- Specific Hernia Types

Содержание
- 2. Inguinal Hernia
- 3. Is the most common hernia in men & women but much more common in men. There
- 4. Basic anatomy of inguinal canal: Superficial inguinal ring: Triangular opening in external oblique aponeurosis 1.25 cm
- 5. Inguinal canal: In infant deep & superficial inguinal ring are almost superimposed, but in adult it
- 7. Boundaries of the canal: Anteriorly: Ext. oblique aponeurosis conjoined muscle laterally. Posteriorly: Transversalis fascia, conjoined tendon
- 8. Contents of the inguinal canal (spermatic canal): * Three layers of fascia: (1) External spermatic fascia
- 9. * Three nerves: (1) ilio-inguinal nerve. (2) iliohypogastric. (3) genital branch of the genitofemoral N .
- 10. In female the inguinal canal contains: Round ligament of the uterus. ilio-inguinal nerve. Genital branch of
- 11. Types of Inguinal Hernia: 1- Indirect inguinal hernia (LATERAL) (OBLIQUE) 2- Direct inguinal hernia ( MEDIAL)
- 12. Diagnosis Of An Inguinal Hernia In most cases, the diagnosis of an inguinal hernia is simple
- 13. With the patient lying down, Once reduced, surgeon identifies the bony landmarks of the anterior superior
- 14. Investigations For Inguinal Hernia Most cases require no diagnostic tests, But: US. CT scan. MRI scan
- 15. Management of Inguinal Hernia It is safe to recommend no active treatment in cases of early,
- 16. Surgical trusses are not recommended but may be required for occasional patients who refuse any form
- 17. Operations for inguinal hernia A: Herniotomy. & B: Repair (herniorrhaphy): I: Open repair: 1- Bassini, Shouldice,
- 18. Laparoscopic Herniorrhaphy Of Inguinal Hernia
- 19. Trans-abdominal approach (TAPP): Establishes a pneumoperitoneum & place a synthetic mesh preperitoneally by dissecting the peritoneum
- 21. Emergency inguinal hernia surgery Ninety-five per cent of inguinal hernia patients present at clinics & only
- 22. Complications of inguinal hernia surgery Early: pain, bleeding, urinary retention, anaesthetic related. Medium: seroma, wound infection.
- 23. Femoral Hernia
- 24. Less common than inguinal hernia. It is more common in females than in males. Easily missed
- 26. Surgical Anatomy:
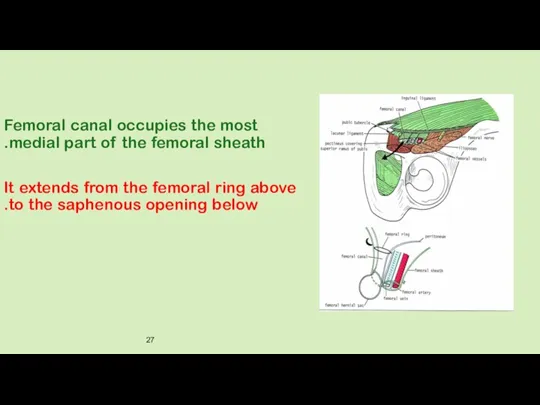
- 27. Femoral canal occupies the most medial part of the femoral sheath. It extends from the femoral
- 28. It is 1.25cm long & 1.25cm wide at its base. Femoral canal contains: Fat. Lymphatic vessels.
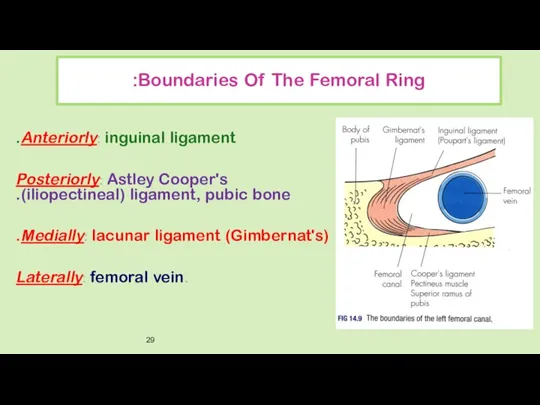
- 29. Boundaries Of The Femoral Ring: Anteriorly: inguinal ligament. Posteriorly: Astley Cooper's (iliopectineal) ligament, pubic bone. Medially:
- 30. Diagnosis : Diagnostic error is common & often leads to delay in diagnosis & treatment. Hernia
- 31. It may only be 1–2 cm in size & can easily be mistaken for a lymph
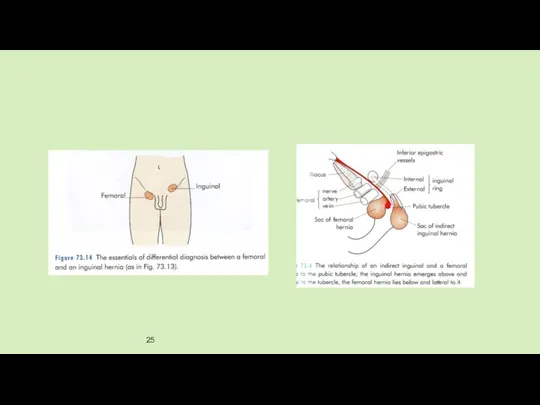
- 32. Differential Diagnosis: Direct inguinal hernia. Lymph node. Saphena varix. Femoral artery aneurysm. Psoas abscess. Rupture of
- 33. Investigations In routine cases, no specific investigations are required. US CT plain x-ray: small bowel obstruction.
- 34. Treatment: There is no alternative to surgery for femoral hernia. it is wise to treat such
- 35. 1. Low approach (Lockwood): Simplest operation but only suitable when there is no risk of bowel
- 36. 2. Inguinal approach (Lotheissen's operation): * Through an inguinal incision. * A femoral hernia lies immediately
- 37. 3. High approach (McEvedy): * This more complex operation is ideal in the emergency situation where
- 38. * Femoral hernia is reduced & sac opened to allow careful inspection of the bowel. *
- 39. * Laparoscopic approach Both the TEP & TAPP approaches can be used for femoral hernia &
- 41. Скачать презентацию
Inguinal Hernia
Inguinal Hernia
Is the most common hernia in men & women but much
Is the most common hernia in men & women but much
Basic anatomy of inguinal canal:
Superficial inguinal ring:
Triangular opening in external
Basic anatomy of inguinal canal:
Superficial inguinal ring:
Triangular opening in external
Inguinal canal:
In infant deep & superficial inguinal ring are almost
Inguinal canal:
In infant deep & superficial inguinal ring are almost
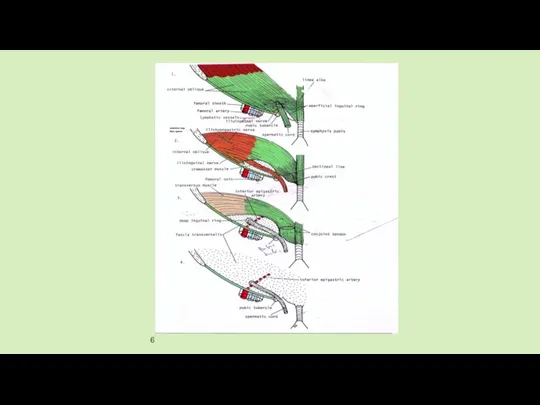
Boundaries of the canal:
Anteriorly: Ext. oblique aponeurosis conjoined muscle laterally.
Posteriorly: Transversalis
Boundaries of the canal:
Anteriorly: Ext. oblique aponeurosis conjoined muscle laterally.
Posteriorly: Transversalis
Contents of the inguinal canal (spermatic canal):
* Three layers of fascia:
Contents of the inguinal canal (spermatic canal):
* Three layers of fascia:
* Three nerves:
(1) ilio-inguinal nerve.
(2) iliohypogastric.
* Three nerves:
(1) ilio-inguinal nerve.
(2) iliohypogastric.
In female the inguinal canal contains:
Round ligament of the uterus.
ilio-inguinal
In female the inguinal canal contains:
Round ligament of the uterus.
ilio-inguinal
Types of Inguinal Hernia:
1- Indirect inguinal hernia (LATERAL) (OBLIQUE)
2- Direct inguinal
Types of Inguinal Hernia:
1- Indirect inguinal hernia (LATERAL) (OBLIQUE)
2- Direct inguinal
Diagnosis Of An Inguinal Hernia
In most cases, the diagnosis of an
Diagnosis Of An Inguinal Hernia
In most cases, the diagnosis of an
With the patient lying down, Once reduced, surgeon identifies the bony
With the patient lying down, Once reduced, surgeon identifies the bony
Investigations For Inguinal Hernia
Most cases require no diagnostic tests, But:
US.
CT scan.
Investigations For Inguinal Hernia
Most cases require no diagnostic tests, But:
US.
CT scan.
Management of Inguinal Hernia
It is safe to recommend no active treatment
Management of Inguinal Hernia
It is safe to recommend no active treatment
Surgical trusses are not recommended but may be required for occasional
Surgical trusses are not recommended but may be required for occasional
Operations for inguinal hernia
A: Herniotomy. & B: Repair (herniorrhaphy):
I:
Operations for inguinal hernia
A: Herniotomy. & B: Repair (herniorrhaphy):
I:
Laparoscopic Herniorrhaphy Of Inguinal Hernia
Laparoscopic Herniorrhaphy Of Inguinal Hernia
Trans-abdominal approach (TAPP):
Establishes a pneumoperitoneum & place a synthetic mesh preperitoneally
Establishes a pneumoperitoneum & place a synthetic mesh preperitoneally
Emergency inguinal hernia surgery
Ninety-five per cent of inguinal hernia patients present
Emergency inguinal hernia surgery
Ninety-five per cent of inguinal hernia patients present
Complications of inguinal hernia surgery
Early: pain, bleeding, urinary retention, anaesthetic related.
Medium:
Complications of inguinal hernia surgery
Early: pain, bleeding, urinary retention, anaesthetic related.
Medium:
Femoral Hernia
Femoral Hernia
Less common than inguinal hernia.
It is more common in females than
Less common than inguinal hernia.
It is more common in females than
Surgical Anatomy:
Surgical Anatomy:
Femoral canal occupies the most medial part of the femoral sheath.
Femoral canal occupies the most medial part of the femoral sheath.
It is 1.25cm long & 1.25cm wide at its base.
Femoral canal
It is 1.25cm long & 1.25cm wide at its base.
Femoral canal
Boundaries Of The Femoral Ring:
Anteriorly: inguinal ligament.
Posteriorly: Astley Cooper's (iliopectineal)
Boundaries Of The Femoral Ring:
Anteriorly: inguinal ligament.
Posteriorly: Astley Cooper's (iliopectineal)
Diagnosis :
Diagnostic error is common & often leads to delay in
Diagnosis :
Diagnostic error is common & often leads to delay in
It may only be 1–2 cm in size & can easily
It may only be 1–2 cm in size & can easily
Differential Diagnosis:
Direct inguinal hernia.
Lymph node.
Saphena varix.
Femoral artery aneurysm.
Psoas abscess.
Rupture of
Differential Diagnosis:
Direct inguinal hernia.
Lymph node.
Saphena varix.
Femoral artery aneurysm.
Psoas abscess.
Rupture of
Investigations
In routine cases, no specific investigations are required.
US
CT
plain
Investigations
In routine cases, no specific investigations are required.
US
CT
plain
Treatment:
There is no alternative to surgery for femoral hernia.
it is wise
Treatment:
There is no alternative to surgery for femoral hernia.
it is wise
1. Low approach (Lockwood):
Simplest operation but only suitable when there is
1. Low approach (Lockwood):
Simplest operation but only suitable when there is
2. Inguinal approach (Lotheissen's operation):
* Through an inguinal incision.
* A femoral
2. Inguinal approach (Lotheissen's operation):
* Through an inguinal incision.
* A femoral
3. High approach (McEvedy):
* This more complex operation is ideal
3. High approach (McEvedy):
* This more complex operation is ideal
* Femoral hernia is reduced & sac opened to allow careful
* Laparoscopic approach
Both the TEP & TAPP approaches can be used
* Laparoscopic approach
Both the TEP & TAPP approaches can be used
 Экзогенді-органикалық және соматогенді бұзылыстар
Экзогенді-органикалық және соматогенді бұзылыстар Жұқпалы емес аурулар эпидемиологиясының өзекті мәселелер
Жұқпалы емес аурулар эпидемиологиясының өзекті мәселелер Обратимое повреждение клеток и тканей. Внеклеточные изменения
Обратимое повреждение клеток и тканей. Внеклеточные изменения Мороженое
Мороженое Одонтогенный гайморит
Одонтогенный гайморит Скелет. Кости нижней конечности
Скелет. Кости нижней конечности Цитостатические препараты
Цитостатические препараты Узелковый периартериит
Узелковый периартериит Семиотика заболеваний органов дыхания
Семиотика заболеваний органов дыхания Медико-этические и социально-правовые аспекты современной трансплантологии
Медико-этические и социально-правовые аспекты современной трансплантологии Значение и состав пищи
Значение и состав пищи Операции на желудке
Операции на желудке Эндокринология. Йододефицитные заболевания. (Лекция 4)
Эндокринология. Йододефицитные заболевания. (Лекция 4) ОЖЖ-дегі ерікті қимылдарды қамтамасыз ететін нейрофизиологиялық үрдістер
ОЖЖ-дегі ерікті қимылдарды қамтамасыз ететін нейрофизиологиялық үрдістер Острая и хроническая специфическая инфекция
Острая и хроническая специфическая инфекция Кровь и остальные компоненты внутренней среды организма
Кровь и остальные компоненты внутренней среды организма Современные молекулярно-прикладные подходы к конструированию корректоров нарушений микробной экологии человека
Современные молекулярно-прикладные подходы к конструированию корректоров нарушений микробной экологии человека Сестринский процесс. Технология сестринского ухода
Сестринский процесс. Технология сестринского ухода Стационарды алмастыратын көмек
Стационарды алмастыратын көмек Спазмофилия
Спазмофилия Лабораторная диагностика воздушно-капельных инфекций
Лабораторная диагностика воздушно-капельных инфекций Здоровье мужчин и женщин зрелого возраста
Здоровье мужчин и женщин зрелого возраста Топография поясничной области и забрюшинного пространства. Операции на почках и мочеточниках
Топография поясничной области и забрюшинного пространства. Операции на почках и мочеточниках Опухоли слезных органов
Опухоли слезных органов Патогенные и условно-патогенные анаэробы, общая характеристика. Возбудители анаэробной инфекции, столбняка, ботулизма
Патогенные и условно-патогенные анаэробы, общая характеристика. Возбудители анаэробной инфекции, столбняка, ботулизма 2020 ESC Guidelines for the management of acute coronary syndromes
2020 ESC Guidelines for the management of acute coronary syndromes Патогенное действие на организм ионизирующей радиации
Патогенное действие на организм ионизирующей радиации Современные аспекты патогенеза болезни Паркинсона
Современные аспекты патогенеза болезни Паркинсона