- Malaria (Febris intermittens)

Содержание
- 2. Overview Introduction Etiology, epidemiology Pathogenesis Clinical features Complications Diagnosis Treatment Prevention
- 3. Malaria is a life-threatening disease caused by parasites that are transmitted to people through the bites
- 4. Between 2010 and 2015, malaria incidence among populations at risk (the rate of new cases) fell
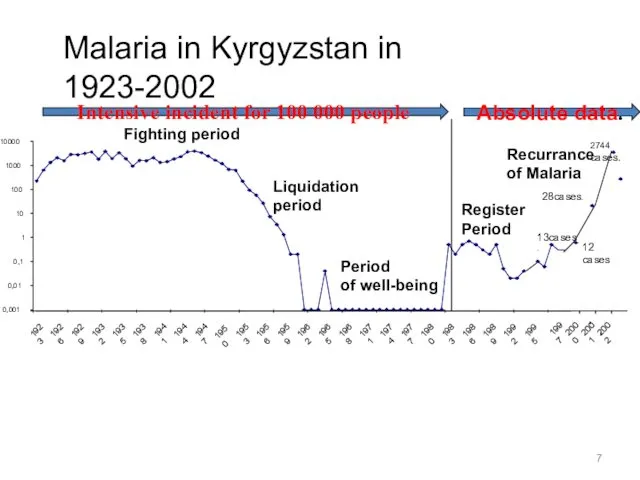
- 7. Malaria in Kyrgyzstan in 1923-2002 0,001 0,01 0,1 1 10 100 1000 10000 1923 1926 1929
- 8. Exo- erythrocytic (hepatic) cycle Malaria Life Cycle Life Cycle Schizogony Sporogony
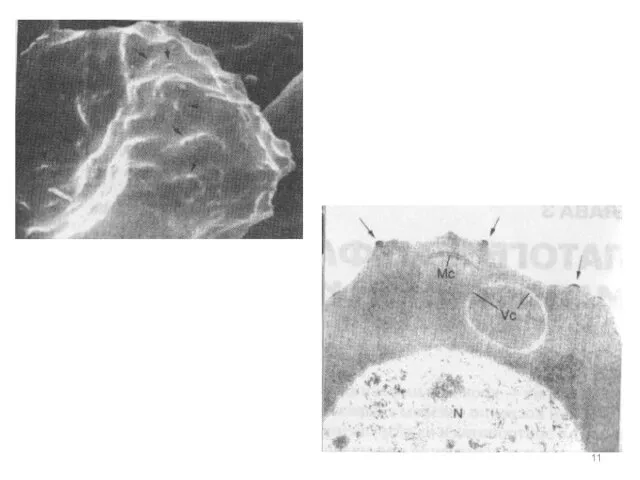
- 10. Plasmodium spp. (Malaria) Pathology and clinical significance: When merozoits invade the blood cells, using hemoglobin as
- 12. Clinical presentation Early symptoms Headache Malaise Fatigue Nausea Muscular pains Slight diarrhea Slight fever, usually not
- 13. Malarial Paroxysm Prodrome 2-3 days before Malaise, fever,fatigue, muscle pains, nausea, anorexia Can mistake for influenza
- 14. Types of Infections Recrudescence exacerbation of persistent undetectable parasitemia, due to survival of erythrocytic forms, no
- 15. Clinical presentation Varies in severity and course Parasite factors Species and strain of parasite Geographic origin
- 16. Malarial Paroxysm Periodicity Days 1 and 3 for P.v., P.o., (and P.f.) - tertian Usually persistent
- 17. paroxysms associated with synchrony of merozoite release between paroxysms temper-ature is normal and patient feels well
- 18. Presentation of P.vivax Most people of West African descent are resistant to P.v. Lack Duffy blood
- 19. Incubation period in non-immunes 12-17 days but can be 8-9 months or longer Some strains from
- 21. Lack classical paroxysm followed by asymptomatic period Headache, dizziness, muscle pain, malaise, anorexia, nausea, vague abdominal
- 22. Temperature curves
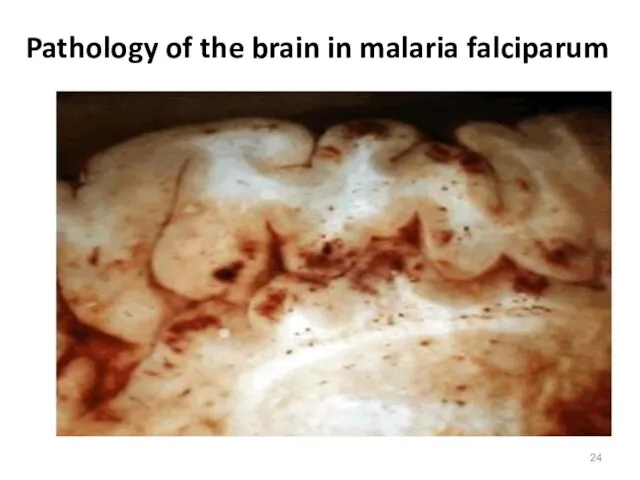
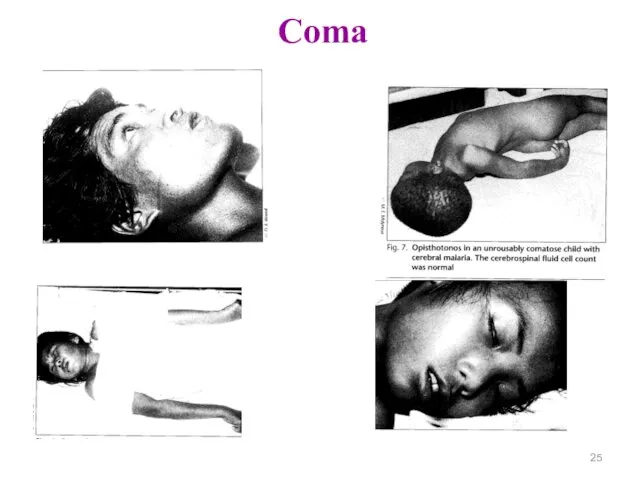
- 23. Complication: Coma - brain edema, disturbance of microcirculation, "sludge" - the aggregates of red blood cells,
- 24. Pathology of the brain in malaria falciparum
- 25. Coma
- 26. Malaria in pregnant women Abortion Premature births Neonatal complications Deaths. Often develop severe anemia. Often observed
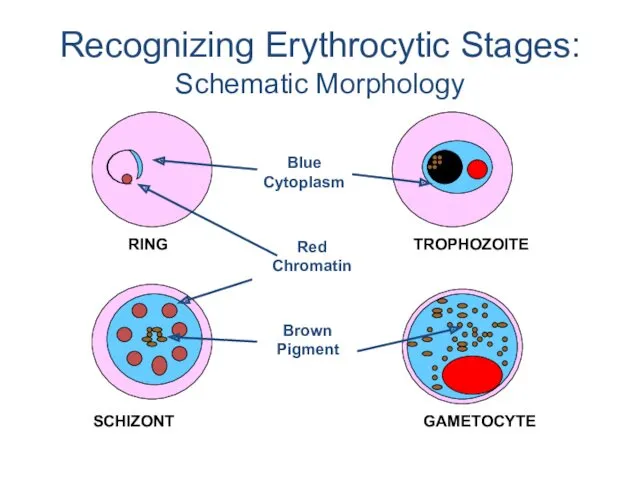
- 27. Recognizing Erythrocytic Stages: Schematic Morphology
- 28. Parasitemia and clinical correlates
- 29. Parasitemia and clinical correlates *WHO criteria for severe malaria are parasitemia > 10,000 /μl and severe
- 36. Malaria Serology – antibody detection Immunologic assays to detect host response Antibodies to asexual parasites appear
- 37. Malaria Serology – antibody detection Valuable epidemiologic tool in some settings Useful for Identifying infective donor
- 38. Polymerase Chain Reaction (PCR) Molecular technique to identify parasite genetic material Uses whole blood collected in
- 40. Скачать презентацию
Overview
Introduction
Etiology, epidemiology
Pathogenesis
Clinical features
Complications
Diagnosis
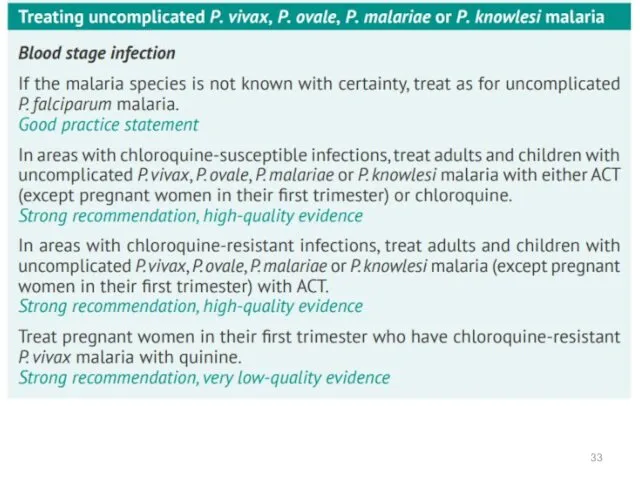
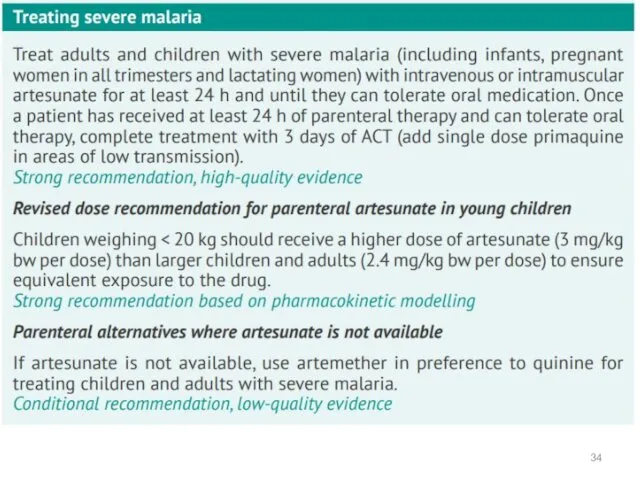
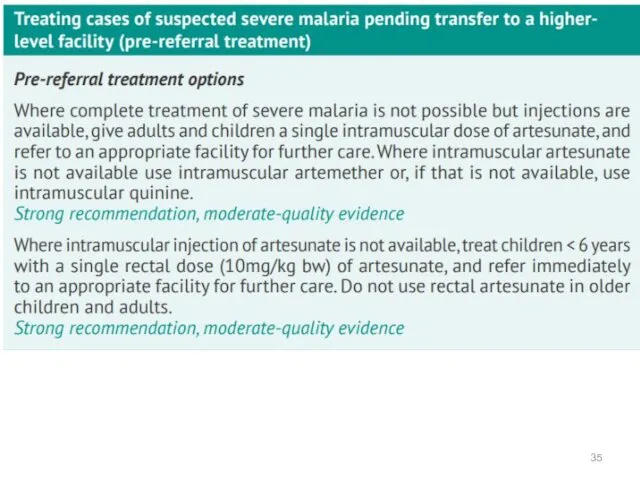
Treatment
Prevention
Overview
Introduction
Etiology, epidemiology
Pathogenesis
Clinical features
Complications
Diagnosis
Treatment
Prevention
Malaria is a life-threatening disease caused by parasites that are
Malaria is a life-threatening disease caused by parasites that are
Between 2010 and 2015, malaria incidence among populations at risk
Between 2010 and 2015, malaria incidence among populations at risk

Malaria in Kyrgyzstan in 1923-2002
0,001
0,01
0,1
1
10
100
1000
10000
1923
1926
1929
1932
1935
1938
1941
1944
1947
1950
1953
1956
1959
1962
1965
1968
1971
1974
1977
1980
1983
1986
1989
1992
1995
Fighting period
Liquidation
period
Period
of well-being
Register
Malaria in Kyrgyzstan in 1923-2002
0,001
0,01
0,1
1
10
100
1000
10000
1923
1926
1929
1932
1935
1938
1941
1944
1947
1950
1953
1956
1959
1962
1965
1968
1971
1974
1977
1980
1983
1986
1989
1992
1995
Fighting period
Liquidation
period
Period
of well-being
Register
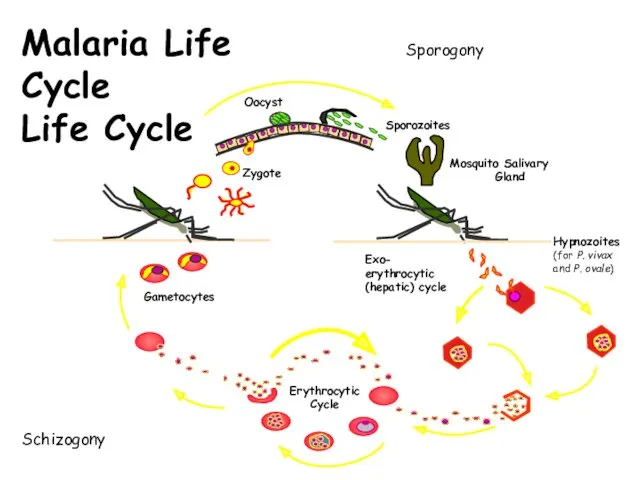
Exo-
erythrocytic
(hepatic) cycle
Malaria Life Cycle
Life Cycle
Schizogony
Sporogony
Exo-
erythrocytic
(hepatic) cycle
Malaria Life Cycle
Life Cycle
Schizogony
Sporogony
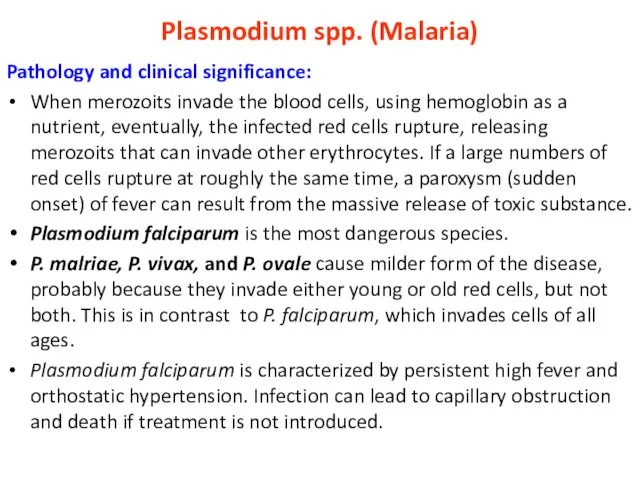
Plasmodium spp. (Malaria)
Pathology and clinical significance:
When merozoits invade the blood cells,
Plasmodium spp. (Malaria)
Pathology and clinical significance:
When merozoits invade the blood cells,
Clinical presentation
Early symptoms
Headache
Malaise
Fatigue
Nausea
Muscular pains
Slight diarrhea
Slight fever, usually not intermittent
Could mistake for
Clinical presentation
Early symptoms
Headache
Malaise
Fatigue
Nausea
Muscular pains
Slight diarrhea
Slight fever, usually not intermittent
Could mistake for
Malarial Paroxysm
Prodrome 2-3 days before
Malaise, fever,fatigue, muscle pains, nausea, anorexia
Can mistake
Malarial Paroxysm
Prodrome 2-3 days before
Malaise, fever,fatigue, muscle pains, nausea, anorexia
Can mistake
Types of Infections
Recrudescence
exacerbation of persistent undetectable parasitemia, due to survival of
Types of Infections
Recrudescence
exacerbation of persistent undetectable parasitemia, due to survival of
Clinical presentation
Varies in severity and course
Parasite factors
Species and strain of parasite
Geographic
Clinical presentation
Varies in severity and course
Parasite factors
Species and strain of parasite
Geographic
Malarial Paroxysm
Periodicity
Days 1 and 3 for P.v., P.o., (and P.f.) -
Malarial Paroxysm
Periodicity
Days 1 and 3 for P.v., P.o., (and P.f.) -
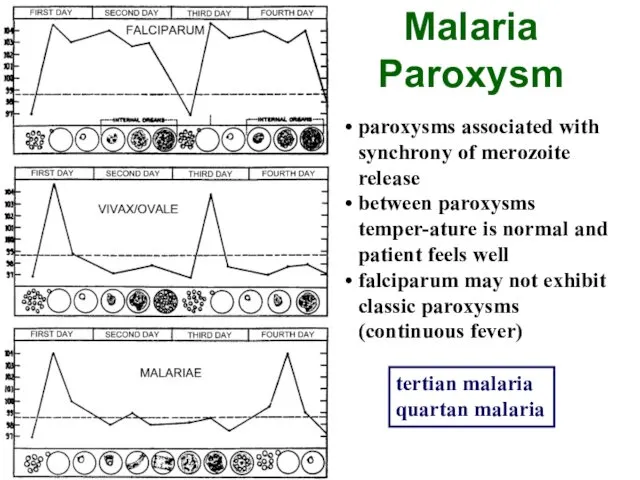
paroxysms associated with synchrony of merozoite release
between paroxysms temper-ature is normal
paroxysms associated with synchrony of merozoite release
between paroxysms temper-ature is normal
Presentation of P.vivax
Most people of West African descent are resistant to
Presentation of P.vivax
Most people of West African descent are resistant to
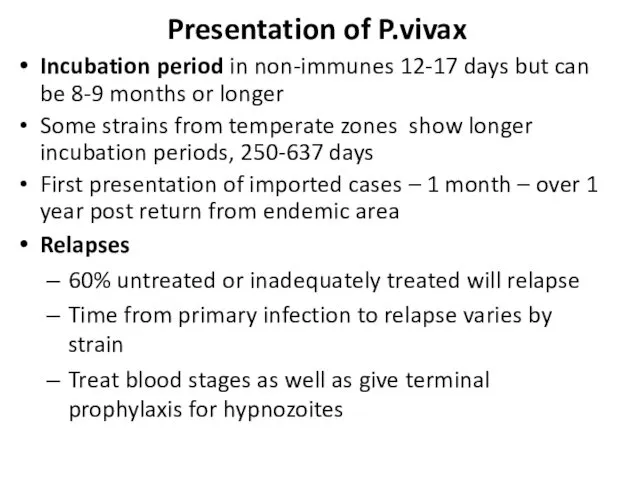
Incubation period in non-immunes 12-17 days but can be 8-9 months
Incubation period in non-immunes 12-17 days but can be 8-9 months

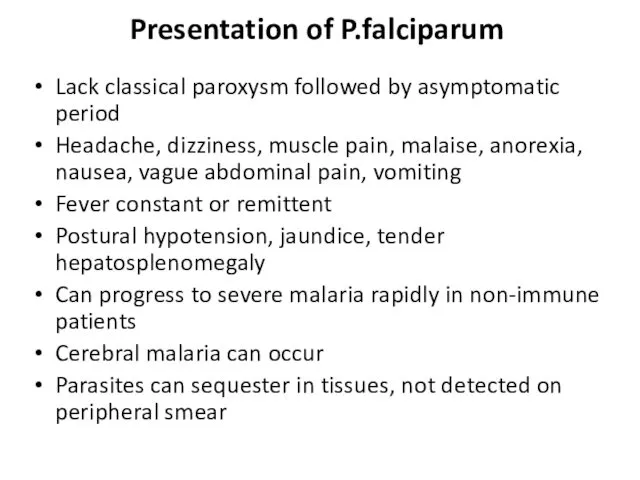
Lack classical paroxysm followed by asymptomatic period
Headache, dizziness, muscle pain, malaise,
Lack classical paroxysm followed by asymptomatic period
Headache, dizziness, muscle pain, malaise,
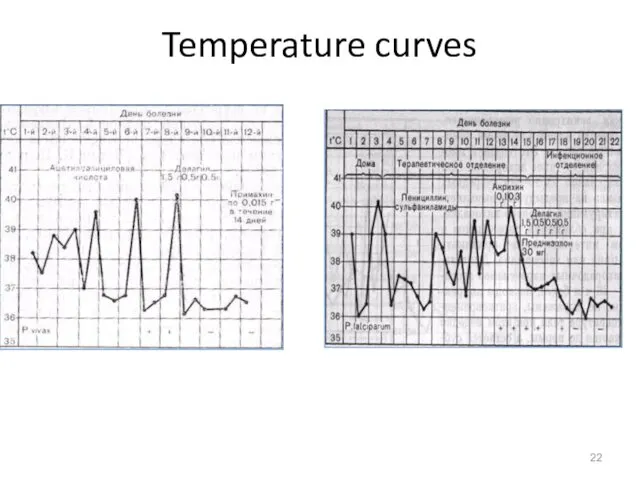
Temperature curves
Temperature curves
Complication:
Coma - brain edema, disturbance of microcirculation, "sludge" - the
Complication:
Coma - brain edema, disturbance of microcirculation, "sludge" - the
Pathology of the brain in malaria falciparum
Pathology of the brain in malaria falciparum
Coma
Coma
Malaria in pregnant women
Abortion
Premature births
Neonatal complications
Deaths.
Often develop severe anemia.
Often observed
Malaria in pregnant women
Abortion
Premature births
Neonatal complications
Deaths.
Often develop severe anemia.
Often observed
Recognizing Erythrocytic Stages:
Schematic Morphology
Recognizing Erythrocytic Stages:
Schematic Morphology
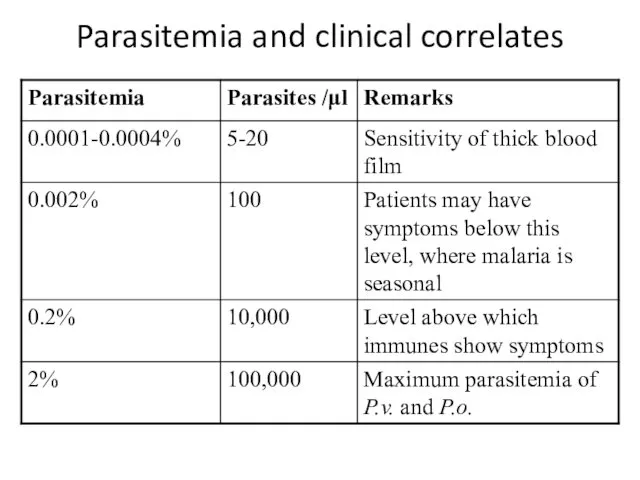
Parasitemia and clinical correlates
Parasitemia and clinical correlates
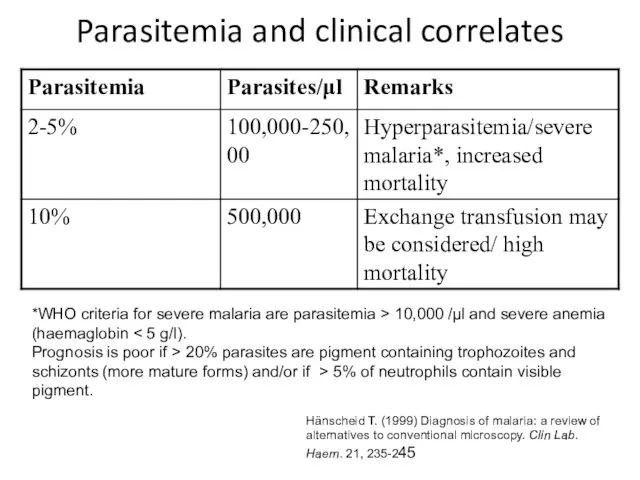
Parasitemia and clinical correlates
*WHO criteria for severe malaria are parasitemia >
Parasitemia and clinical correlates
*WHO criteria for severe malaria are parasitemia >

Malaria Serology – antibody detection
Immunologic assays to detect host response
Antibodies
Malaria Serology – antibody detection
Immunologic assays to detect host response
Antibodies
Malaria Serology – antibody detection
Valuable epidemiologic tool in some settings
Useful for
Identifying
Malaria Serology – antibody detection
Valuable epidemiologic tool in some settings
Useful for
Identifying
Polymerase Chain Reaction (PCR)
Molecular technique to identify parasite genetic material
Uses whole
Polymerase Chain Reaction (PCR)
Molecular technique to identify parasite genetic material
Uses whole
 Қанның тасымалдаушы липопротеиндерінің құрамы, құрылысы және жіктелуі
Қанның тасымалдаушы липопротеиндерінің құрамы, құрылысы және жіктелуі Задачи принципы организации диетического питания
Задачи принципы организации диетического питания Ерте кезеңдегі ұлы дәрігерлер
Ерте кезеңдегі ұлы дәрігерлер Chronic gastritis
Chronic gastritis Болевой синдром и его лечение в ОВП
Болевой синдром и его лечение в ОВП Коматозды жағдайлардың патофизиологиясы
Коматозды жағдайлардың патофизиологиясы Медициналық сұхбаттасу техникасы
Медициналық сұхбаттасу техникасы Анемия. Эритроциттердің формасы мен көлемі
Анемия. Эритроциттердің формасы мен көлемі Хронические обструктивные заболевания легких. Бронхиты
Хронические обструктивные заболевания легких. Бронхиты Лекция 11. Ненаркотические анальгетики
Лекция 11. Ненаркотические анальгетики Основы психосоматики и психологии больного. Сестринское дело. Переподготовка
Основы психосоматики и психологии больного. Сестринское дело. Переподготовка Профилактика ВИЧ-инфекции. СПИД
Профилактика ВИЧ-инфекции. СПИД Ошибки и осложнения после протезирования на имплантатах. Гигиенические мероприятия при наличии в полости рта имплантатов
Ошибки и осложнения после протезирования на имплантатах. Гигиенические мероприятия при наличии в полости рта имплантатов Роль гормонов в обменных процессах, нервно-гуморальная регуляция, её нарушения
Роль гормонов в обменных процессах, нервно-гуморальная регуляция, её нарушения Внутривенные наркотики. Героиновая наркомания. Заменители героина
Внутривенные наркотики. Героиновая наркомания. Заменители героина Опыт хирургического лечения опухолей надпочечников у детей
Опыт хирургического лечения опухолей надпочечников у детей ЭКГ - диагностика при подозрении на инфаркт миокарда
ЭКГ - диагностика при подозрении на инфаркт миокарда Отравление алкоголем и его суррогатами
Отравление алкоголем и его суррогатами NIR
NIR Acquired Immunodeficiency syndrome
Acquired Immunodeficiency syndrome Особенности ведения преждевременных родов
Особенности ведения преждевременных родов Общая характеристика и эпидемиология новообразований ЛОР-органов
Общая характеристика и эпидемиология новообразований ЛОР-органов Цукровий діабет у дітей
Цукровий діабет у дітей Особенности капсульной эндоскопии
Особенности капсульной эндоскопии Дезинфекционные мероприятия при новой коронавирусной инфекции (2019-nCoV)
Дезинфекционные мероприятия при новой коронавирусной инфекции (2019-nCoV) Травмы. Травматический шок
Травмы. Травматический шок Методические указания по приготовлению дезинфицирующим растворов. Отбор проб дезинфектантов
Методические указания по приготовлению дезинфицирующим растворов. Отбор проб дезинфектантов Общий алгоритм подбора очковой коррекции
Общий алгоритм подбора очковой коррекции