- Neurocognitive disorders

Содержание
- 2. Outline Delirium Clinical Description and Statistics Treatment and Prevention Major and Mild Neurocognitive Disorders Clinical Description
- 5. Memory Quiz Which color is on top of a stoplight? Whose image is on a penny?
- 6. Which color is on top of a stoplight? (Answer: red) Whose image is on a penny?
- 7. Neurocognitive Disorders: An Overview Affect learning, memory, and consciousness Most develop later in life Types of
- 8. Delirium: An Overview Nature of delirium Central features – impaired consciousness and cognition Develops rapidly over
- 9. Delirium: An Overview, Continued Facts and statistics Affects up 20% of adults in acute care facilities
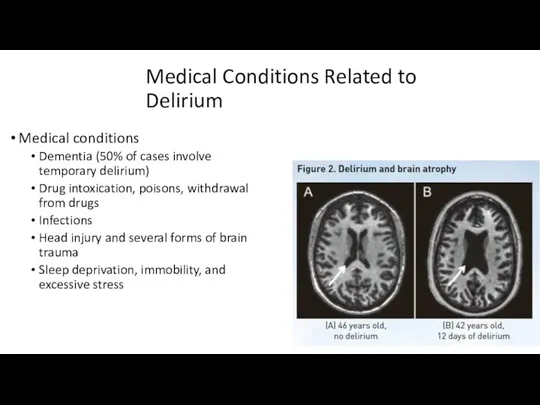
- 10. Medical Conditions Related to Delirium Medical conditions Dementia (50% of cases involve temporary delirium) Drug intoxication,
- 11. Treatment and Prevention of Delirium Treatment Attention to underlying causes Psychosocial interventions Reassurance/comfort, coping strategies, inclusion
- 12. Major and Mild Neurocognitive Disorders Nature of dementia Gradual deterioration of brain functioning Deterioration in judgment
- 13. Major and Mild Neurocognitive Disorders: DSM Criteria Major neurocognitive disorder: The new DSM-5 term for dementia
- 14. Major Neurocognitive Disorder: DSM-5 DSM-5 criteria One or more cognitive deficits that represent a decrease from
- 15. Major Neurocognitive Disorder Prevalence and Statistics Prevalence and statistics New case identified every 7 seconds 5%
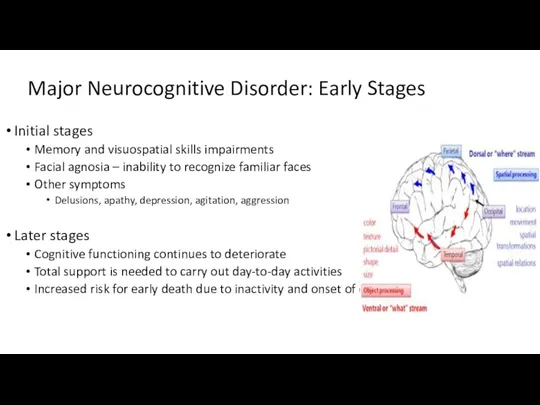
- 16. Major Neurocognitive Disorder: Early Stages Initial stages Memory and visuospatial skills impairments Facial agnosia – inability
- 17. DSM-5 Types of Major and Mild Neurocognitive Disorder Due to Alzheimer’s Disease Frontotemporal Vascular With Lewy
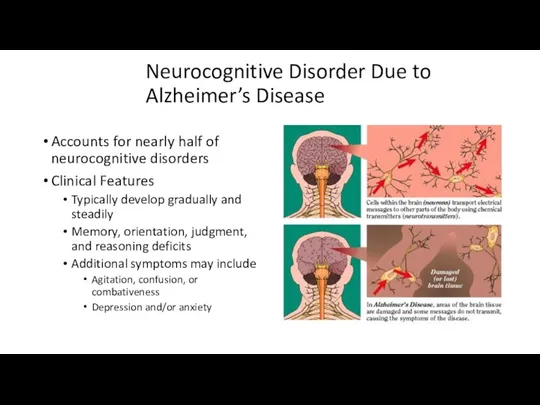
- 18. Neurocognitive Disorder Due to Alzheimer’s Disease Accounts for nearly half of neurocognitive disorders Clinical Features Typically
- 19. Causes of Neurocognitive Disorder: The Example of Alzheimer’s Disease, Continued Multiple genes are involved in Alzheimer’s
- 20. Causes of Neurocognitive Disorder: The Example of Alzheimer’s Disease, Part 3 Deterministic genes Rare genes that
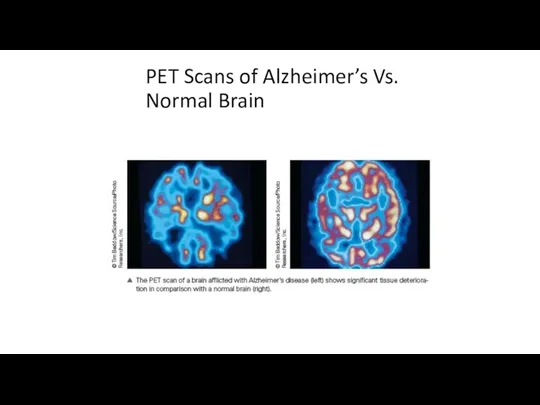
- 21. PET Scans of Alzheimer’s Vs. Normal Brain
- 22. Causes of Neurocognitive Disorder: The Example of Alzheimer’s Disease Features of brains with Alzheimer’s disease Neurofibrillary
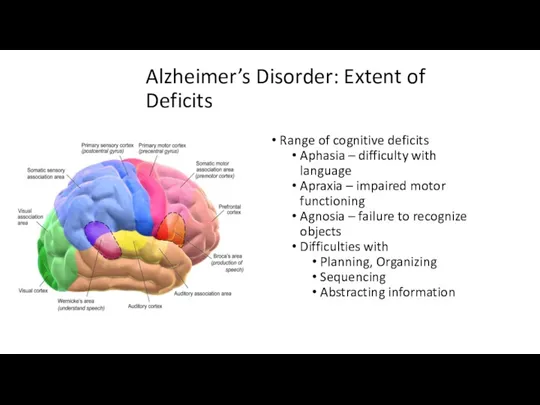
- 23. Alzheimer’s Disorder: Extent of Deficits Range of cognitive deficits Aphasia – difficulty with language Apraxia –
- 24. Neurocognitive Disorder Due to Alzheimer’s Disease : Statistics Early and later stages = slow During middle
- 25. Lisa Genova: Cognitive reserve Cognitive reserve also indicates a resilience to neuropathological damage, but the emphasis
- 26. Neurocognitive Disorder Due to Alzheimer’s Disease : Prevalence Prevalence More common in less educated individuals More
- 27. Graph of Predicted Alzheimer’s Incidence [INSERT Figure 15.1 HERE, p. 548]
- 28. Education Complexity of vocabulary physical and mental activity, positive attitude Nature and progression of the disease
- 29. Vascular Neurocognitive Disorder Caused by blockage or damage to blood vessels Second leading cause of neurocognitive
- 30. Vascular Neurocognitive Disorder: Features Features Cognitive disturbances – identical to dementia Obvious neurological signs of brain
- 31. Vascular Neurocognitive Disorder Caused by blockage or damage to blood vessels Second leading cause of neurocognitive
- 32. Prevention of Neurocognitive Disorders Reducing risk in older adults Use of anti-inflammatory medications Control blood pressure,
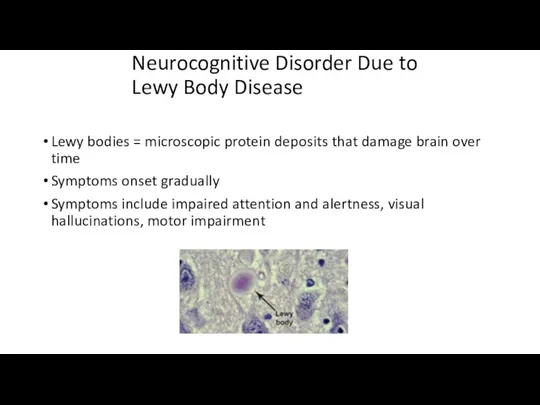
- 33. Neurocognitive Disorder Due to Lewy Body Disease Lewy bodies = microscopic protein deposits that damage brain
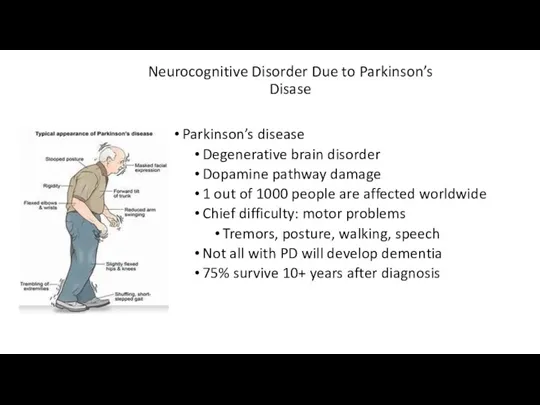
- 34. Neurocognitive Disorder Due to Parkinson’s Disase Parkinson’s disease Degenerative brain disorder Dopamine pathway damage 1 out
- 35. Neurocognitive Disorder Due to Huntington’s Disease Huntington’s Disease = genetic autosomal dominant disorder Caused by a
- 36. Neurocognitive Disorder Due to Prion Disease Disorder of proteins in the brain that reproduce and cause
- 37. Summary of Neurocognitive Disorders Cognitive disorders span a range of deficits Affect attention, memory, language, and
- 39. Скачать презентацию
Outline
Delirium
Clinical Description and Statistics
Treatment and Prevention
Major and Mild Neurocognitive Disorders
Clinical Description
Outline
Delirium
Clinical Description and Statistics
Treatment and Prevention
Major and Mild Neurocognitive Disorders
Clinical Description
Memory Quiz
Which color is on top of a stoplight?
Whose image
Memory Quiz
Which color is on top of a stoplight?
Whose image
Which color is on top of a stoplight? (Answer: red)
Whose image
Which color is on top of a stoplight? (Answer: red)
Whose image
Neurocognitive Disorders: An Overview
Affect learning, memory, and consciousness
Most develop later in
Neurocognitive Disorders: An Overview
Affect learning, memory, and consciousness
Most develop later in
Delirium: An Overview
Nature of delirium
Central features – impaired consciousness and
Delirium: An Overview
Nature of delirium
Central features – impaired consciousness and
Delirium: An Overview, Continued
Facts and statistics
Affects up 20% of adults in
Delirium: An Overview, Continued
Facts and statistics
Affects up 20% of adults in
Medical Conditions Related to Delirium
Medical conditions
Dementia (50% of cases involve
Medical Conditions Related to Delirium
Medical conditions
Dementia (50% of cases involve
Treatment and Prevention of Delirium
Treatment
Attention to underlying causes
Psychosocial interventions
Reassurance/comfort, coping
Treatment and Prevention of Delirium
Treatment
Attention to underlying causes
Psychosocial interventions
Reassurance/comfort, coping
Major and Mild Neurocognitive Disorders
Nature of dementia
Gradual deterioration of brain functioning
Deterioration
Major and Mild Neurocognitive Disorders
Nature of dementia
Gradual deterioration of brain functioning
Deterioration
Major and Mild Neurocognitive Disorders: DSM Criteria
Major neurocognitive disorder:
The new
Major and Mild Neurocognitive Disorders: DSM Criteria
Major neurocognitive disorder:
The new
Major Neurocognitive Disorder:
DSM-5
DSM-5 criteria
One or more cognitive deficits that
Major Neurocognitive Disorder:
DSM-5
DSM-5 criteria
One or more cognitive deficits that
Major Neurocognitive Disorder Prevalence and Statistics
Prevalence and statistics
New case identified
Major Neurocognitive Disorder Prevalence and Statistics
Prevalence and statistics
New case identified
Major Neurocognitive Disorder: Early Stages
Initial stages
Memory and visuospatial skills impairments
Facial agnosia
Major Neurocognitive Disorder: Early Stages
Initial stages
Memory and visuospatial skills impairments
Facial agnosia
DSM-5 Types of Major and Mild Neurocognitive Disorder
Due to Alzheimer’s Disease
Frontotemporal
Vascular
With
DSM-5 Types of Major and Mild Neurocognitive Disorder
Due to Alzheimer’s Disease
Frontotemporal
Vascular
With
Neurocognitive Disorder Due to Alzheimer’s Disease
Accounts for nearly half of neurocognitive
Neurocognitive Disorder Due to Alzheimer’s Disease
Accounts for nearly half of neurocognitive
Causes of Neurocognitive Disorder:
The Example of Alzheimer’s Disease, Continued
Multiple genes
Causes of Neurocognitive Disorder:
The Example of Alzheimer’s Disease, Continued
Multiple genes
Causes of Neurocognitive Disorder:
The Example of Alzheimer’s Disease, Part 3
Deterministic
Causes of Neurocognitive Disorder:
The Example of Alzheimer’s Disease, Part 3
Deterministic
PET Scans of Alzheimer’s Vs. Normal Brain
PET Scans of Alzheimer’s Vs. Normal Brain
Causes of Neurocognitive Disorder:
The Example of Alzheimer’s Disease
Features of brains
Causes of Neurocognitive Disorder:
The Example of Alzheimer’s Disease
Features of brains
Alzheimer’s Disorder: Extent of Deficits
Range of cognitive deficits
Aphasia – difficulty with
Alzheimer’s Disorder: Extent of Deficits
Range of cognitive deficits
Aphasia – difficulty with
Neurocognitive Disorder Due to Alzheimer’s Disease : Statistics
Early and later stages
Neurocognitive Disorder Due to Alzheimer’s Disease : Statistics
Early and later stages
Lisa Genova: Cognitive reserve
Cognitive reserve also indicates a resilience to neuropathological damage,
Lisa Genova: Cognitive reserve
Cognitive reserve also indicates a resilience to neuropathological damage,
Neurocognitive Disorder Due to Alzheimer’s Disease : Prevalence
Prevalence
More common in less
Neurocognitive Disorder Due to Alzheimer’s Disease : Prevalence
Prevalence
More common in less
![Graph of Predicted Alzheimer’s Incidence [INSERT Figure 15.1 HERE, p. 548]](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/247232/slide-26.jpg)
Graph of Predicted Alzheimer’s Incidence
[INSERT Figure 15.1 HERE, p. 548]
Graph of Predicted Alzheimer’s Incidence
[INSERT Figure 15.1 HERE, p. 548]
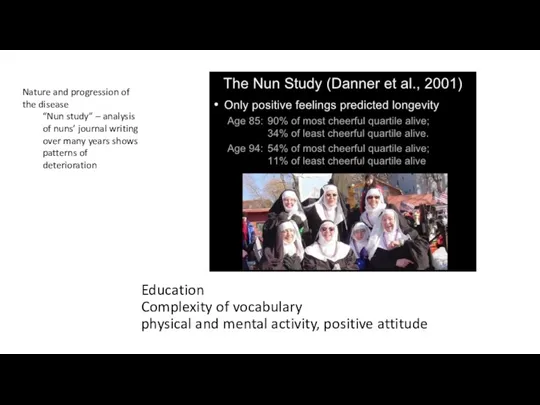
Education
Complexity of vocabulary
physical and mental activity, positive attitude
Nature and progression of
Education
Complexity of vocabulary
physical and mental activity, positive attitude
Nature and progression of
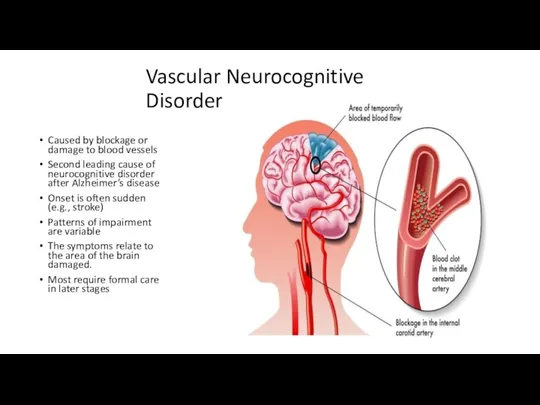
Vascular Neurocognitive Disorder
Caused by blockage or damage to blood vessels
Second leading
Vascular Neurocognitive Disorder
Caused by blockage or damage to blood vessels
Second leading
Vascular Neurocognitive Disorder: Features
Features
Cognitive disturbances – identical to dementia
Obvious neurological signs
Vascular Neurocognitive Disorder: Features
Features
Cognitive disturbances – identical to dementia
Obvious neurological signs
Vascular Neurocognitive Disorder
Caused by blockage or damage to blood vessels
Second leading
Vascular Neurocognitive Disorder
Caused by blockage or damage to blood vessels
Second leading
Prevention of Neurocognitive Disorders
Reducing risk in older adults
Use of anti-inflammatory medications
Control
Prevention of Neurocognitive Disorders
Reducing risk in older adults
Use of anti-inflammatory medications
Control
Neurocognitive Disorder Due to Lewy Body Disease
Lewy bodies = microscopic protein
Neurocognitive Disorder Due to Lewy Body Disease
Lewy bodies = microscopic protein
Neurocognitive Disorder Due to Parkinson’s Disase
Parkinson’s disease
Degenerative brain disorder
Dopamine pathway
Neurocognitive Disorder Due to Parkinson’s Disase
Parkinson’s disease
Degenerative brain disorder
Dopamine pathway
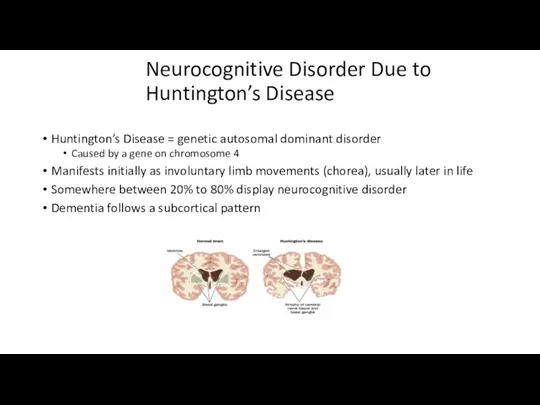
Neurocognitive Disorder Due to Huntington’s Disease
Huntington’s Disease = genetic autosomal
Neurocognitive Disorder Due to Huntington’s Disease
Huntington’s Disease = genetic autosomal
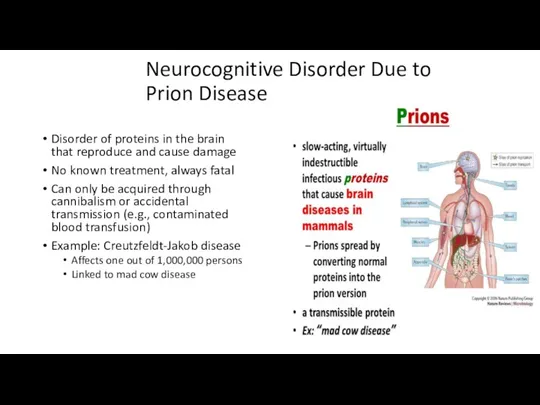
Neurocognitive Disorder Due to Prion Disease
Disorder of proteins in the
Neurocognitive Disorder Due to Prion Disease
Disorder of proteins in the
Summary of Neurocognitive Disorders
Cognitive disorders span a range of deficits
Affect attention,
Summary of Neurocognitive Disorders
Cognitive disorders span a range of deficits
Affect attention,
 Самай төменгі жақ буыны ауруларының ортопедиялық емі
Самай төменгі жақ буыны ауруларының ортопедиялық емі Клеточный, гуморальный иммунитет и их роль в защите от инфекций
Клеточный, гуморальный иммунитет и их роль в защите от инфекций Ойлау және интеллект бұзылыстарының клиникалық мініздемесі
Ойлау және интеллект бұзылыстарының клиникалық мініздемесі Препараты опухолей
Препараты опухолей Основные принципы терапии ДВС-синдрома
Основные принципы терапии ДВС-синдрома Костномозговое кроветворение. Нормы крови. Схема кроветворения
Костномозговое кроветворение. Нормы крови. Схема кроветворения Дифференциальная диагностика заболеваний с синдромом экзантемы
Дифференциальная диагностика заболеваний с синдромом экзантемы Основы здорового образа жизни: правильное питание
Основы здорового образа жизни: правильное питание Російські лікарі-філософи ХІХ століття
Російські лікарі-філософи ХІХ століття Иерсиниоз ауруы
Иерсиниоз ауруы Особенности капсульной эндоскопии
Особенности капсульной эндоскопии ХСН: причины, классификация, консервативное лечение
ХСН: причины, классификация, консервативное лечение Первая помощь при переломах, вывихах, ушибах
Первая помощь при переломах, вывихах, ушибах Высокотехнологичная медицинская помощь
Высокотехнологичная медицинская помощь Одонтогенді гайморит клиникасы, диагностикасы, диагнозы және емдеу принциптері
Одонтогенді гайморит клиникасы, диагностикасы, диагнозы және емдеу принциптері Алгоритм обследования бесплодной пары
Алгоритм обследования бесплодной пары Разработка плана мероприятий по проведению первичной, вторичной, третичной профилактики заболеваний
Разработка плана мероприятий по проведению первичной, вторичной, третичной профилактики заболеваний Применение лекарственных средств, используемых в иммунологии у беременных, в период лактации
Применение лекарственных средств, используемых в иммунологии у беременных, в период лактации Жүрек созылмалы жетіспеушілігі
Жүрек созылмалы жетіспеушілігі Жатыр мойны адам папилломавирусының инфекциясы
Жатыр мойны адам папилломавирусының инфекциясы Компенсаторно - приспособительные процессы
Компенсаторно - приспособительные процессы Вакцинация
Вакцинация Лекарственные растения и лекарственное растительное сырье. Часть III. Слабительные и антидиарейные средства
Лекарственные растения и лекарственное растительное сырье. Часть III. Слабительные и антидиарейные средства Донорское движение РГУФКСМиТ
Донорское движение РГУФКСМиТ Геморрагический васкулит
Геморрагический васкулит Методы лечения рака предстательной железы
Методы лечения рака предстательной железы Кровь. Функции и состав крови. Группы крови
Кровь. Функции и состав крови. Группы крови ЭКГ при электролитных нарушениях в организме
ЭКГ при электролитных нарушениях в организме