- Psoriasis and lichen

Содержание
- 2. Lection 5 Psoriasis and Lichen Ruber Planus.
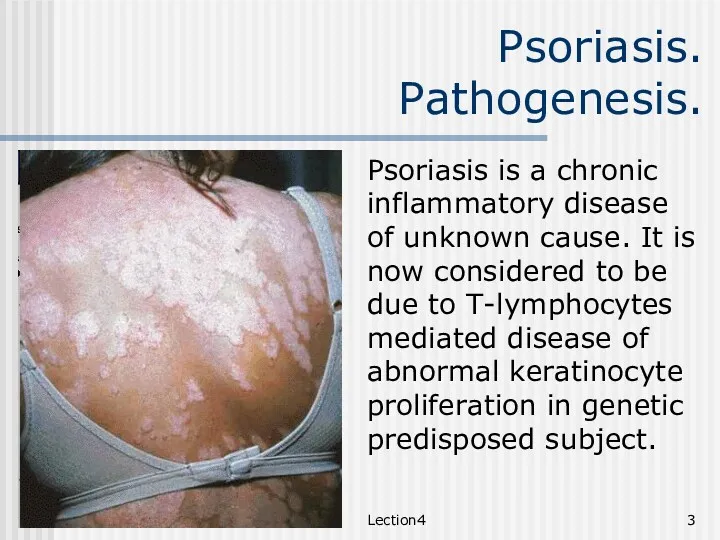
- 3. Lection4 Psoriasis. Pathogenesis. Psoriasis is a chronic inflammatory disease of unknown cause. It is now considered
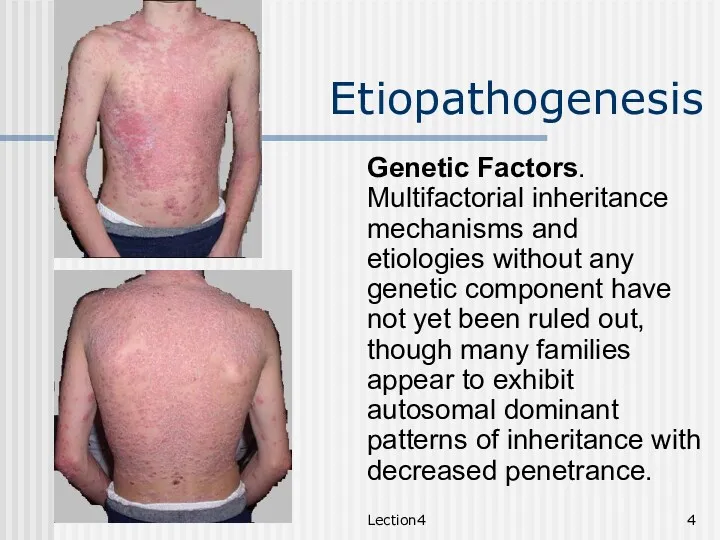
- 4. Lection4 Etiopathogenesis Genetic Factors. Multifactorial inheritance mechanisms and etiologies without any genetic component have not yet
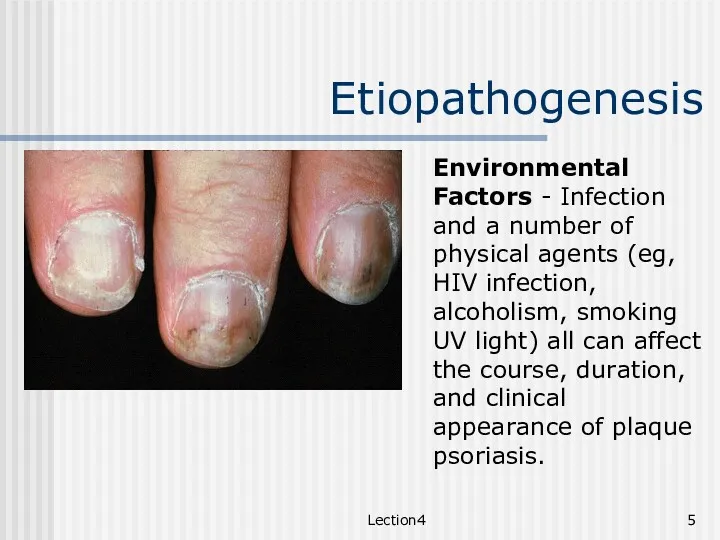
- 5. Lection4 Etiopathogenesis Environmental Factors - Infection and a number of physical agents (eg, HIV infection, alcoholism,
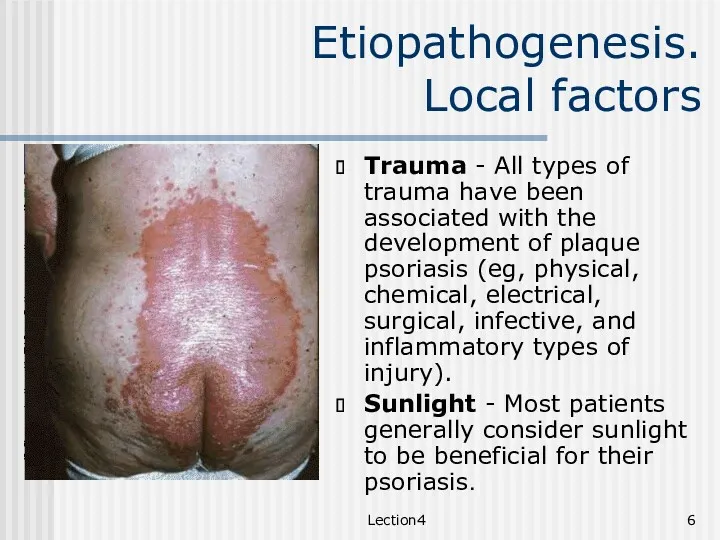
- 6. Lection4 Etiopathogenesis. Local factors Trauma - All types of trauma have been associated with the development
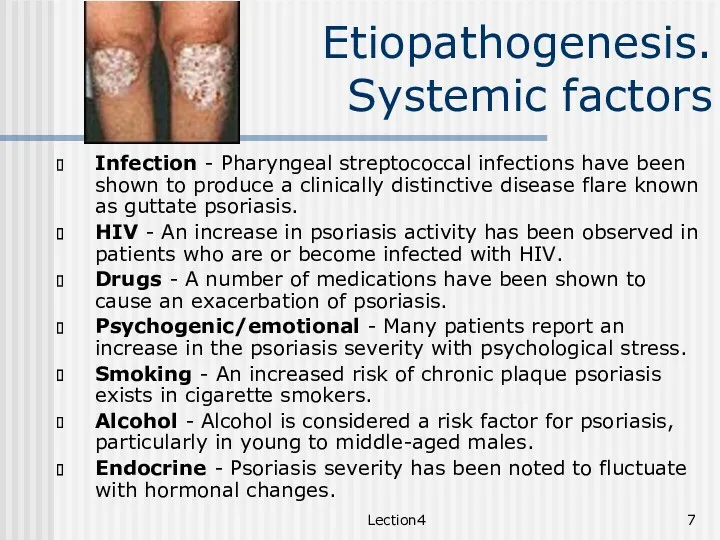
- 7. Lection4 Etiopathogenesis. Systemic factors Infection - Pharyngeal streptococcal infections have been shown to produce a clinically
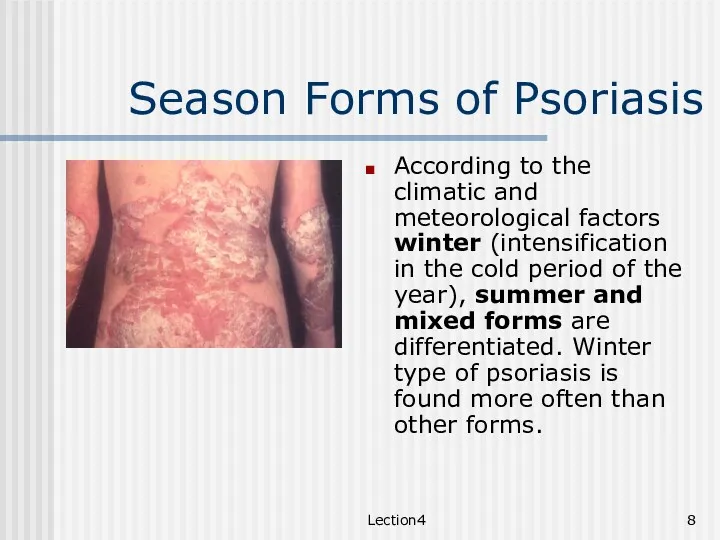
- 8. Lection4 Season Forms of Psoriasis According to the climatic and meteorological factors winter (intensification in the
- 9. Lection4 Stages Stages. In the progress of clinical development three stages of inflammatory process are distinguished:
- 10. Lection4 Clinical classification Non-pustular Psoriasis Chronic Plague type Acute Guttate Inverse, flexural Erythrodermic Regional: palms and
- 11. Lection4 Clinical classification Pustular Psoriasis Generalized Pustular psoriasis (von Zumbusch) Localized pustular psoriasis of palms &
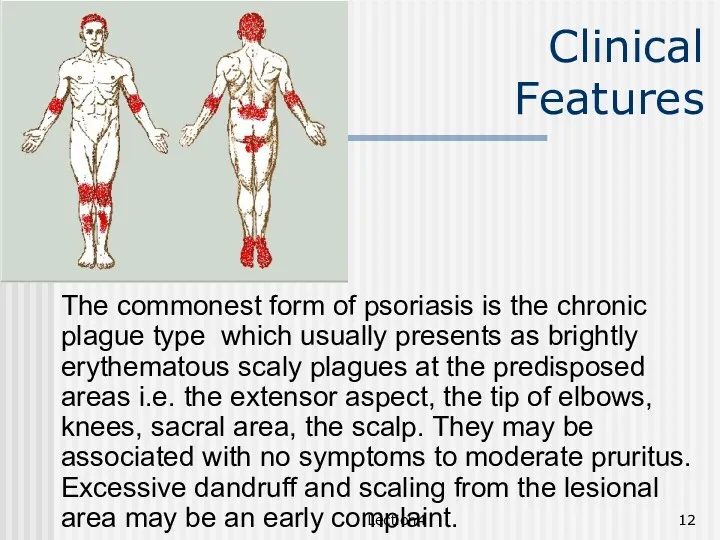
- 12. Lection4 Clinical Features The commonest form of psoriasis is the chronic plague type which usually presents
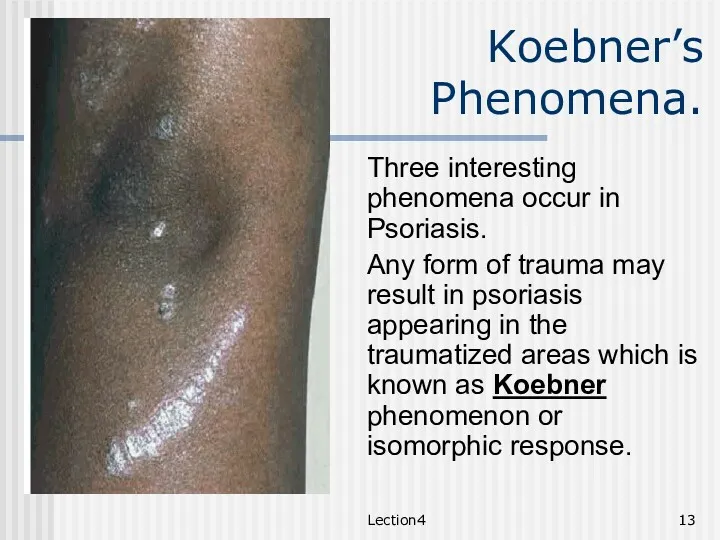
- 13. Lection4 Koebner’s Phenomena. Three interesting phenomena occur in Psoriasis. Any form of trauma may result in
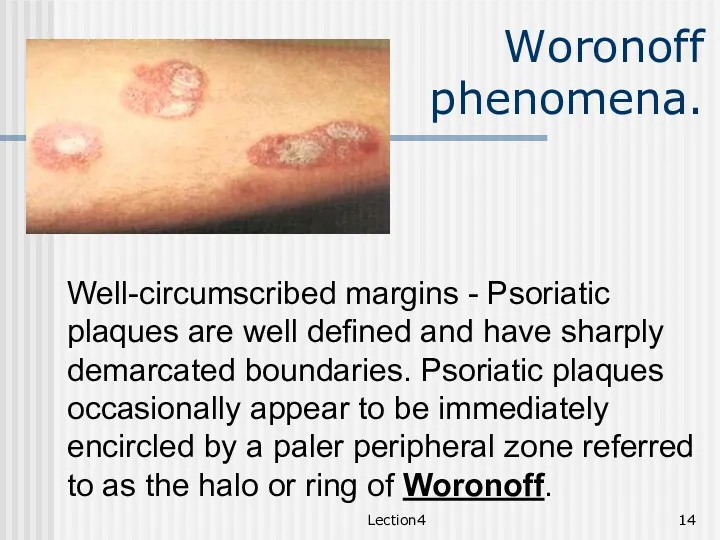
- 14. Lection4 Woronoff phenomena. Well-circumscribed margins - Psoriatic plaques are well defined and have sharply demarcated boundaries.
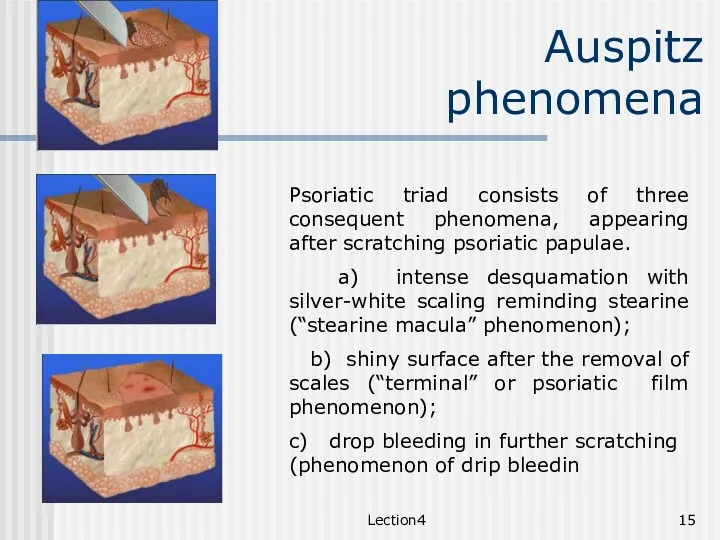
- 15. Lection4 Auspitz phenomena Psoriatic triad consists of three consequent phenomena, appearing after scratching psoriatic papulae. a)
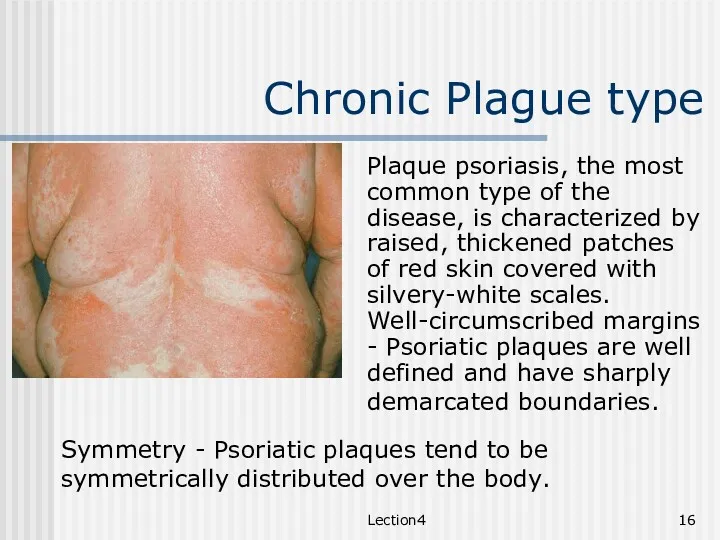
- 16. Lection4 Chronic Plague type Plaque psoriasis, the most common type of the disease, is characterized by
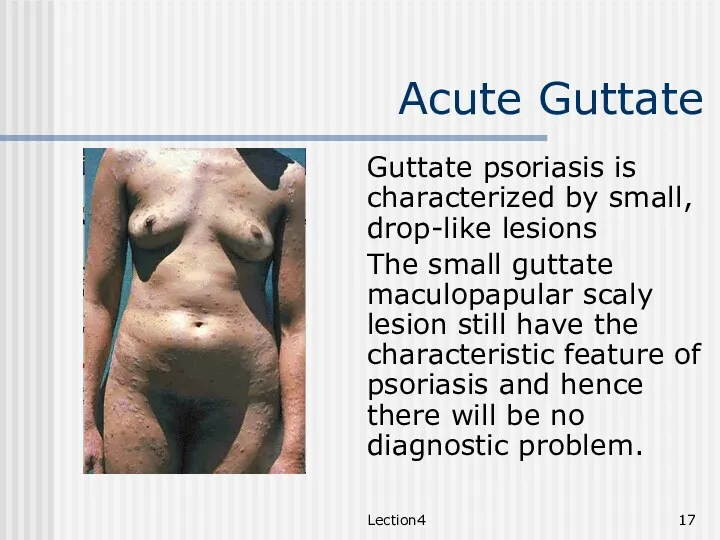
- 17. Lection4 Acute Guttate Guttate psoriasis is characterized by small, drop-like lesions The small guttate maculopapular scaly
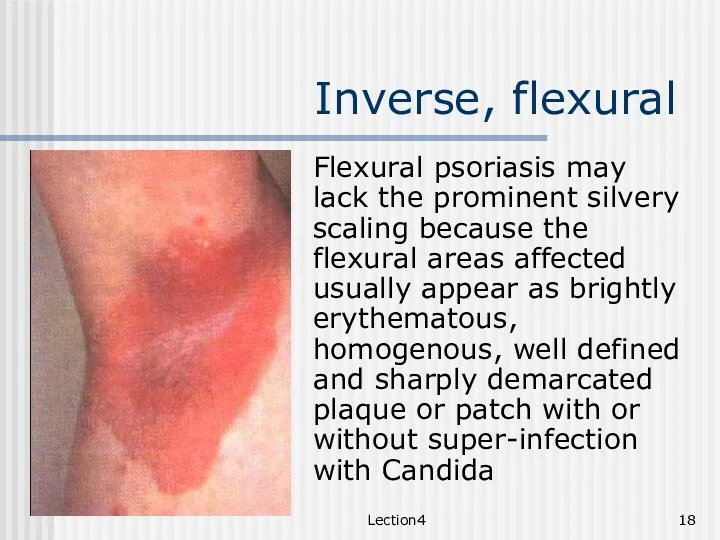
- 18. Lection4 Inverse, flexural Flexural psoriasis may lack the prominent silvery scaling because the flexural areas affected
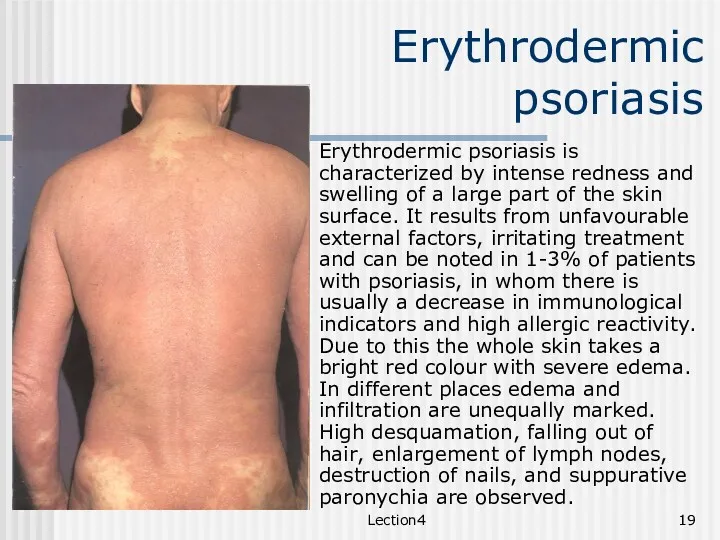
- 19. Lection4 Erythrodermic psoriasis Erythrodermic psoriasis is characterized by intense redness and swelling of a large part
- 20. Lection4 Regional Nails Nail involvement is commonly seen in all types of psoriasis which can affect
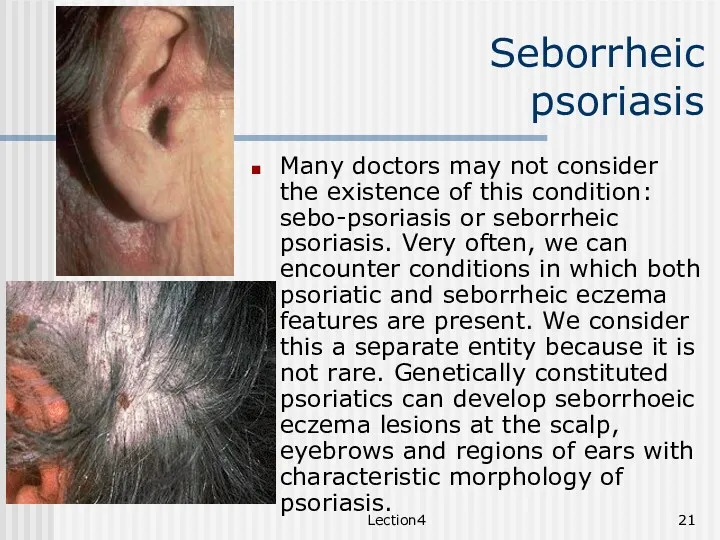
- 21. Lection4 Seborrheic psoriasis Many doctors may not consider the existence of this condition: sebo-psoriasis or seborrheic
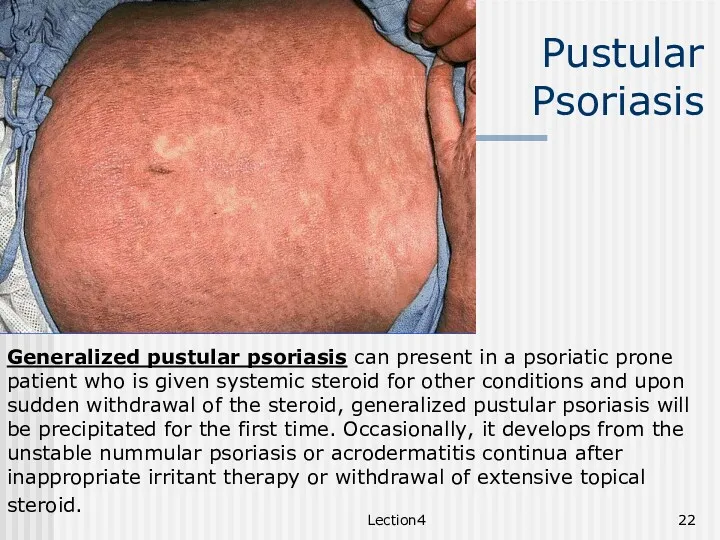
- 22. Lection4 Pustular Psoriasis Generalized pustular psoriasis can present in a psoriatic prone patient who is given
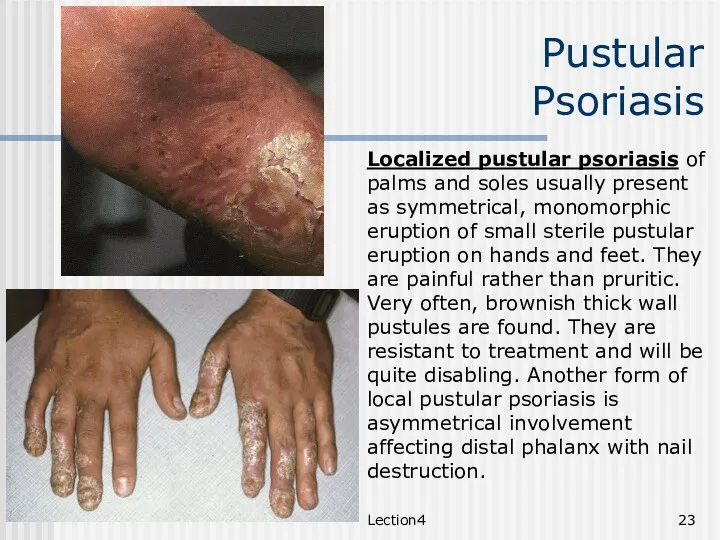
- 23. Lection4 Pustular Psoriasis Localized pustular psoriasis of palms and soles usually present as symmetrical, monomorphic eruption
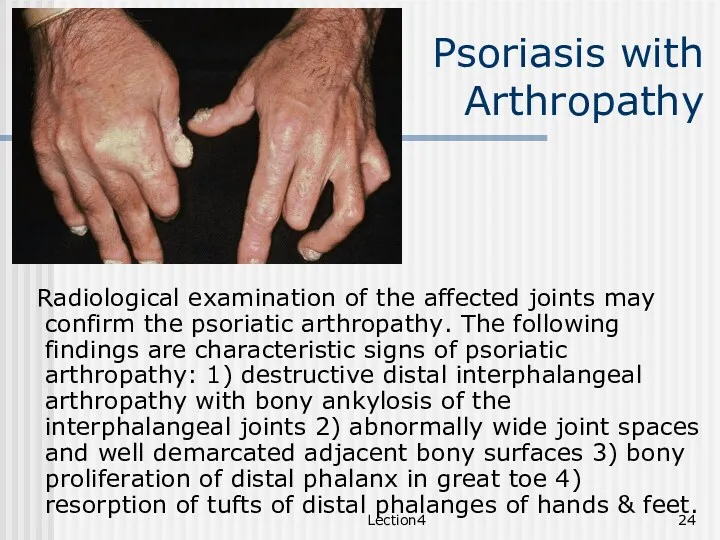
- 24. Lection4 Psoriasis with Arthropathy Radiological examination of the affected joints may confirm the psoriatic arthropathy. The
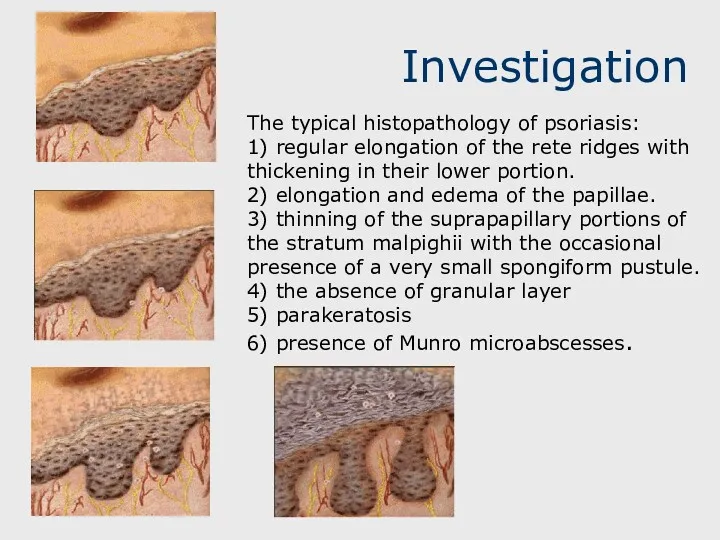
- 25. Investigation The typical histopathology of psoriasis: 1) regular elongation of the rete ridges with thickening in
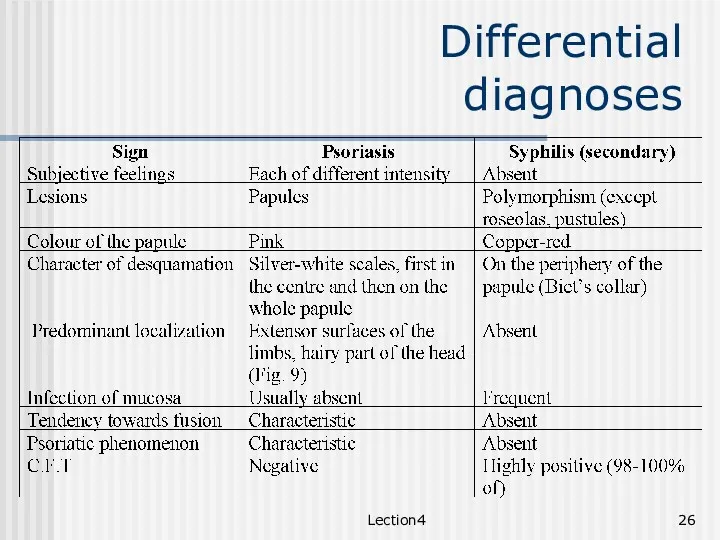
- 26. Lection4 Differential diagnoses
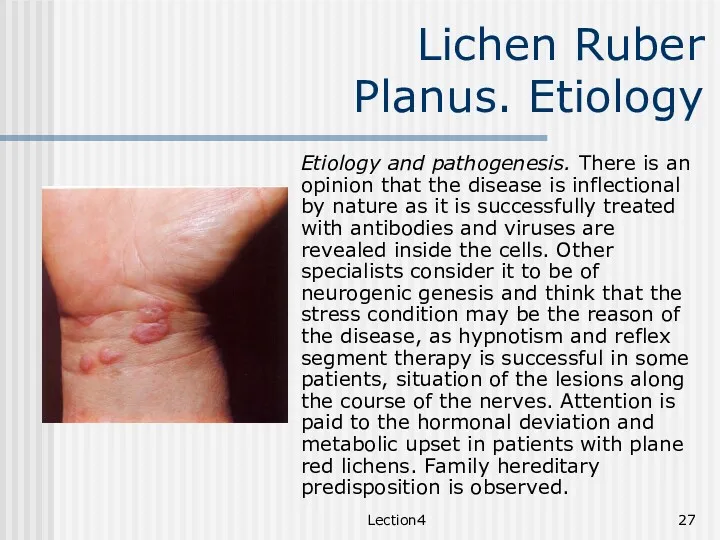
- 27. Lection4 Lichen Ruber Planus. Etiology Etiology and pathogenesis. There is an opinion that the disease is
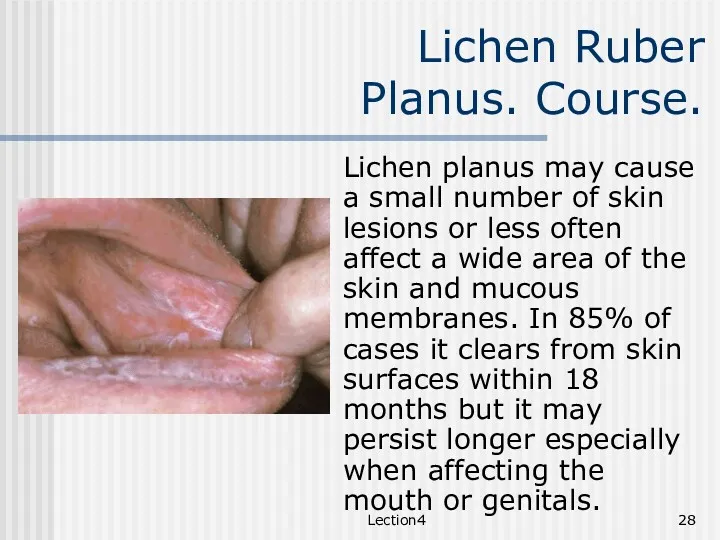
- 28. Lection4 Lichen Ruber Planus. Course. Lichen planus may cause a small number of skin lesions or
- 29. Lection4 Classification Classical lichen planus Oral lichen planus Lichen planus of nails Atypical lichen planus Hypertrophic,
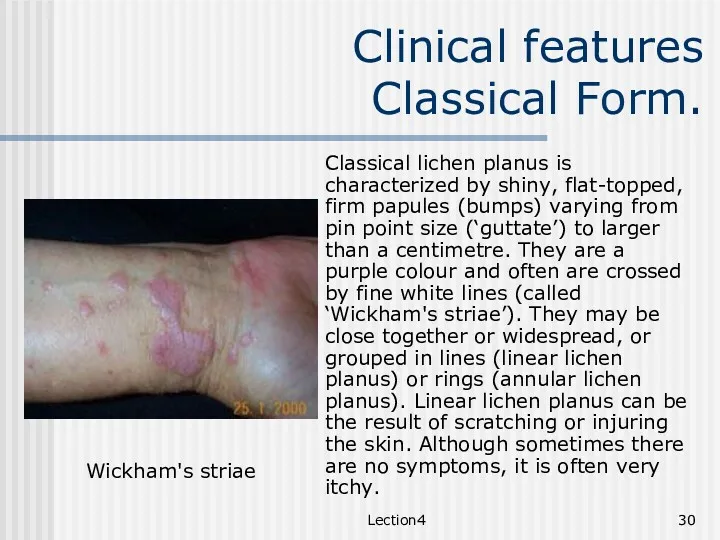
- 30. Lection4 Clinical features Classical Form. Classical lichen planus is characterized by shiny, flat-topped, firm papules (bumps)
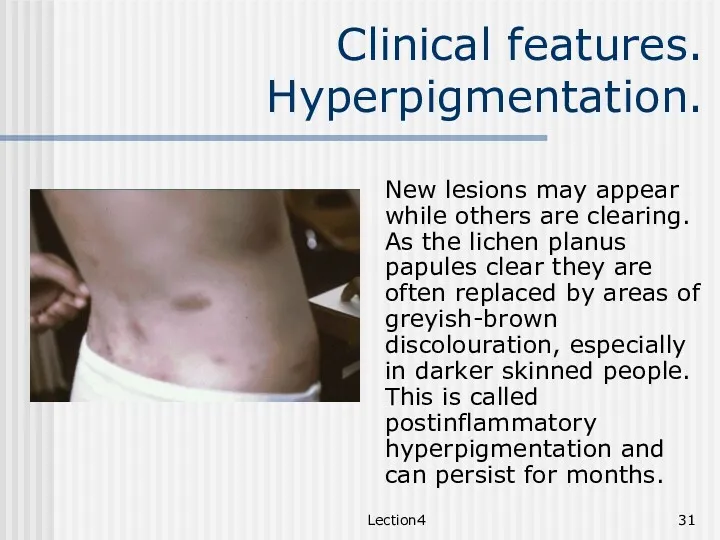
- 31. Lection4 Clinical features. Hyperpigmentation. New lesions may appear while others are clearing. As the lichen planus
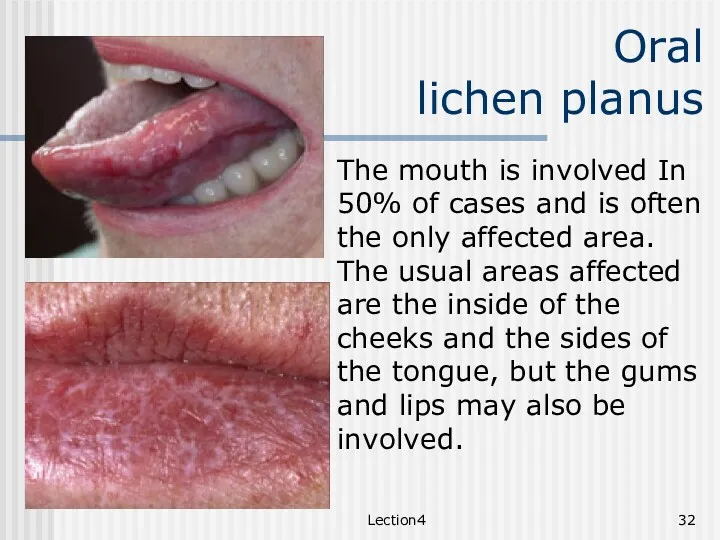
- 32. Lection4 Oral lichen planus The mouth is involved In 50% of cases and is often the
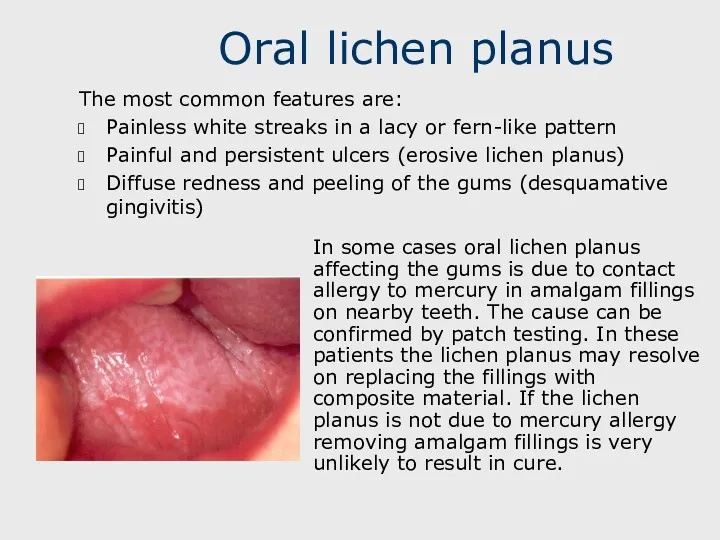
- 33. Oral lichen planus The most common features are: Painless white streaks in a lacy or fern-like
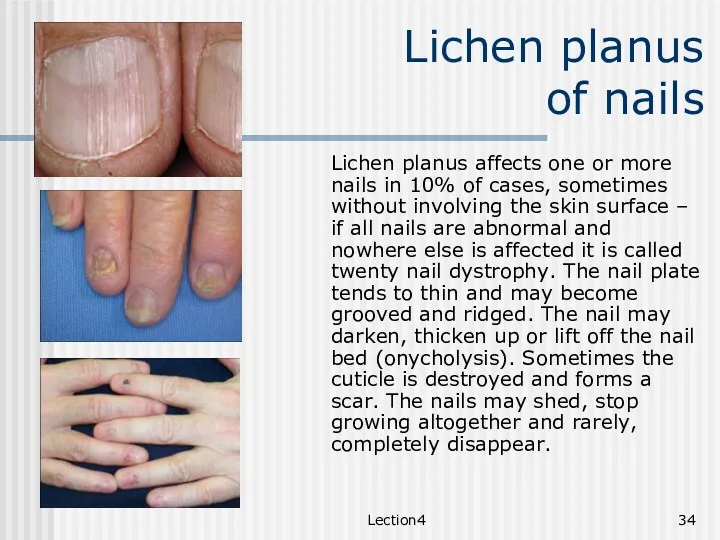
- 34. Lection4 Lichen planus of nails Lichen planus affects one or more nails in 10% of cases,
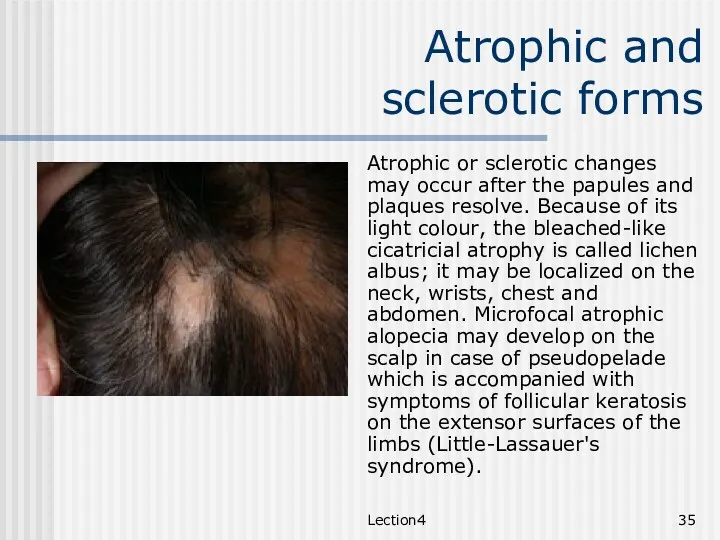
- 35. Lection4 Atrophic and sclerotic forms Atrophic or sclerotic changes may occur after the papules and plaques
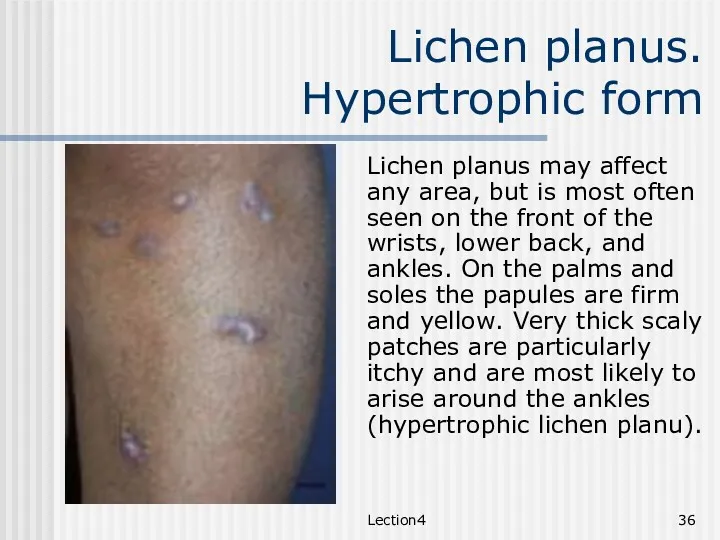
- 36. Lection4 Lichen planus. Hypertrophic form Lichen planus may affect any area, but is most often seen
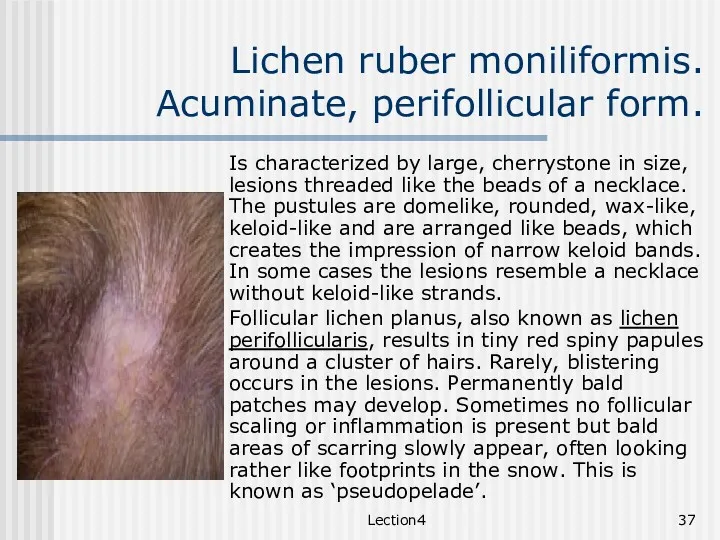
- 37. Lection4 Lichen ruber moniliformis. Acuminate, perifollicular form. Is characterized by large, cherrystone in size, lesions threaded
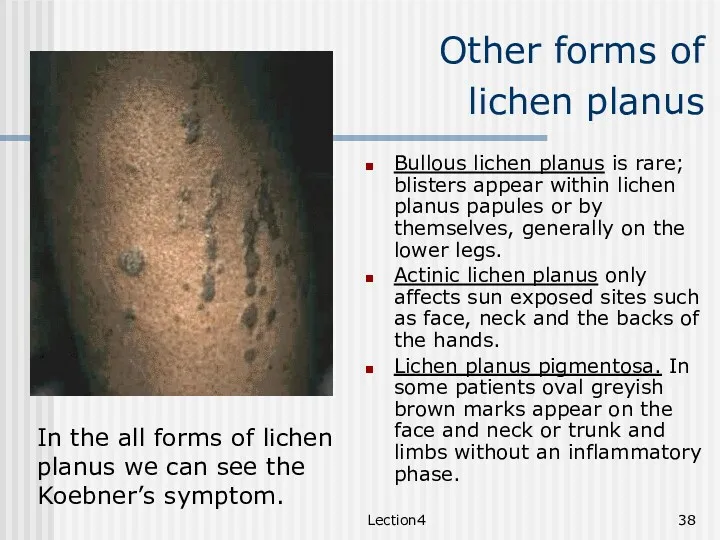
- 38. Lection4 Other forms of lichen planus Bullous lichen planus is rare; blisters appear within lichen planus
- 40. Скачать презентацию
Lection 5
Psoriasis and Lichen Ruber Planus.
Lection 5
Psoriasis and Lichen Ruber Planus.
Lection4
Psoriasis.
Pathogenesis.
Psoriasis is a chronic inflammatory disease of unknown cause. It
Lection4
Psoriasis.
Pathogenesis.
Psoriasis is a chronic inflammatory disease of unknown cause. It
Lection4
Etiopathogenesis
Genetic Factors. Multifactorial inheritance mechanisms and etiologies without any genetic component
Lection4
Etiopathogenesis
Genetic Factors. Multifactorial inheritance mechanisms and etiologies without any genetic component
Lection4
Etiopathogenesis
Environmental Factors - Infection and a number of physical agents (eg,
Lection4
Etiopathogenesis
Environmental Factors - Infection and a number of physical agents (eg,
Lection4
Etiopathogenesis.
Local factors
Trauma - All types of trauma have been associated with
Lection4
Etiopathogenesis.
Local factors
Trauma - All types of trauma have been associated with
Lection4
Etiopathogenesis.
Systemic factors
Infection - Pharyngeal streptococcal infections have been shown to produce
Lection4
Etiopathogenesis.
Systemic factors
Infection - Pharyngeal streptococcal infections have been shown to produce
Lection4
Season Forms of Psoriasis
According to the climatic and meteorological factors winter
Lection4
Season Forms of Psoriasis
According to the climatic and meteorological factors winter
Lection4
Stages
Stages. In the progress of clinical development three stages of inflammatory
Lection4
Stages
Stages. In the progress of clinical development three stages of inflammatory
Lection4
Clinical classification
Non-pustular Psoriasis
Chronic Plague type
Acute Guttate
Inverse, flexural
Erythrodermic
Regional: palms and
Lection4
Clinical classification
Non-pustular Psoriasis
Chronic Plague type
Acute Guttate
Inverse, flexural
Erythrodermic
Regional: palms and
Lection4
Clinical classification
Pustular Psoriasis
Generalized Pustular psoriasis (von Zumbusch)
Localized pustular psoriasis
Lection4
Clinical classification
Pustular Psoriasis
Generalized Pustular psoriasis (von Zumbusch)
Localized pustular psoriasis
Lection4
Clinical Features
The commonest form of psoriasis is the chronic plague
Lection4
Clinical Features
The commonest form of psoriasis is the chronic plague
Lection4
Koebner’s Phenomena.
Three interesting phenomena occur in Psoriasis.
Any form of trauma may
Lection4
Koebner’s Phenomena.
Three interesting phenomena occur in Psoriasis.
Any form of trauma may
Lection4
Woronoff
phenomena.
Well-circumscribed margins - Psoriatic plaques are well defined and have
Lection4
Woronoff
phenomena.
Well-circumscribed margins - Psoriatic plaques are well defined and have
Lection4
Auspitz phenomena
Psoriatic triad consists of three consequent phenomena, appearing after scratching
Lection4
Auspitz phenomena
Psoriatic triad consists of three consequent phenomena, appearing after scratching
Lection4
Chronic Plague type
Plaque psoriasis, the most common type of the disease,
Lection4
Chronic Plague type
Plaque psoriasis, the most common type of the disease,
Lection4
Acute Guttate
Guttate psoriasis is characterized by small, drop-like lesions
The small
Lection4
Acute Guttate
Guttate psoriasis is characterized by small, drop-like lesions
The small
Lection4
Inverse, flexural
Flexural psoriasis may lack the prominent silvery scaling because the
Lection4
Inverse, flexural
Flexural psoriasis may lack the prominent silvery scaling because the
Lection4
Erythrodermic psoriasis
Erythrodermic psoriasis is characterized by intense redness and swelling of
Lection4
Erythrodermic psoriasis
Erythrodermic psoriasis is characterized by intense redness and swelling of

Lection4
Regional
Nails
Nail involvement is commonly seen in all types of psoriasis which
Lection4
Regional
Nails
Nail involvement is commonly seen in all types of psoriasis which
Lection4
Seborrheic psoriasis
Many doctors may not consider the existence of this condition:
Lection4
Seborrheic psoriasis
Many doctors may not consider the existence of this condition:
Lection4
Pustular
Psoriasis
Generalized pustular psoriasis can present in a psoriatic prone patient
Lection4
Pustular
Psoriasis
Generalized pustular psoriasis can present in a psoriatic prone patient
Lection4
Pustular
Psoriasis
Localized pustular psoriasis of palms and soles usually present as
Lection4
Pustular
Psoriasis
Localized pustular psoriasis of palms and soles usually present as
Lection4
Psoriasis with
Arthropathy
Radiological examination of the affected joints may confirm the
Lection4
Psoriasis with
Arthropathy
Radiological examination of the affected joints may confirm the
Investigation
The typical histopathology of psoriasis:
1) regular elongation of the rete
Investigation
The typical histopathology of psoriasis:
1) regular elongation of the rete
Lection4
Differential
diagnoses
Lection4
Differential
diagnoses
Lection4
Lichen Ruber
Planus. Etiology
Etiology and pathogenesis. There is an opinion that
Lection4
Lichen Ruber
Planus. Etiology
Etiology and pathogenesis. There is an opinion that
Lection4
Lichen Ruber
Planus. Course.
Lichen planus may cause a small number of
Lection4
Lichen Ruber
Planus. Course.
Lichen planus may cause a small number of
Lection4
Classification
Classical lichen planus
Oral lichen planus
Lichen planus of nails
Atypical
Lection4
Classification
Classical lichen planus
Oral lichen planus
Lichen planus of nails
Atypical
Lection4
Clinical features
Classical Form.
Classical lichen planus is characterized by shiny, flat-topped, firm
Lection4
Clinical features
Classical Form.
Classical lichen planus is characterized by shiny, flat-topped, firm
Lection4
Clinical features. Hyperpigmentation.
New lesions may appear while others are clearing. As
Lection4
Clinical features. Hyperpigmentation.
New lesions may appear while others are clearing. As
Lection4
Oral
lichen planus
The mouth is involved In 50% of cases
Lection4
Oral
lichen planus
The mouth is involved In 50% of cases
Oral lichen planus
The most common features are:
Painless white streaks in a
Oral lichen planus
The most common features are:
Painless white streaks in a
Lection4
Lichen planus
of nails
Lichen planus affects one or more nails in
Lection4
Lichen planus
of nails
Lichen planus affects one or more nails in
Lection4
Atrophic and
sclerotic forms
Atrophic or sclerotic changes may occur after the
Lection4
Atrophic and
sclerotic forms
Atrophic or sclerotic changes may occur after the
Lection4
Lichen planus.
Hypertrophic form
Lichen planus may affect any area, but is
Lection4
Lichen planus.
Hypertrophic form
Lichen planus may affect any area, but is
Lection4
Lichen ruber moniliformis. Acuminate, perifollicular form.
Is characterized by large, cherrystone in
Lection4
Lichen ruber moniliformis. Acuminate, perifollicular form.
Is characterized by large, cherrystone in
Lection4
Other forms of
lichen planus
Bullous lichen planus is rare; blisters
Lection4
Other forms of
lichen planus
Bullous lichen planus is rare; blisters
 Роль наследственности в патологии
Роль наследственности в патологии Кардиогенный шок
Кардиогенный шок Кодексы разработки и применения ЛС. Этические аспекты КИ. Нежелательные явления в КИ. Оригинальные и генерические препараты
Кодексы разработки и применения ЛС. Этические аспекты КИ. Нежелательные явления в КИ. Оригинальные и генерические препараты Диетотерапия при кишечных заболеваниях у детей
Диетотерапия при кишечных заболеваниях у детей Гострі кишкові інфекції у дітей (1-ша частина)
Гострі кишкові інфекції у дітей (1-ша частина) Новообразования костей лица у детей
Новообразования костей лица у детей Плевриты. Инфекционные и неинфекционные плевриты
Плевриты. Инфекционные и неинфекционные плевриты Гравидограмма интерпритациясы
Гравидограмма интерпритациясы Методи візуалізації. Пакет для підготовки до практичних занять та підсумкового контролю з дисципліни Анатомії людини
Методи візуалізації. Пакет для підготовки до практичних занять та підсумкового контролю з дисципліни Анатомії людини Когнитивно-поведенческая терапия панического расстройства
Когнитивно-поведенческая терапия панического расстройства Бронхиальді тал құрылысы
Бронхиальді тал құрылысы גוף האדם בדגש הומיאוסטזיס
גוף האדם בדגש הומיאוסטזיס Туберкулез және тыныс алу мүшелерінің созылмалы бейарнамалы аурулары
Туберкулез және тыныс алу мүшелерінің созылмалы бейарнамалы аурулары Медико-социальные проблемы демографических процессов
Медико-социальные проблемы демографических процессов Противотуберкулезные препараты
Противотуберкулезные препараты Шашыранды туберкулездің дифференциальды диагностикасы. Дифференциальная диагностика туберкулеза
Шашыранды туберкулездің дифференциальды диагностикасы. Дифференциальная диагностика туберкулеза Жүйке жүйесі туралы түсінік. Жүйке жүйесінің құралу негіздері. Қарапайым және күрделі рефлекторлық доға
Жүйке жүйесі туралы түсінік. Жүйке жүйесінің құралу негіздері. Қарапайым және күрделі рефлекторлық доға Органы гемопоэза и иммуногенеза
Органы гемопоэза и иммуногенеза Предстерилизационная очистка, стерилизация и принцип работы ЦСО
Предстерилизационная очистка, стерилизация и принцип работы ЦСО Рак підшлункової залози
Рак підшлункової залози Секреты сохранения красоты и молодости после 40 лет
Секреты сохранения красоты и молодости после 40 лет Оценка качества препаратов, эффективности и безопасности профилактических и лечебных мероприятий
Оценка качества препаратов, эффективности и безопасности профилактических и лечебных мероприятий mol
mol Организация работы специализированных и линйных бригад скорой медицинской помощи
Организация работы специализированных и линйных бригад скорой медицинской помощи Фармацевтическая технология жидких лекарственных форм
Фармацевтическая технология жидких лекарственных форм Противоэпилептические и противопаркинсонические средства
Противоэпилептические и противопаркинсонические средства Неотложные состояния в акушерстве
Неотложные состояния в акушерстве Гигиенические требования к организации водоснабжения в ДОУ
Гигиенические требования к организации водоснабжения в ДОУ