- Malaria “Bad Air”

Содержание
- 2. Malaria: Lecture Goals Understand basic principles of malaria pathogenesis in the context of relevance to clinical
- 3. Outline Background Organism Epidemiology Pathophysiology Clinical Symptoms Differential diagnosis Malaria in a complex emergency Who is
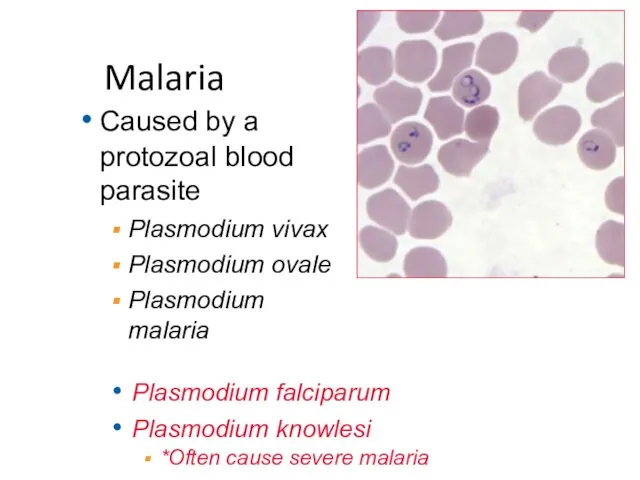
- 4. Malaria Caused by a protozoal blood parasite Plasmodium vivax Plasmodium ovale Plasmodium malaria Plasmodium falciparum Plasmodium
- 5. Transmission: Anopheles mosquito Wide spectrum symptoms Fever 1927 Nobel Prize: pyrotherapy for syphilis Geographical distribution: Tropic
- 7. •Liver stage: Asimptomatic. With P. vivax and P. ovale, has dormant form (hypnozoite) that can relapse
- 8. Malaria: Endemicity and Resistance POWELL B , FORD C Cleveland Clinic Journal of Medicine 2010;77:246-254
- 9. % Malaria P. falciparum 9 http://www.who.int/gho/map_gallery/en/
- 10. Chloroquine resistance and P. falciparum overlap, with exceptions: Central America West of Panama Canal Haiti/Dominican Republic
- 11. P. falciparum: Dangerous Infects various RBC stages Makes RBCs “sticky” Result: Severe hemolysis Obstruction of microcirculation
- 12. Malaria in a Complex Emergency: Symptoms SEVERE > 5% parasitemia Severe anemia Hemoglobinuria Bleeding diathesis Shock/Hypotension
- 13. Malaria in a Complex Emergency: Who is at Risk for severe disease? Highest risk populations: Non-immune
- 14. Malaria in a Complex Emergency Displaced people within malaria endemic areas creates risk for a severe
- 15. Malaria: Practical Aspects of Diagnosis Presumptive treatment has been commonplace for decades Problematic, but hard to
- 16. Malaria in a Complex Emergency Important, when possible, to at least establish a fever epidemic is
- 17. Malaria: Differential Diagnosis Malaria can involve many organs Coinfection well described Differential diagnosis is broad Salmonella
- 18. Malaria: Diagnostics Lateral flow test, relies on antibody-antigen interactions Some RDTs specific for P. falciparum WHO
- 19. Clues to P. falciparum: Trophozoites most commonly seen, and are small, delicate rings, often multiple per
- 20. Malaria: Treatment
- 21. CDC Algorithm for Traveler Returned to US *Not the same as WHO Note: CDC now recommending
- 22. Malaria: Treatment WHO guidelines and update can be found at: http://www.who.int/malaria/publications/atoz/9789241549127/en/
- 23. Malaria: Therapy Options ACT (Artemisinin based combination therapies) Artemethur + lemefantrine (coartem®) Artesunate + amodiaquine (coarsucam/ASAQ
- 24. Suspected malaria Blood films or RDT if available Calculate parasitemia Repeat each 12-24 hours for three
- 25. Uncomplicated malaria: treatment Use local resistance patterns to choose medication: •ACT •artesunate plus tetracycline /doxycycline/clindamycin •Quinine
- 26. Severe Malaria: WHO Criteria creatinine > 265 μmol/l). (radiological) One or more of the following: Clinical
- 27. If illness is with P. ovale/vivax, follow with primaquine if not G6PD Give oral or rectal
- 28. Malaria: Prevention Bed Nets!!!!!! 1000 nets save 5 lives Insecticide impregnated best Cochrane Review, 2009 Indoor/personal
- 30. Скачать презентацию
Malaria: Lecture Goals
Understand basic principles of malaria pathogenesis in the context
Malaria: Lecture Goals
Understand basic principles of malaria pathogenesis in the context
Outline
Background
Organism
Epidemiology
Pathophysiology
Clinical
Symptoms
Differential diagnosis
Malaria in a complex emergency
Who is at risk
How to choose
Outline
Background
Organism
Epidemiology
Pathophysiology
Clinical
Symptoms
Differential diagnosis
Malaria in a complex emergency
Who is at risk
How to choose
Malaria
Caused by a protozoal blood parasite
Plasmodium vivax
Plasmodium ovale
Plasmodium malaria
Plasmodium falciparum
Plasmodium knowlesi
*Often
Malaria
Caused by a protozoal blood parasite
Plasmodium vivax
Plasmodium ovale
Plasmodium malaria
Plasmodium falciparum
Plasmodium knowlesi
*Often
Transmission: Anopheles mosquito
Wide spectrum symptoms
Fever
1927 Nobel Prize: pyrotherapy for syphilis
Geographical distribution:
Tropic
Transmission: Anopheles mosquito
Wide spectrum symptoms
Fever
1927 Nobel Prize: pyrotherapy for syphilis
Geographical distribution:
Tropic

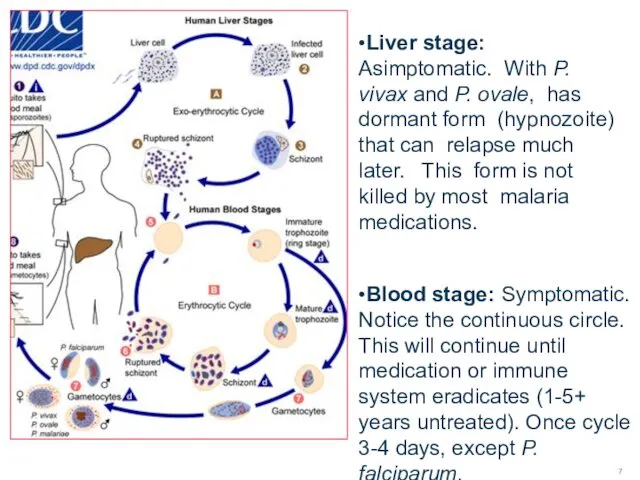
•Liver stage: Asimptomatic. With P. vivax and P. ovale, has dormant
•Liver stage: Asimptomatic. With P. vivax and P. ovale, has dormant
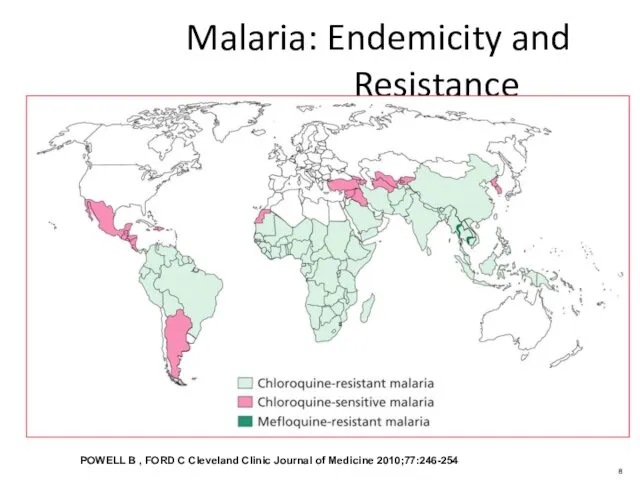
Malaria: Endemicity and Resistance
POWELL B , FORD C Cleveland Clinic Journal
Malaria: Endemicity and Resistance
POWELL B , FORD C Cleveland Clinic Journal
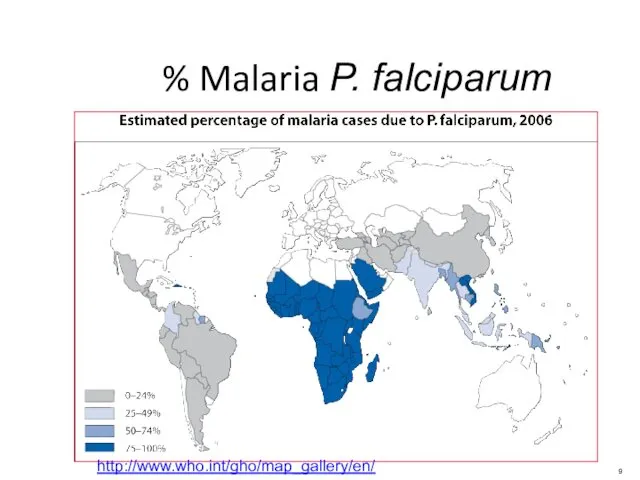
% Malaria P. falciparum
9
http://www.who.int/gho/map_gallery/en/
% Malaria P. falciparum
9
http://www.who.int/gho/map_gallery/en/
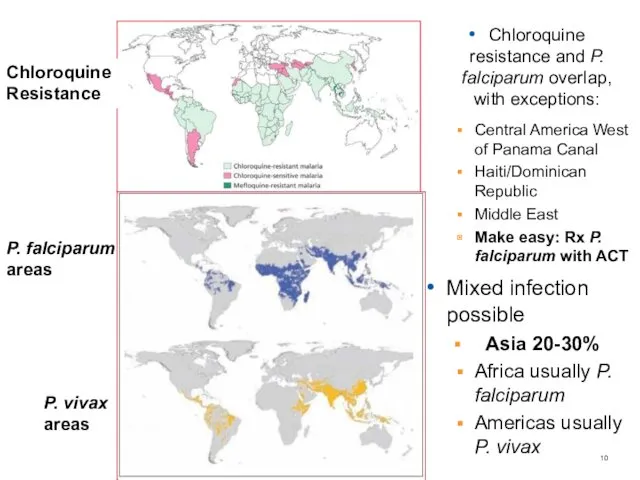
Chloroquine resistance and P. falciparum overlap, with exceptions:
Central America West of
Chloroquine resistance and P. falciparum overlap, with exceptions:
Central America West of
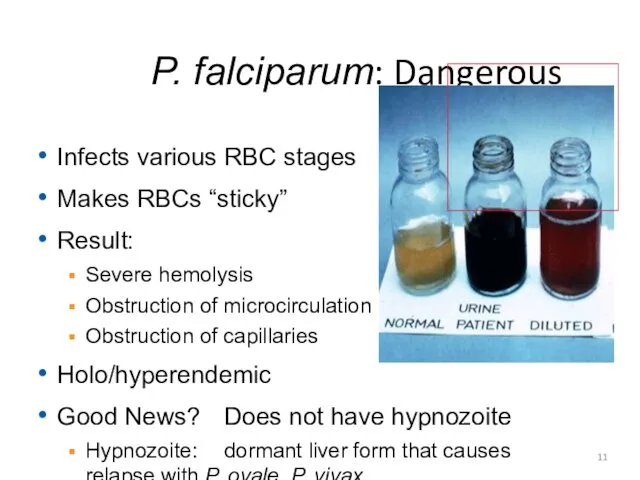
P. falciparum: Dangerous
Infects various RBC stages
Makes RBCs “sticky”
Result:
Severe hemolysis
Obstruction of microcirculation
Obstruction
P. falciparum: Dangerous
Infects various RBC stages
Makes RBCs “sticky”
Result:
Severe hemolysis
Obstruction of microcirculation
Obstruction
Malaria in a Complex Emergency: Symptoms
SEVERE
> 5% parasitemia
Severe anemia
Hemoglobinuria
Bleeding diathesis
Shock/Hypotension
Renal failure
Hypoglycemia
Acidosis
Neurologic
Malaria in a Complex Emergency: Symptoms
SEVERE
> 5% parasitemia
Severe anemia
Hemoglobinuria
Bleeding diathesis
Shock/Hypotension
Renal failure
Hypoglycemia
Acidosis
Neurologic
Malaria in a Complex Emergency: Who is at Risk for severe
Malaria in a Complex Emergency: Who is at Risk for severe
Malaria in a Complex Emergency
Displaced people within malaria endemic areas creates
Malaria in a Complex Emergency
Displaced people within malaria endemic areas creates
Malaria: Practical Aspects of Diagnosis
Presumptive treatment has been commonplace for decades
Problematic,
Malaria: Practical Aspects of Diagnosis
Presumptive treatment has been commonplace for decades
Problematic,
Malaria in a Complex Emergency
Important, when possible, to at least establish
Malaria in a Complex Emergency
Important, when possible, to at least establish
Malaria: Differential Diagnosis
Malaria can involve many organs
Coinfection well described
Differential diagnosis is
Malaria: Differential Diagnosis
Malaria can involve many organs
Coinfection well described
Differential diagnosis is
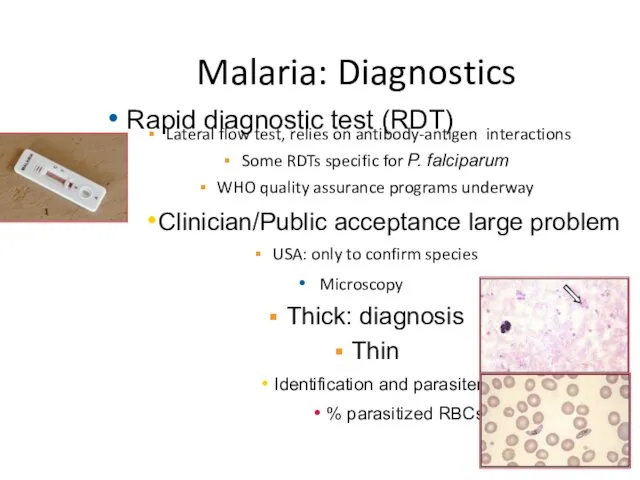
Malaria: Diagnostics
Lateral flow test, relies on antibody-antigen interactions
Some RDTs specific for
Malaria: Diagnostics
Lateral flow test, relies on antibody-antigen interactions
Some RDTs specific for
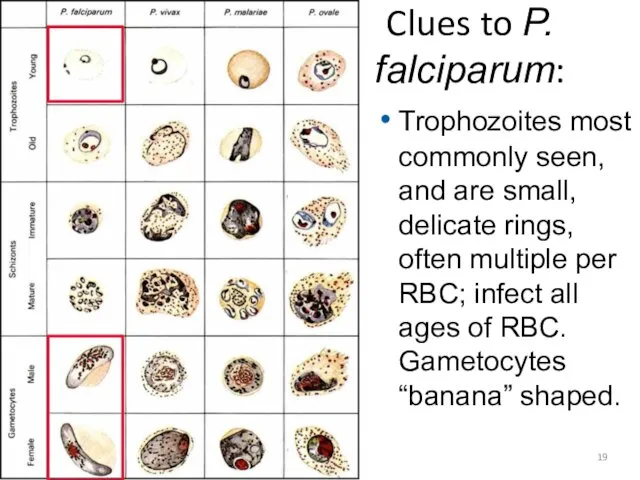
Clues to P. falciparum:
Trophozoites most commonly seen, and are small, delicate
Clues to P. falciparum:
Trophozoites most commonly seen, and are small, delicate
Malaria: Treatment
Malaria: Treatment
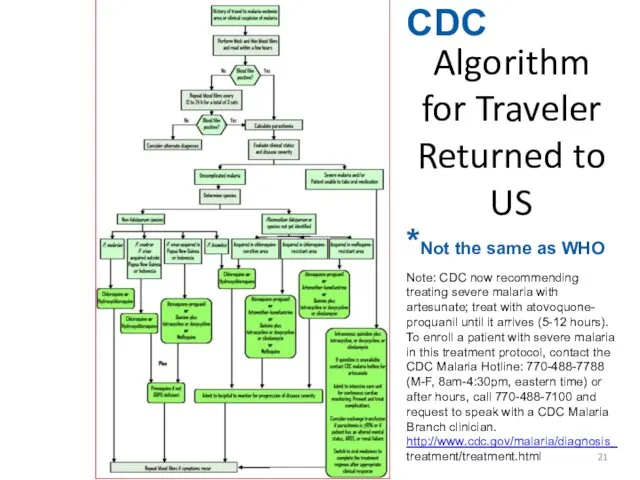
CDC
Algorithm for Traveler Returned to US
*Not the same as WHO
Note: CDC
CDC
Algorithm for Traveler Returned to US
*Not the same as WHO
Note: CDC
Malaria: Treatment
WHO guidelines and update can be found at: http://www.who.int/malaria/publications/atoz/9789241549127/en/
Malaria: Treatment
WHO guidelines and update can be found at: http://www.who.int/malaria/publications/atoz/9789241549127/en/
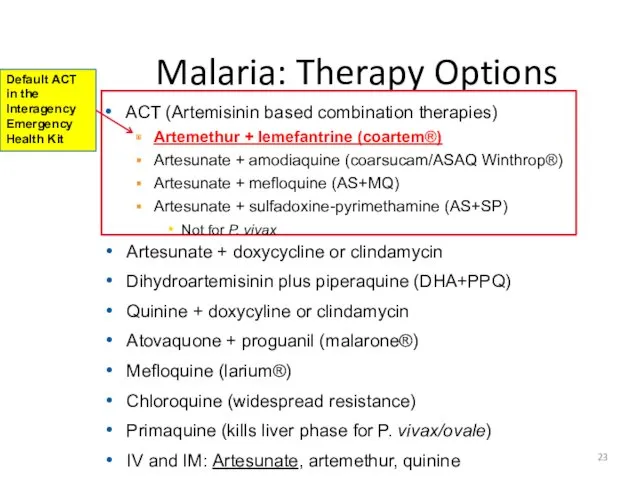
Malaria: Therapy Options
ACT (Artemisinin based combination therapies)
Artemethur + lemefantrine (coartem®)
Artesunate +
Malaria: Therapy Options
ACT (Artemisinin based combination therapies)
Artemethur + lemefantrine (coartem®)
Artesunate +
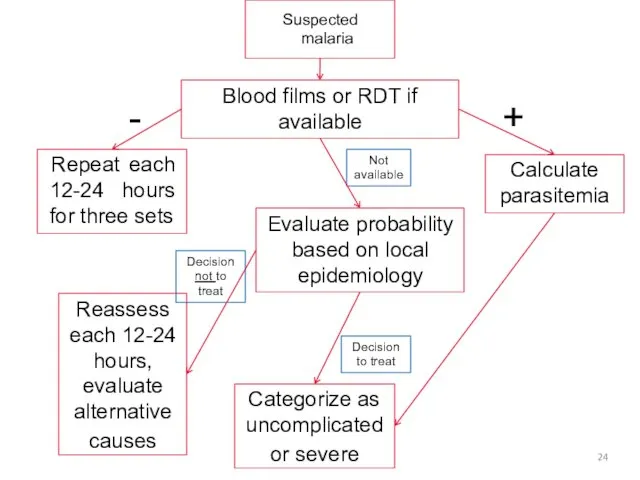
Suspected malaria
Blood films or RDT if available
Calculate parasitemia
Repeat each 12-24 hours
Suspected malaria
Blood films or RDT if available
Calculate parasitemia
Repeat each 12-24 hours
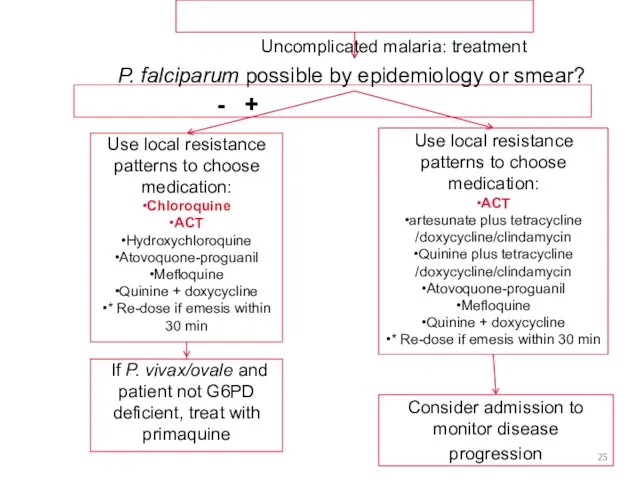
Uncomplicated malaria: treatment
Use local resistance patterns to choose medication:
•ACT
•artesunate plus tetracycline
/doxycycline/clindamycin
•Quinine
Uncomplicated malaria: treatment
Use local resistance patterns to choose medication:
•ACT
•artesunate plus tetracycline
/doxycycline/clindamycin
•Quinine
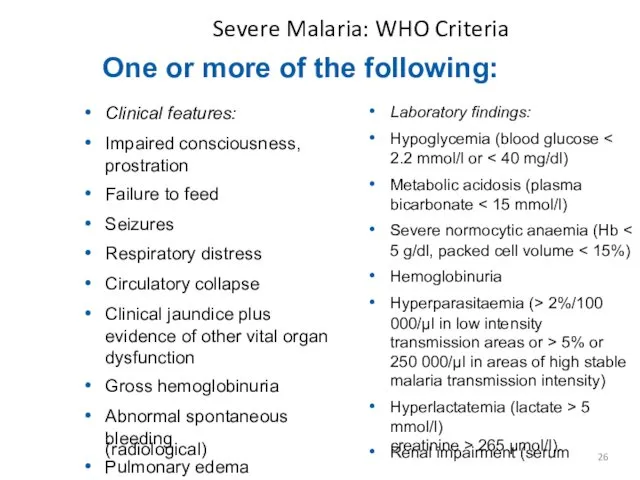
Severe Malaria: WHO Criteria
creatinine > 265 μmol/l).
(radiological)
One or more of the
Severe Malaria: WHO Criteria
creatinine > 265 μmol/l).
(radiological)
One or more of the
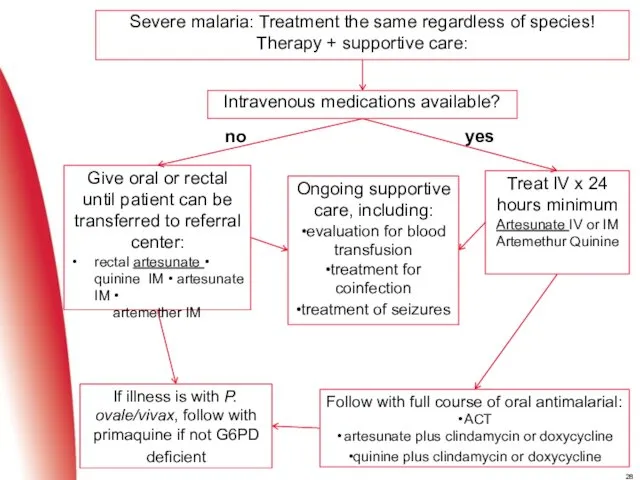
If illness is with P. ovale/vivax, follow with primaquine if not
If illness is with P. ovale/vivax, follow with primaquine if not
Malaria: Prevention
Bed Nets!!!!!!
1000 nets save 5 lives
Insecticide impregnated best
Cochrane Review, 2009
Indoor/personal
Malaria: Prevention
Bed Nets!!!!!!
1000 nets save 5 lives
Insecticide impregnated best
Cochrane Review, 2009
Indoor/personal
 Частная патология. Учение о болезни. Болезни органов кроветворения. Анемии
Частная патология. Учение о болезни. Болезни органов кроветворения. Анемии Сестринская помощь при скарлатине и коклюше
Сестринская помощь при скарлатине и коклюше ИПРА. Категории детей-инвалидов
ИПРА. Категории детей-инвалидов Свойства эфирных масел
Свойства эфирных масел Тағамның маңызы құрамы және қызметі
Тағамның маңызы құрамы және қызметі Медицинская гельминтология. Нематоды – паразиты человека
Медицинская гельминтология. Нематоды – паразиты человека Вкладки. Классификация вкладок
Вкладки. Классификация вкладок Коматозні стани
Коматозні стани Организация работы специализированных и линейных бригад скорой помощи
Организация работы специализированных и линейных бригад скорой помощи Рак підшлункової залози
Рак підшлункової залози Повышенный риск кумуляции. Биологическое воздействие лекарств на организм. 7-тема СРИ
Повышенный риск кумуляции. Биологическое воздействие лекарств на организм. 7-тема СРИ Грипп и острые респираторные вирусные инфекции
Грипп и острые респираторные вирусные инфекции Аноректальные пороки развития у детей
Аноректальные пороки развития у детей Сестринская деятельность и сестринский уход в реабилитации пациентов с патологией дыхательной системы
Сестринская деятельность и сестринский уход в реабилитации пациентов с патологией дыхательной системы Врожденные пороки сердца с препятствием кровотоку (с синдромом шлюза)
Врожденные пороки сердца с препятствием кровотоку (с синдромом шлюза) Асқорыту органдарының қатерсіз және қатерлі ісіктері
Асқорыту органдарының қатерсіз және қатерлі ісіктері Раннее выявление и диагностика туберкулеза
Раннее выявление и диагностика туберкулеза Пациент-орталықтандырылған күтімнің принциптері мен мәселелері
Пациент-орталықтандырылған күтімнің принциптері мен мәселелері Острая дыхательная недостаточность
Острая дыхательная недостаточность Классификация по этиологии
Классификация по этиологии Планирование семьи. Регулирование рождаемости. Контрацепция
Планирование семьи. Регулирование рождаемости. Контрацепция Медицинские показания и противопоказания для обеспечения инвалидов протезами с внешним источником энергии
Медицинские показания и противопоказания для обеспечения инвалидов протезами с внешним источником энергии Операции на нервных стволах
Операции на нервных стволах Взаимоотношения врача и фармацевтического работника
Взаимоотношения врача и фармацевтического работника Pirmās palīdzības apmācība
Pirmās palīdzības apmācība Принципы рационального питания
Принципы рационального питания Иммунитет. Термины. Виды иммунитета. ВИЧ и СПИД
Иммунитет. Термины. Виды иммунитета. ВИЧ и СПИД Исследование отделяемого половых органов
Исследование отделяемого половых органов