- Pneumonia

Содержание
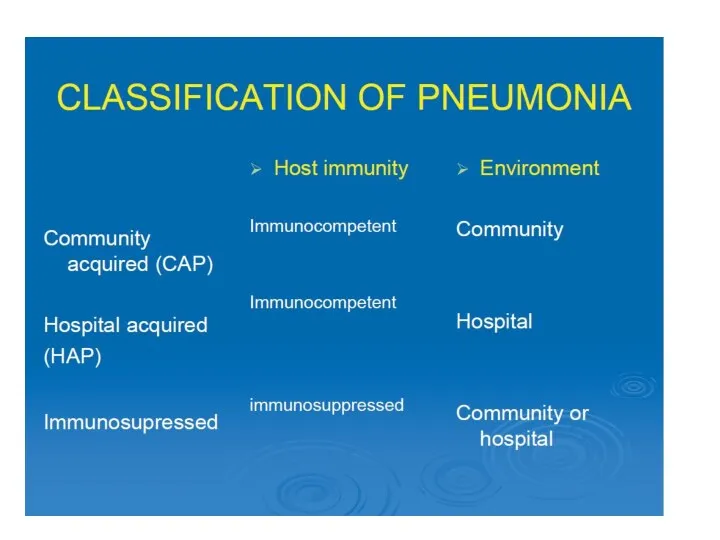
- 2. Definitions Ethiology (general), risk factors Diagnosis criteria and evaluation Peculiarities of the disease in different causative
- 3. Pneumonia: infection of the lung parenchyma, in which consolidation of the affected part and a filling
- 4. Ethiology (general) Bacterial – most common Viral Rickettsiae Fungi Yeasts Mycobacteria
- 5. Risk factors (general) Influenza (especially H1N1) local lung pathologies (tumors, COPD, bronchiectasis), smoking Chronic gingivitis and
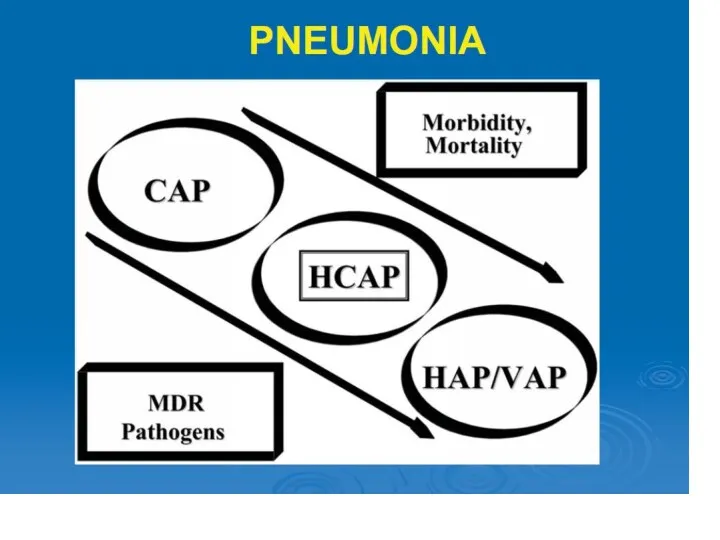
- 7. CAP: Pneumonia not acquired in a hospital or a long-term care facility Hospital acquired pneumonia (with/without
- 8. Epidemiology 5.6 million cases of CAP annually in the United States total annual cost for CAP
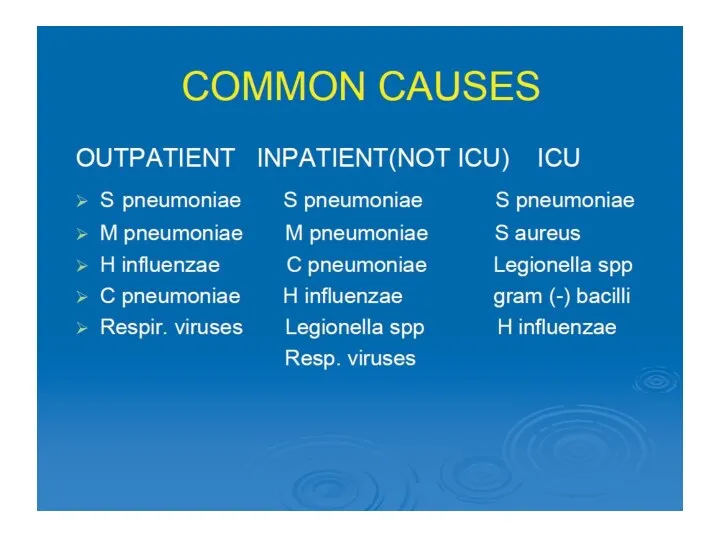
- 9. Ethiology Typical: up to 70% Usually caused by Streptococcus pneumoniae Atypical: 30-40% “My Lungs Contain Viruses”
- 12. Risk factors for some etiological factors Resistent S.pneumoniae >65 лет Beta-lactams during last 3 mo, chronic
- 13. Intoxication fever, chills, fatigue, dyspnea, headache and myalgia Cough may be persistent and dry, or it
- 14. CXR (PA and Lateral): American Thoracic Society (ATS) guidelines, “all patients with suspected CAP should have
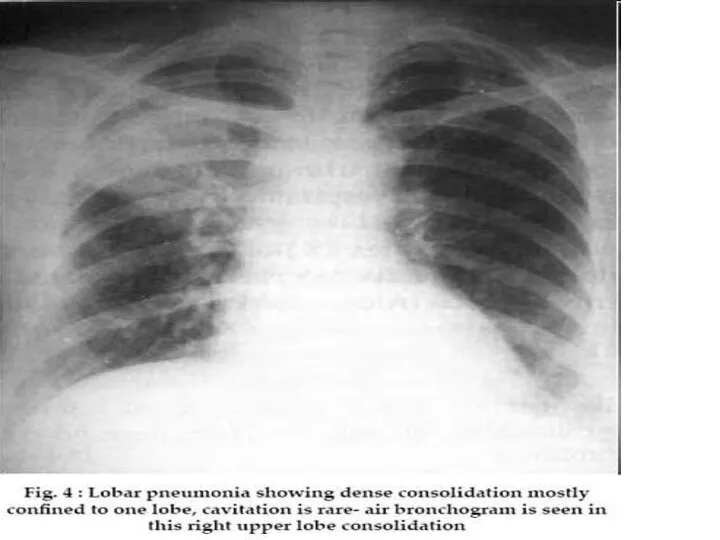
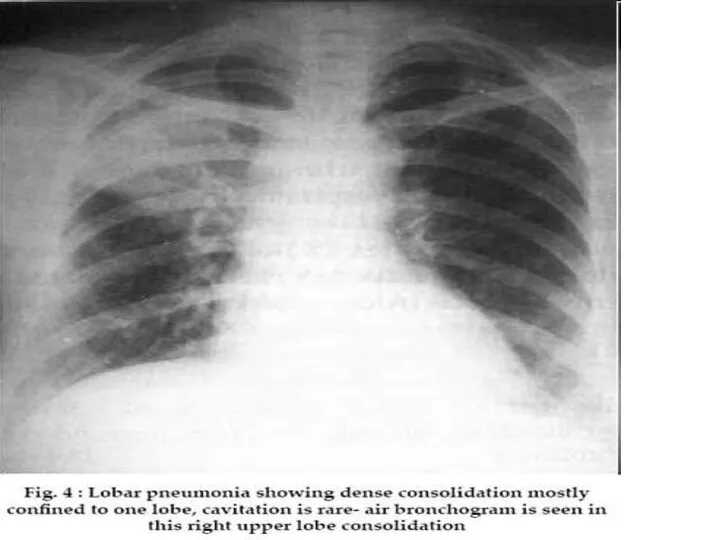
- 18. Lobar pneumonia (also known as a non-segmental pneumonia or focal non-segmental pneumonia 7) is a radiological
- 19. Other causative organisms Klebsiella pneumoniae Legionella pneumophila Haemophilus influenzae Mycobacterium tuberculosis
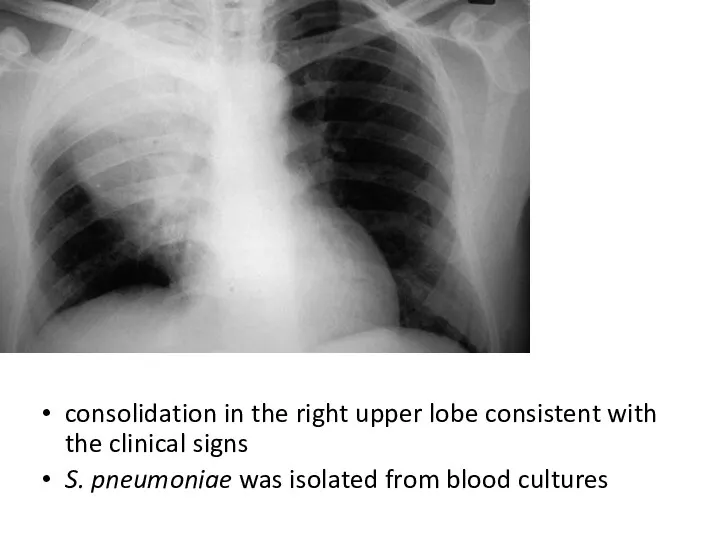
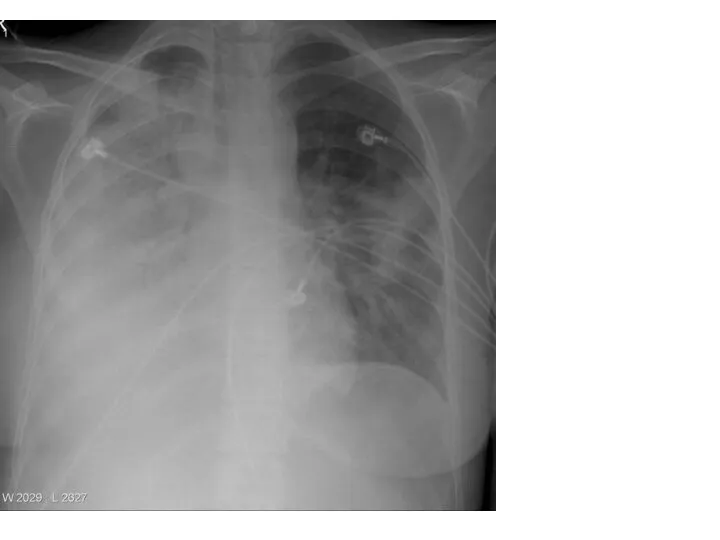
- 20. consolidation in the right upper lobe consistent with the clinical signs S. pneumoniae was isolated from
- 22. Middle lobe Str pneum
- 23. Right upper lobe
- 24. consolidation in the right upper lobe consistent with the clinical signs S. pneumoniae was isolated from
- 25. Coronal and saggital lungs windows
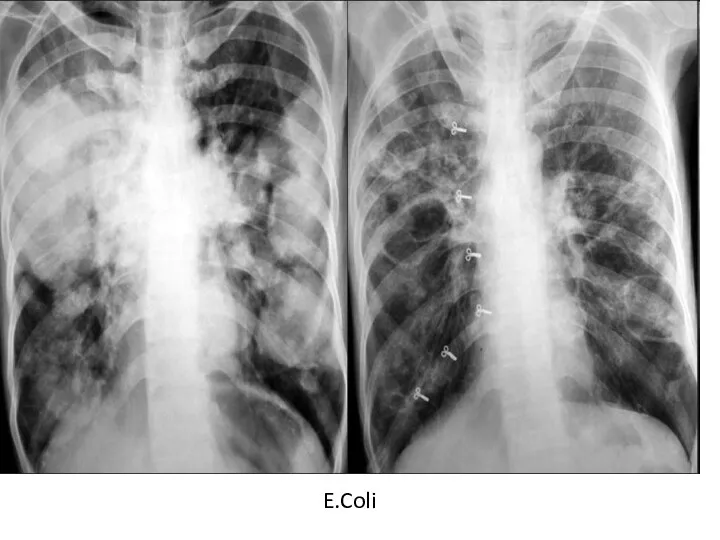
- 28. E.Coli
- 29. Pneumocystis pneumonia
- 31. E.Coli
- 34. Acute respiratory failure severity – necessity of non-invasive ventilation
- 59. Round pneumonia: usually seen in paediatric patients. They are well defined, rounded opacities that represent regions
- 62. Bronchopneumonia also sometimes known as lobular pneumonia radiological pattern associated with suppurative peribronchiolar inflammation and subsequent
- 63. Causative organisms of a bronchopneumonia pattern include 3: Staphylococcus aureus Klebsiella pneumoniae Haemophilus influenzae Pseudomonas aeruginosa
- 64. Radiology Plain film Bronchopneumonia is characterised by multiple small nodular or reticulonodular opacities which tend to
- 65. Staphyl pneum with empyema
- 66. Posteroanterior chest radiograph of a 15-year-old with staphylococcal endocarditis and multiple septic emboli, revealing borderline cardiomegaly,
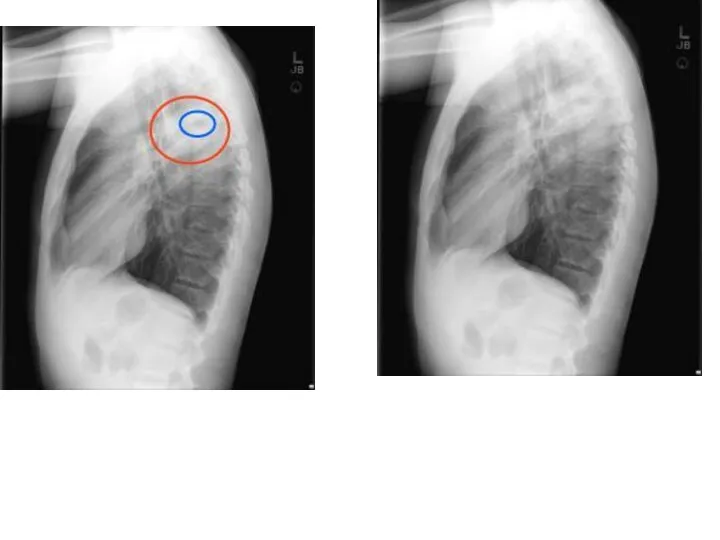
- 67. Lat/view
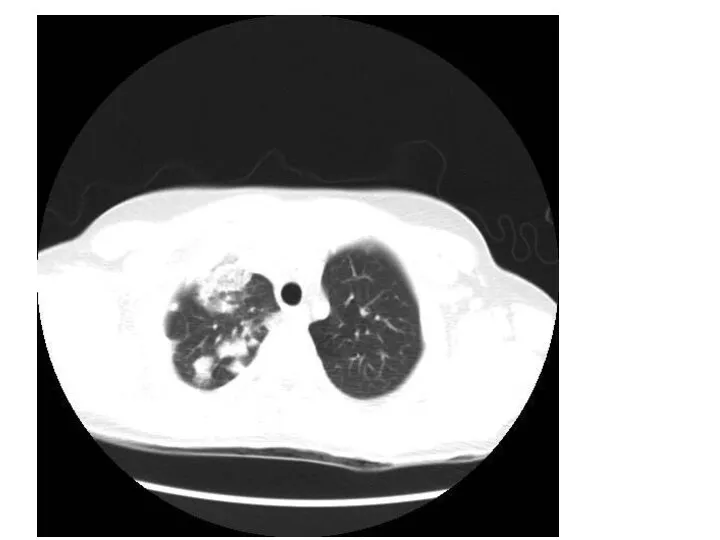
- 68. CT scan
- 69. Cont.
- 70. same
- 72. T scan of the thorax (mediastinal windows) .
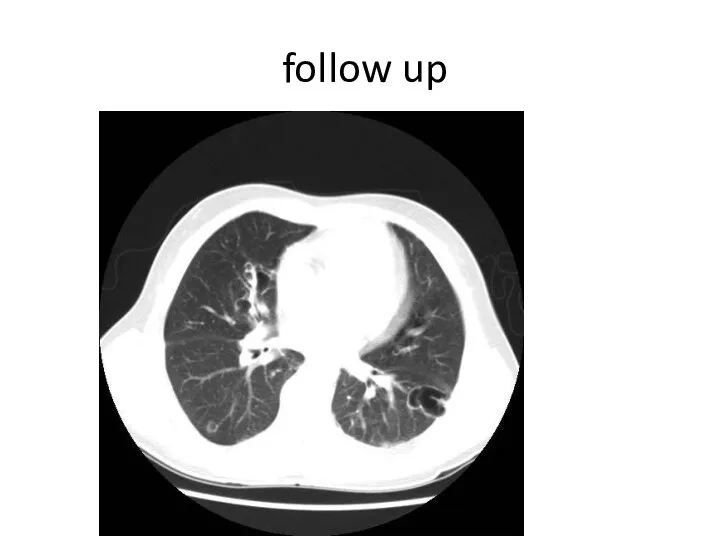
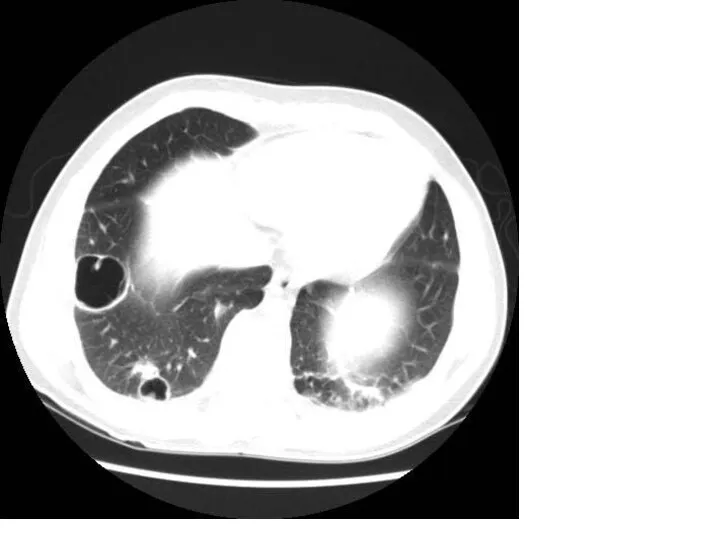
- 73. follow up
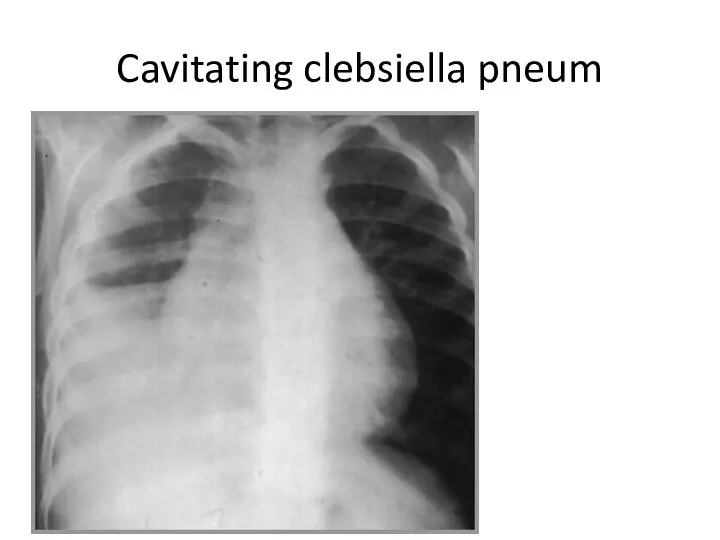
- 75. Cavitating clebsiella pneum
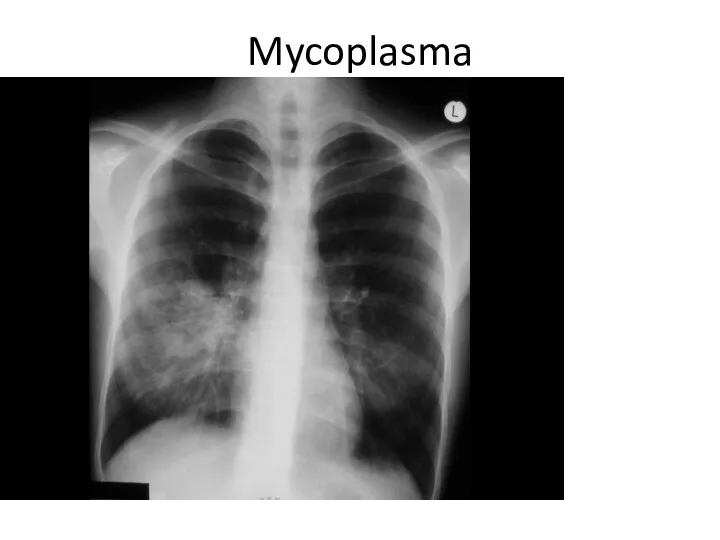
- 76. Mycoplasma
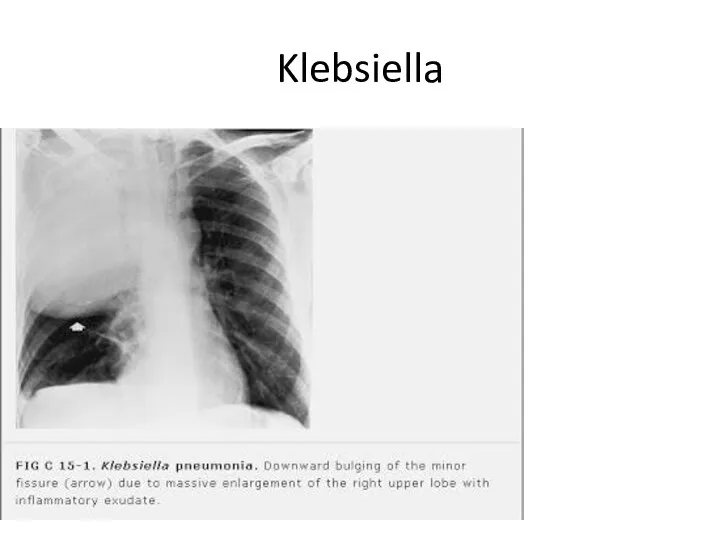
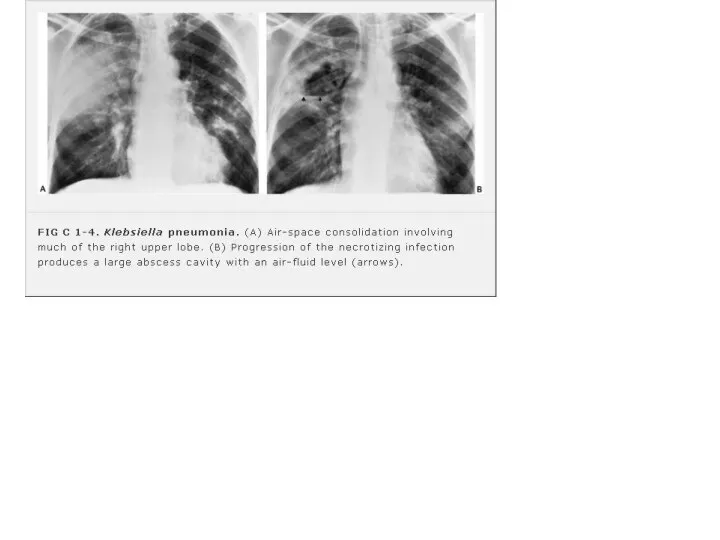
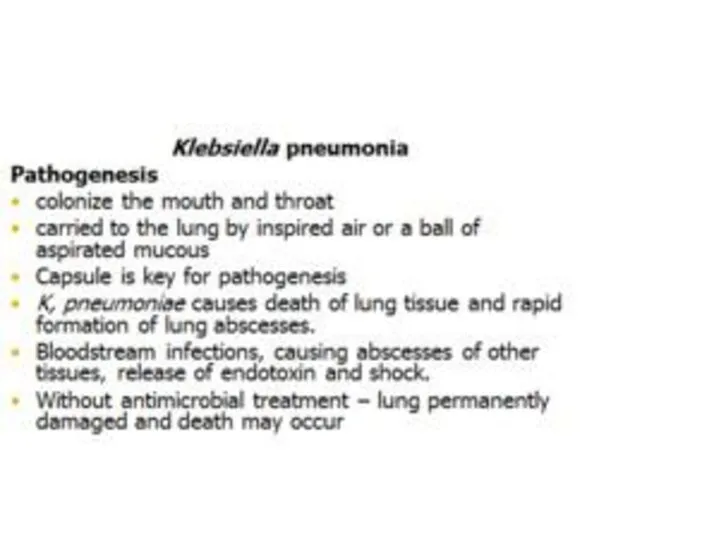
- 78. Klebsiella
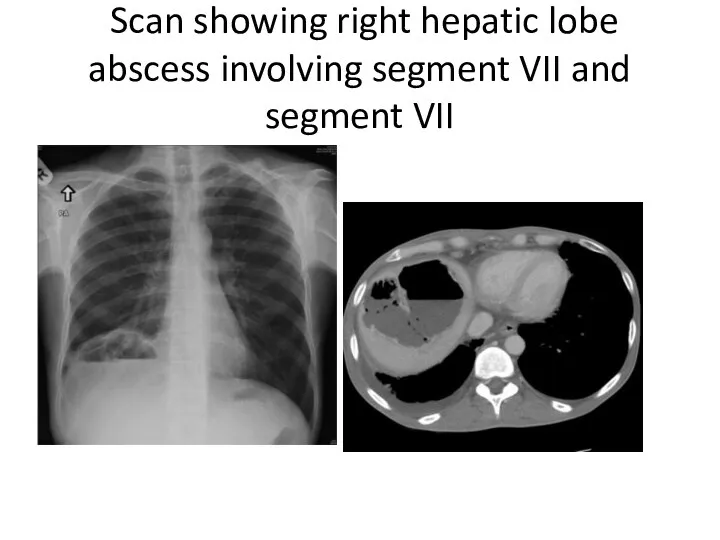
- 81. A 45 years old male with 5 years history of type 2 diabetes mellitus 2 weeks
- 82. Scan showing right hepatic lobe abscess involving segment VII and segment VII
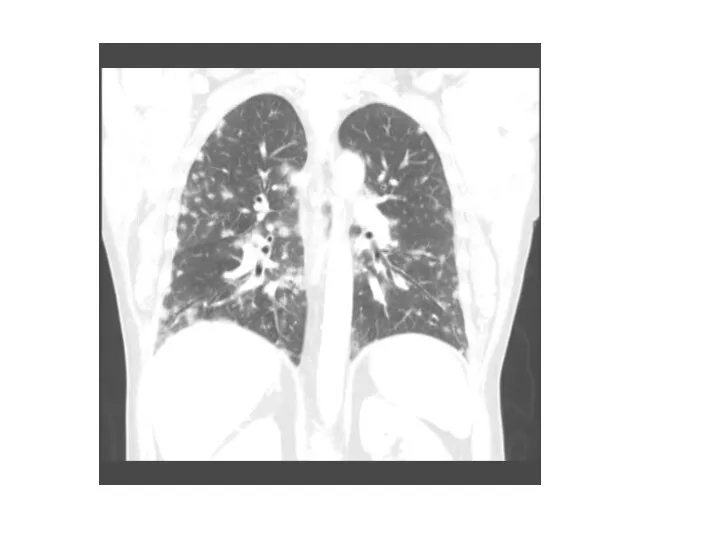
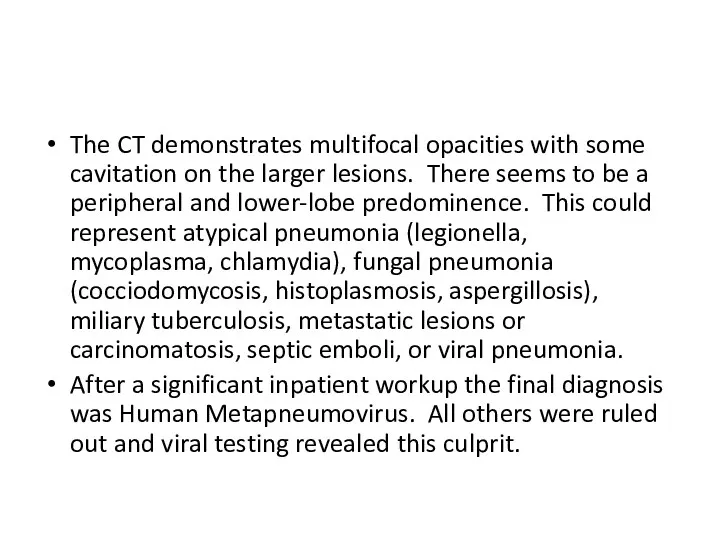
- 85. The CT demonstrates multifocal opacities with some cavitation on the larger lesions. There seems to be
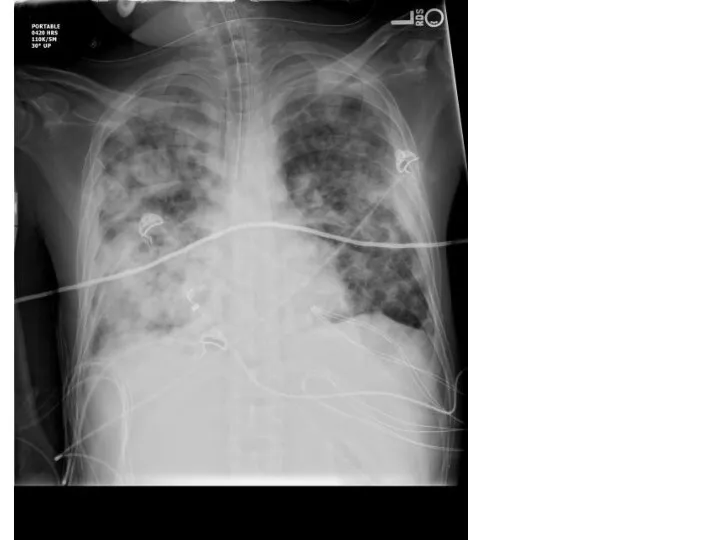
- 87. This is a multilobar pneumonia vs. ARDS (Acute Respiratory Distress Syndrome). AIDS patients can have the
- 88. Multilobar infiltrates Pneumocystis Jiroveci (PCP pneumonia) Coccidioides species Cytomegalovirus (CMV) Tuberculosis (TB) Histoplasma species Aspergillus species
- 89. Non-infectious causes of multilobar infiltrates diffuse alveolar hemorrhage, cardiogenic pulmonary edema, ARDS, multilobar involvement of the
- 90. Cavitary lesions in the lungs are gas or fluid filled compartments in an area of pathology,
- 124. Скачать презентацию
Definitions
Ethiology (general), risk factors
Diagnosis criteria and evaluation
Peculiarities of the disease
Definitions
Ethiology (general), risk factors
Diagnosis criteria and evaluation
Peculiarities of the disease
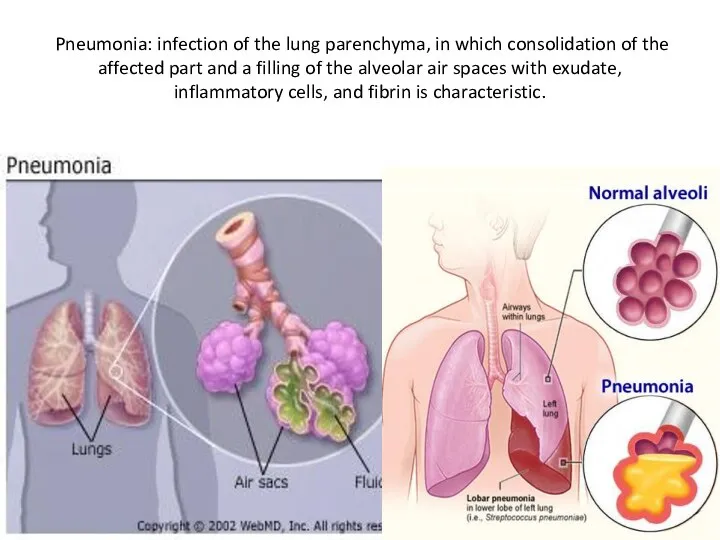
Pneumonia: infection of the lung parenchyma, in which consolidation of the
Pneumonia: infection of the lung parenchyma, in which consolidation of the
Ethiology (general)
Bacterial – most common
Viral
Rickettsiae
Fungi
Yeasts
Mycobacteria
Ethiology (general)
Bacterial – most common
Viral
Rickettsiae
Fungi
Yeasts
Mycobacteria
Risk factors (general)
Influenza (especially H1N1)
local lung pathologies (tumors, COPD, bronchiectasis), smoking
Chronic
Risk factors (general)
Influenza (especially H1N1)
local lung pathologies (tumors, COPD, bronchiectasis), smoking
Chronic
CAP: Pneumonia not acquired in a hospital or a long-term care
CAP: Pneumonia not acquired in a hospital or a long-term care
Epidemiology
5.6 million cases of CAP annually in the United States
total annual
Epidemiology
5.6 million cases of CAP annually in the United States
total annual
Ethiology
Typical: up to 70%
Usually caused by Streptococcus pneumoniae
Atypical: 30-40%
“My Lungs Contain
Ethiology
Typical: up to 70%
Usually caused by Streptococcus pneumoniae
Atypical: 30-40%
“My Lungs Contain
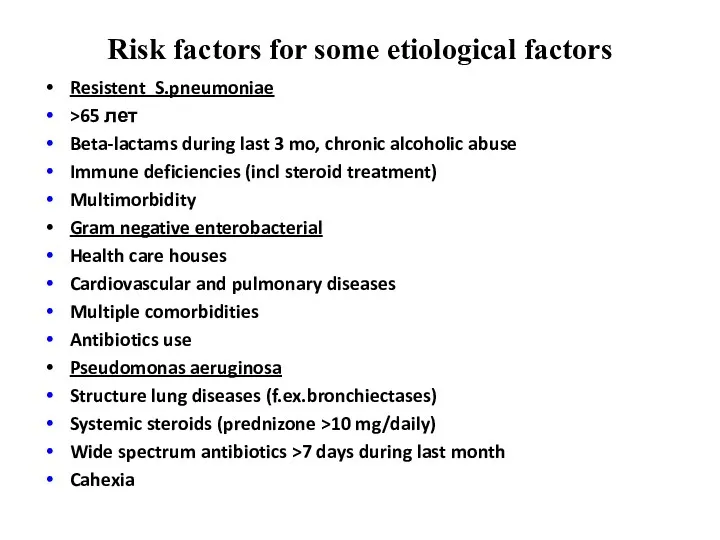
Risk factors for some etiological factors
Resistent S.pneumoniae
>65 лет
Beta-lactams during
Risk factors for some etiological factors
Resistent S.pneumoniae
>65 лет
Beta-lactams during
Intoxication fever, chills, fatigue, dyspnea, headache and myalgia
Cough may be
Intoxication fever, chills, fatigue, dyspnea, headache and myalgia
Cough may be
CXR (PA and Lateral):
American Thoracic Society (ATS) guidelines, “all patients
CXR (PA and Lateral):
American Thoracic Society (ATS) guidelines, “all patients
Lobar pneumonia
(also known as a non-segmental pneumonia or focal non-segmental pneumonia 7) is a radiological pattern
Lobar pneumonia
(also known as a non-segmental pneumonia or focal non-segmental pneumonia 7) is a radiological pattern
Other causative organisms
Klebsiella pneumoniae
Legionella pneumophila
Haemophilus influenzae
Mycobacterium tuberculosis
Other causative organisms
Klebsiella pneumoniae
Legionella pneumophila
Haemophilus influenzae
Mycobacterium tuberculosis
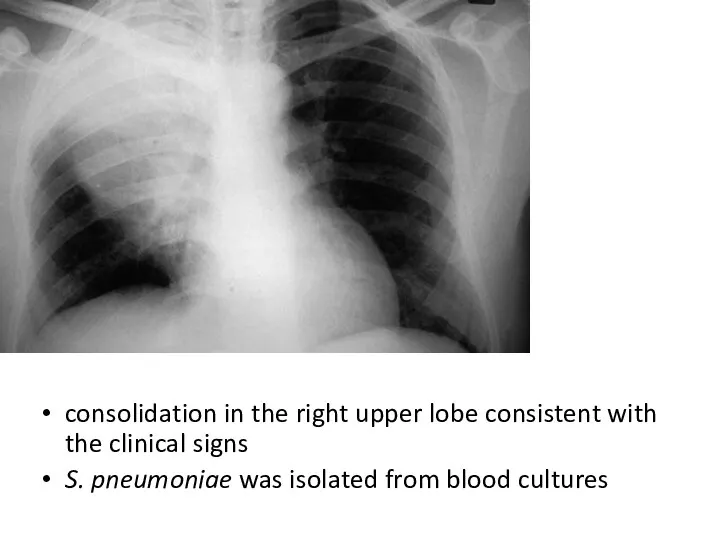
consolidation in the right upper lobe consistent with the clinical signs
S.
consolidation in the right upper lobe consistent with the clinical signs
S.
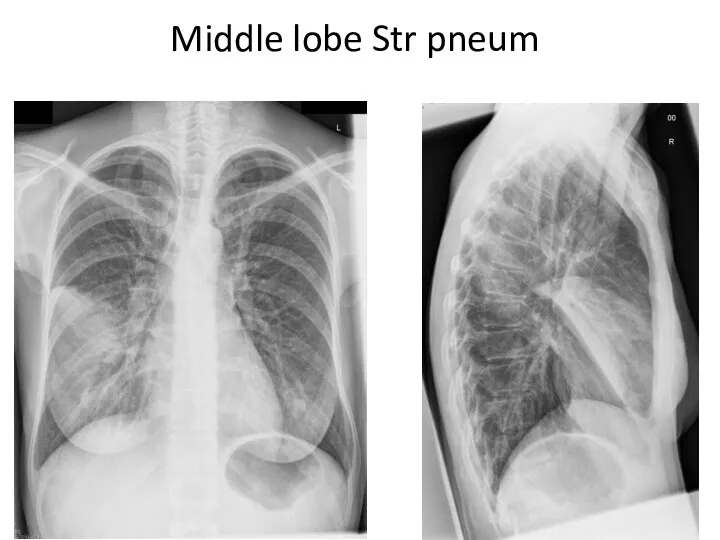
Middle lobe Str pneum
Middle lobe Str pneum
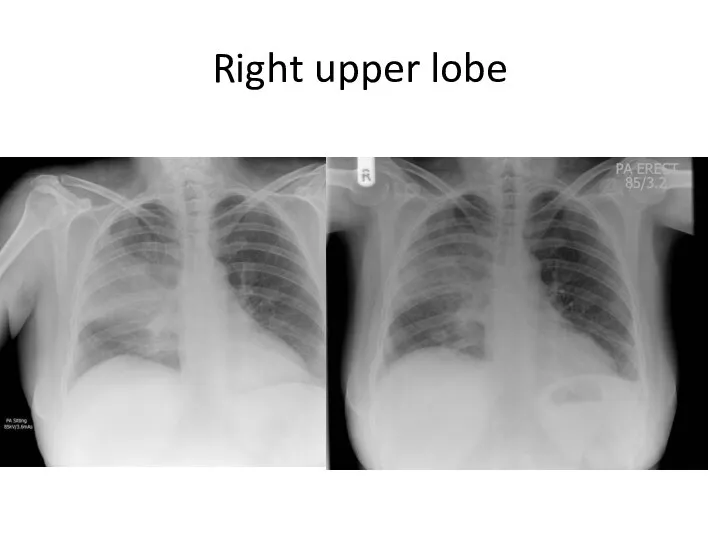
Right upper lobe
Right upper lobe
consolidation in the right upper lobe consistent with the clinical signs
S.
consolidation in the right upper lobe consistent with the clinical signs
S.
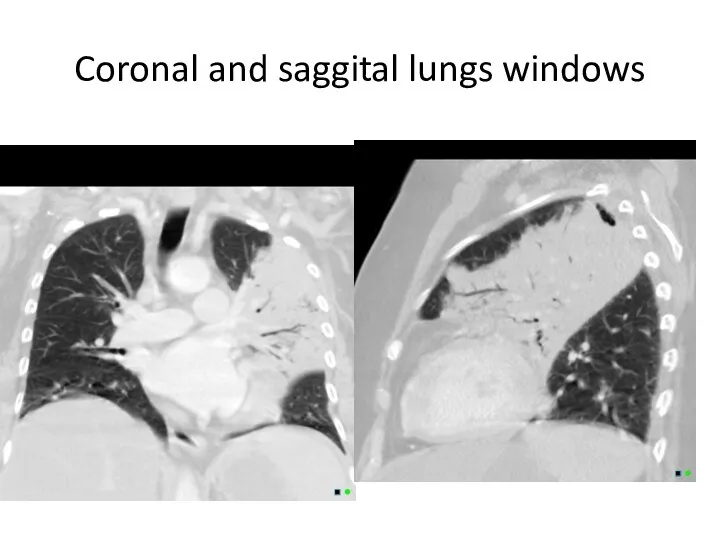
Coronal and saggital lungs windows
Coronal and saggital lungs windows
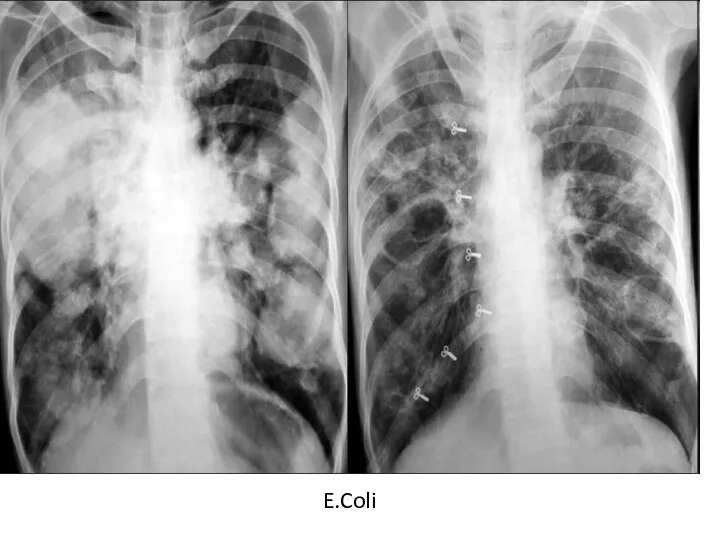
E.Coli
E.Coli
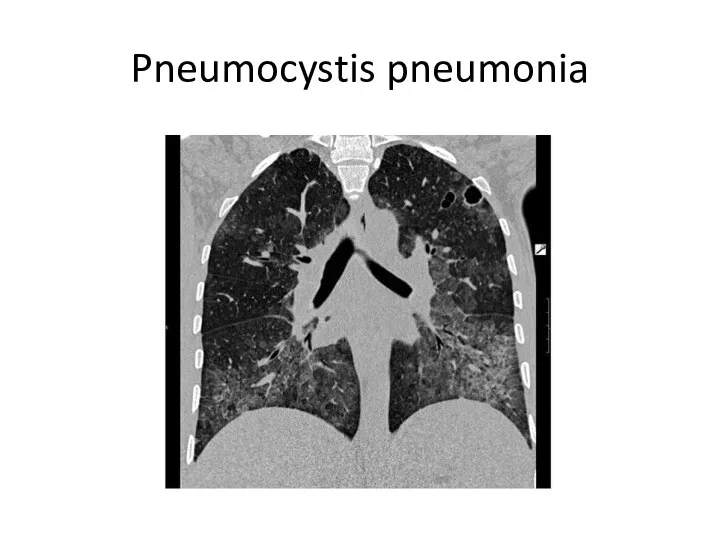
Pneumocystis pneumonia
Pneumocystis pneumonia
E.Coli
E.Coli
Acute respiratory failure severity –
necessity of non-invasive ventilation
Acute respiratory failure severity –
necessity of non-invasive ventilation
Round pneumonia: usually seen in paediatric patients. They are well defined, rounded
Round pneumonia: usually seen in paediatric patients. They are well defined, rounded


Bronchopneumonia
also sometimes known as lobular pneumonia
radiological pattern associated with suppurative peribronchiolar inflammation
Bronchopneumonia
also sometimes known as lobular pneumonia
radiological pattern associated with suppurative peribronchiolar inflammation
Causative organisms of a bronchopneumonia pattern include 3:
Staphylococcus aureus
Klebsiella pneumoniae
Haemophilus influenzae
Pseudomonas aeruginosa
Escherichia
Causative organisms of a bronchopneumonia pattern include 3:
Staphylococcus aureus
Klebsiella pneumoniae
Haemophilus influenzae
Pseudomonas aeruginosa
Escherichia
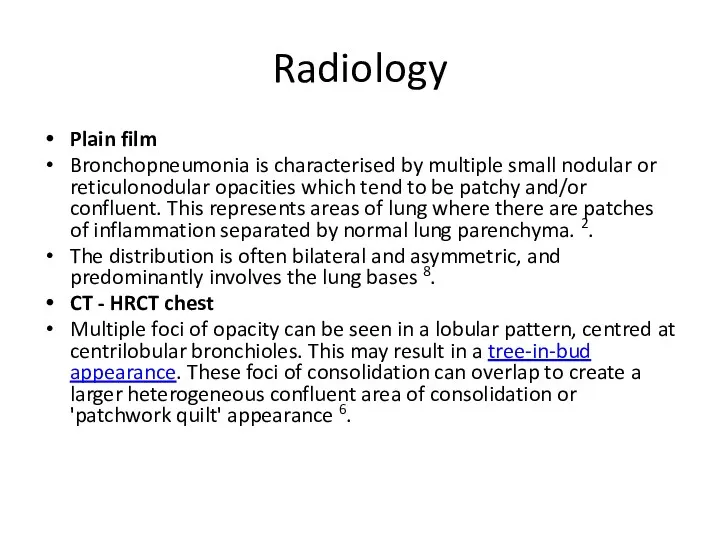
Radiology
Plain film
Bronchopneumonia is characterised by multiple small nodular or reticulonodular opacities which
Radiology
Plain film
Bronchopneumonia is characterised by multiple small nodular or reticulonodular opacities which
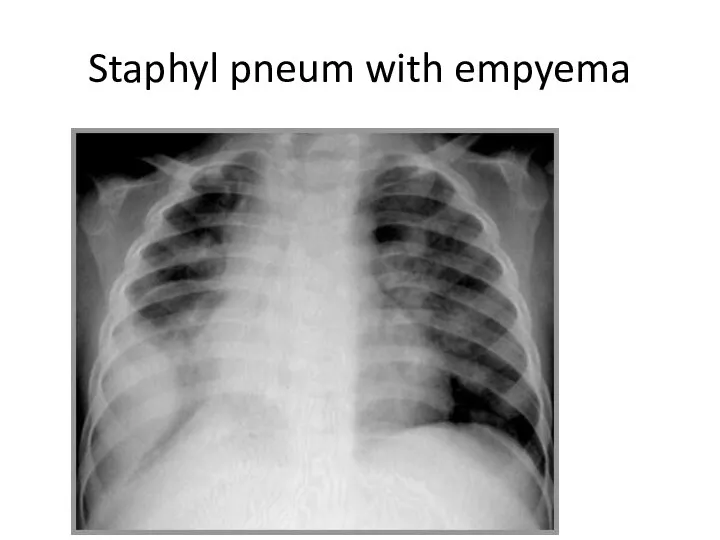
Staphyl pneum with empyema
Staphyl pneum with empyema
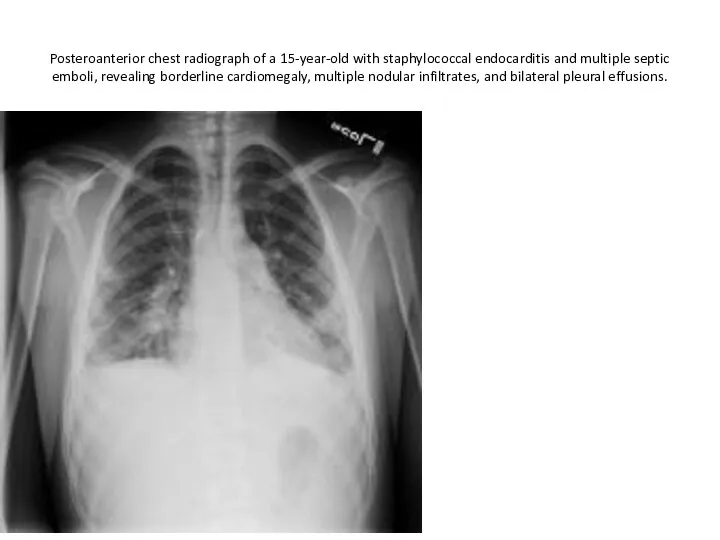
Posteroanterior chest radiograph of a 15-year-old with staphylococcal endocarditis and multiple
Posteroanterior chest radiograph of a 15-year-old with staphylococcal endocarditis and multiple

Lat/view
Lat/view
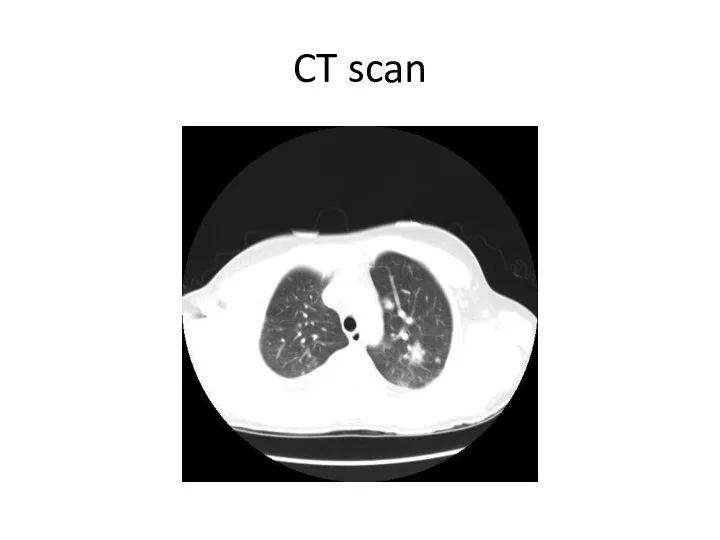
CT scan
CT scan
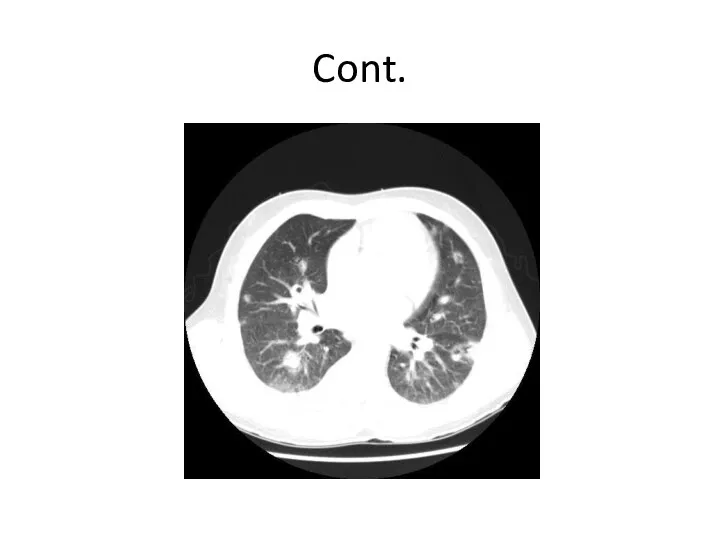
Cont.
Cont.
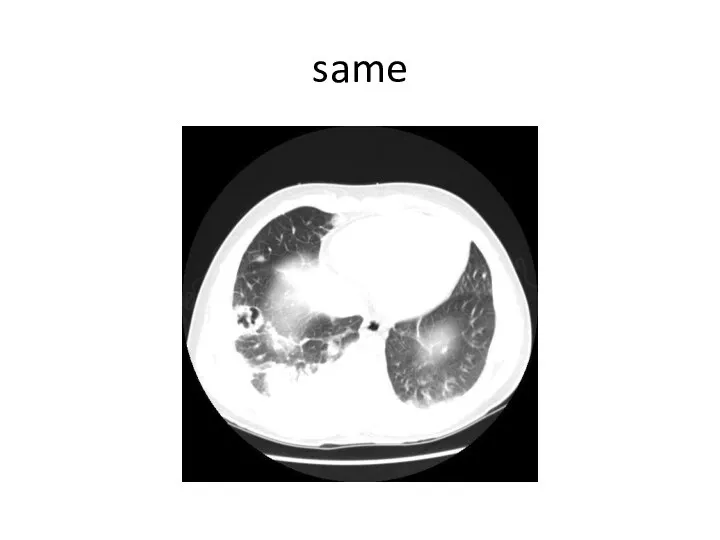
same
same
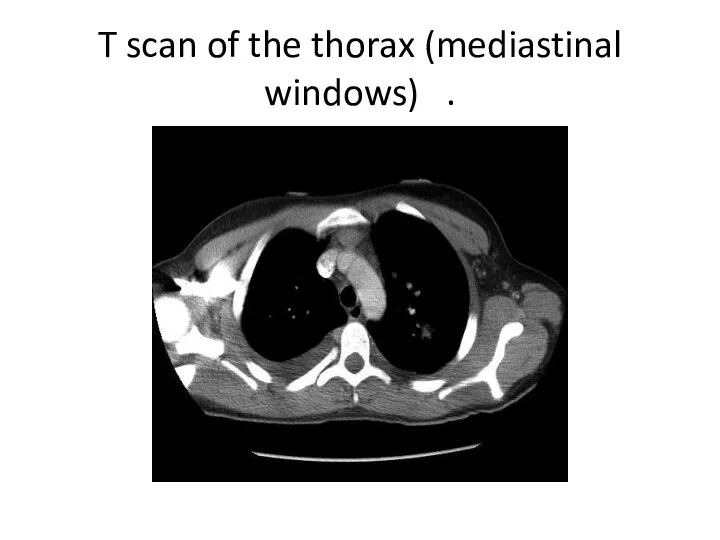
T scan of the thorax (mediastinal windows) .
T scan of the thorax (mediastinal windows) .
follow up
follow up
Cavitating clebsiella pneum
Cavitating clebsiella pneum
Mycoplasma
Mycoplasma

Klebsiella
Klebsiella
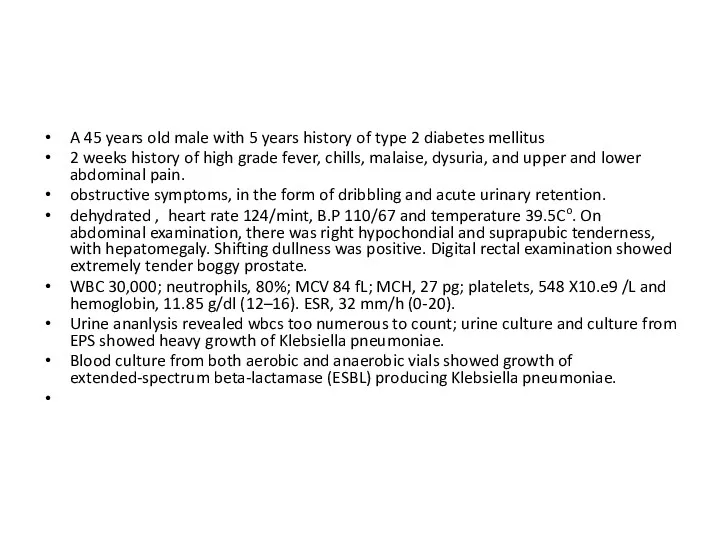
A 45 years old male with 5 years history of type
A 45 years old male with 5 years history of type
Scan showing right hepatic lobe abscess involving segment VII and segment
Scan showing right hepatic lobe abscess involving segment VII and segment

The CT demonstrates multifocal opacities with some cavitation on the larger
The CT demonstrates multifocal opacities with some cavitation on the larger
This is a multilobar pneumonia vs. ARDS (Acute Respiratory Distress Syndrome).
This is a multilobar pneumonia vs. ARDS (Acute Respiratory Distress Syndrome).
Multilobar infiltrates
Pneumocystis Jiroveci (PCP pneumonia)
Coccidioides species
Cytomegalovirus (CMV)
Tuberculosis (TB)
Histoplasma species
Aspergillus species
Mycobacterium avium complex (MAC)
Influenza
Herpes simplex virus (HSV)
Varicella-zoster
Multilobar infiltrates
Pneumocystis Jiroveci (PCP pneumonia)
Coccidioides species
Cytomegalovirus (CMV)
Tuberculosis (TB)
Histoplasma species
Aspergillus species
Mycobacterium avium complex (MAC)
Influenza
Herpes simplex virus (HSV)
Varicella-zoster
Non-infectious causes of multilobar infiltrates
diffuse alveolar hemorrhage,
cardiogenic pulmonary edema,
Non-infectious causes of multilobar infiltrates
diffuse alveolar hemorrhage,
cardiogenic pulmonary edema,
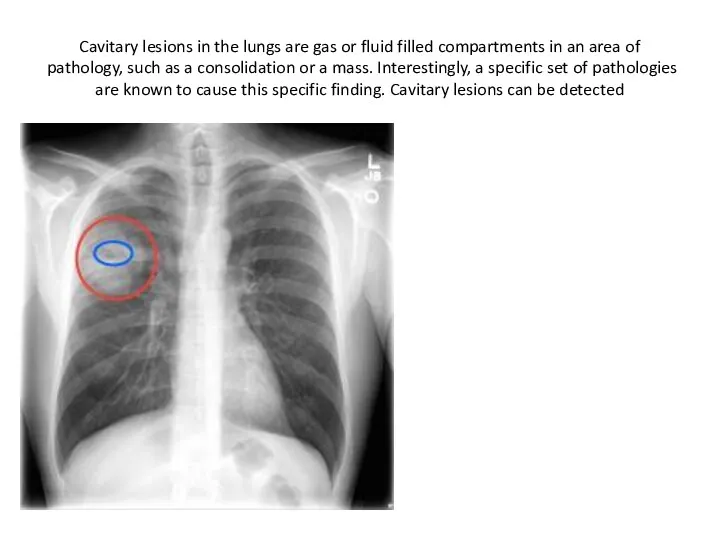
Cavitary lesions in the lungs are gas or fluid filled compartments
Cavitary lesions in the lungs are gas or fluid filled compartments

 Посттрансплантационные осложнения. Что такое РТПХ? Иммуносупрессивная терапия
Посттрансплантационные осложнения. Что такое РТПХ? Иммуносупрессивная терапия Правила личной гигиены и здоровья
Правила личной гигиены и здоровья Роль зовнішніх факторів у патології. Патогенна дія фізичних факторів на організм. (Лекція 3)
Роль зовнішніх факторів у патології. Патогенна дія фізичних факторів на організм. (Лекція 3) Оказание первой помощи. Современные требования. Часть 1
Оказание первой помощи. Современные требования. Часть 1 Кардиомиопатии (КМП)
Кардиомиопатии (КМП) Глубокое резцовое перекрытие и дистальное смещение нижней челюсти
Глубокое резцовое перекрытие и дистальное смещение нижней челюсти Акушериядағы қан кетулер. Босанғаннан кейінгі ҚК
Акушериядағы қан кетулер. Босанғаннан кейінгі ҚК Развитие зубов. Закладка зачатков зубов
Развитие зубов. Закладка зачатков зубов Местное лечение заболеваний пародонта
Местное лечение заболеваний пародонта Зубы. Твердые и мягкие ткани зуба. Поддерживающий аппарат зуба
Зубы. Твердые и мягкие ткани зуба. Поддерживающий аппарат зуба Жынысты көбею. Мейоз, оның биологиялық маңызы
Жынысты көбею. Мейоз, оның биологиялық маңызы Повреждения острыми предметами
Повреждения острыми предметами Синтетические противомикробные средства
Синтетические противомикробные средства Алгоритм ранней диагностики злокачественных новообразований на уровне ПМСП
Алгоритм ранней диагностики злокачественных новообразований на уровне ПМСП Новые горизонты в лечении ИБС
Новые горизонты в лечении ИБС Хроническая обструктивная болезнь легких
Хроническая обструктивная болезнь легких 12 жұп бас ми нервтері
12 жұп бас ми нервтері Синдром Марфана
Синдром Марфана Ампутации и экзартикуляции конечностей
Ампутации и экзартикуляции конечностей Психологія діагностичного процесу
Психологія діагностичного процесу The hormonal regulation of the body
The hormonal regulation of the body Оба қоздырғышы
Оба қоздырғышы Бригаданың медициналық қызметі
Бригаданың медициналық қызметі Александр Николаевич Кудрин
Александр Николаевич Кудрин The physiology of childbirth
The physiology of childbirth Приоритеты в медикаментах
Приоритеты в медикаментах Доказательная профилактика. Основные виды, проблемы внедрения и анализа результатов скрининговых программ
Доказательная профилактика. Основные виды, проблемы внедрения и анализа результатов скрининговых программ Семейная наследственная гиперхолестеринемия
Семейная наследственная гиперхолестеринемия