
(UC Vs CD Vs others)
Diagnosis
Determine anatomic involvement
Determine nature of involvement
(UC Vs CD Vs others)
Diagnosis
Endoscopic examinations:
Rectosigmoidoscopy- rectum? Mucosal morphology? (ulcer type, skip areas)
Colonoscopy- Same +
Diagnosis
Endoscopic examinations: Rectosigmoidoscopy- rectum? Mucosal morphology? (ulcer type, skip areas) Colonoscopy- Same +
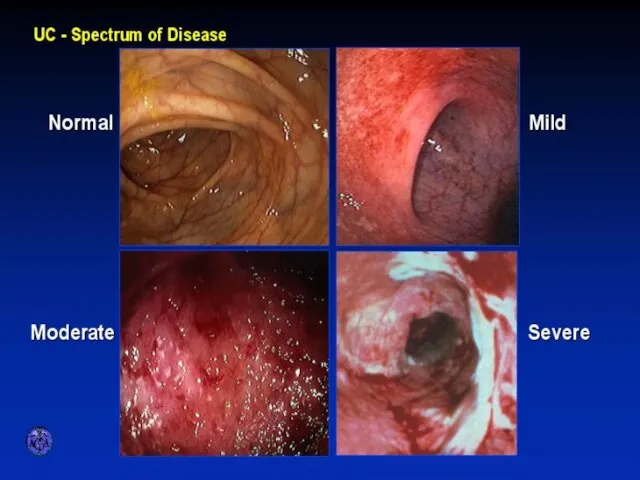
ENDOSCOPIC SPECTRUM OF SEVERITY
ENDOSCOPIC SPECTRUM OF SEVERITY
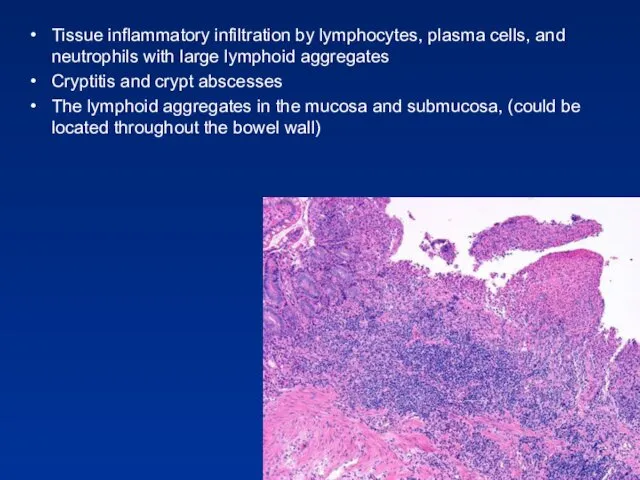
Tissue inflammatory infiltration by lymphocytes, plasma cells, and neutrophils with large
Tissue inflammatory infiltration by lymphocytes, plasma cells, and neutrophils with large

ENDOSCOPIC APPEARANCES
CD
aphthae
stellate ulcer
longitudinal ulcer
Macroulcerations and pseudoplyps
ENDOSCOPIC APPEARANCES
CD
aphthae
stellate ulcer
longitudinal ulcer
Macroulcerations and pseudoplyps
Diagnosis Radiology
Barium enema:
fistula, sinus tract, stricturing (not used today)
Small bowel
Diagnosis Radiology
Barium enema:
fistula, sinus tract, stricturing (not used today)
Small bowel
TRANSVERSE COLON STRICTURE
TRANSVERSE COLON STRICTURE
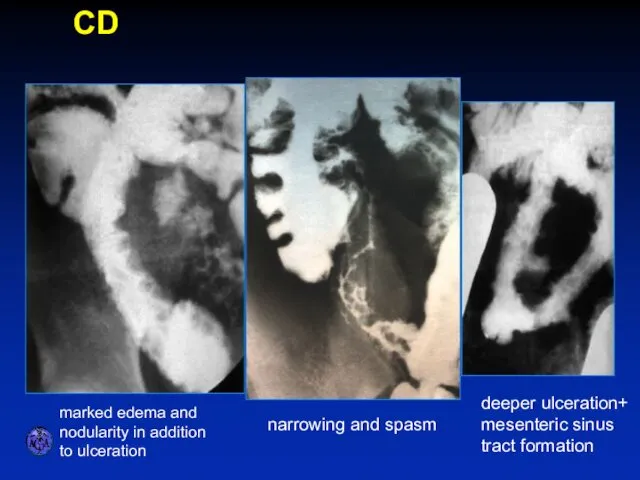
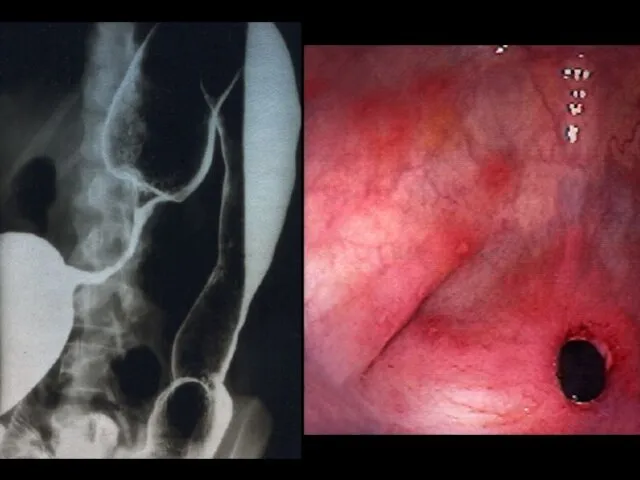
SPECTRUM OF ILEITIS
marked edema and nodularity in addition to ulceration
narrowing and
SPECTRUM OF ILEITIS
marked edema and nodularity in addition to ulceration
narrowing and
Diagnosis
CT – replaced SBFT, allows for detection of extramural complications
(
Diagnosis
CT – replaced SBFT, allows for detection of extramural complications (
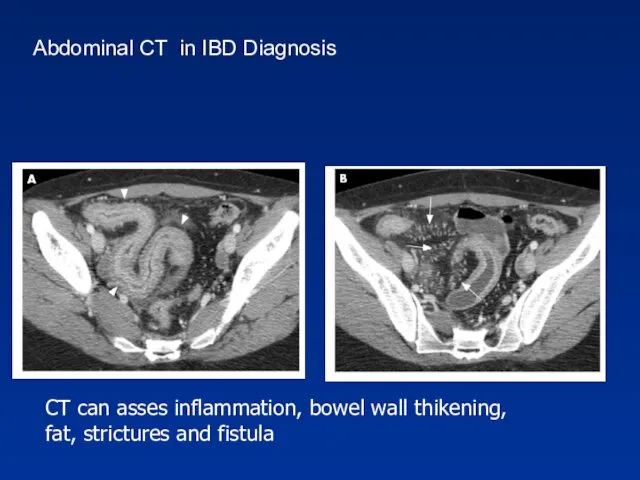
CT can asses inflammation, bowel wall thikening,
fat, strictures and fistula
Abdominal
CT can asses inflammation, bowel wall thikening,
fat, strictures and fistula
Abdominal
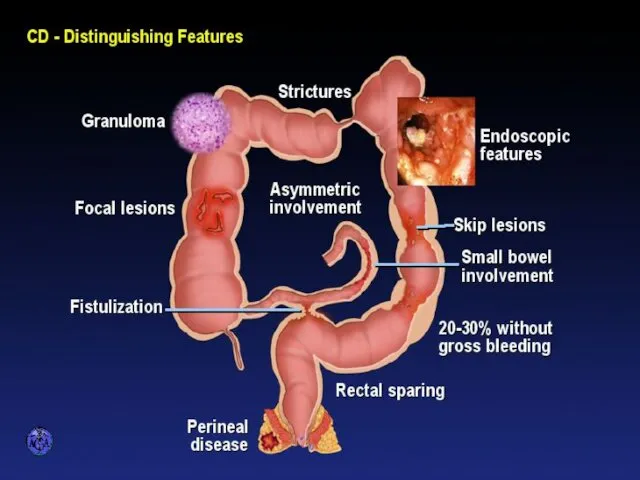
DISTINGUISHING FEATURES OF CROHN’S DISEASE
DISTINGUISHING FEATURES OF CROHN’S DISEASE
GOALS OF THERAPY
GOALS OF THERAPY
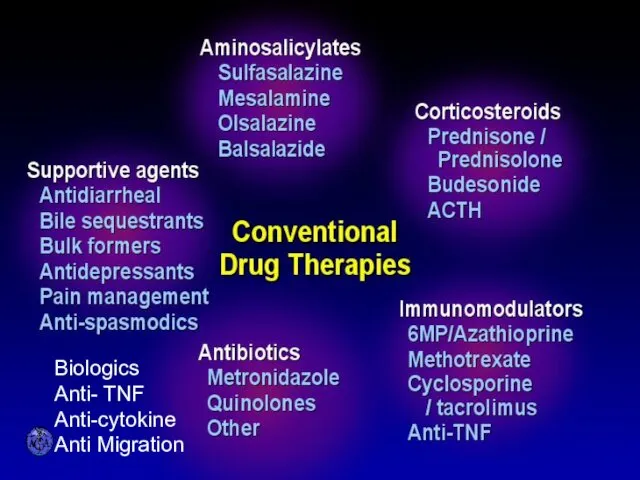
CONVENTIONAL DRUG THERAPIES
Biologics
Anti- TNF
Anti-cytokine
Anti Migration
CONVENTIONAL DRUG THERAPIES
Biologics
Anti- TNF
Anti-cytokine
Anti Migration
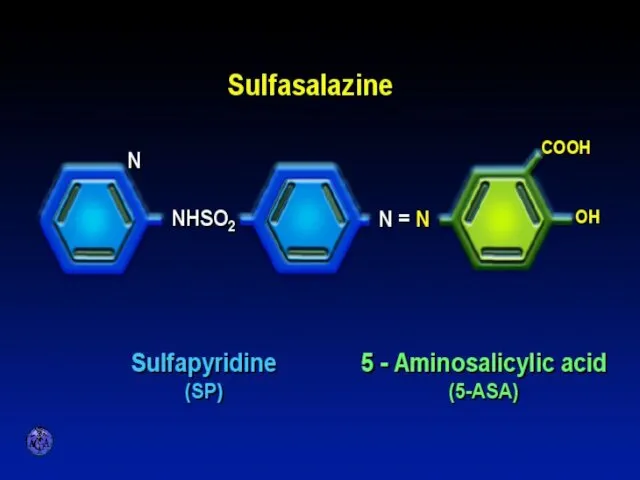
SULFASALAZINE
SULFASALAZINE
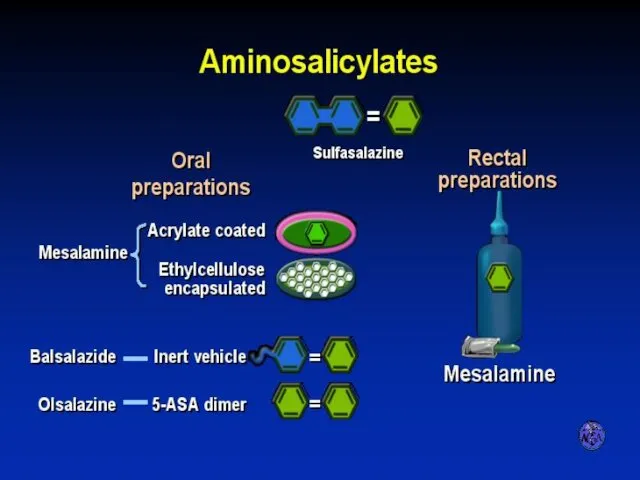
AMINOSALICYLATES
AMINOSALICYLATES
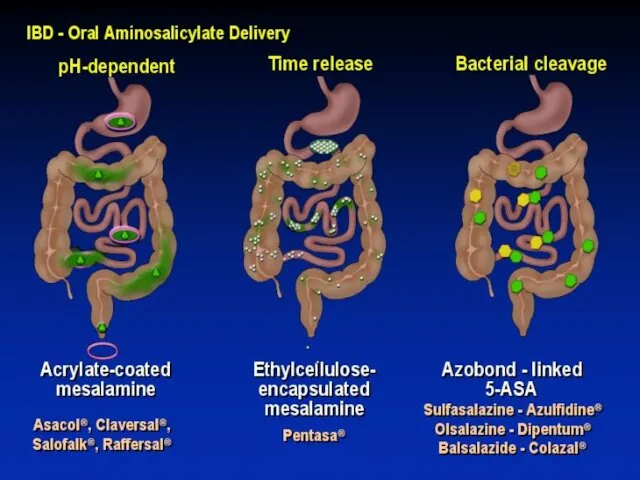
AMINOSALICYLATE DISTRIBUTION
AMINOSALICYLATE DISTRIBUTION
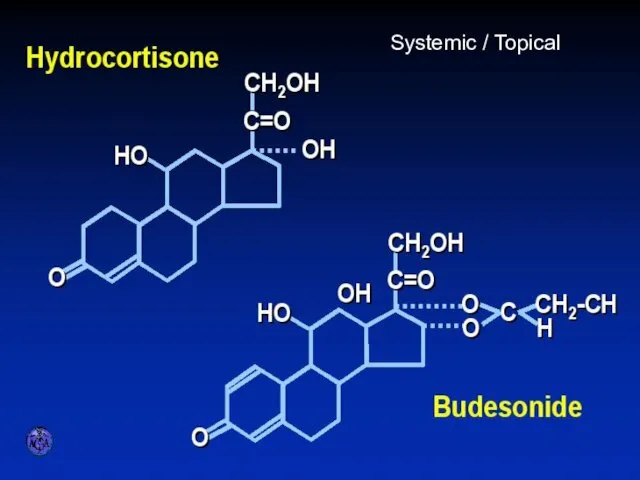
STEROID PREPARATIONS
Systemic / Topical
STEROID PREPARATIONS
Systemic / Topical
Immuno-suppressors in IBD
Azathioprine, 6-Mercaptopurine
Methotrexate
Cyclosporin
Tacrolimus
Immuno-suppressors in IBD
Azathioprine, 6-Mercaptopurine
Methotrexate
Cyclosporin
Tacrolimus
Side effects thiopurines (cont.)
Small increased risk of developing lymphoma
Increased risk of
Side effects thiopurines (cont.)
Small increased risk of developing lymphoma
Increased risk of
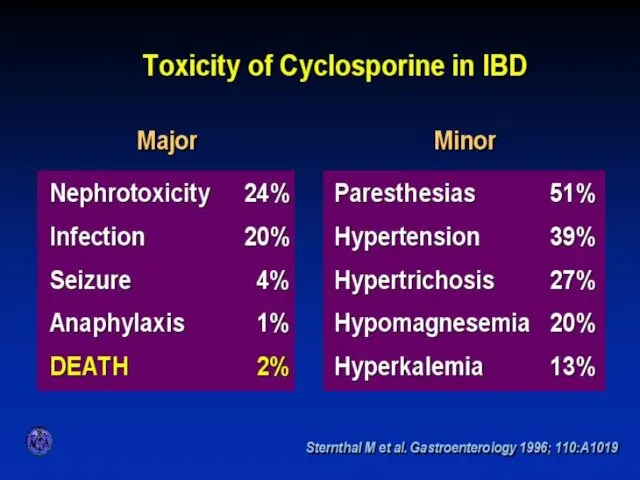
TOXICITY OF CYCLOSPORINE
TOXICITY OF CYCLOSPORINE
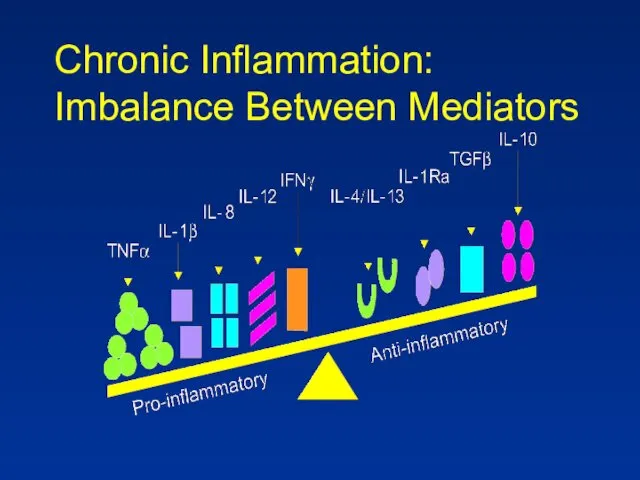
Chronic Inflammation:
Imbalance Between Mediators
Chronic Inflammation:
Imbalance Between Mediators
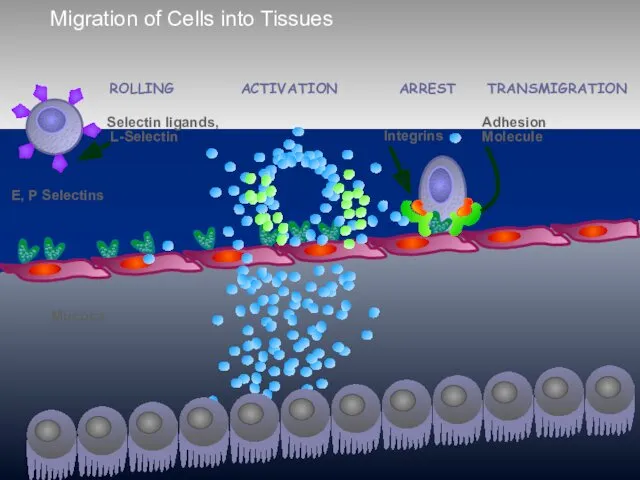
Migration of Cells into Tissues
E, P Selectins
Mucosa
ACTIVATION
ARREST
ROLLING
TRANSMIGRATION
Migration of Cells into Tissues
E, P Selectins
Mucosa
ACTIVATION
ARREST
ROLLING
TRANSMIGRATION
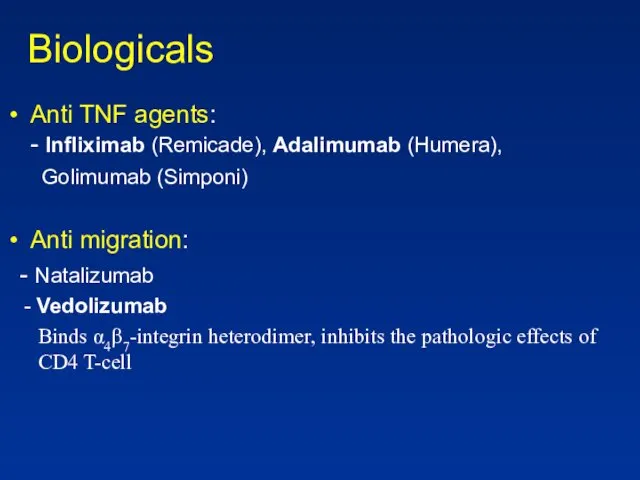
Biologicals
Anti TNF agents:
- Infliximab (Remicade), Adalimumab (Humera),
Golimumab (Simponi)
Anti
Biologicals
Anti TNF agents:
- Infliximab (Remicade), Adalimumab (Humera),
Golimumab (Simponi)
Anti
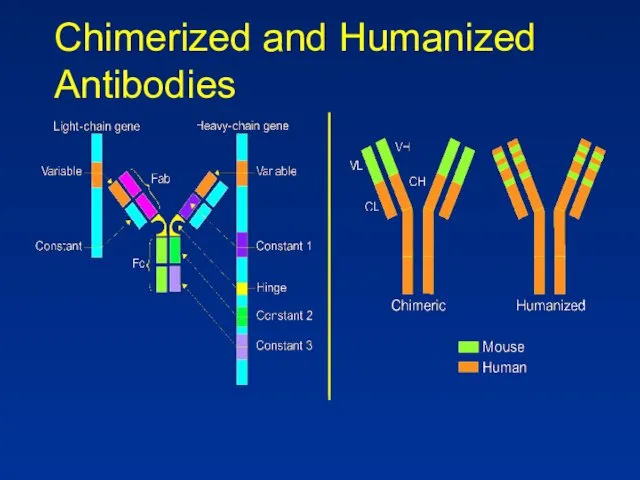
Chimerized and Humanized Antibodies
Chimerized and Humanized Antibodies
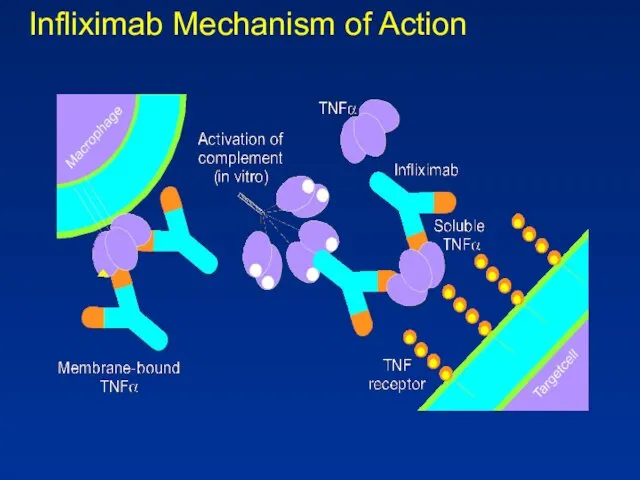
Infliximab Mechanism of Action
Infliximab Mechanism of Action
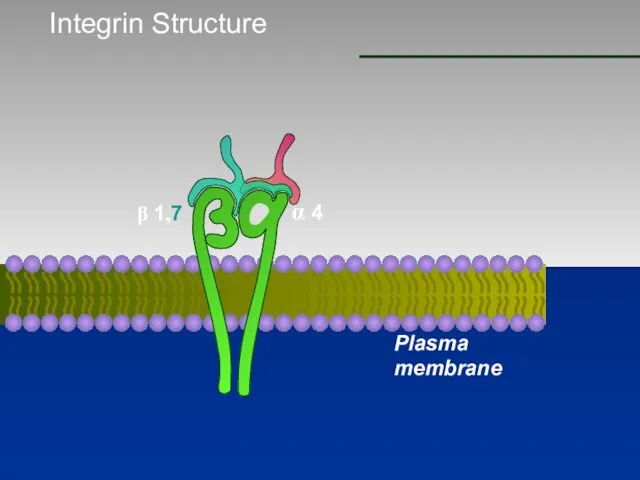
Integrin Structure
β 1,7
α 4
Plasma membrane
Integrin Structure
β 1,7
α 4
Plasma membrane
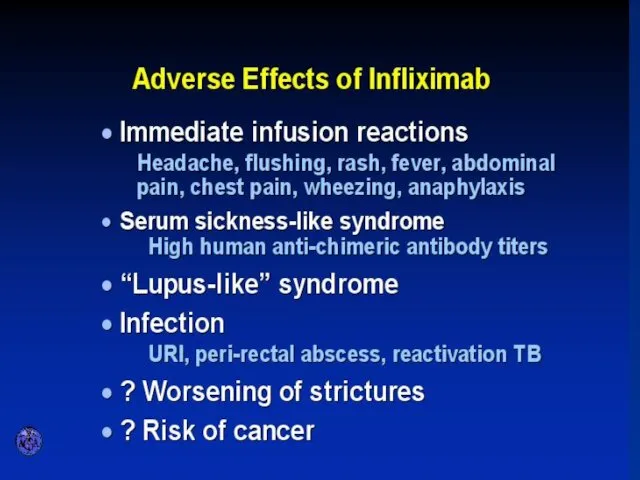
ADVERSE EFFECTS OF INFLIXIMAB
ADVERSE EFFECTS OF INFLIXIMAB
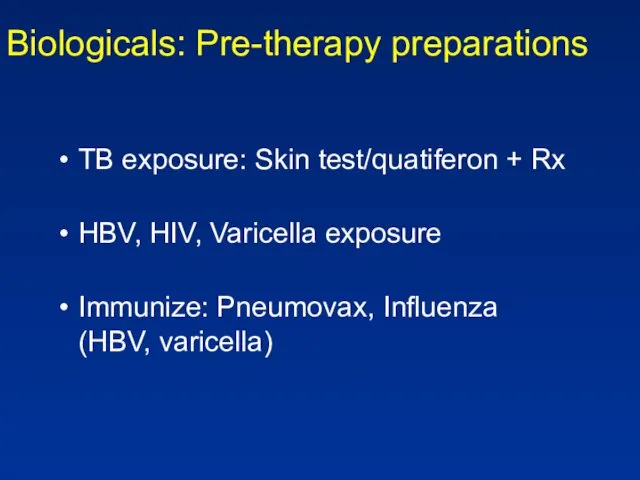
Biologicals: Pre-therapy preparations
TB exposure: Skin test/quatiferon + Rx
HBV, HIV, Varicella
Biologicals: Pre-therapy preparations
TB exposure: Skin test/quatiferon + Rx
HBV, HIV, Varicella
Diagnosis
Diagnosis
UC
Active Disease
Highly Active
Mild-Moderate
Remission
Extent of Disease
UC
Active Disease
Highly Active
Mild-Moderate
Remission
Extent of Disease
Main clinical points to address
Factors that affect treatment choice:
- Disease
Main clinical points to address
Factors that affect treatment choice: - Disease
Patient assessment
Exclusion of infectious agents:
STD in proctitis Bacterial (including
Patient assessment
Exclusion of infectious agents: STD in proctitis Bacterial (including
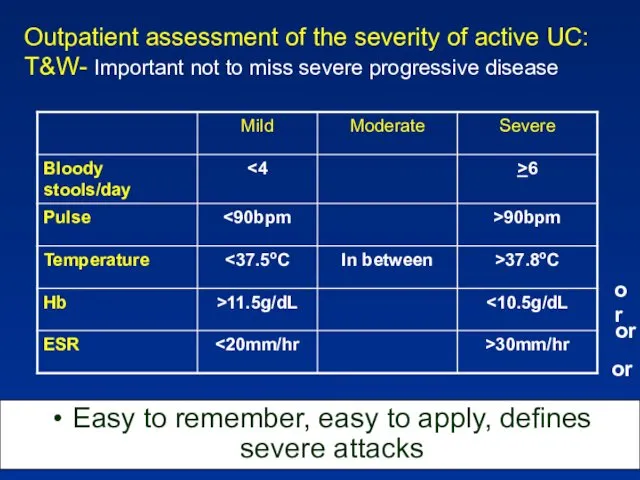
Outpatient assessment of the severity of active UC: T&W- Important not
Outpatient assessment of the severity of active UC: T&W- Important not
UC - Mild to moderate activity
5-ASA/SZP:
Both induction of remission and maintenance
UC - Mild to moderate activity
5-ASA/SZP: Both induction of remission and maintenance
UC - Left sided & Pan colitis
Mild to moderate activity
If
UC - Left sided & Pan colitis
Mild to moderate activity
If
Severe UC
Prevalence ~ 20% for first and recurrent attacks
Severe active UC
Severe UC
Prevalence ~ 20% for first and recurrent attacks
Severe active UC
Severe UC
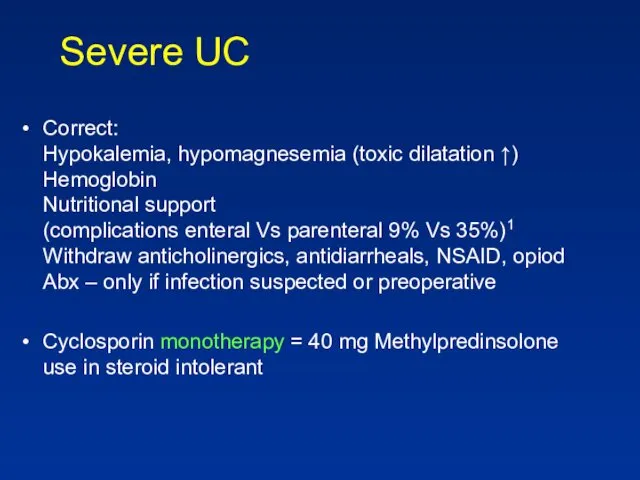
Correct:
Hypokalemia, hypomagnesemia (toxic dilatation ↑)
Hemoglobin
Nutritional support
(complications enteral Vs
Severe UC
Correct: Hypokalemia, hypomagnesemia (toxic dilatation ↑) Hemoglobin Nutritional support (complications enteral Vs
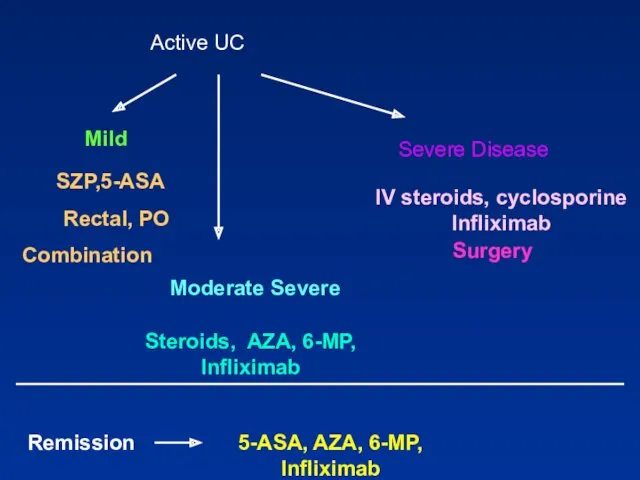
Active UC
Mild
Steroids, AZA, 6-MP, Infliximab
IV steroids, cyclosporine
Infliximab
Surgery
Remission
5-ASA, AZA, 6-MP, Infliximab
Active UC
Mild
Steroids, AZA, 6-MP, Infliximab
IV steroids, cyclosporine
Infliximab
Surgery
Remission
5-ASA, AZA, 6-MP, Infliximab
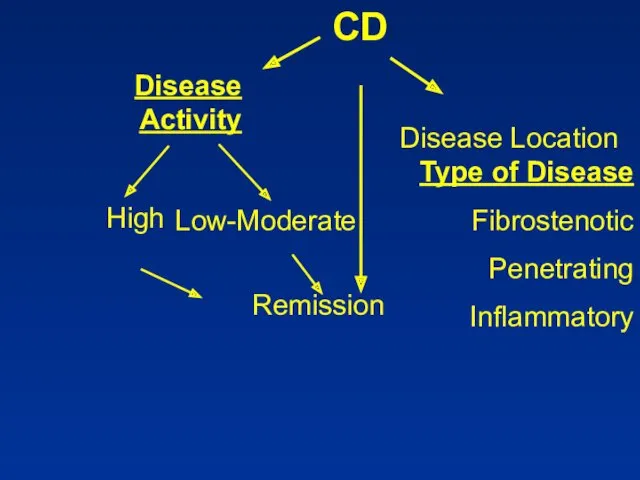
CD
CD
CD- Colon Mild -Moderate
SZP-/5-ASA for colonic disease only
Side effects: paradoxical
CD- Colon Mild -Moderate
SZP-/5-ASA for colonic disease only
Side effects: paradoxical
CD-Small Bowel
Steroids:
Generally try to avoid due to side effects
Controlled trials show
CD-Small Bowel
Steroids:
Generally try to avoid due to side effects
Controlled trials show
CD – Moderate Activity
Immunosuppressive agents
Azathioprine, 6 MP
Steroid dependent or resistant
CD – Moderate Activity
Immunosuppressive agents
Azathioprine, 6 MP
Steroid dependent or resistant
CD-Moderate Disease
Methotrexate
IM - 40% efficiency for 16 wks
Reduced Steroid use
Max
CD-Moderate Disease
Methotrexate
IM - 40% efficiency for 16 wks
Reduced Steroid use
Max
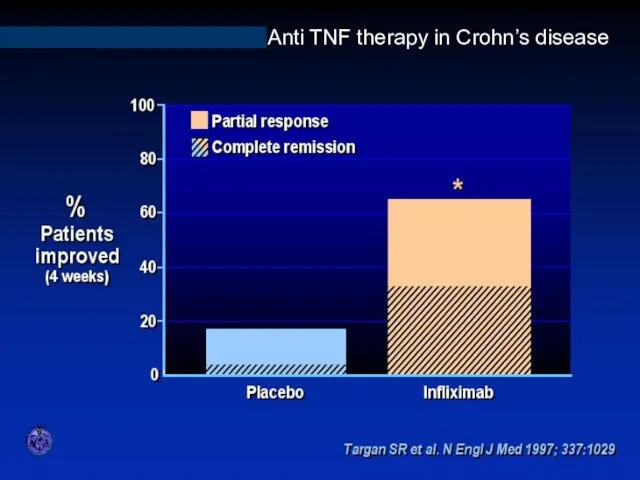
INFLIXIMAB IN ACTIVE CROHN’S DISEASE
Anti TNF therapy in Crohn’s disease
INFLIXIMAB IN ACTIVE CROHN’S DISEASE
Anti TNF therapy in Crohn’s disease
Biologicals
No difference between Infliximab and Adalimumab for efficacy
Different modes of administration
Biologicals
No difference between Infliximab and Adalimumab for efficacy
Different modes of administration
CD- Severe Disease
Hospitalization
IV steroids
If abscess, fistula- drain, consider TPN
Anti TNF Abs
CD- Severe Disease
Hospitalization
IV steroids
If abscess, fistula- drain, consider TPN
Anti TNF Abs
CD- Effect of Disease Type
Perianal & fistula:
Antibiotics
Azathioprine/6 MP
Infliximab
Surgery
Treatment sequence: Image,
CD- Effect of Disease Type
Perianal & fistula:
Antibiotics
Azathioprine/6 MP
Infliximab
Surgery
Treatment sequence: Image,
CD- Effect of Disease Type
Fibrostenotic disease
- Need to differentiate inflammation/scare
If
CD- Effect of Disease Type
Fibrostenotic disease
- Need to differentiate inflammation/scare
If
CD- Maintenance of Remission
Not Steroids !
5-ASA: low efficiency (1:13), SE
CD- Maintenance of Remission
Not Steroids !
5-ASA: low efficiency (1:13), SE
CD- Maintenance of Remission
Immunomodulatory drugs
Azathioprine/6MP: efficient regardless of therapy mode
MTX: Good
CD- Maintenance of Remission
Immunomodulatory drugs
Azathioprine/6MP: efficient regardless of therapy mode
MTX: Good
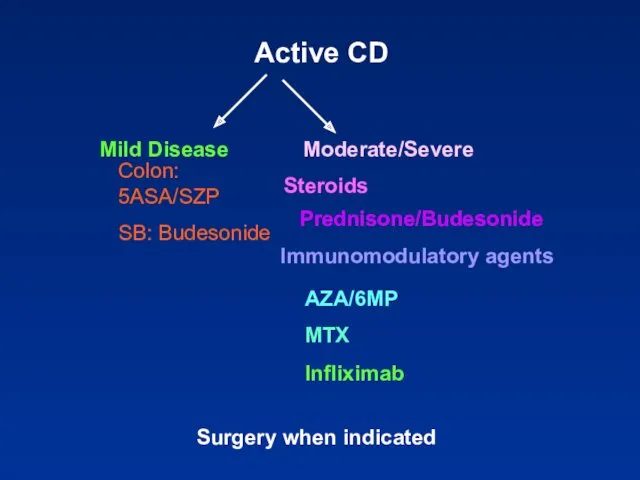
Active CD
Colon: 5ASA/SZP
SB: Budesonide
Steroids
Prednisone/Budesonide
Immunomodulatory agents
AZA/6MP
MTX
Infliximab
Surgery when indicated
Active CD
Colon: 5ASA/SZP
SB: Budesonide
Steroids
Prednisone/Budesonide
Immunomodulatory agents
AZA/6MP
MTX
Infliximab
Surgery when indicated
CD in Remission
Medical
Immunomodulation
AZA/6MP/MTX
Infliximab
CD in Remission
Medical
Immunomodulation
AZA/6MP/MTX
Infliximab
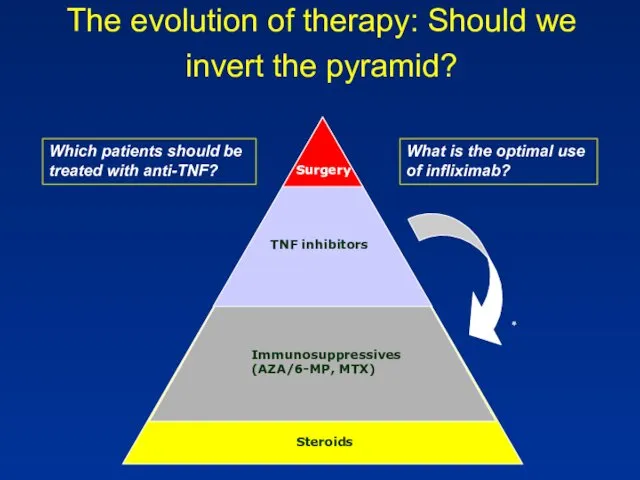
The evolution of therapy: Should we invert the pyramid?
Which patients
The evolution of therapy: Should we invert the pyramid?
Which patients
Future evolution
Should we aim for mucosal healing?
Should we perform early surgery?
Risk
Future evolution
Should we aim for mucosal healing?
Should we perform early surgery?
Risk
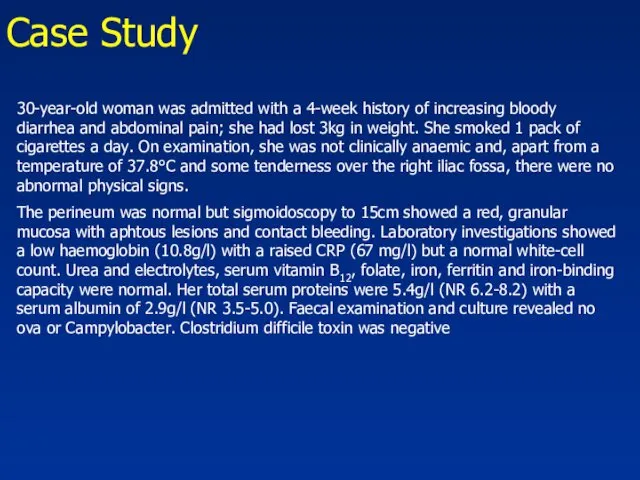
Case Study
30-year-old woman was admitted with a 4-week history of increasing
Case Study
30-year-old woman was admitted with a 4-week history of increasing
Case Study
The rectal biopsy : many crypt abscesses were present. The
Case Study
The rectal biopsy : many crypt abscesses were present. The
י.ע. 9/2011
בת 54, מזה כחודש וחצי סובלת משלשולים רבים, יציאות
י.ע. 9/2011
בת 54, מזה כחודש וחצי סובלת משלשולים רבים, יציאות
אושפזה בפנימית להמשך בירור וטיפול.
בקבלתה הוחל טיפול בסטרואידים ורפסל.במהלך אשפוזה שיפור
בקבלתה הוחל טיפול בסטרואידים ורפסל.במהלך אשפוזה שיפור
באשפוז הקודם הותחל גם טיפול גם ב6-MP. שוחחתי ארוכות עם החולה
י.ע. 18/10/2011
הגיעה לביקורת, טופלה עד כה בפרדניזון עם ירידה הדרגתית וסיימה
י.ע. 18/10/2011
הגיעה לביקורת, טופלה עד כה בפרדניזון עם ירידה הדרגתית וסיימה
י.ע. 26/12/2011
שני אשפוזים בפנימית: פעם אחת בשל החמרה שטופלה בסטרואידים,
י.ע. 26/12/2011
שני אשפוזים בפנימית: פעם אחת בשל החמרה שטופלה בסטרואידים,
י.ע. 23/7/2012
מזה 4 ימים עלייה בתדירות היציאות, 6-7 ליום, חלקן
י.ע. 23/7/2012
מזה 4 ימים עלייה בתדירות היציאות, 6-7 ליום, חלקן
 Мужское бесплодие
Мужское бесплодие Оценка комплексного состояния здоровья ребенка, определение группы здоровья по форме 112/у
Оценка комплексного состояния здоровья ребенка, определение группы здоровья по форме 112/у Нейролептические экстрапирамидные расстройства
Нейролептические экстрапирамидные расстройства Тірі ағзаларға ульракүлгін сәулелерінің әсері
Тірі ағзаларға ульракүлгін сәулелерінің әсері Лечение и профилактика гриппа, вызванного вирусом типа A/H1N1
Лечение и профилактика гриппа, вызванного вирусом типа A/H1N1 Порядок оказания акушерско-гинекологической помощи в Российской Федерации
Порядок оказания акушерско-гинекологической помощи в Российской Федерации Военная токсикология. Отравляющие вещества психотомиметического действия. Клиника, диагностика, лечение
Военная токсикология. Отравляющие вещества психотомиметического действия. Клиника, диагностика, лечение Лихорадка неясного генеза - вчера, сегодня, завтра
Лихорадка неясного генеза - вчера, сегодня, завтра Первая помощь при ранении
Первая помощь при ранении Аппендициттің асқынулары
Аппендициттің асқынулары Біологія і медицина XVIII-XIX
Біологія і медицина XVIII-XIX Муталлапова 301М Орг. мед. пом. жен. и детям
Муталлапова 301М Орг. мед. пом. жен. и детям Основи курортології. Курортні ресурси України. (Тема 2)
Основи курортології. Курортні ресурси України. (Тема 2) Лечебная физическая культура при заболевании глаз
Лечебная физическая культура при заболевании глаз Сепсис новонароджених етіологія, клініка, лікування. Синдром системної запальної відповіді
Сепсис новонароджених етіологія, клініка, лікування. Синдром системної запальної відповіді Коронавирус COVID-19
Коронавирус COVID-19 Амилоидоз почек. Диагностика, принципы лечения
Амилоидоз почек. Диагностика, принципы лечения Рак эндометрия
Рак эндометрия Толстокишечные кровотечение
Толстокишечные кровотечение Внешние признаки внутренних болезней
Внешние признаки внутренних болезней Сестринский уход за спинальными больными
Сестринский уход за спинальными больными Основы трансфузиологии
Основы трансфузиологии Язвенная болезнь. Патогенетические механизмы и принципы терапии
Язвенная болезнь. Патогенетические механизмы и принципы терапии Заболевания шейки матки
Заболевания шейки матки Трехуровневая модель оказания реабилитационной помощи
Трехуровневая модель оказания реабилитационной помощи Особливості формування серця і стимуляція регенерації серцевої м'язової тканини в умовах сучасної медицини
Особливості формування серця і стимуляція регенерації серцевої м'язової тканини в умовах сучасної медицини Функциональные пробы в ЛФК
Функциональные пробы в ЛФК Артериялық гипертензия
Артериялық гипертензия