- Multiple pregnancy

Содержание
- 2. Multiple Pregnancy/ Multifetalpregnancy The presence of more than one fetus in the gravid uterus is called
- 3. INCIDENCE Hellin’s Law: Twins: 1:89 Triplets: 1:892 Quadruplets: 1:893 Quintuplets: 1:894 Conjoined twins: 1 : 60,000
- 4. Demography Race: most common in Negroes Age: Increased maternal age Parity: more common in multipara Heredity
- 5. Twins Varieties: 1. Dizygotic twins: commonest (Two-third) 2. Monozygotic twins (one-third) Genesis of Twins: Dizygotic twins
- 6. Monozygotic twins (syn: Identical, uniovular): Upto 3 days - diamniotic-dichorionic Between 4th & 7th day -
- 8. Conjoined twins Ventral: 1) Omphalopagus 2) Thoracopagus 3) Cephalopagus 4) Caudal/ ischiopagus Lateral: 1) Parapagus Dorsal:
- 9. Superfecundation Fertilization of two different ova released in the same cycle Superfetation Fertilization of two ova
- 10. Differences in zygocity Monozygotic 1 ova + 1 sperm Same sex Identical features Single or double
- 11. Differences in chorionicity with single placenta D / D ( fused placenta ) Monozygotic or dizygotic
- 12. Diagnosis HISTORY: History of ovulation inducing drugs specially gonadotrophins Family history of twinning (maternal side). SYMPTOMS:
- 13. GENERAL EXAMINATION: Prevalence of anaemia is more than in singleton pregnancy Unusual weight gain, not explained
- 14. Palpation: Fundal height more than the period of amenorrhoea girth more than normal Palpation of too
- 15. D/D of increased fundal height Full bladder Wrong dates Hydramnios Macrosomia Fibroid with preg Ovarian tumor
- 16. INVESTIGATIONS Sonography: In multi fetal pregnancy it is done to obtain the following information: Suspecting twins
- 17. Fetal anomalies Fetal growth monitoring (at every 3-4 weeks interval) for IUGR Presentation and lie of
- 18. Radiography Biochemical tests: raised but not diagnostic Maternal serum chorionic gonadotrophin, Alpha fetoprotein Unconjugated oestriol
- 19. Lie and Presentation Longitudinal lie (90%) both vertex (40%) Vertex + breech (28%) breech + vertex
- 20. Complications Maternal Pregnancy Labour Puerperium Fetal MATERNAL: During pregnancy: - miscarriages Hyperemesis gravidorum Anaemia Pre-eclampsia (25%)
- 21. GDM ( 2 – 3 times) Antepartum hemorrhage – placenta previa and placental abruption Cholestasis of
- 22. During Labour: Prelabour rupture of the membranes Cord prolapse Incoordinate uterine contractions Increased operative interference Placental
- 23. FETAL – more with monochorionic Spontaneous abortion Single fetal demise Vanishing twin – before 10 weeks
- 24. FETAL – more with monochorionic Low birth weight ( 90%) Prematurity – spontaneous or iatrogenic Fetal
- 25. FETAL COMPLICATIONS (ctd) Congenital anomalies – conjoined twins, neural tube defects – anencephaly, hydrocephaly, microcephaly, cardiac
- 26. FETAL COMPLICATIONS (ctd) TRAP -Twin reversed arterial perfusion syndrome or Acardiac twin - absent heart in
- 27. Monoamniotic twins high perinatal morbidity, mortality. Causes : cord entanglement congenital anomaly preterm birth twin to
- 28. Antenatal Management Diet: additional 300 K cal per day, increased proteins, 60 to 100 mg of
- 29. Management During Labour Place of delivery: tertiary level hospital FIRST STAGE: blood to be cross matched
- 30. Management During Labour SECOND STAGE –delivery of first baby as in singleton pregnancy start an IV
- 31. Management During Labour Delivery of second twin – problems & interventions -inadequate contraction- augmentation – ARM,
- 33. Скачать презентацию
Multiple Pregnancy/ Multifetalpregnancy
The presence of more than one fetus in the
Multiple Pregnancy/ Multifetalpregnancy
The presence of more than one fetus in the
INCIDENCE
Hellin’s Law:
Twins: 1:89
Triplets: 1:892
Quadruplets: 1:893
Quintuplets: 1:894
Conjoined twins: 1 : 60,000
Worldwide incidence
INCIDENCE
Hellin’s Law:
Twins: 1:89
Triplets: 1:892
Quadruplets: 1:893
Quintuplets: 1:894
Conjoined twins: 1 : 60,000
Worldwide incidence
Demography
Race: most common in Negroes
Age: Increased maternal age
Parity: more common in
Demography
Race: most common in Negroes
Age: Increased maternal age
Parity: more common in
Twins
Varieties:
1. Dizygotic twins: commonest (Two-third)
2. Monozygotic twins (one-third)
Genesis of
Twins
Varieties:
1. Dizygotic twins: commonest (Two-third)
2. Monozygotic twins (one-third)
Genesis of
Monozygotic twins (syn: Identical, uniovular):
Upto 3 days - diamniotic-dichorionic
Between 4th
Monozygotic twins (syn: Identical, uniovular):
Upto 3 days - diamniotic-dichorionic
Between 4th
Conjoined twins
Ventral:
1) Omphalopagus
2) Thoracopagus
3) Cephalopagus
4) Caudal/
Conjoined twins
Ventral:
1) Omphalopagus
2) Thoracopagus
3) Cephalopagus
4) Caudal/
Superfecundation
Fertilization of two different ova released in the same cycle
Superfetation
Superfecundation
Fertilization of two different ova released in the same cycle
Superfetation
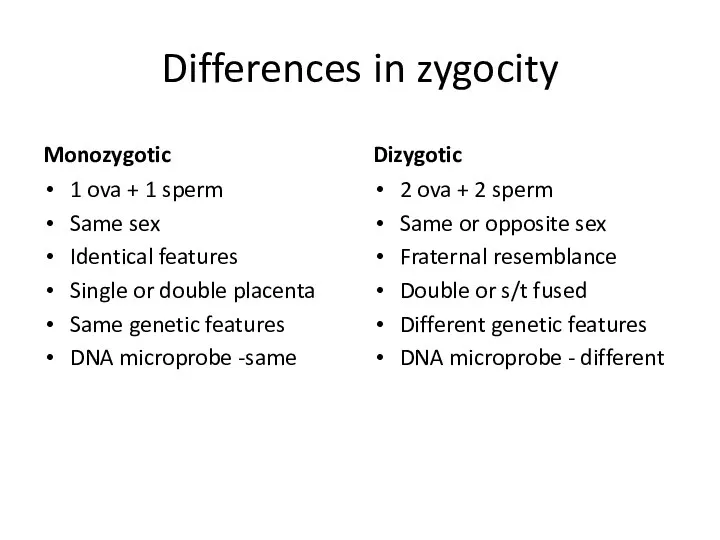
Differences in zygocity
Monozygotic
1 ova + 1 sperm
Same sex
Identical features
Single or double
Differences in zygocity
Monozygotic
1 ova + 1 sperm
Same sex
Identical features
Single or double
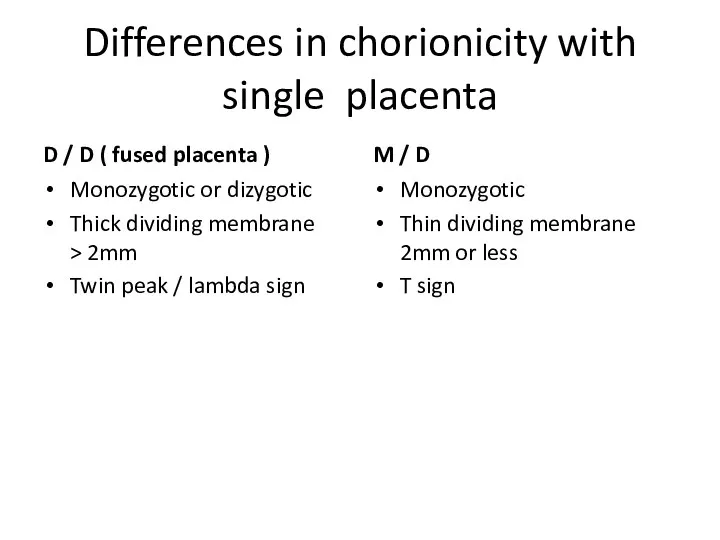
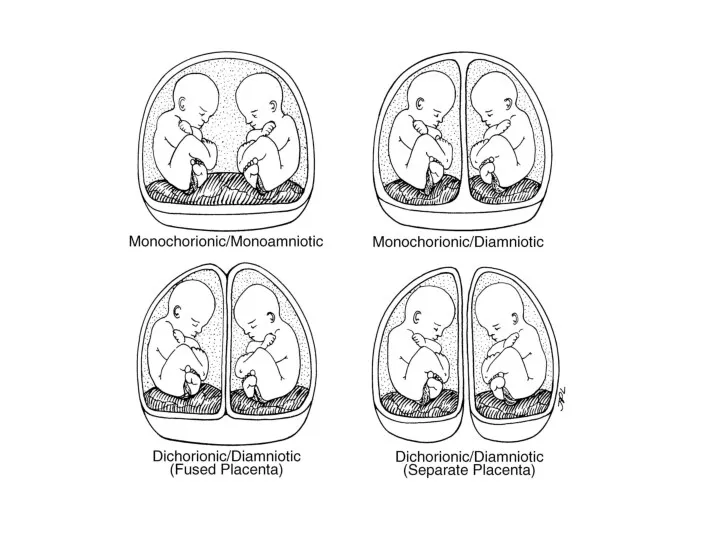
Differences in chorionicity with single placenta
D / D ( fused placenta
Differences in chorionicity with single placenta
D / D ( fused placenta
Diagnosis
HISTORY:
History of ovulation inducing drugs specially gonadotrophins
Family history of twinning
Diagnosis
HISTORY:
History of ovulation inducing drugs specially gonadotrophins
Family history of twinning
GENERAL EXAMINATION:
Prevalence of anaemia is more than in singleton pregnancy
GENERAL EXAMINATION:
Prevalence of anaemia is more than in singleton pregnancy
Palpation:
Fundal height more than the period of amenorrhoea
girth more than
Palpation:
Fundal height more than the period of amenorrhoea
girth more than
D/D of increased fundal height
Full bladder
Wrong dates
Hydramnios
Macrosomia
Fibroid with preg
Ovarian tumor
D/D of increased fundal height
Full bladder
Wrong dates
Hydramnios
Macrosomia
Fibroid with preg
Ovarian tumor
INVESTIGATIONS
Sonography: In multi fetal pregnancy it is done to obtain the
INVESTIGATIONS
Sonography: In multi fetal pregnancy it is done to obtain the
Fetal anomalies
Fetal growth monitoring (at every 3-4 weeks interval) for
Fetal growth monitoring (at every 3-4 weeks interval) for
Radiography
Biochemical tests: raised but not diagnostic
Maternal serum chorionic
Radiography
Biochemical tests: raised but not diagnostic
Maternal serum chorionic
Lie and Presentation
Longitudinal lie (90%)
both vertex (40%)
Vertex + breech
Lie and Presentation
Longitudinal lie (90%)
both vertex (40%)
Vertex + breech
Complications
Maternal
Pregnancy
Labour
Puerperium
Fetal
MATERNAL: During pregnancy:
- miscarriages
Hyperemesis gravidorum
Anaemia
Complications
Maternal
Pregnancy
Labour
Puerperium
Fetal
MATERNAL: During pregnancy:
- miscarriages
Hyperemesis gravidorum
Anaemia
GDM ( 2 – 3 times)
Antepartum hemorrhage – placenta previa and
GDM ( 2 – 3 times)
Antepartum hemorrhage – placenta previa and
During Labour:
Prelabour rupture of the membranes
Cord prolapse
Incoordinate uterine contractions
Increased
Prelabour rupture of the membranes
Cord prolapse
Incoordinate uterine contractions
Increased
FETAL – more with monochorionic
Spontaneous abortion
Single fetal demise
Vanishing twin
FETAL – more with monochorionic
Spontaneous abortion
Single fetal demise
Vanishing twin
FETAL – more with monochorionic
Low birth weight ( 90%)
Prematurity –
FETAL – more with monochorionic
Low birth weight ( 90%)
Prematurity –
FETAL COMPLICATIONS (ctd)
Congenital anomalies – conjoined twins, neural tube defects
FETAL COMPLICATIONS (ctd)
Congenital anomalies – conjoined twins, neural tube defects
FETAL COMPLICATIONS (ctd)
TRAP -Twin reversed arterial perfusion syndrome or Acardiac
FETAL COMPLICATIONS (ctd)
TRAP -Twin reversed arterial perfusion syndrome or Acardiac
Monoamniotic twins
high perinatal morbidity, mortality.
Causes : cord entanglement
Monoamniotic twins
high perinatal morbidity, mortality.
Causes : cord entanglement
Antenatal Management
Diet: additional 300 K cal per day, increased proteins, 60
Antenatal Management
Diet: additional 300 K cal per day, increased proteins, 60
Management During Labour
Place of delivery: tertiary level hospital
FIRST STAGE:
blood to
Management During Labour
Place of delivery: tertiary level hospital
FIRST STAGE:
blood to
Management During Labour
SECOND STAGE –delivery of first baby
as in singleton
Management During Labour
SECOND STAGE –delivery of first baby
as in singleton
Management During Labour
Delivery of second twin – problems & interventions
-inadequate
Management During Labour
Delivery of second twin – problems & interventions
-inadequate
 Медиастинит. Этиология және патогенез
Медиастинит. Этиология және патогенез Патанатомия неспецифического язвенного колита, аппендицита
Патанатомия неспецифического язвенного колита, аппендицита Основы медицинской протозоологии. Тип простейшие. Представители классов споровики и инфузории
Основы медицинской протозоологии. Тип простейшие. Представители классов споровики и инфузории ОМС АО Страховая компания СОГАЗ-Мед. Обязательное медицинское страхование
ОМС АО Страховая компания СОГАЗ-Мед. Обязательное медицинское страхование Аудиологический скрининг новорожденных. Генетические аспекты тугоухости
Аудиологический скрининг новорожденных. Генетические аспекты тугоухости Язвенная болезнь желудка и двенадцатиперстной кишки
Язвенная болезнь желудка и двенадцатиперстной кишки Психиатриялық науқастарды тексеру әдістері
Психиатриялық науқастарды тексеру әдістері Аборты. О вреде абортов
Аборты. О вреде абортов Antimicrobial drugs
Antimicrobial drugs Көз туберкулезі
Көз туберкулезі Фонетико-фонематическое недоразвитие
Фонетико-фонематическое недоразвитие Анксиолитики (транквилизаторы)
Анксиолитики (транквилизаторы) Психические расстройства позднего возраста
Психические расстройства позднего возраста Взаимодействие лекарственных препаратов
Взаимодействие лекарственных препаратов Жасушалық иммунитет жүйесінің негізгі қызметтері. Иммунологиялық төзімділік
Жасушалық иммунитет жүйесінің негізгі қызметтері. Иммунологиялық төзімділік Дискинезия желчевыводящих путей у детей
Дискинезия желчевыводящих путей у детей Патологиялык анатомияның заманауи зерттеу әдістері. Қр патологиялық анатомиялық қызметі
Патологиялык анатомияның заманауи зерттеу әдістері. Қр патологиялық анатомиялық қызметі Психическая предрасположенность к развитию зависимости от ПАВ
Психическая предрасположенность к развитию зависимости от ПАВ Питание кормящей матери
Питание кормящей матери Отек легких
Отек легких Развитие отечественной медицины в годы Первой мировой войны
Развитие отечественной медицины в годы Первой мировой войны Симптоматика урологических заболеваний (изменения мочи)
Симптоматика урологических заболеваний (изменения мочи) Наружные кишечные свищи
Наружные кишечные свищи Клинический случай вестибулярного синдрома. Плоскоклеточная карцинома (SCC) слюнной железы у кошки
Клинический случай вестибулярного синдрома. Плоскоклеточная карцинома (SCC) слюнной железы у кошки Первая помощь при повреждениях головы и позвоночника
Первая помощь при повреждениях головы и позвоночника Тканевая совместимость и переливание крови
Тканевая совместимость и переливание крови Парентералды жолмен берілетін вирусты аурулар (ЖИТС) және олардың алдын алу шаралары
Парентералды жолмен берілетін вирусты аурулар (ЖИТС) және олардың алдын алу шаралары Гнатология. Основные задачи современной гнатологии
Гнатология. Основные задачи современной гнатологии