- Peptic Ulcer Disease Complications

Содержание
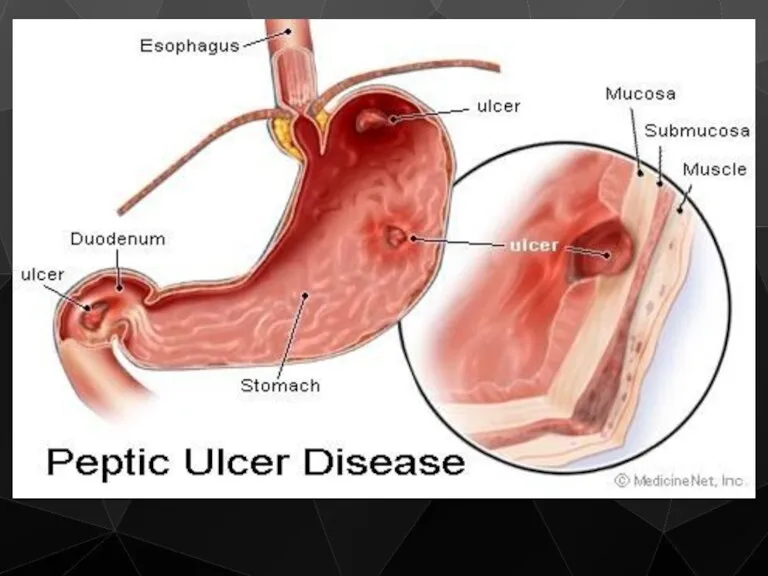
- 2. A peptic ulcer is an open sore in the upper digestive tract. There are two types
- 4. Classification Stomach (called gastric ulcer) Duodenum (called duodenal ulcer) Oesophagus (called Oesophageal ulcer) Types of peptic
- 5. SYMPTOMS
- 7. CAUSES
- 8. Helicobacter pylori, a bacteria that is frequently found in the stomach Nonsteroidal anti-inflammatory drugs (NSAIDS) such
- 9. Helicobacter pylori infection H. pylori is a helix-shaped Gram-negative, slow-growing organism
- 10. The bacterium persists in the stomach for decades in most people. Most individuals infected by H.
- 11. Effects of smoking on PUD Increased rate of gastric emptying Diminished pancreatic bicarbonate secretion Decreased duodenal
- 12. NICOTINE parasympathetic nerve activity in gastrointestinal tract INCREASE stimulation to the enterochromaffin-like cells and G cells
- 13. Gastrinomas (Zollinger Ellison syndrome), rare gastrin-secreting tumors, also cause multiple and difficult to heal ulcers. Excessive
- 14. Caffeine Beverages and foods that contain caffeine can stimulate acid secretion in the stomach. This can
- 15. The complications of Peptic Ulceration The common complications are: Perforation Penetration Bleeding Stenosis
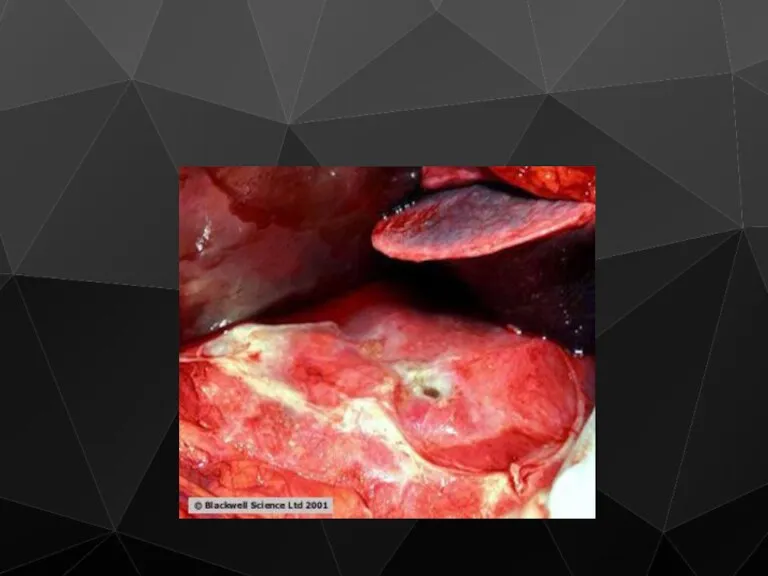
- 16. Perforation (a hole in the wall) often leads to catastrophic consequences. Erosion of the gastro-intestinal wall
- 17. Perforation Clinical Features History of peptic ulcer Sudden onset, severe, generalized abdominal pain Starts as chemical
- 18. Perforation Clinical symptoms Tachycardia, pyrexia Shock Board like rigidity of abdomen Abdominal splinting
- 19. Perforation Clinical Features In elderly, the classical presentation of PPU may be absent Use of NSAID
- 20. Perforation Clinical Features The most frequent place for perforation is the anterior wall of duodenum Anterior
- 21. Perforation Investigations Observe chest X-ray will reveal free gas under the diaphragm in more than 50%
- 22. On X-ray is crescent-shaped illumination under the diaphragm
- 23. Perforation Treatment Hospitalisation and analgesia The treatment is principally surgical Midline laparotomy Thorough peritoneal toilet Duodenal
- 26. Suturing of Perforated Peptic Ulcer
- 27. Graham Omental Patching
- 28. Excision of ulcer with pyloroplasty by JADD
- 29. Perforation Treatment Systemic antibiotics Vagotomy, highly selective vagotomy Minimally invasive Conservative treatment - Small leak -
- 30. Gastrointestinal bleeding is the most common complication. Sudden large bleeding can be life-threatening. It occurs when
- 31. Penetration is when the ulcer continues into adjacent organs such as the liver and pancreas
- 32. Penetration is a form of perforation in which the perforating ulcers erode the whole thickness of
- 33. Bleeding Epidemiology Mirror that of PPU NSAID
- 34. Bleeding
- 35. Classification of bleeding according to J. Forrest (1974)
- 36. Bleeding Treatment / Medical Limited efficacy All patients are started on PPI (omeprasole) Endoscopic control -
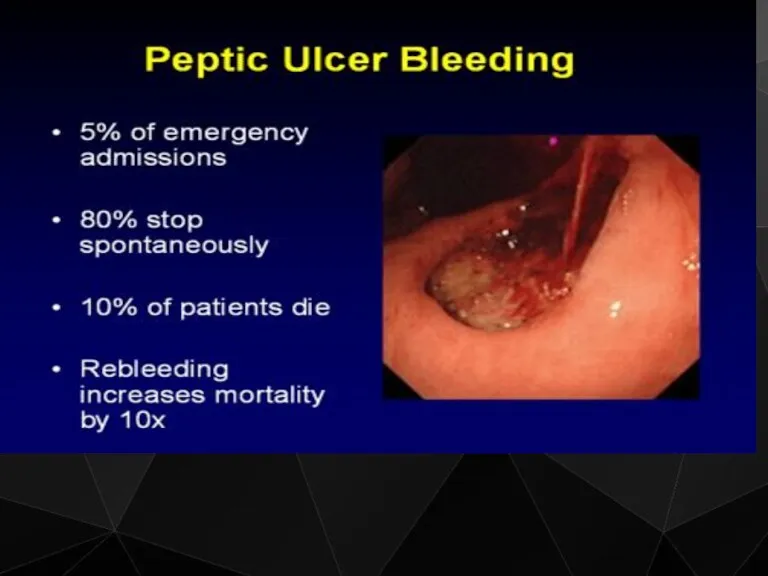
- 37. Bleeding Peptic Ulcer
- 39. Bleeding Treatment / Surgical Indications Patient continue to bleed Visible vessel in ulcer base Spurting vessel
- 40. Bleeding Treatment / Surgical Aim to stop bleeding Upper midline incision Site usually localized by prior
- 41. Bleeding Treatment / Surgical Definitive acid lowering surgery is not required PPI (omeprasole) Anti H pylori
- 42. Stenosis Stenosis is usually found in the 1st part of duodenum This condition occurs less and
- 43. Scar tissue Scarring and swelling due to ulcers causes narrowing in the duodenum and gastric outlet
- 45. Stenosis Clinical Features Long history of peptic ulcer disease Vomiting, unpleasant in nature, totally lacking in
- 46. X-ray of Pyloric Stenosis
- 47. Stenosis Metabolic effects Vomiting of HCl results in hypochloremic acidosis Initially Na+ & K+ levels are
- 48. Stenosis Metabolic effects Then because of dehydration, a phase of Na+ retention follows and K+ and
- 49. Stenosis Management 1) Correct metabolic abnormality Rehydration with isotonic saline with K + supplementation Replacing NaCl
- 50. Stenosis Management 2) Empty the stomach with wide-bore N/G tube, may need lavage 3) Endoscopy and
- 51. Stenosis Management Early cases may settle with conservative measurement, presumably as the edema around the ulcer
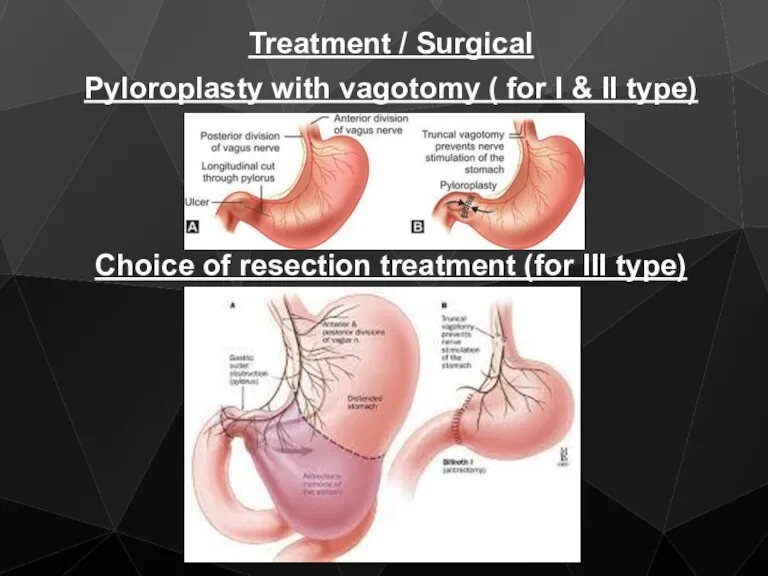
- 52. Treatment / Surgical Pyloroplasty with vagotomy ( for I & II type) Choice of resection treatment
- 54. Скачать презентацию
A peptic ulcer is an open sore in the upper digestive
A peptic ulcer is an open sore in the upper digestive
Classification
Stomach (called gastric ulcer)
Duodenum (called duodenal ulcer)
Oesophagus (called Oesophageal ulcer)
Types of
Classification
Stomach (called gastric ulcer)
Duodenum (called duodenal ulcer)
Oesophagus (called Oesophageal ulcer)
Types of
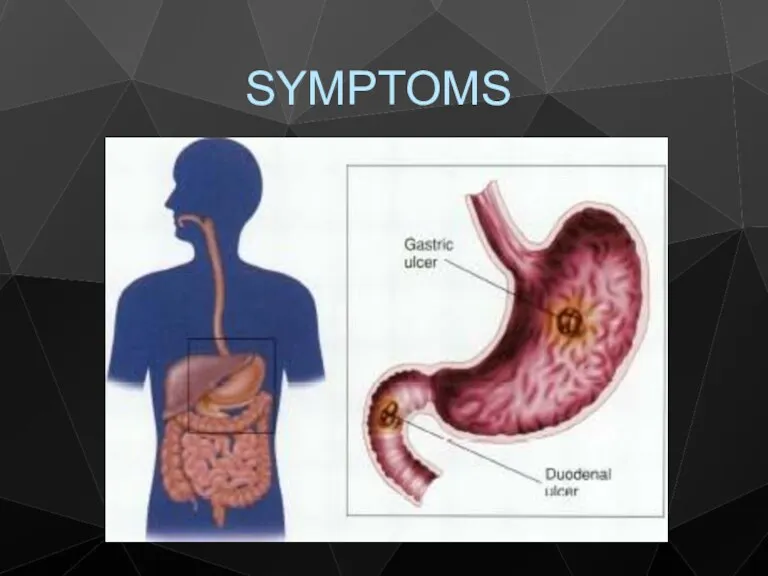
SYMPTOMS
SYMPTOMS

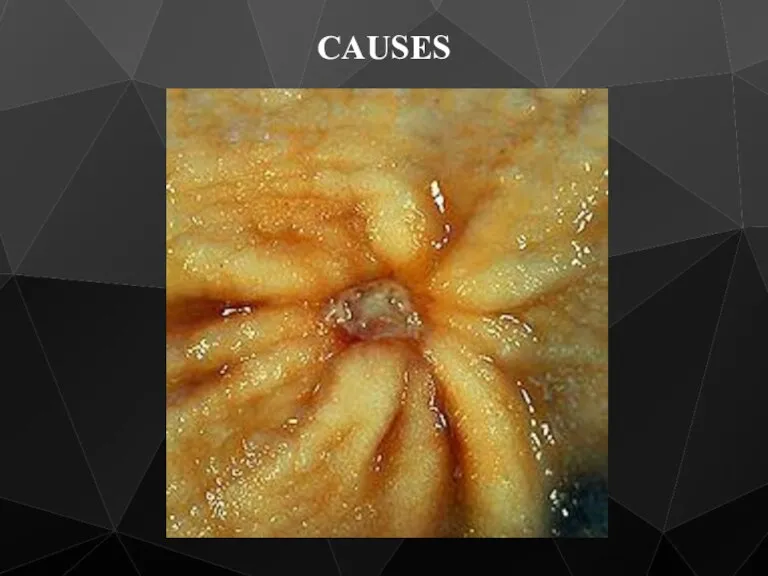
CAUSES
CAUSES
Helicobacter pylori, a bacteria that is frequently found in the stomach
Helicobacter pylori, a bacteria that is frequently found in the stomach
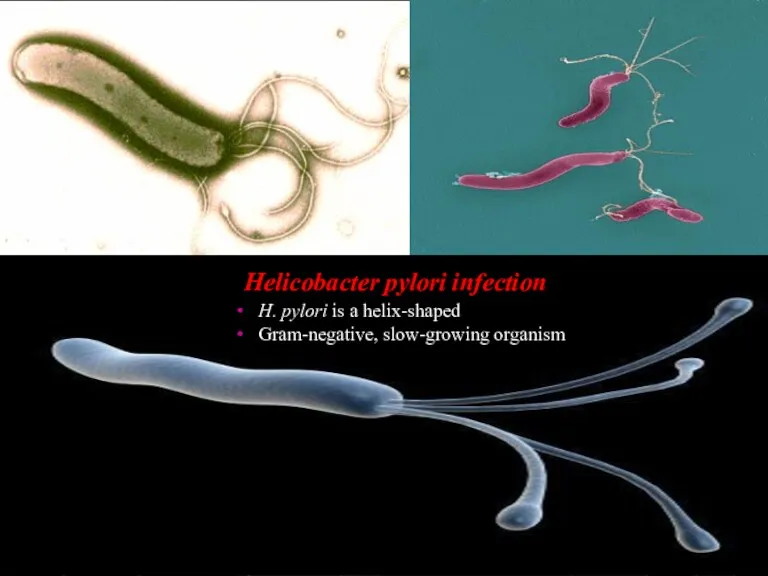
Helicobacter pylori infection
H. pylori is a helix-shaped
Gram-negative, slow-growing organism
Helicobacter pylori infection
H. pylori is a helix-shaped
Gram-negative, slow-growing organism
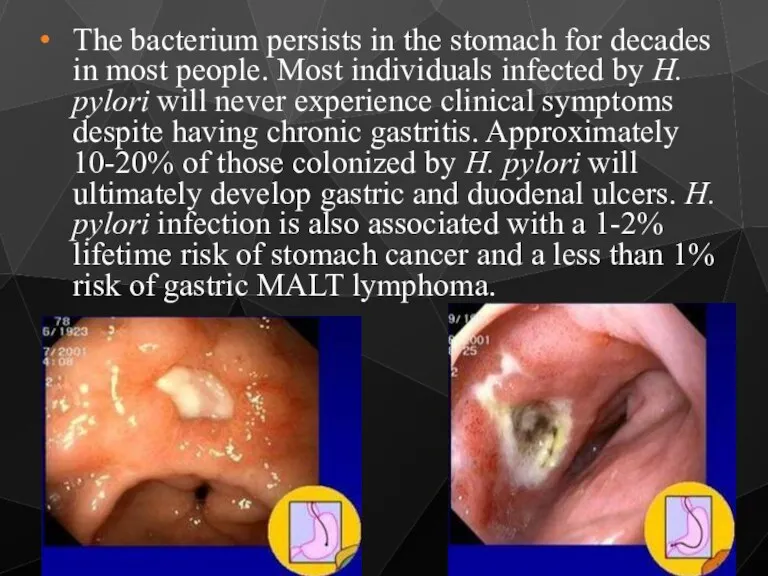
The bacterium persists in the stomach for decades in most people.
The bacterium persists in the stomach for decades in most people.
Effects of smoking on PUD
Increased rate of gastric emptying
Diminished
Effects of smoking on PUD
Increased rate of gastric emptying
Diminished
NICOTINE
parasympathetic nerve
activity in
gastrointestinal tract
INCREASE
stimulation to
the enterochromaffin-like cells
NICOTINE
parasympathetic nerve
activity in
gastrointestinal tract
INCREASE
stimulation to
the enterochromaffin-like cells
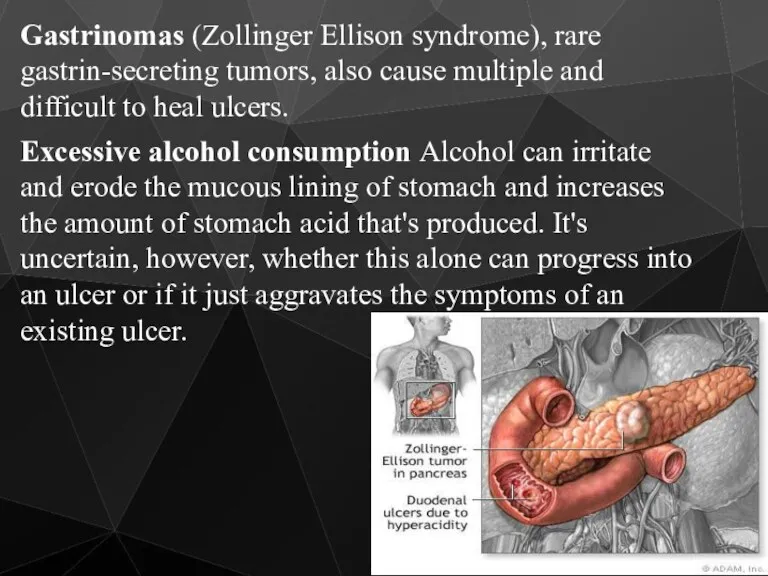
Gastrinomas (Zollinger Ellison syndrome), rare gastrin-secreting tumors, also cause multiple and
Gastrinomas (Zollinger Ellison syndrome), rare gastrin-secreting tumors, also cause multiple and
Caffeine
Beverages and foods that contain caffeine can stimulate acid secretion in
Caffeine
Beverages and foods that contain caffeine can stimulate acid secretion in
The complications of Peptic Ulceration
The common complications are:
Perforation
Penetration
Bleeding
Stenosis
The complications of Peptic Ulceration
The common complications are:
Perforation
Penetration
Bleeding
Stenosis
Perforation (a hole in the wall) often leads to catastrophic consequences.
Perforation (a hole in the wall) often leads to catastrophic consequences.
Perforation
Clinical Features
History of peptic ulcer
Sudden onset, severe, generalized abdominal pain
Starts as
Perforation
Clinical Features
History of peptic ulcer
Sudden onset, severe, generalized abdominal pain
Starts as
Perforation
Clinical symptoms
Tachycardia, pyrexia
Shock
Board like rigidity of abdomen
Abdominal splinting
Perforation
Clinical symptoms
Tachycardia, pyrexia
Shock
Board like rigidity of abdomen
Abdominal splinting
Perforation
Clinical Features
In elderly, the classical presentation of PPU may be absent
Use
Perforation
Clinical Features
In elderly, the classical presentation of PPU may be absent
Use
Perforation
Clinical Features
The most frequent place for perforation is the anterior wall
Perforation
Clinical Features
The most frequent place for perforation is the anterior wall
Perforation
Investigations
Observe chest X-ray will reveal free gas under the diaphragm in
Perforation
Investigations
Observe chest X-ray will reveal free gas under the diaphragm in
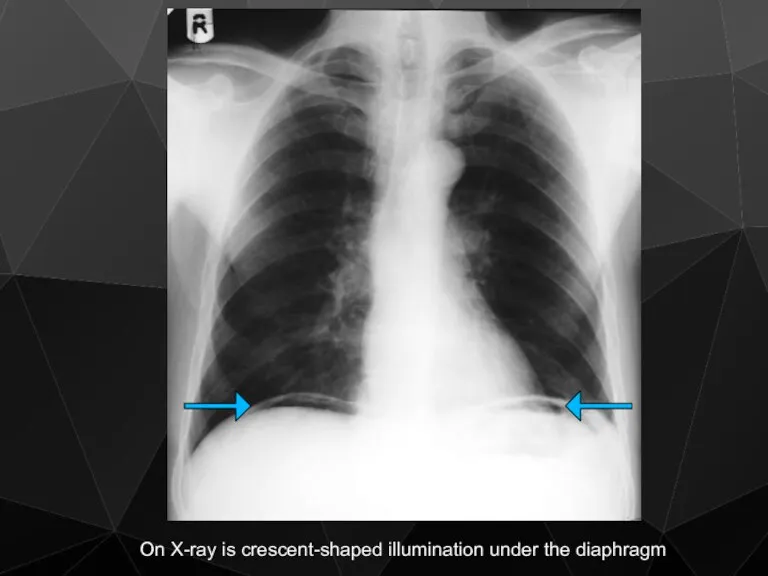
On X-ray is crescent-shaped illumination under the diaphragm
On X-ray is crescent-shaped illumination under the diaphragm
Perforation
Treatment
Hospitalisation and analgesia
The treatment is principally surgical
Midline laparotomy
Thorough peritoneal toilet
Duodenal
Perforation
Treatment
Hospitalisation and analgesia
The treatment is principally surgical
Midline laparotomy
Thorough peritoneal toilet
Duodenal

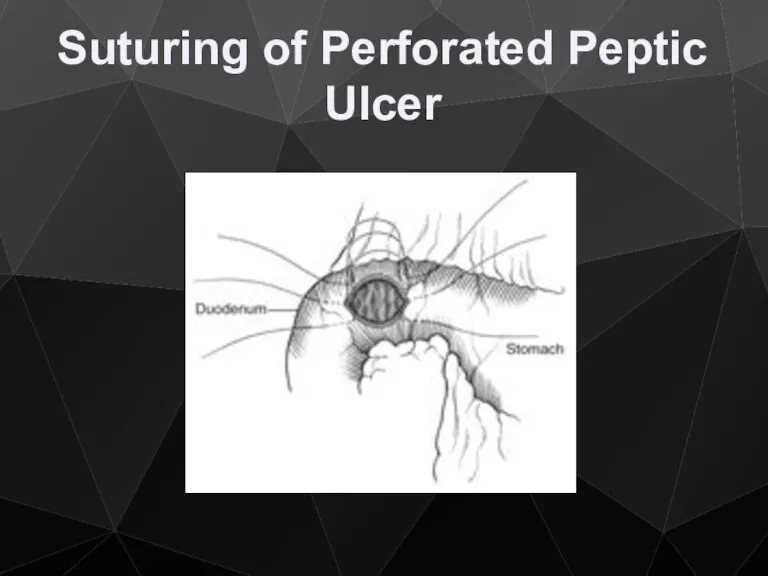
Suturing of Perforated Peptic Ulcer
Suturing of Perforated Peptic Ulcer
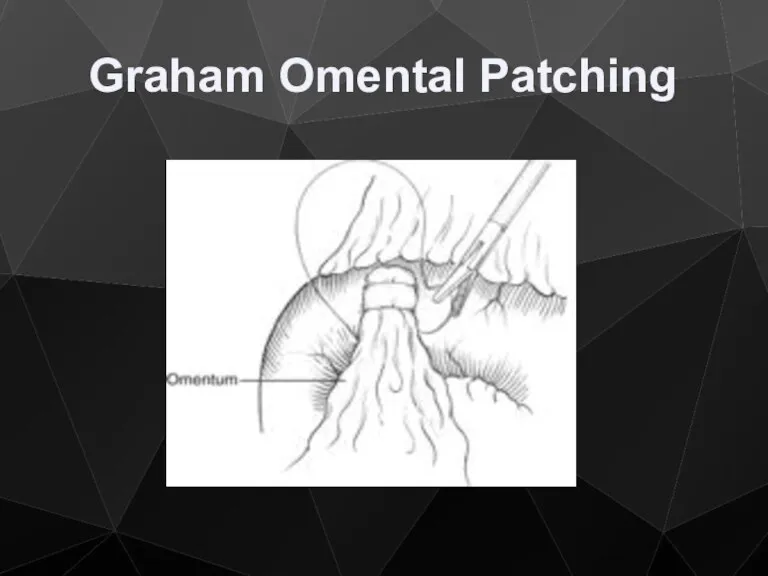
Graham Omental Patching
Graham Omental Patching
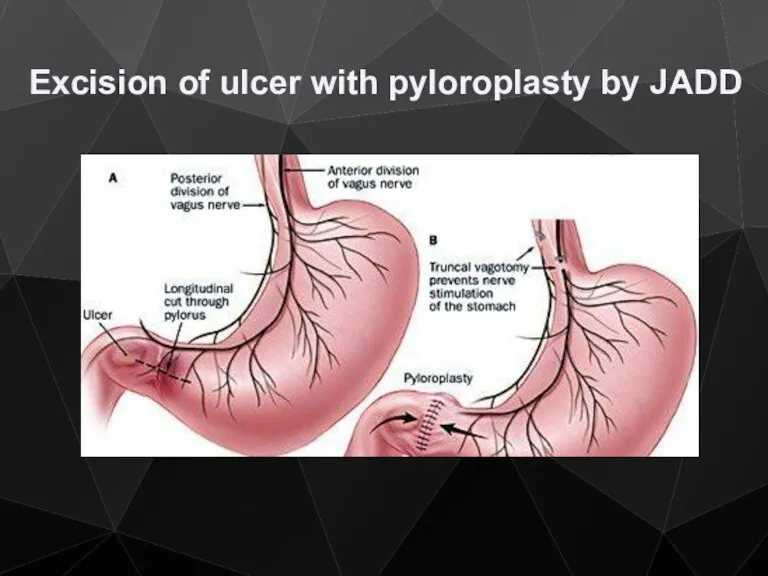
Excision of ulcer with pyloroplasty by JADD
Excision of ulcer with pyloroplasty by JADD
Perforation
Treatment
Systemic antibiotics
Vagotomy, highly selective vagotomy
Minimally invasive
Conservative treatment
- Small leak
-
Perforation
Treatment
Systemic antibiotics
Vagotomy, highly selective vagotomy
Minimally invasive
Conservative treatment
- Small leak
-
Gastrointestinal bleeding is the most common complication. Sudden large bleeding can
Gastrointestinal bleeding is the most common complication. Sudden large bleeding can
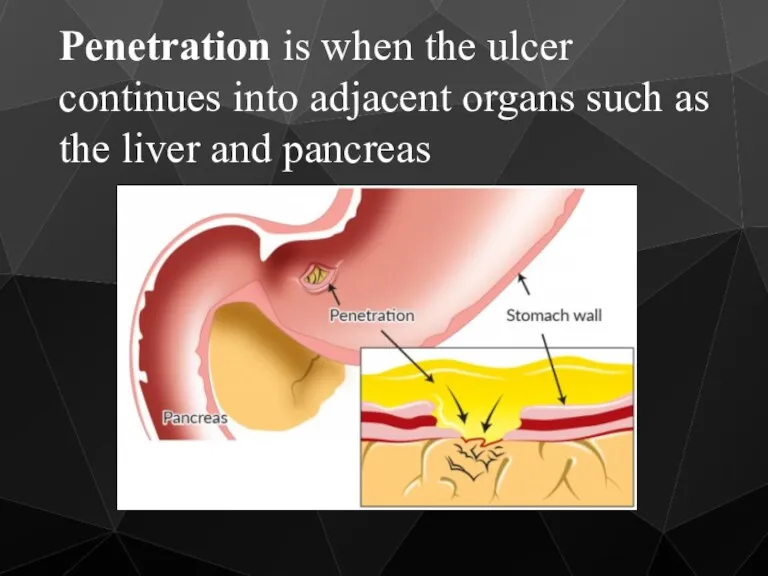
Penetration is when the ulcer continues into adjacent organs such as
Penetration is when the ulcer continues into adjacent organs such as
Penetration is a form of perforation in which the perforating ulcers
Penetration is a form of perforation in which the perforating ulcers
Bleeding
Epidemiology
Mirror that of PPU
NSAID
Bleeding
Epidemiology
Mirror that of PPU
NSAID
Bleeding
Bleeding
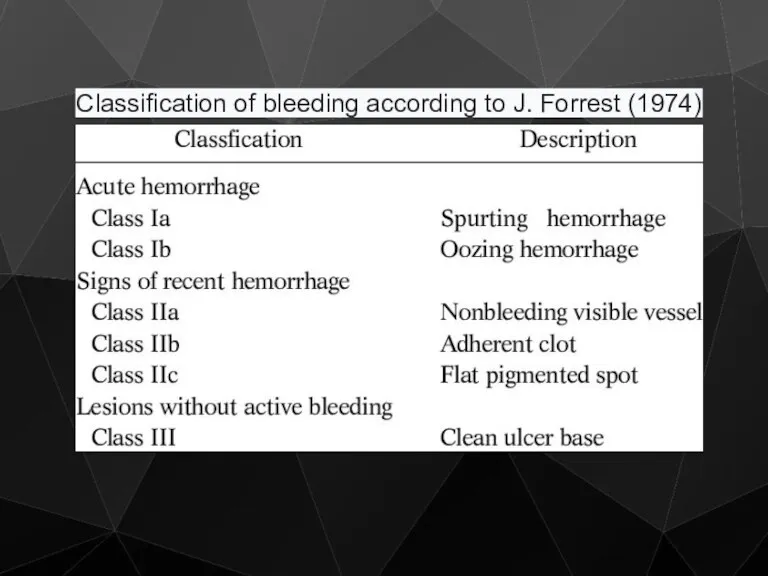
Classification of bleeding according to J. Forrest (1974)
Classification of bleeding according to J. Forrest (1974)
Bleeding
Treatment / Medical
Limited efficacy
All patients are started on PPI (omeprasole)
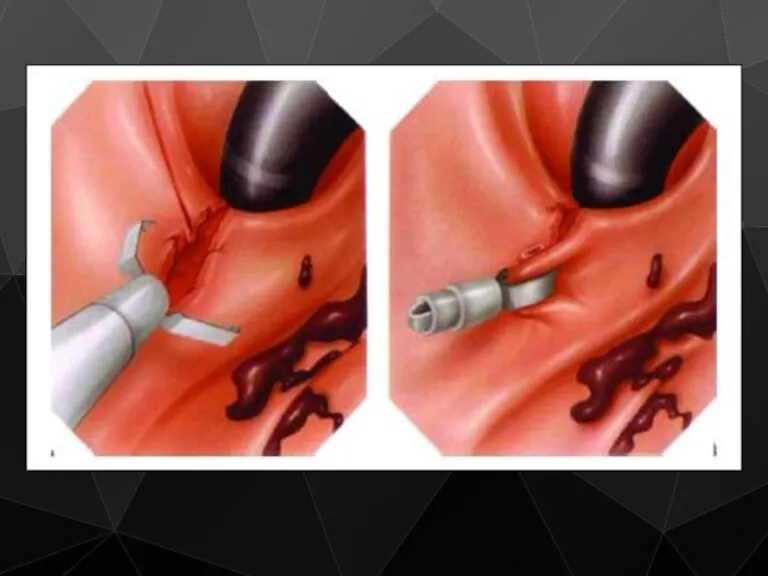
Endoscopic control
Bleeding
Treatment / Medical
Limited efficacy
All patients are started on PPI (omeprasole)
Endoscopic control
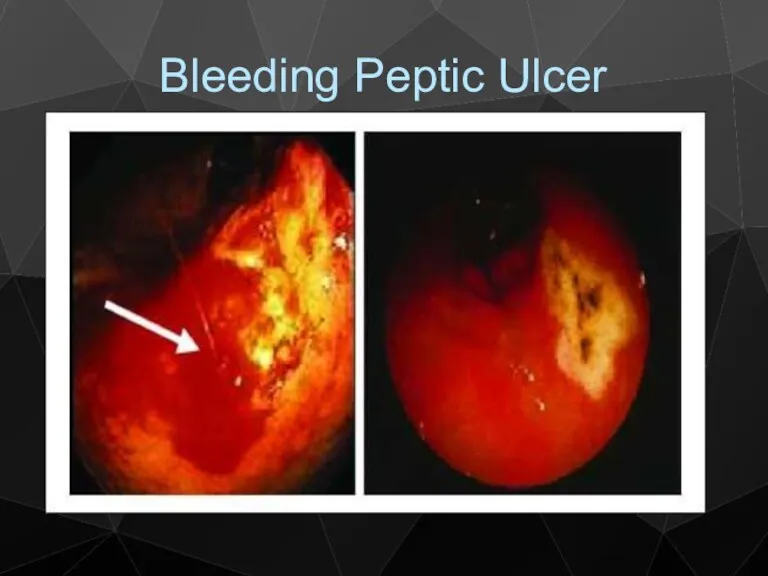
Bleeding Peptic Ulcer
Bleeding Peptic Ulcer
Bleeding
Treatment / Surgical
Indications
Patient continue to bleed
Visible vessel in ulcer base
Spurting
Bleeding
Treatment / Surgical
Indications
Patient continue to bleed
Visible vessel in ulcer base
Spurting
Bleeding
Treatment / Surgical
Aim to stop bleeding
Upper midline incision
Site usually localized
Bleeding
Treatment / Surgical
Aim to stop bleeding
Upper midline incision
Site usually localized
Bleeding
Treatment / Surgical
Definitive acid lowering surgery is not required
PPI (omeprasole)
Anti
Bleeding
Treatment / Surgical
Definitive acid lowering surgery is not required
PPI (omeprasole)
Anti
Stenosis
Stenosis is usually found in the 1st part of duodenum
This condition
Stenosis
Stenosis is usually found in the 1st part of duodenum
This condition
Scar tissue Scarring and swelling due to ulcers causes narrowing in
Scar tissue Scarring and swelling due to ulcers causes narrowing in

Stenosis
Clinical Features
Long history of peptic ulcer disease
Vomiting, unpleasant in nature, totally
Stenosis
Clinical Features
Long history of peptic ulcer disease
Vomiting, unpleasant in nature, totally
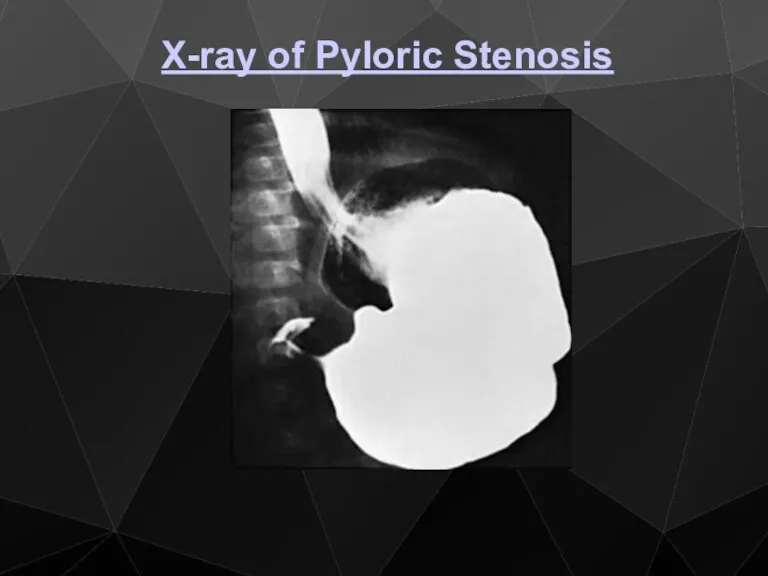
X-ray of Pyloric Stenosis
X-ray of Pyloric Stenosis
Stenosis
Metabolic effects
Vomiting of HCl results in hypochloremic acidosis
Initially Na+ & K+
Stenosis
Metabolic effects
Vomiting of HCl results in hypochloremic acidosis
Initially Na+ & K+
Stenosis
Metabolic effects
Then because of dehydration, a phase of Na+ retention follows
Stenosis
Metabolic effects
Then because of dehydration, a phase of Na+ retention follows
Stenosis
Management
1) Correct metabolic abnormality
Rehydration with isotonic saline with K + supplementation
Replacing
Stenosis
Management
1) Correct metabolic abnormality
Rehydration with isotonic saline with K + supplementation
Replacing
Stenosis
Management
2) Empty the stomach with wide-bore N/G tube, may need lavage
3)
Stenosis
Management
2) Empty the stomach with wide-bore N/G tube, may need lavage
3)
Stenosis
Management
Early cases may settle with conservative measurement, presumably as the edema
Stenosis
Management
Early cases may settle with conservative measurement, presumably as the edema
Treatment / Surgical
Pyloroplasty with vagotomy ( for I & II
Treatment / Surgical
Pyloroplasty with vagotomy ( for I & II
 Hygiene of work
Hygiene of work Общественное здоровье и организация здравоохранения как наука и предмет преподавания
Общественное здоровье и организация здравоохранения как наука и предмет преподавания Сенсорные нарушения, их коррекция и реабилитация (речевые, зрительные и другие)
Сенсорные нарушения, их коррекция и реабилитация (речевые, зрительные и другие) Антибактериальные химиотерапевтические средства. Антибиотики разных групп
Антибактериальные химиотерапевтические средства. Антибиотики разных групп Правила клинического использования донорской крови и (или) ее компонентов
Правила клинического использования донорской крови и (или) ее компонентов Менингококковая инфекция
Менингококковая инфекция Мукополисахаридоз
Мукополисахаридоз Диагностика беременности. Методы акушерского исследования (урок 3)
Диагностика беременности. Методы акушерского исследования (урок 3) Митральді клапанның минимальді-инвазивті оң жақтық торактомия өткізілген хирургияның ерте және ұзақ мерзімді
Митральді клапанның минимальді-инвазивті оң жақтық торактомия өткізілген хирургияның ерте және ұзақ мерзімді Клизмы. Классификация клизм как процедур
Клизмы. Классификация клизм как процедур Организация работы в специализированных бригадах скорой помощи
Организация работы в специализированных бригадах скорой помощи Механизмы отторжения трапсплантата на примере трансплантации сердца
Механизмы отторжения трапсплантата на примере трансплантации сердца Анатомия и физиология как медицинские науки. Человек как предмет изучения анатомии и физиологии. Лекция № 1
Анатомия и физиология как медицинские науки. Человек как предмет изучения анатомии и физиологии. Лекция № 1 Основные принципы местной анестезии в стоматологии. Оперативная хирургия и топографическая анатомия ЧЛО
Основные принципы местной анестезии в стоматологии. Оперативная хирургия и топографическая анатомия ЧЛО Производственная практика 2018-2019
Производственная практика 2018-2019 Сосудистые заболевания нервной системы
Сосудистые заболевания нервной системы Медициналық клиникалық зерттеулердің дизайны
Медициналық клиникалық зерттеулердің дизайны Опухоли (новообразования)
Опухоли (новообразования) Методы лечения психофармакотерапии с позиции доказательной медицины
Методы лечения психофармакотерапии с позиции доказательной медицины Менингококковая инфекция
Менингококковая инфекция Микрохирургия. Планирование восстановительных операций
Микрохирургия. Планирование восстановительных операций Итальянский метод ринопластики
Итальянский метод ринопластики Инновационные методы лечения головной боли
Инновационные методы лечения головной боли Исследование мочи
Исследование мочи Функциональная анатомия лимфатической системы
Функциональная анатомия лимфатической системы GDP. Склад медикаментов
GDP. Склад медикаментов Световая микроскопия
Световая микроскопия Гипоплазия эмали
Гипоплазия эмали