- Semey medical university siw age physiology of skeletal system in child

Содержание
- 2. CONTENT
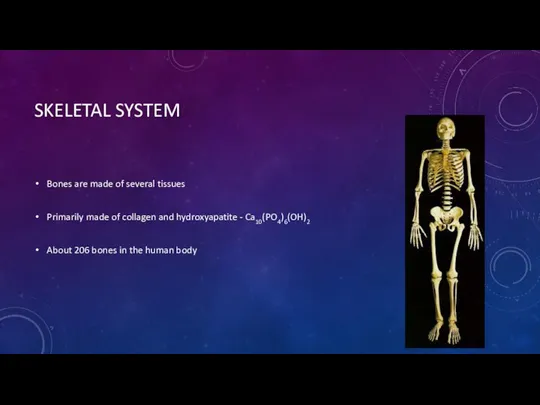
- 3. SKELETAL SYSTEM Bones are made of several tissues Primarily made of collagen and hydroxyapatite - Ca10(PO4)6(OH)2
- 4. FUNCTIONS OF SKELETAL SYSTEM SUPPORT: Hard framework that supports and anchors the soft organs of the
- 5. PARTS OF THE SKELETAL SYSTEM Axial skeleton Skull and bones that support it Includes vertebra and
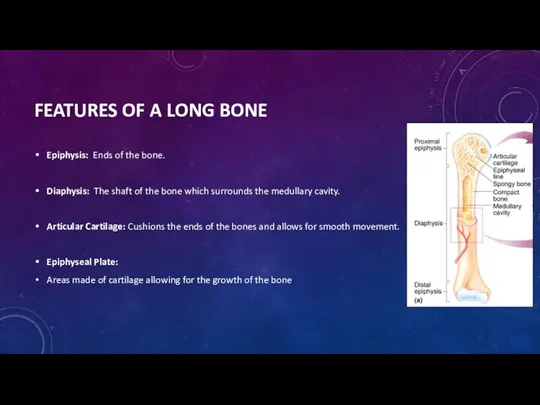
- 6. FEATURES OF A LONG BONE Epiphysis: Ends of the bone. Diaphysis: The shaft of the bone
- 7. BONE DEVELOPMENT Initial skeleton of cartilage in infants Replaced with bone by osteoblasts More than 300
- 8. BONE STRUCTURE Periosteum – hard outer covering Cells for growth and repair Compact bone – hard
- 9. BONE MARROW Red marrow – produces blood cells and clotting factors Found in humerus, femur, sternum,
- 10. SKELETAL SYSTEM OF CHILD Bone in children and toddlers is more porous than adult bone, with
- 11. The periosteal sleeve is much thicker in children than in adults and acts as a restraint
- 12. The epiphysis is an important part of the growing skeleton. It is a secondary ossification center.
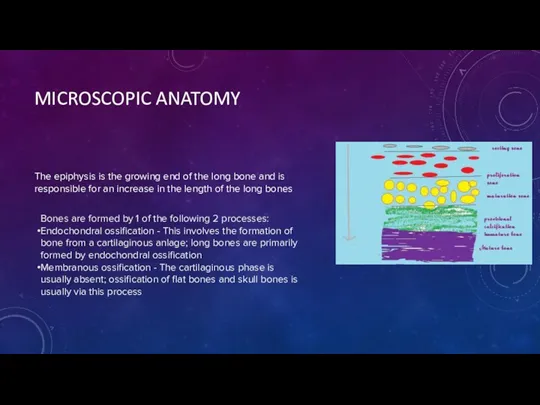
- 13. MICROSCOPIC ANATOMY The epiphysis is the growing end of the long bone and is responsible for
- 14. Histologically, the physis consists of a number of layers that reflect the process of bone formation.
- 15. The epiphysis and the metaphysis are connected by mammillary processes internally and by the tough fibrous
- 16. REMODELING Remodeling of a fracture or deformity is a process that is carried out more efficiently
- 17. An injury to a long bone can stimulate excessive growth and effectively create a temporary limb
- 18. NATURAL VARIANTS Bone in children undergoes serial changes and adaptations to achieve its adult form over
- 19. At birth, the sutures in the skull are unfused at the anterior and posterior fontanelles. However,
- 20. The varus and valgus alignments are believed to be dictated by the relative growth rates of
- 21. DEFECTS Matrix deficiencies can give rise to a myriad of conditions, the best known of which
- 22. osteogenesis imperfecta, Epiphyseal dysplasias
- 23. BROKEN BONES Fracture is a break of the bone Simple or Complex fracture Regrowth of bone:
- 24. REFRENCE https://emedicine.medscape.com/article/1899256-overview#a4 https://www.google.kz/search?q=skeletal+system+medscape&rlz=1C1ASRW_enKZ800KZ800&oq=skeletal+system+medscape&aqs=chrome..69i57j69i60.9086j0j4&sourceid=chrome&ie=UTF-8 Slide share Physiology essentials book http://www.innerbody.com/image/skelfov.html
- 26. Скачать презентацию
CONTENT
CONTENT
SKELETAL SYSTEM
Bones are made of several tissues
Primarily made of collagen and
SKELETAL SYSTEM
Bones are made of several tissues
Primarily made of collagen and
FUNCTIONS OF SKELETAL SYSTEM
SUPPORT: Hard framework that supports and anchors the
FUNCTIONS OF SKELETAL SYSTEM
SUPPORT: Hard framework that supports and anchors the
PARTS OF THE SKELETAL SYSTEM
Axial skeleton
Skull and bones that support it
Includes
PARTS OF THE SKELETAL SYSTEM
Axial skeleton
Skull and bones that support it
Includes
FEATURES OF A LONG BONE
Epiphysis: Ends of the bone.
Diaphysis: The shaft
FEATURES OF A LONG BONE
Epiphysis: Ends of the bone.
Diaphysis: The shaft
BONE DEVELOPMENT
Initial skeleton of cartilage in infants
Replaced with bone by osteoblasts
More
BONE DEVELOPMENT
Initial skeleton of cartilage in infants
Replaced with bone by osteoblasts
More
BONE STRUCTURE
Periosteum – hard outer covering
Cells for growth and repair
Compact bone
BONE STRUCTURE
Periosteum – hard outer covering
Cells for growth and repair
Compact bone
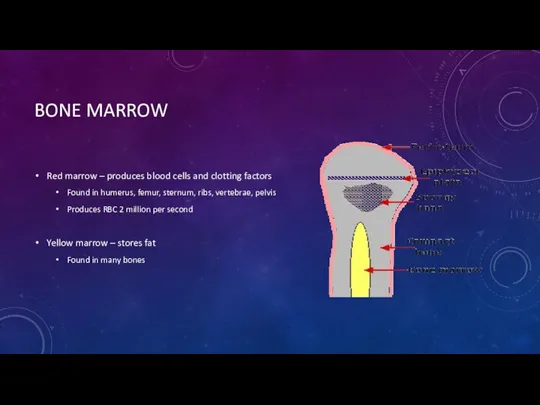
BONE MARROW
Red marrow – produces blood cells and clotting factors
Found in
BONE MARROW
Red marrow – produces blood cells and clotting factors
Found in
SKELETAL SYSTEM OF CHILD
Bone in children and toddlers is more porous
SKELETAL SYSTEM OF CHILD
Bone in children and toddlers is more porous
The periosteal sleeve is much thicker in children than in adults
The periosteal sleeve is much thicker in children than in adults
The epiphysis is an important part of the growing skeleton. It
The epiphysis is an important part of the growing skeleton. It
MICROSCOPIC ANATOMY
The epiphysis is the growing end of the long bone
MICROSCOPIC ANATOMY
The epiphysis is the growing end of the long bone
Histologically, the physis consists of a number of layers that reflect
Histologically, the physis consists of a number of layers that reflect
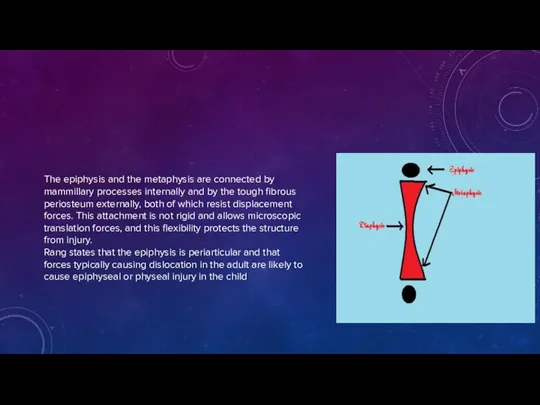
The epiphysis and the metaphysis are connected by mammillary processes internally
The epiphysis and the metaphysis are connected by mammillary processes internally
REMODELING
Remodeling of a fracture or deformity is a process that is
REMODELING
Remodeling of a fracture or deformity is a process that is
An injury to a long bone can stimulate excessive growth and
An injury to a long bone can stimulate excessive growth and
NATURAL VARIANTS
Bone in children undergoes serial changes and adaptations to achieve
NATURAL VARIANTS
Bone in children undergoes serial changes and adaptations to achieve
At birth, the sutures in the skull are unfused at the
At birth, the sutures in the skull are unfused at the
The varus and valgus alignments are believed to be dictated by
The varus and valgus alignments are believed to be dictated by
DEFECTS
Matrix deficiencies can give rise to a myriad of conditions, the
DEFECTS
Matrix deficiencies can give rise to a myriad of conditions, the

osteogenesis imperfecta,
Epiphyseal dysplasias
osteogenesis imperfecta,
Epiphyseal dysplasias

BROKEN BONES
Fracture is a break of the bone
Simple or Complex fracture
Regrowth
BROKEN BONES
Fracture is a break of the bone
Simple or Complex fracture
Regrowth
REFRENCE
https://emedicine.medscape.com/article/1899256-overview#a4
https://www.google.kz/search?q=skeletal+system+medscape&rlz=1C1ASRW_enKZ800KZ800&oq=skeletal+system+medscape&aqs=chrome..69i57j69i60.9086j0j4&sourceid=chrome&ie=UTF-8
Slide share
Physiology essentials book
http://www.innerbody.com/image/skelfov.html
REFRENCE
https://emedicine.medscape.com/article/1899256-overview#a4
https://www.google.kz/search?q=skeletal+system+medscape&rlz=1C1ASRW_enKZ800KZ800&oq=skeletal+system+medscape&aqs=chrome..69i57j69i60.9086j0j4&sourceid=chrome&ie=UTF-8
Slide share
Physiology essentials book
http://www.innerbody.com/image/skelfov.html
 Гипогонадизм. Недостаточность функций половых желез
Гипогонадизм. Недостаточность функций половых желез General gynaecology
General gynaecology Психиатрияның зерттеу қағидалары мен диагностиканың заманауи
Психиатрияның зерттеу қағидалары мен диагностиканың заманауи Деконгестанты: как выбрать оптимальный препарат
Деконгестанты: как выбрать оптимальный препарат Атеросклероз и его проявления
Атеросклероз и его проявления Лечебная гимнастика и массаж при вибрационной болезни
Лечебная гимнастика и массаж при вибрационной болезни Түбір өзектерін пломбылауға(бітеуге) арналған материалдар (силерлер).Жүйесі.Жұмсақ қатаймайтын созылымтал материалдар
Түбір өзектерін пломбылауға(бітеуге) арналған материалдар (силерлер).Жүйесі.Жұмсақ қатаймайтын созылымтал материалдар Кашель или затрудненное дыхание
Кашель или затрудненное дыхание Хроническая обструктивная болезнь легких
Хроническая обструктивная болезнь легких Клинические стоматологические материалы
Клинические стоматологические материалы Вирусные гепатиты на современном этапе
Вирусные гепатиты на современном этапе ормональные лекарственные средства, их синтетические заменители и антагонисты. Анаболические стероиды
ормональные лекарственные средства, их синтетические заменители и антагонисты. Анаболические стероиды Пищеварение. Нарушения экзокринной секреции поджелудочной железы
Пищеварение. Нарушения экзокринной секреции поджелудочной железы Қант диабеті және жүктілік
Қант диабеті және жүктілік Хирургия паразитарных заболеваний
Хирургия паразитарных заболеваний Prophylaxis of tuberculosis. (Lecture 4)
Prophylaxis of tuberculosis. (Lecture 4) Наименование вида ПАВ
Наименование вида ПАВ Ятрогении. Врачебные ошибки
Ятрогении. Врачебные ошибки Организация и проведение медицинской экспертизы трудоспособности населения
Организация и проведение медицинской экспертизы трудоспособности населения Лучевое исследование костей и суставов
Лучевое исследование костей и суставов Мерез. Эпидемиологиясы
Мерез. Эпидемиологиясы Новые вакцины: рекомбинантные, синтетические
Новые вакцины: рекомбинантные, синтетические Клинико-психологическая характеристика акалькулии и дискалькулии детского возраста
Клинико-психологическая характеристика акалькулии и дискалькулии детского возраста الأسبوع الثالث و الرابع
الأسبوع الثالث و الرابع Физиология беременности
Физиология беременности Электрокардиография. История ЭКГ
Электрокардиография. История ЭКГ Мышцы нижней конечности
Мышцы нижней конечности Выделение. Кровообращение почки
Выделение. Кровообращение почки