- Lung cancer epidemiology, aetiology, clinical presentation, diagnosis and treatment

Содержание
- 2. Lung Cancer: Basic statistics Over 37,500 new cases per year in UK Over 33,000 deaths per
- 3. Ma-In Fe-In Ma-Mo Fe-Mo
- 4. Lung Cancer: Age distribution 2006 England and Wales
- 7. LUNG CANCER: Smoking Smoking causes: ~90% of lung cancer deaths in men ~80% of lung cancer
- 8. Constituents of Tobacco Smoke Gases Carbon Monoxide Hydrogen Cyanide Nitrogen Oxide, etc. etc. Nicotine Irritant substances
- 10. LUNG CANCER Risk factors other than smoking COPD (relative risk 3 – 6 fold) Asbestos Radon
- 12. LUNG CANCER: Symptoms Primary tumor Cough Dyspnoea; bronchial obstruction, p.effusion, pneumonia, phrenic N paralysis Wheezing Hemoptysis
- 13. Superior Vena Cava Obstruction
- 14. LUNG CANCER:Paraneoplastic syndromes Endocrine - Hypercalcaemia - ectopic ACTH secretion; Cushing’s syndrome - Syndrome of Inappropriate
- 15. Lung Cancer : Finger Clubbing
- 16. LUNG CANCER: Local and distant spread Brain Draining lymph nodes Pericardium Lung Pleura Liver Adrenals Bone
- 17. Lung Cancer: Investigation On first clinical suspicion: Plain Chest X-Ray Diagnosis and staging: Serum Biochemistry (Sodium,
- 18. LUNG CANCER Chest X Ray
- 19. Fibreoptic Bronchoscopy
- 20. LUNG CANCER Bronchoscopy
- 21. Lung cancer staging TNM T- tumor size. N- lymph node involvement. M- distant metastasis. CT, PET,
- 22. Transbronchial biopsy Endoscopic Ultrasound (CT biopsy) Endoscopic Ultrasound Endoscopic Ultrasound Neck Ultrasound Endobronchial Ultrasound Transbronchial biopsy
- 23. RC Rintoul, Papworth Hospital Endobronchial Ultrasound (EBUS)
- 24. RC Rintoul, Papworth Hospital RC Rintoul, Papworth Hospital
- 25. NON-SMALL CELL LUNG CANCER Stages at presentation i.e. More than 2/3rds have inoperable disease at presentation
- 26. SMALL CELL LUNG CANCER Extent at presentation i.e. 3/4 have metastatic disease at presentation Limited Disease
- 27. Lung Cancer: Screening with low-dose CT scanning 9mm
- 28. Day 0 Day 36
- 29. Prognosis of lung cancer Overall survival is poor: less than 10% live for 5 years Survival
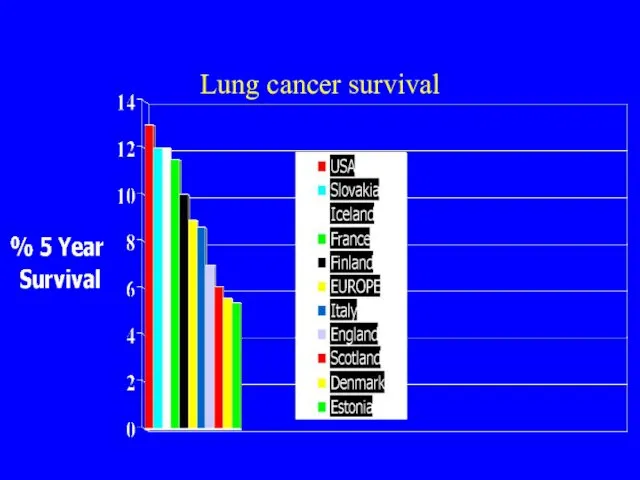
- 30. Lung cancer survival
- 31. Treatment of lung cancer Surgery Mostly for Non-Small Cell (less than 20% operable) Radiotherapy ‘Radical’ -
- 32. Treatment of Non-small cell lung cancer Management of non-small cell lung cancer often involves multi-modality therapy
- 33. Prognosis of non-small cell cancer Up to 20% operable Overall surgical survival 50% at 5 years
- 34. Prognosis of Non-small cell cancer Survival by stage
- 35. Treatment and prognosis of small cell cancer A systemic disease in >80% of cases Rarely operable
- 36. Survival of small cell cancer by stage
- 37. Lung cancer palliative care A disease with multiple symptoms and often poor survival - need for
- 38. What are the problems of lung cancer? Late Diagnosis Overall poor prognosis Very symptomatic Professional nihilism
- 40. Скачать презентацию
Lung Cancer: Basic statistics
Over 37,500 new cases per year in UK
Over
Lung Cancer: Basic statistics
Over 37,500 new cases per year in UK
Over
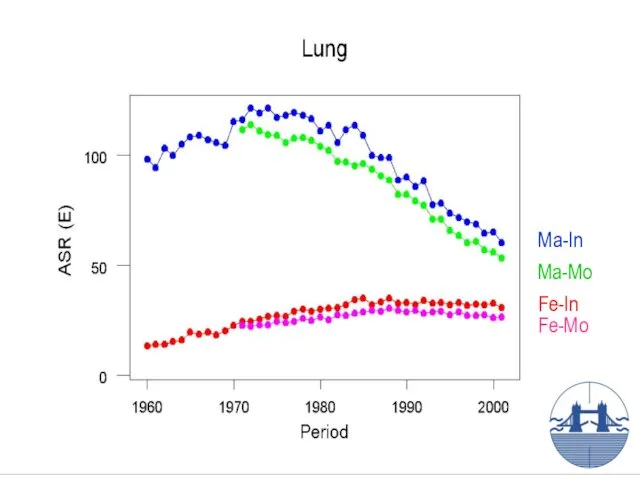
Ma-In
Fe-In
Ma-Mo
Fe-Mo
Ma-In
Fe-In
Ma-Mo
Fe-Mo
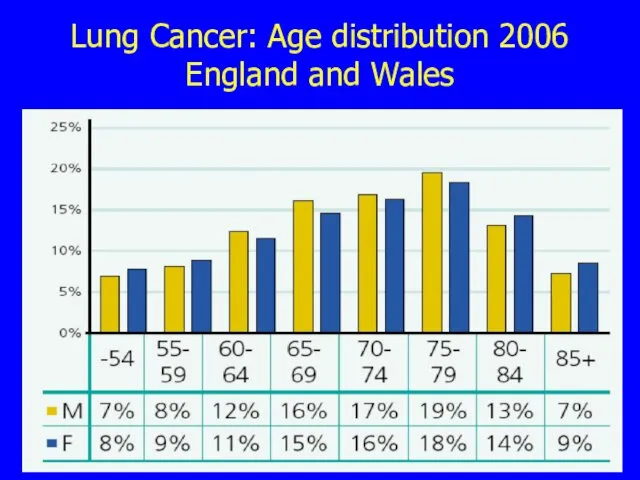
Lung Cancer: Age distribution 2006 England and Wales
Lung Cancer: Age distribution 2006 England and Wales
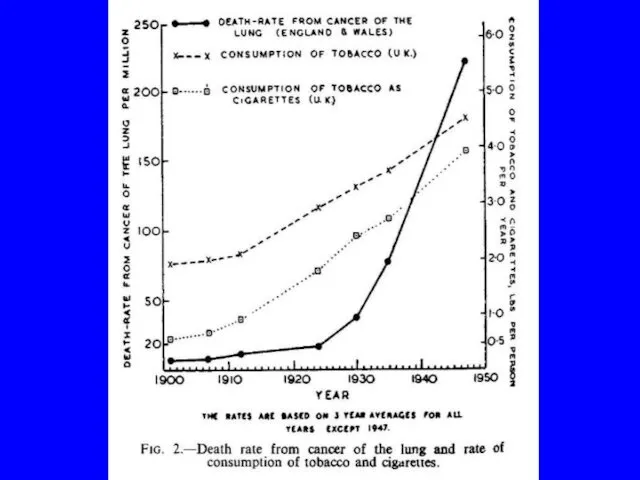
LUNG CANCER: Smoking
Smoking causes:
~90% of lung cancer deaths in men
~80% of
LUNG CANCER: Smoking
Smoking causes:
~90% of lung cancer deaths in men
~80% of
Constituents of Tobacco Smoke
Gases
Carbon Monoxide
Hydrogen Cyanide
Nitrogen Oxide, etc. etc.
Nicotine
Irritant substances
Carcinogens
Poly-Aromatic Hydrocarbons
N-Nitroso
Constituents of Tobacco Smoke
Gases
Carbon Monoxide
Hydrogen Cyanide
Nitrogen Oxide, etc. etc.
Nicotine
Irritant substances
Carcinogens
Poly-Aromatic Hydrocarbons
N-Nitroso
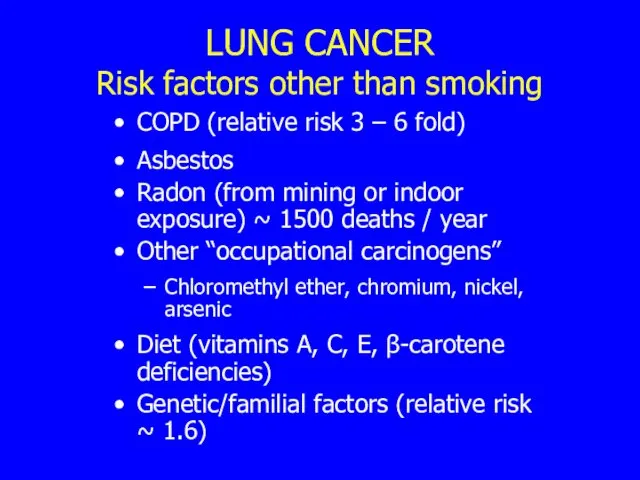
LUNG CANCER
Risk factors other than smoking
COPD (relative risk 3 – 6
LUNG CANCER
Risk factors other than smoking
COPD (relative risk 3 – 6
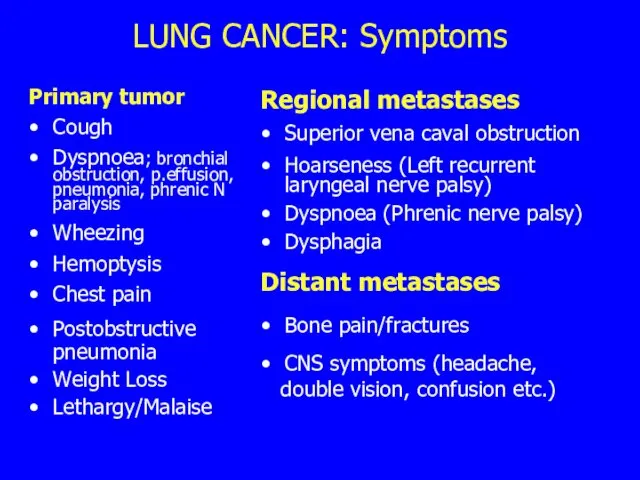
LUNG CANCER: Symptoms
Primary tumor
Cough
Dyspnoea; bronchial obstruction, p.effusion, pneumonia, phrenic N
LUNG CANCER: Symptoms
Primary tumor
Cough
Dyspnoea; bronchial obstruction, p.effusion, pneumonia, phrenic N
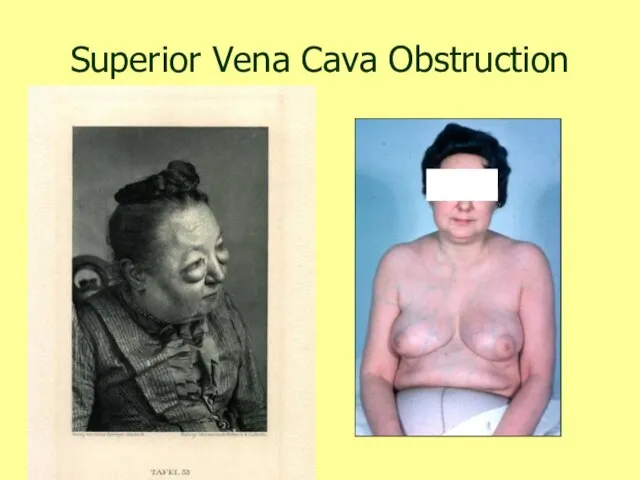
Superior Vena Cava Obstruction
Superior Vena Cava Obstruction
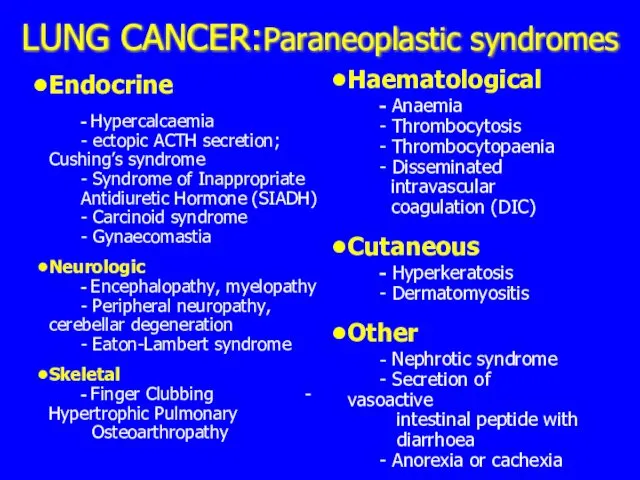
LUNG CANCER:Paraneoplastic syndromes
Endocrine
- Hypercalcaemia
- ectopic ACTH secretion; Cushing’s syndrome
- Syndrome of
LUNG CANCER:Paraneoplastic syndromes
Endocrine
- Hypercalcaemia
- ectopic ACTH secretion; Cushing’s syndrome
- Syndrome of

Lung Cancer : Finger Clubbing
Lung Cancer : Finger Clubbing
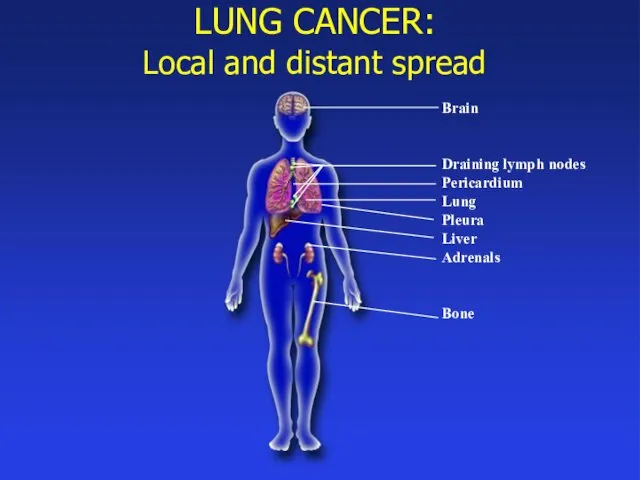
LUNG CANCER:
Local and distant spread
Brain
Draining lymph nodes
Pericardium
Lung
Pleura
Liver
Adrenals
Bone
LUNG CANCER:
Local and distant spread
Brain
Draining lymph nodes
Pericardium
Lung
Pleura
Liver
Adrenals
Bone
Lung Cancer: Investigation
On first clinical suspicion:
Plain Chest X-Ray
Diagnosis and staging:
Serum
Lung Cancer: Investigation
On first clinical suspicion:
Plain Chest X-Ray
Diagnosis and staging:
Serum
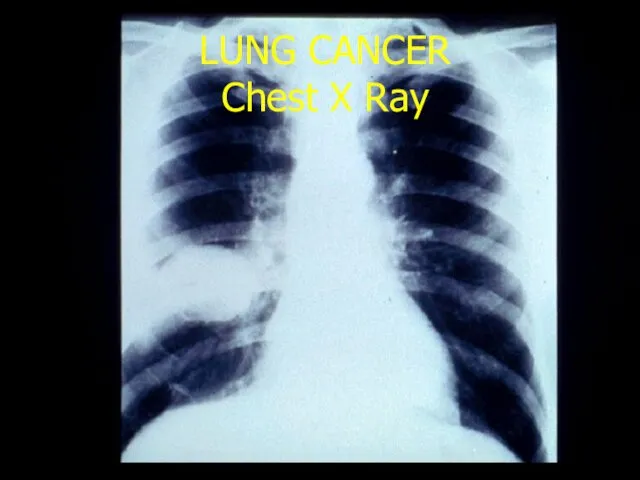
LUNG CANCER
Chest X Ray
LUNG CANCER
Chest X Ray
Fibreoptic Bronchoscopy
Fibreoptic Bronchoscopy

LUNG CANCER
Bronchoscopy
LUNG CANCER
Bronchoscopy
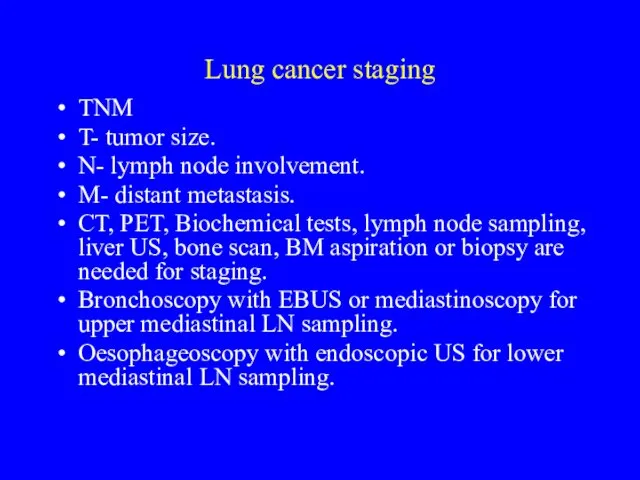
Lung cancer staging
TNM
T- tumor size.
N- lymph node involvement.
M- distant metastasis.
CT,
Lung cancer staging
TNM
T- tumor size.
N- lymph node involvement.
M- distant metastasis.
CT,
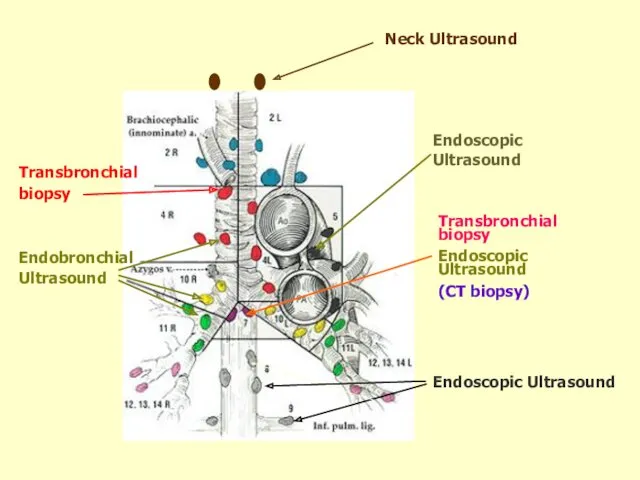
Transbronchial biopsy
Endoscopic Ultrasound
(CT biopsy)
Endoscopic Ultrasound
Endoscopic Ultrasound
Neck Ultrasound
Endobronchial
Ultrasound
Transbronchial
biopsy
Transbronchial biopsy
Endoscopic Ultrasound
(CT biopsy)
Endoscopic Ultrasound
Endoscopic Ultrasound
Neck Ultrasound
Endobronchial
Ultrasound
Transbronchial
biopsy

RC Rintoul, Papworth Hospital
Endobronchial Ultrasound (EBUS)
RC Rintoul, Papworth Hospital
Endobronchial Ultrasound (EBUS)

RC Rintoul, Papworth Hospital
RC Rintoul, Papworth Hospital
RC Rintoul, Papworth Hospital
RC Rintoul, Papworth Hospital
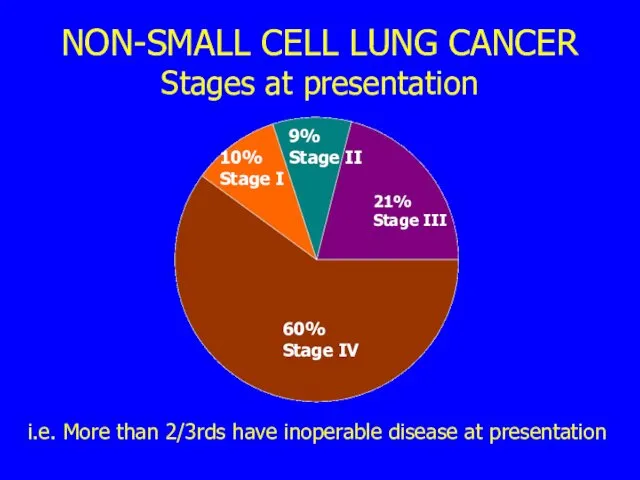
NON-SMALL CELL LUNG CANCER
Stages at presentation
i.e. More than 2/3rds have inoperable
NON-SMALL CELL LUNG CANCER
Stages at presentation
i.e. More than 2/3rds have inoperable
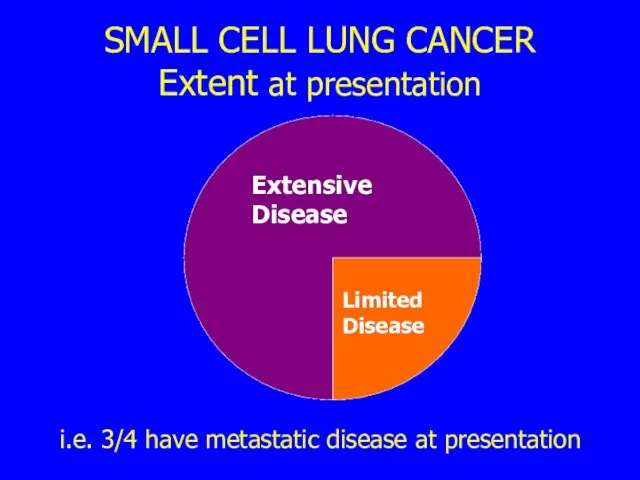
SMALL CELL LUNG CANCER
Extent at presentation
i.e. 3/4 have metastatic disease at
SMALL CELL LUNG CANCER
Extent at presentation
i.e. 3/4 have metastatic disease at
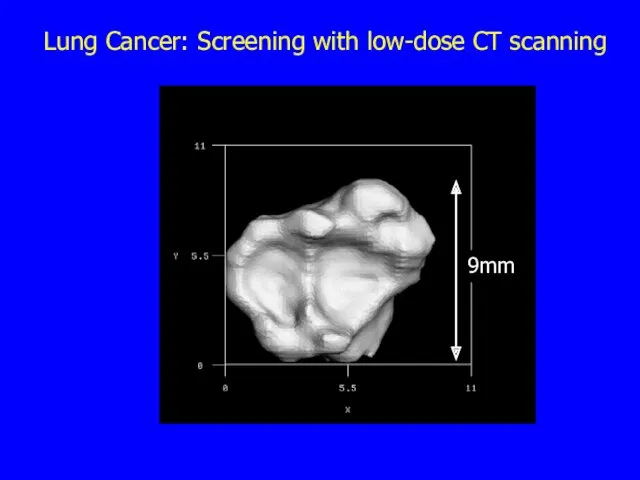
Lung Cancer: Screening with low-dose CT scanning
9mm
Lung Cancer: Screening with low-dose CT scanning
9mm
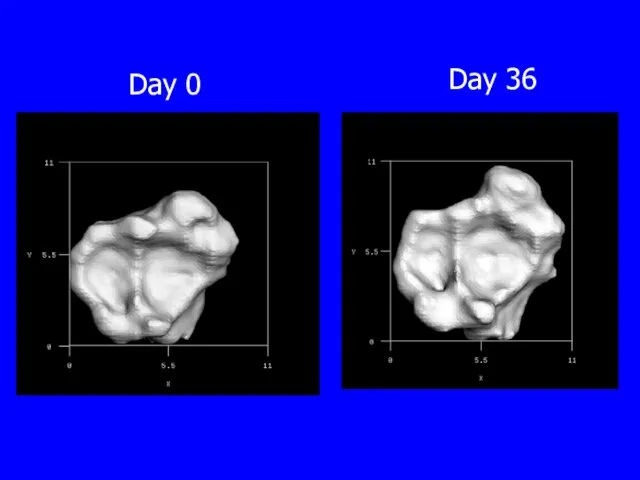
Day 0
Day 36
Day 0
Day 36
Prognosis of lung cancer
Overall survival is poor: less than 10% live
Prognosis of lung cancer
Overall survival is poor: less than 10% live
Lung cancer survival
Lung cancer survival
Treatment of lung cancer
Surgery
Mostly for Non-Small Cell (less than 20% operable)
Radiotherapy
‘Radical’
Treatment of lung cancer
Surgery
Mostly for Non-Small Cell (less than 20% operable)
Radiotherapy
‘Radical’
Treatment of Non-small cell lung cancer
Management of non-small cell lung cancer
Treatment of Non-small cell lung cancer
Management of non-small cell lung cancer
Prognosis of non-small cell cancer
Up to 20% operable
Overall surgical survival 50%
Prognosis of non-small cell cancer
Up to 20% operable
Overall surgical survival 50%
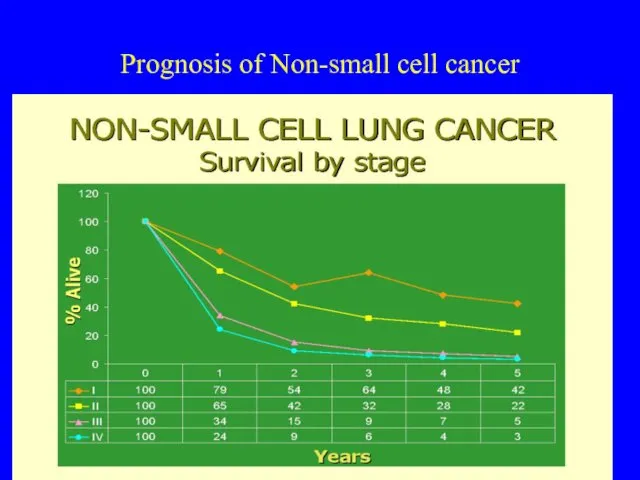
Prognosis of Non-small cell cancer
Survival by stage
Prognosis of Non-small cell cancer
Survival by stage
Treatment and prognosis of small cell cancer
A systemic disease in >80%
Treatment and prognosis of small cell cancer
A systemic disease in >80%
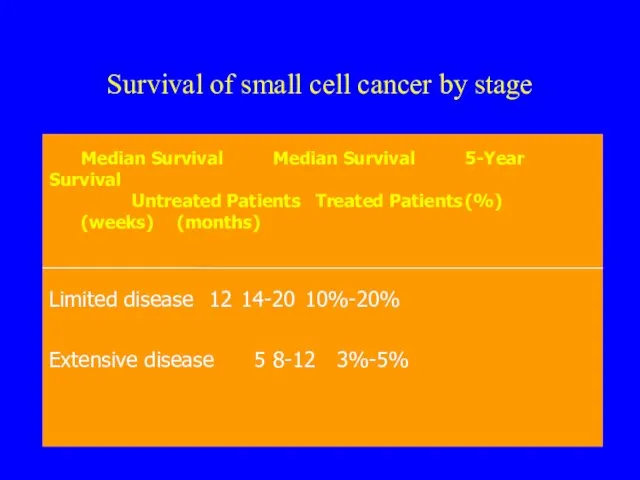
Survival of small cell cancer by stage
Survival of small cell cancer by stage
Lung cancer palliative care
A disease with multiple symptoms and often
Lung cancer palliative care
A disease with multiple symptoms and often
What are the problems of lung cancer?
Late Diagnosis
Overall poor prognosis
Very symptomatic
Professional
What are the problems of lung cancer?
Late Diagnosis
Overall poor prognosis
Very symptomatic
Professional
 Введение в генетику. Семиотика и принципы клинической диагностики наследственных болезней
Введение в генетику. Семиотика и принципы клинической диагностики наследственных болезней Сурдология. Тугоухость. Ототоксические препараты
Сурдология. Тугоухость. Ототоксические препараты Патофизиология обмена веществ
Патофизиология обмена веществ Внутрилабораторный контроль качества для метода иммуноферментного анализа
Внутрилабораторный контроль качества для метода иммуноферментного анализа Строма-тамырлық дистрофиялар
Строма-тамырлық дистрофиялар Воспалительные заболевания сосудистой оболочки
Воспалительные заболевания сосудистой оболочки Қанжасау. Адамның жасына байланысты ерекшеліктері
Қанжасау. Адамның жасына байланысты ерекшеліктері Фармакогнозия. Основные понятия дисциплины
Фармакогнозия. Основные понятия дисциплины Метаболический синдром
Метаболический синдром Общая характеристика нематод. Подотряд Ascaridata
Общая характеристика нематод. Подотряд Ascaridata Исследование мочи
Исследование мочи Female reproductive system
Female reproductive system Кандидозы. Классификация. Лечение
Кандидозы. Классификация. Лечение Острые эндогенные психозы
Острые эндогенные психозы Бруцеллез крупного рогатого скота. Эпизоотическая ситуация. Патогенез, меры борьбы
Бруцеллез крупного рогатого скота. Эпизоотическая ситуация. Патогенез, меры борьбы Дәрілік заттарды дұрыс пайдалану жүйесінің тұжырымдамасы
Дәрілік заттарды дұрыс пайдалану жүйесінің тұжырымдамасы Нарушения походки при различных заболеваниях ЦНС
Нарушения походки при различных заболеваниях ЦНС Жүйке жүйесі
Жүйке жүйесі Тірек – қимыл жүйесінің балалардағы ерекшеліктері
Тірек – қимыл жүйесінің балалардағы ерекшеліктері Синдром дисплазии соединительной ткани
Синдром дисплазии соединительной ткани Рентгенологические методы исследования, применяемые в кардиологии
Рентгенологические методы исследования, применяемые в кардиологии Нейропсихологические основы коррекционной педагогики
Нейропсихологические основы коррекционной педагогики Оппортунистические заболевания при ВИЧ‐инфекции
Оппортунистические заболевания при ВИЧ‐инфекции Клинический случай: миопатия Дюшена
Клинический случай: миопатия Дюшена Клещевой энцефалит в Республике Башкортостан (11 класс)
Клещевой энцефалит в Республике Башкортостан (11 класс) Кардиотокография. Ұрық жағдайын бағалаудың негізгі әдісі. Ұрық жүрек әрекетінің сипатын бағалау
Кардиотокография. Ұрық жағдайын бағалаудың негізгі әдісі. Ұрық жүрек әрекетінің сипатын бағалау Ботулизм. Классификация
Ботулизм. Классификация Методы исследования зубочелюстного аппарата
Методы исследования зубочелюстного аппарата