- Prophylaxis of tuberculosis. (Lecture 4)

Содержание
- 2. Prophylaxis of tuberculosis: Social, Infectious control, Sanitary, BCG vaccination, Preventive Chemotherapy
- 3. Social prophylaxis Principles of prophylactic orientation, state character, toll-free medi-care are fixed in basis of social
- 4. A social prophylaxis is directed on: making healthy of environment; it is an increase of financial
- 5. BCG VACCINE attenuated (virulence-reduced) live bovine tuberculosis bacillus, Mycobacterium bovis, that has lost its virulence in
- 6. Because the living bacilli evolve to make the best use of available nutrients, they become less
- 7. Microscopic image of the Calmette-Guérin bacillus, Ziehl–Neelsen stain, magnification:1,000
- 8. The bacille Calmette-Guérin (BCG) vaccine has existed for 80 years and is one of the most
- 9. The biological interaction between MTB and the human host is complex and only partially understood. Recent
- 10. RECOMBINANT BCG VACCINE
- 11. is used for active specific prophylaxis of tuberculosis – dry for intracutaneoud transfusion. These are live
- 12. BCG-M vaccine is manufactured in a half dose (0,5 mg in an ampulla, which contains 20
- 13. BCG-STRAINS There have been many (WHO estimated 40 or more in 1999) manufacturers of BCG around
- 14. when the vaccine had been administered in infancy, as is recommended by WHO and widely practiced,
- 15. VACCINATION PROCEDURE BCG is given as a single intradermal injection at the insertion of the deltoid
- 16. THE RULES OF TRANSFUSION The dry vaccine (1 ampulla ) is dissolved in 2 ml of
- 17. IN 4-6 WEEKS pustule
- 18. IN 6-8 WEEKS crust
- 19. IN 2-4 MONTHS cicatrix
- 20. BCG IN ADOLESCENTS AND ADULTS There is no evidence that revaccination with BCG affords any additional
- 21. BCG IN HIV-INFECTED NEWBORNS In children who are known to be HIV-infected, BCG vaccine should not
- 22. COMPLICATIONS (BCG-RELATED DISEASES) CLASSIFICATION (WHO, 1984) Local (the most frequent) – cold abscess, ulcer, regional lymphadenitis.
- 23. The term "BCG lymphadenitis" is usually coined when ipsi-lateral axillary, supraclavicular or lower cervical lymph node
- 24. There are two forms of BCG lymphadenitis. The nonsuppurative form (simple form) is characterised by a
- 25. Overlying skin changes is universal, with erythema, edema, increased pigmentation and pustule formation. If left untreated,
- 26. BCG LYMPHADENITIS Three treatment options have been described for BCG lymphadenitis. Antibiotic Therapy Several antibiotics (e.g.
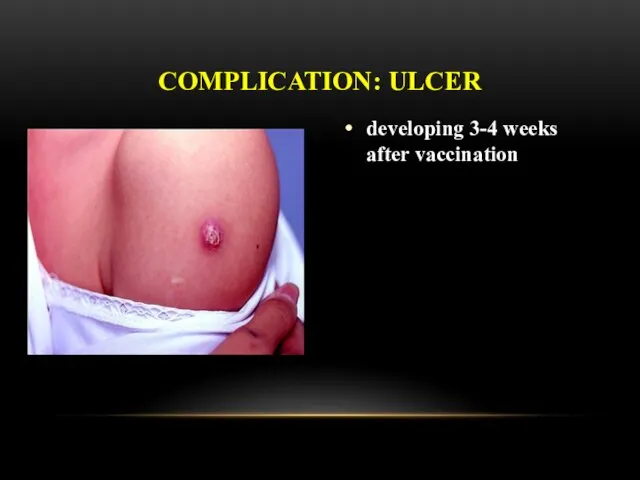
- 27. developing 3-4 weeks after vaccination COMPLICATION: ULCER
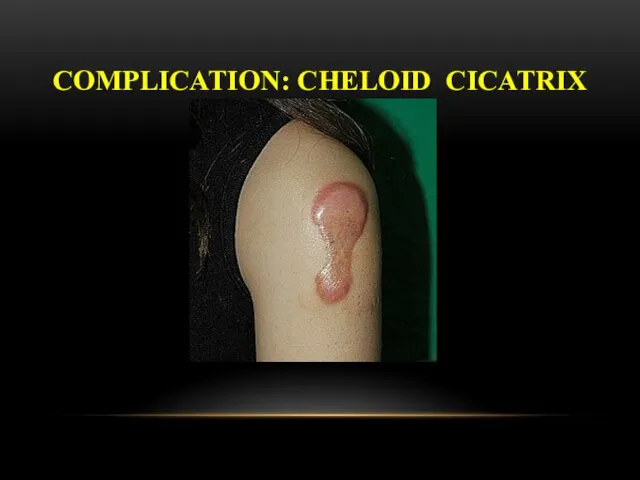
- 28. COMPLICATION: CHELOID CICATRIX
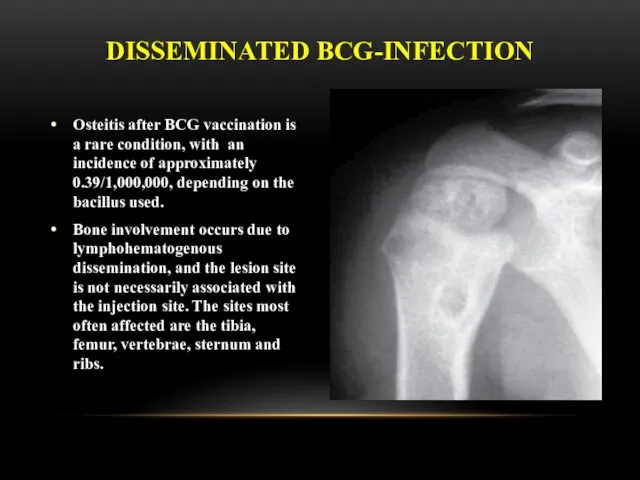
- 29. Osteitis after BCG vaccination is a rare condition, with an incidence of approximately 0.39/1,000,000, depending on
- 30. Clinical manifestations usually occur 18 months after vaccination, this interval can range from a few months
- 31. GENERALIZED BCG-INFECTION Generalized infection due to BCG vaccination has also been reported, sometimes being fatal. Systemic
- 32. LATENT TB INFECTION Latent tuberculosis infection (LTBI) is defined as a state of persistent immune response
- 33. PREVENTIVE CHEMOTHERAPY Guidelines on the management of latent tuberculosis infection were developed in accordance to the
- 34. PREVENTIVE CHEMOTHERAPY Systematic testing and treatment of LTBI should be performed in people living with HIV,
- 35. PREVENTIVE CHEMOTHERAPY Systematic testing and treatment of LTBI should be considered for prisoners, health-care workers, immigrants
- 36. PREVENTIVE CHEMOTHERAPY Systematic testing for LTBI is not recommended in people with diabetes, people with harmful
- 37. PREVENTIVE CHEMOTHERAPY Individuals should be asked about symptoms of TB before being tested for LTBI. Chest
- 38. PREVENTIVE CHEMOTHERAPY Either TST or IGRA can be used to test for LTBI in high-income and
- 39. FOR RESOURCE-LIMITED COUNTRIES AND OTHER MIDDLE-INCOME COUNTRIES THAT DO NOT BELONG TO THE ABOVE CATEGORY People
- 40. PREVENTIVE CHEMOTHERAPY Treatment options recommended for LTBI include: 6-month isoniazid, or 9-month isoniazid, or 3-month regimen
- 41. MDR-TB CASES Strict clinical observation and close monitoring for the development of active TB disease among
- 42. RISK OF DRUG RESISTANCE FOLLOWING LTBI TREATMENT A systematic review was conducted to determine whether LTBI
- 43. INFECTION CONTROL OF TUBERCULOSIS
- 44. EMPHASISE THAT TRANSMISSION IS NOT ONE-WAY AND DOES NOT DISCRIMINATE! PATIENTS CAN TRANSMIT TO WORKERS, VISITORS
- 45. HIERARCHY OF INFECTION PREVENTION & CONTROL Administrative controls Reduce risk of exposure, infection and disease thru
- 46. ADMINISTRATIVE CONTROLS Develop and implement written policies and protocols to ensure: Rapid identification of TB cases
- 47. ENVIRONMENTAL CONTROLS: VENTILATION AND AIR FLOW Ventilation is the movement of air Should be done in
- 48. EVIDENCE FROM PERU Open windows and doors produced 6x greater air exchanges than mechanical ventilation and
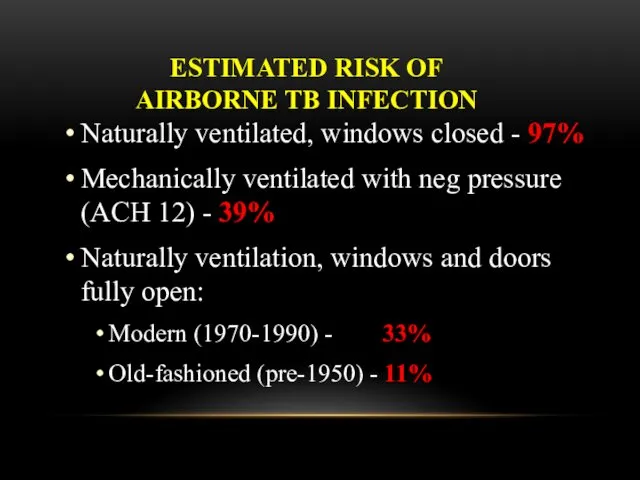
- 49. ESTIMATED RISK OF AIRBORNE TB INFECTION Naturally ventilated, windows closed - 97% Mechanically ventilated with neg
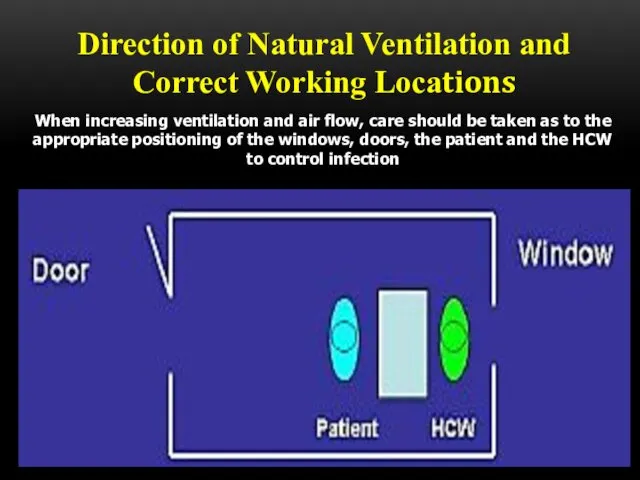
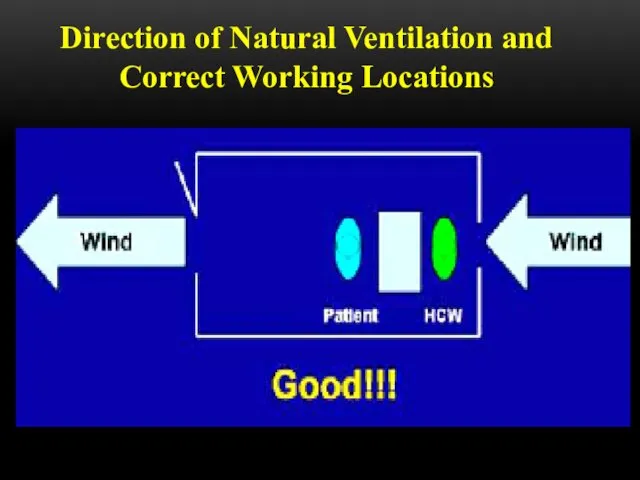
- 50. Direction of Natural Ventilation and Correct Working Locations When increasing ventilation and air flow, care should
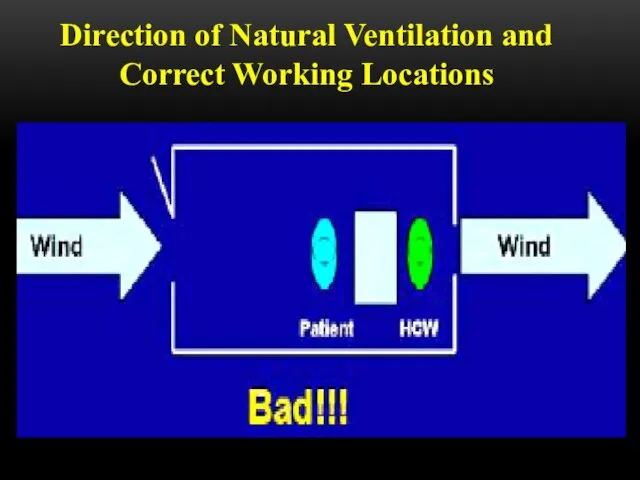
- 51. Direction of Natural Ventilation and Correct Working Locations
- 52. Direction of Natural Ventilation and Correct Working Locations
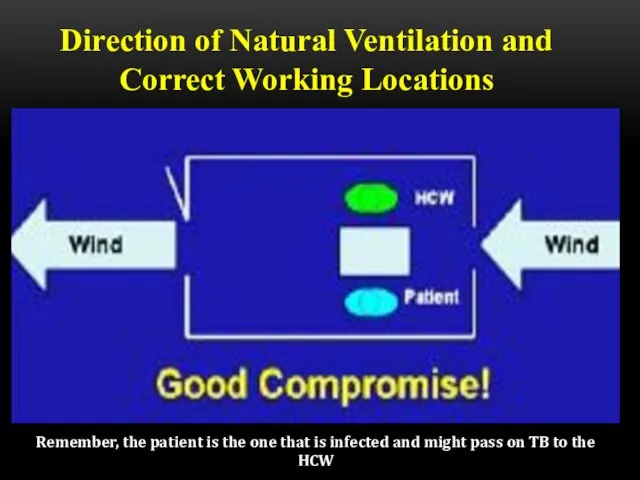
- 53. Direction of Natural Ventilation and Correct Working Locations Remember, the patient is the one that is
- 55. ENVIRONMENTAL CONTROLS Ultraviolet Light HEPA (high efficiency particulate air) filters Both indirect ultraviolet irradiation of air
- 56. PERSONAL RESPIRATORY PROTECTION Respirators: Can protect HCWs Should be encouraged in high-risk settings May be unavailable
- 57. N95 RESPIRATOR DOS AND DON’TS
- 58. Be sure your respirator is properly fitted! It should fit snugly at nose and chin
- 59. Note poor fit at the bridge of nose Note poor fit at the chin Respirator should
- 60. High efficiency particulate air (HEPA) filters HEPA filters or absolute filters are those able to remove
- 61. The use of HEPA filters and/or UV light is strongly recommended for rooms where the following
- 62. HEPA filters are used: • To purify the exhaustion of air of contaminated environments • To
- 63. DON’T FORGET TO WEAR IT! Remember, respirators and masks don’t do you any good if kept
- 65. Скачать презентацию
Prophylaxis of tuberculosis:
Social,
Infectious control,
Sanitary,
BCG vaccination,
Preventive Chemotherapy
Prophylaxis of tuberculosis:
Social,
Infectious control,
Sanitary,
BCG vaccination,
Preventive Chemotherapy
Social prophylaxis
Principles of prophylactic orientation, state character, toll-free medi-care are fixed
Social prophylaxis
Principles of prophylactic orientation, state character, toll-free medi-care are fixed
A social prophylaxis is directed on:
making healthy of environment;
it is
A social prophylaxis is directed on:
making healthy of environment;
it is
BCG VACCINE
attenuated (virulence-reduced) live bovine tuberculosis bacillus, Mycobacterium bovis, that has
BCG VACCINE
attenuated (virulence-reduced) live bovine tuberculosis bacillus, Mycobacterium bovis, that has
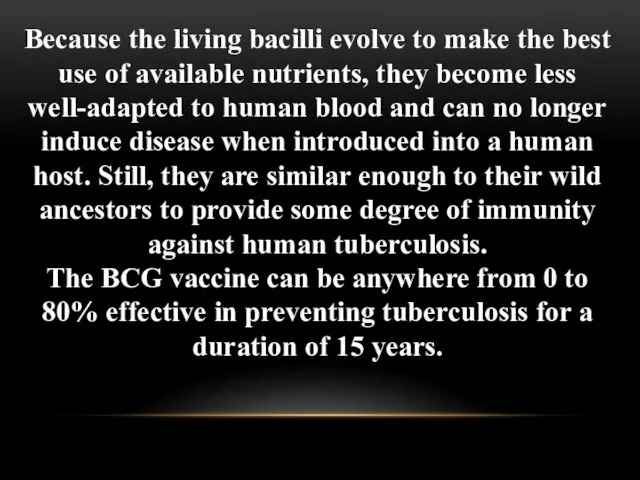
Because the living bacilli evolve to make the best use of
Because the living bacilli evolve to make the best use of
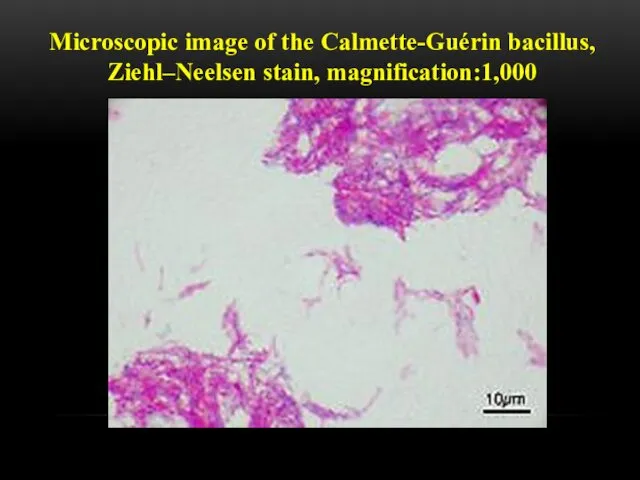
Microscopic image of the Calmette-Guérin bacillus, Ziehl–Neelsen stain, magnification:1,000
Microscopic image of the Calmette-Guérin bacillus, Ziehl–Neelsen stain, magnification:1,000
The bacille Calmette-Guérin (BCG) vaccine has existed for 80 years and
The bacille Calmette-Guérin (BCG) vaccine has existed for 80 years and
The biological interaction between MTB and the human host is complex
The biological interaction between MTB and the human host is complex
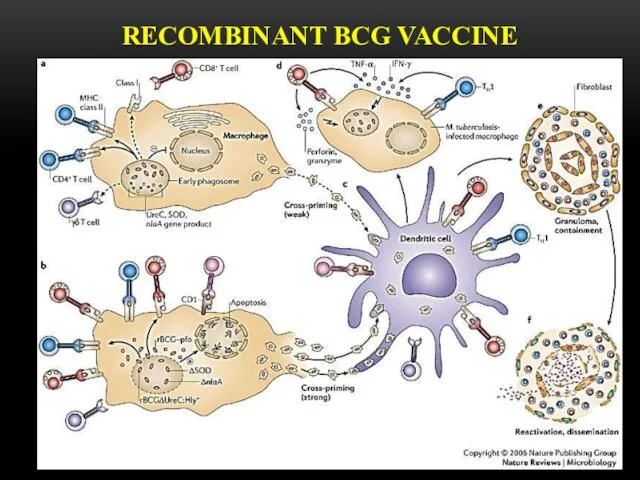
RECOMBINANT BCG VACCINE
RECOMBINANT BCG VACCINE
is used for active specific prophylaxis of tuberculosis – dry for
is used for active specific prophylaxis of tuberculosis – dry for
BCG-M vaccine
is manufactured in a half dose (0,5 mg
BCG-M vaccine
is manufactured in a half dose (0,5 mg
BCG-STRAINS
There have been many (WHO estimated 40 or more in 1999)
BCG-STRAINS
There have been many (WHO estimated 40 or more in 1999)
when the vaccine had been administered in infancy, as is recommended
when the vaccine had been administered in infancy, as is recommended
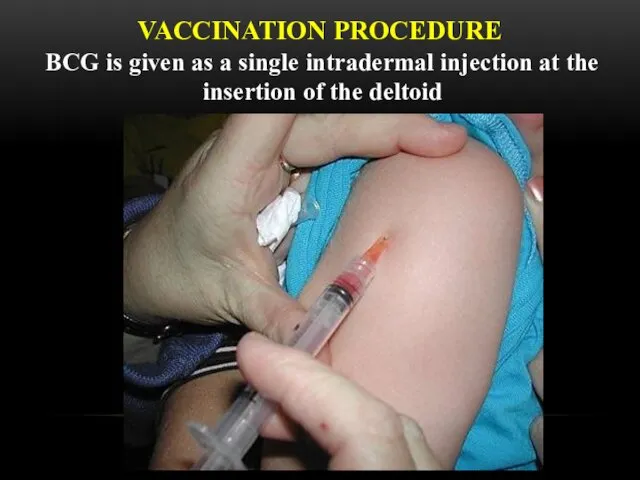
VACCINATION PROCEDURE
BCG is given as a single intradermal injection at the
VACCINATION PROCEDURE
BCG is given as a single intradermal injection at the
THE RULES OF TRANSFUSION
The dry vaccine (1 ampulla )
THE RULES OF TRANSFUSION
The dry vaccine (1 ampulla )
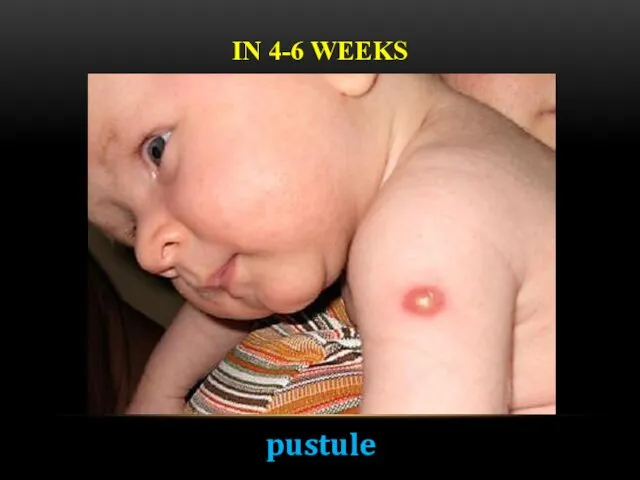
IN 4-6 WEEKS
pustule
IN 4-6 WEEKS
pustule

IN 6-8 WEEKS
crust
IN 6-8 WEEKS
crust
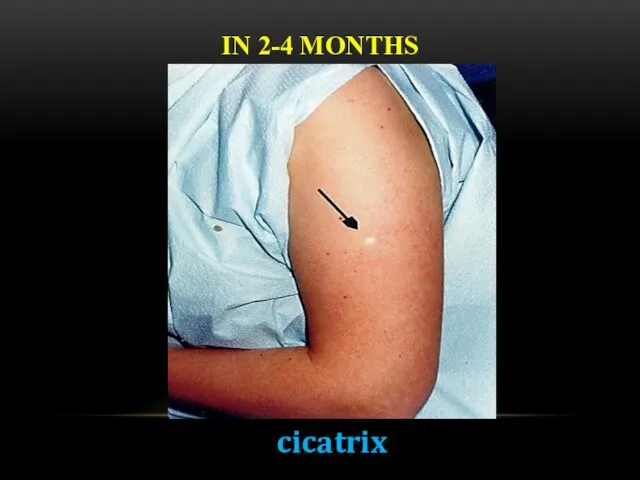
IN 2-4 MONTHS
cicatrix
IN 2-4 MONTHS
cicatrix
BCG IN ADOLESCENTS AND ADULTS
There is no evidence that revaccination with
BCG IN ADOLESCENTS AND ADULTS
There is no evidence that revaccination with
BCG IN HIV-INFECTED NEWBORNS
In children who are known to be HIV-infected,
BCG IN HIV-INFECTED NEWBORNS
In children who are known to be HIV-infected,
COMPLICATIONS (BCG-RELATED DISEASES) CLASSIFICATION (WHO, 1984)
Local (the most frequent) –
COMPLICATIONS (BCG-RELATED DISEASES) CLASSIFICATION (WHO, 1984)
Local (the most frequent) –
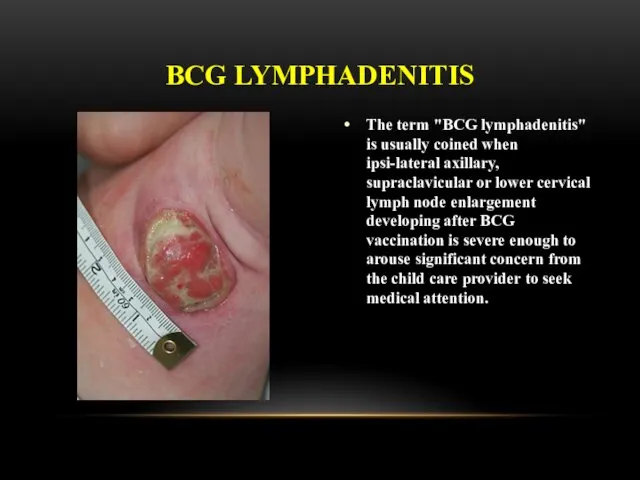
The term "BCG lymphadenitis" is usually coined when ipsi-lateral axillary, supraclavicular
The term "BCG lymphadenitis" is usually coined when ipsi-lateral axillary, supraclavicular
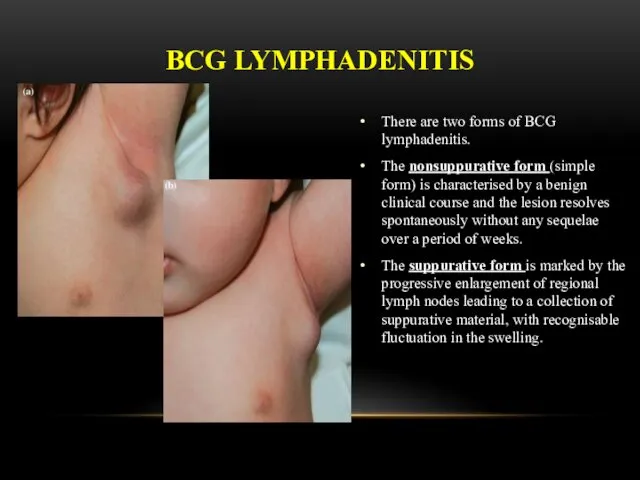
There are two forms of BCG lymphadenitis.
The nonsuppurative form (simple form)
There are two forms of BCG lymphadenitis.
The nonsuppurative form (simple form)
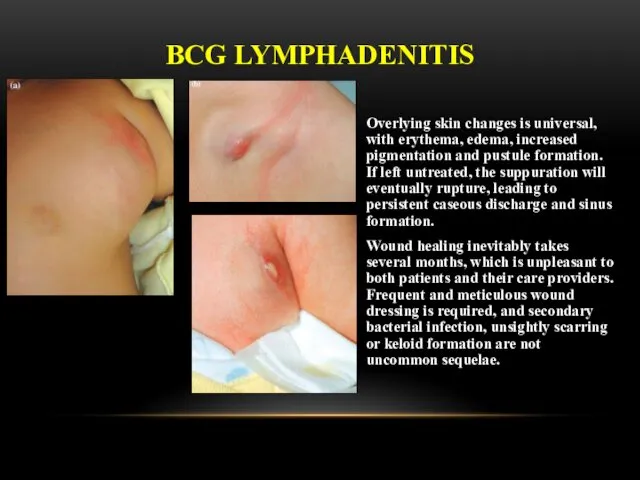
Overlying skin changes is universal, with erythema, edema, increased pigmentation and
Overlying skin changes is universal, with erythema, edema, increased pigmentation and
BCG LYMPHADENITIS
Three treatment options have been described for BCG lymphadenitis.
Antibiotic Therapy
Several
BCG LYMPHADENITIS
Three treatment options have been described for BCG lymphadenitis.
Antibiotic Therapy
Several
developing 3-4 weeks after vaccination
COMPLICATION: ULCER
developing 3-4 weeks after vaccination
COMPLICATION: ULCER
COMPLICATION: CHELOID CICATRIX
COMPLICATION: CHELOID CICATRIX
Osteitis after BCG vaccination is a rare condition, with an incidence
Osteitis after BCG vaccination is a rare condition, with an incidence
Clinical manifestations usually occur 18 months after vaccination, this interval
Clinical manifestations usually occur 18 months after vaccination, this interval
GENERALIZED BCG-INFECTION
Generalized infection due to BCG vaccination has also been reported,
GENERALIZED BCG-INFECTION
Generalized infection due to BCG vaccination has also been reported,
LATENT TB INFECTION
Latent tuberculosis infection (LTBI) is defined as a state
LATENT TB INFECTION
Latent tuberculosis infection (LTBI) is defined as a state
PREVENTIVE CHEMOTHERAPY
Guidelines on the management of latent tuberculosis infection were developed
PREVENTIVE CHEMOTHERAPY
Guidelines on the management of latent tuberculosis infection were developed
PREVENTIVE CHEMOTHERAPY
Systematic testing and treatment of LTBI should be performed in
PREVENTIVE CHEMOTHERAPY
Systematic testing and treatment of LTBI should be performed in
PREVENTIVE CHEMOTHERAPY
Systematic testing and treatment of LTBI should be considered for
PREVENTIVE CHEMOTHERAPY
Systematic testing and treatment of LTBI should be considered for
PREVENTIVE CHEMOTHERAPY
Systematic testing for LTBI is not recommended in people with
PREVENTIVE CHEMOTHERAPY
Systematic testing for LTBI is not recommended in people with
PREVENTIVE CHEMOTHERAPY
Individuals should be asked about symptoms of TB before being
PREVENTIVE CHEMOTHERAPY
Individuals should be asked about symptoms of TB before being
PREVENTIVE CHEMOTHERAPY
Either TST or IGRA can be used to test for
PREVENTIVE CHEMOTHERAPY
Either TST or IGRA can be used to test for
FOR RESOURCE-LIMITED COUNTRIES AND OTHER MIDDLE-INCOME COUNTRIES THAT DO NOT BELONG
FOR RESOURCE-LIMITED COUNTRIES AND OTHER MIDDLE-INCOME COUNTRIES THAT DO NOT BELONG
PREVENTIVE CHEMOTHERAPY
Treatment options recommended for LTBI include:
6-month isoniazid, or
9-month
PREVENTIVE CHEMOTHERAPY
Treatment options recommended for LTBI include:
6-month isoniazid, or
9-month
MDR-TB CASES
Strict clinical observation and close monitoring for the development of
MDR-TB CASES
Strict clinical observation and close monitoring for the development of
RISK OF DRUG RESISTANCE FOLLOWING LTBI TREATMENT
A systematic review was conducted
RISK OF DRUG RESISTANCE FOLLOWING LTBI TREATMENT
A systematic review was conducted
INFECTION CONTROL OF TUBERCULOSIS
INFECTION CONTROL OF TUBERCULOSIS
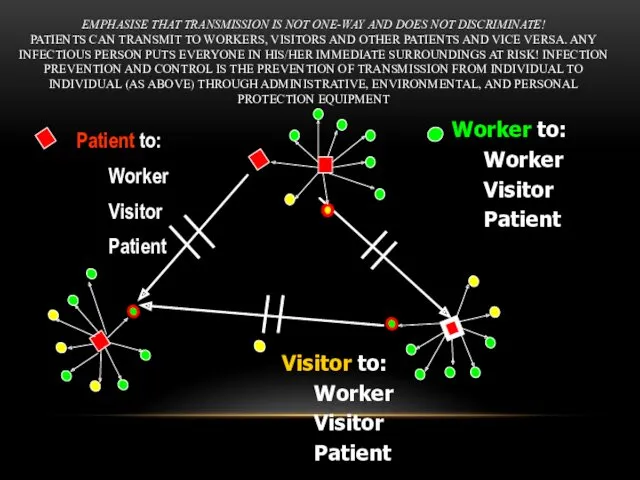
EMPHASISE THAT TRANSMISSION IS NOT ONE-WAY AND DOES NOT DISCRIMINATE!
PATIENTS CAN
EMPHASISE THAT TRANSMISSION IS NOT ONE-WAY AND DOES NOT DISCRIMINATE! PATIENTS CAN
HIERARCHY OF
INFECTION PREVENTION & CONTROL
Administrative controls
Reduce risk of exposure, infection
HIERARCHY OF
INFECTION PREVENTION & CONTROL
Administrative controls
Reduce risk of exposure, infection
ADMINISTRATIVE CONTROLS
Develop and implement written policies and protocols to ensure:
Rapid identification
ADMINISTRATIVE CONTROLS
Develop and implement written policies and protocols to ensure:
Rapid identification
ENVIRONMENTAL CONTROLS:
VENTILATION AND AIR FLOW
Ventilation is the movement of air
Should
ENVIRONMENTAL CONTROLS:
VENTILATION AND AIR FLOW
Ventilation is the movement of air
Should
EVIDENCE FROM PERU
Open windows and doors produced 6x greater air exchanges
EVIDENCE FROM PERU
Open windows and doors produced 6x greater air exchanges
ESTIMATED RISK OF
AIRBORNE TB INFECTION
Naturally ventilated, windows closed - 97%
Mechanically
ESTIMATED RISK OF
AIRBORNE TB INFECTION
Naturally ventilated, windows closed - 97%
Mechanically
Direction of Natural Ventilation and Correct Working Locations
When increasing ventilation
Direction of Natural Ventilation and Correct Working Locations
When increasing ventilation
Direction of Natural Ventilation and Correct Working Locations
Direction of Natural Ventilation and Correct Working Locations
Direction of Natural Ventilation and Correct Working Locations
Direction of Natural Ventilation and Correct Working Locations
Direction of Natural Ventilation and Correct Working Locations
Remember, the patient is
Direction of Natural Ventilation and Correct Working Locations
Remember, the patient is


ENVIRONMENTAL CONTROLS
Ultraviolet Light
HEPA (high efficiency particulate air) filters
Both indirect ultraviolet irradiation
ENVIRONMENTAL CONTROLS
Ultraviolet Light
HEPA (high efficiency particulate air) filters
Both indirect ultraviolet irradiation
PERSONAL RESPIRATORY PROTECTION
Respirators:
Can protect HCWs
Should be encouraged in high-risk settings
May be
PERSONAL RESPIRATORY PROTECTION
Respirators:
Can protect HCWs
Should be encouraged in high-risk settings
May be
N95 RESPIRATOR DOS AND DON’TS
N95 RESPIRATOR DOS AND DON’TS

Be sure your respirator is properly fitted!
It should fit snugly
Be sure your respirator is properly fitted!
It should fit snugly
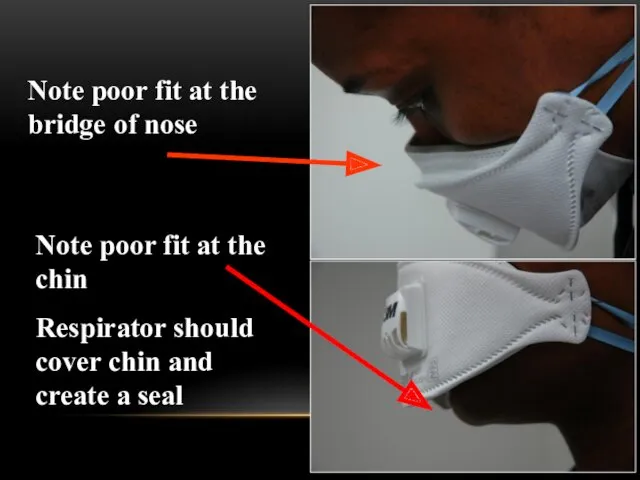
Note poor fit at the bridge of nose
Note poor fit at
Note poor fit at the bridge of nose
Note poor fit at
High efficiency particulate air (HEPA) filters
HEPA filters or absolute filters
High efficiency particulate air (HEPA) filters
HEPA filters or absolute filters
The use of HEPA filters and/or UV light is strongly recommended
The use of HEPA filters and/or UV light is strongly recommended
HEPA filters are used:
• To purify the exhaustion of air of
HEPA filters are used:
• To purify the exhaustion of air of

DON’T FORGET TO WEAR IT!
Remember, respirators and masks don’t do
DON’T FORGET TO WEAR IT!
Remember, respirators and masks don’t do
 Гигиена аптечные учреждений
Гигиена аптечные учреждений Өзектілігі Жүрек қантамыр аурулары, атап айтсақ миокард инфаркты, стенокардия, инсульт, әлем бойынша өлім көрсеткіші жағынан
Өзектілігі Жүрек қантамыр аурулары, атап айтсақ миокард инфаркты, стенокардия, инсульт, әлем бойынша өлім көрсеткіші жағынан Вегето-сосудистая дистония: диагностика, клиника
Вегето-сосудистая дистония: диагностика, клиника Спецификалық алдын алу
Спецификалық алдын алу Общие анестетики
Общие анестетики Бронхиальная астма
Бронхиальная астма ВИЧ-инфекция, остановить эпидемию
ВИЧ-инфекция, остановить эпидемию Средства, угнетающие ЦНС
Средства, угнетающие ЦНС Плазменное звено системы гемостаза
Плазменное звено системы гемостаза Болезнь Бюргера (облитерирующий тромбоангиит)
Болезнь Бюргера (облитерирующий тромбоангиит) Новообразования женских половых органов
Новообразования женских половых органов Патофизиология опухолевого роста
Патофизиология опухолевого роста Заболевания суставов
Заболевания суставов Средства, влияющие на эфферентную нервную систему: Адренергические ЛС
Средства, влияющие на эфферентную нервную систему: Адренергические ЛС Ерік. Балада ерікті дамыту жолдары
Ерік. Балада ерікті дамыту жолдары Растения, кровоостанавливающего действия
Растения, кровоостанавливающего действия Черепно-мозговая травма
Черепно-мозговая травма Острый мастит
Острый мастит Антисептика. Этапы развития асептики и антисептики
Антисептика. Этапы развития асептики и антисептики Переломы верхней челюсти
Переломы верхней челюсти Абдоминальная патология
Абдоминальная патология Шизофрения. Kahlbaum (1828-1899)
Шизофрения. Kahlbaum (1828-1899) Операция Негейбауэра-Лефора
Операция Негейбауэра-Лефора Эстрогендерді қабылдау мен әйелдерде эдометрийдің қатерлі ісігінің дамуы арасындағы байланыс
Эстрогендерді қабылдау мен әйелдерде эдометрийдің қатерлі ісігінің дамуы арасындағы байланыс Печень. Участие печени в процессах гомеостаза/гомеокинеза организма
Печень. Участие печени в процессах гомеостаза/гомеокинеза организма Кодекс республики Казахстан о здоровье народа и системе здравоохранения
Кодекс республики Казахстан о здоровье народа и системе здравоохранения Инфектология. Понятие об инфекции. Патогенность и вирулентность бактерий
Инфектология. Понятие об инфекции. Патогенность и вирулентность бактерий ДНҚ репарациясы
ДНҚ репарациясы