- Нарушения половой дифференцировки

Содержание
- 2. Неопределенного вида гениталии у новорожденного являются, sine qua non*, парадигмой DSD Consequences of the ESPE/LWPES guidelines
- 3. В составе междисциплинарной команды Мы должны сообща определять тактику лечения детей, Для этого необходимо понимать друг
- 4. Терминология/номенклатура Римский бог Терминус Commentary to «Attitudes towards ‘disorders of sex development’ nomenclature among affected” The
- 5. Терминология в англоязычной литературе: disorders of sex development (DSD) variations of sex development differences of sex
- 6. Терминология в отечественной литературе При этом некоторые авторы, использующие термин «нарушения формирования пола», с одной стороны
- 7. К терминологии «Нарушения полового развития» – прямой перевод «disorders of sex development (DSD)». При этом, строго
- 8. Терминология в отечественной литературе Вызывает вопросы: интерсексуальное строение гермафродитное строение двойственное строение и т.д. Описание НПО,
- 9. Классификация Пример классификации Чикагского консенсуса: АМН, anti-mullerian hormone, CAlS, complete androgen insensitivity syndrome, DSD, disorders of
- 10. К терминологии A Practical Approach to Ambiguous Genitalia in the Newborn Period CHAPTER The evaluation and
- 11. Вариант классификации Consequences of the ESPE/LWPES guidelines for diagnosis and treatment of disorders of sex leuan
- 12. Классификация: расширенное толкование DSD How should we classify intersex disorders? It is a tall order to
- 13. Варианты классификации «non-hormonal/non-chromosomal DSD» «non-endocrine/malformative DSD» Surgery in disorders of sex development (DSD) with a gender
- 14. Классификация: имеющиеся проблемы Отсутствие единой общепризнанной классификации Включение в одну группу больных, имеющих совершенно разные клинические
- 15. Терминология и классификация Без общего языка трудно понимать друг друга Таким образом, как представляется, назрела насущная
- 16. Рабочая классификация Женский псевдогермафродитизм Интерсекс Нарушения половой дифференцировки (НПД = DSD) Мужской псевдогермафродитизм Истинный гермафродитизм Смешанная
- 17. Назначение пола INVESTIGATION AND MANAGEMENT OF DSD Pediatrics Official journal of the American academy of pediatrics
- 18. Регистрация новорожденного без назначения пола Intersex and gender assignment: the third way? S F Ahmed S
- 19. Назначение мужского пола при 46,ХХ САН Approach to assigning gender in 46,XX Congenital Adrenal Hyperplasia with
- 20. Хирургическое лечение: решение Консенсуса Surgical Management Pediatrics Official journal of the American academy of pediatrics The
- 21. Хирургическое лечение: изменение при обновлении Консенсуса Global Disorders of Sex Development Update since 2006: Perceptions, Approach
- 22. Запрет хирургического лечения В 2017 году ПАСЕ была принята резолюция о необходимости запрета любого лечения, в
- 23. Хирургическое лечение: мнение ESPU Open letter to the Council of Europe European Sociaty for Paediatric Urology
- 24. Хирургическое лечение: консенсус ESPU и SPU Сложные медицинские проблемы должны оставаться в компетенции семьи и квалифицированной
- 25. Хирургическое лечение: конструктивный взгляд Should CAH in Females Be Classified as DSD? Ricardo Gonzalez and Barbara
- 26. Чикагский консенсус 2005 г. Management framework paradigms for disorder of sex development ABSTRACT Until 2005, questions
- 27. Тихая революция The quiet revolution best practice & research clinical endocrinology & metabolism Ieuan A A.Hughes
- 28. «Поддерживающие группы»: ISNA peer support groups, patient advocacy groups, gender-right activist groups, intersex advocates…
- 29. «Поддерживающие группы»: работа с ООН
- 30. «Поддерживающие группы»: работа с ВОЗ
- 31. «Поддерживающие группы»: работа с правозащитными организациями
- 32. «Поддерживающие группы»: взгляд на лечение Хирургические вмешательства на гениталиях и гонадах у младенцев и детей с
- 33. «Поддерживающие группы»: работа с ООН Report of the Special Rapporteur on torture and other cruel, inhuman
- 34. «Поддерживающие группы»: мнение ESPU и SPU The ESPU/SPU standpoint on the surgical management of Disorders of
- 35. «Поддерживающие группы»: отсутствие единой реакции медицинского сообщества Кажется странным, но медицинское сообщество на Западе, по сути,
- 36. «Поддерживающие группы»: ARSI Наверное, можно считать, что ничего страшного не происходит, и все образуется. Однако, как
- 37. Поддерживающие группы»: Intersex Russia В-третьих, теперь у нас в стране появилась и вторая такая группа, представители
- 38. «Поддерживающие группы»: работа в России ТАКТИКА ВЕДЕНИЯ СИНДРОМА АНДРОГЕННОЙ РЕЗИСТЕНТНОСТИ В РОССИЙСКОЙ ФЕДЕРАЦИИ И СОВРЕМЕННЫЙ ВЗГЛЯД
- 40. Скачать презентацию
Неопределенного вида гениталии
у новорожденного являются,
sine qua non*, парадигмой DSD
Consequences
Неопределенного вида гениталии
у новорожденного являются,
sine qua non*, парадигмой DSD
Consequences
В составе междисциплинарной команды
Мы должны сообща определять тактику лечения детей,
Для этого
В составе междисциплинарной команды
Мы должны сообща определять тактику лечения детей,
Для этого
Терминология/номенклатура
Римский бог Терминус
Commentary to «Attitudes towards ‘disorders of sex development’ nomenclature
Терминология/номенклатура
Римский бог Терминус
Commentary to «Attitudes towards ‘disorders of sex development’ nomenclature

Терминология
в англоязычной литературе:
disorders
of sex development (DSD)
variations
of sex development
differences
of sex development
Терминология
в англоязычной литературе:
disorders
of sex development (DSD)
variations
of sex development
differences
of sex development
Терминология в отечественной литературе
При этом некоторые авторы, использующие термин «нарушения формирования
Терминология в отечественной литературе
При этом некоторые авторы, использующие термин «нарушения формирования
К терминологии
«Нарушения полового развития» – прямой перевод «disorders of sex development
К терминологии
«Нарушения полового развития» – прямой перевод «disorders of sex development
Терминология в отечественной литературе
Вызывает вопросы:
интерсексуальное строение
гермафродитное строение
двойственное строение и т.д.
Описание НПО,
Терминология в отечественной литературе
Вызывает вопросы:
интерсексуальное строение
гермафродитное строение
двойственное строение и т.д.
Описание НПО,
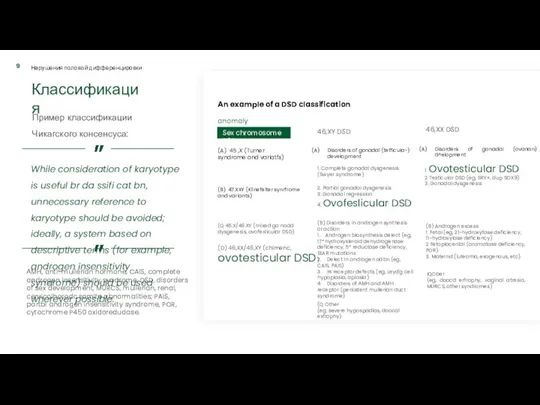
Классификация
Пример классификации
Чикагского консенсуса:
АМН, anti-mullerian hormone, CAlS, complete androgen insensitivity
Классификация
Пример классификации
Чикагского консенсуса:
АМН, anti-mullerian hormone, CAlS, complete androgen insensitivity
К терминологии
A Practical Approach to Ambiguous Genitalia in the Newborn Period
CHAPTER
The
К терминологии
A Practical Approach to Ambiguous Genitalia in the Newborn Period
CHAPTER
The
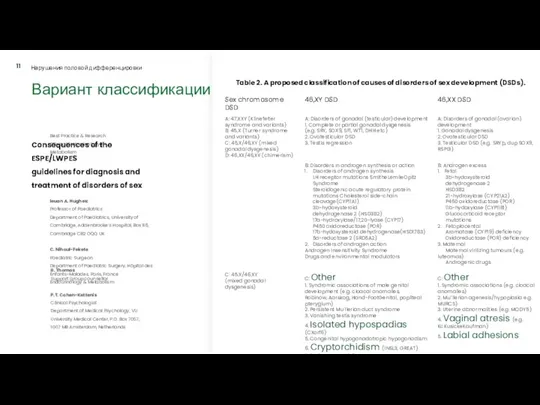
Вариант классификации
Consequences of the ESPE/LWPES
guidelines for diagnosis and treatment of disorders
Вариант классификации
Consequences of the ESPE/LWPES
guidelines for diagnosis and treatment of disorders
Классификация: расширенное толкование DSD
How should we classify intersex disorders?
It is a
Классификация: расширенное толкование DSD
How should we classify intersex disorders?
It is a
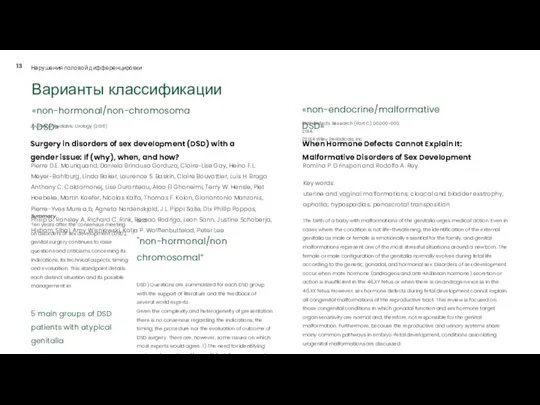
Варианты классификации
«non-hormonal/non-chromosomal DSD»
«non-endocrine/malformative DSD»
Surgery in disorders of sex development (DSD) with
Варианты классификации
«non-hormonal/non-chromosomal DSD»
«non-endocrine/malformative DSD»
Surgery in disorders of sex development (DSD) with
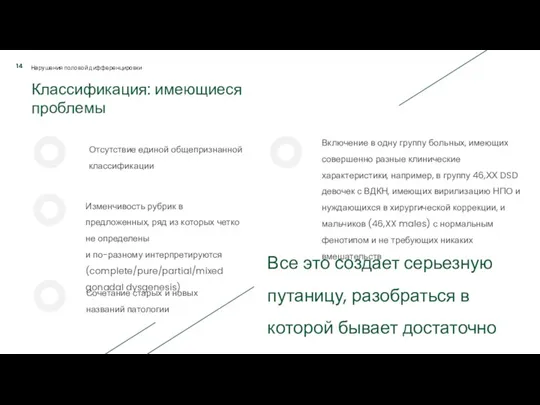
Классификация: имеющиеся проблемы
Отсутствие единой общепризнанной классификации
Включение в одну группу больных, имеющих
Классификация: имеющиеся проблемы
Отсутствие единой общепризнанной классификации
Включение в одну группу больных, имеющих

Терминология и классификация
Без общего языка трудно понимать друг друга
Таким образом, как
Терминология и классификация
Без общего языка трудно понимать друг друга
Таким образом, как
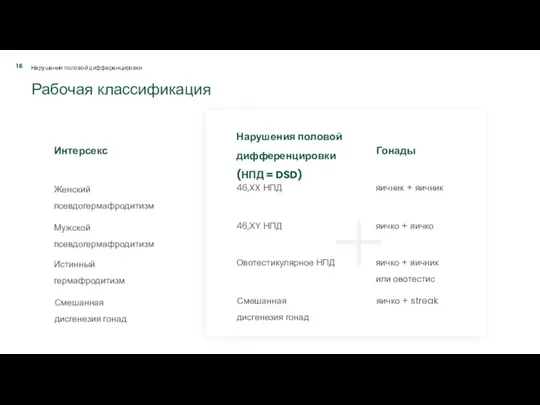
Рабочая классификация
Женский псевдогермафродитизм
Интерсекс
Нарушения половой дифференцировки (НПД = DSD)
Мужской
псевдогермафродитизм
Истинный гермафродитизм
Смешанная дисгенезия
Рабочая классификация
Женский псевдогермафродитизм
Интерсекс
Нарушения половой дифференцировки (НПД = DSD)
Мужской
псевдогермафродитизм
Истинный гермафродитизм
Смешанная дисгенезия
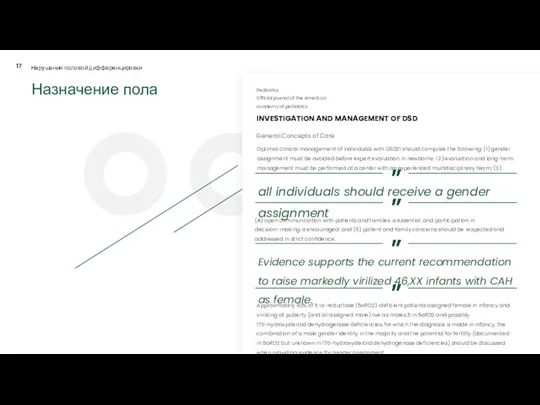
Назначение пола
INVESTIGATION AND MANAGEMENT OF DSD
Pediatrics
Official journal of the American academy
Назначение пола
INVESTIGATION AND MANAGEMENT OF DSD
Pediatrics
Official journal of the American academy
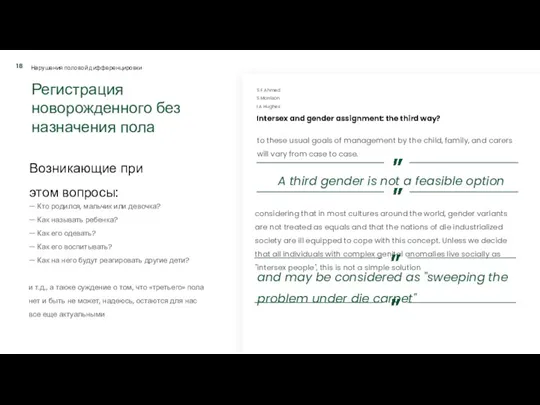
Регистрация новорожденного без назначения пола
Intersex and gender assignment: the third way?
Регистрация новорожденного без назначения пола
Intersex and gender assignment: the third way?
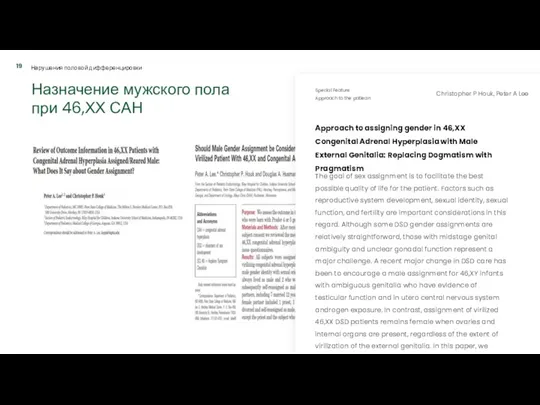
Назначение мужского пола
при 46,ХХ САН
Approach to assigning gender in 46,XX
Назначение мужского пола
при 46,ХХ САН
Approach to assigning gender in 46,XX
Хирургическое лечение: решение Консенсуса
Surgical Management
Pediatrics
Official journal of the American academy of
Хирургическое лечение: решение Консенсуса
Surgical Management
Pediatrics
Official journal of the American academy of
Хирургическое лечение:
изменение при обновлении Консенсуса
Global Disorders of Sex Development Update
Хирургическое лечение:
изменение при обновлении Консенсуса
Global Disorders of Sex Development Update
Запрет хирургического
лечения
В 2017 году ПАСЕ была принята резолюция о необходимости
Запрет хирургического
лечения
В 2017 году ПАСЕ была принята резолюция о необходимости
Хирургическое лечение: мнение ESPU
Open letter to the Council of Europe
European
Хирургическое лечение: мнение ESPU
Open letter to the Council of Europe
European

Хирургическое лечение: консенсус ESPU и SPU
Сложные медицинские проблемы должны оставаться
Хирургическое лечение: консенсус ESPU и SPU
Сложные медицинские проблемы должны оставаться

Хирургическое лечение: конструктивный взгляд
Should CAH in Females Be Classified as DSD?
Ricardo
Хирургическое лечение: конструктивный взгляд
Should CAH in Females Be Classified as DSD?
Ricardo
Чикагский консенсус
2005 г.
Management framework paradigms for disorder of sex development
ABSTRACT
Until
Чикагский консенсус
2005 г.
Management framework paradigms for disorder of sex development
ABSTRACT
Until
Тихая революция
The quiet revolution
best practice
& research clinical endocrinology & metabolism
Ieuan
Тихая революция
The quiet revolution
best practice
& research clinical endocrinology & metabolism
Ieuan
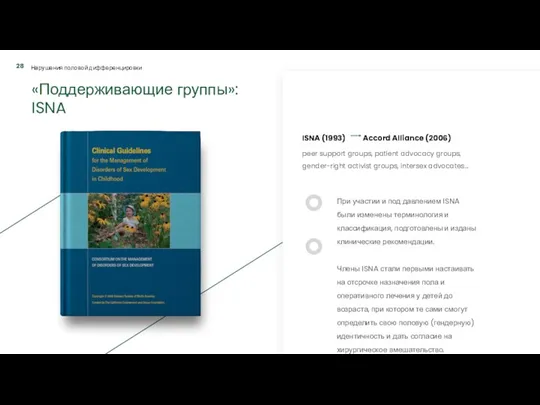
«Поддерживающие группы»: ISNA
peer support groups, patient advocacy groups, gender-right activist groups,
«Поддерживающие группы»: ISNA
peer support groups, patient advocacy groups, gender-right activist groups,
«Поддерживающие группы»: работа с ООН
«Поддерживающие группы»: работа с ООН
«Поддерживающие группы»: работа с ВОЗ
«Поддерживающие группы»: работа с ВОЗ
«Поддерживающие группы»: работа с правозащитными организациями
«Поддерживающие группы»: работа с правозащитными организациями
«Поддерживающие группы»: взгляд на лечение
Хирургические вмешательства на гениталиях и гонадах
«Поддерживающие группы»: взгляд на лечение
Хирургические вмешательства на гениталиях и гонадах
«Поддерживающие группы»: работа с ООН
Report of the Special Rapporteur on
«Поддерживающие группы»: работа с ООН
Report of the Special Rapporteur on
«Поддерживающие группы»: мнение ESPU и SPU
The ESPU/SPU standpoint on the
«Поддерживающие группы»: мнение ESPU и SPU
The ESPU/SPU standpoint on the
«Поддерживающие группы»: отсутствие единой реакции медицинского сообщества
Кажется странным, но медицинское сообщество
«Поддерживающие группы»: отсутствие единой реакции медицинского сообщества
Кажется странным, но медицинское сообщество
«Поддерживающие группы»: ARSI
Наверное, можно считать, что ничего страшного не происходит,
«Поддерживающие группы»: ARSI
Наверное, можно считать, что ничего страшного не происходит,
Поддерживающие группы»: Intersex Russia
В-третьих, теперь у нас в стране появилась
Поддерживающие группы»: Intersex Russia
В-третьих, теперь у нас в стране появилась

«Поддерживающие группы»: работа в России
ТАКТИКА ВЕДЕНИЯ СИНДРОМА АНДРОГЕННОЙ РЕЗИСТЕНТНОСТИ В
«Поддерживающие группы»: работа в России
ТАКТИКА ВЕДЕНИЯ СИНДРОМА АНДРОГЕННОЙ РЕЗИСТЕНТНОСТИ В
 Вирусты. Гепатит В. Эпидемиологиясы
Вирусты. Гепатит В. Эпидемиологиясы Реабилитация при Инфаркте Миокарда
Реабилитация при Инфаркте Миокарда Отбеливание зубов
Отбеливание зубов Базовая модель медико-социальной работы
Базовая модель медико-социальной работы Дизайны клинических исследований
Дизайны клинических исследований Составление схемы диспансерного наблюдений курируемых хронических больных
Составление схемы диспансерного наблюдений курируемых хронических больных Общая анестезия. . Виды общей анестезии. Клиническая фармакология средств применяемых в анестезиологическом пособии
Общая анестезия. . Виды общей анестезии. Клиническая фармакология средств применяемых в анестезиологическом пособии Нарушения речи при детских неврозах. Мутизм, сурдомутизм, заикание
Нарушения речи при детских неврозах. Мутизм, сурдомутизм, заикание Профессиональные нейротоксикозы
Профессиональные нейротоксикозы Жұқпалы үрдіс патофизиологиясы. Сепсис және сепсистік сілейменің патогенезі
Жұқпалы үрдіс патофизиологиясы. Сепсис және сепсистік сілейменің патогенезі Лечебное питание при различных нарушениях обмена веществ
Лечебное питание при различных нарушениях обмена веществ Электрическая ось сердца и электрическая позиция сердца
Электрическая ось сердца и электрическая позиция сердца Biological Therapy in Psychiatry
Biological Therapy in Psychiatry Облитерирующий атеросклероз брюшной аорты и артерий нижних конечностей
Облитерирующий атеросклероз брюшной аорты и артерий нижних конечностей Жүрек гликозидтері
Жүрек гликозидтері Визуальная диагностика при гипоталамо-гипофизарном ожирении
Визуальная диагностика при гипоталамо-гипофизарном ожирении Топографическая анатомия нижней конечности. Области мышечной и сосудистой лакуны, бедра, подколенная ямка, ягодичная область
Топографическая анатомия нижней конечности. Области мышечной и сосудистой лакуны, бедра, подколенная ямка, ягодичная область Внелегочной туберкулез
Внелегочной туберкулез Ұрықтың туа пайда болған орталық жүйке жүйесінің ақаулары
Ұрықтың туа пайда болған орталық жүйке жүйесінің ақаулары Ультразвуковая терапия
Ультразвуковая терапия Морфология и цикл развития дизентерийной амебы
Морфология и цикл развития дизентерийной амебы Дифференциальный диагноз анемий
Дифференциальный диагноз анемий Тәуліктік PH-метрия
Тәуліктік PH-метрия Заболевания простаты
Заболевания простаты Абдоминальный массаж
Абдоминальный массаж Электронное здравоохранение. Медицинские информационные системы
Электронное здравоохранение. Медицинские информационные системы Организация работы с непригодными для медицинского использования лекарственными средствами
Организация работы с непригодными для медицинского использования лекарственными средствами Алгоритм диагностики заболеваний органов дыхания
Алгоритм диагностики заболеваний органов дыхания